Cellular and HumoralImmune Responses to Herpes Simplex ... · Atotal of 17 children, aged 1 to 15...
7
Vol. 22, No. 2 INFECTION AND IMMUNITY, Nov. 1978, p. 445-457 0019-9567/78/0022-0445$02.00/0 Copyright © 1978 American Society for Microbiology Printed in U.S.A. Cellular and Humoral Immune Responses to Herpes Simplex Virus During and After Primary Gingivostomatitis ANNE M0LLER-LARSEN,' * SVEN HAAHR,' AND FINN T. BLACK2 Institute of Medical Microbiology, University of Aarhus,' and Department of Medical Epidemiology, Marselisborg Hospital,2 DK-8000 Aarhus C, Denmark Received for publication 6 September 1978 A total of 17 children, aged 1 to 15 years, with gingivostomatitis were investi- gated to follow the development of immune parameters in those who suffered from herpes simplex virus stomatitis. Mouth swabs were obtained during the acute attack. Blood samples were collected on this occasion and again about 3 weeks later. Humoral immunity to herpes simplex virus was investigated by a complement fixation test and by an antibody-dependent cell-mediated cytotox- icity test. Cell-mediated immunity was investigated in a blast transformation assay with herpes simplex virus type 1 antigen and phytohemagglutinin. Inter- feron production in herpes-stimulated cultures was measured. Thirteen patients had a herpes simplex stomatitis. Twelve of these children were negative in the complement fixation test on the first serum specimen, but only five were negative in the antibody-dependent cell-mediated cytotoxicity test. These five were still febrile at the time of investigation. Blast transformation was negative at the first investigation in most children, whereas interferon was produced both in leukocyte cultures obtained during the infection and also in cultures made 3 to 4 weeks after the infection. An increase in immune parameters was seen in all patients with herpes stomatitis. From results in blast transformation and antibody-de- pendent cell-mediated cytotoxicity, it is seen that cell-mediated and humoral immunity can be found at the same time during recovery from this type of infection. Most individuals are infected with herpes sim- plex virus type 1 (HSV-1) during the first few years of life, with the greatest frequency of the infection between the ages of 1 and 3 years. Most of the infections are subclinical, conveying im- munity to the infected individual and implying latent infection with the risk of later develop- ment of recurrent herpes eruptions. About 15% of the primary infections appear as an acute herpetic gingivostomatitis (7), which is the most common form of a symptomatic manifestation of the primary infection with HSV-1. The role of humoral and cell-mediated immunity in the recovery from the primary infection and in con- trolling recrudescence of subsequent latent in- fection is still a matter of debate. In the present study we investigated the de- velopment of humoral and cell-mediated im- mune parameters in relation to the acute pri- mary attack of gingivostomatitis. Virus isola- tions were performed to ensure the diagnosis. Humoral immunity was measured by a comple- ment fixation (CF) test and by an antibody- dependent cell-mediated cytotoxicity (ADCC) test. Cell-mediated immunity was measured by blast transformation assays with specific antigen or phytohemagglutinin (PHA) and by measuring interferon production in HSV-1-stimulated lym- phocyte cultures. The clinical response was com- pared with the immune parameters. MATERIALS AND METHODS Blood samples. Seventeen otherwise healthy chil- dren, nine girls and eight boys, aged 1 to 15 years, attending the outpatients clinic of Marselisborg Hos- pital, Aarhus, Denmark, with an acute primary attack of gingivostomatitis were examined. Samples of 5 to 10 ml of heparinized blood (20 IU of heparin per ml) and 5 to 10 ml of clotted blood were obtained during the acute attack and 3 to 4 weeks later. The clinical condition was recorded on both occasions. Oral specimens. Two mouth swabs were obtained from each individual. One was placed in 2 ml of RPMI- 1640 medium for transportation and within 2 h was investigated for the content of herpes virus by inoc- ulation on human embryonic lung fibroblast (HEL) monolayers. The other was placed in Stuart transport medium and investigated for the content of Candida albicans. Mouth swabs were obtained only during the acute attack. CF test. All sera were inactivated and tested for antibodies to HSV by the CF test. CF antigen was prepared from HEL cells, infected as described below for antigen used in blast transformation, and otherwise 445 on July 21, 2020 by guest http://iai.asm.org/ Downloaded from
Transcript of Cellular and HumoralImmune Responses to Herpes Simplex ... · Atotal of 17 children, aged 1 to 15...

Vol. 22, No. 2INFECTION AND IMMUNITY, Nov. 1978, p. 445-4570019-9567/78/0022-0445$02.00/0Copyright © 1978 American Society for Microbiology Printed in U.S.A.
