Chapter 3: Antigen Recognition by T lymphocytes TCR T H 1 - T Helper cell type 1 T H 2 - T Helper...
56
Chapter 3: Antigen Recognition by T lymphocytes TCR T H 1 - T Helper cell type 1 T H 2 - T Helper cell type 2 T C or TCL - cytotoxic T cell
-
Upload
mavis-norman -
Category
Documents
-
view
216 -
download
1
Transcript of Chapter 3: Antigen Recognition by T lymphocytes TCR T H 1 - T Helper cell type 1 T H 2 - T Helper...
Chapter 3: Antigen Recognition by T lymphocytes
TCRTH1 - T Helper cell type 1TH2 - T Helper cell type 2TC or TCL - cytotoxic T cell
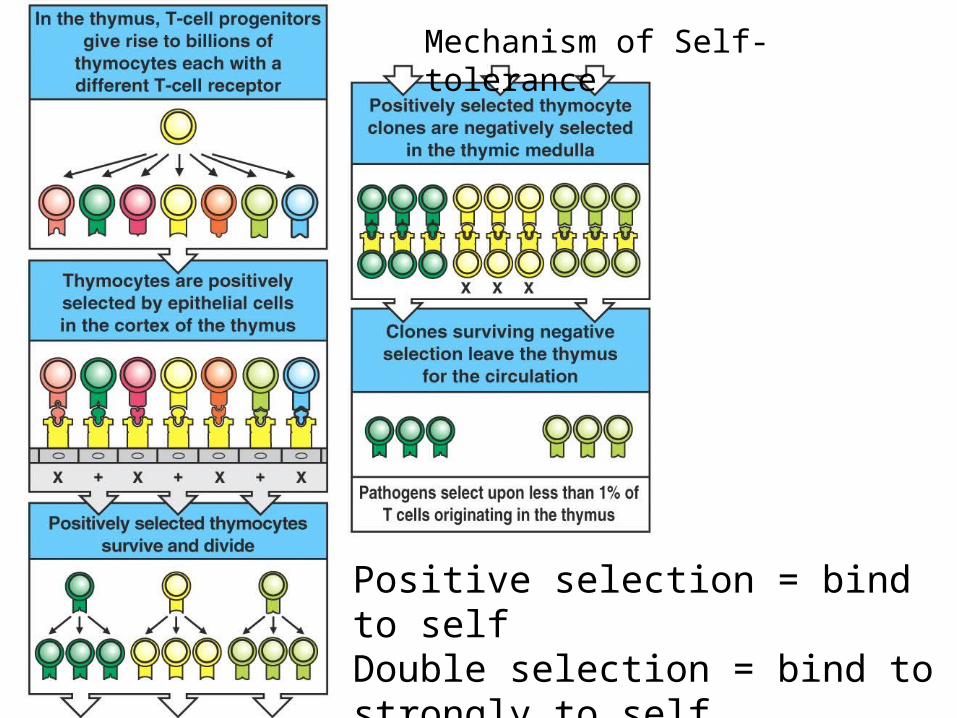
Mechanism of Self-tolerance
Positive selection = bind to selfDouble selection = bind to strongly to self
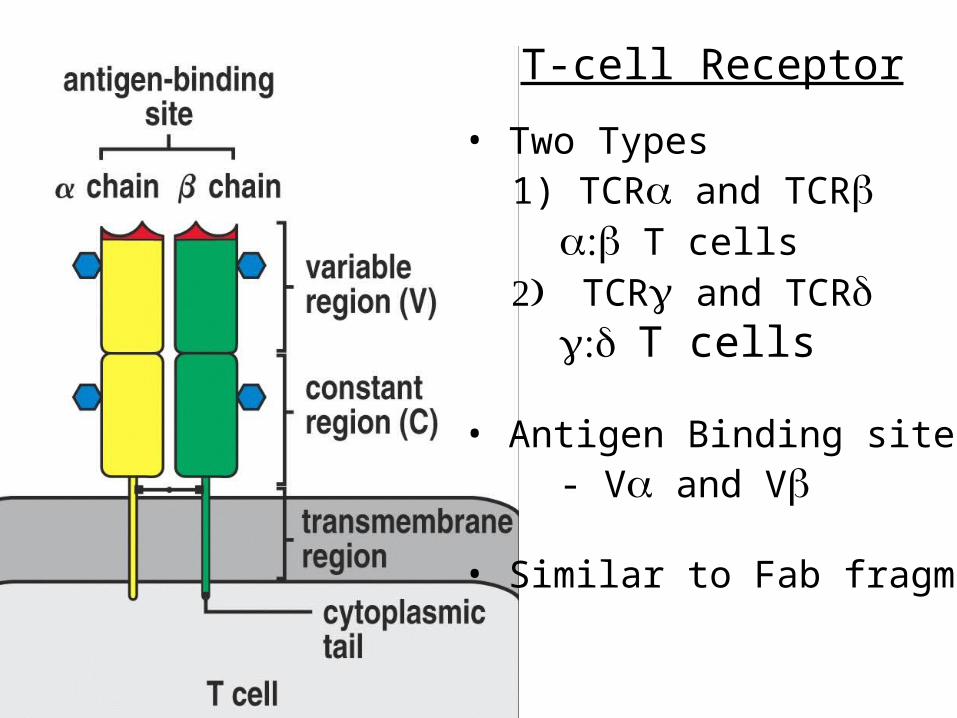
• Two Types1) TCR and TCR
T cellsTCR and TCR
T cells
• Antigen Binding site- V and V
• Similar to Fab fragment
T-cell Receptor
• T cells- Recognize MHC:peptide complex- Diverse Functions
A) Stimulate other immune cellsB) Cytotoxic - kill infected host cells
- Cell:cell interactions
• T cells- Dominant T-cell in epithelial tissue
(only 1-5% in circulation)- Recognizes more than MHC:peptide- Not well characterized
Functions and Properties of T Cells
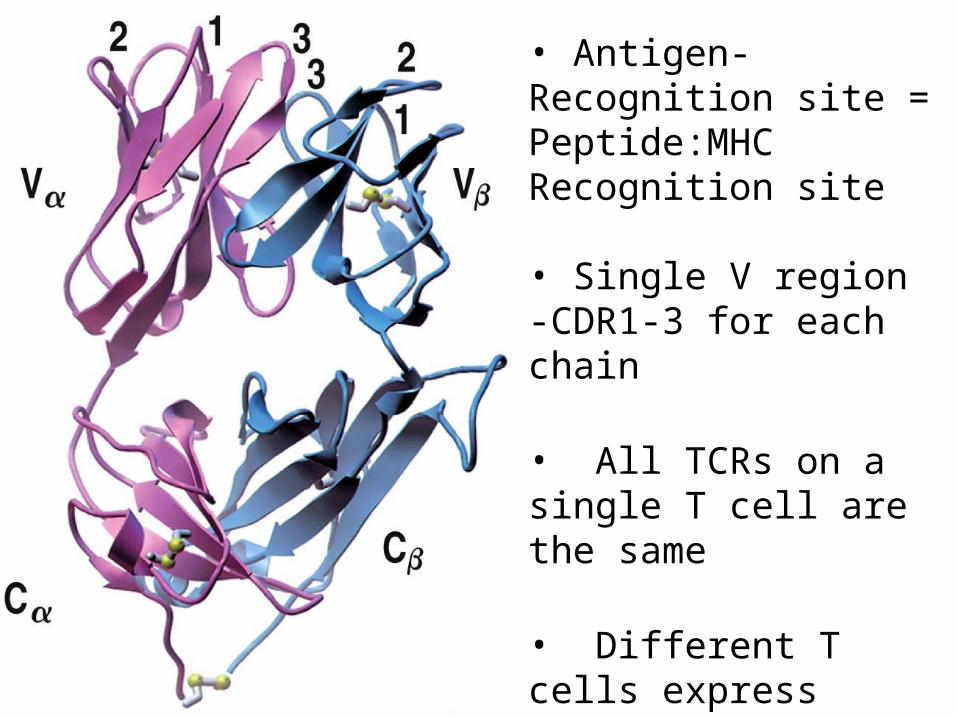
• Antigen-Recognition site = Peptide:MHC Recognition site
• Single V region -CDR1-3 for each chain
• All TCRs on a single T cell are the same
• Different T cells express different TCRs
• Diversity mechanisms like BCRs
