Cardiovascular system ppt
51
-
Upload
mahendra-lamba -
Category
Education
-
view
356 -
download
15
Transcript of Cardiovascular system ppt


HEARTThe heart is a roughly cone-shaped hollow muscular
organ found in all animals and human beings with a
circulatory system, that is responsible for pumping
blood throughout the blood vessels by repeated,
rhythmic contractions. The term cardiac means
"related to the heart" and comes from the Greek
word, kardia, for "heart".
The human heart is about the size of a fist and has a
mass of between 250 and 300 grams. It is about 10
cm long and located slightly left of middle in the
chest, anterior to the vertebral column and posterior
to the sternum.

POSITION OF HEART
The heart situated in thoracic cavity in mediasternum, the space
between the lungs. It lies little more to the left than the right, and have
base above and an apex below. The apex is about 9 cm to the left of the
midline at the level of the 5th intercostal space, little below the nipple
and slightly nearer the midline. The base extends to the level of the 2nd
rib.
ORGANS ASSOCIATED WITH THE HEART:
Inferiorly: central tendon of the diaphragm
Superiorly: the great blood vessels; aorta, superior venacova,
pulmonary artery and vein.
Posteriorly: oesophagus, trachea, bronchus, descending aorta
Laterally: the lungs
Anteriorly: the sternum, ribs and intercostal muscle.


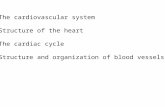
STRUCTURE OF THE HEART
The heart is composed of three layers of tissue pericardium, myocardium and endocardium;
Pericardium: The pericardium is a triple-layered fluid-filled sacthat surrounds the heart. The outer layer of this sac is the fibrouspericardium. It is a strong layer of connective tissue. It adheresto the diaphragm inferiorly, and superiorly it is fused to the rootsof the great vessels that leave and enter the heart. The fibrouspericardium acts as a tough outer coat that holds the heart inplace and keeps it from overfilling with blood. Deep to thefibrous pericardium is the double layered serouspericardium. The serous pericardium is a closed sac sandwichedbetween the fibrous pericardium and the heart. The outer layeris the parietal layer of the serous pericardium and adheres to theinner surface of the fibrous pericardium. The parietal layer iscontinuous with the visceral layer of the serous pericardium,which lies on the heart and is considered a part of the heart wall.

Myocardium: The myocardium is the basic muscle thatmakes up the heart. This muscle is involuntary. The cardiacmuscle structure consists of basic units of cardiac musclecells known as myocytes. Coordinated contraction of thecardiac muscles is what makes the heart propel blood tovarious parts of the body. It is the function of the coronaryarteries to supply blood and oxygen to the cardiac muscles.This is the thickest of all the layers of the heart. The cardiacmuscles cannot afford to rest even for a single second So, it isabsolutely essential that these muscles get blood supply andnutrition continuously, as any kind of disruption in the bloodand nutrition supply to these muscles can result in death of apart of the cardiac muscle, which is known as myocardialinfarction or heart attack. This could in turn lead to acomplete cessation of functioning of the heart muscles,known as cardiac arrest.

