Indirect bronchial provocation tests in childhood asthma
29
University of Groningen Indirect bronchial provocation tests in childhood asthma Kersten, Elin IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2015 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Kersten, E. (2015). Indirect bronchial provocation tests in childhood asthma: Monitoring short-term treatment changes. University of Groningen. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 09-12-2021
Transcript of Indirect bronchial provocation tests in childhood asthma

University of Groningen
Indirect bronchial provocation tests in childhood asthmaKersten, Elin
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2015
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Kersten, E. (2015). Indirect bronchial provocation tests in childhood asthma: Monitoring short-termtreatment changes. University of Groningen.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 09-12-2021

1
2
3
4
5
6
7
8
9
Chapter 8Summary, General Discussion
and Directions for Further Research


Summary and General Discussion 147
8
IndIrECT BronChIal ProvoCaTIon TEsTs
In chapter 1 we describe the current approach to diagnosing, monitoring and treat-ing childhood asthma. We discuss several clinical dilemmas of this approach that are debated in current literature. We postulate that indirect bronchial provocation tests (BPTs) can be used to monitor BHR and airway inflammation. In the following chapters of this thesis we used exercise challenge tests (ECTs) and mannitol tests for short term monitoring of asthmatic children.
The idea that indirect BPTs can be used to monitor airway inflammation is not new. In 2003 the European Respiratory Society task force on indirect airway challenges already concluded: ‘Indirect challenges may reflect acute changes in airway inflammation more closely and be clinically relevant markers to assess the clinical course of asthma.’1 A re-view by Cockcroft and Davis compared the use of direct and indirect BPTs in the clinical assessment of asthma2 and concluded that indirect BPTs should be the challenges of choice for evaluating and monitoring asthma treatment.
BHR to an indirect stimulus has advantages over other parameters used to monitor the response to anti-inflammatory treatment.
Symptoms and lung function are accessible parameters to monitor treatment, but poorly correlate to the underlying disease severity in asthmatic children.3,4 Question-naires to assess asthma control, such as the Asthma Control Test (ACT), do not correlate with measures of airway inflammation in the follow-up of asthmatic children.5,6
Invasive techniques, such as analysis of induced sputum, broncho-alveolar lavage and lung biopsies can be used to assess airway inflammation. In adults, tailoring treatment to sputum eosinophils reduces asthma exacerbations.7 In children, invasive tests are not suitable for routine use. Safety issues, technical demands and costs of sputum induction and analysis limit the use in clinical practice.
Analysis of Fraction of exhaled Nitric Oxide (FeNO) is relatively easy to perform in chil-dren. However, various other factors can influence FeNO levels, such as atopy, allergic rhinitis (AR), exercise, age, and viral respiratory tract infections.8,9 A 2012 pediatric (mean age 10-14y) meta-analysis concluded that tailoring the dose of inhaled corticosteroids (ICSs) to FeNO compared to symptoms and lung function cannot be recommended for clinical practice, as it leads to increased use of ICSs without meaningful changes in clini-cal outcomes.9
BHR to direct stimuli reflects chronic inflammation and responds slowly to anti-inflammatory treatment. In adults, tailoring treatment to direct BHR for 2 years leads to fewer exacerbations, better lung function and a greater reduction in basement membrane thickness compared to tailoring treatment to symptoms and lung function alone.10 A similar study in asthmatic children (aged 6-16y) treated with ICSs over 2 years
148 Chapter 8
showed no benefit in number of exacerbations, but a better pre-bronchodilator FEV1, in children whose treatment was tailored to direct BHR compared to symptoms alone.11 This could result from differences in the pathophysiology of asthma between adults and children.12,13 Direct BHR reflects chronic inflammation leading to functional and anatomic airway remodeling1,2, which may play a larger role in adults.
BHR to indirect stimuli is closely associated with current airway inflammation. In adults, there is a significant relationship between sputum eosinophilia and the sensitivity to indirect, but not direct, BPTs.15,16 In adolescents and adults, the percentage of sputum eosinophils correlates with the severity of EIB17 and sensitivity to mannitol.16 In children (aged 8-14y), BHR to hypertonic saline is strongly associated with the presence of mast cells in sputum.18
A response to an indirect BPT could identify patients who are likely to benefit from ICSs, as it reflects the presence of inflammatory cells that are targets for ICS treatment.19 The regular use of ICSs can attenuate airway sensitivity and reactivity to indirect stimuli.20-22 In adults, the increase in BHR to mannitol during down-titration of the dose of ICSs was predictive of an asthma exacerbation.23
Airway sensitivity and reactivity to adenosine monophosphate (AMP; an osmotic indirect BPT) correlated significantly with guideline derived asthma control in adults.24 Abolishing the response to indirect stimuli, as a marker of asthma control, may be a treatment goal.25 Tailoring treatment with ICSs to BHR to mannitol was demonstrated to improve quality of life in asthmatic adults in a primary care setting.26 In a larger study in adults with mild-to-moderate asthma, tailoring ICS treatment to BHR to mannitol for a year led to reductions in number of mild exacerbations, FeNO, eosinophilic cat-ionic protein, symptoms and rescue β2-agonist use, compared to tailoring treatment to symptoms and lung function.27
In summary, indirect BPTs are clinically relevant parameters to assess and monitor airway inflammation and the short term response to anti-inflammatory treatment in asthmatic children.
Further research is necessary to assess the complex relationship between BHR and airway inflammation. Unraveling the exact pathophysiologic mechanisms of BHR to different stimuli would lead to a better understanding of childhood asthma and pos-sible targets for therapy. Larger, randomized placebo controlled studies are necessary to evaluate how indirect BPTs can be used to monitor long-term changes in airway inflam-mation. The effect of tailoring treatment to indirect BHR should be studied for longer treatment periods and in different subgroups of patients.
Summary and General Discussion 149
8
mannITol ProvoCaTIon TEsT
In chapter 2 we studied the clinical utility of the mannitol test to identify asthmatic children with exercise induced bronchoconstriction (EIB). In this study, 33 asthmatic children, aged 9-18 years, with a history of EIB, performed both mannitol and exercise tests. Data were composed of a cross tabulation comparing the reaction on an exer-cise test to a mannitol test. Correlations between post-exercise % fall in FEV1 and RDR (response-dose ratio) and PD15 (provoking dose to cause a 15% fall in FEV1) of mannitol were calculated. Twenty-five children completed both tests. Pearson’s correlation be-tween log-transformed RDR for mannitol and post-exercise % fall in FEV1 was rp = 0.666 (P < 0.001). There was no significant relationship between the log PD15 of mannitol and post-exercise % fall in FEV1. Positive and negative predictive values of the mannitol test for EIB were respectively 69% and 92%. We concluded that a mannitol test is a suitable alternative for an exercise challenge test (ECT) to assess EIB in asthmatic children.
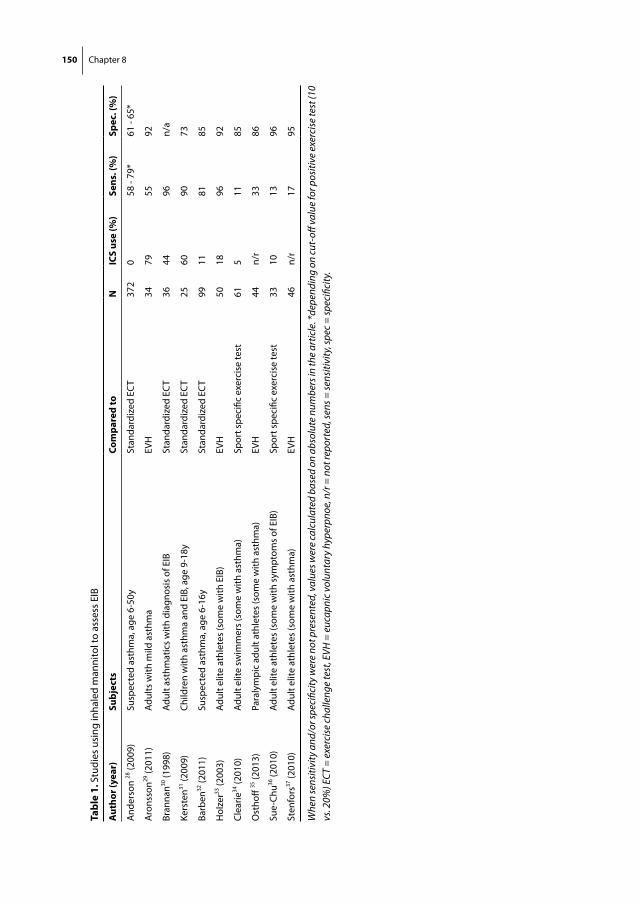
In 2011, Stickland et al. performed a systematic meta-analysis to determine the sen-sitivity and specificity of the mannitol test to diagnose EIB.38 They concluded that the sensitivity and specificity ranged from 58–96% and 65–78% respectively.38 Since then, several other studies have been performed to assess the concordance between BHR to mannitol and exercise and/or eucapnic voluntary hyperpnoea (which is considered a sensitive test for EIB, especially in athletes).39 The results of these and previous studies are summarized in Table 1.