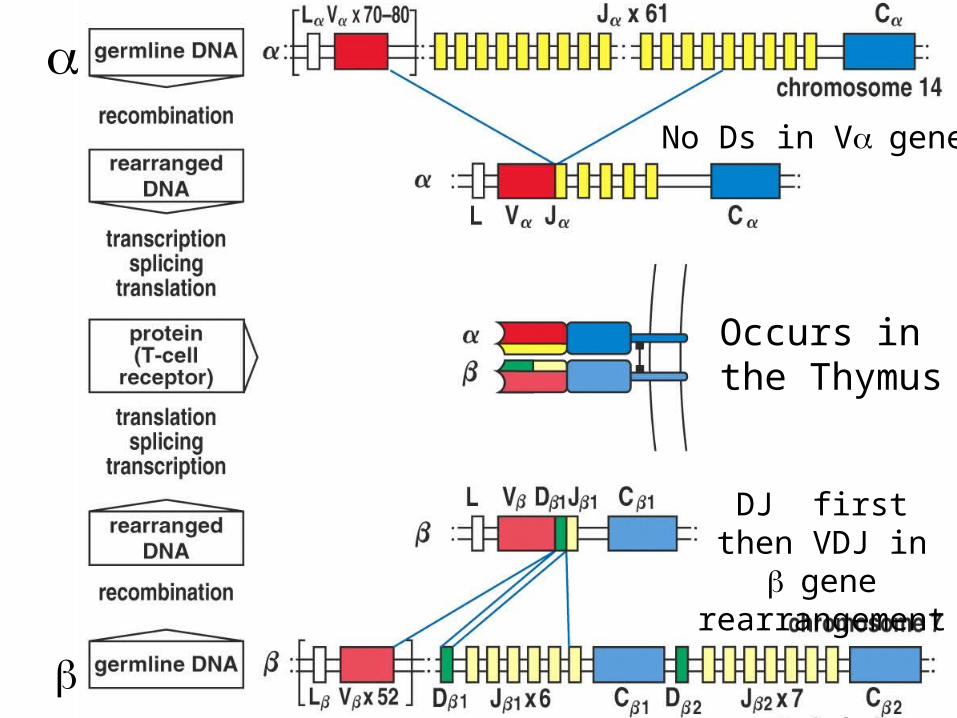
Figure 3-3
No Ds in Vgene
DJ first then VDJ in gene
rearrangement
Occurs in the Thymus
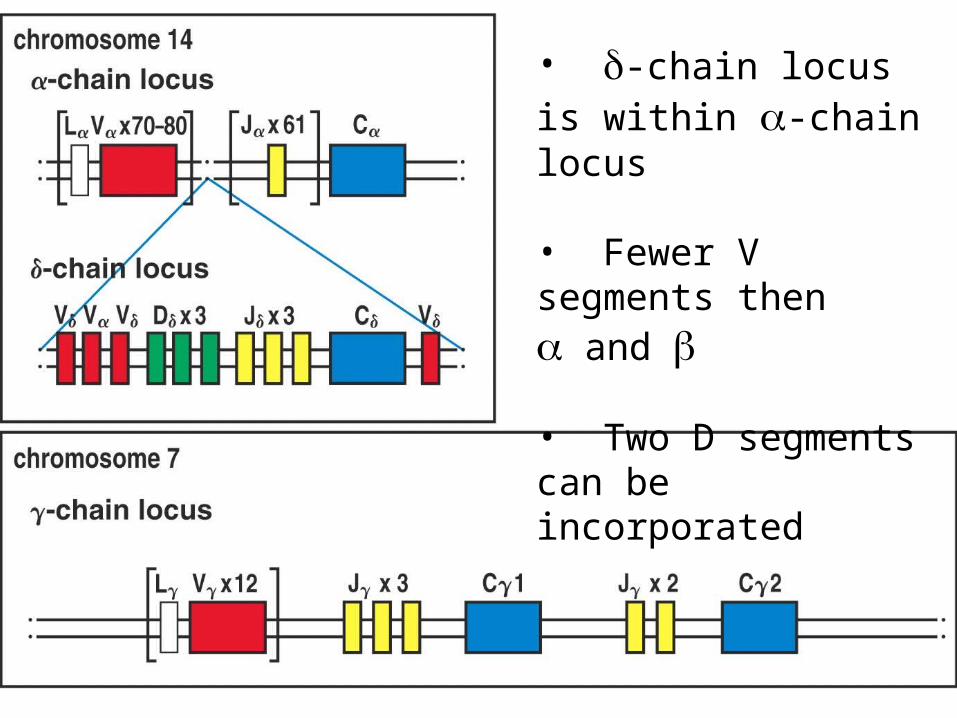
Figure 3-8• -chain locus is within -chain locus
• Fewer V segments then and
• Two D segments can be incorporated
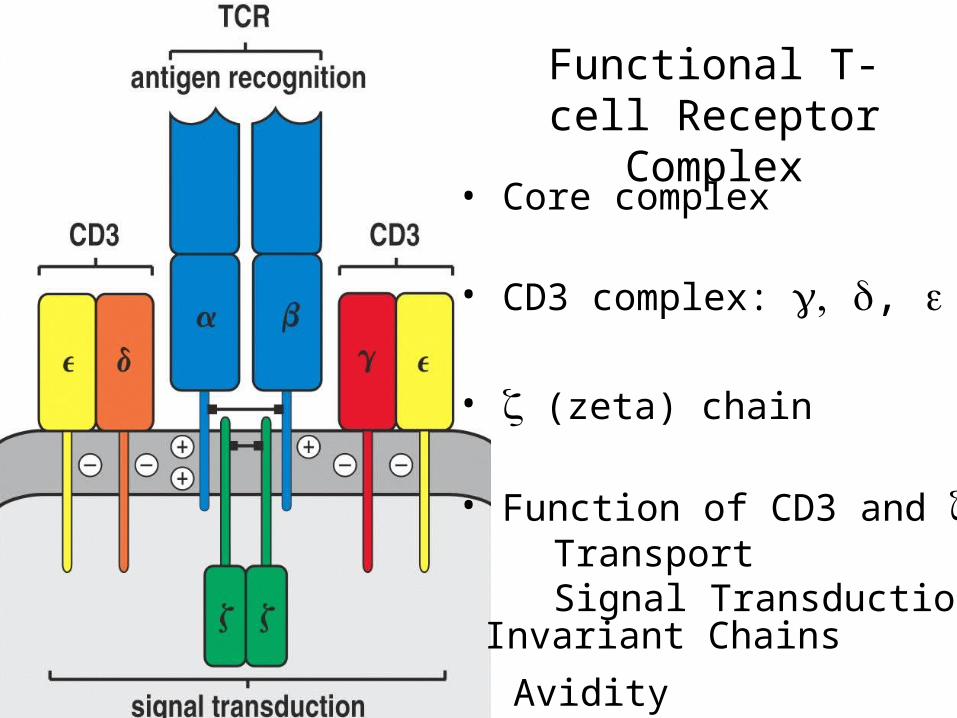
Functional T-cell Receptor Complex
• Core complex
• CD3 complex: ,
• (zeta) chain
• Function of CD3 and :TransportSignal Transduction
Invariant Chains
Avidity
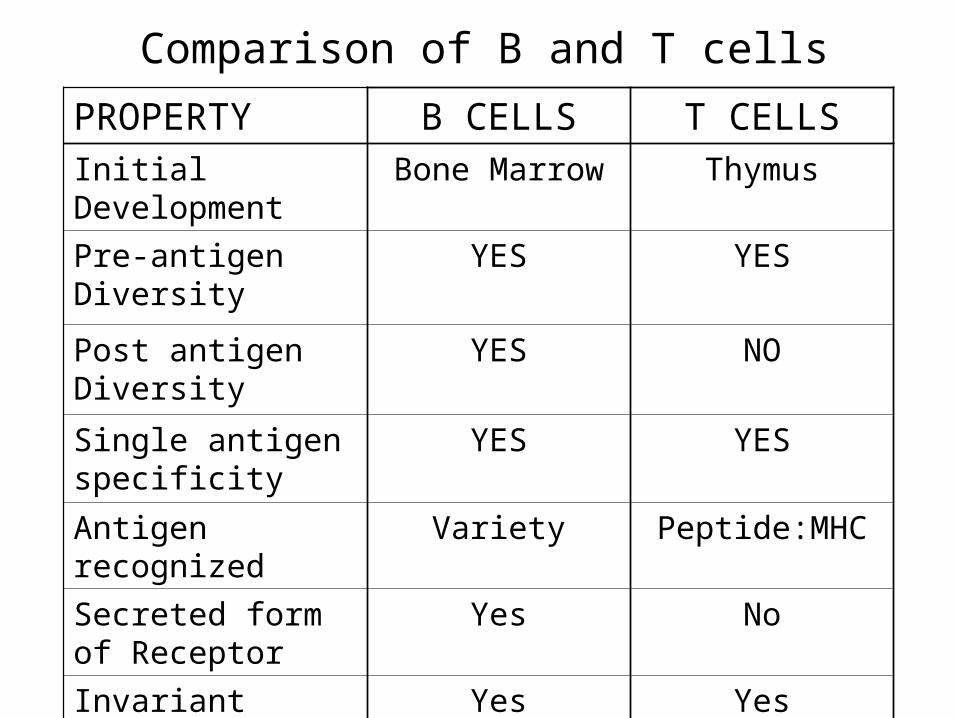
PROPERTY B CELLS T CELLSInitial Development Bone Marrow Thymus
Pre-antigen Diversity
YES YES
Post antigen Diversity
YES NO
Single antigen specificity
YES YES
Antigen recognized Variety Peptide:MHC
Secreted form of Receptor
Yes No
Invariant signaling subunits
Yes Yes
Comparison of B and T cells
• SCID - severe combined immunodeficiency disease- Many causes but a rare disease- Classified according to lymphocyte profile (T B NK)- Bone Marrow transplant can cure
• Omenn syndrome- RAG proteins have reduced activity- Patient is: T+ B- NK+
• CD3 and CD3 deficiency diseases- Mutations in some CD3 genes- Patient is: T+/TCR- B+ NK+
or T- B+ NK+
Immunodeficiency diseases
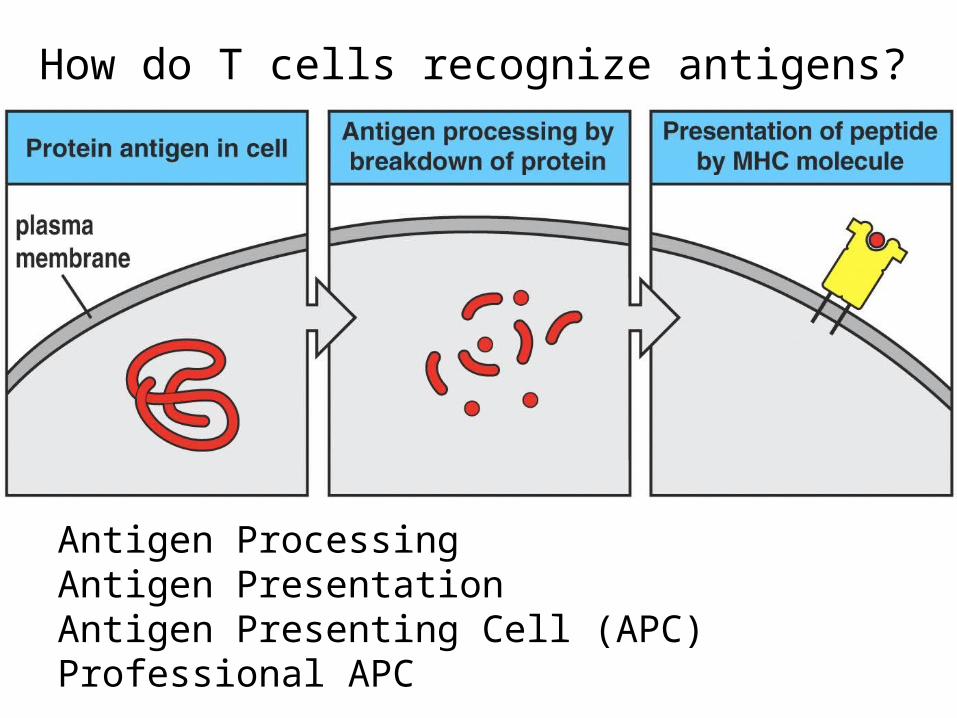
How do T cells recognize antigens?
Antigen ProcessingAntigen PresentationAntigen Presenting Cell (APC)Professional APC
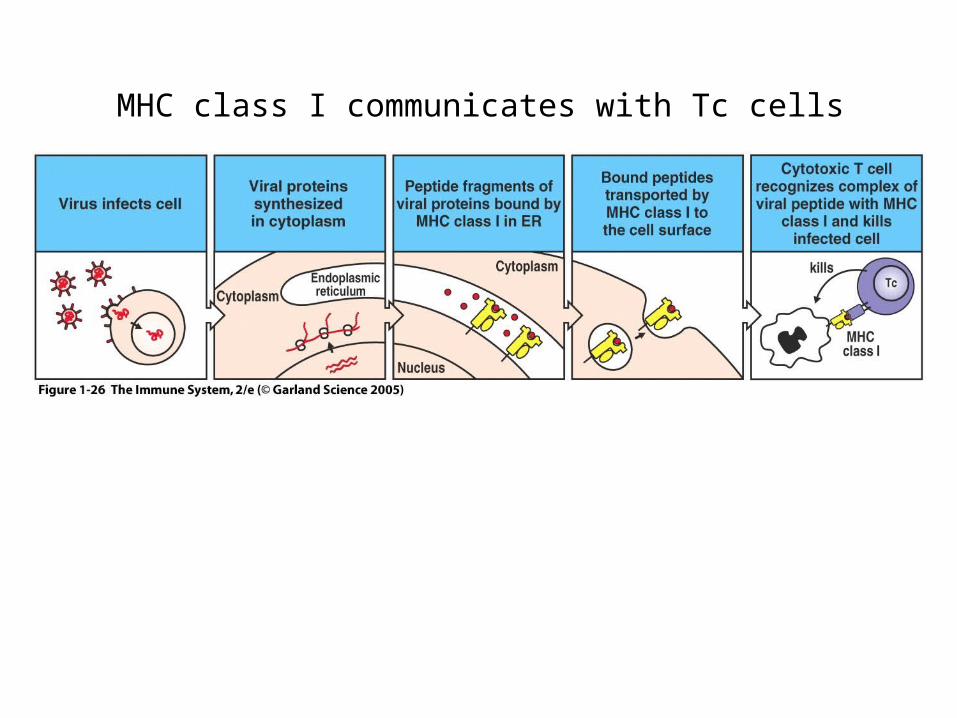
MHC class I communicates with Tc cells
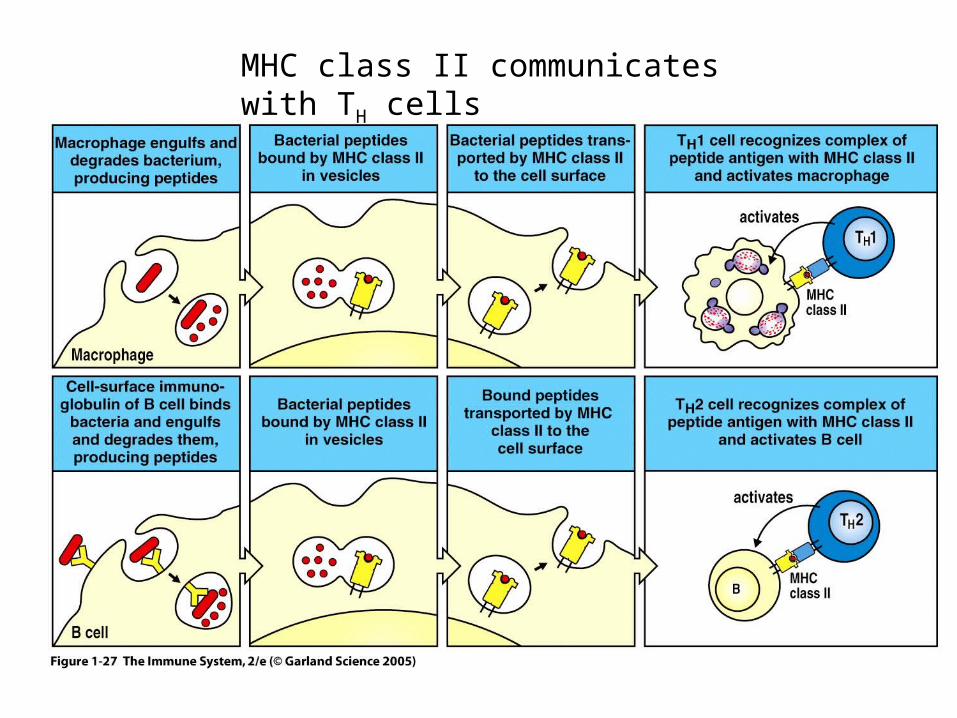
