An epilogue to plasma-cell gingivostomatitis (allergic ...
7
Reprinted from ORAL Su RGERY, ORAL ORAL PATHOLOGY, St. Louis Vol. 43, No . 2, Pages 211-217, February, 1977 (Printed In the U. S. A.) (Copyright €) 1977 by The C. V. 1\Iosby Company) An epilogue to plasma-cell gingivostomatitis (allergic gingivostomatitis) Sol Silverman, J1·., j]f..tL, D.D.S.,• and Francinn Lozada, D.D.s.,•• San Francisco, Calif. UNIVERSITY OF CALIFORNIA SCHOOL OF DENTISTRY Twelve women and four men with plasma-cell gingivostomatitis were studied. This syndrome, consisting of gingivitis, cheilitis, and glossitis, apparently occurred for only a limited number of yearA, commencing in the mid-1960's. Although the cause remains obscure, the features of the disease and the response to tr eatment indicated that this condition 'ms most likely a hypersensitivity reaction. Follow-up observations showed that there have been no recurrences following treatment, and there were no associated sequelae. Between 1966 and 1971, sixteen patients with a new syndrome consisting of a diffuse homogeneous gingivitis, glossitis, and angular cheilitis were evaluated at the University of California San Francisco Oral Medicine Clinic. Because of the characteristic microscopic features that accompanied this condition, it was described as an idiopathic plasma-cell gingivostomatitis. These patients were generally in good health, and there was no apparent uniform inciting factor. Prior to and following the sixteen cases seen during this limited period of time, no similar cases have been seen or reported. Owings,S in 1969, described four patients with a similar plasma-cell gingivo- stomatitis triad of signs. He postulated that the pathogenesis was an immune re- sponse, possibly to some microorganism. In 1971 Kerr, l\IcClatchey, and RegezF described eight similar patients and indicated that the syndrome was due to a hy- persensitivity reaction to one of the constituents of chewing gum. All eight of their patients were habitual gum chewers, and with elimination of gum chewing all *Professor and Chairman, Division of Oral Biology. **Special Postdoctoral Fellow, Division of Oral Biology. 211
Transcript of An epilogue to plasma-cell gingivostomatitis (allergic ...
Reprinted from ORAL S u RGERY, ORAL 1\I~;mcil'(E, ORAL PATHOLOGY, St. Louis Vol. 43, No. 2, Pages 211-217, February, 1977 (Printed In the U . S. A . ) (Copyright €) 1977 by The C. V . 1\Iosby Company)
An epilogue to plasma-cell gingivostomatitis (allergic gingivostomatitis)
Sol Silverman, J1·., j]f..tL, D.D.S.,• and Francinn Lozada, D.D.s.,•• San Francisco, Calif.
UNIVERSITY OF CALIFORNIA SCHOOL OF DENTISTRY
Twelve women and four men with plasma-cell gingivostomatitis were studied. This syndrome, consisting of gingivitis, cheilitis, and glossitis, apparently occurred for only a limited number of yearA, commencing in the mid-1960's. Although the cause remains obscure, the features of the disease and the response to treatment indicated that this condition 'ms most likely a hypersensitivity reaction. Follow-up observations showed that there have been no recurrences following treatment, and there were no associated sequelae.
Between 1966 and 1971, sixteen patients with a new syndrome consisting of a diffuse homogeneous gingivitis, glossitis, and angular cheilitis were evaluated at the University of California San Francisco Oral Medicine Clinic. Because of the characteristic microscopic features that accompanied this condition, it was described as an idiopathic plasma-cell gingivostomatitis. These patients were generally in good health, and there was no apparent uniform inciting factor. Prior to and following the sixteen cases seen during this limited period of time, no similar cases have been seen or reported.
Owings,S in 1969, described four patients with a similar plasma-cell gingivostomatitis triad of signs. He postulated that the pathogenesis was an immune response, possibly to some microorganism. In 1971 Kerr, l\IcClatchey, and RegezF described eight similar patients and indicated that the syndrome was due to a hypersensitivity reaction to one of the constituents of chewing gum. All eight of their patients were habitual gum chewers, and with elimination of gum chewing all
*Professor and Chairman, Division of Oral Biology. **Special Postdoctoral Fellow, Division of Oral Biology.
