Childhood Bronchial Asthma
115
Mona Mostafa El-Falaki Mona Mostafa El-Falaki Professor of Pediatric Allergy & Professor of Pediatric Allergy & Pulmonology Pulmonology Head of Pediatric Allergy & Head of Pediatric Allergy & Pulmonology Unit Pulmonology Unit
-
Upload
ahmed-el-halawany -
Category
Documents
-
view
52 -
download
5
Transcript of Childhood Bronchial Asthma

Mona Mostafa El-FalakiMona Mostafa El-FalakiProfessor of Pediatric Allergy & Pulmonology Professor of Pediatric Allergy & Pulmonology Head of Pediatric Allergy & Pulmonology Unit Head of Pediatric Allergy & Pulmonology Unit
Cairo UniversityCairo University

Increasing Prevalence of Asthma in Increasing Prevalence of Asthma in Children/AdolescentsChildren/Adolescents
00 55 1010 1515 2020 2525 3030 3535
19921992198219821989198919751975199219921982198219941994198919891992199219821982199219921982198219911991197919791989198919661966FinlandFinland
(Haahtela (Haahtela et alet al))
SwedenSweden(Aberg (Aberg et alet al))
JapanJapan(Nakagomi (Nakagomi etet al al))
ScotlandScotland(Rona (Rona et alet al))
UKUK(Omran (Omran et alet al))
USAUSA(NHIS)(NHIS)
New ZealandNew Zealand(Shaw (Shaw et alet al))
AustraliaAustralia(Peat (Peat et alet al))
{{
Prevalence (%)Prevalence (%)
{{
{{{{{{{{{{{{
WorldwideWorldwide prevalence rates are increasing, on average, by 50% / decade. prevalence rates are increasing, on average, by 50% / decade. ( (WHO, Bronchial Asthma Fact Sheet, 2000)

The prevalence of pre-school asthma is on the rise. • The general prevalence of asthma in children aged 0 to 17 years constitutes about 33% of the entire asthmatic patient population.
•The prevalence of asthma in children 4 years of age and younger rose 160% from 1980-1994
• In children aged 2 to 5 years 100,000 new cases are diagnosed each year.
CDC. Surveillance for Asthma--United States, 1960-1995 (CDC Surveillance Summaries). MMWR. 1998;47(SS-1):1-26).Yunginger JW et al. Community-based study of the epidemiology of asthma. Am Rev Respir Dis 1992;146:888-894.

Silverstein MD et al., N. Engl J Med ,1994 Silverstein MD et al., N. Engl J Med ,1994
Distribution of Ages at the Onset of Asthma Among 2499 Distribution of Ages at the Onset of Asthma Among 2499 Residents of Rochester, MinnesotaResidents of Rochester, Minnesota
50% < 3 years80% < 5 years

Burden of Asthma – One of the Most Burden of Asthma – One of the Most Common Chronic Illnesses in ChildrenCommon Chronic Illnesses in Children
Asthma
Affects ~5 million children <18 years in the US
Number 1 chronic illness
causing school absences
658,000 emergency department visits
for asthma in US children<15 years in 1999
AAAAI. Pediatric Asthma: Promoting Best Practice University of Rochester 2004; American Lung Association. http://www.lungusa.org/site/pp.asp?c=dvLUK9O0E&b=44352.
Estimated annual costof treatment $3.2 billion
14 million school days
lost due to asthma
Interferes withactivities

19641964 19891989 19941994
0
5
10
15
20
25
% D
iagn
osed
AsthmaEczemaRhinitis
CDC 1996CDC 1996
(n=2743) (n=4003) (n=4034)

4 or more children are likely to have asthmaand/or other allergies
In a classroom of 30 children,

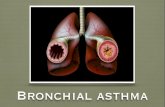
Inflammation Remodeling

Mucus Plug


Airway mucosal oedemaAirway mucosal oedema

Definition of AsthmaDefinition of Asthma
Asthma is a chronic inflammatory disorder of the Asthma is a chronic inflammatory disorder of the airways in which many cells and cellular elements play a airways in which many cells and cellular elements play a role role
Chronic inflammation causes an associated increase in Chronic inflammation causes an associated increase in airway hyperresponsiveness that leads to recurrent airway hyperresponsiveness that leads to recurrent episodes of wheezing, breathlessness, chest tightness, and episodes of wheezing, breathlessness, chest tightness, and coughing, particularly at night or in the early morning coughing, particularly at night or in the early morning
These episodes are usually associated with widespread These episodes are usually associated with widespread but variable airflow obstruction that is often reversible but variable airflow obstruction that is often reversible either spontaneously or with treatmenteither spontaneously or with treatment