MHC class II communicates with TH cells
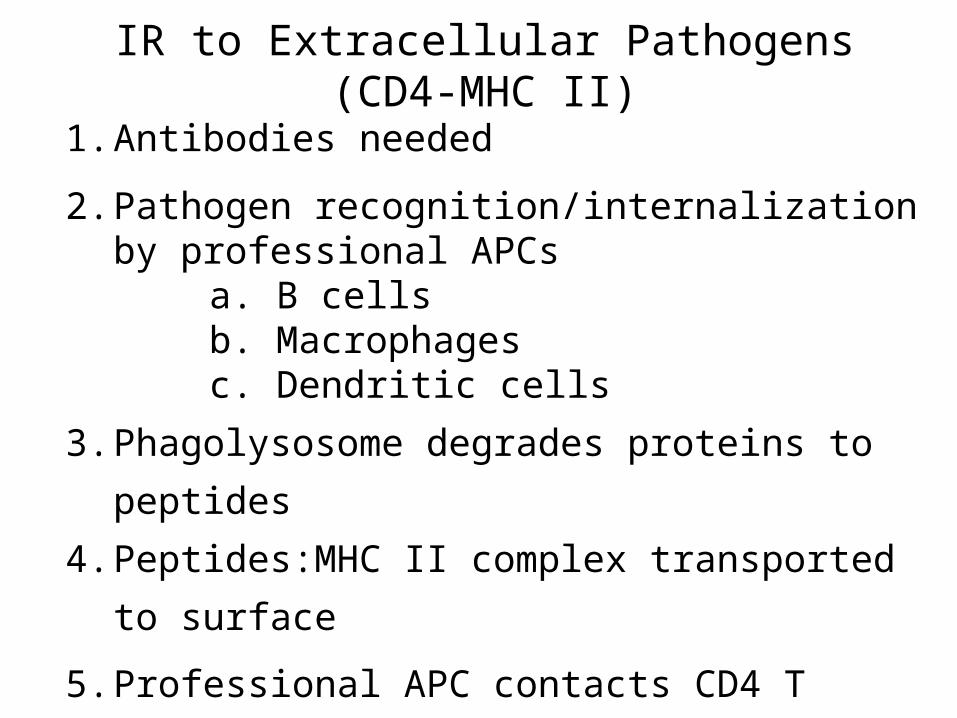
IR to Extracellular Pathogens(CD4-MHC II)
1. Antibodies needed
2. Pathogen recognition/internalization by professional APCs
a. B cellsb. Macrophagesc. Dendritic cells
3. Phagolysosome degrades proteins to peptides
4. Peptides:MHC II complex transported to surface
5. Professional APC contacts CD4 T cells
6. CD4 TH cells secrete cytokines to signal B cell maturation
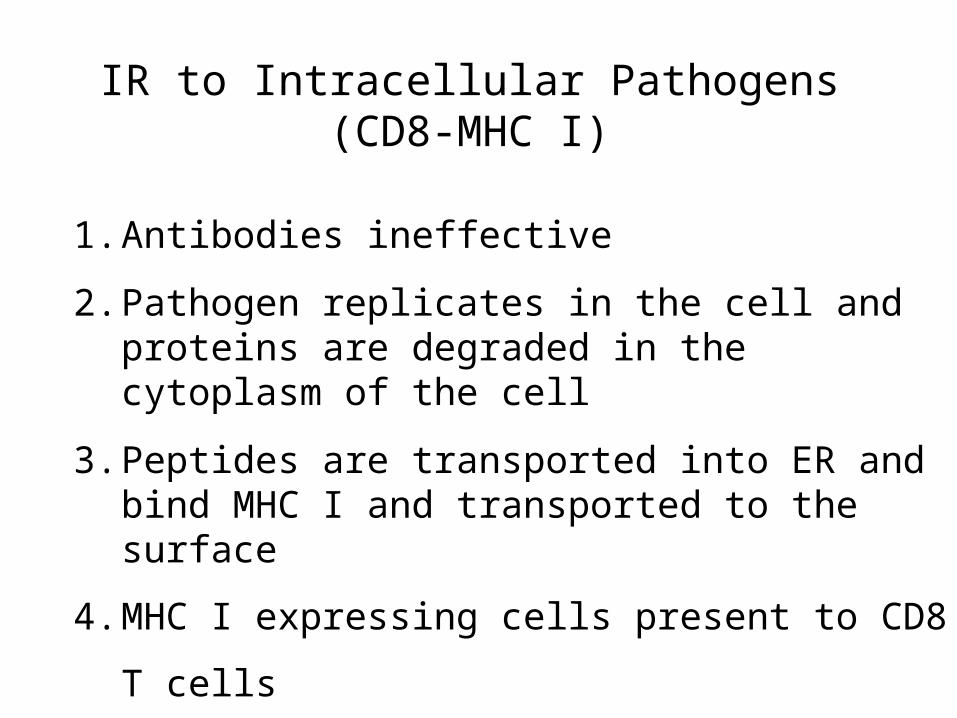
IR to Intracellular Pathogens(CD8-MHC I)
1. Antibodies ineffective
2. Pathogen replicates in the cell and proteins are degraded in the cytoplasm of the cell
3. Peptides are transported into ER and bind MHC I and transported to the surface
4. MHC I expressing cells present to CD8 T cells
5. CD8 T cells (cytotoxic T cell, CTL) kills host cell
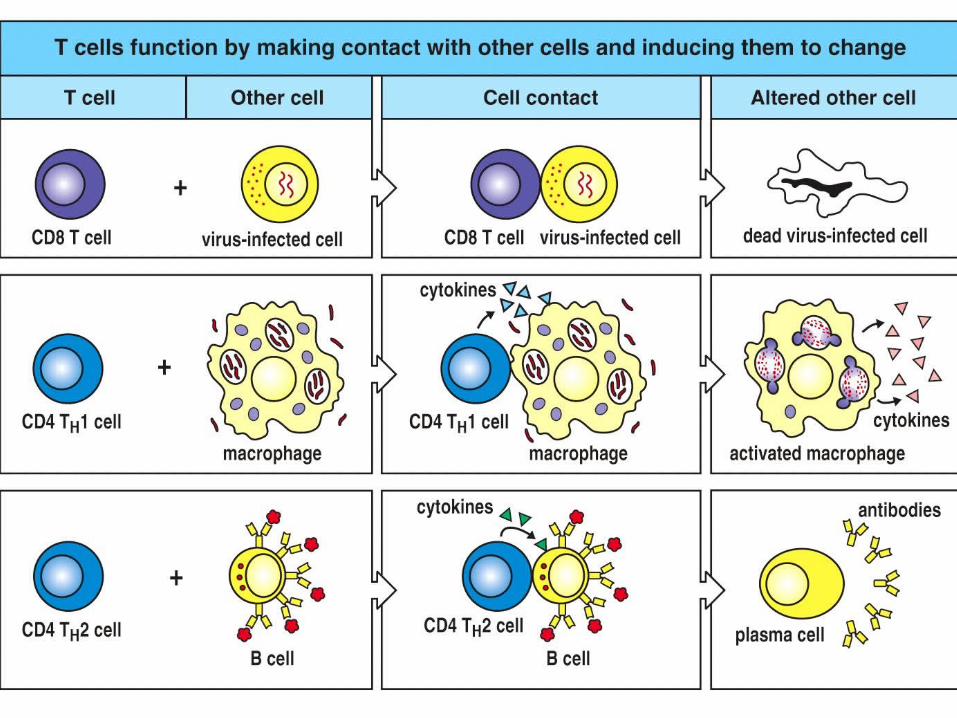
Figure 3-11
Structures involved in MHC Presentation
TCR
CD4 and CD8
MHC1 and MHCII
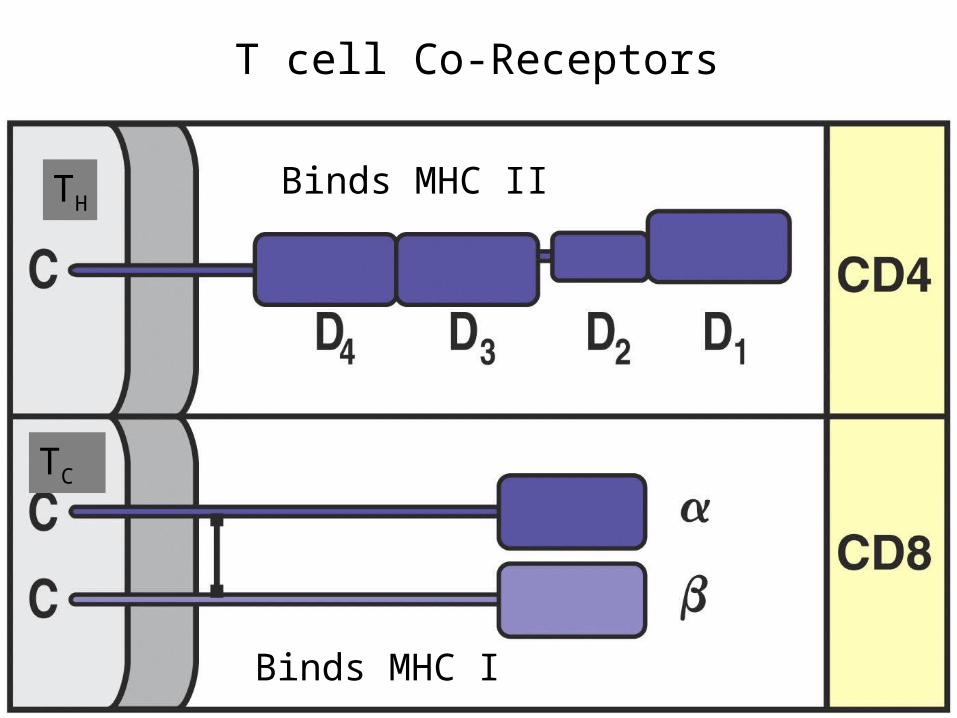
T cell Co-Receptors
Binds MHC I
Binds MHC IITH
TC
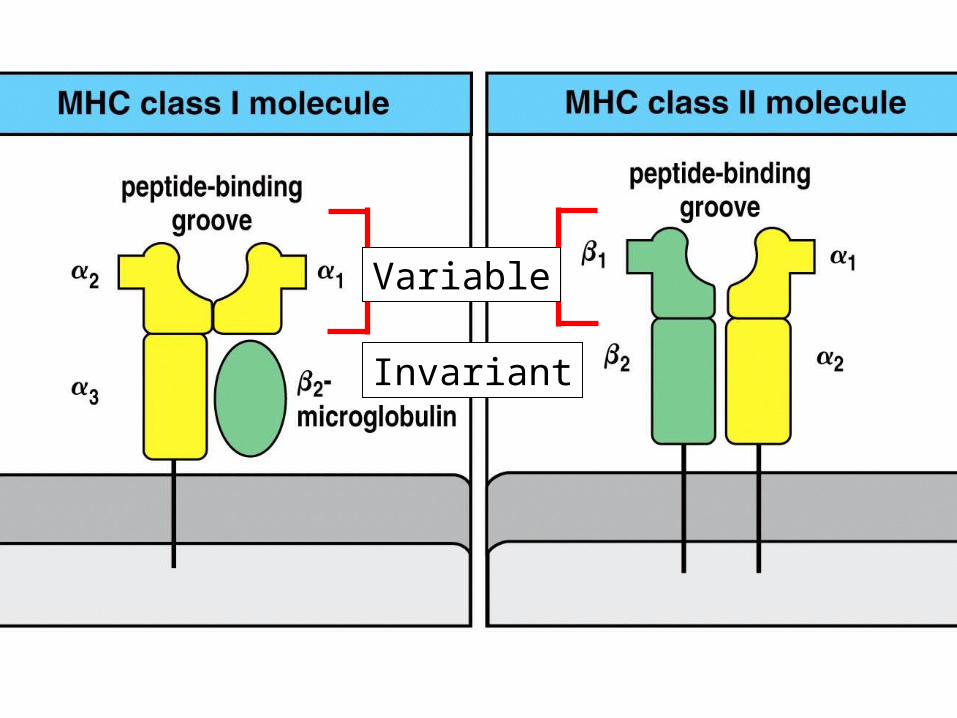
Figure 3-13 part 1 of 2
Variable
Invariant
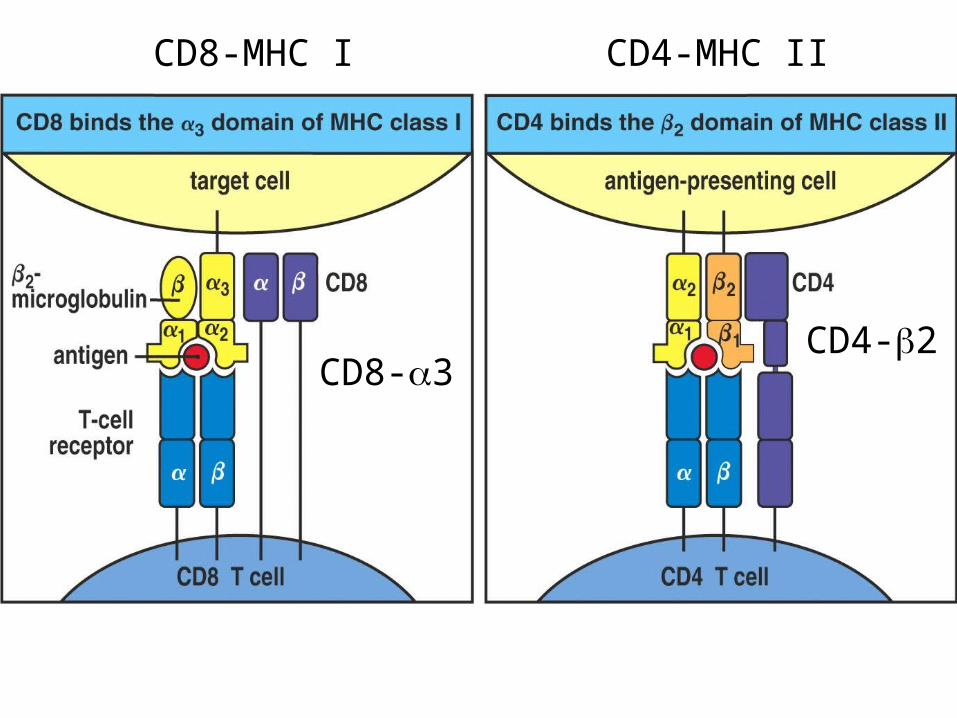
CD8-MHC I CD4-MHC II
CD8-3CD4-2
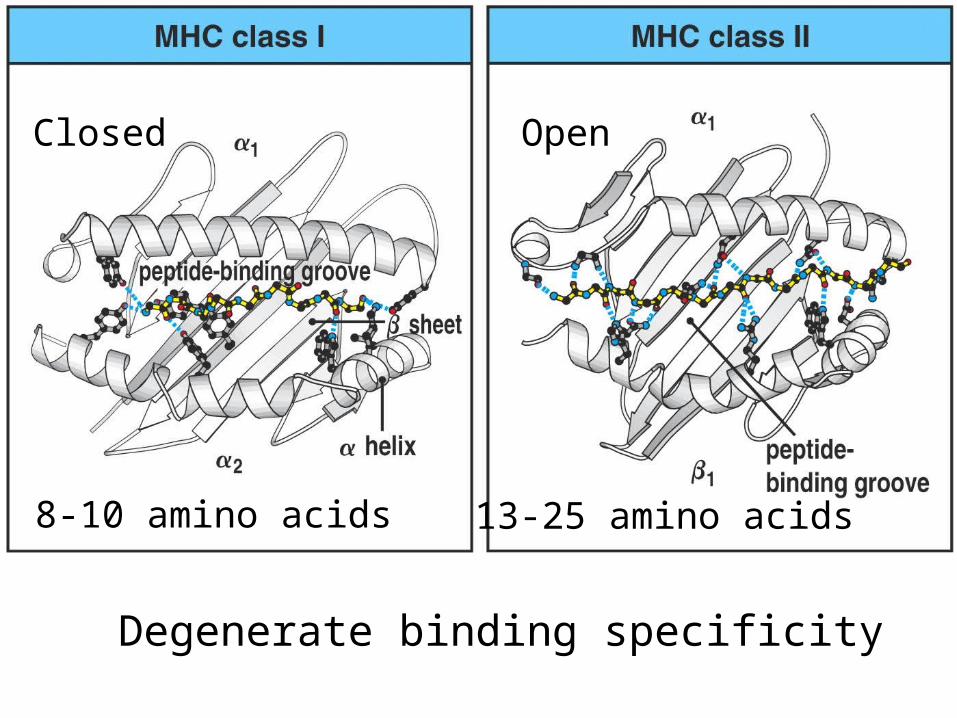
Figure 3-15Closed Open
8-10 amino acids 13-25 amino acids
Degenerate binding specificity
Figure 3-16
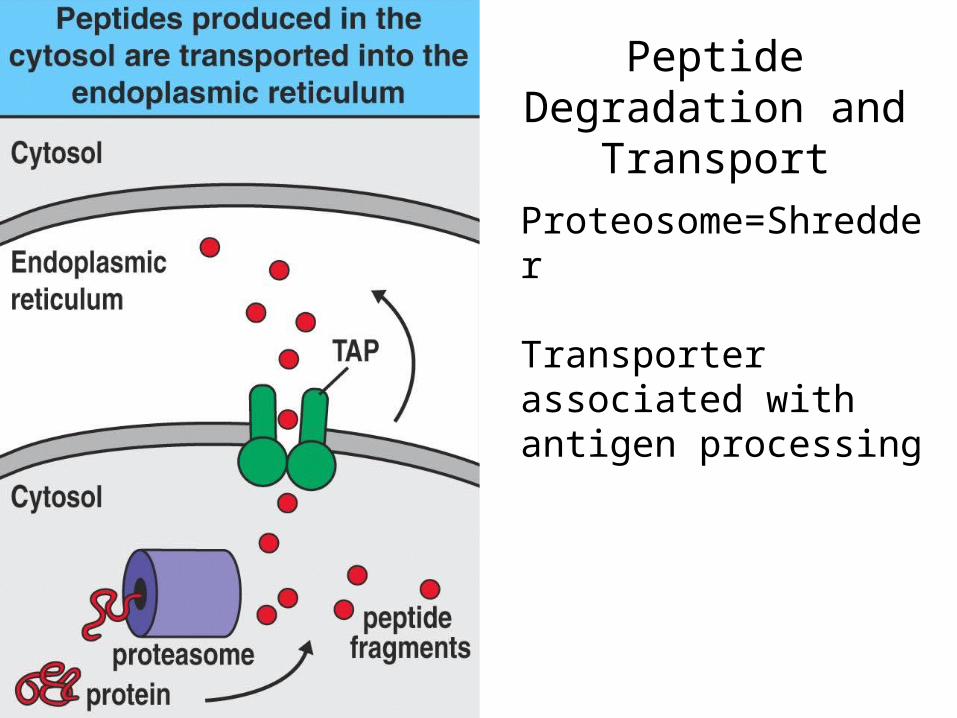
Proteosome=Shredder
Transporter associated with antigen processing
