Herpes Zoster!
26
Oleh: Nurul Iska Ulmarika Idris C111 10 831 Ruth Faustine J. Rayo C111 10 180 Advisor: dr. Elfa Wirdani Fitri Supervisor: dr. Airin Mappewali, Sp. Kk, M.Kes HERPES ZOSTER
-
Upload
ruth-faustine-jontah-rayo -
Category
Documents
-
view
90 -
download
10
description
herpes zoster
Transcript of Herpes Zoster!
HERPES ZOSTER
Oleh:Nurul Iska Ulmarika IdrisC111 10 831Ruth Faustine J. RayoC111 10 180
Advisor:dr. Elfa Wirdani FitriSupervisor:dr. Airin Mappewali, Sp. Kk, M.Kes
HERPES ZOSTER
DEFINITIONHerpes zoster is an infectious disease by the varicella zoster virus that attacks the skin and mucosa, is a reactivation of the virus infection that occurs as a reactivation of the varicella zoster virus entering through periferal nerve during the initial episode of chickenpox, then settled in posterior spinal ganglion.
EPIDEMIOLOGYHerpes zoster occurs sporadically and not seasonally.The average age of patients with herpes zoster is 64 years, while the average age of the U.S. population is 46 years. The incidence of shingles ranged from 1.2 to 3.4 cases per 1,000 person-years in the study of immunocompetent individuals in society, but increased to 3.9 to 11.8 cases per 1,000 person-years among those > 65 years aged.RISK FACTORThe main risk factor is old age Immune dysfunction Female gender Physical trauma to the affected dermatome White race People with a family history of herpes zosterETIOLOGYVaricella and herpes zoster is caused by the same virus, called varicella-zoster virus (VZV)VZV contain icosahedral capsid shaped surrounded by a lipid envelope covering the virus genome, the genome which contains a linear molecule of double-stranded DNA. 150-200 nm in diameter and has a molecular weight of approximately 80 million.
PATHOGENESIS
CLINICAL MANIFESTATION
Fever, Dizzy, Malaise Muscle pain, Itchy, Soreness
Erythematous macules and papules Vesicle, with edema at the skin base crusts in the end.CLINICAL MANIFESTATION Unilateral, depend of the skin that innervated by a single sensory ganglion.Mostly; trunk from T3 L2, trigeminal nerve (ophtalmic division).Rarely; distal, to the elbows or kneesPain; 30 days following rash onset
CLINICAL MANIFESTATION
CLINICAL MANIFESTATION
12DIAGNOSEAnamnesis & Physical Examination; see the distributionHistophatology; intraepider- mal vesicle, acantholysisTzank Smears; multinucleate giant cell, with nuclear changesPCR; detect DNA of VZVELISA; enzyme linked immunosorbent assay
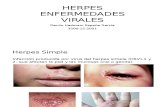
COMPLICATIONOphtalmic Zoster (1st Trigeminal Nerve); Neurothropic Keratitis, Chronic Ulceration2nd & 3rd Trigeminal Nerve; Ramsay-Hunt syndrome (facial palsy), Tinnitus, Vertigo, and DeafnessPain Herpetic Neuralgia (PHN); Neurons damage in the spinal cord and ganglion, to the peripheral nerve. Its persists after the rash has healed.COMPLICATIONCutaneousVisceralNeurologicBacterial SuperinfectionPneumonitisPHNScarring HepatitisMeningoencephalitisZoster GangrenosumEsophagitisTranverse MyelitisCutaneous DiseeminationGastritisPeripheral Nerve PalsiesPericarditisMotorCystitisAutonomicArthritisCranial Nerve PalsiesSensory LossDeafnessOcular ComplicationDIFFERENTIAL DIAGNOSISHerpes Simplex; Vesicle (with clear fluid &becoming seropurulen)with erythematous, andcrusts at the end. Patientalso complaining burning,itchy and pain feeling.Herpes simplex canattacking all parts of thebody.
DIFFERENTIAL DIAGNOSIS Contact Dermatitis; Erythema with vesicle, & edema skin base. Confirmation test:Patch Test
THERAPYPrincipal for HZ therapy is for (1) limit the extent, duration, and severity of pain and rash in the primary dermatome, (2) for prevent disease elsewhere, (3) prevent the PHN. Kind of treatment of HZ:Topical therapyAntiviral therapyAnti-inflammatory therapyAnalgesicsTreatment for PHNPrevention of HZTOPICAL THERAPYCool compressesCalamine lotionCornstarchBaking sodaFor help to alleviate local symptoms &hasten the drying of vesicular lesions, for acute phase of HZ.
ANTIVIRAL THERAPYPatient GroupRegimenNormal Age