Cellular and Humoral Immune Responses to Herpes SimplexVirus During and After Primary Gingivostomatitis
ANNE M0LLER-LARSEN,' * SVEN HAAHR,' AND FINN T. BLACK2
Institute ofMedical Microbiology, University ofAarhus,' and Department ofMedical Epidemiology,Marselisborg Hospital,2 DK-8000 Aarhus C, Denmark
Received for publication 6 September 1978
A total of 17 children, aged 1 to 15 years, with gingivostomatitis were investi-gated to follow the development of immune parameters in those who sufferedfrom herpes simplex virus stomatitis. Mouth swabs were obtained during theacute attack. Blood samples were collected on this occasion and again about 3weeks later. Humoral immunity to herpes simplex virus was investigated by a
complement fixation test and by an antibody-dependent cell-mediated cytotox-icity test. Cell-mediated immunity was investigated in a blast transformationassay with herpes simplex virus type 1 antigen and phytohemagglutinin. Inter-feron production in herpes-stimulated cultures was measured. Thirteen patientshad a herpes simplex stomatitis. Twelve of these children were negative in thecomplement fixation test on the first serum specimen, but only five were negativein the antibody-dependent cell-mediated cytotoxicity test. These five were stillfebrile at the time of investigation. Blast transformation was negative at the firstinvestigation in most children, whereas interferon was produced both in leukocytecultures obtained during the infection and also in cultures made 3 to 4 weeksafter the infection. An increase in immune parameters was seen in all patientswith herpes stomatitis. From results in blast transformation and antibody-de-pendent cell-mediated cytotoxicity, it is seen that cell-mediated and humoralimmunity can be found at the same time during recovery from this type ofinfection.
Most individuals are infected with herpes sim-plex virus type 1 (HSV-1) during the first fewyears of life, with the greatest frequency of theinfection between the ages of 1 and 3 years. Mostof the infections are subclinical, conveying im-munity to the infected individual and implyinglatent infection with the risk of later develop-ment of recurrent herpes eruptions. About 15%of the primary infections appear as an acuteherpetic gingivostomatitis (7), which is the mostcommon form of a symptomatic manifestationof the primary infection with HSV-1. The roleof humoral and cell-mediated immunity in therecovery from the primary infection and in con-trolling recrudescence of subsequent latent in-fection is still a matter of debate.
In the present study we investigated the de-velopment of humoral and cell-mediated im-mune parameters in relation to the acute pri-mary attack of gingivostomatitis. Virus isola-tions were performed to ensure the diagnosis.Humoral immunity was measured by a comple-ment fixation (CF) test and by an antibody-dependent cell-mediated cytotoxicity (ADCC)test. Cell-mediated immunity was measured byblast transformation assays with specific antigen
or phytohemagglutinin (PHA) and by measuringinterferon production in HSV-1-stimulated lym-phocyte cultures. The clinical response was com-pared with the immune parameters.
MATERIALS AND METHODSBlood samples. Seventeen otherwise healthy chil-
dren, nine girls and eight boys, aged 1 to 15 years,attending the outpatients clinic of Marselisborg Hos-pital, Aarhus, Denmark, with an acute primary attackof gingivostomatitis were examined. Samples of 5 to10 ml of heparinized blood (20 IU of heparin per ml)and 5 to 10 ml of clotted blood were obtained duringthe acute attack and 3 to 4 weeks later. The clinicalcondition was recorded on both occasions.