Peptide Degradation and Transport
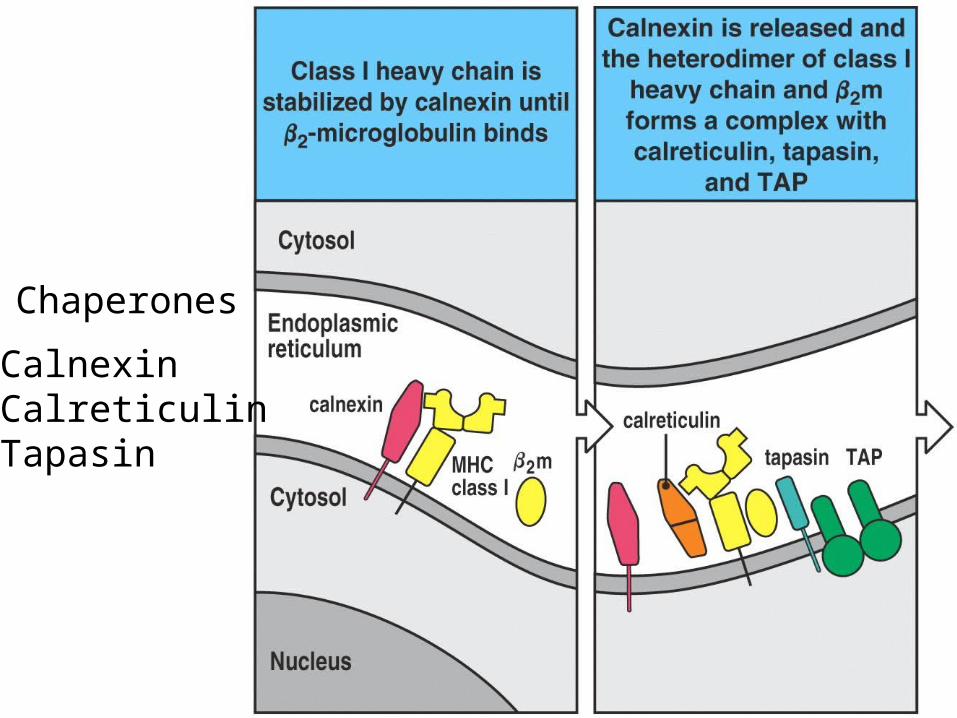
Chaperones
CalnexinCalreticulinTapasin
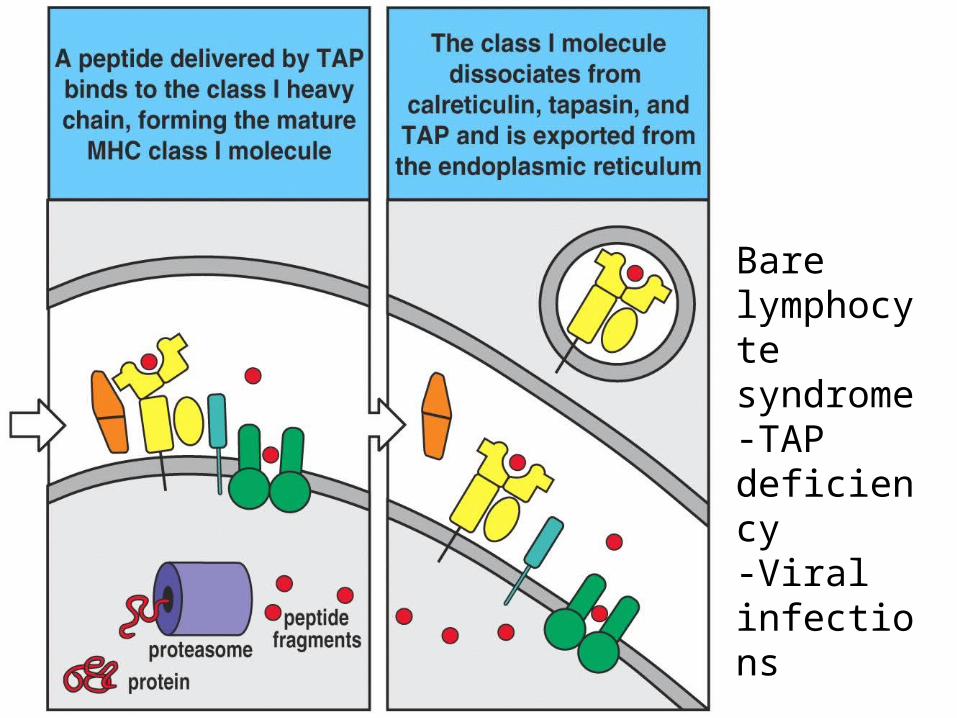
Bare lymphocyte syndrome-TAP deficiency-Viral infections
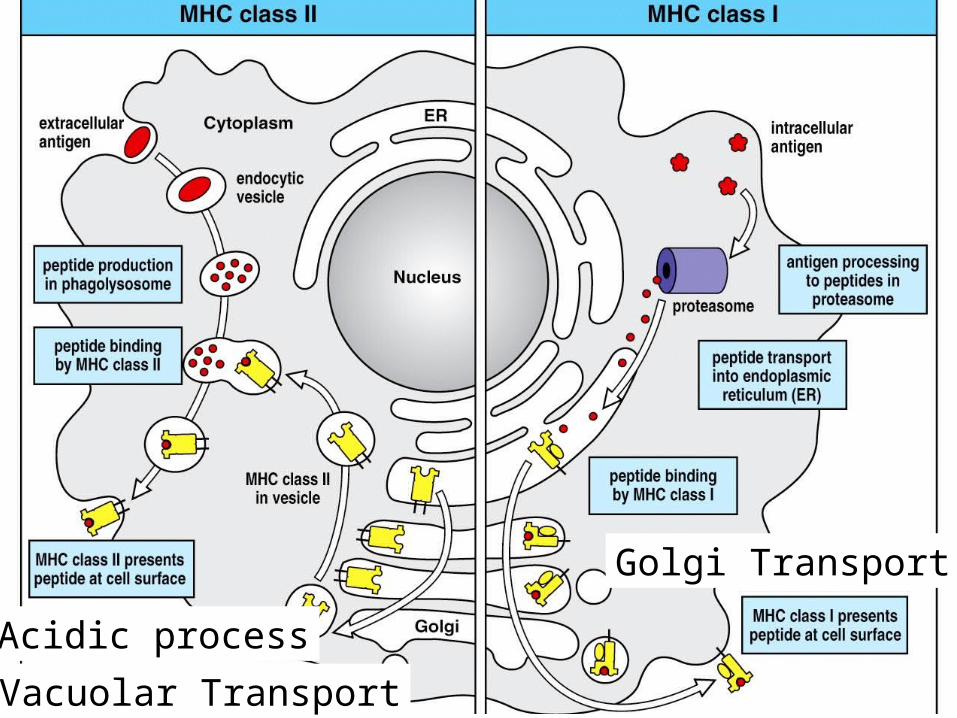
Figure 3-19
Acidic process
Golgi Transport
Vacuolar Transport
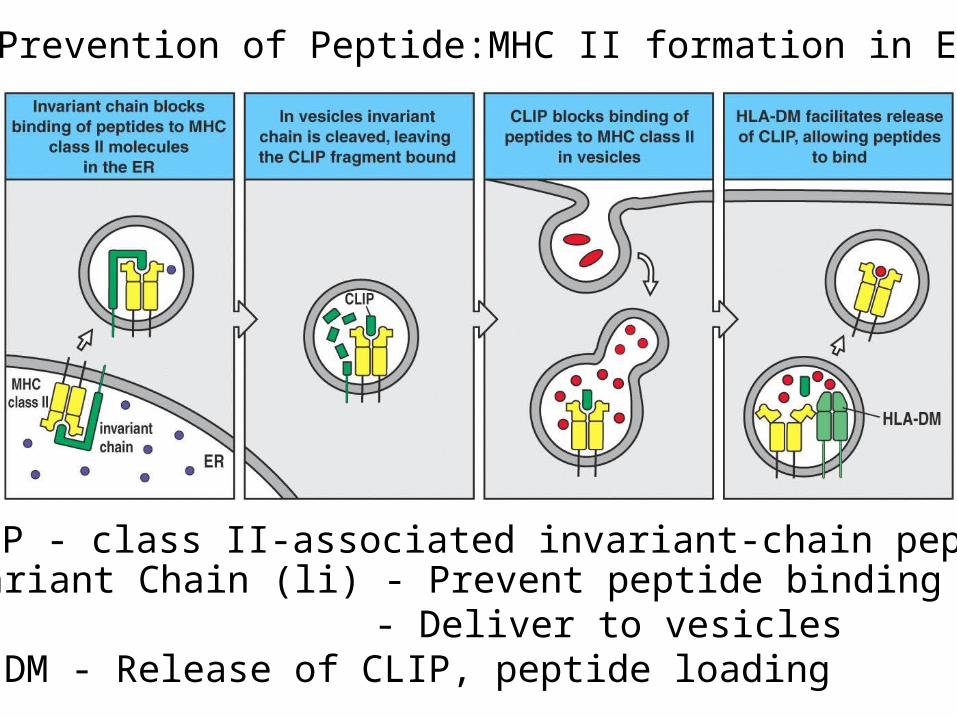
CLIP - class II-associated invariant-chain peptide
Prevention of Peptide:MHC II formation in ER
Invariant Chain (li) - Prevent peptide binding in ER - Deliver to vesicles
HLA-DM - Release of CLIP, peptide loading
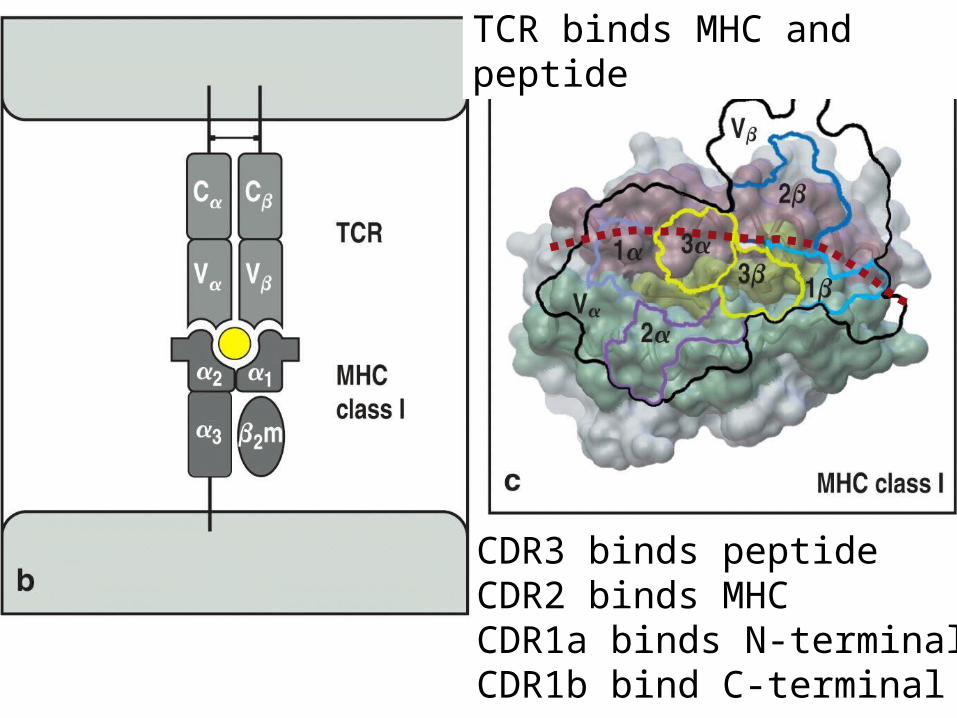
Figure 3-21 part 2 of 3
TCR binds MHC and peptide
CDR3 binds peptideCDR2 binds MHCCDR1a binds N-terminalCDR1b bind C-terminal
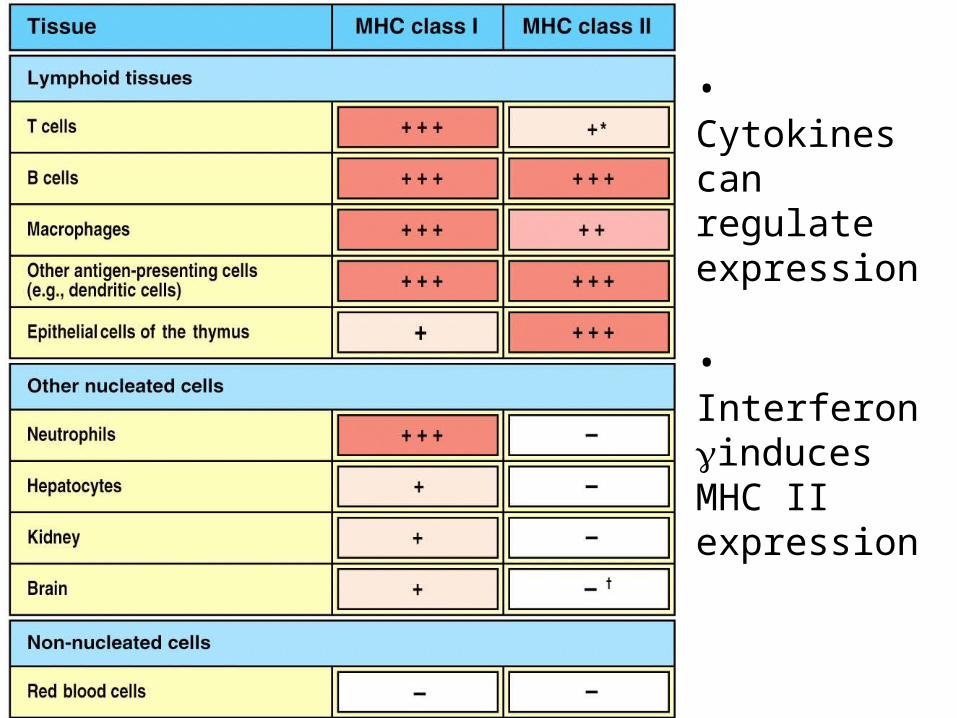
• Cytokines can regulate expression
• Interferon induces MHC II expression
T-cell Diversity- Recombination- Structure of TCR and associated molecules- Immunodeficiency diseases
Antigen Processing and Presentation- Intracellular vs Extracellular- MHC structure
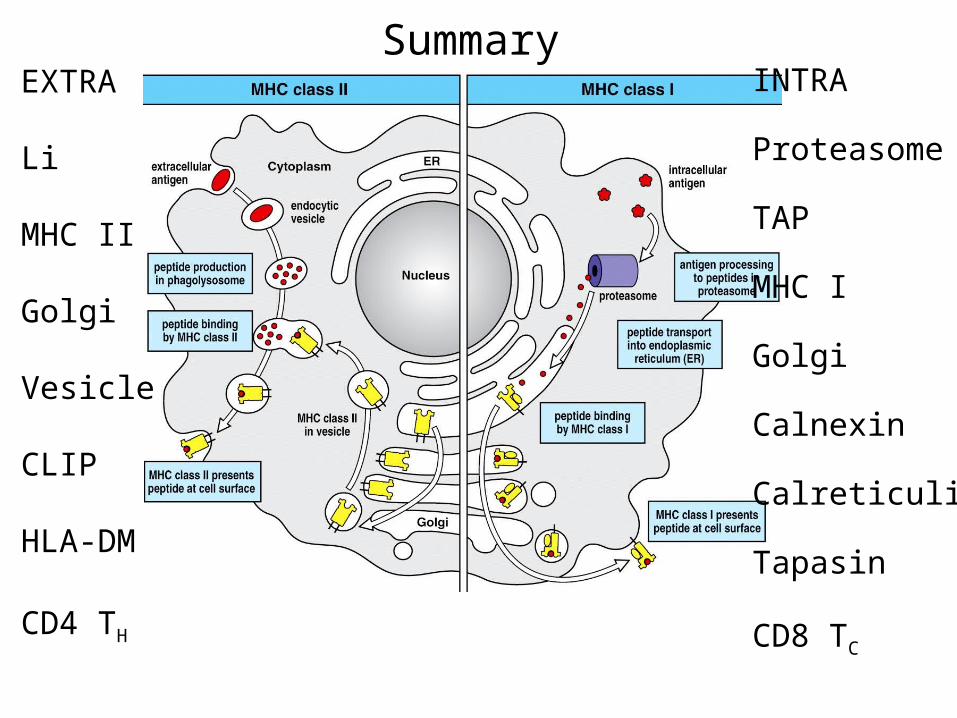
INTRA
Proteasome
TAP
MHC I
Golgi
Calnexin
Calreticulin
Tapasin
CD8 TC
EXTRA
Li
MHC II
Golgi
Vesicle
CLIP
HLA-DM
CD4 TH
Summary
Alleles: different forms of one geneAllotypes: different forms of one protein (isoforms)
Polymorphic: alternative forms of one gene = Many allelesOligomorphic: a few forms of one gene = Few allelesMonomorphic: no polymorphism
