L2 bronchial asthma
37
Bronchial ASTHMA DR.Bilal Natiq Nuaman,MD CABM,FIBMS,DIM 2016-2017 1
-
Upload
bilal-natiq -
Category
Health & Medicine
-
view
214 -
download
0
Transcript of L2 bronchial asthma

Bronchial ASTHMA
DR.Bilal Natiq Nuaman,MD CABM,FIBMS,DIM 2016-2017 1

Global Initiative for Asthma (GINA) gives the following definition:
’Asthma is a chronic inflammatory disorder of the airways in which many cells and cellular elements play a role. The chronic inflammation is associated with airway hyperresponsiveness that leads to recurrent episodes of wheezing, breathlessness , chest tightness, and coughing, particularly at night or in the early morning. These episodes are usually associated with
widespread, but variable, airflow obstruction within the lung that is often reversible either spontaneously or with treatment’.
2

Asthma is a common condition that has increased in prevalence over the last 20 years with estimated global prevalence of 7 %.
• Asthma may be clinically defined as a syndrome of variable airway obstruction and bronchial hyperresponsiveness.
• Asthma is not a single disease entity with a unique pathogenesis, but rather recognized to be a clinical syndrome and heterogeneous disorder; that is, asthma comprises multiple endotypes that manifest common symptoms, but have distinct and probably different etiologic and pathophysiologic mechanisms with an interplay between genetic and environmental factors.
3

Many inflammatory cells play roles in the pathogenesis of asthma: eosinophils, mast cells, macrophages, and lymphocytes. Among these lymphocytes, the CD4 (helper) T-cells include TH1 and predominantelyTH2 phenotypes.
A variety of inflammatory mediators are released, including histamine, leukotrienes, and, bradykinin
4

Causes

6
AIR-SMOG: A MNEMONIC OF CONTRIBUTORS TO ASTHMA A—allergy(pets, dust mites) I—infection(viruses and Mycoplasma pneumonia), irritants (dyes, latex) R—rhinosinusitis S—smoking M—medications beta-blockers , NSAIDS 10%. O—occupational exposures (wood, flour ) G—gastroesophageal reflux disease
Predisposing factors

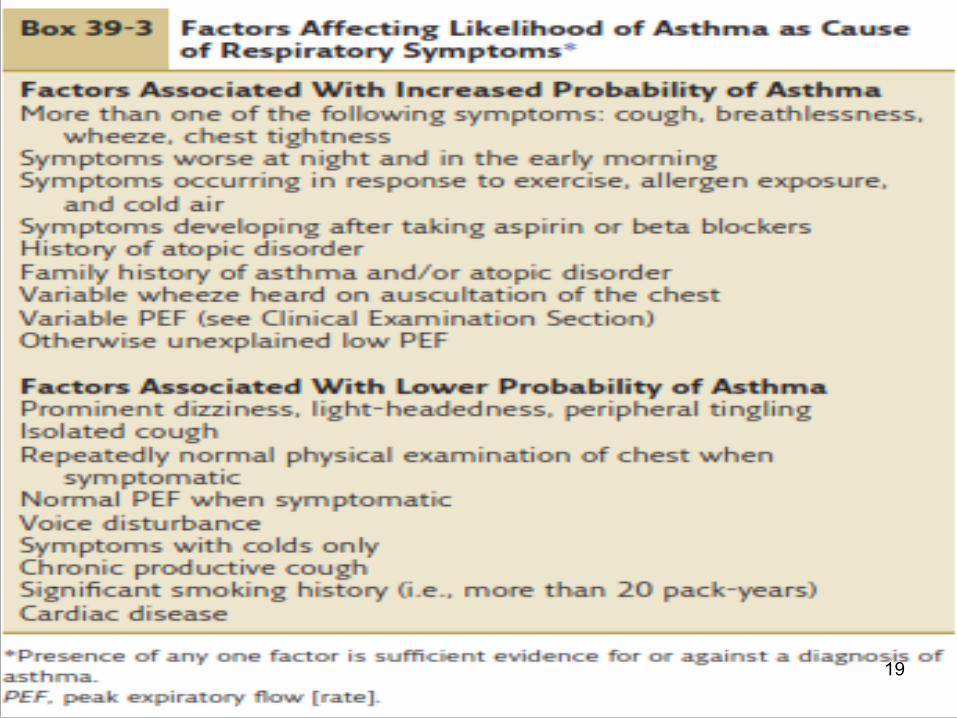
DIAGNOSIS OF ASTHMA
• History
• Physical examination
• Pulmonary function test
7