These studies demonstrate a variable sensitivity and specificity of mannitol, depend-ing on the research population. Especially in elite athletes, sensitivity of mannitol ap-peared low.34-37 However, the pathophysiology of EIB differs between asthmatic children and adult athletes. In childhood asthma, EIB is a consequence of the inflammatory substrate present in the airway wall. In adult athletes, EIB results from repetitive thermal, osmotic and mechanical stress due to extensive training, causing injury to the airway epithelium.40,41 Only one other study was performed in asthmatic children (aged 6-16y) and found similar positive and negative predictive values of the mannitol test for EIB compared to our study. 32
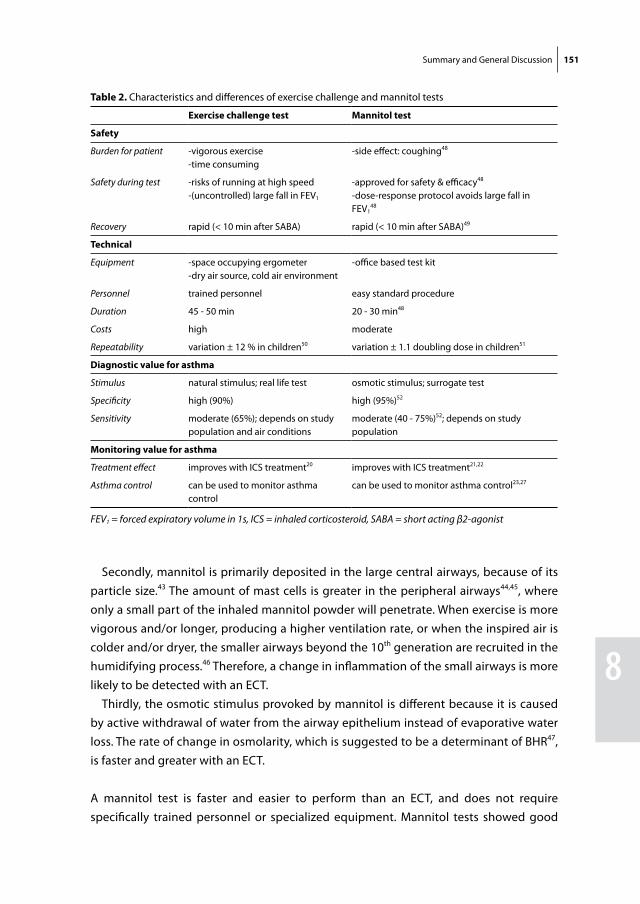
Although a mannitol test can be used as an alternative for an ECT, there are some differ-ences between the physical responses to exercise and mannitol (Table 2.)
Firstly, exercise induces a variety of other physiologic changes, such as the release of steroids and catecholamines and an increase in minute ventilation, cardiac output and oxygen uptake. Some of these mechanisms protect the airway from narrowing and compensate for the ventilation-perfusion (VA/Q) imbalance caused by bronchoconstric-tion.42 These compensatory mechanisms do not occur during a mannitol test.42
150 Chapter 8 Summary and General Discussion 151
8
Tabl
e 1.
Stu
dies
usi
ng in
hale
d m
anni
tol t
o as
sess
EIB
aut
hor (
year
)su
bjec
tsCo
mpa
red
ton
ICs
use
(%)
sens
. (%
)sp
ec. (
%)
And
erso
n 28
(200
9)Su
spec
ted
asth
ma,
age
6-5
0ySt
anda
rdiz
ed E
CT
372
058
- 79
*61
- 65
*
Aro
nsso
n29 (2
011)
Adul
ts w
ith m
ild a
sthm
aEV
H34
7955
92
Bran
nan30
(199
8)Ad
ult a
sthm
atic
s w
ith d
iagn
osis
of E
IBSt
anda
rdiz
ed E
CT
3644
96n/
a
Kers
ten31
(200
9)Ch
ildre
n w
ith a
sthm
a an
d EI
B, a
ge 9
-18y
Stan
dard
ized
EC
T25
6090
73
Barb
en32
(201
1)Su
spec
ted
asth
ma,
age
6-1
6ySt
anda
rdiz
ed E
CT
9911
8185
Hol
zer33
(200
3)Ad
ult e
lite
athl
etes
(som
e w
ith E
IB)
EVH
5018
9692
Clea
rie34
(201
0)Ad
ult e
lite
swim
mer
s (s
ome
with
ast
hma)
Spor
t spe
cific
exe
rcis
e te
st61
511
85
Ost
hoff
35 (2
013)
Para
lym
pic
adul
t ath
lete
s (s
ome
with
ast
hma)
EVH
44n/
r33
86
Sue-
Chu36
(201
0)Ad
ult e
lite
athl
etes
(som
e w
ith s
ympt
oms
of E
IB)
Spor
t spe
cific
exe
rcis
e te
st33
1013
96
Sten
fors
37 (2
010)
Adul
t elit
e at
hlet
es (s
ome
with
ast
hma)
EVH
46n/
r17
95
Whe
n se
nsiti
vity
and
/or s
peci
ficity
wer
e no
t pre
sent
ed, v
alue
s wer
e ca
lcul
ated
bas
ed o
n ab
solu
te n
umbe
rs in
the
artic
le. *
depe
ndin
g on
cut-
off v
alue
for p
ositi
ve e
xerc
ise
test
(10
vs. 2
0%) E
CT =
exe
rcis
e ch
alle
nge
test
, EVH
= e
ucap
nic
volu
ntar
y hy
perp
noe,
n/r
= n
ot re
port
ed, s
ens =
sens
itivi
ty, s
pec
= sp
ecifi
city
.
150 Chapter 8 Summary and General Discussion 151
8
Secondly, mannitol is primarily deposited in the large central airways, because of its particle size.43 The amount of mast cells is greater in the peripheral airways44,45, where only a small part of the inhaled mannitol powder will penetrate. When exercise is more vigorous and/or longer, producing a higher ventilation rate, or when the inspired air is colder and/or dryer, the smaller airways beyond the 10th generation are recruited in the humidifying process.46 Therefore, a change in inflammation of the small airways is more likely to be detected with an ECT.
Thirdly, the osmotic stimulus provoked by mannitol is different because it is caused by active withdrawal of water from the airway epithelium instead of evaporative water loss. The rate of change in osmolarity, which is suggested to be a determinant of BHR47, is faster and greater with an ECT.
A mannitol test is faster and easier to perform than an ECT, and does not require specifically trained personnel or specialized equipment. Mannitol tests showed good
Table 2. Characteristics and differences of exercise challenge and mannitol tests
Exercise challenge test mannitol test
safety
Burden for patient -vigorous exercise-time consuming
-side effect: coughing48
Safety during test -risks of running at high speed-(uncontrolled) large fall in FEV1
-approved for safety & efficacy48
-dose-response protocol avoids large fall in FEV1
48
Recovery rapid (< 10 min after SABA) rapid (< 10 min after SABA)49
Technical
Equipment -space occupying ergometer-dry air source, cold air environment
-office based test kit
Personnel trained personnel easy standard procedure
Duration 45 - 50 min 20 - 30 min48
Costs high moderate
Repeatability variation ± 12 % in children50 variation ± 1.1 doubling dose in children51
diagnostic value for asthma
Stimulus natural stimulus; real life test osmotic stimulus; surrogate test
Specificity high (90%) high (95%)52
Sensitivity moderate (65%); depends on study population and air conditions
moderate (40 - 75%)52; depends on study population
monitoring value for asthma
Treatment effect improves with ICS treatment20 improves with ICS treatment21,22
Asthma control can be used to monitor asthma control
can be used to monitor asthma control23,27
FEV1 = forced expiratory volume in 1s, ICS = inhaled corticosteroid, SABA = short acting β2-agonist
152 Chapter 8
repeatability in asthmatic children (aged 6-16y).51,53 Its safety was demonstrated in 592 asthmatic and non-asthmatic subjects, including 126 children (aged 6-18y).48 In this study, only 14/592 subjects experienced > 30% fall in FEV1
48, as the test can be stopped before major falls in FEV1 occur. The mannitol test is also feasible in younger children, aged 3-7 years.54
A limitation of the mannitol test is the occurrence of a dry cough, which almost all patients experience. This cough can interfere with the fixed time schedule. The test should be performed quickly (next dose within 60s after spirometry). Prolonging the time between the inhalation of subsequent doses of mannitol could lead to a milder os-motic stimulus and give falsely negative results. Severe coughing, leading to disruption of the test, occurs in 1.3% of tested subjects.52 Mannitol provoked coughing can occur immediately after inhalation due to the impaction of powder on the oropharynx30,53 or later due to deposition of powder in the lower respiratory tract, stimulating nerve fibers by hyperosmolarity.55,56 Mannitol induced coughing is related to the increased sensitiv-ity of the asthmatic airways, making it useful in the diagnosis of asthma.57
In summary, mannitol has a high specificity and moderate sensitivity to diagnose EIB in asthmatic children; but there are some differences in the physiological responses to exercise and mannitol. As mannitol is a practical, fast and safe test, it has the potential to become an office based test to monitor treatment alterations in asthmatic children with EIB.
Future research studying the differences in physical responses to mannitol and exercise could present new information on the pathophysiology of EIB. The effects of tailoring treatment to BHR to mannitol in children with asthma and EIB should be further explored.
β2-aGonIsTs
In chapter 3 and 4 we investigated the effect of the development of tolerance to long-acting β2-agonists (LABAs) on BHR to indirect BPTs. We analyzed clinically stable asthmatic children who were stepped down from LABA/ICS combination therapy to monotherapy with the same dose of the ICS. As regular use of β2-agonists can increase BHR to indirect stimuli, we hypothesized that this step down could do the opposite.
In chapter 3 we analyzed the effect of stepping down combination therapy to mono-therapy with an ICS on EIB in clinically stable asthmatic children with a history of mild to moderate EIB. Nineteen children, aged 8-16 years, were analyzed in this open-label pilot study. Children performed a baseline ECT after a 4 week run-in period on combination
Summary and General Discussion 153
8
therapy and 3 weeks after the medication was stepped down. Maximum % fall in FEV1 was significantly lower after 3 weeks of ICS monotherapy (P = 0.03).
Eight children had a ≥ 15% fall in FEV1 after exercise at the initial ECT. The cutoff value to diagnose EIB on an ECT is controversial. A fall of ≥ 10% is considered abnormal; a fall of ≥ 15% appears to be more diagnostic of EIB, particularly if exercise has been performed in the field. Haby et al.50 found that 1.96 SD above the mean fall in FEV1 when testing 8-11 year old healthy children in the field was 15.3%. Because the environmental cir-cumstances in which the test was performed in our study were more similar to outdoor circumstances than to laboratory settings, a cut-off value of 15% was used.
In the subgroup of patients with EIB, maximum % fall in FEV1 was significantly lower (P < 0.01) after the medication was stepped down and in 6 children it decreased to < 15%. We concluded that in clinically stable asthmatic children with mild to moderate EIB despite LABA/ICS combination therapy, the cessation of the LABA can reduce and in most cases even abolish EIB.
In chapter 4 we performed a similar study design, analyzing the effect of stepping down combination therapy to ICS monotherapy on BHR to a mannitol test. Seventeen chil-dren, aged 12-17 years, with clinically stable asthma and a history of mild to moderate EIB were analyzed in this prospective open-label study. Children performed a mannitol test after a 4 week run-in period on combination therapy and 30 ± 4 days after their medication was stepped down. The changes in mannitol PD15, RDR and recovery time following a short-acting β2-agonist (SABA) to ≥ 95% of baseline FEV1 were calculated. Mannitol PD15 and RDR did not change after stepping down. The recovery time following a SABA was significantly shorter (P = 0.01) after the cessation of the LABA. We concluded that in clinically stable asthmatic children with mild to moderate EIB despite LABA/ICS combination therapy, the cessation of the LABA does not change BHR to mannitol, but does shorten recovery time to baseline lung function following a rescue SABA.