Endocardium: The endocarium is the innermost, thin and
smooth layer of epithelial tissue that lines the inner surface
of all the heart chambers and valves. This layer is made of
thin and flat cells that are in direct contact with the blood
that flows in and out of the heart. Each heart valve is formed
by a fold of endocardium with connective tissue between the
two layers. However, rather than just being an inner lining of
the heart, the endocardium also has an endocrine function.
This is one of the only layers of the heart that has a single
cell lining that secretes the hormone endocardin, which is
responsible for prolonging myocardial contraction.
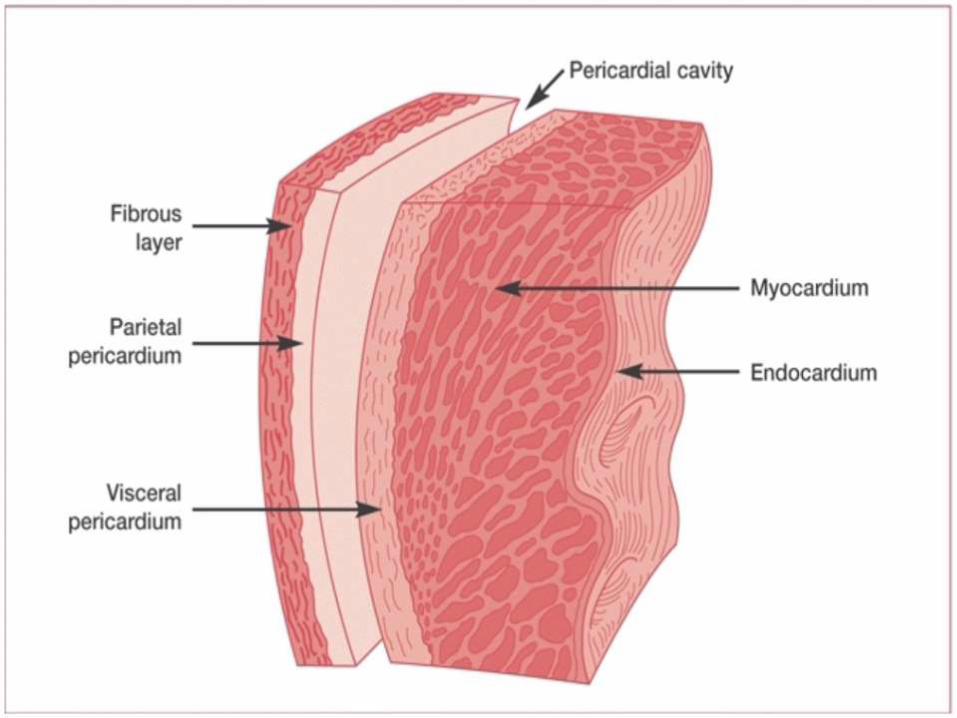
DIFFERENT VIEWS OF HEART
CHAMBERS OF HEART
The heart is a hollow organ divided into four chambers:
Right atrium
Right ventricle
Left atrium
Left ventricle

FOUR CHAMBERS OF HEART

The heart is divided into a right and left side by the septum. After
birth blood can not pass through the septum from one side to
another side. Each side is divided by an atrioventricle valve into
an upper chamber , the atrium and lower chamber, the ventricle.
The atrioventricular valves are formed by double folds of
endocardium. The heart consists of four chambers in which blood
flows. Blood enters the right atrium and passes through the right
ventricle. The right ventricle pumps the blood to the lungs where
it becomes oxygenated. The oxygenated blood is brought back to
the heart by the pulmonary veins which enter the left atrium.
From the left atrium blood flows into the left ventricle. The left
ventricle pumps the blood to the aorta which will distribute the
oxygenated blood to all parts of the body.
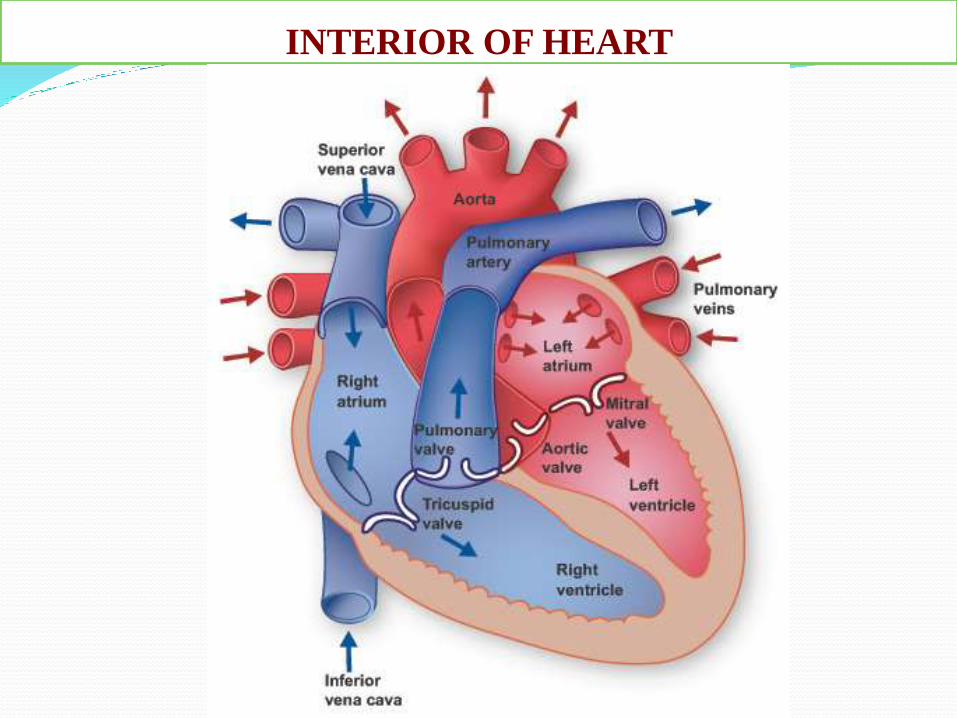
INTERIOR OF HEART