Homozygous: same allele on both inherited chromosomesHeterozygous: different allele on both inherited chromosomes
MHC in humans is called HLA (human leukocyte antigen complex)
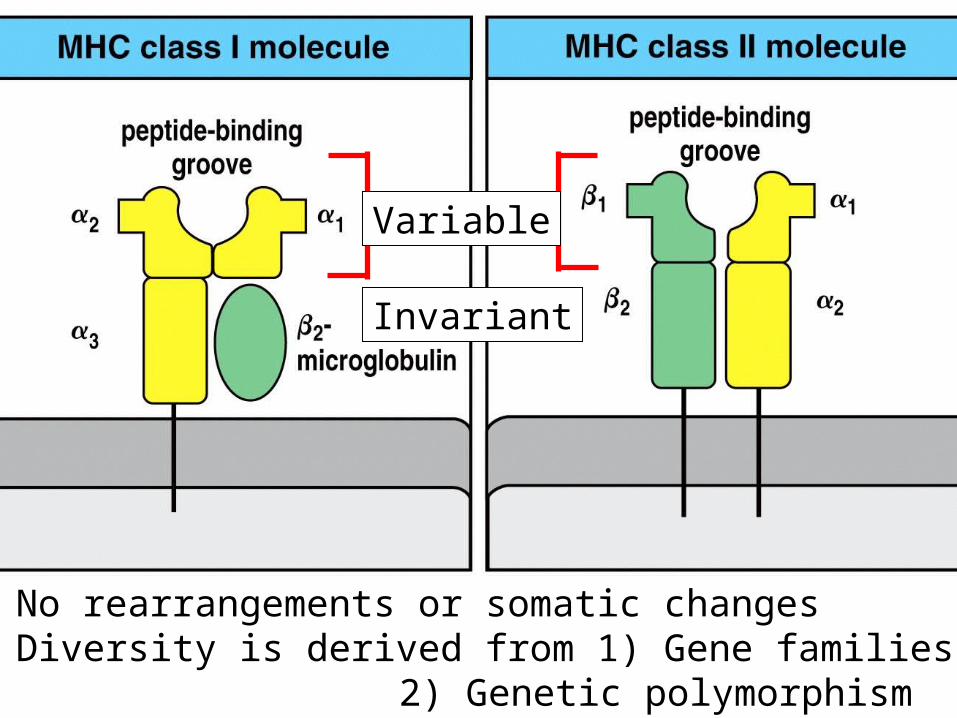
Figure 3-13 part 1 of 2
Variable
Invariant
No rearrangements or somatic changesDiversity is derived from 1) Gene families
2) Genetic polymorphism
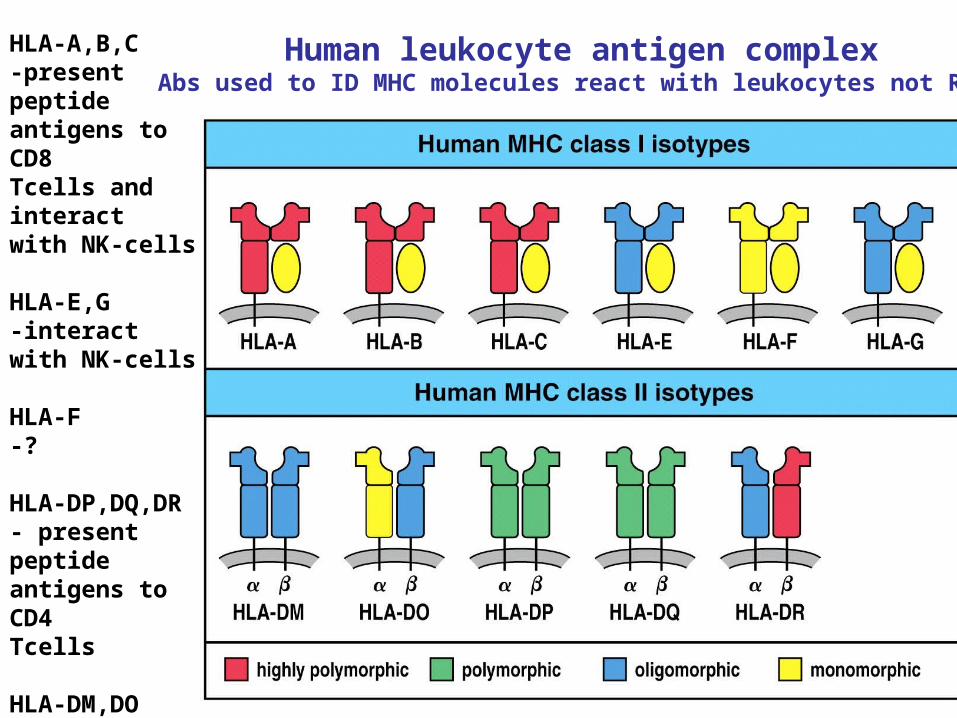
HLA-A,B,C-present peptide antigens to CD8Tcells and interactwith NK-cells
HLA-E,G-interactwith NK-cells
HLA-F-?
HLA-DP,DQ,DR- present peptide antigens to CD4Tcells
HLA-DM,DO-regulate peptide loading of DP,DQ,DR
Human leukocyte antigen complexAbs used to ID MHC molecules react with leukocytes not RBCs
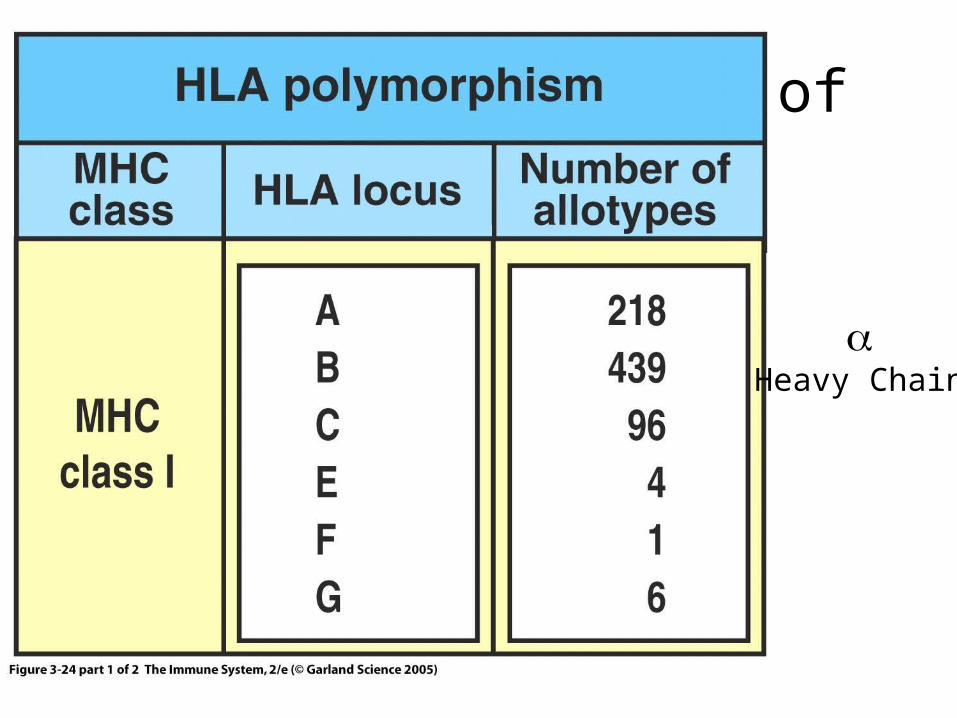
Figure 3-24 part 1 of 2
Heavy Chain
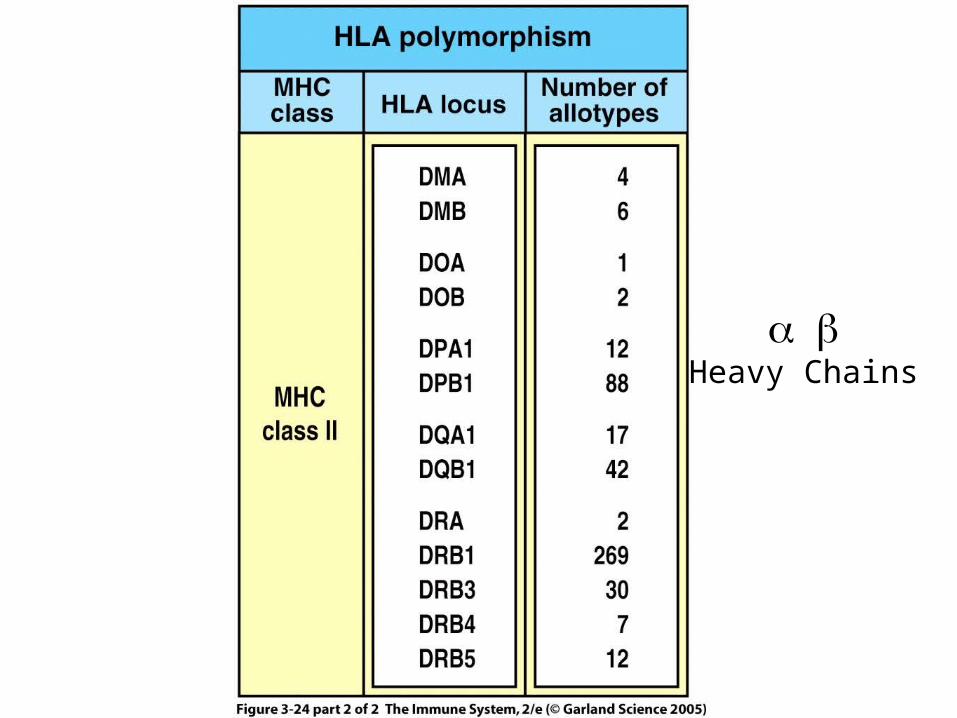
Heavy Chains
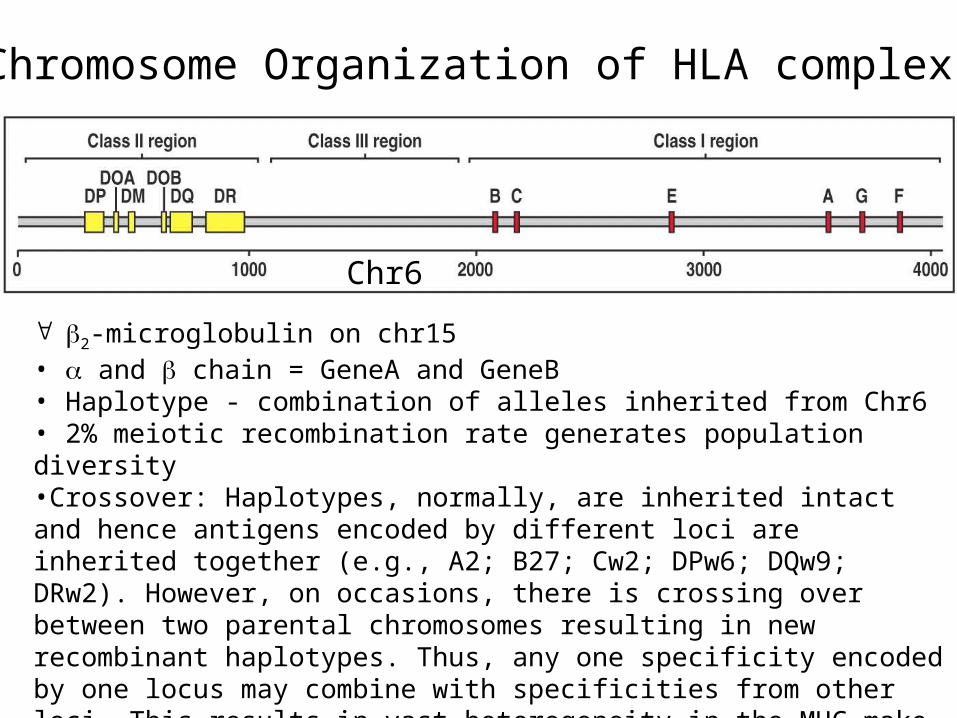
2-microglobulin on chr15• and chain = GeneA and GeneB• Haplotype - combination of alleles inherited from Chr6• 2% meiotic recombination rate generates population diversity•Crossover: Haplotypes, normally, are inherited intact and hence antigens encoded by different loci are inherited together (e.g., A2; B27; Cw2; DPw6; DQw9; DRw2). However, on occasions, there is crossing over between two parental chromosomes resulting in new recombinant haplotypes. Thus, any one specificity encoded by one locus may combine with specificities from other loci. This results in vast heterogeneity in the MHC make-up in a given
population.