Histopathologic featuresHistopathologic features
–Denuded respiratory epithelium Denuded respiratory epithelium –Inflammatory cell infiltrationInflammatory cell infiltration–EdemaEdema–Vessel dilatation &congestionVessel dilatation &congestion–Airway thickeningAirway thickening
Busse WW, Lemanske RF. NEJM 2001;344(5):350-62
No asthma
Mild asthma
Chronic inflammation
Structural changes

Airway Remodeling in AsthmaAirway Remodeling in Asthma
Airway wall thickeningAirway wall thickening Subepithelial collagen deposition (Lamina reticularis)Subepithelial collagen deposition (Lamina reticularis) Smooth muscle hyperplasia and hypertrophySmooth muscle hyperplasia and hypertrophy Mucus metaplasiaMucus metaplasia Epithelial hypertrophyEpithelial hypertrophy Vascular abnormalitiesVascular abnormalities
Elias JA et al. J Clin Invest 1999; 104:1001Elias JA et al. J Clin Invest 1999; 104:1001




Airway inflammation in asthmaAirway inflammation in asthma
AsthmaticAsthmaticNormalNormalP Jeffery, in: Asthma, Academic Press 1998

Vascular Adhesion and Margination of Inflammatory Vascular Adhesion and Margination of Inflammatory Cells in Allergic Airways InflammationCells in Allergic Airways Inflammation
Chang et al., 1997Chang et al., 1997


Allergic Airways InflammationAllergic Airways Inflammation
EarlyEarly LateLate
Ohkawara, Y. et al., 1997Ohkawara, Y. et al., 1997


Creola bodiesCreola bodiesCharcot –Leyden CrystalsCharcot –Leyden Crystals



Normal Normal Rapid Rapid Bronchospasm Bronchospasm
Direct acting Direct acting mediators mediators
Late, sustained Late, sustained reaction reaction
Subacute/chronic Subacute/chronic inflammation inflammation
EosinophilsEosinophils NeutrophilsNeutrophils MonocytesMonocytes Epithelial cells Epithelial cells LymphocytesLymphocytes Cytokines Cytokines


Early Asthmatic Early Asthmatic responseresponse
Late asthmatic Late asthmatic responseresponse
Onset Onset <10 min<10 min3-4 hrs3-4 hrsPeak Peak 10-30 min10-30 min8-12 hrs8-12 hrs
Duration Duration 1.5-3 hrs1.5-3 hrs> 12 hrs> 12 hrs
Enhanced resp.Enhanced resp.+/-+/-++
Treatment responseTreatment response ββ-agonists-agonists CromolynCromolyn Corticosteroids Corticosteroids
ReversesReversesPremed-inhibitsPremed-inhibitsPremed-inhibitsPremed-inhibitsPremed no effectPremed no effect
Partially reversesPartially reversesPremed-no effectPremed-no effectPremed-inhibitsPremed-inhibitsPremed-inhibitsPremed-inhibits


Is it Asthma?Is it Asthma?
Recurrent episodes of wheezingRecurrent episodes of wheezing Troublesome cough at nightTroublesome cough at night Cough or wheeze after exerciseCough or wheeze after exercise Cough, wheeze or chest tightness after Cough, wheeze or chest tightness after
exposure to airborne allergens or exposure to airborne allergens or pollutantspollutants
Colds “go to the chest” or take more than Colds “go to the chest” or take more than 10 days to clear10 days to clear

To establish a diagnosis of asthma, the To establish a diagnosis of asthma, the clinician should determine that:clinician should determine that: Episodic symptoms of airflow obstruction Episodic symptoms of airflow obstruction
(with symptoms free intervals).(with symptoms free intervals). Airflow obstruction is at least partially Airflow obstruction is at least partially
reversible.reversible. A number of known risk factors are presentA number of known risk factors are present Alternative diagnoses are excluded. Alternative diagnoses are excluded. When the child responds to anti-asthma When the child responds to anti-asthma
therapytherapy

