Case Report Deep Peroneal Nerve Palsy Caused by an Extraneural Ganglion...
5
Case Report Deep Peroneal Nerve Palsy Caused by an Extraneural Ganglion Cyst: A Rare Case Dimitrios Nikolopoulos, 1 George Safos, 1 Neoptolemos Sergides, 1 and Petros Safos 2 1 Orthopaedic Department, Central Clinic of Athens, 31 Asklepiou Street, 10680 Athens, Greece 2 Orthopaedic Department, Ikaria General Hospital, 83302 Ikaria, Greece Correspondence should be addressed to Dimitrios Nikolopoulos; [email protected] Received 4 October 2014; Revised 5 December 2014; Accepted 24 December 2014 Academic Editor: ierry B´ egu´ e Copyright © 2015 Dimitrios Nikolopoulos et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Lower extremities peripheral neuropathies caused by ganglion cysts are rare. e most frequent location of occurrence is the common peroneal nerve and its branches, at the level of the fibular neck. We report the case of a 57-year-old patient admitted with foot drop, due to an extraneural ganglion of the upper tibiofibular syndesmosis, compressing the deep branch of the peroneal nerve. Although there have been many previous reports of intraneural ganglion involvement with the lower limb nerves, to our knowledge, this is the second reported occurrence of an extraneural ganglion distinctly localized to the upper tibiofibular syndesmosis and palsying deep peroneal nerve. e diagnosis was made preoperatively using MRI. e common peroneal nerve and its branches were recognized and traced to its bifurcation during the operation, and the ganglion cyst was removed. Two months aſter surgery, the patient was pain-free and asymptomatic except for cutaneous anesthesia in the distribution of the deep peroneal nerve. 1. Introduction Ganglion cysts are the most frequent tumors of the upper and lower extremity. Despite their high incidence, ganglion cysts rarely result in peripheral nerve compression [1]. According to the English literature, previous reports of intraneural ganglion involvement with the common peroneal nerve and its branches, the sural nerve, and the posterior tibial nerve have been described, whereas extraneural ganglion sciatic and common peroneal nerve palsy cases are scarce [2–6]. However, leg pain, sensory loss, and weakness in ankle dorsiflexion due to deep peroneal nerve palsy from an extraneural ganglion distinctly localized to the upper tibiofibular syndesmosis have not been reported until nowa- days. Historically, the first reported case of compression neuropathy to peroneal nerve by a synovial cyst was by Sultan in 1921 [7], whereas the first reported rare cause of deep peroneal nerve palsy due to compression of synovial cyst was by Erdil et al. in 2013 [8]. e common peroneal nerve is derived from the dorsal branches of the fourth and fiſth lumbar and the first and second sacral nerves. It descends obliquely along the lateral side of the popliteal fossa to the head of the fibula, close to the medial margin of the biceps femoris muscle. e common peroneal nerve (CPN) winds round the head of the fibula and divides beneath the muscle into the superficial peroneal nerve (SPN) and the deep peroneal nerve (DPN). e SPN supplies the peroneus longus and peroneus brevis muscles. e DPN innervates the muscles of the anterior compartment of the lower extremity, such as tibialis anterior, extensor hallucis longus, extensor digitorum longus, and the fibularis (peroneus) tertius. Together these muscles are responsible for dorsiflexion of the foot and extension of the toes. It also innervates intrinsic muscles of the foot including the extensor digitorum brevis and the extensor hallucis brevis [5, 6, 9, 10]. We report the case of a 57-year-old patient admitted to our clinic with foot drop since 4 weeks. At first the deep peroneal nerve palsy was misdiagnosed as being L5-S1 disk herniation. Aſter electromyography (EMG) of the lower extremities and knee magnetic resonance imaging (MRI), an extraneural ganglion of the upper tibiofibular syndesmosis was diagnosed, compressing the deep branch of the peroneal nerve. Hindawi Publishing Corporation Case Reports in Orthopedics Volume 2015, Article ID 861697, 4 pages http://dx.doi.org/10.1155/2015/861697
Transcript of Case Report Deep Peroneal Nerve Palsy Caused by an Extraneural Ganglion...

