Community Health Improvement Planning
40
COMMUNITY HEALTH IMPROVEMENT PLANNING Theresa Green • Director of Community Health Policy and Education Center for Community Health, URMC • Faculty, Public Health Sciences Department
Transcript of Community Health Improvement Planning

COMMUNITY HEALTH
IMPROVEMENT
PLANNING Theresa Green
• Director of Community Health Policy and Education
Center for Community Health, URMC
• Faculty, Public Health Sciences Department

URMC Core Missions
2
1. Education
2. Research
3. Patient Care
4. Community Health (2004)
In 2006, Center for Community Health was established to
further advance the community health mission
“that the skills and talents be used
to make Rochester the healthiest
community in the world.”
- George Eastman

Comprehensive Approach to
Community Health
3
Provide community services and conduct community based
research, in order to
• INFORM policy makers and community about local health
challenges,
• EVALUATE the effectiveness of interventions, and
• SERVE as a foundation for evidence-based practices to
improve health and overall quality of life.
URMC Strategic Plan 2007-2012

Center for Community Health:
Staff, Faculty, Resources
• Over 60 full time staff
• Nancy (Nana) M. Bennett, MD, MS
Director, Center for Community Health
Professor of Medicine and of Public Health Sciences
• Five full time faculty – 30 secondary appointments
4
• 46 Prince Street
• Library and 2 conference rooms
• 2 exam rooms
• Teaching kitchen and physical
activity space

History of ‘Community Benefits’ • Commissioner of Health’s statewide mission to improve
the health of all New Yorkers; Prevention Agenda towards
the Healthiest State
• In April 2008, Commissioner called for hospital to
collaborate for community health assessment and
planning and to document those efforts in a hospital’s
Community Service Plan (CSP).
• Asked hospitals to work together with their community
partners, including local health departments, to address
the state’s Prevention Agenda

History
• New York Local Health Departments (LHDs) instructed to
participate in this process and to record their efforts in
their Community Health Assessments (CHA) and
Municipal Public Health Service Plans
• Hospital Community Service 3-year Plans were due in
2009 and updates were due in 2010, 2011, and 2012

Collaboration in Monroe County
• Monroe County successfully petitioned to complete a
JOINT Community Service Plan for Monroe County
• Partners:
• Strong Memorial Hospital - URMC
• Highland Hospital - URMC
• Lakeside Health System
• Rochester General Health System
• Unity Health System
• Monroe County Department of Public Health
• Finger Lakes Health System Agency
• Center for Community Health


New York 2013
• New York Health Commissioner Dr. Shah has asked local
health departments and hospitals to work together with
community partners to assess the health challenges in
communities, identify local priorities and develop and
implement plans to address them.
• Addressing at least two priorities in the new
2013 Prevention Agenda. At least one of
these priorities should address a health
disparity.

Prevention Agenda
• The Prevention Agenda vision is:
New York as the Healthiest State in the Nation.
• The plan features five priority areas:
• Prevent chronic diseases
• Promote healthy and safe environments
• Promote healthy women, infants and children
• Promote mental health and prevent substance abuse
• Prevent HIV, sexually transmitted diseases,
vaccine-preventable diseases and
healthcare-associated Infections
http://www.health.ny.gov

Meanwhile, Affordable Care Act
• New 501(r) Requirements
• Community Needs Assessment
• Financial Assistance Policy
• Limits on Charges
• Collections
• Apply to 501(c)(3) hospitals
• Requirements are mandatory and tax exemption depends
on compliance
• Reported in Schedule H (Form 990)

Community Health Needs Assessment
(CHNA)
Each hospital is required to conduct a community health
needs assessment:
• At least once every three years
• Includes input from individuals who represent the broad
interests of the community, including those with special
knowledge or expertise in public health
• Adopt implementation strategy to meet identified needs
• Make the assessment widely available to the public
• IRS due spring 2013 for Strong