Asthma DiagnosisAsthma Diagnosis
History and patterns of symptomsHistory and patterns of symptoms
Physical examinationPhysical examination
Measurements of lung functionMeasurements of lung function
Measurements of allergic status to identify risk Measurements of allergic status to identify risk factorsfactors






Markers of atopyMarkers of atopy– Positive FHPositive FH– Other atopic manifestationsOther atopic manifestations– InvestigationInvestigation
• +ve PST+ve PST Serum total IgESerum total IgE specific IgEspecific IgE• Perpheral blood and tissue eosinophiliaPerpheral blood and tissue eosinophilia• Inflammatory markers e.g. S-ECPInflammatory markers e.g. S-ECP• T-cell profile Th1 versus Th2T-cell profile Th1 versus Th2
Diagnosis of Bronchial Asthma (cont.)Diagnosis of Bronchial Asthma (cont.)

TechniquesTechniques

Allergy Prick Skin TestAllergy Prick Skin Test
AA BB CC DD

Number of allergensNumber of allergensQuality of allergens Quality of allergens
((purification + purification + standardizationstandardization))
Patient exposure Patient exposure ((residence + occupation residence + occupation etcetc.).)
Quality control (Quality control (positive + positive + negative controlnegative control))
Interpretation + clinical Interpretation + clinical correlation.correlation.



Silver birchSilver birch AlderAlder HazelHazel

Dust miteDust mite Cat hairCat hair
Mite legsMite legsCockroachCockroach



Early Wheezers:Predictive Index of Developing Early Wheezers:Predictive Index of Developing AsthmaAsthma
3 Episodes of Wheezing During Previous Year
PLUSPLUS
OrOrOne Major
Criteria
• Parent with asthma
• Atopic dermatitis
• Aeroallergic sensitivity
Two Minor
Criteria
• Food sensitivity
• Peripheral eosinophilia
• Wheezing not related to infection
Castro-Rodriguez J et al. Am J Resp Crit Care Med. 162:1403-6, 2001
If + , then 65% likelihood of persistent wheezingIf + , then 65% likelihood of persistent wheezingIf – , then 92% likelihood of not developing clinical asthmaIf – , then 92% likelihood of not developing clinical asthma

Differential Diagnosis of Asthma in Differential Diagnosis of Asthma in ChildrenChildren
Congenital malformationCongenital malformation (Laryngeal web ,cyst ,stenosis ,TOF ,vascular (Laryngeal web ,cyst ,stenosis ,TOF ,vascular ring ) ring )
BronchiolitisBronchiolitis BronchietasisBronchietasis Bronchopulmonary dysplasiaBronchopulmonary dysplasia LaryngotracheobronchitisLaryngotracheobronchitis LaryngotracheobronchomalaciaLaryngotracheobronchomalacia Immunodeficiency syndromesImmunodeficiency syndromes Primary ciliary dyskinesiaPrimary ciliary dyskinesia
Rhino-sinusitisRhino-sinusitis Cystic fibrosisCystic fibrosis Foreign bodyForeign body Gastro-esophageal refluxGastro-esophageal reflux Congenital heart diseaseCongenital heart disease Chronic respiratory Chronic respiratory
infectioninfection Recurrent aspiration Recurrent aspiration
syndromessyndromes Vocal cord dysfunctionVocal cord dysfunction

An atypical history may include:An atypical history may include:– Onset of symptoms in the neonatal periodOnset of symptoms in the neonatal period– History of ventilatory support in the neonatal History of ventilatory support in the neonatal
period.period.– Intractable wheezing that is unresponsive to Intractable wheezing that is unresponsive to
bronchodilators.bronchodilators.– Wheezing associated with feeding; vomitingWheezing associated with feeding; vomiting– The sudden onset of coughing or choking The sudden onset of coughing or choking – StridorStridor– Steatorrhea Steatorrhea

Additional or Alternative Diagnosis:Additional or Alternative Diagnosis:– Failure thriveFailure thrive– ClubbingClubbing– A cardiac murmurA cardiac murmur– No reversibility of airflow obstruction after No reversibility of airflow obstruction after
administration of a bronchodilatoradministration of a bronchodilator– A focal or persistent finding on chest radiograph.A focal or persistent finding on chest radiograph.