Oral specimens. Two mouth swabs were obtainedfrom each individual. One was placed in 2 ml of RPMI-1640 medium for transportation and within 2 h wasinvestigated for the content of herpes virus by inoc-ulation on human embryonic lung fibroblast (HEL)monolayers. The other was placed in Stuart transportmedium and investigated for the content of Candidaalbicans. Mouth swabs were obtained only during theacute attack.CF test. All sera were inactivated and tested for
antibodies to HSV by the CF test. CF antigen wasprepared from HEL cells, infected as described belowfor antigen used in blast transformation, and otherwise
445
on July 21, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

446 M0LLER-LARSEN, HAAHR, AND BLACK
treated as described by Andersen (2).Target cells for cytotoxicity assays. Skin fibro-
blasts from healthy human adults obtained as de-scribed by Therkelsen (27) were grown in monolayersin 250-ml Falcon bottles. Two days after being pas-saged, the cells were infected with HSV-1 strainMaclntyre (1 plaque-forming unit per cell in 5 ml ofmedium). After 24 h, when about one third of the cellsshowed a well-developed cytopathic effect, they weretrypsinized, washed and suspended in Parker mediumTC-199 with 5% heat-inactivated fetal calf serum. Un-infected fibroblasts were treated similarly and used ascontrol cells.Lymphocytes for cytotoxicity assays. As de-
scribed in previous papers on ADCC (10, 11), buffycoat lymphocytes from unknown donors were used aseffector cells. Before use the lymphocytes were washedseven times in TC-199 with 5% fetal calf serum. Thetotal amount of lymphocytes obtained from one buffycoat is usually 2 x 108 to 6 x 108.ADCC assay. The test was performed in conical
plastic tubes (Nunc plastic, 11 by 70 mm). To 1 ml oflymphocyte suspension, i.e., 106 cells, was added 60 plof serum or serum dilution. Target cells labeled with5"Cr by standard methods were added in 0.1-ml vol-umes from a cell suspension containing 105 cells perml (effector-target ratio, 100:1). Total activity andspontaneous release were determined from tubes con-taining 1 ml of medium instead of lymphocyte suspen-sion.The tubes were incubated in humidified air with 5%
CO2 at 37°C for 16 to 18 h. After incubation the tubeswere capped, agitated thoroughly, and centrifuged at200 x g for 10 min. A 0.7-ml amount of supernatantwas withdrawn for the determination of 5'Cr release.
Test tubes with infected target cells were run induplicate, whereas control tubes were mostly single,because control counts usually were at the same level.The percentage of 5"Cr release was calculated by
the following formula: [(A - B) x 100]/(C - B), whereA = release from target, serum and lymphocytes; B =spontaneous release; and C = total activity in 0.7 mlof target cell suspension.The percentage of 51Cr release from infected target
minus the percentage of 51Cr release from controltarget gives the percentage of specific 51Cr release. Thevalues given in figures and tables are percentages ofspecific 5"Cr release.
Preparation of antigen for blast transforma-tion. HEL cells grown in Eagle minimal essentialmedium with 2% calf serum were infected by HSV-1strain MacIntyre (2 to 3 plaque-forming units/cell). Atthe time of maximum cytopathic effect (24 to 48 hafter infection), the culture was frozen and thawedtwice and centrifuged at 1,000 x g for 10 min to spindown cellular debris. The supernatant containing 7 x107 to 9 x 107 plaque-forming units/ml was inactivatedby UV light for 5 min at a distance of 15 cm. Afterinactivation the virus titer was 0. Control antigen wasprepared from uninfected HEL cells treated like theinfected cells. Antigens were stored in small aliquotsat -700C.
Preparation of leukocytes for blast transfor-mation. Mononuclear cells, obtained from heparin-ized peripheral venous blood after Ficoll-Isopaque flo-tation (5), were washed twice in RPMI-1640 medium
INFECT. IMMUN.
containing 2% heat-inactivated human HSV-negativeserum, HEPES buffer (N-2-hydroxyethyl piperazine-N'-2-ethanesulfonic acid), penicillin, streptomycinand, for the first wash, 15 to 20 IU of heparin per ml.After washing, the cells were resuspended in RPMI-1640 with buffer and antibiotics like the wash fluid,but with 15% of the human serum. After counting, thecell suspension was adjusted to contain 106 cells perml and dispensed in 0.2-ml portions in the wells of amicroplate (Linbro no. IS-MRC-96). To the cultureswas added 30 or 10 p1 of undiluted antigen (HSV-1 orcontrol antigen) or 10 ul of the dilutions 1:4, 1:16, and1:64. PHA was added in 10-,Il portions from solutionscontaining 1.0 or 0.1 .tg/ml. All stimulations were madein triplicate. The plates were closed with plastic cov-ers, and antigen-stimulated cultures and unstimulatedcultures were incubated in 5% CO2 at 37°C for a totalof 6 days. PHA-stimulated cultures were incubated fora total of 3 days.Thymidine incorporation. For the final 18 h of
incubation, 1 pl of a [2-'4C]thymidine solution (0.02tLCi/ml) was added to each well. The cells were har-vested on glass fiber paper (Whatman CF 81) with aSkatron harvester type POB 8. The paper disks wereplaced in plastic vials with 2 ml of Triton-Toluolscintillation fluid and counted in a Packard Tri-Carbliquid scintillation spectrometer. Counts per minutewere converted to disintegrations per minute. Theresults are given as herpes-stimulated cultures - con-trol-stimulated cultures = incremental counts, and asherpes-stimulated cultures/control-stimulated cul-tures = stimulation index (SI). Results from PHA-stimulated cultures and unstimulated cultures aregiven as disintegrations per minute.