1. Right Atrium
The right atrium is a broad, triangular structure. The superiorvena cava opens into dome of right atrium and the inferiorvena cava into its lower posterior part. It is an extensivemuscular pouch projects anteriorly to overlap the right sideof the ascending aorta. Anteriorly, the right atrium is relatedto the anterior part of the surface of the right lung. Laterally,it is related to the surface of the right lung.

The interior surface of the right atrium can be divided asmooth-walled venous component posteriorly, the vestibuleof the tricuspid valve. The wall of the vestibule is smooth, butits junction with the auricle is ridged all around theatrioventricular junction. The smooth-walled part receivesthe opening of the venae cavae and the coronary sinus. Itrepresents the venous component. The wall of the vestibulehas a ridged surface.

The coronary sinus opens into the atrial component betweenthe orifice of the inferior vena cava, and the vestibule of theatrioventricular opening. Coronary sinus is often guarded bya thin, semicircular valve.

2. Right Ventricle
The right ventricle extends from the right atrioventricular(tricuspid) orifice nearly to the cardiac apex. It then reachingthe pulmonary orifice and supporting the cusps of thepulmonary valve. The ventricle possesses an inlet componentwhich supports and surrounds the tricuspid valve.
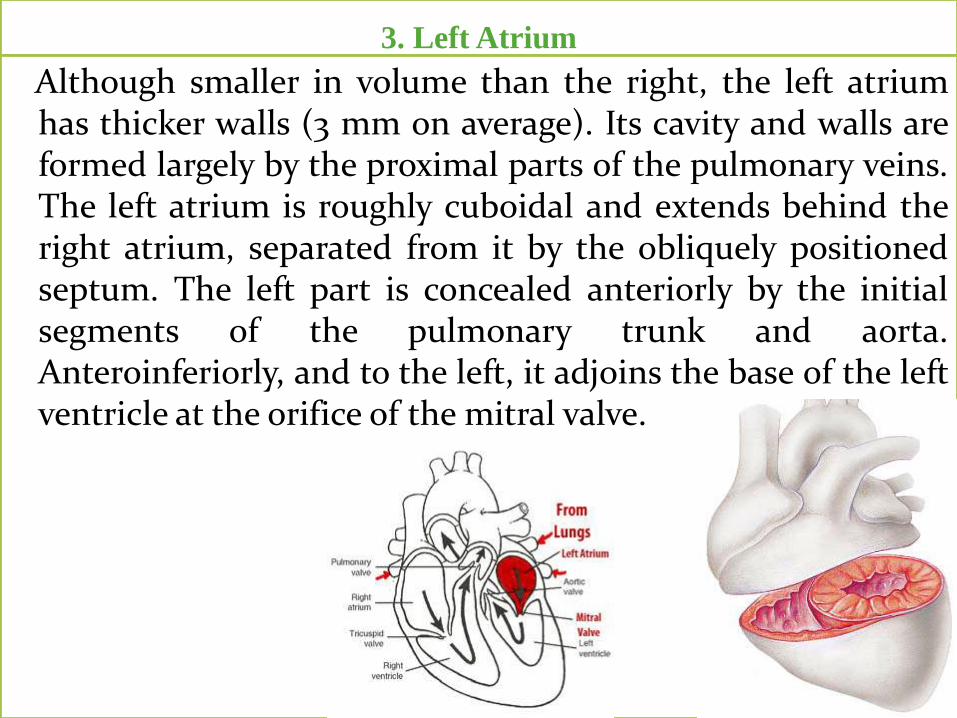
3. Left Atrium
Although smaller in volume than the right, the left atriumhas thicker walls (3 mm on average). Its cavity and walls areformed largely by the proximal parts of the pulmonary veins.The left atrium is roughly cuboidal and extends behind theright atrium, separated from it by the obliquely positionedseptum. The left part is concealed anteriorly by the initialsegments of the pulmonary trunk and aorta.Anteroinferiorly, and to the left, it adjoins the base of the leftventricle at the orifice of the mitral valve.
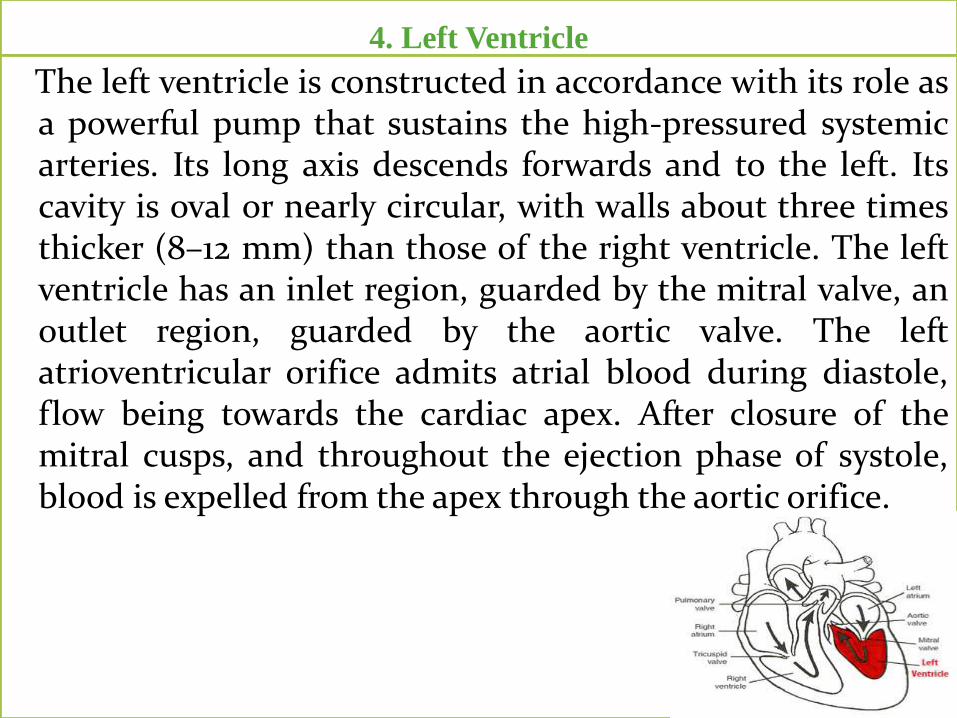
4. Left Ventricle