PATIENT HISTORY• Has the patient had an attack or
recurrent episodes of wheezing? • Does the patient have a troublesome
cough, worse particularly at night, or on awakening?
• Does the patient cough after physical activity?
• Does the patient have breathing problems during a particular season (or change of season)?
8

• Do the patient’s colds ‘go to the chest’ or take more than 10 days to resolve?
• Does the patient use any medication (e.g. bronchodilator) when symptoms occur? Is there a response?
If the patient answers “YES” to any of the above questions, suspect asthma.
9

10

11
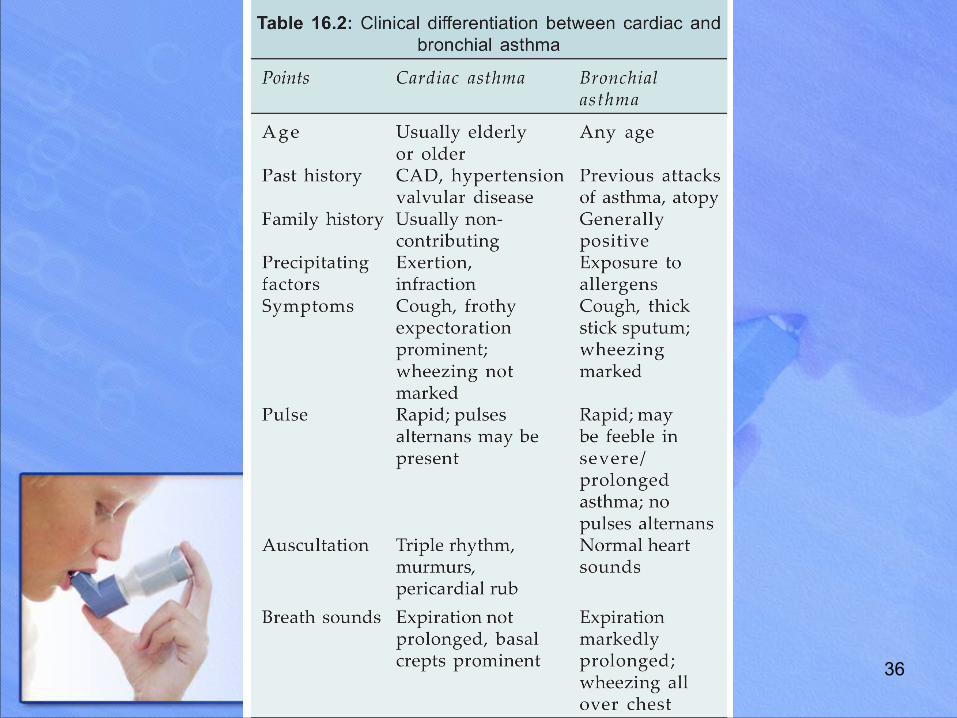
WHEEZE not mean always ASTHMA

12
DIFFERENTIAL DIAGNOSIS OF WHEEZING EXTRATHORACIC AIRWAY OBSTRUCTION · OROPHARYNX—enlarged tonsils, obesity, post-nasal drip · LARYNX—laryngeal edema, epiglottitis, anaphylaxis. INTRATHORACIC AIRWAY OBSTRUCTION · TRACHEAL OBSTRUCTION— foreign body · TRACHEAL COMPRESSION—goiter. · LOWER AIRWAY OBSTRUCTION—asthma, COPD, bronchiectasis, malignancy · PARENCHYMA—pulmonary edema · VASCULAR—pulmonary embolism
Inspiratory wheeze is associated with Extrathoracic airway obstruction Expiratory wheeze is associated with Intrathoracic airway obstruction.

Pulmonary function test❖OBSTRUCTIVE PATTERN
➢FEV1 ↓ <80% ➢FVC normal OR < 80%
predicted ➢FEV1/ FVC ↓ <70%
13

Confirm Diagnostic testing OBSTRUCTIVE PATTERN Diagnosis of asthma can be confirmed by : Compatible clinical history and examination plus
either/or : ❖FEV1 ≥15% (200ML)increase following
administration of inhalation bronchodilator (20 minutes) or trial of oral corticosteroids (2 weeks) (reversibility test).
❖ >20%diurnal variation on ≥3days in a week for 2 weeks on PEF diary (PEF test).
14

15

A home monitoring of peak expiratory flow (PEF) for 2 weeks may help to detect an increased variability of the airway caliber, and assist in making the diagnosis of asthma.diurnal variability of PEF of more than 20% is diagnostic of asthma
16