Due to concerns about the safety of LABA use, the US Food and Drug Administration (FDA) advised that in asthmatic children on combination therapy, LABAs should be withdrawn once asthma control is achieved.59 A recent meta-analysis reviewed the effect of stepping down to ICS monotherapy compared to continuation of LABA/ICS combination therapy in asthmatic adults.60 They concluded that the LABA step-down regimen resulted in worse asthma control and quality of life.60 However, they did not assess the effect on BHR, and no pediatric studies were included.
The results from our studies are consistent with findings from studies that stepped up treatment with a LABA. Regular treatment with β2-agonists leads to downregulation and desensitization of the β2-adrenoreceptor (β2AR), resulting in a reduced protection
154 Chapter 8
against BHR61-66 and a prolonged recovery time after rescue therapy with a SABA.61,64,65 Because this process occurs faster in mast cells than smooth muscle cells, the effects of tolerance are more pronounced when measured with an indirect BPT compared to a direct BPT.67-70 As BHR to exercise decreased after the cessation of the LABA, and BHR to mannitol did not, we speculate that EIB gives a better reflection of inflammation in the peripheral airways, where more mast cells reside45 and the amount of β2ARs on smooth muscle is highest.58
Downregulation of β2ARs on the mast cell increases its susceptibility to degranulate, as was shown by increased levels of mast cell mediators following an allergen challenge in adults treated with a SABA.71 This could lead to more instable asthma and an increase in BHR.
The number of β2ARs on leukocytes in asthmatic children (aged 11-16y) has a negative correlation with BHR to exercise.72 Regular treatment of steroid-naïve asthmatic adults with a SABA increases BHR to exercise73,74 and hypertonic saline.75 This has not been studied after regular treatment with LABA monotherapy. However, in studies compar-ing a step-up to LABA/ICS combination therapy to the same dose of ICS monotherapy, asthmatic children (aged 6-18y) showed a significantly lower improvement in BHR to methacholine76 and a non-significantly lower improvement in BHR to exercise63 on LABA/ICS combination therapy. This suggests that LABAs may attenuate the beneficial effects of ICSs on BHR.
In daily life, the effect of LABA tolerance may be less apparent than in clinical trials due to poor compliance. The effects of tolerance have been shown to be reversed within three days after a LABA is discontinued.77 Therefore, patients who regularly take a ‘drug holiday’ might not experience the adverse effects of LABA tolerance.
The clinical relevance of β2AR downregulation and β2-agonist associated increased BHR to indirect stimuli is still debated. In chapter 5 we review current literature on the benefits and safety of β2-agonists in childhood asthma. We hypothesize that the combination of increased BHR and a reduced response to rescue bronchodilators could account for the association between serious asthma related adverse events and regular β2-agonist use.
Asthmatic patients with specific genotypes might be more susceptible to this. β2AR-gene polymorphisms result in changes in the amino acid sequence of the β2AR, leading to alterations of its properties, possibly representing a risk factor for adverse responses to β2-agonist therapy.
The rare Thr164Ile polymorphism results in a decreased β2AR ligand binding in vitro78 and was associated with severe exacerbations requiring hospitalizations and systemic corticosteroids in African American adults treated with a LABA.79
Summary and General Discussion 155
8
The more extensively studied Arg16Gly polymorphism, which is prevalent in 12-15%80,81 of the Caucasian population, has also been shown to interfere with treatment responses to β2-agonists. In vitro, receptors with the homozygous Arg16 genotype show enhanced susceptibility for homologous desensitization and receptor downregu-lation.82
Retrospective analyses of data from trials in adults on ICSs have demonstrated adverse effects of the Arg16 homozygous variant on BHR83 and exacerbations84 after receiving a SABA as regular therapy. In a genotype stratified prospective trial in steroid-naïve asthmatic adults the response to 16 weeks regular albuterol was compared to placebo plus ipratropium rescue treatment.85 In this study, Arg16 homozygotes did not demon-strated a deterioration of symptom control during albuterol treatment, in contrast to Gly16 homozygotes.
Studies searching for the effect of the Arg16 homozygous genotype on the response to treatment with LABAs have shown conflicting results, which appear to be dependent on the age of the study group.
In children, an increased risk for exacerbations in Arg16 homozygotes in a cohort of 1182 patients on ICSs (aged 3-22y) with daily use of salmeterol was reported.86 Another study described an increase in oral corticosteroid use and emergency department visits in the past year in 597 Arg16 homozygotes (aged 4-12y) on LABA/ICS combination therapy compared to Gly16 homozygotes.87 A prospective randomized controlled trial in asthmatic children (aged 5-18y) showed that in Arg16 homozygotes adding montelukast compared to salmeterol to inhaled fluticasone significantly improved asthma symptoms and quality of life.88 This study suggests that in children the Arg16Gly genotype could help to determine the appropriate step-up or step-down regimen.
In summary, regular treatment with β2-agonists leads to a loss of bronchoprotection and a reduced bronchodilator response to rescue SABAs. Downregulation of β2ARs on the mast cell could lead to more instable asthma, increased BHR and a higher risk of exacerbations. Therefore, if asthmatic children on LABA/ICS combination therapy experience EIB, a withdrawal of the LABA or a switch to another step 3 option should be considered. If asthmatic children with EIB need SABAs more than twice weekly, includ-ing pre-exercise use, a step-up in controller therapy should be considered.
Future trials should study the effects of different LABA treatment regimens, with con-comitant ICSs, on BHR and other outcome measures of inflammation, asthma control and quality of life. More research in children < 12 years is necessary to provide evidence based recommendations on the safety and efficacy of LABA/ICS combination therapy in general, and in different genetic subgroups.
156 Chapter 8
InTranasal CorTICosTEroIds
In chapter 6 we studied the effect of intranasal anti-inflammatory treatment on lower airway inflammation and BHR. In this study, children aged 12-17 years, with mild-to-moderate asthma, intermittent AR and ≥ 10% fall in FEV1 at a screening ECT were randomized (double-blind) to 22 ± 3 days treatment with nasal fluticasone furoate or placebo. The primary outcome was change in exercise induced fall in FEV1. Secondary outcomes were changes in scores on the asthma control questionnaire, pediatric asthma quality of life questionnaire and FeNO.
Twenty-five children completed the study. Exercise induced fall in FEV1 decreased significantly in the fluticasone furoate group compared to the placebo group (P = 0.04). Although total quality of life score did not improve after nasal fluticasone furoate treat-ment, the activity limitation domain score improved significantly within the fluticasone furoate group (P = 0.03). No significant changes were observed in FeNO and asthma control questionnaire scores. We concluded that treatment with an intranasal cortico-steroid reduces EIB in children with mild-to-moderate asthma.
Preceding studies on the effect of INCS on measures of BHR and lower airway inflam-mation have shown conflicting results.89,90 The 2010 Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines concluded there was no clear benefit from the use of INCS for asthma.91 However, since 2010 several new studies have been published and a meta-analysis of both adult and pediatric studies concluded that INCS significantly improve FEV1, symptom scores, rescue medication use and BHR to methacholine and histamine compared to placebo in steroid-naïve patients.92 There was no significant change in asthma outcomes with the addition of INCS to ICSs.92 This may reflect the fact that most patients on ICSs already have good baseline asthma control with less room for improve-ment with additional INCS. In our study, we included children with a ≥ 10% fall in FEV1 post-exercise, which is a sign of partially uncontrolled asthma. This may explain why we did demonstrate an improvement in EIB with INCS even in children on ICSs.
Although the effect of INCS on BHR to direct BPTs was statistically significant in the 2013 meta-analysis, it was only small (improvement in PC20 of 0.43 doubling doses; 95% CI 0.16 – 0.69) and not clinically relevant.92 An indirect BPT might be more suitable to measure the short-term effects of INCS on the lower airways. The effect of INCS on BHR to indirect stimuli was only studied in one other study.93 Henriksen et al. investigated the effect of intranasal budesonide on EIB in room temperature in steroid-naïve al-lergic asthmatic children (mean age 11.6y) with chronic nasal obstruction and found a non-significant trend towards a reduction in EIB after 4 weeks treatment.93 The main differences compared to our study were the inclusion criteria and the condition of the inhaled air during the ECT. We included children with intermittent symptoms of AR
Summary and General Discussion 157
8
whereas Henriksen selected children with a persistently blocked nose. Furthermore, we used cold, dry air, which amplifies EIB, and may explain the greater difference between groups in our study.
Results of our study support the existence of an important physiologic relation between upper and lower airway inflammation.
It could be argued that treatment effects result from deposition of INCS into the lungs. However, studies assessing drug delivery of intranasal sprays in adults observed no significant deposition of medication into the lower airways.94,95 An effect of INCS through systemic absorption is also unlikely, since absorption of fluticasone furoate after intranasal administration is low.96
It was suggested that post nasal drip may lead to aspiration of nasal secretions, spreading inflammatory and infectious cells and mediators to the lower airways. This concept was studied in adults by Bardin et al., who concluded that there was no seeding of the lower airways by nasal secretions.97
Improved nasal breathing may reduce chronic irritation of the lower airways as the nose warms, humidifies and filters the inspired air. In contrast, nasal blockage leads to exposure of the bronchial mucosa to cold, dry air. This has an acute effect on EIB in daily life, as it amplifies evaporative water loss from the airway surface liquid, but it has no effect on EIB in laboratory testing, as patients wear a nose clip during an ECT. Chronic exposure of the bronchial mucosa to cold, dry and unfiltered air increases the deposition of allergen to the lower airways, leading to increased lower airway inflammation and BHR.