The left ventricle is constructed in accordance with its role asa powerful pump that sustains the high-pressured systemicarteries. Its long axis descends forwards and to the left. Itscavity is oval or nearly circular, with walls about three timesthicker (8–12 mm) than those of the right ventricle. The leftventricle has an inlet region, guarded by the mitral valve, anoutlet region, guarded by the aortic valve. The leftatrioventricular orifice admits atrial blood during diastole,flow being towards the cardiac apex. After closure of themitral cusps, and throughout the ejection phase of systole,blood is expelled from the apex through the aortic orifice.

VALVES OF HEART Every opening between the chambers and into the vessels issupplied with a valve that protects backward flow of blood.
The two Atrioventricular (AV) valves , which are between
the atria and the ventricles;
I. Mitral valve
II. Tricuspid valve
The two Semilunar (SL) valves, which are in the arteries
leaving the heart;
I. Aortic valve
II. Pulmonary valve

Atrioventricular (AV) valves: These are small valves that
prevent backflow from the ventricles into the atrium during
systole. They are anchored to the wall of the ventricle by
chordae tendineae, which prevent the valve from inverting.
The chordae tendineae are attached to papillary muscles that
cause tension to better hold the valve. Together, the papillary
muscles and the chordae tendineae are known as the
subvalvular apparatus. The function of the subvalvular
apparatus is to keep the valves from prolapsing into the atria
when they close. The subvalvular apparatus have no effect
on the opening and closure of the valves, however. This is
caused entirely by the pressure gradient across the valve.
The closure of the AV valves is heard as the first heart
sound (S1).

I. Mitral valve: Also known as the "bicuspid valve"contains two flaps. It allows the blood to flow from theleft atrium into the left ventricle. It is on the left side ofthe heart and has two cusps. A common complicationof rheumatic fever is thickening and stenosis of themitral valve.