17

Other investigations Measurement of allergic status: the presence of atopy may be demonstrated by skin prick
tests, measurement of total and allergen-specific IgE, and eosinophilia.
Radiological examination: A chest X-ray may be helpful in excluding a pneumothorax,
which can occur as a complication ,or in detecting the pulmonary infiltrates associated with allergic broncho- pulmonary aspergillosis.
• Assessment of eosinophilic airway inflammation: An induced sputum differential eosinophil count of greater
than 2% or exhaled breath nitric oxide concentration (FENO) may support the diagnosis of steroid sensitive asthma.
18
19

20
● Following diagnosis, it is necessary to classify the severity of asthma and monitor at every visit.
The following questions are important in assessing patients with asthma: In the past 4 weeks, how many times have you: • Had problems with coughing, wheezing, shortness of
breath, or chest tightness during the day? • Awakened at night from sleep because of coughing or
other asthma symptoms? ● Had asthma symptoms that did not improve within 15 minutes of inhaling a short-acting beta2 agonist? ● Missed days from work? ● Had symptoms while exercising ? ● What are your highest and lowest peak flow rates since your last visit?
Assessment of asthma

Chronic Stable Asthma (outpatient management )
21

22
23

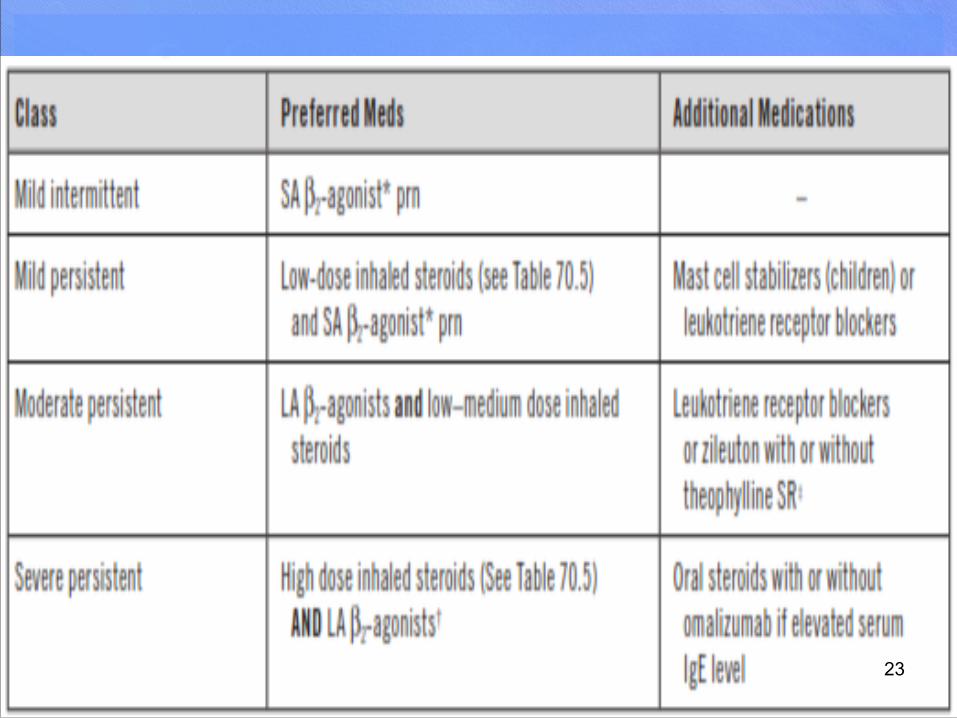
Mild intermittent asthma
For patients with mild intermittent asthma (symptoms less than once a week for 3 months and fewer than two nocturnal episodes per month), it is usually sufficient to prescribe an inhaled short-acting ß-agonist (SABA), such as salbutamol to be used as required.
24

Mild persistent asthma Regular anti-inflammatory therapy (preferably inhaled
corticosteroids-ICS) should be started in addition to inhaled β2-agonists taken on an as required basis in any patient who:
✓ has experienced an exacerbation of asthma in the last 2 years
✓ uses inhaled β2-agonists three times a week or more ✓ reports symptoms three times a week or more ✓ is awakened by asthma one night per week. A reasonable starting dose is 400 µg beclometasone
dipropionate (BDP) or equivalent per day in adults.
25

Moderate persistent asthma If the patient remains poorly controlled despite regular use
of ICS , we can add one of the followings: • Long-acting β2-agonists (LABAs), such as salmeterol
and formoterol (duration of action of at least 12 hours), represent the first choice of add-on therapy.
• Leukotriene receptor antagonists (e.g. montelukast 10 mg daily) are a relatively new class of agent that may be delivered orally and may reduce exacerbations.
• Theophyllines may be useful in some patients but their
unpredictable metabolism, propensity for drug interactions and prominent side-effect profile have limited their use.
26