Interferon assay. The supematant from herpesantigen-stimulated lymphocytes (10 pl of antigen per2 x 105 cells in 0.2 ml) was harvested after incubationfor 6 days and centrifuged at 3,000 x g for 10 min. Theassay was done by a micromethod by which MicroTest II (Falcon) wells were seeded with 2.5 x 104human embryonic skin fibroblasts in a 0.1-ml volume,with Eagle minimum essential medium with 10% calfserum. After growth to confluence, 0.05 ml of thesupernatant to be tested was added to wells in the firstrow. Further threefold dilutions were made directly inthe wells with an automatic microdiluter equippedwith 0.05-ml diluting loops. All samples were tested induplicate rows (6). An interferon standard of knowntiter was included on each plate. The cells were chal-lenged with vesicular stomatitis virus after 18 h, andcytopathic effect was read microscopically after incu-bation for 24 h. The interferon titer is the dilution thatreduces vesicular stomatitis virus cytopathic effect by50%.
Characterization of interferons. Interferonswere characterized as type I (classical) or type II(immune) interferons by the description by Valle etal. (28), i.e., influence of exposure to 56-C for 1 h,influence of exposure to pH 2 for 24 h, and neutrali-zation with anti-human leukocyte interferon sera.
RESULTSIsolation of HSV and C. albicans from
oral swabs. Herpesvirus was found in 13 of the17 patients and C. albicans in two patients from
on July 21, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

IMMUNITY DURING AND AFTER GINGIVOSTOMATITIS 447
whom no virus could be grown. In two patientsneither of the two agents was found. The causeof their stomatitis was not further investigated.CF test. As seen from Table 1, only one in
the group of patients from whom herpesviwuscould be grown showed a positive CF titer in thefirst serum specimen. All patients with herpes-virus in oral specimens showed a positive CFtiter in the second serum specimen, and a slight,but not significant, increase in titer was seen in
TABLE 1. Isolation experiments on oral specimens,taken during the acute attack of stomatitis
HSV C. albi- CF titeraPatient Age Sex oral cans inno. (Yr) swabs oral Serum Serum
swabs I II
1 4 Female + - <4 642 1½/2 Male + - <4 643 2 Female + - <4 2564 3 Male + - <4 325 1½ Male + - <4 326 1 Male + - <4 327 6 Female + - <4 648 3 Male + - <4 329 8 Female + - <4 3210 1 Male + - 16 3211 11 Female + - <4 3212 11 Male + - ND ND13 2 Female + (+) b <4 3214 1 Male - + <4 <415 10 Female - + <4 ND16 9 Female - - 32 3217 15 Female - - 32 NDa CF titers were made from serum specimens taken
during the acute attack (serum I) and 3 to 4 weekslater (serum II). ND, Not done.
b A small amount of C. albicans.
the patient with positive titer in the first speci-men. Neither of the two patients with C. albi-cans infection was herpes positive. Both patientswith totally negative findings in oral specimenswere herpes positive in the CF test.ADCC. Previous ADCC assays have shown
that ADCC is a very sensitive serological test(10, 11, 22, 26). Results of the ADCC assay
(Table 2) in this study indicate that antibodiescan be found in serum in many patients after a
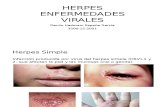
few days of illness if the serological test used fordetection is sensitive enough. In our series, 7 outof 11 patients with primary herpetic gingivosto-matitis were investigated during days 4 to 8 ofillness. Six of those seven patients showed"ADCC antibodies" in serum (Table 2 and Fig.1). The four patients investigated on days 2 and3 did not show ADCC antibodies in the serum.