Case ReportDeep Peroneal Nerve Palsy Caused by an ExtraneuralGanglion Cyst: A Rare Case
Dimitrios Nikolopoulos,1 George Safos,1 Neoptolemos Sergides,1 and Petros Safos2
1Orthopaedic Department, Central Clinic of Athens, 31 Asklepiou Street, 10680 Athens, Greece2Orthopaedic Department, Ikaria General Hospital, 83302 Ikaria, Greece
Correspondence should be addressed to Dimitrios Nikolopoulos; [email protected]
Received 4 October 2014; Revised 5 December 2014; Accepted 24 December 2014
Academic Editor: Thierry Begue
Copyright © 2015 Dimitrios Nikolopoulos et al.This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in anymedium, provided the originalwork is properly cited.
Lower extremities peripheral neuropathies caused by ganglion cysts are rare. The most frequent location of occurrence is thecommon peroneal nerve and its branches, at the level of the fibular neck. We report the case of a 57-year-old patient admittedwith foot drop, due to an extraneural ganglion of the upper tibiofibular syndesmosis, compressing the deep branch of the peronealnerve. Although there have been many previous reports of intraneural ganglion involvement with the lower limb nerves, toour knowledge, this is the second reported occurrence of an extraneural ganglion distinctly localized to the upper tibiofibularsyndesmosis and palsying deep peroneal nerve. The diagnosis was made preoperatively using MRI. The common peroneal nerveand its brancheswere recognized and traced to its bifurcation during the operation, and the ganglion cyst was removed. Twomonthsafter surgery, the patient was pain-free and asymptomatic except for cutaneous anesthesia in the distribution of the deep peronealnerve.
1. Introduction
Ganglion cysts are themost frequent tumors of the upper andlower extremity. Despite their high incidence, ganglion cystsrarely result in peripheral nerve compression [1]. Accordingto the English literature, previous reports of intraneuralganglion involvement with the common peroneal nerveand its branches, the sural nerve, and the posterior tibialnerve have been described, whereas extraneural ganglionsciatic and common peroneal nerve palsy cases are scarce[2–6]. However, leg pain, sensory loss, and weakness inankle dorsiflexion due to deep peroneal nerve palsy froman extraneural ganglion distinctly localized to the uppertibiofibular syndesmosis have not been reported until nowa-days. Historically, the first reported case of compressionneuropathy to peroneal nerve by a synovial cyst was by Sultanin 1921 [7], whereas the first reported rare cause of deepperoneal nerve palsy due to compression of synovial cyst wasby Erdil et al. in 2013 [8].
The common peroneal nerve is derived from the dorsalbranches of the fourth and fifth lumbar and the first andsecond sacral nerves. It descends obliquely along the lateral
side of the popliteal fossa to the head of the fibula, close tothemedialmargin of the biceps femorismuscle.The commonperoneal nerve (CPN) winds round the head of the fibulaand divides beneath the muscle into the superficial peronealnerve (SPN) and the deep peroneal nerve (DPN). The SPNsupplies the peroneus longus and peroneus brevis muscles.TheDPN innervates themuscles of the anterior compartmentof the lower extremity, such as tibialis anterior, extensorhallucis longus, extensor digitorum longus, and the fibularis(peroneus) tertius. Together these muscles are responsiblefor dorsiflexion of the foot and extension of the toes. Italso innervates intrinsic muscles of the foot including theextensor digitorum brevis and the extensor hallucis brevis[5, 6, 9, 10].
We report the case of a 57-year-old patient admittedto our clinic with foot drop since 4 weeks. At first thedeep peroneal nerve palsy was misdiagnosed as being L5-S1disk herniation. After electromyography (EMG) of the lowerextremities and knee magnetic resonance imaging (MRI), anextraneural ganglion of the upper tibiofibular syndesmosiswas diagnosed, compressing the deep branch of the peronealnerve.