Nasal provocation with allergen leads to increased trafficking of eosinophils and pro-genitor cells from the bone marrow to peripheral blood98,99 and thereby increases the blood levels of eosinophils and inflammatory mediators.100 These could spread to the lower airways through the systemic circulation. It has been shown in adolescents and adults that INCS can reduce the number of circulating eosinophils in peripheral blood101 and surrogate markers of inflammation, such as pulmonary FeNO.102 In our study, we found no significant reduction in FeNO after treatment with intranasal fluticasone furoate, but steroid-naïve children tended to have a greater decrease in FeNO than ICS treated children. Previously, Pedroletti et al. described unchanged levels of FeNO in asthmatic children (mean age 13y) with mild to moderate AR treated with INCS added to ICSs.103 Conversely, Sandrini et al. found a significant decrease in FeNO in steroid-naïve asthmatic adults after treatment of AR with intranasal triamcinolone.102 This may reflect a difference in the severity of allergic inflammation due to ICS use.
In summary, in children with concomitant asthma and AR, treatment of the upper air-ways with an INCS can improve EIB and asthma outcomes, especially in steroid-naïve
158 Chapter 8
children. This effect is most likely due to a combination of improved nasal breathing and a decreased number of circulating inflammatory cells and mediators.
Further research studying the cells and mediators involved in the pathophysiologic connection between the upper and lower airways could increase our understanding of both asthma and AR. Larger studies in adults and children, with different asthma severity and control status and intermittent vs. persistent AR are required to develop evidence-based integrated treatment strategies.
PharmaColoGIC PhEnoTyPInG
Asthma is a heterogeneous disease, which is also exemplified in the variability of in-dividual patients’ responses to medications. Guideline recommendations for treatment are primarily based on evidence from trials comparing mean responses between medi-cation regimens. However, there is a considerable inter-individual variability in response to medications. There is currently a lack of evidence to guide clinicians in selecting the medication most likely to achieve a favorable response in an individual patient.
In the past decade, the Childhood Asthma Research and Education (CARE) Network examined the variability in response to step 2 treatment options (i.e., initial controller therapy with an ICS or LTRA) to assess phenotypic factors indicative of a specific favor-able response.104 They found that children (aged 6-17y) who responded better to ICSs had higher baseline FeNO, blood eosinophils, serum Eosinophil Cationic Protein and IgE and lower FEV1 and methacholine PC20.105-107 A parental history of asthma and prior ICS use also predicted a favorable response to ICSs.107 Those who responded better to MLK were significantly younger and had a shorter duration of asthma and a higher urinary leukotriene E4 (uLTE4)105 and uLTE4 / FeNO ratio.108 These results suggest that an eo-sinophilic inflammatory phenotype is associated with a better ICS response, and a high CysLT inflammatory phenotype is associated with a better LTRA response.
Subsequently, differential response to step 3 treatment (i.e., step-up therapy in children uncontrolled on low dose ICSs) was analyzed by the CARE network in the Best Add-On Giving Effective Response (BADGER) study.109 By using a composite outcome measure of exacerbations, asthma control days and FEV1, 44.1% of asthmatic children (aged 6-17y) responded best to add-on LABA, 26.7% to medium dose ICS (250μg fluti-casone twice daily) and 29.2% to add-on LTRA. In a multivariate analysis with data from this study, higher uLTE4 levels were associated with a favorable response to LTRA over LABA step-up therapy and higher impulse oscillometry reactance area with a favorable response of LABA over ICS step-up therapy.110 There were no apparent baseline predic-tors of differential responses comparing ICS with LTRA step-up therapy.110

Summary and General Discussion 159
8
Phenotypic variables that predict a favorable response to treatment are dependent on the definition of response that is used, for example an improvement in lung function or asthma control, or the prevention of exacerbations.111 As a single dose of MLK and regular daily treatment with MLK both attenuate EIB, we hypothesized that we could pharmacologically phenotype children who would be protected against EIB by MLK by measuring the response to a single dose on EIB.
In chapter 7, we describe a prospective open-label study, in which 24 adolescents on low dose ICSs, aged 12-17 years, with a history of persistent asthma and ≥ 10% post-exercise fall in FEV1, were treated with MLK once daily for 30 ± 4 days. Children performed an ECT 3 times: at baseline, 20h after the first dose and 40-44h after the last dose of 4 weeks treatment. The relationship between the effect of a single MLK-dose and 4 weeks treatment on EIB was analyzed. The positive and negative predictive values of ≥ 25% reduction in area under the curve for 20 min post-exercise (AUC0-20min) after a single dose were calculated.
Twenty-one children completed the study. There was a moderate correlation between the effect of a single MLK-dose and the effect of 4 weeks treatment on AUC0-20min, r = 0.49 (P = 0.011). The AUC0-20min decreased significantly after a single MLK-dose (P = 0.001), but not after 4 weeks treatment (P = 0.080). The positive and negative predictive values of ≥ 25% reduction in AUC0-20min after a single dose were resp. 84.6% and 50.0% (P = 0.146). We concluded that the effect of a single MLK-dose on EIB only modestly predicts the effect of 4 weeks treatment on EIB in adolescent asthmatics on low dose ICSs. The single dose response to MLK was stronger than the response to 4 weeks regular treatment, implying that a high adherence is essential to profit from the full protective effect of MLK against EIB. If used on a daily base, MLK offered clinically significant protection against EIB in the large majority (80%) of children uncontrolled by low dose ICS.
Instead of phenotyping patients responsive to different treatment regimens, pharmaco-genetic studies analyze how different genotypes predict individual responses to phar-macological therapies.112 Genetic variation can influence the drug response through pharmacodynamic mechanisms (for example variation in the receptor pathway) of pharmacokinetic mechanisms. As described in a previous paragraph, polymorphisms of the β2AR can influence the response to LABA treatment. Similarly, polymorphisms of the glucocorticoid pathway and CysLT pathway can influence responses to ICSs and LTRAs.113
In summary, our results suggest that pharmacologic phenotyping of children by measuring the single dose effect on an indirect BPT is not useful for MLK. Studies that assessed phenotypic factors indicative of a favorable response to different step 2 and step 3 treatment options showed no consistent pattern of baseline predictors. Phar-
160 Chapter 8
macogenetic studies may have the potential to identify genetic polymorphisms that predict a favorable response to treatments.
In future research, larger prospective genotype-stratified studies are required to further explore the impact of genetic variations on therapeutic responses. Furthermore, additional factors influencing variability in treatment response, such as gene-gene interactions and environmental effects (such as smoking) should be identified.
TrEaTmEnT of ExErCIsE InduCEd BronChoConsTrICTIon
The presence of EIB in asthmatic children is a sign of partially uncontrolled asthma. Physical activity is the most important trigger for asthma symptoms and EIB has a great impact on a child’s quality of life. Therefore, protection against EIB should be a priority for pediatricians treating asthmatic children.
Non-pharmaceutical treatment options include warming up114, maneuvers to pre-warm and humidify the air during exercise, improving cardiovascular condition and losing weight.115 Furthermore, co-morbid conditions should be treated. For example, al-lergic asthmatic children with concomitant AR can be treated with an INCS, as described in chapter 6.
Pharmaceutical management of EIB follows guidelines of asthma management in gen-eral. However, treatment directed at the prevention of EIB may lead to other step-up or step-down decisions than treatment directed at other outcome measures.
The first step in the treatment of EIB is the prophylactic use of SABAs shortly before exercise.116 A large body of evidence supports the use of SABAs and it was calculated that post-exercise maximum fall in FEV1 was reduced with 18.99% (95% CI 16.60 – 21.38) by administration of a single dose of SABA.117 However, daily use of SABAs leads to toler-ance and an increase in EIB.73,74 If a SABA is needed more than twice a week (even if only before exercise), controller therapy is recommended.
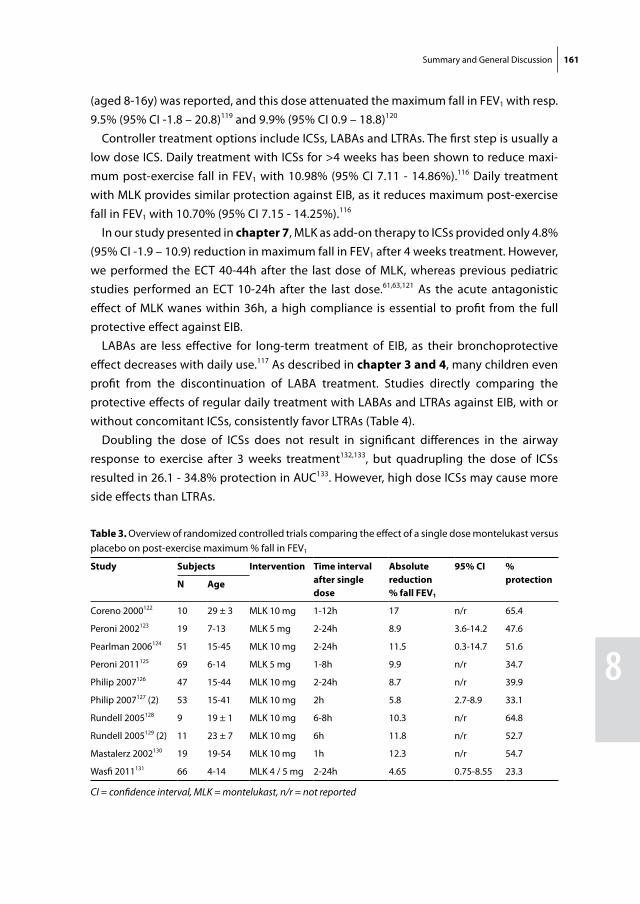
Alternative prophylactic treatment options include LABAs, LTRAs and ICSs. A single dose of a LABA reduces post-exercise maximum fall in FEV1 with 15.60% (95% CI 12.92 – 18.29).117 A single dose of MLK was reported to reduce maximum fall in FEV1 4.65 to 17.0% within hours (Table 3). In our study presented in chapter 7, MLK provided 5.8% (95% CI 2.4 – 9.2) reduction in maximum fall in FEV1 20h after a single dose.
A single dose of an ICS has also been shown to attenuate maximum post-exercise fall in FEV1.