211
212 Silvennan and Lozada Oral Surg. February, l 977
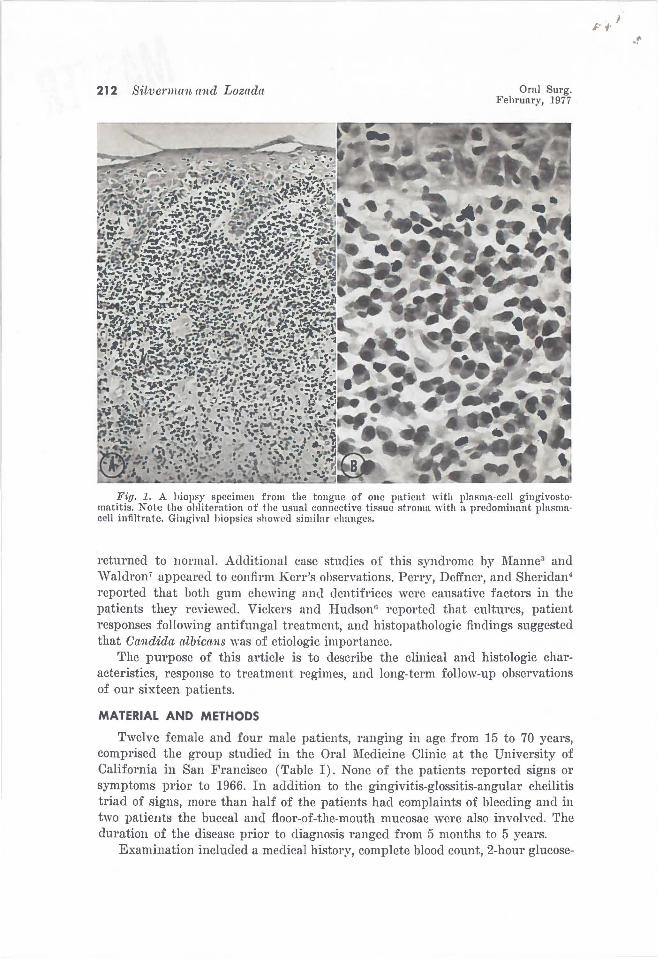
Fig. 1. A biopsy specimen from the tongue of one patient \lith plasma·eell gingivosto· matitis. Note the obliteration of the usual connective tissue stroma with a predominant plasma· cell infiltrate. Gingival hiopsics showl'd similar changes.
returned to normaL Additional case studies of this syndrome by l\fanne3 and \Valdron' appeared to confirm Kerr's observations. Perry, Dcffncr, and Sheridan4
reported that both gum chewing and dentifrices were causative factors in the patients they rc\'iewed. Vickers and Hudsonn reported that cultures, patient responses following antifungal treatment, and histopathologic findings suggested that Candida albicans was of etiologic importance.
The purpose of this article is to describe the clinical and histologic characteristics, response to treatment regimes, and long-term follow-up observations of our sixteen patients.
MATERIAL AND METHODS
Twelve female and four male patients, ranging in age from 15 to 70 years, comprised the group studied in the Oral Medicine Clinic at the University of California in San Francisco (Table I). None of the patients reported signs or symptoms prior to 1966. In addition to the gingivitis-glossitis-angular cheilitis triad of signs, more than half of the patients had complaints of bleeding and in two patients the buccal and floor-of-the-mouth mu<>osae were also involved. The duration of the disease prior to diagnosis ranged from 5 months to 5 years.