Hindawi Publishing CorporationCase Reports in OrthopedicsVolume 2015, Article ID 861697, 4 pageshttp://dx.doi.org/10.1155/2015/861697

2 Case Reports in Orthopedics
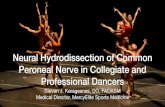
Figure 1: Left knee MRI demonstrated a lobulated, multilocular, and well-demarcated cystic-appearing mass medial to the fibular head(ganglion).
Figure 2: Left knee lateral approach.TheCPN and its branches were recognized and traced to its bifurcation.The ganglionmass was followeddown to its stalk and removed completely.
2. Case Presentation
A 57-year-old Caucasian male presented to his physicianwith an acute onset of left lower limb pain and suddenfoot drop. The patient referred to numbness and motorweakness in the lateral aspect of his left leg, after the onsetof severe pain. His medical history revealed a single episodeof low back pain without numbness, motor weakness, andsevere pain four years before. The physician resulted in themisdiagnosis of degenerative disc disease of the lumbar spineand recommended MRI of the lumbar spine and prescribedpainkillers and anti-inflammatory treatment for one week.Lumbar’s spine MRI was normal, whereas one week after theonset of the symptoms, there was no clinical improvement.
The patient visited our clinic 4 weeks after the onset ofthe symptoms. He was unable to perform foot eversion anddorsiflexion, especially of the first toe, when he was referredto our hospital. Inversion was normal. Manual muscle testingof the left tibialis anterior, extensor hallucis longus, extensordigitorum longus, and peroneus muscles revealed musclestrength at the level of 2 (trace), according to the Daniels andWorthinghammuscle power grading system [11]. Diminishedsensation in the first web space and positive Tinel’s sign nearthe head of the fibula on the left footwere also detected during
the examination. Tenderness in the area of the left fibularhead with gradual development of swelling in the same areawas determined, although no mass lesion was palpable.
Electromyogram studies of the CPN and its branchesdemonstrated significant neuropathic abnormalities of theDPN. No abnormality was found in the muscles innervatedby the tibial nerve. Subsequent left knee MRI demon-strated a lobulated, multilocular, and well-demarcated cystic-appearing mass medial to the fibular head. It measuredapproximately 3.2 cm × 2.5 cm × 2 cm (Figure 1). The lesionwas located anteromedial to the fibular neck, anterior of theupper tibiofibular syndesmosis, compressing the DPN.
With a lateral approach, the CPN and its branches wererecognized and traced to its bifurcation (Figure 2). The masswas followed down to its stalk and removed completely.The DPN was recognized as intact. All nerve branches werepreserved under loupe magnification. The tumor had noconnection with the proximal tibiofibular joint or with theknee joint. Histopathological evaluation of the decompressedgelatinous material verified the diagnosis of ganglion.
Postoperatively, he was treated with an antifoot droppolyethylene splint, fixed in neutral ankle position, andphysiotherapy. Forty-eight hours postoperatively the patienthad no complaints of pain, but the foot drop remained

Case Reports in Orthopedics 3
although the sensation in the first web space improved (4/5).The patient recovered to grade 4 toe extension and ankledorsiflexion within six weeks after the surgery. Two monthsafter operation there was an almost full recovery of themotorfunction with minimal numbness in the first web space.
3. Discussion
Peripheral nerve lesions owing to ganglionic cysts are infre-quent findings [2]. Since the first description of a peronealnerve neuropathy by Sultan in 1921 [7], a minority of casesof the lower extremity compression neuropathies have beendescribed in the surgical literature [1–7, 10–12]. The CPN,derived from L4, L5, S1, and S2 as a main division of thesciatic nerve, arises near the upper level of the popliteal fossaand becomes most vulnerable at its entrance to the fibulartunnel, where it courses superficial to the lateral surface ofthe fibula just distal to the fibular head, having little soft tissueprotection [1, 7].Theproximal tibiofibular joint consists of thearticulating surfaces of the upper end of the fibular head andthe tibial lateral condyle. Both these surfaces are covered withhyaline cartilage. This joint is lined by a synovial membraneand is often in communication with the knee joint. The jointis surrounded by an articular capsule which is reinforced bythe anterior and posterior ligaments [13]. Rawal et al. [4]hypothesized that the origin of peroneal nerve ganglia is theproximal tibiofibular joint, via the articular branch.