Cough variant asthmaCough variant asthma Hypersecretory asthmaHypersecretory asthma Exercise induced asthmaExercise induced asthma Subclinical early asthmaSubclinical early asthma Severe asthmaSevere asthma





PathogenesisPathogenesis ManagementManagement Nonpharmacological Nonpharmacological therapy: therapy:
– patient educationpatient education– Environmental controlEnvironmental control– ImmunotherapyImmunotherapy
Genetic Genetic factorsfactors
Anti-inflammatory therapyAnti-inflammatory therapy
Bronchodilator therapyBronchodilator therapy
ASTHMAASTHMAAirflow obstructionAirflow obstruction
AirwayAirwayHyper-responsivenessHyper-responsiveness
Bronchial smooth Bronchial smooth muscle contraction muscle contraction bronchial inflammationbronchial inflammation
Environmental factorsEnvironmental factors – Air pollutionAir pollution– AllergensAllergens– Cigarette smokingCigarette smoking– Viral infectious agentsViral infectious agents

Six-part Asthma Management ProgramSix-part Asthma Management Program
Control of AsthmaControl of Asthma
Minimal (ideally no) chronic symptoms Minimal (infrequent) exacerbations No emergency visits Minimal (ideally no) need for “as needed” use of
β2-agonist No limitations on activities, including exercise PEF circadian variation of less than 20 percent (Near) normal PEF Minimal (or no) adverse effects from medicine

Recommendations for the Recommendations for the primary prevention of allergyprimary prevention of allergy
Unspecific Measures:Unspecific Measures:– Non traumatic deliveryNon traumatic delivery
– No exposure to tobacco smokeNo exposure to tobacco smoke
– Reduce air pollutionReduce air pollution
– Breast feeding for as long as possibleBreast feeding for as long as possible[kjellman, NIM, 1993 & ACI News 5/5: 131-134] [kjellman, NIM, 1993 & ACI News 5/5: 131-134]


When you light your cigarette in
pregnancy, you're not the only one who
smokes – Your baby does too!



Recommendations for the Recommendations for the primary prevention of allergyprimary prevention of allergy
Allergen avoidance:Allergen avoidance:– Reduce exposure to major allergensReduce exposure to major allergens– Consider maternal elimination diet during breast Consider maternal elimination diet during breast
feedingfeeding– No “solid” foods for the first 6 monthsNo “solid” foods for the first 6 months– Egg and fish only after 12 months of age.Egg and fish only after 12 months of age.– Extensively hydrolyzed milk-based formula as Extensively hydrolyzed milk-based formula as
“back-up”.“back-up”.– Avoid day-care centers during infancy (risk of Avoid day-care centers during infancy (risk of
infection).infection).





Asthma Management GuidelinesAsthma Management Guidelines
National Heart Lung and Blood Institute (NHLBI) and National National Heart Lung and Blood Institute (NHLBI) and National Institute of Health (NIH) National Asthma Education Prevention Institute of Health (NIH) National Asthma Education Prevention Program (NAEPP). EPR3 (2007).Program (NAEPP). EPR3 (2007).
www.nhlbi.nih.govwww.nhlbi.nih.gov Global Initiative for Asthma (GINA, up dated 2007).Global Initiative for Asthma (GINA, up dated 2007).
NHLBI & WHONHLBI & WHO
www.ginasthma.org.www.ginasthma.org. PRACTALL Consensus ReportPRACTALL Consensus Report . .
(EAACI / AAAAI) Allergy 2008(EAACI / AAAAI) Allergy 2008
Treatment should be tailored for each child within theTreatment should be tailored for each child within the framework of international guidelinesframework of international guidelines

The choice of treatment should be guided by:
Level of asthma severity only for initiating therapy Level of asthma control
Current treatment
Pharmacological properties and availability of the various forms of asthma treatment
Economic considerations
Asthma Management and Prevention ProgramAsthma Management and Prevention Program
Assess, Treat and Monitor AsthmaAssess, Treat and Monitor Asthma

Component 4: Asthma Management and Prevention Program
Controller Medications Inhaled glucocorticosteroids. Leukotriene modifiers - LTRA ( montelukast ). Long-acting inhaled β2-agonists – LABA (Salmeterol-
Formeterol). Long-acing theophylline. Cromones. Long-acting oral β2-agonists. Systemic glucocorticosteroids. Anti-IgE.