Both groups showed an increase in the amountof antibodies in serum from the first to thesecond investigation. This is best seen in theserum dilution 1:102 (Table 2).Blast transformation. All patients with her-
pesvirus in the oral specimen showed an increasein blast transfornation from the first to thesecond investigation, both in SI and in incre-mental counts (Table 3). Two patients showeda positive SI already in the first specimen (SI2 2). One of these was positive in the CF test(patient 10). The other one was not investigateduntil 8 days after the beginning of the illness(patient 11).The two patients (16 and 17) with negative
oral specimens, but with positive CF tests, wereboth stimulated by the HSV antigen in the firstspecimen (SI > 2), and also incremental counts
TABLE 2. Duration of illness, fever on the day of examination or on previous days, and percentages ofkilling of HSV-1-infected fibroblasts in an ADCC system using the same effector lymphocytes (buffy coat) for
paired sera a
Duration of Percentage of specific 51Cr release
ulness before Fever at first examination (°C)Patient no. first specimen Serum I Serum II
(days) Previous days Present Undiluted 1:102 Undiluted 1:102
1 3 39.5 38.5 3.2 -3.2 22.4 11.72 1½ 39.0 39.0 2.2 1.9 27.5 21.13 2 39.8 39.7 1.5 -2.2 38.2 37.14 2 39.0 39.0 4.2 2.7 33.9 25.65 4 38.0 38.0 0.8 2.5 37.6 34.86 4 38.0 No fever 28.3 4.6 26.6 15.27 6 38.2 No fever 23.8 1.5 25.7 16.88 5 38.8 No fever 45.5 20.9 59.2 58.89 4 39.6 No fever 20.6 4.9 19.9 11.510 6 39.0 No fever 25.9 5.4 35.9 11.511 8 38.5 No fever 33.3 14.5 38.9 24.912 NK NK No fever 24.0 6.4 27.9 19.013 NK NK NK 21.7 10.6 25.4 17.1
a Serum I was taken during the acute attack and serum II was taken 3 to 4 weeks later. All results are frompatients with HSV in oral specimens.
b NK, Not known.
VOL. 22, 1978
on July 21, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

448 MOLLER-LARSEN, HAAHR, AND BLACK
60
50
40L
x
30-0
20-U-
0
10
0
- 39OU
-38 WL-3
CL
37
1 2 3 4 5 6 7DAYS OF DISEASE
FIG. 1. Comparison of the duration of illness before the first investigation, temperature on the day of thefirst investigation, and percentages of specific cytotoxicity in ADCC with serum collected on this occasion.
TABLE 3. Effect of infection on blast transformation and interferon production in lymphocytes obtainedduring the acute attack and 3 to 4 weeks later
HSV cultures (dpm) Si PHA cultures (dpm) Unstimulated lym- Interferon titerPatient Incremental counts phocytes (dpm)no.
I a II'a I II I II I II I II1 1 4,747 1.0 7.6 1,313 5,534 22 440 2,100 2,1002 141 1,283 1.6 6.7 15,181 15,130 186 289 81 2403 -5 1,619 0.9 3.4 16,129 13,073 40 259 240 7204 -44 4,534 1.0 38.5 3,042 6,935 670 126 NDb ND5 -237 4,281 0.4 10.4 10,905 14,557 356 476 ND ND6 -5 818 0.9 1.3 935 6,065 42 1,855 720 2,1007 211 4,348 1.4 5.9 10,060 10,998 398 ND ND ND8 1 96 1.0 1.5 12,643 8,743 45 375 81 2409 12 2,828 1.1 14.6 9,791 8,725 183 292 240 72010 181 898 2.2 2.6 10,919 13,096 246 470 81 ND11 244 4,765 4.8 7.5 7,519 6,354 77 1,361 240 72012 14 2,473 1.4 41.5 6,244 2,587 51 80 ND ND13 29 4,769 1.2 3.2 2,673 10,208 39 1,692 2,100 2,10014 244 676 1.6 1.7 11,207 13,015 156 325 720 72015 -45 ND 0.6 ND 14,289 ND 196 ND ND ND16 1,878 1,653 4.4 3.5 8,715 10,186 987 592 720 2,10017 1,248 ND 3.8 ND 5,168 ND 1,057 ND 720 ND
a I, lymphocytes obtained during acute attack; II, those obtained 3 to 4 weeks later.'ND, Not done.
were higher for these than for the other patients. cytes could be stimulated. Results from PHAAs can be seen from the incremental counts cultures given in Table 3 are all obtained with
and, although at a lower level, from lymphocyte the higher of the two concentrations used. Re-counts without addition of antigen, the level of sults from HSV-stimulated cultures are from theincorporation of ['4C]thymidine markedly in- dilution giving the highest counts, which differedcreased from the first to the second specimen. from patient to patient.All patients were stimulated by PHA, which was Interferon production in HSV-stimulatedincluded as antigen to ensure that the lympho- cultures. All patients tested showed production
. TEMPERATURE* CYTOTOXICITY
hi
1
INFECT. IMMUN.
on July 21, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

IMMUNITY DURING AND AFTER GINGIVOSTOMATITIS 449
of interferon already in the first specimen, someof them even at a fairly high level. Most of thepatients showed an increase in production fromthe first to the second investigation. The restshowed interferon titers at the same level atboth investigations, whereas a decrease in pro-duction never was observed. The interferon pro-duced was characterized as type I, i.e., classicalinterferon.Fever. All patients from whom HSV was
isolated had a history of fever. On day 1 ofexamination, five patients, with no or only slightamounts of ADCC antibodies, were the onlyones who were febrile, whereas the other pa-tients who had fever on previous days but werenow afebrile all showed antibodies in their se-rum. Figure 1 shows temperature, cytotoxicity,and days of illness from 11 patients. A clearnegative correlation is found between fever andcytotoxicity (0.005 > P > 0.001). It is also note-worthy that all but one in the group of patientsstill being febrile (Tables 2 and 3) showed verylow incremental counts in the first specimen.