Chr6
Chromosome Organization of HLA complex
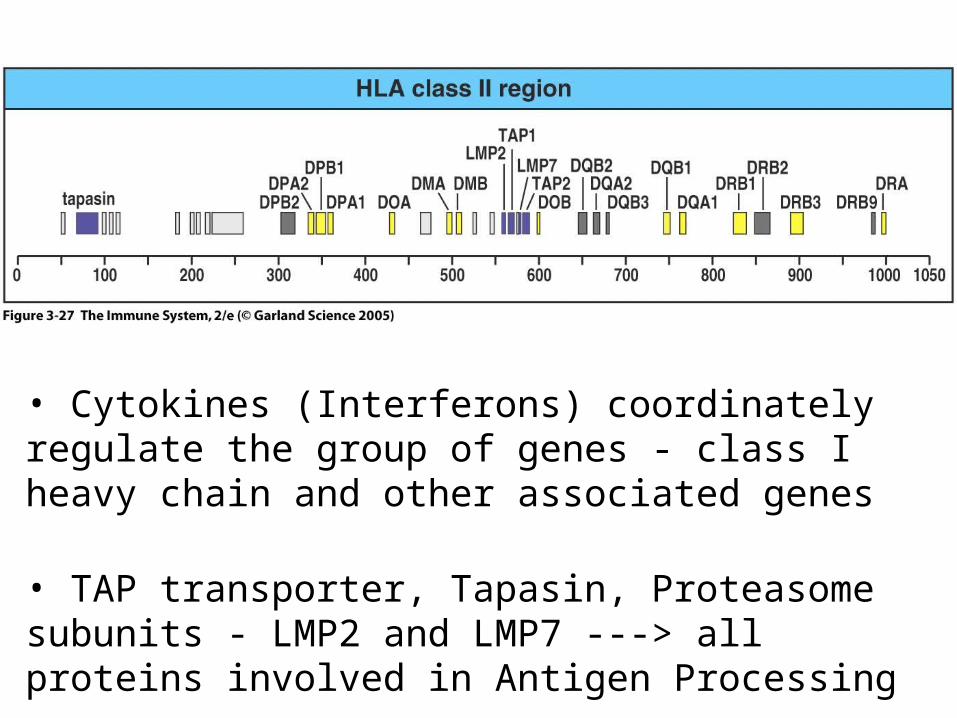
• Cytokines (Interferons) coordinately regulate the group of genes - class I heavy chain and other associated genes
• TAP transporter, Tapasin, Proteasome subunits - LMP2 and LMP7 ---> all proteins involved in Antigen Processing
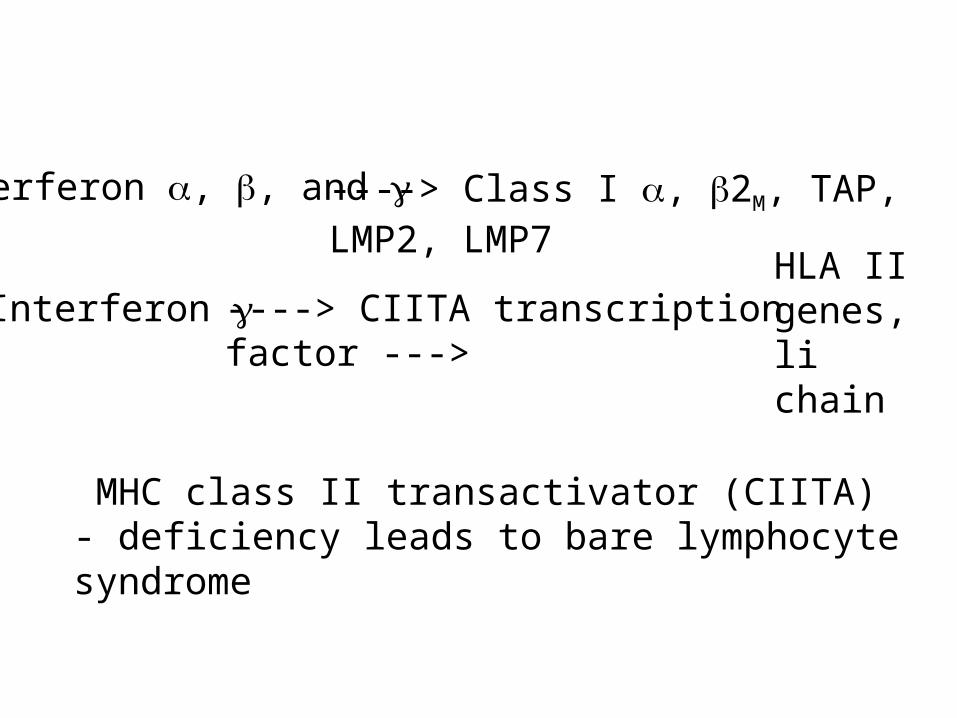
Interferon , , and ----> Class I , 2M, TAP, LMP2, LMP7
Interferon ----> CIITA transcription factor --->
MHC class II transactivator (CIITA) - deficiency leads to bare lymphocyte syndrome
HLA II genes, li chain
MHC I (single peptide binding chain ): 3 genes to present antigen
HLA-A, HLA-B, HLA-C
MHC II (two chains, and ): 3 genesb to present antigen
HLA-DQ, HLA-DP, HLA-DR
Each MHC II locus encodes a gene for the chain and a gene for the chain:
e.g. HLA-DQA, HLA-DQB => MHC II isoformsHLA-DPA, HLA-DPB => MHC II isoformsHLA-DRA, HLA-DRB => MHC II isoforms
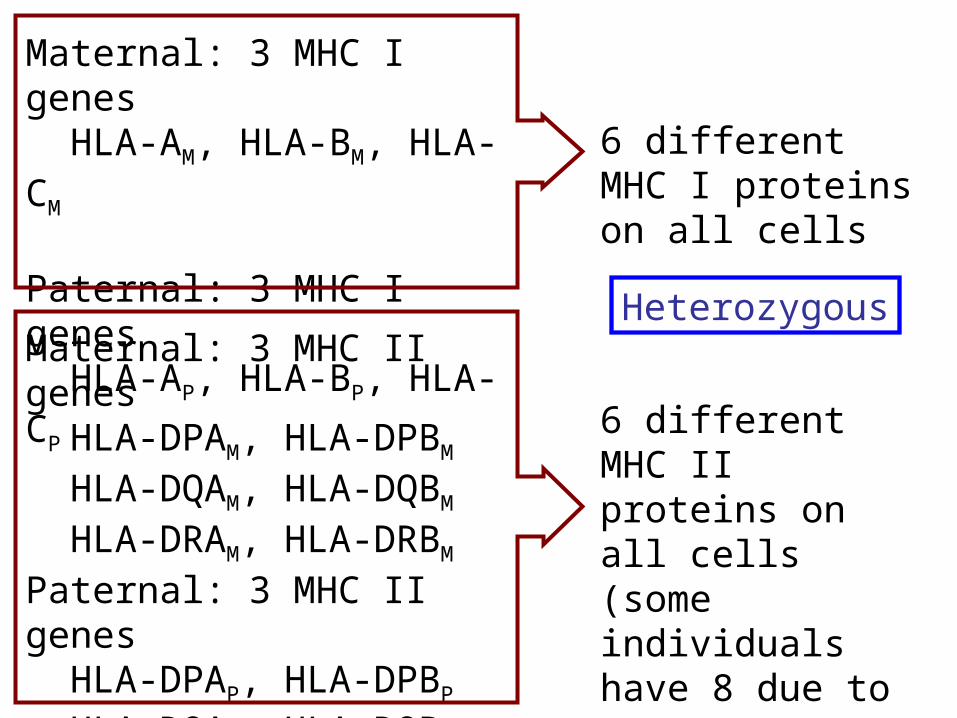
Maternal: 3 MHC I genes HLA-AM, HLA-BM, HLA-CM
Paternal: 3 MHC I genes HLA-AP, HLA-BP, HLA-CP
Maternal: 3 MHC II genes HLA-DPAM, HLA-DPBM
HLA-DQAM, HLA-DQBM
HLA-DRAM, HLA-DRBM
Paternal: 3 MHC II genes HLA-DPAP, HLA-DPBP
HLA-DQAP, HLA-DQBP
HLA-DRAP, HLA-DRBP
6 different MHC I proteins on all cells
6 different MHC II proteins on all cells(some individuals have 8 due to two HLA-DRB genes)
Heterozygous
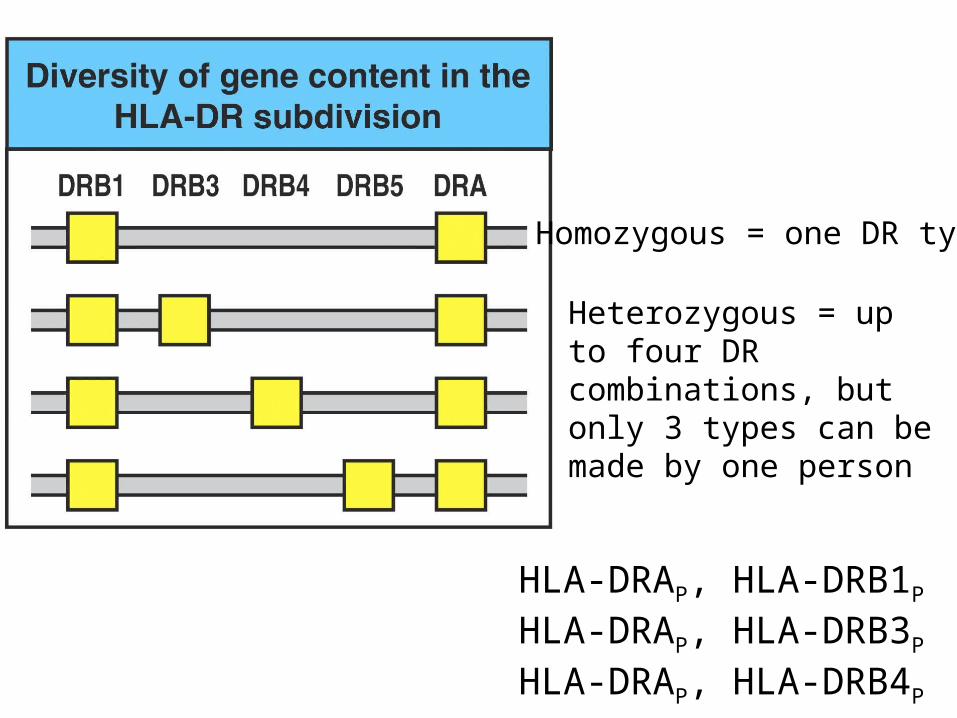
Homozygous = one DR type
Heterozygous = up to four DR combinations, but only 3 types can be made by one person
HLA-DRAP, HLA-DRB1P
HLA-DRAP, HLA-DRB3P
HLA-DRAP, HLA-DRB4P
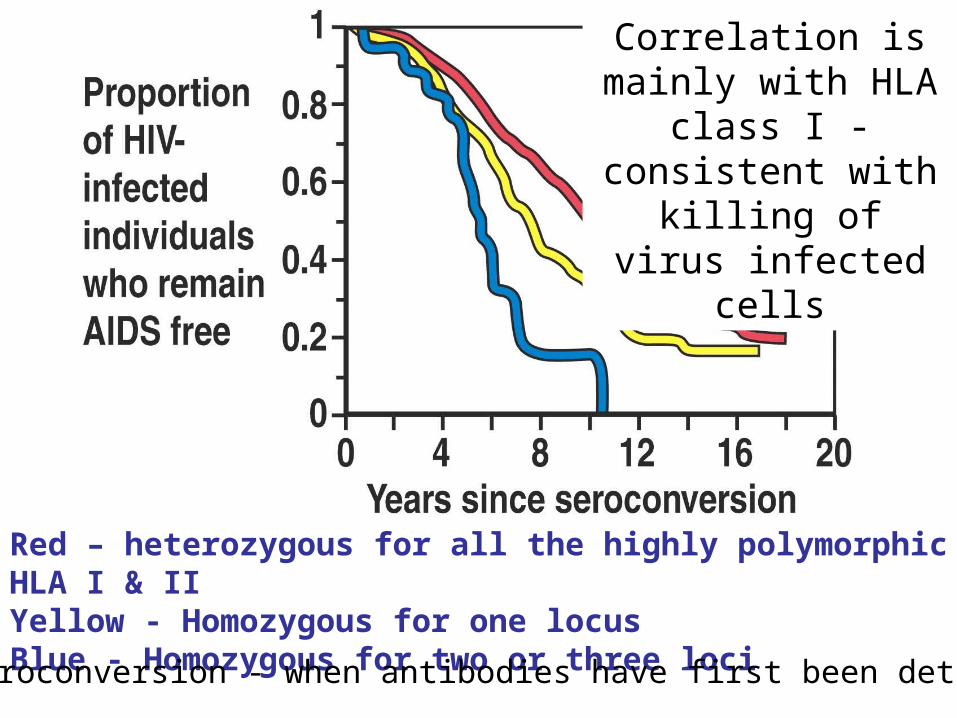
Figure 3-34