Severe persistent asthma In adults the dose of ICS may be increased to 2000
µg beclomethasone dipropionate (BDP)/ budesonide (BUD) daily. Oral therapy with leukotriene receptor antagonists, theophyllines or a slow-release β2-agonist may be considered. If the trial of add-on therapy is ineffective it should be discontinued.
Oral itraconazole should be contemplated in patients with ABPA.
New therapies such as monoclonal antibodies directed against IgE (omalizumab) may prove helpful
27

prednisolone therapy (usually administered as a single daily dose in the morning) should be prescribed in the lowest amount necessary to control symptoms.
Patients on long-term corticosteroid tablets (> 3 months) or receiving more than three or four courses per year will be at risk of systemic side-effects.
Osteoporosis can be prevented in this group of patients using bisphosphonates.
Steroid-sparing therapies such as methotrexate, ciclosporin or oral gold may be considered.
28
Step-down therapy
Once asthma control is established (3months), the dose of inhaled (or oral) corticosteroid should be titrated to the lowest dose at which effective control of asthma is maintained
29

MONITORING ASTHMA AT HOME
A peak flow meter is a hand-held device that measures how fast you can blow air out of your lungs. Measuring your peak flow regularly can help you tell whether your asthma is getting worse.
30

Clinical criteria defining good asthma control
• 1- negligible symptoms . • 2-no severe acute attacks . • 3- normal exercise tolerance and
daily activities . • 4-Normal PEFR .
31

acute severe asthma (STATUS ASTHMATICUS)Need hospital management ❖ Features • Peak flow less than 50% of your personal best • Shortness of breath (RR >25/MIN) • Heart rate >110/MIN • Inability to complete sentences in 1 breath.
32

Life-threatening features • PEF 33-50% predicted (< 100 l/min) • SpO2 < 92% • Silent chest • Cyanosis • Feeble respiratory effort • Bradycardia or arrhythmias • Hypotension • Exhaustion • Confusion • Coma
33
34
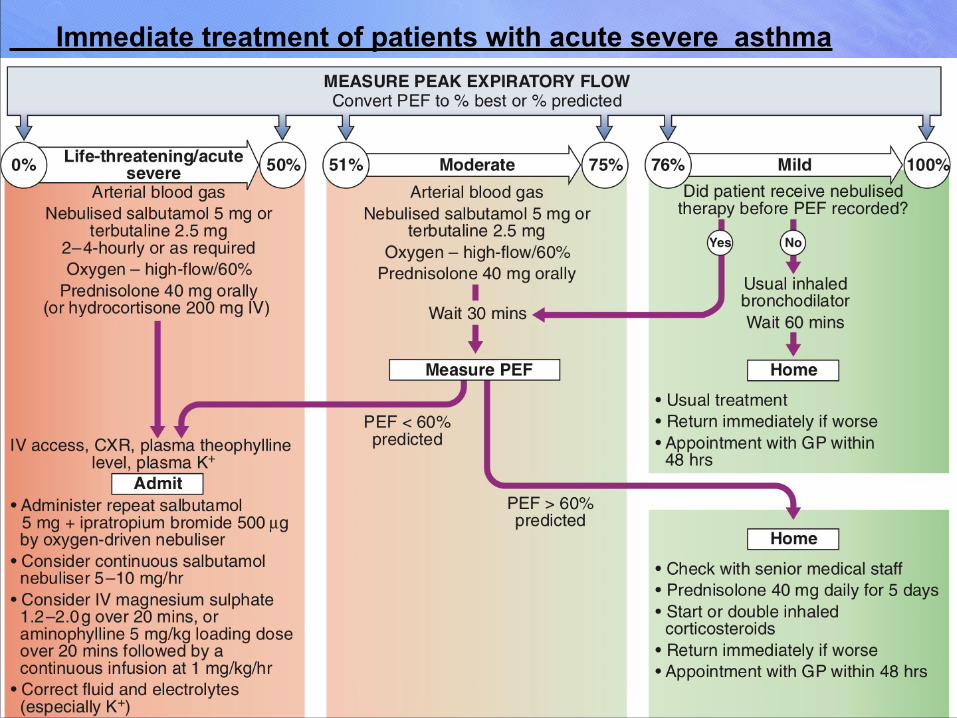
Immediate treatment of patients with acute severe asthma

Indications for assisted ventilation in acute severe asthma• COMA • RESPIRATORY ARREST • PaO2 <60 mm HG • PaCO2 >45 mm HG • Low PH
35
36

THANK YOU
37