DISCUSSIONThe natural history and the clinical picture of
herpectic gingivostomatitis have been thor-oughly described by several investigators (3, 13,29). In the series presented here it was seen fromisolation experiments that 4 out of 17 patientsdid not have an acute infection with herpesvirus.Because the physicians referring the patients forfurther investigations have described the clinicalpicture in these four patients as different fromthat in the rest of the patients, it can be con-cluded that the diagnosis of herpetic gingivos-tomatitis is fairly easy and can be correctly madefrom the clinical picture only.
In recent years, when improved techniques formeasuring humoral and cell-mediated immunityhave become available, this group of patientshave not received much attention. In publica-tions mostly concerned with HSV-immune ornonimmune adults (21, 22) a few such patientshave been included, whereas several papers havebeen published on groups of patients sufferingfrom recurrent "cold sores" (6, 8, 19, 21, 25; L.Rasmussen and T. C. Merrigan, Proc. Natl.Acad. Sci. U.S.A., in press).HSV belongs to a group of viruses known to
produce severe and sometimes life-threateninginfections in patients with hematological malig-nancies (9,12) or patients in immunosuppression(15), both groups having defects in cell-mediatedimmunity, whereas the level of antibodies re-mains largely unchanged. In healthy individualswith recurrent cold sores, the level of CF anti-bodies also remains unchanged in connectionwith an attack. Compared with "normal" sero-
positive individuals without cold sores, theseindividuals have been found to have higher lev-els of neutralizing antibodies (8), but in spite ofthis they are not able to avoid recurrences.Because of these observations, most investi-
gators have focused attention on the role of thecell-mediated immune responses, usually bymeasuring blast transformation and interferonproduction. Alterations in these parameters inconnection with an acute attack of herpes labi-abs have been reported in several publications,with an increase of transformation in convales-cence compared with transformation during theattack (8, 21; Rasmussen and Merigan, in press).A decrease in interferon production has beenobserved in convalescence (16) in individualswith many attacks of herpes labialis. As men-tioned by Rasmussen and Merigan (in press), itis not known whether the transforming lympho-cytes (shown to be T lymphocytes in combina-tion with macrophages) have a direct effectorfunction in combating the infection or whetherthey are mostly limiting the extension of theeruptions. Rand et al. (15) found that amongpatients receiving a heart transplant those withlow transformation reactions to herpesviruseswere at a greater risk to suffer from a seriousinfection by these viruses than were patientswith higher transformation reactions. Whethera causal relationship exists between low blasttransformation and severe and prolonged her-pesvirus infections is not known. They mightboth be expressions of a common defect. A defectin ADCC perhaps based on decreased numbersof effector lymphocytes (K cells) might be ofimportance for the serious infections. Russelland Essery (20) found K cell activity largelywithin the normal range patients with Hodgkin'sdisease or malignant lymphoma and in a groupof patients receiving cytotoxic drugs or largedoses of prednisone, but none of the patients intheir series had a herpesvirus eruption wheninvestigated. In patients with malignant dis-eases, the ADCC reaction, if active in vivo, mightalso be blocked by circulating immune com-plexes (1, 31).
Patients with hypo- or agammaglobulinemiaare known to overcome some virus infectionswithout problems. Shore et al. (24) and Wisloffet al. (30) found that such patients had normaleffector cell function in ADCC. Because onlyvery small amounts of antibodies are necessaryin ADCC, this type of reaction might also beactive during viral infections in these patients.No final proof of ADCC activity in vivo has
been provided, but it seems most likely to occur(14). Furthermore, the reaction is found to beenhanced by complement (18) and to destroyvirus-infected cells very early in the infectious
VOL. 22, 1978
on July 21, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

450 M0LLER-LARSEN, HAAHR, AND BLACK
cycle (23), indicating it to be a very efficientdefense mechanism if active in vivo.The main purpose with the series presented
here was to investigate immunological mecha-nisms which might be at work in the recoveryfrom primary infection with herpesvirus. In ourseries, blast transformation was found to be neg-ative (SI < 2) in most patients with herpesinfection if investigated during the first week ofillness, whether being febrile or not, although atendency against lower SI was seen in patientswith fever on the day of examination. Comparedwith the group of patients with no fever, thistendency was increased when the results weregiven as incremental counts, although the differ-ence between the two groups was not significant(5% < P < 10%) when compared in a Mann-Whitney test. As our series is limited in size, itwould be of interest to investigate a possiblecorrelation between blast transformation andfever or no fever in a larger series.