IRS/NY Reporting Requirements
• Community Health (Needs) Assessment
• Description of the community
• Summary of assets and resources in community
• Documentation of the process for data and community input
• Identification of the main health challenges facing the community
• Community Health Improvement Plan
“Address needs identified in the CHNA?”
• Identify 2 priority areas from prevention agenda
• Identify process for setting priorities including community input
• Identify goals and objectives, time-framed targets for 5-year plan
• Description of strategies and evidence-based practices
• Identify needs NOT addressed and state why

14
CHNA – Assets and Resources

CHNA – Data
• Monroe County Adult Health Survey (AHS)
• Fourth survey of health risks and behaviors of adults in fall 2012
(2006, 2000, and 1997)
• Countywide random digit dial telephone survey for 18+year olds
• 1800 responses collected
• ½ in City zip codes
• 140 Latino, 1400 white, 225 African American
• Local information such as the Blood Pressure Registry

% All
residents
% African
Americans
% Latinos % Whites %
Residents
of the
Crescent
Obesity (BMI > 30) 27 39 37 24 36
Diabetes Mellitus 10 20 9 9 13
Hypertension 32 41 19 32 36
High Cholesterol 37 35 26 38 36
Taken from the Monroe County Adult Health Survey, 2006 self report indicators
Adult Health Survey 2006
(Monroe County Residents)

% All
residents
% African
Americans
% Latinos % Whites %
Residents
of the
Crescent
No past month
leisure time activity
15 33 36 11 27
Recommended
Physical Activity
53 46 43 54 42
Nutrition-5 +
fruit/vegs/day
21 12 10 22 13
Nutrition-most often
use whole milk
10 28 24 5 25
Nutrition-fast food
usually/almost
always
18 35 25 15 27
Tobacco use-
current
18 27 34 16 28
Monroe County Residents
Taken from the Monroe County Adult Health Survey, 2006 self report indicators

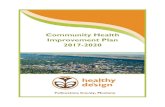
County Health Rankings 2013
www.countyhealthrankings.org
Even though our clinical
care score is very high,
our health outcomes
scores are low – maybe
due to socio-economic,
behaviors and
environmental factors?
Monroe County:
Results of the 2013
County Health
Rankings for New
York (62 counties)
26
43
30
9
33
23
33
43
18

Other sources of Data - NYS
• Mortality and natality data: New York State birth and death files
• Hospitalization data: Statewide Planning and Research Cooperative Systems (SPARCS) files, based on hospital discharges
• Disease and condition specific data: Department of Health disease registries, including cancer, AIDS/HIV, communicable disease, rabies, tuberculosis and sexually transmitted disease
• Program-based data: WIC program, Youth Tobacco Survey, Childhood Lead Poisoning Prevention Program, and Heavy Metals Registry
• National survey data: Behavioral Risk Factor Surveillance System (BRFSS) and Youth Risk Behavior Survey (YRBS)
• Pregnancy Risk Assessment Monitoring System (PRAMS): Prevalence of Smoking During Pregnancy
• Youth Tobacco Survey: Use of Cigarettes Among Middle and High School Students

New York Tracking PH Priority Indicators
http://www.health.ny.gov/prevention/prevention_agenda/
indicators/county/monroe.htm

Monroe County “Problem Areas”
Indicator US NYS Monroe Cnty
% Cigarette smoking in adults 21.2% 18.1% 19.6% (2009)
Lung Cancer Incidence – Male per 100K 76.4 75.8 80.6
Lung Cancer Incidence – Fem per 100K 52.7 53.9 59.7
Infant Mortality per 1,000 live births 6.1 5.1 7.7
Pregnancy rate 15-17 per 1,000 39.5 28.5 33.2
% of Adults who are obese 27.8% 24.5% 31.7% (2009)
% WIC mothers breastfeeding @ 6 mths 25.1% 38.8% 18.9%
Stroke mortality per 100,000 39.0 27.5 36.0
Gonorrhea case rate (per 100K) 100.8 94.3 180.7
http://www.health.ny.gov/prevention/preven
tion_agenda/indicators/county/monroe.htm