Examination included a medical history, complete blood count, 2-hour glucose-
.r
' ,
Volume 43 Number 2
Epilogne to plasma-cell gingivostomatitis 213
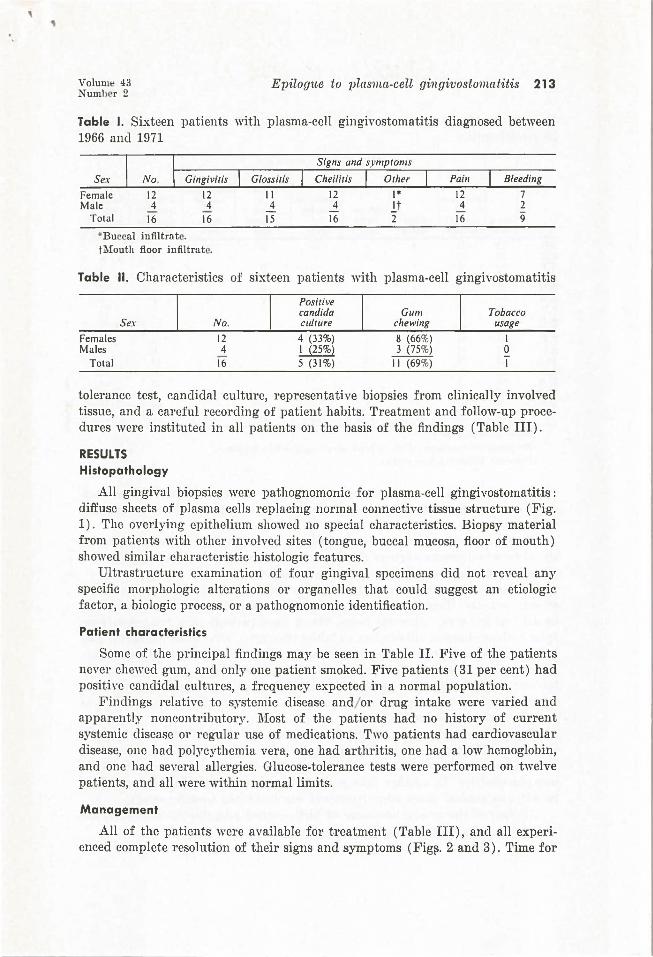
Table I. Sixteen patients with plasma-cell gingivostomatitis diagnosed between 1966 and 1971
Sex
Female Male
Total 16
*Buccal infiltra t c.
16
t Mouth floor infiltrate.
15 16 16
Bleeding
7 2 9
Table II. Characteristics of sixteen patients with plasma-cell gingivostomatitis
Positive candida Gum Tobacco
Sex No. culture chewing usage
Females 12 4 (33%) 8 (66%) I Males 4 I (25%) 3 (75%) 0
Total 16 5 (31%) II (69%) I
tolerance test, candida! culture, representative biopsies from clinically involved tissue, and a careful recording of patient habits. Treatment and follow-up procedures were instituted in all patients on the basis of the findings (Table III).
RESULTS Histopathology
All gingival biopsies were pathognomonic for plasma-cell gingivostomatitis: diffuse sheets of plasma cells replacing normal connective tissue structure (Fig. 1). The overlying epithelium showed no special characteristics. Biopsy material from patients with other involved sites (tongue, buccal mucosa, floor of mouth) showed similar characteristic histologic features.
Ultrastructure examination of four gingival specimens did not reyeal any specific morphologic alterations or organelles that could suggest an etiologic factor, a biologic process, or a pathognomonic identification.
Patient characteristics
Some of the principal findings may be seen in Table II. Five of the patients never chewed gum, and only one patient smoked. Five patients (31 per cent) had posith·c candida! cultures, a frequency expected in a normal population.
Findings relative to systemic disease and/ or drug intake were varied and apparently noncontributory. l\Iost of the patients had no history of current systemic disease or regular use of medications. Two patients had cardiovascular disease, one had polycythemia vera, one had arthritis, one had a low hemoglobin, and one had several allergies. Glucose-tolerance tests were performed on twelve patients, and all were within normal limits.