Production of interferon was found in bothspecimens from all patients, in some at a higherlevel in the second specimen, in others at anunaltered level. Because type I interferon hasbeen found in herpes-stimulated cultures also inhealthy herpes-negative donors (6; Rasmussenand Merigan, in press), it is not possible to decidewhether interferon plays a role in the recoveryfrom this type of infection. Differences in inter-feron production have been demonstrated inpatients being immune and nonimmune to ru-bella virus (4). The unexpected demonstrationof interferon production in the first sample fromstomatitis patients may simply be related to anearly start of interferon production during theinfection. An explanation of interferon produc-tion in HSV-stimulated cultures from "serone-gative" adults might be that they will prove tobe seropositive if tested in ADCC (10, 11, 26).When ADCC was used as a serological assay
in our series, we found that several patients hadantibodies to HSV in serum already in the firstspecimen, at a time when all were negative whentested in a CF test. Particularly remarkable isthe observation that those with antibodies in thefirst serum specimen were afebrile on the day ofexamination, whereas fever had been present onprevious days. Those who were still febrile didnot have detectable antibodies in their serum.Although the series presented here is based
on a small group of patients, we think that it isrendered likely from incremental counts in blasttransformation and the results in ADCC thatcell-mediated and humoral immunity work inconcert in the recovery from viral infections.The findings of Rosenberg and Notkins (17) inexperiments on rabbits showing that cell-me-
diated immunity develops before humoral im-munity could not be confirmed in our study onhuman material when a sensitive assay is used.We find it important in future investigations
to pay attention to ADCC not only in the recov-ery from primary infections, but also in thecontrol of latent infections.
ACKNOWLEDGMENTS
We thank the general practitioners for referring patientsfor this study. We thank A. Stenderup for diagnosing C.albicans stomatitis, and we thank Aase Hvergel, Aase Rafn,and Margit Schjerven for excellent technical assistance.
This study was supported by a grant from Aarhus Univer-sitets Forskningsfond.
LITERATURE CITED1. Amlot, P. L., B. Pussell, J. M. Slaney, and B. D.
Williams. 1978. Correlation between immune com-plexes and prognostic factors in Hodgkin's disease. Clin.Exp. Immunol. 31:166-175.
2. Andersen, H. K. 1970. Complement fixing and virus-neutralizing antibodies in cytomegalovirus infection asmeasured against homologous and heterologous anti-gen. Acta Pathol. Microbiol. Scand. Sect. B 78:504-508.
3. Buddingh, J., D. I. Schrum, J. C. Lanier, and D. J.Guidry. 1953. Studies of the natural history of herpessimplex infections. Pediatrics 11:595-610.
4. Buimovici-Klein, E., K. E. Weiss, and L. Z. Cooper.1977. Interferon production in lymphocyte cultures afterrubella infection in humans. J. Infect. Dis. 135:380-385.
5. Boyum, A. 1968. Separation of leucocytes from blood andbone marrow. Scand. J. Clin. Lab. Invest. Suppl.97:31-50.
6. Haahr, S., L. Rasmussen, and T. C. Merigan. 1976.Lymphocyte transformation and interferon productionin human mononuclear cell microcultures for assay ofcellular immunity to herpes simplex virus. Infect. Im-mun. 14:47-54.
7. Kaplan, A. S. (ed.). 1973. The herpesviruses. AcademicPress Inc., New York.
8. Lopez, C., and R. J. O'Reilly. 1977. Cell mediated im-mune responses in recurrent herpesvirus infections. J.Immunol. 118:895-902.
9. Merigan, T. C., and D. A. Stevens. 1971. Viral infectionsin man associated with acquired immunological defi-ciency states. Fed. Proc. 30:1858-1864.
10. Moller-Larsen, A., I. Heron, and S. Haahr. 1977. Cell-mediated cytotoxicity to herpes-infected cells in hu-mans: dependence on antibodies. Infect. Immun.16:43-47.
11. Mo1ler-Larsen, A., and S. HIaahr. 1978. Humoral andcell-mediated immune responses in humans before andafter revaccination with vaccinia virus. Infect. Immun.19:34-39.