118-120 The 2012 ATS clinical practice guideline on EIB calculated that the single dose effect of ICSs is only small (mean difference in maximum fall in FEV1 4.68%, 95% CI -7.01 – 16.37) and pre-exercise ICS use is therefore not recommended. However, in two studies the effect of a high dose of 1 mg Fluticasone Proprionate in asthmatic children
Summary and General Discussion 161
8
(aged 8-16y) was reported, and this dose attenuated the maximum fall in FEV1 with resp. 9.5% (95% CI -1.8 – 20.8)119 and 9.9% (95% CI 0.9 – 18.8)120
Controller treatment options include ICSs, LABAs and LTRAs. The first step is usually a low dose ICS. Daily treatment with ICSs for >4 weeks has been shown to reduce maxi-mum post-exercise fall in FEV1 with 10.98% (95% CI 7.11 - 14.86%).116 Daily treatment with MLK provides similar protection against EIB, as it reduces maximum post-exercise fall in FEV1 with 10.70% (95% CI 7.15 - 14.25%).116
In our study presented in chapter 7, MLK as add-on therapy to ICSs provided only 4.8% (95% CI -1.9 – 10.9) reduction in maximum fall in FEV1 after 4 weeks treatment. However, we performed the ECT 40-44h after the last dose of MLK, whereas previous pediatric studies performed an ECT 10-24h after the last dose.61,63,121 As the acute antagonistic effect of MLK wanes within 36h, a high compliance is essential to profit from the full protective effect against EIB.
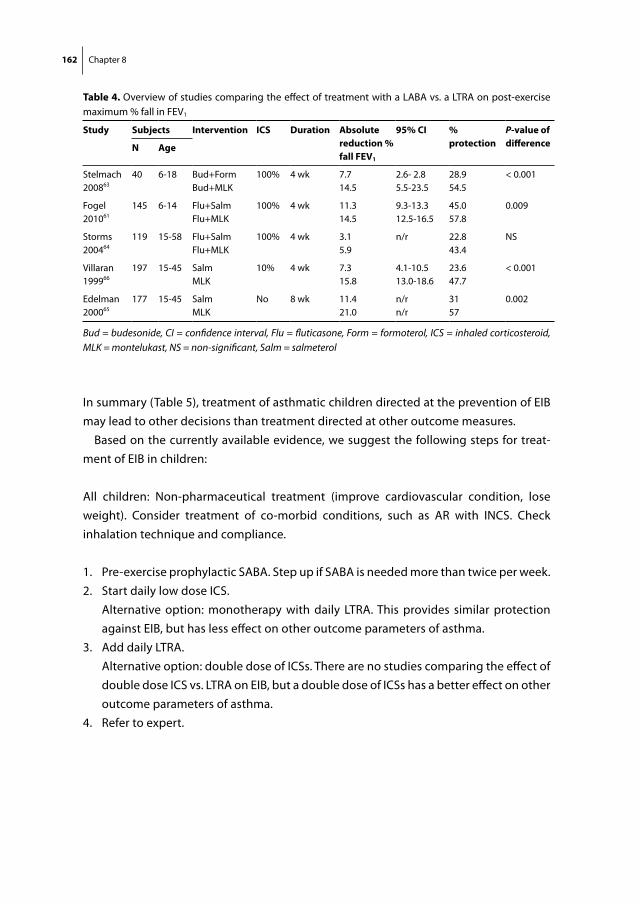
LABAs are less effective for long-term treatment of EIB, as their bronchoprotective effect decreases with daily use.117 As described in chapter 3 and 4, many children even profit from the discontinuation of LABA treatment. Studies directly comparing the protective effects of regular daily treatment with LABAs and LTRAs against EIB, with or without concomitant ICSs, consistently favor LTRAs (Table 4).
Doubling the dose of ICSs does not result in significant differences in the airway response to exercise after 3 weeks treatment132,133, but quadrupling the dose of ICSs resulted in 26.1 - 34.8% protection in AUC133. However, high dose ICSs may cause more side effects than LTRAs.
Table 3. Overview of randomized controlled trials comparing the effect of a single dose montelukast versus placebo on post-exercise maximum % fall in FEV1
study subjects Intervention Time interval after single dose
absolute reduction% fall fEv1
95% CI % protectionn age
Coreno 2000122 10 29 ± 3 MLK 10 mg 1-12h 17 n/r 65.4
Peroni 2002123 19 7-13 MLK 5 mg 2-24h 8.9 3.6-14.2 47.6
Pearlman 2006124 51 15-45 MLK 10 mg 2-24h 11.5 0.3-14.7 51.6
Peroni 2011125 69 6-14 MLK 5 mg 1-8h 9.9 n/r 34.7
Philip 2007126 47 15-44 MLK 10 mg 2-24h 8.7 n/r 39.9
Philip 2007127 (2) 53 15-41 MLK 10 mg 2h 5.8 2.7-8.9 33.1
Rundell 2005128 9 19 ± 1 MLK 10 mg 6-8h 10.3 n/r 64.8
Rundell 2005129 (2) 11 23 ± 7 MLK 10 mg 6h 11.8 n/r 52.7
Mastalerz 2002130 19 19-54 MLK 10 mg 1h 12.3 n/r 54.7
Wasfi 2011131 66 4-14 MLK 4 / 5 mg 2-24h 4.65 0.75-8.55 23.3
CI = confidence interval, MLK = montelukast, n/r = not reported
162 Chapter 8
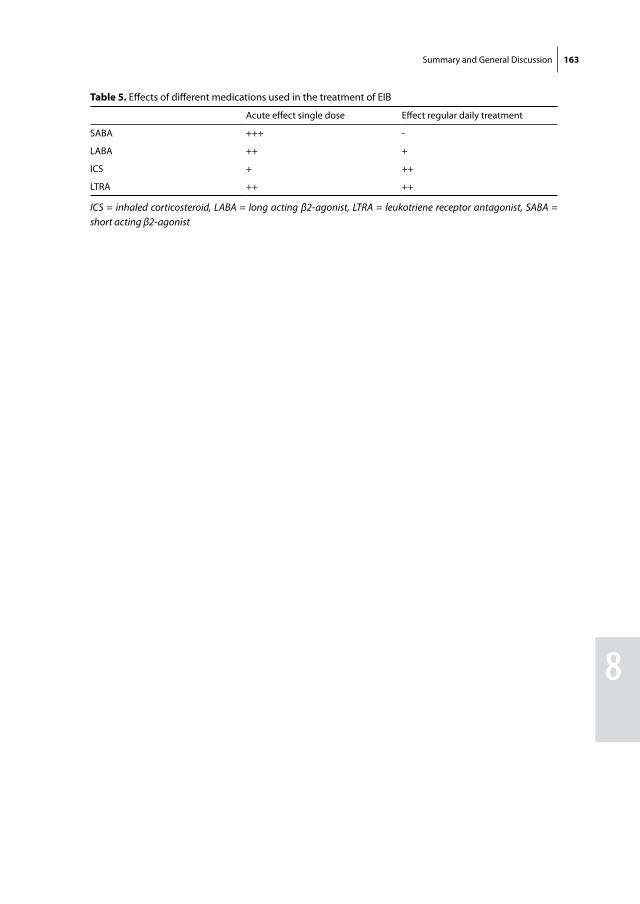
In summary (Table 5), treatment of asthmatic children directed at the prevention of EIB may lead to other decisions than treatment directed at other outcome measures.
Based on the currently available evidence, we suggest the following steps for treat-ment of EIB in children:
All children: Non-pharmaceutical treatment (improve cardiovascular condition, lose weight). Consider treatment of co-morbid conditions, such as AR with INCS. Check inhalation technique and compliance.
1. Pre-exercise prophylactic SABA. Step up if SABA is needed more than twice per week.2. Start daily low dose ICS. Alternative option: monotherapy with daily LTRA. This provides similar protection
against EIB, but has less effect on other outcome parameters of asthma.3. Add daily LTRA. Alternative option: double dose of ICSs. There are no studies comparing the effect of
double dose ICS vs. LTRA on EIB, but a double dose of ICSs has a better effect on other outcome parameters of asthma.
4. Refer to expert.
Table 4. Overview of studies comparing the effect of treatment with a LABA vs. a LTRA on post-exercise maximum % fall in FEV1
study subjects Intervention ICs duration absolute reduction % fall fEv1
95% CI % protection
P-value of differencen age
Stelmach200863
40 6-18 Bud+FormBud+MLK
100% 4 wk 7.714.5
2.6- 2.85.5-23.5
28.954.5
< 0.001
Fogel 201061
145 6-14 Flu+SalmFlu+MLK
100% 4 wk 11.314.5
9.3-13.312.5-16.5
45.057.8
0.009
Storms 200464
119 15-58 Flu+SalmFlu+MLK
100% 4 wk 3.15.9
n/r 22.843.4
NS
Villaran 199966
197 15-45 SalmMLK
10% 4 wk 7.315.8
4.1-10.513.0-18.6
23.647.7
< 0.001
Edelman 200065
177 15-45 SalmMLK
No 8 wk 11.421.0
n/rn/r
3157
0.002
Bud = budesonide, CI = confidence interval, Flu = fluticasone, Form = formoterol, ICS = inhaled corticosteroid, MLK = montelukast, NS = non-significant, Salm = salmeterol
Summary and General Discussion 163
8
Table 5. Effects of different medications used in the treatment of EIB
Acute effect single dose Effect regular daily treatment
SABA +++ -
LABA ++ +
ICS + ++
LTRA ++ ++
ICS = inhaled corticosteroid, LABA = long acting β2-agonist, LTRA = leukotriene receptor antagonist, SABA = short acting β2-agonist

164 Chapter 8
rEfErEnCEs
1. Joos GF, O’Connor B, Anderson SD, Chung F, Cockcroft DW, Dahlen B, et al. Indirect airway chal-lenges. Eur Respir J 2003; 21(6): 1050-68.
2. Cockcroft D, Davis B. Direct and indirect challenges in the clinical assessment of asthma. Ann Allergy Asthma Immunol 2009; 103(5): 363-9.
3. Bacharier LB, Strunk RC, Mauger D, White D, Lemanske RF, Jr., Sorkness CA. Classifying asthma severity in children: mismatch between symptoms, medication use, and lung function. Am J Respir Crit Care Med 2004; 170(4): 426-32.
4. Yoos HL, Kitzman H, McMullen A, Sidora-Arcoleo K, Anson E. The language of breathlessness: do families and health care providers speak the same language when describing asthma symptoms? J Pediatr Health Care 2005; 19(4): 197-205.
5. Piacentini GL, Peroni DG, Bodini A, Bonafiglia E, Rigotti E, Baraldi E, et al. Childhood Asthma Con-trol Test and airway inflammation evaluation in asthmatic children. Allergy 2009; 64(12): 1753-7.
6. Carroll W. Limitations of asthma control questionnaires in the management and follow up of childhood asthma. Paediatr Respir Rev 2013; 14(4): 229-31.