Long-Long-TermTerm, , Controller Controller MedicationsMedications
Advair

SpacersSpacers


Don’t give me an inhaler; Its addictive !!!

Classification of SeverityClassification of Severity
CLASSIFY SEVERITYClinical Features Before Treatment
SymptomsSymptoms NocturnalNocturnalSymptomsSymptoms FEVFEV1 1 or PEFor PEF
STEP 4STEP 4Severe Severe
PersistentPersistentSTEP 3STEP 3
Moderate Moderate PersistentPersistentSTEP 2STEP 2
Mild Mild PersistentPersistent
STEP 1STEP 1IntermittentIntermittent
ContinuousContinuousLimited physical Limited physical activityactivityDailyDailyAttacks affect activityAttacks affect activity
> 1 time a week > 1 time a week but < 1 time a daybut < 1 time a day
< 1 time a week< 1 time a week
Asymptomatic and Asymptomatic and normal PEF between normal PEF between attacksattacks
FrequentFrequent
> 1 time week> 1 time week
> 2 times a month> 2 times a month
2 times a month2 times a month
60% predicted60% predictedVariability > 30%Variability > 30%
60 - 80% predicted 60 - 80% predicted Variability > 30%Variability > 30%
80% predicted80% predictedVariability 20 - 30%Variability 20 - 30%
80% predicted80% predictedVariability < 20%Variability < 20%
The presence of one feature of severity is sufficient to place patients in that The presence of one feature of severity is sufficient to place patients in that category.category.

Levels of Asthma Levels of Asthma ControlControl
CharacteristicCharacteristicControlled
(All of the following)Partly controlled
(Any present in any week)Uncontrolled
Daytime symptomsDaytime symptomsNone (2 or less / week)More than twice / week
3 or more features of partly controlled asthma present in any week
Limitations of activitiesLimitations of activitiesNoneAny
Nocturnal symptoms / Nocturnal symptoms / awakeningawakeningNoneAny
Need for rescue / Need for rescue / “reliever” treatment“reliever” treatmentNone (2 or less / week)More than
twice / week
Lung function Lung function (PEF or FEV(PEF or FEV11))
Normal< 80% predicted or
personal best (if known) on any day
ExacerbationExacerbationNoneNone One or more / year 1 in any weekOne or more / year 1 in any week

controlled
partly controlled
uncontrolled
exacerbation
LEVEL OF CONTROLLEVEL OF CONTROL
maintain and find lowest controlling step
consider stepping up to gain control
step up until controlled
treat as exacerbation
TREATMENT OF ACTIONTREATMENT OF ACTION
TREATMENT STEPSREDUCE INCREASE
STEP1
STEP2
STEP3
STEP4
STEP5
RED
UC
EIN
CR
EASE







Estimate Comparative Daily Dosages for Inhaled Glucocorticosteroids by Age
Drug Low Daily Dose (g) Medium Daily Dose (g) High Daily Dose (g) > 5 y Age < 5 y > 5 y Age < 5 y > 5 y Age < 5 y
Beclomethasone 200-500 100-200 >500-1000 >200-400 >1000 >400
Budesonide200-600 100-200 600-1000 >200-400 >1000 >400
Budesonide-Neb Inhalation Suspension
250-500 >500-1000 >1000
Ciclesonide 80 – 160 80-160 >160-320 >160-320 >320-1280 >320
Flunisolide500-1000 500-750 >1000-2000 >750-1250 >2000 >1250
Fluticasone100-250 100-200 >250-500 >200-500 >500 >500
Mometasone furoate200-400 100-200 > 400-800 >200-400>800-1200 >400
Triamcinolone acetonide400-1000 400-800 >1000-2000 >800-1200 >2000 >1200


Part 4: Establish Medication Plans for Long-Part 4: Establish Medication Plans for Long-Term Asthma Management in Infants and Term Asthma Management in Infants and
ChildrenChildren
Long-term treatment with inhaled glucocorticosteroids (ICS) has not been shown to be associated with any increase in osteoporosis or bone fracture.
Studies including a total of over 3,500 children treated for periods of 1 – 13 years have found no sustained adverse effect of inhaled ICS on growth.