12. Muller, S. A., E. C. Herrmann, and R. K. Winkel-mann. 1972. Herpes simplex infections in hematologicmalignancies. Am. J. Med. 52:102-114.
13. Nahmias, A. J., and B. Roizmann. 1973. Infection withherpes simplex viruses 1 and 2. N. Engl. J. Med.289:781-789.
14. Rager-Zisman, B., and A. C. Allison. 1976. Mechanismsof immunologic resistance to herpes simplex virus 1(HSV-1) infection. J. Immunol. 116:35-40.
15. Rand, K. H., L. E. Rasmussen, R. B. Pollard, A.Arvin, and T. C. Merigan. 1976. Cellular immunityand herpesvirus infections in cardiac-transplant pa-tients. N. Engl. J. Med. 296:1372-1377.
16. Rasmussen, L. E., G. W. Jordan, D. A. Stevens, and
INFECT. IMMUN.
on July 21, 2020 by guesthttp://iai.asm
.org/D
ownloaded from

IMMUNITY DURING AND AFTER GINGIVOSTOMATITIS 451
T. C. Merigan. 1974. Lymphocyte interferon produc-tion and transformation after herpes simplex infectionsin humans. J. Immunol. 112:728-736.
17. Rosenberg, G. L, and A.L Notkins. 1974. Introductionof cellular immunity to herpes simplex virus. Relation-ship to the humoral immune response. J. Immunol.122:1019-1025.
18. Rouse, B. T., A. S. Grewal, and L A. Babiuk. 1977.Complement enhances antiviral antibody-dependentcell cytotoxicity. Nature (London) 266:456-458.
19. Russell, A. S. 1973. Cell-mediated immunity to herpessimplex virus in man. Am. J. Clin. Pathol. 60:828-830.
20. Russell, A. S., and G. Essery. 1977. Cellular immunityto herpes simplex virus in man. VII. K-cell activity toHSV 1 infected target cells in disease. Cancer 40:4245.
21. Shillitoe, E. J., J. M. A. Wilton, and T. Lehner. 1978.Sequential changes in T and B lymphocyte responsesto herpes simplex virus in man. Scand. J. Immunol.7:357-366.
22. Shore, S. L., C. M. Black, F. M. Melewieg, P. A. Wood,and A. J. Nahmias. 1976. Antibody-dependent cell-mediated cytotoxicity to target cells infected with type1 and type 2 herpes simplex virus. J. Iminunol.116:194-201.
23. Shore, S. L., T. L. Cromeans, and T. J. Romano. 1976.Immune destruction of virus-infected celis early in theinfectious cycle. Nature (London) 262:695-696.
24. Shore, S. L., F. M. Melewieg, and D. S. Gordon. 1977.The mononuclear cell in human blood which mediates
antibody-dependent cellular cytotoxicity to virus-in-fected target cells. J. Iminunol. 118:558-566.
25. Steele, R. W., M. M. Vincent, S. A. Hensen, D. A.Fuccillo, I. A. Chapa, and L Canales. 1975. Cellularimmune responses to herpes simplex virus type 1 inrecurrent herpes labialis: in vitro blastogenesis and cy-totoxicity to infected cell-lines. J. Infect. Dis.113:528-534.
26. Subramanian, T., and W. E. Rawls. 1977. Comparisonofantibody-dependent cellular cytotoxicity and comple-ment-dependent antibody lysis of herpes simplex virus-infected cells as methods of detecting antiviral antibod-ies in human sera. J. Clin. Microbiol. 5:551-558.
27. Therkelsen, A. J. 1964. "Sandwich" technique for theestablishment of human skin for chromosome investi-gation. Acta Pathol. Microbiol. Scand. 61:317.
28. Valle, M. J., G. W. Jordan, S. Haahr, and T. C.Merigan. 1975. Characterization of immune interferonproduced by human lymphocyte cultures compared toother human interferons. J. Immunol. 115:230-233.
29. von Wowern, N. 1971. Gingivostomatitis herpetica.Ugeskr. Laeg. 133:877-880.
30. Wisloff, F., and S. S. Froland. 1973. Antibody-depend-ent lymphocyte-mediated cytotoxicity in man. No re-quirement for lymphocytes with membrane bound im-munoglobulin. Scand. J. Immunol. 2:151-157.
31. Ziegler, H. K., and C. S. Henney. 1977. Studies on thecytotoxic activity of human lymphocytes. J. Immunol.119: 1010-1017.
VOL. 22, 1978
on July 21, 2020 by guesthttp://iai.asm
.org/D
ownloaded from