7. Petsky HL, Cates CJ, Lasserson TJ, Li AM, Turner C, Kynaston JA, et al. A systematic review and meta-analysis: tailoring asthma treatment on eosinophilic markers (exhaled nitric oxide or spu-tum eosinophils). Thorax 2012; 67(3): 199-208.
8. Taylor DR, Pijnenburg MW, Smith AD, de Jongste JC. Exhaled nitric oxide measurements: clinical application and interpretation. Thorax 2006; 61(9): 817-27.
9. Jartti T, Wendelin-Saarenhovi M, Heinonen I, Hartiala J, Vanto T. Childhood asthma management guided by repeated FeNO measurements: a meta-analysis. Paediatr Respir Rev 2012; 13(3): 178-83.
10. Sont JK, Willems LN, Bel EH, van Krieken JH, Vandenbroucke JP, Sterk PJ. Clinical control and histopathologic outcome of asthma when using airway hyperresponsiveness as an additional guide to long-term treatment. The AMPUL Study Group. Am J Respir Crit Care Med 1999; 159(4 Pt 1): 1043-51.
11. Nuijsink M, Hop WC, Sterk PJ, Duiverman EJ, de Jongste JC. Long-term asthma treatment guided by airway hyperresponsiveness in children: a randomised controlled trial. Eur Respir J 2007; 30(3): 457-66.
12. Jenkins HA, Cherniack R, Szefler SJ, Covar R, Gelfand EW, Spahn JD. A comparison of the clinical characteristics of children and adults with severe asthma. Chest 2003; 124(4): 1318-24.
13. Gelfand EW. Pediatric asthma: a different disease. Proc Am Thorac Soc 2009; 6(3): 278-82. 14. Global initiative for Asthma (GINA). From the Global Strategy for Asthma Managment and Preven-
tion. 2014. Available from: http://www.ginasthma.org/. 15. van den Berge M, Meijer RJ, Kerstjens HA, de Reus DM, Koeter GH, Kauffman HF, et al. PC(20)
adenosine 5’-monophosphate is more closely associated with airway inflammation in asthma than PC(20) methacholine. Am J Respir Crit Care Med 2001; 163(7): 1546-50.
16. Porsbjerg C, Brannan JD, Anderson SD, Backer V. Relationship between airway responsiveness to mannitol and to methacholine and markers of airway inflammation, peak flow variability and quality of life in asthma patients. Clin Exp Allergy 2008; 38(1): 43-50.
17. Duong M, Subbarao P, Adelroth E, Obminski G, Strinich T, Inman M, et al. Sputum eosinophils and the response of exercise-induced bronchoconstriction to corticosteroid in asthma. Chest 2008; 133(2): 404-11.
Summary and General Discussion 165
8
18. Gibson PG, Wlodarczyk JW, Hensley MJ, Gleeson M, Henry RL, Cripps AW, et al. Epidemiological association of airway inflammation with asthma symptoms and airway hyperresponsiveness in childhood. Am J Respir Crit Care Med 1998; 158(1): 36-41.
19. Chauhan BF, Ducharme FM. Anti-leukotriene agents compared to inhaled corticosteroids in the management of recurrent and/or chronic asthma in adults and children. Cochrane Database Syst Rev 2012; 5: CD002314.
20. Koh MS, Tee A, Lasserson TJ, Irving LB. Inhaled corticosteroids compared to placebo for preven-tion of exercise induced bronchoconstriction. Cochrane Database Syst Rev 2007; (3): CD002739.
21. Brannan JD, Koskela H, Anderson SD, Chan HK. Budesonide reduces sensitivity and reactivity to inhaled mannitol in asthmatic subjects. Respirology 2002; 7(1): 37-44.
22. Koskela HO, Hyvarinen L, Brannan JD, Chan HK, Anderson SD. Sensitivity and validity of three bronchial provocation tests to demonstrate the effect of inhaled corticosteroids in asthma. Chest 2003; 124(4): 1341-9.
23. Leuppi JD, Salome CM, Jenkins CR, Anderson SD, Xuan W, Marks GB, et al. Predictive markers of asthma exacerbation during stepwise dose reduction of inhaled corticosteroids. Am J Respir Crit Care Med 2001; 163(2): 406-12.
24. Volbeda F, Broekema M, Lodewijk ME, Hylkema MN, Reddel HK, Timens W, et al. Clinical control of asthma associates with measures of airway inflammation. Thorax 2013; 68(1): 19-24.
25. Brannan JD. Bronchial hyperresponsiveness in the assessment of asthma control: Airway hyper-responsiveness in asthma: its measurement and clinical significance. Chest 2010; 138(2 Suppl): 11S-7S.
26. Turton JA, Glasgow NJ, Brannan JD. Feasibility and acceptability of using bronchial hyperrespon-siveness to manage asthma in primary care: a pilot study. Prim Care Respir J 2012; 21(1): 28-34.
27. Lipworth BJ, Short PM, Williamson PA, Clearie KL, Fardon TC, Jackson CM. A randomized primary care trial of steroid titration against mannitol in persistent asthma: STAMINA trial. Chest 2012; 141(3): 607-15.
28. Anderson SD, Charlton B, Weiler JM, Nichols S, Spector SL, Pearlman DS. Comparison of mannitol and methacholine to predict exercise-induced bronchoconstriction and a clinical diagnosis of asthma. Respir Res 2009; 10: 4.
29. Aronsson D, Tufvesson E, Bjermer L. Comparison of central and peripheral airway involvement before and during methacholine, mannitol and eucapnic hyperventilation challenges in mild asthmatics. Clin Respir J 2011; 5(1): 10-8.
30. Brannan JD, Koskela H, Anderson SD, Chew N. Responsiveness to mannitol in asthmatic subjects with exercise- and hyperventilation-induced asthma. Am J Respir Crit Care Med 1998; 158(4): 1120-6.
31. Kersten ET, Driessen JM, van der Berg JD, Thio BJ. Mannitol and exercise challenge tests in asth-matic children. Pediatr Pulmonol 2009; 44(7): 655-61.
32. Barben J, Kuehni CE, Strippoli MP, Schiller B, Hammer J, Trachsel D. Mannitol dry powder chal-lenge in comparison with exercise testing in children. Pediatr Pulmonol 2011; 46(9): 842-8.
33. Holzer K, Anderson SD, Chan HK, Douglass J. Mannitol as a challenge test to identify exercise-induced bronchoconstriction in elite athletes. Am J Respir Crit Care Med 2003; 167(4): 534-7.
34. Clearie KL, Williamson PA, Vaidyanathan S, Short P, Goudie A, Burns P, et al. Disconnect between standardized field-based testing and mannitol challenge in Scottish elite swimmers. Clin Exp Allergy 2010; 40(5): 731-7.
166 Chapter 8
35. Osthoff M, Michel F, Strupler M, Miedinger D, Taegtmeyer AB, Leuppi JD, et al. Bronchial hyper-responsiveness testing in athletes of the Swiss Paralympic team. BMC Sports Sci Med Rehabil 2013; 5(1): 7.
36. Sue-Chu M, Brannan JD, Anderson SD, Chew N, Bjermer L. Airway hyperresponsiveness to methacholine, adenosine 5-monophosphate, mannitol, eucapnic voluntary hyperpnoea and field exercise challenge in elite cross-country skiers. Br J Sports Med 2010; 44(11): 827-32.
37. Stenfors N. Self-reported symptoms and bronchial hyperresponsiveness in elite cross-country skiers. Respir Med 2010; 104(11): 1760-3.
38. Stickland MK, Rowe BH, Spooner CH, Vandermeer B, Dryden DM. Accuracy of eucapnic hyperpnea or mannitol to diagnose exercise-induced bronchoconstriction: a systematic review. Ann Allergy Asthma Immunol 2011; 107(3): 229-34.
39. Fitch KD, Sue-Chu M, Anderson SD, Boulet LP, Hancox RJ, McKenzie DC, et al. Asthma and the elite athlete: summary of the International Olympic Committee’s consensus conference, Lausanne, Switzerland, January 22-24, 2008. J Allergy Clin Immunol 2008; 122(2): 254-60.
40. Kippelen P, Anderson SD. Pathogenesis of exercise-induced bronchoconstriction. Immunol Al-lergy Clin North Am 2013; 33(3): 299-312, vii.
41. Anderson SD, Kippelen P. Airway injury as a mechanism for exercise-induced bronchoconstriction in elite athletes. J Allergy Clin Immunol 2008; 122(2): 225-35.
42. Munoz PA, Gomez FP, Manrique HA, Roca J, Barbera JA, Young IH, et al. Pulmonary gas exchange response to exercise- and mannitol-induced bronchoconstriction in mild asthma. J Appl Physiol 2008; 105(5): 1477-85.
43. Glover W, Chan HK, Eberl S, Daviskas E, Verschuer J. Effect of particle size of dry powder mannitol on the lung deposition in healthy volunteers. Int J Pharm 2008; 349(1-2): 314-22.
44. Hamid Q, Song Y, Kotsimbos TC, Minshall E, Bai TR, Hegele RG, et al. Inflammation of small airways in asthma. J Allergy Clin Immunol 1997; 100(1): 44-51.
45. Carroll NG, Mutavdzic S, James AL. Distribution and degranulation of airway mast cells in normal and asthmatic subjects. Eur Respir J 2002; 19(5): 879-85.
46. Anderson SD. How does exercise cause asthma attacks? Curr Opin Allergy Clin Immunol 2006; 6(1): 37-42.
47. Eggleston PA, Kagey-Sobotka A, Lichtenstein LM. A comparison of the osmotic activation of basophils and human lung mast cells. Am Rev Respir Dis 1987; 135(5): 1043-8.
48. Brannan JD, Anderson SD, Perry CP, Freed-Martens R, Lassig AR, Charlton B. The safety and efficacy of inhaled dry powder mannitol as a bronchial provocation test for airway hyperresponsiveness: a phase 3 comparison study with hypertonic (4.5%) saline. Respir Res 2005; 6: 144.
49. Anderson SD, Brannan J, Spring J, Spalding N, Rodwell LT, Chan K, et al. A new method for bronchial-provocation testing in asthmatic subjects using a dry powder of mannitol. Am J Respir Crit Care Med 1997; 156: 758-65.