Six-part Asthma Management ProgramSix-part Asthma Management Program
Part 6: Provide Regular Part 6: Provide Regular Follow-up CareFollow-up Care
Continual monitoring is essential to assure thattherapeutic goals are met. Frequent follow-up visitsare necessary to review: Home PEF and symptom records Techniques in use of medications Risk factors and their controlOnce asthma control is established, follow-upvisits should be scheduled (at 1 to 6 month intervalsas appropriate)



Asthma Action Plan
Adapted from NHLBI Expert Panel Guidelines (EPR-3)http://www.health.state.ny.us/diseases/asthma/pdf/4850.pdf
• Patient instrument • Personalized• Zone system• Actions based on symptoms• When and how to get help• Influence on outcomes controversial


Part 4: Long-term Asthma Management
Pharmacologic Therapy
Reliever Medications: Short-acting inhaled β2-agonists
Systemic glucocorticosteroids Anticholinergics Methylxanthines
Short-acting oral β2-agonists


Quick Relief MedicationsQuick Relief MedicationsLoosens your muscles & stops the wheezing
Albuterol for Nebulizer


PULSE OXIMETRY, PaO2, PaCO2, PEFR:PULSE OXIMETRY, PaO2, PaCO2, PEFR:

Establish Plans for Managing Establish Plans for Managing ExacerbationsExacerbations
Primary therapies for exacerbations:Primary therapies for exacerbations: Repetitive administration of rapid-acting Repetitive administration of rapid-acting
inhaled inhaled ββ22-agonist-agonist Early introduction of systemic Early introduction of systemic
glucocorticosteroidsglucocorticosteroids Oxygen supplementationOxygen supplementationClosely monitor response to treatmentClosely monitor response to treatmentwith serial measures of lung functionwith serial measures of lung function

Emergency Department Management
Acute Asthma
Good Response
Observe for at least 1 hour
If Stable, Discharge to
Home
Initial AssessmentHistory, Physical Examination, PEF or FEV1
Initial TherapyBronchodilators; O2 if needed
Incomplete/Poor Response
Add Systemic Glucocorticosteroids
Good Response
Discharge
Poor Response
Admit to Hospital
Respiratory Failure
Admit to ICU

Dosage of Drugs in Acute Asthma Dosage of Drugs in Acute Asthma Attacks in ChildrenAttacks in Children
Inhaled Inhaled ββ2 2 AgonistAgonist Salbutamol (Ventolin) :Salbutamol (Ventolin) : .Nebulizer solution 0.5%(5mg /ml) Dose: 0.1-0.15 mg/kg/dose (max. 5mg /dose) every 20 min. for 3 Dose: 0.1-0.15 mg/kg/dose (max. 5mg /dose) every 20 min. for 3
doses (minimum dose 1.25 mg /dose)doses (minimum dose 1.25 mg /dose) ..Metered- dose inhaler(100Metered- dose inhaler(100μμg/puff)g/puff)
Dose: 2 inhalations every 5 min. for a total of 12 puffs.Dose: 2 inhalations every 5 min. for a total of 12 puffs. .. IV IV Dose: loading dose 1 Dose: loading dose 1 μμg/kg/min. Maintenance 0.2 g/kg/min. Maintenance 0.2 μμg/kg/min. g/kg/min.
(max. 4 (max. 4 μμg/kg/min). Only in ICU.g/kg/min). Only in ICU. ..Oral solutionOral solution Dose:0.6mg/kg/day divided in3-4 dosesDose:0.6mg/kg/day divided in3-4 doses

Development of Nerves and Smooth Muscle Development of Nerves and Smooth Muscle in Human Fetal Lungin Human Fetal Lung
Sparrow et al., 1999Sparrow et al., 1999
Airway branch from a human fetal lung 18 wk gestationAirway branch from a human fetal lung 18 wk gestation