Leading Causes of Death by County, New York State, 2009
County and # of
Deaths
#1 Cause of Death
and # of Deaths
#2 Cause of Death
and # of Deaths
#3 Cause of Death
and # of Deaths
#4 Cause of Death
and # of Deaths
#5 Cause of Death
and # of Deaths
Age-adjusted
Death Rate
Age-adjusted
Death Rate
Age-adjusted
Death Rate
Age-adjusted
Death Rate
Age-adjusted
Death Rate
Monroe Cancer Heart Disease Stroke
Chronic Lower
Respiratory
Diseases (CLRD)
Pneumonia and
Influenza
1,492 1,434 326 267 185
Total: 6,168 176 per 100,000 157 per 100,000 36 per 100,000 30 per 100,000 20 per 100,000
Ontario Cancer Heart Disease Stroke
Chronic Lower
Respiratory
Diseases (CLRD)
Unintentional Injury
231 226 52 51 31
Total: 949 175 per 100,000 169 per 100,000 39 per 100,000 39 per 100,000 25 per 100,000
Orleans Heart Disease Cancer
Chronic Lower
Respiratory
Diseases (CLRD)
Stroke Unintentional Injury
127 97 24 19 11
Total: 408 256 per 100,000 194 per 100,000 50 per 100,000 39 per 100,000* 25 per 100,000*
Wayne Cancer Heart Disease
Chronic Lower
Respiratory
Diseases (CLRD)
Stroke Liver Disease
193 184 59 35 32
Total: 780 182 per 100,000 175 per 100,000 59 per 100,000 33 per 100,000 31 per 100,000

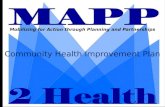
Cancer and Heart Disease: Number of Deaths
Monroe County, 1994-2010
0
500
1000
1500
2000
2500
Num
ber
of D
eath
s
Cancer Heart
Source: Vital Records, MCDPH

Ultimate Priority Areas…
24

Smoking
• Current smoking rate among adults is 16%, similar to
statewide rate of 18%, but…
2012 City Suburbs
Smoking rate 24.9 (21.0-28.8) 12.7 (9.6-15.7)

Infant Mortality (7.7 for County, but…) Monroe County By Race and Latino Origin, 2008-2010
0
2
4
6
8
10
12
14
16
18
African American Latino White
Rate
per
1,0
00 B
irth
s
Source: Vital Records, MCDPH

CHNA – Community Input
GOAL: to improve the health of the
citizens of Monroe County by aligning
community resources to focus on selected
priorities for action

Health Action • Going strong since 1995
• Steering committee establishes subcommittees that review data, and convene community forums to set action priorities.
• Health “report cards” are available • Maternal Child Health Report Card -2011
• Adolescent Health Report Card – 2012
• Adult/Older Adult Health Report Card – 2008 (slated for 2013)
• Community Action Priorities for Adult/Older Adult: • Increase Physical Activity and Improve Nutrition
• Improve Prevention and Management of Chronic Disease
• Improve Mental Health (reduce violence among adults and elder abuse among older adults).

http://www2.monroecounty.gov/health-healthdata.php#surveys

CHNA - Main Health Challenges
CANCER – HEART DISEASE – STROKE
Chronic Disease, especially HTN
Obesity, smoking, social
determinants of health
Not addressed: Infant mortality, STDs, teen pregnancy

CHIP – Process for Prioritization and
Community Input IMPORTANCE (How important is this goal?)
Number affected
How much disability/illness this will prevent
Long term impact on health
LIKELIHOOD of IMPACTFUL SUCCESS
What is the likelihood that setting this goal will
result in substantial health improvements in 3-5 years?
COMMUNITY SUPPORT
Is there willingness on the part of community
leaders and partner organizations, and
residents to address this goal?
HOSPITAL SUPPORT
How likely are hospital leaders to strongly
support this initiative and dedicate resources to
its success?
LEVEL of CURRENT COMPLEMENTARY ACTIVITY
What is the level of community plans, activities and
resources already directed to address similar goals?
What is the potential to address health disparity
OVERALL RANK