Management
All of the patients were available for treatment (Table III), and all experienced complete resolution of their signs and symptoms (Fig~. 2 and 3). Time for
214 Silverman and Lozada Oral Surg. February, 1977
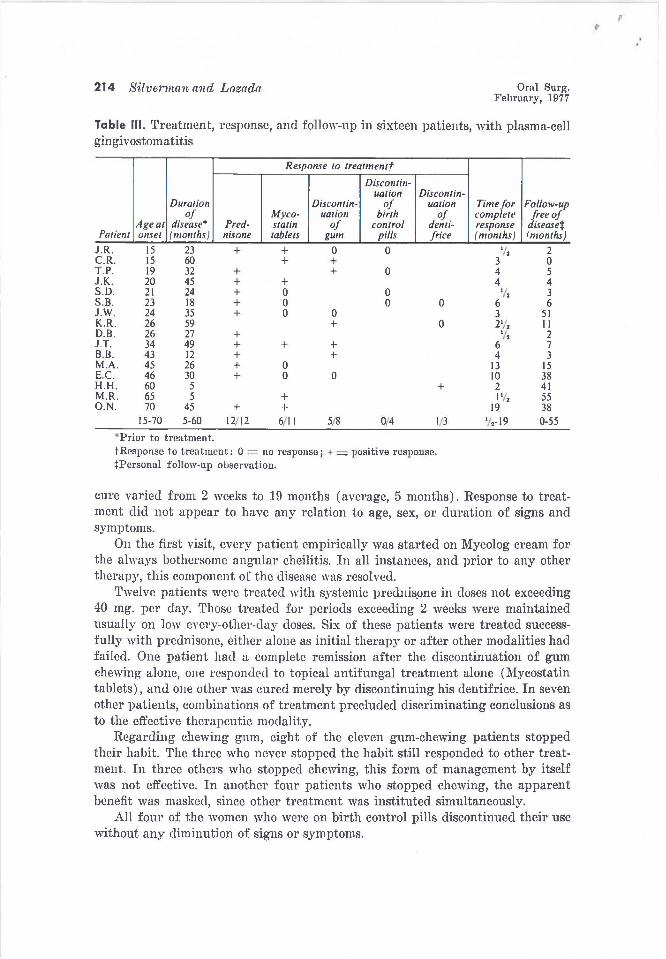
Table Ill. Treatment, response, and follow-up in sixteen patients, with plasma-cell gingi vostoma ti tis
Duration of
Age at disease• Pred-Patient onset (months) nisone
J.R. 15 23 + C.R. 15 60 T.P. 19 32 + J.K. 20 45 + S.D. 21 24 + S.B. 23 18 + J.W. 24 35 + K.R. 26 59 D.B. 26 27 + J.T. 34 49 + B. B. 43 12 + M.A. 45 26 + E. C. 46 30 + H.H. 60 5 M.R. 65 5 O.N. 70 45 +
15-70 5-60 12/12 "Prior to treatment.
Response to treatmentf
Discontin-Myco- uation stalin of tablets gum
+ 0 + +
+ + 0 0 0 0
+
+ + +
0 0 0
+ + 6/ 11 5/8
Discontin-uation
of birth
control pills
0
0
0
Discontin-uation
of denti-frice
0 0
0
+
0/4 1/3
t Response to treatment: 0 = no response; + = positive response. tPersonal follow-up observation.
Time for Follow-up complete free of response (months)
disease+ (months)
•;, 2 3 0 4 5 4 4 '/, 3
6 6 3 51 2'/, II '/, 2
6 7 4 3
13 15 10 38 2 41 1'/, 55
19 38 1/,-19 0-55
cure varied from 2 weeks to 19 months (average, 5 months). Response to treatment did not appear to have any relation to age, sex, or duration of signs and symptoms.
On the first visit, every patient empirically was started on lVIycolog cream for the always bothersome angular cheilitis. In all instances, and prior to any other therapy, this component of the disease was resolved.
Twelve patients were treated with systemic prednis.one in doses not exceeding 40 mg. per day. Those treated for periods exceeding 2 weeks were maintained usually on low every-other-day doses. Six of these patients were treated successfully with prednisone, either alone as initial therapy or after other modalities had failed. One patient had a complete remission after the discontinuation of gum chewing alone, one responded to topical antifungal treatment alone (Mycostatin tablets), and one other was cured merely by discontinuing his dentifrice. In seven other patients, combinations of treatment precluded discriminating conclusions as to the effective therapeutic modality.
Regarding chewing gum, eight of the eleven gum-chewing patients stopped their habit. The three who never stopped the habit still responded to other treatment. In three others who stopped chewing, this form of management by itself was not effective. In another four patients who stopped chewing, the apparent benefit was masked, since other treatment was instituted simultaneously.
All four of the women who were on birth control pills discontinued their usc without any diminution of signs or symptoms.