[[McCray, 1993McCray, 1993]]

Anti-cholinergicsAnti-cholinergics Ipratropium bromide (Atrovent):Ipratropium bromide (Atrovent): .Nebulizer solution 0.025%(0.25mg /ml) Dose: 0.25mg/20min. For 3 doses then every 2-4 hoursDose: 0.25mg/20min. For 3 doses then every 2-4 hours ..Metered- dose inhaler(20Metered- dose inhaler(20μμg/puff)g/puff) Dose: 2-4 inhalations as needed.Dose: 2-4 inhalations as needed.
CorticosteroidsCorticosteroids Methylprednisolone (solu-medrol)Methylprednisolone (solu-medrol)
Dose in severe attacks as emergency management: Dose in severe attacks as emergency management: 2mg/kg iv then 1- 2mg/kg/24h.2mg/kg iv then 1- 2mg/kg/24h.
Prednisolone, PrednisonePrednisolone, Prednisone::
Dose: 1-2mg /kg/day in divided doses oral or ivDose: 1-2mg /kg/day in divided doses oral or iv Hydrocortisone (solu-cortef)Hydrocortisone (solu-cortef) Dose: 5mg/kg/dose every 6h Dose: 5mg/kg/dose every 6h

History of near fatal asthma.History of near fatal asthma. Hospitalization or emergency visit within one year.Hospitalization or emergency visit within one year. Current use or recent withdrawal of oral Current use or recent withdrawal of oral
corticosteroids.corticosteroids. Overdependence on rapidly-acting inhaled beta-2 Overdependence on rapidly-acting inhaled beta-2
agonist.agonist. Psychological problems or denial of asthma or its Psychological problems or denial of asthma or its
severity.severity. Non-compliance with treatment plan.Non-compliance with treatment plan.
Risk Factors for Fatal or Near Risk Factors for Fatal or Near Fatal AsthmaFatal Asthma

Six-part Asthma Management Six-part Asthma Management Program:Program: SummarySummary
Asthma can be effectively controlled, although it Asthma can be effectively controlled, although it cannot be curedcannot be cured
Effective asthma management programs include Effective asthma management programs include education, objective measures of lung function, education, objective measures of lung function, environmental control, and pharmacologic environmental control, and pharmacologic therapytherapy
A stepwise approach to pharmacologic therapy is A stepwise approach to pharmacologic therapy is recommended. The aim is to accomplish the recommended. The aim is to accomplish the goals of therapy with the least possible goals of therapy with the least possible medicationmedication

Thank Thank YouYou

Require symptomatic treatment > 2 times a wk. Have had ≥ 2 exacerbations in 6 months requiring
systemic steroids. Have had > 3 wheezy episodes in the past year that
lasted > 1 day and affected sleep and have risk factors for asthma (intermittent asthma with allergic sensitization).
With intermittent asthma and severe exacerbation are managed as moderately severe asthma.
NAEPP expert panel considers initiation of a controller therapy in infants & young children who:

When Should Cough/Wheeze When Should Cough/Wheeze be Called “Asthma”?be Called “Asthma”?When wheeze/cough becomes recurrentWhen wheeze/cough becomes recurrentWhen other wheeze/cough conditions When other wheeze/cough conditions
have been excludedhave been excludedWhen a number of known risk factors When a number of known risk factors
are presentare presentWhen the child responds to anti-asthma When the child responds to anti-asthma
therapytherapy

PEFR Zones
Red: Below 50% of Personal Best
Yellow: 50% to 80% of Personal Best
Green: 80% to 100% of Personal Best



Component 4: Asthma Management and Prevention Program
Controller Medications Inhaled glucocorticosteroids Leukotriene modifiers - LTRA ( montelukast ) Long-acting inhaled β2-agonists – LABA (Salmeterol-
Formeterol) Long-acing theophylline Cromones Long-acting oral β2-agonists Systemic glucocorticosteroids Anti-IgE

Acute Allergen Induced Airway Remodeling
Phipps et al., AJR Cell Mol. Biol 2004Phipps et al., AJR Cell Mol. Biol 2004