CHIP – Public Input and Collaboration
• Group discussion and prioritization
• Director of Perioperative Services - Lakeside
• Director of Marketing and Public Relations - RGH
• Chief Operating Officer - Unity
• Chief Operating Officer – Strong - designated CCH COO
• Director of Public relations - Highland
• Director of Community Engagement FLHSA
• Public Health Program Coordinator MCDPH
• Balance between hospital missions and public health

CHIP – Priority Areas
• Identify 2 Priority Areas from Prevention Agenda:
• Prevent Chronic Disease
• Promote a healthy and safe environment
• Promote healthy women, infants and children
• Promote mental health and prevent substance abuse
• Prevent HIV, STD, Vaccine preventable diseases and HAI
PREVENT
CHRONIC DISEASE

CHIP – Evidence Based Strategies
• NY PREVENTION AGENDA: Increasing physical activity, improving nutrition, and decreasing tobacco use form the core of the Preventing Chronic Disease action plan
Three key areas:
1. Health Promotion activities
2. Early detection opportunities
3. Successful management strategies

Focus Area 1:
Reduce obesity in children and adults • Goal 1.1: By December 31, 2017, reduce the percentage
of adults ages18 years and older who are obese by 5% from 27% (Monroe County AHS, 2009) to 22% among all adults.
• Goal 1.2: Expand the role of public and private employers in obesity prevention • Objective 1.2.1. By December 31, 2017 increase by 10% the
percentage of small to medium worksites that offer a comprehensive worksite wellness program for all employees and that is fully accessible to people with disabilities
• Objective 1.2.2. By December 31, 2017 expand the worksite wellness package at each hospital system by 3 effective interventions, as measured by increase in each hospital systems score on the Monroe County worksite wellness index

Intervention for Consideration
• Implement evidence-based wellness programs for all
public and private employees, retirees and their
dependents through collaboration with unions, health
plans and community partnerships that include but are not
limited to increased opportunities for physical activity;
access to and promotion of healthful foods and
beverages; and health benefit coverage and/or incentives
for obesity prevention and treatment, including
breastfeeding support (IOM Obesity Prevention)
• Use the worksite wellness index (FLHSA)

Focus Area 2: Reduce illness, disability and
death related to tobacco use and second hand
smoke exposure
• Goal 2.1. Promote tobacco use cessation, especially
among low SES populations and those with poor mental
health
• Objective 2.1.1.By December 31, 2017, increase the number of
unique callers from Monroe County to the NYS Smokers’ Quitline
by 20%, from *** (2012) to *** annually. (Data source: NYS
Smokers’ Quitline Annual Report)
• Through the CMMI medical homes to start
• Objective 2.1.2. By December 31, 2017, increase the number of
employers that provide insurance benefits for tobacco dependence
treatment, counseling and medications by 10%. (Baseline?)

Focus Area 3: Increase access to high quality chronic
disease preventive care and management in both
clinical and community settings
• Goal 3.1. Promote use of evidence-based care to
manage chronic disease.
• Objective 3.1.1. By December 31, 2017, increase the percentage
of adults ages 18+ years with hypertension who have controlled
their blood pressure (below 140/90) by 10% from **% for residents
in the blood pressure registry to **%
• Interventions: BP Ambassadors, BPAP, worksite demonstrations,
practice improvement consultants
• Objective 3.1.2. By December 31, 2017, provide 6 primary care
medical home practices serving at-risk patients with a meaningful,
comprehensive interface between care managers and community
resources
• Intervention: CMMI grant and CHW with electronic database

Next Steps:
• Clarify improvement strategies and performance measures
• Description of strategies and evidence-base
• Each hospitals’ specific role and responsibility
• Identify needs not addressed and why
• Board approval of CHNA and CHIP (May 2013)
• Disseminate plans community wide

Thank you!
•Theresa Green, AA-C, MBA Director of Community Health Policy and Education
Center for Community Heath URMC