A review of the literature supplies an extensive list of eti-ologies for peroneal nerve palsy, intraneural (schwannoma,nerve herniation through a fascial defect, and giant plexiformneurofibromatosis) [1, 12, 14–16] and extraneural (varicoseveins and pneumatic compression, after knee surgical oper-ation such as a valgus knee total arthroplasty or proximaltibial osteotomy and ganglion cysts) [1, 2, 4, 14, 17]. Althoughrare, intraneural ganglions located within the substance ofnerves may cause direct nerve compression with acute onsetof symptoms [5]. As already mentioned, there have beenmany previous reports of intraneural ganglion involvementwith the CPN and its branches [3, 5, 12]; however, this isthe second reported occurrence of an extraneural gangliondistinctly localized to the upper tibiofibular syndesmosis andpalsying DPN.
Ganglion cysts are commonly accompanied by signs ofnerve irritation such as numbness, tingling, and pain in thedistribution of the affected nerve. In peroneal nerve palsies,the patients often complain of altered ambulation secondaryto paretic or paralyzed ankle dorsiflexors. A steppage gaitpattern is common, due to the weakness in the tibialisanterior, the extensor hallucis longus, the extensor digitorumlongus, and the peroneus longus and brevis muscles. Theaffected foot requires extra lift from the ground during theswing phase of ambulation to clear the foot [1, 2].The extensordigitorum brevis is the most profoundly affected. The tibialisanterior can also be significantly affected with weakness inankle and toe dorsiflexion. Often, ankle eversion is normal,because patients can have relative sparing of these muscles[1, 2]. While pain is not universal, when present, it is oftenrelated to the specific site of the CPN compression or its
branches (superficial or deep). Sensory testing often showsa loss in the cutaneous distribution of the superficial anddeep peroneal nerves. Tinel’s sign is generally positive in thesensory distribution of the peroneal nerve [1].
The differential diagnosis should include L5 root pathol-ogy (compression), a nerve compression near the tendinousarch of the peroneal longus muscle, a nerve-sheath tumor,the osteocartilaginous exostosis at the proximal lower leg [6,10, 12, 18, 19], and intermittent claudication [2]. Plain radio-graphs have little importance in the diagnosis of ganglioncyst but may be beneficial in eliminating a bony anomaly orfracture of the proximal part of fibula. Furthermore, theymaybe useful in excluding degenerative disc disease of the lumbarspine [1, 10]. An EMG study may be helpful to distinguishthe level of the palsy and the extent of sensory and motorimpairment. MRI is the noninvasive technique of choicefor diagnostic imaging. It may be difficult to differentiate aganglion cyst fromnerve sheath tumors and also solidmasseson magnetic resonance imaging. Ganglia characteristicallypresent with low signal on T1-weighted images and high sig-nal on T2-weighted images [20]. Ultrasonography (US) maybe effective in showing the cystic nature of the mass (well-circumscribed) and in differentiating it from solid tumors(anechoic lesion) [1, 10, 21–23]. Although US is a noninvasiveand cheap screening method, it is not sensitive enough todistinguish ganglia from other nerve sheath tumors [8].Nevertheless, Visser [22] and Bayrak et al. [23] presentedthat sonographic detection of multifocal nerve enlargementis useful for the diagnosis of hereditary neuropathy withliability to pressure palsies especially when electrodiagnosticstudies are limited and/or genetic analysis is not compatible.
Currently, the gold standard treatment for a peronealnerve palsy due to a peripheral nerve ganglion compressionis surgical removal of the ganglion [1–5, 12–17]. Carefulsurgical planning and proper delineation of the mass is vitalin identifying its origin. It is important to excise the stalkand its base in the superior tibiofibular joint so as to lessenthe risk of recurrence. Sometimes the small sensory articularbranch of the joint has to be sacrificed [4]. The prognosis ofthe peroneal nerve palsies of compressive origin is excellent.When conservatively treated, recovery may take 1 year or 2years and it may be incomplete, requiring the patient to use aperoneal brace. Instead recovery ismuch faster after operativedecompression and will take place after few days or a fewweeks [3, 13, 14]. In our case the patient recovered to grade 4toe extension and ankle dorsiflexionwithin sixweeks after thesurgery, and two months after operation there was an almostfull recovery of the motor function with minimal numbnessin the first web space.