Red – heterozygous for all the highly polymorphic HLA I & IIYellow - Homozygous for one locusBlue - Homozygous for two or three loci
Correlation is mainly with HLA class I -
consistent with killing of virus infected cells
Seroconversion - when antibodies have first been detected
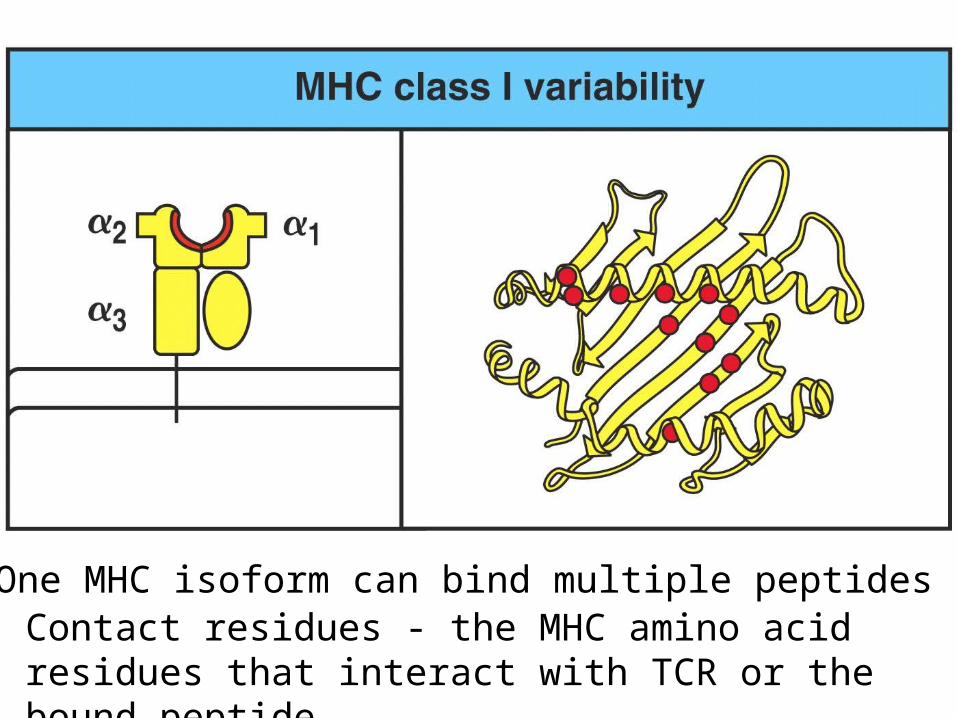
Figure 3-28 part 1 of 2
MHC
One MHC isoform can bind multiple peptidesContact residues - the MHC amino acid residues that interact with TCR or the bound peptide
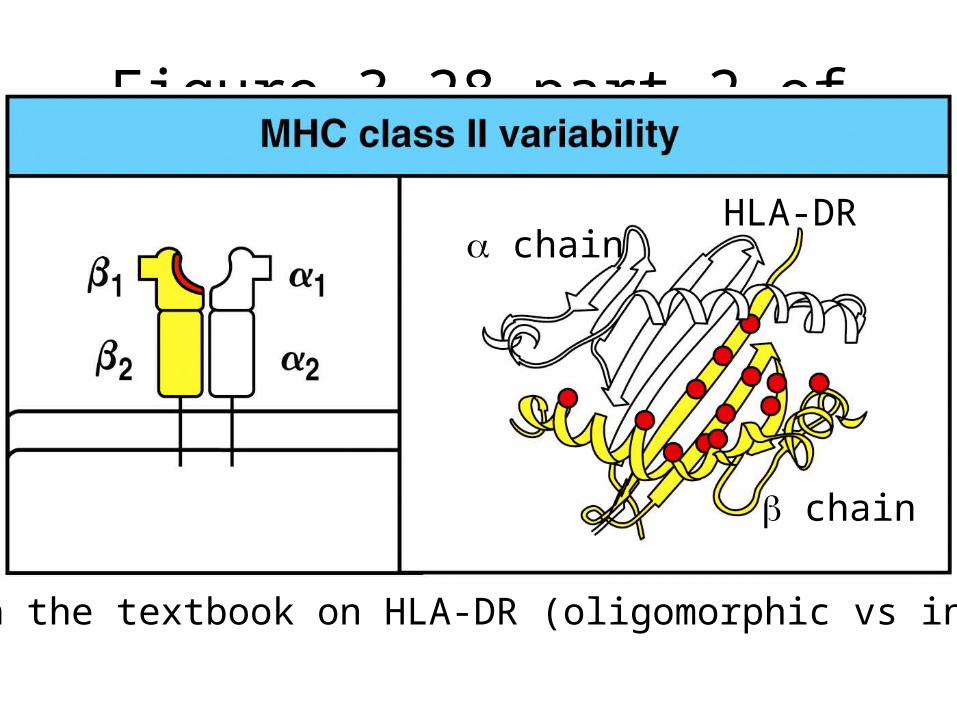
Figure 3-28 part 2 of 2
Error in the textbook on HLA-DR (oligomorphic vs invariant)
chain
chain
HLA-DR
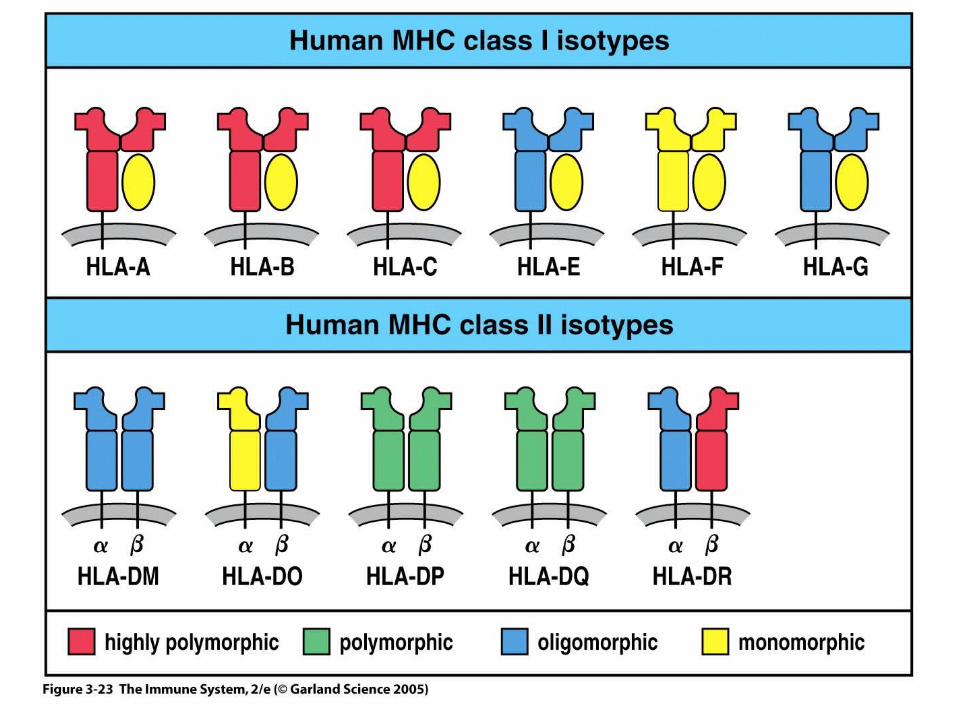
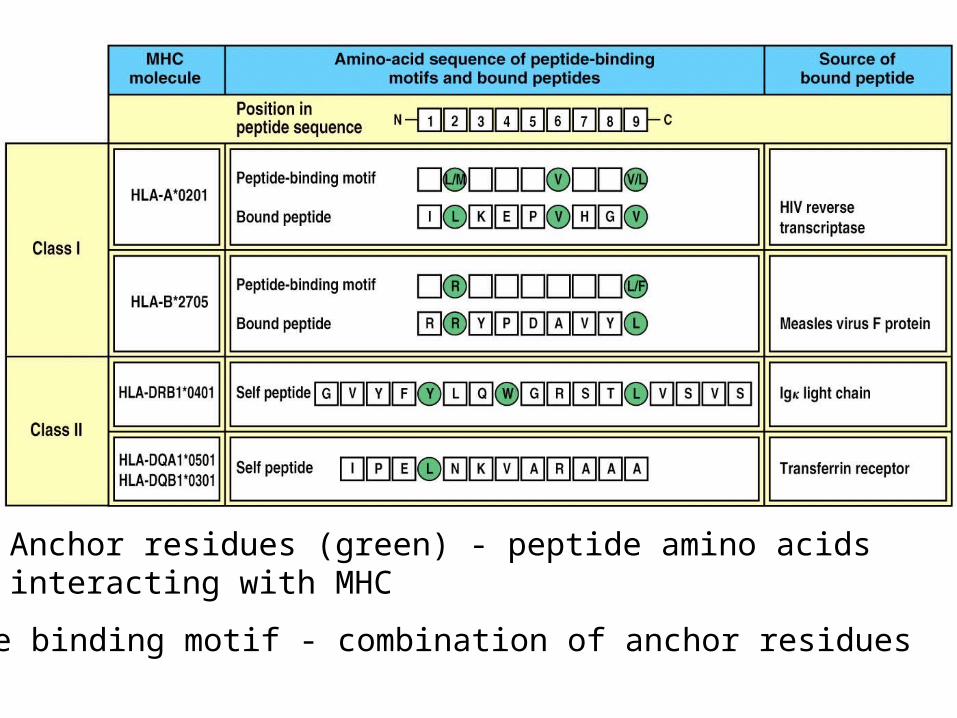
Figure 3-29
Peptide binding motif - combination of anchor residues
Anchor residues (green) - peptide amino acids interacting with MHC
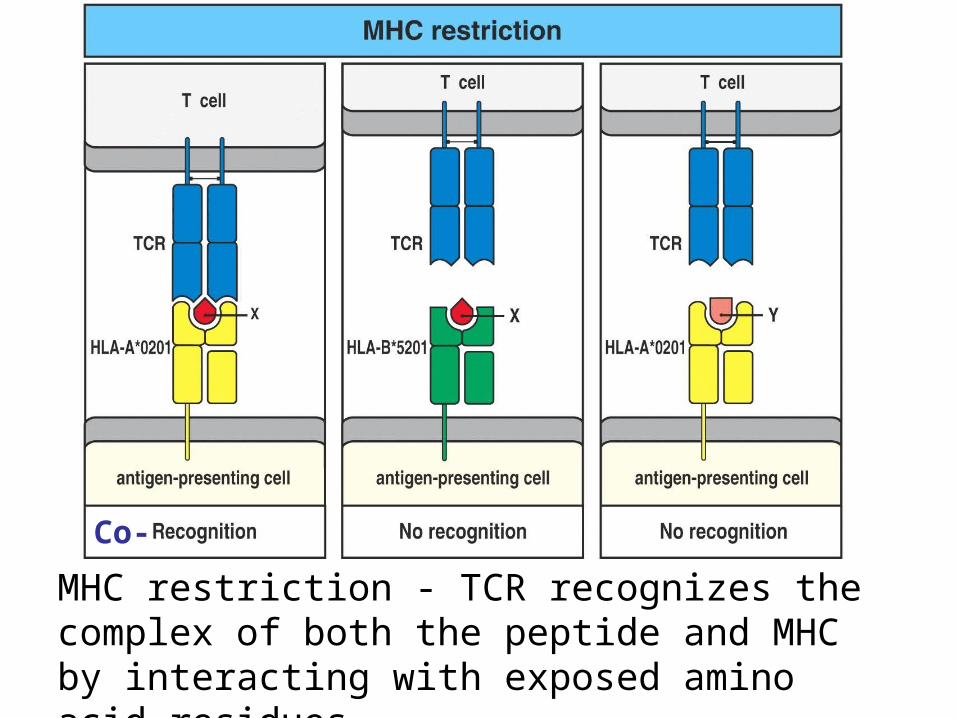
Figure 3-30
Co-
MHC restriction - TCR recognizes the complex of both the peptide and MHC by interacting with exposed amino acid residues
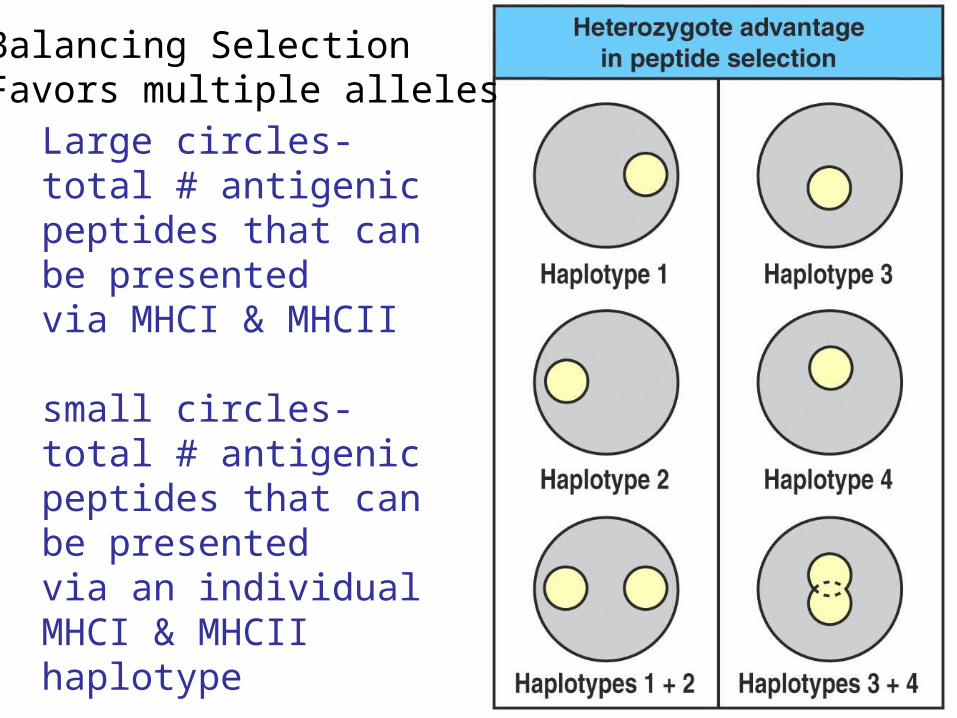
Figure 3-31Large circles- total # antigenicpeptides that can be presentedvia MHCI & MHCII
small circles- total # antigenicpeptides that can be presentedvia an individual MHCI & MHCII haplotype
Balancing SelectionFavors multiple alleles
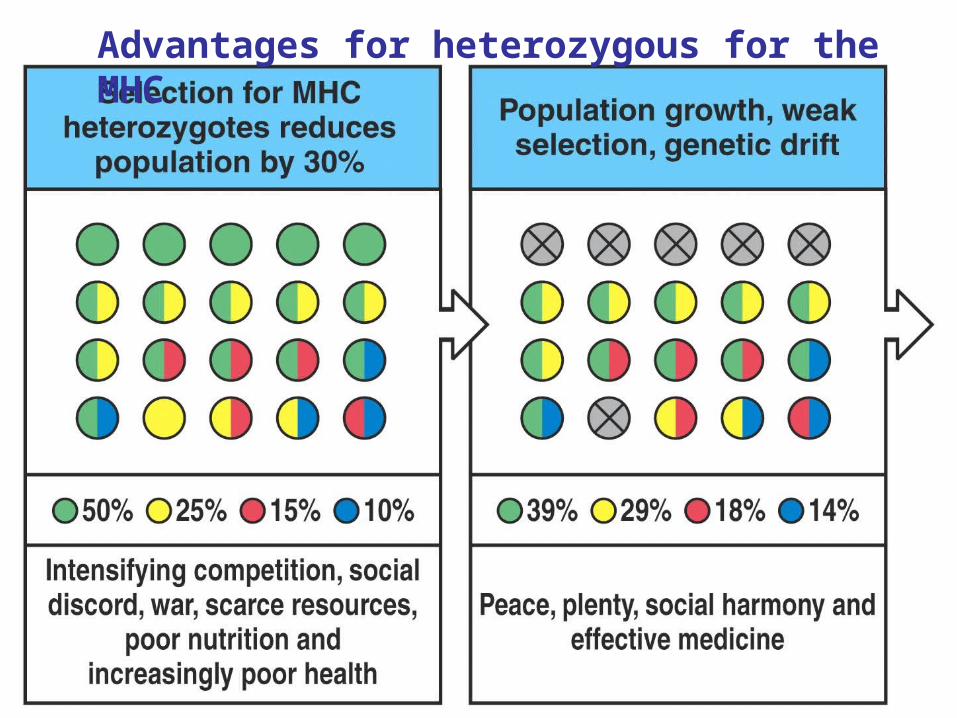
Figure 3-32 part 1 of 2
Advantages for heterozygous for the MHC
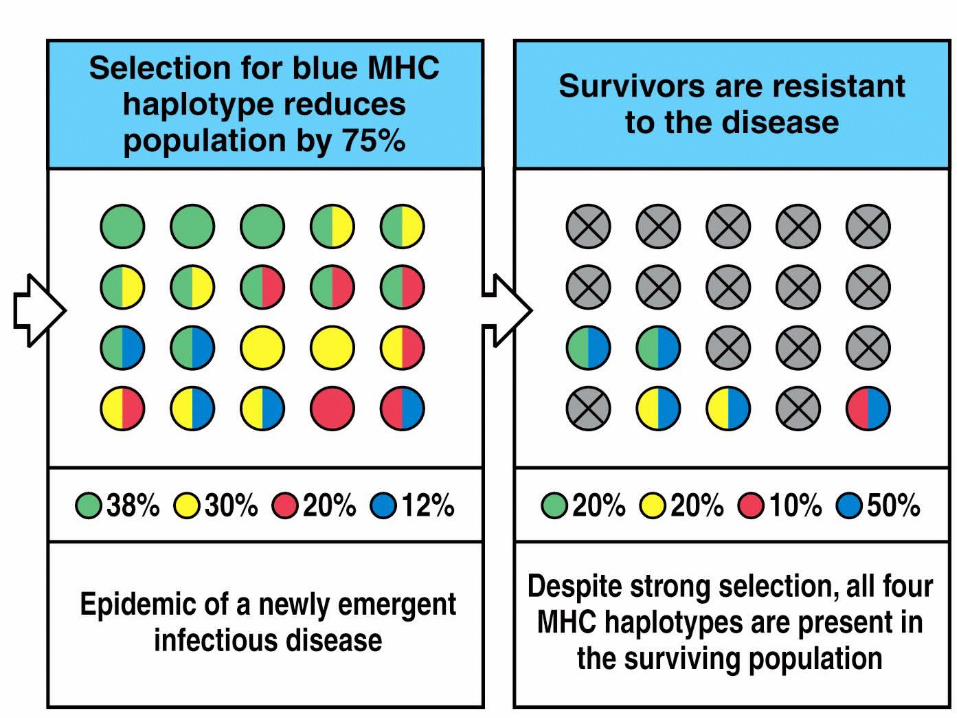
Figure 3-32 part 2 of 2
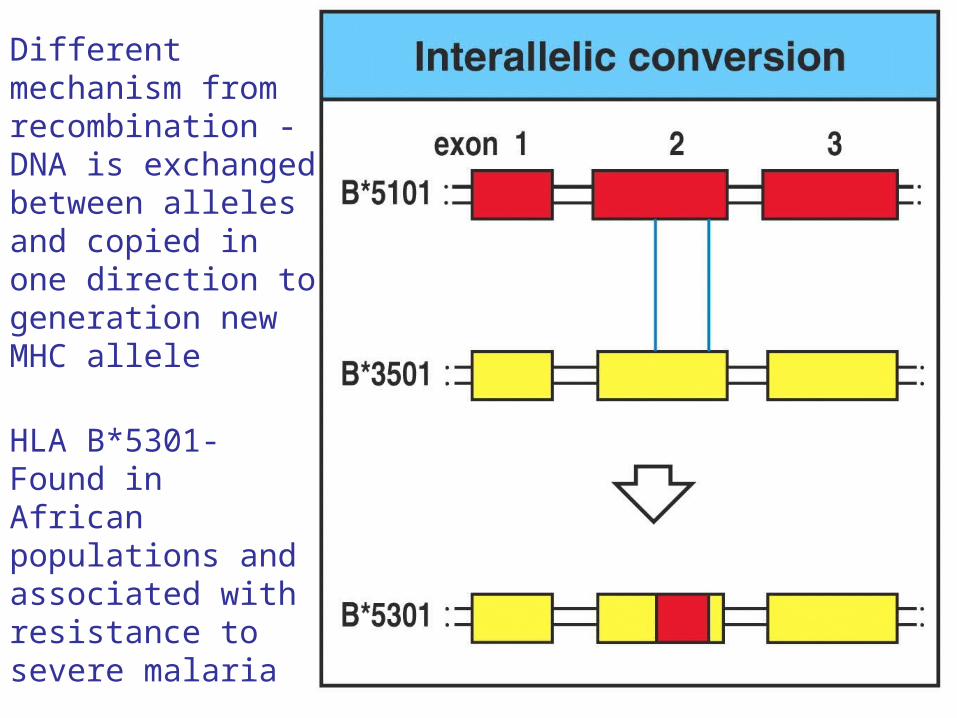
Different mechanism from recombination - DNA is exchanged between alleles and copied in one direction to generation new MHC allele
HLA B*5301-Found in African populations and associated with resistance to severe malaria