50. Haby MM, Peat JK, Mellis CM, Anderson SD, Woolcock AJ. An exercise challenge for epidemiologi-cal studies of childhood asthma: validity and repeatability. Eur Respir J 1995; 8(5): 729-36.
51. Barben J, Roberts M, Chew N, Carlin JB, Robertson CF. Repeatability of bronchial responsiveness to mannitol dry powder in children with asthma. Pediatr Pulmonol 2003; 36(6): 490-4.
52. Sverrild A, Porsbjerg C, Backer V. The use of inhaled mannitol in the diagnosis and management of asthma. Expert Opin Pharmacother 2012; 13(1): 115-23.
53. Subbarao P, Brannan JD, Ho B, Anderson SD, Chan HK, Coates AL. Inhaled mannitol identifies methacholine-responsive children with active asthma. Pediatr Pulmonol 2000; 29(4): 291-8.
Summary and General Discussion 167
8
54. Alblooshi AS, Simpson SJ, Stick SM, Hall GL. The safety and feasibility of the inhaled mannitol challenge test in young children. Eur Respir J 2013; 42(5): 1420-3.
55. Pisarri TE, Jonzon A, Coleridge HM, Coleridge JC. Vagal afferent and reflex responses to changes in surface osmolarity in lower airways of dogs. J Appl Physiol 1992; 73(6): 2305-13.
56. Fox AJ, Barnes PJ, Dray A. Stimulation of guinea-pig tracheal afferent fibres by non-isosmotic and low-chloride stimuli and the effect of frusemide. J Physiol 1995; 482: 179-87.
57. Koskela HO, Hyvarinen L, Brannan JD, Chan HK, Anderson SD. Coughing during mannitol chal-lenge is associated with asthma. Chest 2004; 125(6): 1985-92.
58. Johnson M. Molecular mechanisms of beta(2)-adrenergic receptor function, response, and regu-lation. J Allergy Clin Immunol 2006; 117(1): 18-24.
59. Chowdhury BA, Dal PG. The FDA and Safe Use of Long-Acting Beta-Agonists in the Treatment of Asthma. N Engl J Med 2010; 362(13): 1169-71.
60. Brozek JL, Kraft M, Krishnan JA, Cloutier MM, Lazarus SC, Li JT, et al. Long-acting beta2-agonist step-off in patients with controlled asthma. Arch Intern Med 2012; 172(18): 1365-75.
61. Fogel RB, Rosario N, Aristizabal G, Loeys T, Noonan G, Gaile S, et al. Effect of montelukast or sal-meterol added to inhaled fluticasone on exercise-induced bronchoconstriction in children. Ann Allergy Asthma Immunol 2010; 104(6): 511-7.
62. Simons FE, Gerstner TV, Cheang MS. Tolerance to the bronchoprotective effect of salmeterol in adolescents with exercise-induced asthma using concurrent inhaled glucocorticoid treatment. Pediatrics 1997; 99(5): 655-9.
63. Stelmach I, Grzelewski T, Majak P, Jerzynska J, Stelmach W, Kuna P. Effect of different antiasthmatic treatments on exercise-induced bronchoconstriction in children with asthma. J Allergy Clin Im-munol 2008; 121(2): 383-9.
64. Storms W, Chervinsky P, Ghannam AF, Bird S, Hustad CM, Edelman JM. A comparison of the effects of oral montelukast and inhaled salmeterol on response to rescue bronchodilation after chal-lenge. Respir Med 2004; 98(11): 1051-62.
65. Edelman JM, Turpin JA, Bronsky EA, Grossman J, Kemp JP, Ghannam AF, et al. Oral montelukast compared with inhaled salmeterol to prevent exercise-induced bronchoconstriction. A random-ized, double-blind trial. Exercise Study Group. Ann Intern Med 2000; 132(2): 97-104.
66. Villaran C, O’Neill SJ, Helbling A, van Noord JA, Lee TH, Chuchalin AG, et al. Montelukast versus salmeterol in patients with asthma and exercise-induced bronchoconstriction. Montelukast/Salmeterol Exercise Study Group. J Allergy Clin Immunol 1999; 104: 547-53.
67. O’Connor BJ, Aikman SL, Barnes PJ. Tolerance to the nonbronchodilator effects of inhaled beta 2-agonists in asthma. N Engl J Med 1992; 327(17): 1204-8.
68. Jokic R, Swystun VA, Davis BE, Cockcroft DW. Regular inhaled salbutamol: effect on airway respon-siveness to methacholine and adenosine 5’-monophosphate and tolerance to bronchoprotec-tion. Chest 2001; 119(2): 370-5.
69. Yates DH, Worsdell M, Barnes PJ. Effect of an inhaled glucocorticosteroid on mast cell and smooth muscle beta 2 adrenergic tolerance in mild asthma. Thorax 1998; 53(2): 110-3.
70. Cockcroft DW, McParland CP, Britto SA, Swystun VA, Rutherford BC. Regular inhaled salbutamol and airway responsiveness to allergen. Lancet 1993; 342(8875): 833-7.
71. Swystun VA, Gordon JR, Davis EB, Zhang X, Cockcroft DW. Mast cell tryptase release and asthmatic responses to allergen increase with regular use of salbutamol. J Allergy Clin Immunol 2000; 106: 57-64.
168 Chapter 8
72. Kubota T, Koga K, Araki H, Odajima H, Nishima S, Miyamoto H, et al. The relationships of mono-nuclear leukocyte beta-adrenergic receptors to aerobic capacity and exercise-induced asthma in asthmatic children. Arerugi 2000; 49(1): 40-51.
73. Hancox RJ, Subbarao P, Kamada D, Watson RM, Hargreave FE, Inman MD. Beta2-agonist tolerance and exercise-induced bronchospasm. Am J Respir Crit Care Med 2002; 165(8): 1068-70.
74. Inman MD, O’Byrne PM. The effect of regular inhaled albuterol on exercise-induced bronchocon-striction. Am J Respir Crit Care Med 1996; 153(1): 65-9.
75. Aldridge RE, Hancox RJ, Taylor RD, Cowan JO, Winn MC, Frampton CM, et aI. Effects of terbutaline and budesonide on sputum cells and bronchial hyperresponsiveness in asthma. Am J Respir Crit Care Med 2000; 161(5): 1459-64.
76. Sorkness CA, Lemanske RF, Jr., Mauger DT, Boehmer SJ, Chinchilli VM, Martinez FD, et al. Long-term comparison of 3 controller regimens for mild-moderate persistent childhood asthma: the Pediatric Asthma Controller Trial. J Allergy Clin Immunol 2007; 119(1): 64-72.
77. Haney S, Hancox RJ. Rapid onset of tolerance to beta-agonist bronchodilation. Respir Med 2005; 99(5): 566-71.
78. Green SA, Rathz DA, Schuster AJ, Liggett SB. The Ile164 beta(2)-adrenoceptor polymorphism alters salmeterol exosite binding and conventional agonist coupling to G(s). Eur J Pharmacol 2001; 421(3): 141-7.
79. Ortega VE, Hawkins GA, Moore WC, Hastie AT, Ampleford EJ, Busse WW, et al. Effect of rare variants in ADRB2 on risk of severe exacerbations and symptom control during longacting beta agonist treatment in a multiethnic asthma population: a genetic study. Lancet Respir Med 2014; 2(3): 204-13.
80. Chung LP, Waterer G, Thompson PJ. Pharmacogenetics of beta2 adrenergic receptor gene poly-morphisms, long-acting beta-agonists and asthma. Clin Exp Allergy 2011; 41(3): 312-26.
81. Ortega VE, Meyers DA. Pharmacogenetics: implications of race and ethnicity on defining genetic profiles for personalized medicine. J Allergy Clin Immunol 2014; 133(1): 16-26.
82. Green SA, Turki J, Bejarano P, Hall IP, Liggett SB. Influence of beta 2-adrenergic receptor genotypes on signal transduction in human airway smooth muscle cells. Am J Respir Cell Mol Biol 1995 Jul; 13(1): 25-33.
83. Hancox RJ, Sears MR, Taylor DR. Polymorphism of the beta2-adrenoceptor and the response to long-term beta2-agonist therapy in asthma. Eur Respir J 1998; 11(3): 589-93.
84. Taylor DR, Drazen JM, Herbison GP, Yandava CN, Hancox RJ, Town GI. Asthma exacerbations dur-ing long term beta agonist use: influence of beta(2) adrenoceptor polymorphism. Thorax 2000; 55(9): 762-7.
85. Israel E, Chinchilli VM, Ford JG, Boushey HA, Cherniack R, Craig TJ, et al. Use of regularly scheduled albuterol treatment in asthma: genotype-stratified, randomised, placebo-controlled cross-over trial. Lancet 2004; 364(9444): 1505-12.
86. Basu K, Palmer CN, Tavendale R, Lipworth BJ, Mukhopadhyay S. Adrenergic beta(2)-receptor genotype predisposes to exacerbations in steroid-treated asthmatic patients taking frequent albuterol or salmeterol. J Allergy Clin Immunol 2009; 124(6): 1188-94.
87. Zuurhout MJ, Vijverberg SJ, Raaijmakers JA, Koenderman L, Postma DS, Koppelman GH, et al. Arg16 ADRB2 genotype increases the risk of asthma exacerbation in children with a reported use of long-acting beta2-agonists: results of the pacman cohort. Pharmacogenomics 2013; 14(16): 1965-71.
88. Lipworth BJ, Basu K, Donald HP, Tavendale R, Macgregor DF, Ogston SA, et al. Tailored second-line therapy in asthmatic children with the Arg(16) genotype. Clin Sci (Lond) 2013; 124(8): 521-8.
Summary and General Discussion 169
8
89. Taramarcaz P, Gibson PG. Intranasal corticosteroids for asthma control in people with coexisting asthma and rhinitis. Cochrane Database Syst Rev 2003; (4): CD003570.
90. Taramarcaz P, Gibson PG. The effectiveness of intranasal corticosteroids in combined allergic rhinitis and asthma syndrome. Clin Exp Allergy 2004; 34(12): 1883-9.
91. Brozek JL, Bousquet J, Baena-Cagnani CE, Bonini S, Canonica GW, Casale TB, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines: 2010 revision. J Allergy Clin Immunol 2010; 126(3): 466-76.
92. Lohia S, Schlosser RJ, Soler ZM. Impact of intranasal corticosteroids on asthma outcomes in al-lergic rhinitis: a meta-analysis. Allergy 2013; 68(5): 569-79.