Fabre et al. [24] reported 60 patients with peroneal nervepalsies, many idiopathic, who were treated with operativedecompression. Postoperative recovery of motor functionwas good to excellent in 87% of those who had both sensoryand motor involvement preoperatively. Decompression isrecommended even for patients presenting with only sensorysymptoms, if the symptoms have been substantiated byelectrophysiological studies. Local cyst recurrence postoper-atively is reported and stresses the importance of articularbranch ligation to avoid this complication [1, 20, 25, 26].

4 Case Reports in Orthopedics
Simple excision of the ganglia is not sufficient. Other com-plications include traction injuries and perineural fibrosiswith incomplete return of function. Less commonly, nervetransection occurs, leading to permanent dysfunction [1].
4. Conclusions
Ganglion cysts should be considered in the differentialdiagnosis of progressive peroneal or sciatic nerve palsy. Otherclinical entities that should be considered in the differentialdiagnosis include L5 root lesions and nerve sheath tumors.After a complete history and physical examination, EMGand MRI should be performed in terms of the differentialdiagnosis of a ganglion cyst. Careful preoperative evaluationand early surgical excision, including also decompression ofthe nerve by microsurgical technique in the management ofthe ganglion cyst, should be recommended.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
References
[1] R. J. Greer-Bayramoglu, A. S. Nimigan Bsc, and B. S. Gan,“Compression neuropathy of the peroneal nerve secondary toa ganglion cyst,” Canadian Journal of Plastic Surgery, vol. 16, no.3, pp. 181–183, 2008.
[2] R. Ozden, V. Uruc, A. Kalaci, and Y. Dogramaci, “Compressionof common peroneal nerve caused by an extraneural ganglioncyst mimicking intermittent claudication,” Journal of BrachialPlexus and Peripheral Nerve Injury, vol. 8, no. 1, article 5, 2013.
[3] K. Muramatsu, T. Hashimoto, Y. Tominaga, K. Tamura, and T.Taguchi, “Unusual peroneal nerve palsy caused by intraneuralganglion cyst: pathological mechanism and appropriate treat-ment,” Acta Neurochirurgica, vol. 155, no. 9, pp. 1757–1761, 2013.
[4] A. Rawal, K. R. Ratnam, Q. Yin, C. Sinopidis, and S. P. Frostick,“Compression neuropathy of common peroneal nerve causedby an extraneural ganglion: a report of two cases,”Microsurgery,vol. 24, no. 1, pp. 63–66, 2004.
[5] O. Tehli, R. C. Celikmez, B. Birgili, I. Solmaz, and E. Celik, “Pureperoneal intraneural ganglion cyst ascending along the sciaticnerve,” Turkish Neurosurgery, vol. 21, no. 2, pp. 254–258, 2011.
[6] D. A. Frank and M. J. Sangimino, “Peroneal nerve palsysecondary to ganglion cyst of the proximal tibiofibular joint ina pediatric patient,” Orthopedics, vol. 31, no. 1, p. 86, 2008.
[7] C. Sultan, “Ganglion der Nervenscheide des Nervus Peroneus,”Zentralblatt fur Chirurgie, vol. 48, pp. 963–965, 1921.
[8] M. Erdil, K. Ozkan, F. U. Ozkan et al., “A rare cause of deepperoneal nerve palsy due to compression of synovial cyst—casereport,” International Journal of Surgery Case Reports, vol. 4, no.5, pp. 515–517, 2013.
[9] D. V. Davies, Gray’s Anatomy, edited by R. E. Coupland, 3rdimpression, Longmans, Longuang, 34th edition, 1972.
[10] R. J. Spinner, N. M. Desy, and K. K. Amrami, “Sequentialtibial and peroneal intraneural ganglia arising from the superiortibiofibular joint,” Skeletal Radiology, vol. 37, no. 1, pp. 79–84,2008.