I' ,
Volume 43 Number 2
Epilog1te to plasma-cell gingivostomatitis 21 S
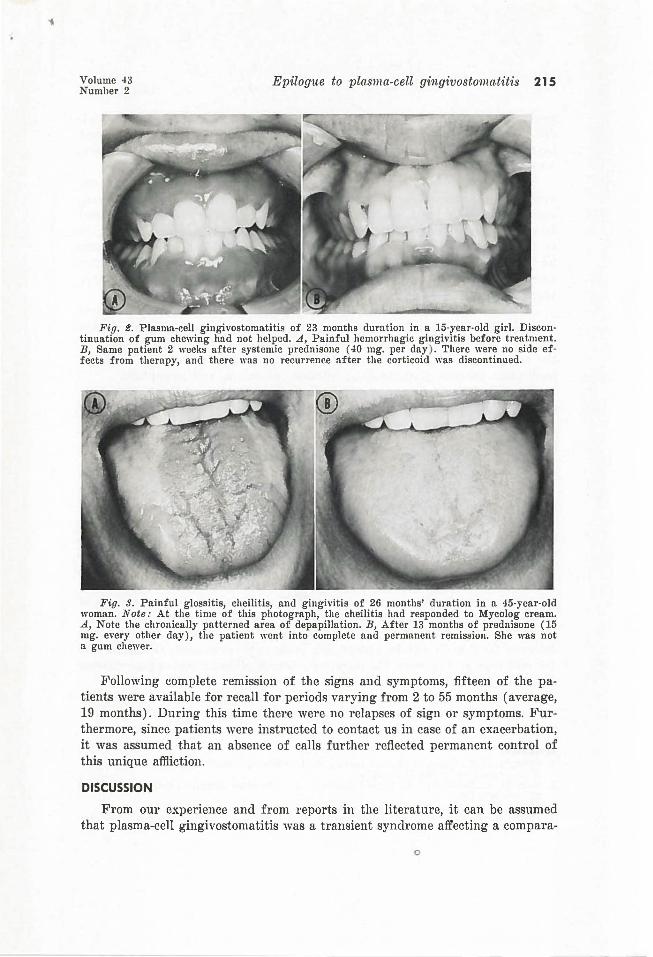
Fig. t. Plasma-cell gingivostomatitis of 23 months duration in a 15·year-old girl. Discontinuation of gum chewing had not helped . .A, Painful hemorrhagic gingivitis before treatment. B, Same patient 2 weeks after systemic prednisone (40 mg. per day ) . There were no side effects from therapy, and there was no recurrence after the corticoid was discontinued.
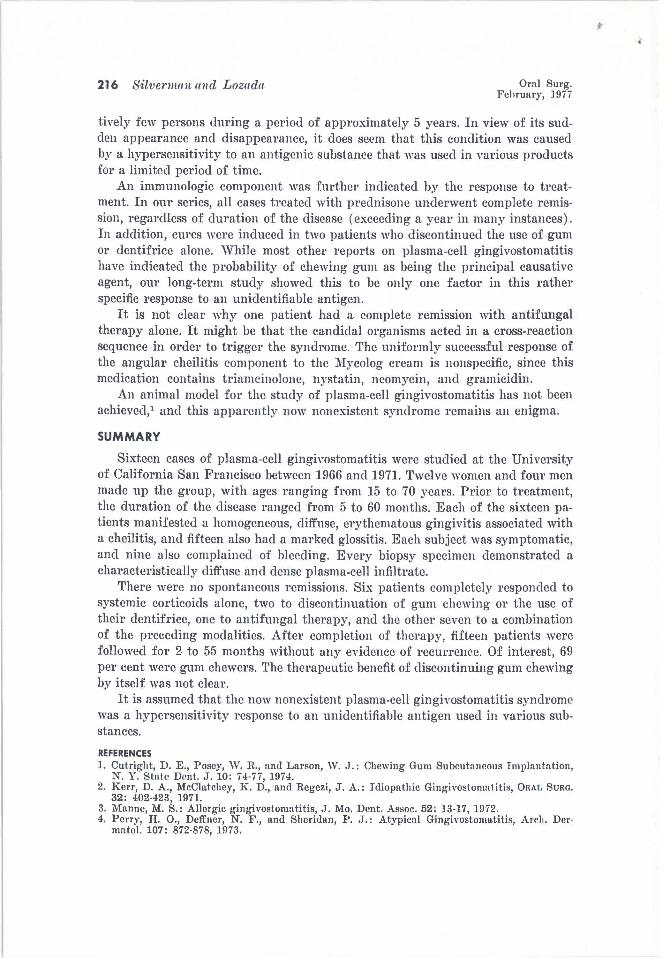
Fig. 3. Painful glossitis, cheilitis, and gingivitis of 26 months' duration in a 45-ycar-old woman. Note: At the time of this photograph, the cheilitis had responded to Mycolog cream. A, Note the chronically patterned area of depapillation. B, After 13 months of prednisone (15 mg. every other day), the patient went into complete and permanent remission. She was not o. gum chewer.