II. Tricuspid valve: The tricuspid valve is the three-flapped
valve on the right side of the heart, between the right
atrium and the right ventricle which stops the backflow of
blood between the two. It has three cusps.

Semilunar valves: These are located at the base of both thepulmonary trunk (pulmonary artery) and the aorta, thetwo arteries taking blood out of the ventricles. Thesevalves permit blood to be forced into the arteries, butprevent backflow of blood from the arteries into theventricles. These valves do not have chordae tendineae,and are more similar to valves in veins thanatrioventricular valves.

I. Aortic valve: The aortic valve lies between the left ventricleand the aorta. The aortic valve has three cusps. Duringventricular systole, pressure rises in the left ventricle.When the pressure in the left ventricle rises above thepressure in the aorta, the aortic valve opens, allowing bloodto exit the left ventricle into the aorta. When ventricularsystole ends, pressure in the left ventricle rapidly drops.When the pressure in the left ventricle decreases, the aorticpressure forces the aortic valve to close. The closure of theaortic valve cause second heart sound (S2). The mostcommon congenital abnormality of the heart is thebicuspid aortic valve. In this condition, instead of threecusps, the aortic valve has two cusps. This condition isoften undiagnosed until the person develops calcific aorticstenosis. Aortic stenosis occurs in this condition usually inpatients in their 40s or 50s, an average of over 10 yearsearlier than in people with normal aortic valves.

II. Pulmonary valve: The pulmonary valve (sometimesreferred to as the pulmonic valve) is the semilunar valveof the heart that lies between the right ventricle and thepulmonary artery and has three cusps. Similar to theaortic valve, the pulmonary valve opens in ventricularsystole, when the pressure in the right ventricle risesabove the pressure in the pulmonary artery. At the end ofventricular systole, when the pressure in the rightventricle falls rapidly, the pressure in the pulmonaryartery will close the pulmonary valve. The closure of thepulmonary valve cause second heart sound (S2).