[11] H. J. Hislop and J. Montgomery, Daniels and Worthingham'sMuscle Testing: Techniques of Manual Examination, WB Saun-ders, Philadelphia, Pa, USA, 6th edition, 1995.
[12] E. D. Stamatis, N. E. Manidakis, and P. P. Patouras, “Intraneuralganglion of the superficial peroneal nerve: a case report,” Journalof Foot and Ankle Surgery, vol. 49, no. 4, pp. 400–e1, 2010.
[13] F. de Schrijver, J. P. Simon, L. de Smet, and G. Fabry, “Ganglia ofthe superior tibiofibular joint: report of three cases and reviewof the literature,” Acta Orthopaedica Belgica, vol. 64, no. 2, pp.233–241, 1998.
[14] M. Yazid Bajuri, B. C. Tan, S. Das, S. Hassan, and S. Subanesh,“Compression neuropathy of the common peroneal nervesecondary to a ganglion cyst,” Clinica Terapeutica, vol. 162, no.6, pp. 549–552, 2011.
[15] L. J. S. Yang, V. C. Gala, and J. E. McGillicuddy, “Superficialperoneal nerve syndrome: an unusual nerve entrapment—casereport,” Journal of Neurosurgery, vol. 104, no. 5, pp. 820–823,2006.
[16] O. Cebesoy, E. Tutar, M. Isik, and O. Arpacioglu, “A case ofisolated giant plexiform neurofibroma involving all branchesof the common peroneal nerve,” Archives of Orthopaedic andTrauma Surgery, vol. 127, no. 8, pp. 709–712, 2007.
[17] U.Waldschmidt and T. Slongo, “An unusual cause of paralysis ofthe peroneal nerve-a case report,” Journal of Pediatric Surgery,vol. 45, no. 1, pp. 259–261, 2010.
[18] J. P. Huaux, J. Malghem, B. Maldague et al., “Pathology of theupper peroneotibial joint. History of cysts. Apropos of 4 cases,”Revue duRhumatisme et desMaladies Osteo-Articulaires, vol. 53,pp. 723–726, 1986.
[19] G. P. Ramelli, L. Nagy, E. Tuncdogan, and J. Mathis, “Ganglioncyst of the peroneal nerve: a differential diagnosis of peronealnerve entrapment neuropathy,” European Neurology, vol. 41, no.1, pp. 56–58, 1999.
[20] D. J. Iverson, “MRI detection of cysts of the knee causingcommon peroneal neuropathy,” Neurology, vol. 65, no. 11, pp.1829–1831, 2005.
[21] M. Lucchetta, G. A. Liotta, C. Briani et al., “Ultrasounddiagnosis of peroneal nerve variant in a child with compressivemononeuropathy,” Journal of Pediatric Surgery, vol. 46, no. 2, pp.405–407, 2011.
[22] L. H. Visser, “High-resolution sonography of the commonperoneal nerve: detection of intraneural ganglia,” Neurology,vol. 67, no. 8, pp. 1473–1475, 2006.
[23] A. O. Bayrak, I. K. Bayrak, E. Battaloglu et al., “Ultrasono-graphic findings in hereditary neuropathy with liability topressure palsies,” Neurological Research, vol. 37, no. 2, pp. 106–111, 2014.
[24] T. Fabre, C. Piton, D. Andre, E. Lasseur, and A. Duran-deau, “Peroneal nerve entrapment,” Journal of Bone and JointSurgery—Series A, vol. 80, no. 1, pp. 47–53, 1998.
[25] S. Rein, S. Weindel, H.-E. Schaller, M. Mittelbronn, and G.Schmidt, “Peroneal nerve palsy caused by a recurrent proximaltibiofibular joint ganglion—a case report and review of theliterature,” Handchirurgie Mikrochirurgie Plastische Chirurgie,vol. 37, no. 4, pp. 267–275, 2005.
[26] A. S. Dubuisson and A. Stevenaert, “Recurrent ganglion cystof the peroneal nerve: radiological and operative observations:case report,” Journal of Neurosurgery, vol. 84, no. 2, pp. 280–283,1996.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com