Following complete remiSSIOn of the signs and symptoms, fifteen of the patients were available for recall for periods varying from 2 to 55 months (average, 19 months). During this time there were no relapses of sign or symptoms. Furthermore, since patients were instructed to contact us in case of an exacerbation, it was assumed that an absence of calls further reflected permanent control of this unique affliction.
DISCUSSION
From our experience and from reports in the literature, it can be assumed that plasma-cell gingivostomatitis was a transient syndrome affecting a compara-
0
216 Silvenwm and Lozada Oral Surg. Fehruary, 1977
tively few persons during a period of approximately 5 years. In view of its sudden appearance and disappearance, it does seem that this condition was caused by a hypersensitivity to an antigenic substance that was used in various products for a limited period of time.
An immunologic component was further indicated by the response to treatment. In our series, all cases treated with prednisone underwent complete remission, regardless of duration of the disease (exceeding a year in many instances). In addition, cures were induced in two patients who discontinued the usc of gum or dentifrice alone. While most other reports on plasma-cell gingivostomatitis have indicated the probability of chewing gum as being the principal causative agent, our long-term study showed this to be only one factor in this rather specific response to an unidentifiable antigen.
It is not clear why one patient had a complete remission with antifungal therapy alone. It might be that the candidal organisms acted in a cross-reaction sequence in order to trigger the syndrome. The uniformly successful response of the angular cheilitis component to the 1\iycolog cream is nonspecific, since this medication contains triamcinolone, nystatin, neomycin, and gramicidin.
An animal model for the study of plasma-cell gingivostomatitis has not been achieved/ and this apparently now nonexistm1t syndrome remains an enigma.
SUMMARY
Sixteen cases of plasma-cell gingivostomatitis were studied at the University of California San Francisco between 1966 and 1971. Twelve women and four men made up the group, with ages ranging from 15 to 70 years. Prior to treatment, the duration of the disease ranged .from 5 to 60 months. Each of the sixteen patients manifested a homogeneous, diffuse, erythematous gingivitis associated with a cheilitis, and fifteen also had a marked glossitis. Each subject was symptomatic, and nine also complained of bleeding. Every biopsy specimen demonstrated a characteristically diffuse and dense plasma-cell infiltrate.
There were no spontaneous remissions. Six patients completely responded to systemic corticoids alone, two to discontinuation of gum chewing or the usc of their dentifrice, one to antifungal therapy, and the other seven to a combination of the preceding modalities. After completion of therapy, fifteen patients were followed for 2 to 55 months without any evidence of recurrenre. Of interest, 69 per cent were gum chewers. The therapeutic benefit of discontinuing gum chewing by itself was not clear.
It is assumed that the now nonexistent plasma-cell gingivostomatitis syndrome was a hypersensitivity response to an unidentifiable antigen used in various substances.
REFERENCES 1. Cutright, D. E., Posey, \V. R., and Larson, \V. J.: Chewing Gum Subcutaneous Implantation,
N. Y. State Dent. J. 10: 74-77, 1974. 2. Kerr, D. A., McClatchey, K. D., and Regezi, J. A.; Idiopathic Gingivostomatitis, ORAl, SuRa.
32: 402-423, 1971. 3. Manne, M. S.: Allergic gingivostomatitis, J. Mo. Dent. Assoc. 52: 13-17, 1972. 4. Perry, H. 0., Deffner, N. F., and Sheridan, P .• T.: Atypical Gingivostomatitis, Arrh. Der
ma to!. 107: 872-878, 1973.
'• ..
Volume 43 Number 2
Epilog1te to plasma-cell gingivosfo111atitis 217
5. Owings, J. R.: An Atypical Gingivostomatitis: A Report of Four Cases, J. Periodontal. 40: 538-42, 1969.
6. Vickers, R. A., and Hudson, C. D.: A Clinicopathologic Investigation of "Plasma Cell Gingivostomatitis," IADR Abstracts, 1971, 755, p. 241.
7. Waldron, C.: Idiopathic Gingivostomatitis, Georgia Dent. Assoc. 46: 13, 1973.
Reprint request to: Dr. Sol Silverman, Jr. Division of Oral Biology University of California School of Dentistry San Francisco, Calif. 94143