Figure 3-33 part 2 of 2
HLA B*4601- Found in southeast Asian populations andassociated with susceptibility to nasopharyngeal carcinoma.
Recombination betweenalleles of a differentgene
Generation of newMHC alleles
MHC selection by Infectious Disease
• Pathogens adapt to avoid MHC - recent MHC isoform may provide a survival advantage (hence higher frequency level)
• Epidemic diseases place survival advantages on those who can best present pathogenic peptides
• Only a minority of HLA alleles are common to all humans- most are recent and specific to ethnic groups
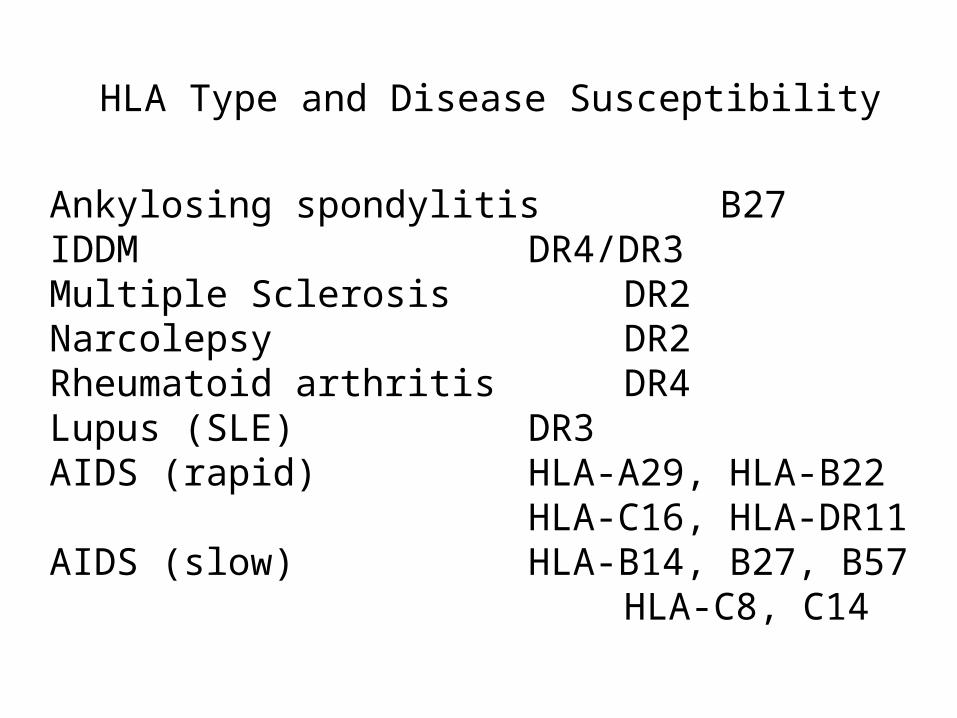
HLA Type and Disease Susceptibility
Ankylosing spondylitis B27IDDM DR4/DR3Multiple Sclerosis DR2Narcolepsy DR2Rheumatoid arthritis DR4Lupus (SLE) DR3AIDS (rapid) HLA-A29, HLA-B22
HLA-C16, HLA-DR11AIDS (slow) HLA-B14, B27, B57
HLA-C8, C14
MHC polymorphism and Organ Transplants
• Developing T cells that recognize complexes of peptide and MHC molecules on HEALTHY tissue (self-peptides presented by self MHC) are DESTROYED
• This results in the preservation of T cells that recognize non-self MHC (allogeneic MHC). These are alloreactive T cells and are 1-10% of total T-cell repertoire
• Immune system is primed for rejection of foreign organs that express allogeneic MHC
• THIS IS WHY YOU WANT TO MATCH HLA TYPE
![Circulating and Tumor-Infiltrating Foxp3 Regulatory T Cell ... · traditional Th1, Th2 helper T cell subsets, Foxp3+ reg-ulatory T cell (Tregs) and IL-17-producing Th17 cells[9].](https://static.fdocuments.in/doc/165x107/5e4b79c0f61ac961cb5bf5de/circulating-and-tumor-infiltrating-foxp3-regulatory-t-cell-traditional-th1.jpg)