93. Henriksen JM, Wenzel A. Effect of an intranasally administered corticosteroid (budesonide) on nasal obstruction, mouth breathing, and asthma. Am Rev Respir Dis 1984; 130(6): 1014-8.
94. Djupesland PG, Skretting A. Nasal deposition and clearance in man: comparison of a bidirectional powder device and a traditional liquid spray pump. J Aerosol Med Pulm Drug Deliv 2012; 25(5): 280-9.
95. Moller W, Saba GK, Haussinger K, Becker S, Keller M, Schuschnig U. Nasally inhaled pulsating aerosols: lung, sinus and nose deposition. Rhinology 2011; 49(3): 286-91.
96. McCormack PL, Scott LJ. Fluticasone furoate: intranasal use in allergic rhinitis. Drugs 2007; 67(13): 1905-15.
97. Bardin PG, Van Heerden BB, Joubert JR. Absence of pulmonary aspiration of sinus contents in patients with asthma and sinusitis. J Allergy Clin Immunol 1990; 86(1): 82-8.
98. Wood LJ, Inman MD, Watson RM, Foley R, Denburg JA, O’Byrne PM. Changes in bone marrow inflammatory cell progenitors after inhaled allergen in asthmatic subjects. Am J Respir Crit Care Med 1998; 157(1): 99-105.
99. Togias AG. Systemic immunologic and inflammatory aspects of allergic rhinitis. J Allergy Clin Immunol 2000; 106(5 Suppl): S247-S250.
100. Beeh KM, Beier J, Kornmann O, Meier C, Taeumer T, Buhl R. A single nasal allergen challenge in-creases induced sputum inflammatory markers in non-asthmatic subjects with seasonal allergic rhinitis: correlation with plasma interleukin-5. Clin Exp Allergy 2003; 33(4): 475-82.
101. Foresi A, Pelucchi A, Gherson G, Mastropasqua B, Chiapparino A, Testi R. Once daily intranasal fluticasone propionate (200 micrograms) reduces nasal symptoms and inflammation but also attenuates the increase in bronchial responsiveness during the pollen season in allergic rhinitis. J Allergy Clin Immunol 1996; 98(2): 274-82.
102. Sandrini A, Ferreira IM, Jardim JR, Zamel N, Chapman KR. Effect of nasal triamcinolone acetonide on lower airway inflammatory markers in patients with allergic rhinitis. J Allergy Clin Immunol 2003; 111(2): 313-20.
103. Pedroletti C, Lundahl J, Alving K, Hedlin G. Effect of nasal steroid treatment on airway inflam-mation determined by exhaled nitric oxide in allergic schoolchildren with perennial rhinitis and asthma. Pediatr Allergy Immunol 2008; 19(3): 219-26.
104. Szefler SJ, Martin RJ. Lessons learned from variation in response to therapy in clinical trials. J Allergy Clin Immunol 2010; 125(2): 285-92.
105. Szefler SJ, Phillips BR, Martinez FD, Chinchilli VM, Lemanske RF, Strunk RC, et al. Characterization of within-subject responses to fluticasone and montelukast in childhood asthma. J Allergy Clin Immunol 2005; 115(2): 233-42.
106. Zeiger RS, Szefler SJ, Phillips BR, Schatz M, Martinez FD, Chinchilli VM, et al. Response profiles to fluticasone and montelukast in mild-to-moderate persistent childhood asthma. J Allergy Clin Immunol 2006; 117(1): 45-52.
170 Chapter 8
107. Knuffman JE, Sorkness CA, Lemanske RF, Jr., Mauger DT, Boehmer SJ, Martinez FD, et al. Phenotypic predictors of long-term response to inhaled corticosteroid and leukotriene modifier therapies in pediatric asthma. J Allergy Clin Immunol 2009; 123(2): 411-6.
108. Rabinovitch N, Graber NJ, Chinchilli VM, Sorkness CA, Zeiger RS, Strunk RC, et al. Urinary leukot-riene E4/exhaled nitric oxide ratio and montelukast response in childhood asthma. J Allergy Clin Immunol 2010; 126(3): 545-51.
109. Lemanske RF, Jr., Mauger DT, Sorkness CA, Jackson DJ, Boehmer SJ, Martinez FD, et al. Step-up therapy for children with uncontrolled asthma receiving inhaled corticosteroids. N Engl J Med 2010; 362(11): 975-85.
110. Rabinovitch N, Mauger DT, Reisdorph N, Covar R, Malka J, Lemanske RF, Jr. Predictors of asthma control and lung function responsiveness to step 3 therapy in children with uncontrolled asthma. J Allergy Clin Immunol 2014; 133(2): 350-6.
111. Rogers AJ, Tantisira KG, Fuhlbrigge AL, Litonjua AA, Lasky-Su JA, Szefler SJ, et al. Predictors of poor response during asthma therapy differ with definition of outcome. Pharmacogenomics 2009; 10(8): 1231-42.
112. Miller SM, Ortega VE. Pharmacogenetics and the development of personalized approaches for combination therapy in asthma. Curr Allergy Asthma Rep 2013; 13(5): 443-52.
113. Ortega VE, Wechsler ME. Asthma pharmacogenetics: responding to the call for a personalized approach. Curr Opin Allergy Clin Immunol 2013; 13(4): 399-409.
114. Elkins MR, Brannan JD. Warm-up exercise can reduce exercise-induced bronchoconstriction. Br J Sports Med 2013; 47(10): 657-8.
115. van Leeuwen JC, Hoogstrate M, Duiverman EJ, Thio BJ. Effects of dietary induced weight loss on exercise-induced bronchoconstriction in overweight and obese children. Pediatr Pulmonol 2014; 49(12): 1155-61.
116. Parsons JP, Hallstrand TS, Mastronarde JG, Kaminsky DA, Rundell KW, Hull JH, et al. An official American Thoracic Society clinical practice guideline: exercise-induced bronchoconstriction. Am J Respir Crit Care Med 2013; 187(9): 1016-27.
117. Bonini M, di Mambro C., Calderon MA, Compalati E, Schunemann H, Durham S, et al. Beta-agonists for exercise-induced asthma. Cochrane Database Syst Rev 2013; 10: CD003564.
118. Yazigi R, Sly RM, Frazer M. Effect of triamcinolone acetonide aerosol upon exercise-induced asthma. Ann Allergy 1978; 40(5): 322-5.
119. Thio BJ, Slingerland GL, Nagelkerke AF, Roord JJ, Mulder PG, Dankert-Roelse JE. Effects of single-dose fluticasone on exercise-induced asthma in asthmatic children: a pilot study. Pediatr Pulmonol 2001; 32(2): 115-21.
120. Driessen JM, Nieland H, van der Palen JA, van Aalderen WM, Thio BJ, de Jongh FH. Effects of a single dose inhaled corticosteroid on the dynamics of airway obstruction after exercise. Pediatr Pulmonol 2011; 46(9): 849-56.
121. de Benedictis FM, del Giudice MM, Forenza N, Decimo F, de Benedictis D, Capristo A. Lack of toler-ance to the protective effect of montelukast in exercise-induced bronchoconstriction in children. Eur Respir J 2006; 28(2): 291-5.
122. Coreno A, Skowronski M, Kotaru C, McFadden ER, Jr. Comparative effects of long-acting beta2-agonists, leukotriene receptor antagonists, and a 5-lipoxygenase inhibitor on exercise-induced asthma. J Allergy Clin Immunol 2000; 106(3): 500-6.
123. Peroni DG, Piacentini GL, Ress M, Bodini A, Loiacono A, Aralla R, et al. Time efficacy of a single dose of montelukast on exercise-induced asthma in children. Pediatr Allergy Immunol 2002; 13(6): 434-7.
124. Pearlman DS, van Adelsberg J, Philip G, Tilles SA, Busse W, Hendeles L, et al. Onset and duration of protection against exercise-induced bronchoconstriction by a single oral dose of montelukast. Ann Allergy Asthma Immunol 2006; 97(1): 98-104.
125. Peroni DG, Pescollderungg L, Sandri M, Chinellato I, Boner AL, Piacentini GL. Time-effect of mon-telukast on protection against exercise-induced bronchoconstriction. Respir Med 2011; 105(12): 1790-7.
126. Philip G, Pearlman DS, Villaran C, Legrand C, Loeys T, Langdon RB, et al. Single-dose montelukast or salmeterol as protection against exercise-induced bronchoconstriction. Chest 2007; 132(3): 875-83.
127. Philip G, Villaran C, Pearlman DS, Loeys T, Dass SB, Reiss TF. Protection against exercise-induced bronchoconstriction two hours after a single oral dose of montelukast. J Asthma 2007; 44(3): 213-7.
128. Rundell KW, Spiering BA, Baumann JM, Evans TM. Bronchoconstriction provoked by exercise in a high-particulate-matter environment is attenuated by montelukast. Inhal Toxicol 2005; 17(2): 99-105.
129. Rundell KW, Spiering BA, Baumann JM, Evans TM. Effects of montelukast on airway narrowing from eucapnic voluntary hyperventilation and cold air exercise. Br J Sports Med 2005; 39(4): 232-6.
130. Mastalerz L, Gawlewicz-Mroczka A, Nizankowska E, Cmiel A, Szczeklik A. Protection against exercise-induced bronchoconstriction by montelukast in aspirin-sensitive and aspirin-tolerant patients with asthma. Clin Exp Allergy 2002; 32(9): 1360-5.
131. Wasfi YS, Kemp JP, Villaran C, Massaad R, Xin W, Smugar SS, et al. Onset and duration of attenua-tion of exercise-induced bronchoconstriction in children by single-dose of montelukast. Allergy Asthma Proc 2011; 32(6): 453-9.
132. Hofstra WB, Neijens HJ, Duiverman EJ, Kouwenberg JM, Mulder PG, Kuethe MC, et al. Dose-responses over time to inhaled fluticasone propionate treatment of exercise- and methacholine-induced bronchoconstriction in children with asthma. Pediatr Pulmonol 2000; 29(6): 415-23.
133. Subbarao P, Duong M, Adelroth E, Otis J, Obminski G, Inman M, et al. Effect of ciclesonide dose and duration of therapy on exercise-induced bronchoconstriction in patients with asthma. J Al-lergy Clin Immunol 2006; 117(5): 1008-13.