STRUCTURE OF VALVE
Heart valves are made up offlaps of thin, strong, tissueattached to the heart withfibrous cords called ascusps. They can only openin one direction. Valveshave two functions. Theyallow blood to flowthrough them smoothlyand prevent it from leakingback against this flow.Valves allow blood to flowin one direction only.
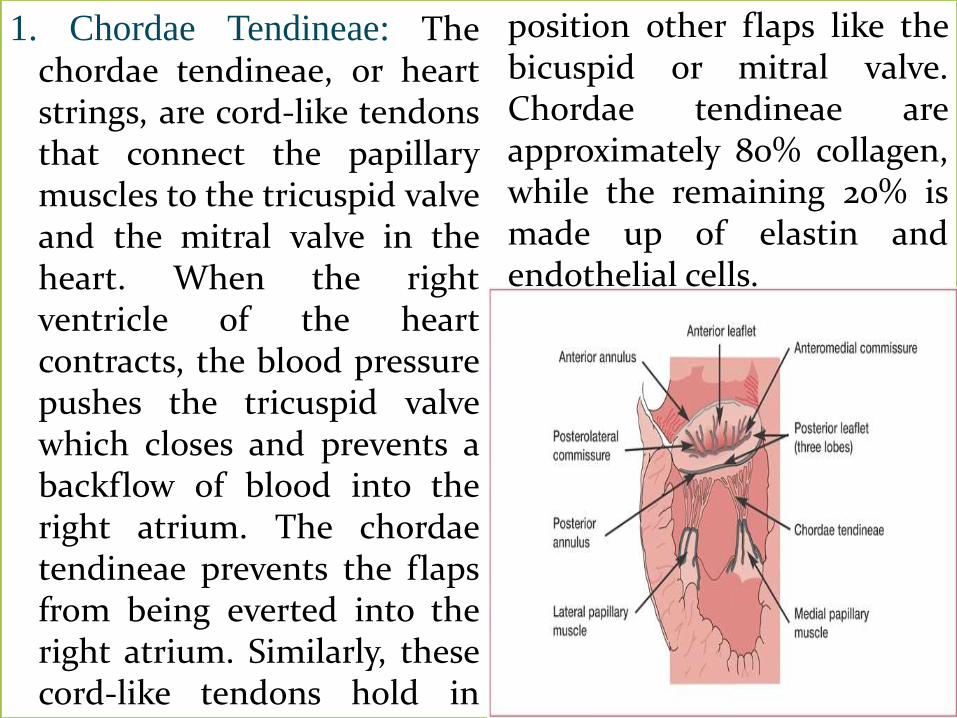
1. Chordae Tendineae: Thechordae tendineae, or heartstrings, are cord-like tendonsthat connect the papillarymuscles to the tricuspid valveand the mitral valve in theheart. When the rightventricle of the heartcontracts, the blood pressurepushes the tricuspid valvewhich closes and prevents abackflow of blood into theright atrium. The chordaetendineae prevents the flapsfrom being everted into theright atrium. Similarly, thesecord-like tendons hold in
position other flaps like thebicuspid or mitral valve.Chordae tendineae areapproximately 80% collagen,while the remaining 20% ismade up of elastin andendothelial cells.
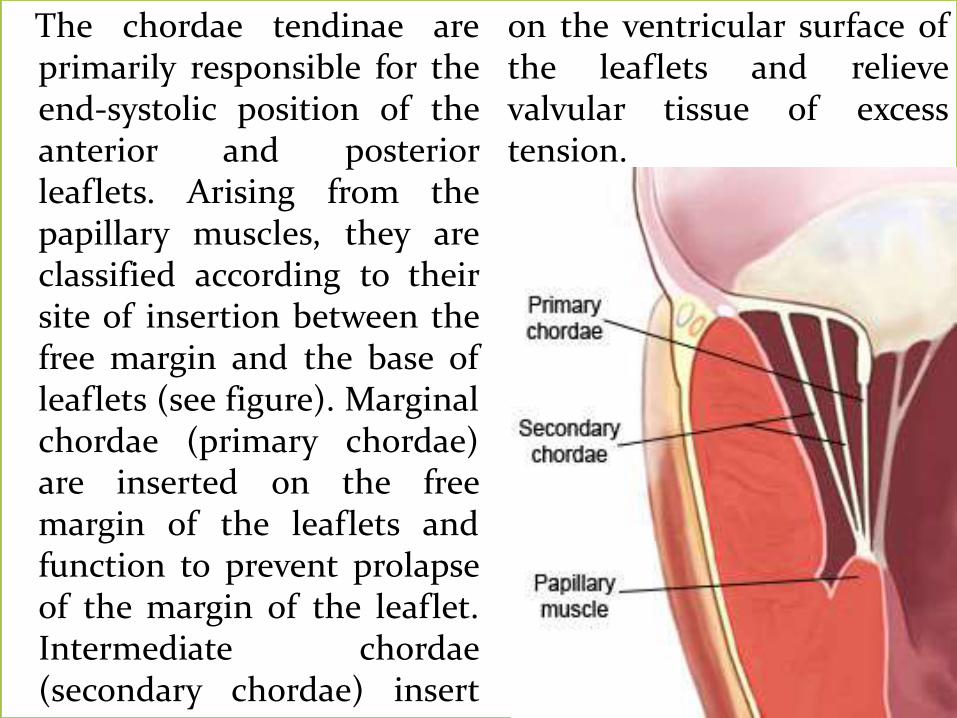
The chordae tendinae areprimarily responsible for theend-systolic position of theanterior and posteriorleaflets. Arising from thepapillary muscles, they areclassified according to theirsite of insertion between thefree margin and the base ofleaflets (see figure). Marginalchordae (primary chordae)are inserted on the freemargin of the leaflets andfunction to prevent prolapseof the margin of the leaflet.Intermediate chordae(secondary chordae) insert
on the ventricular surface ofthe leaflets and relievevalvular tissue of excesstension.

2. Papillary Muscles: Thechordae tendinae areconnected to the ventriclevia the papillary muscles,mitral valve function isrelated to theventricle. There are twopapillary muscles; medialand lateral papillarymuscles. Each papillarymuscle provides chordae toleaflets. The left circumflexor right coronary arteryprovides the blood supplyto the papillary muscles.

3.Commissures: Thecommissures define a distinctarea where the anterior andposterior leaflets cometogether at their insertioninto the annulus. Sometimesthe commissures exist as welldefined leaflet segments andcan be identified using twoanatomic landmarks: the axisof corresponding papillarymuscles and the commissuralchordae, which have aspecific configuration.

4. Leaflets: The valves hastwo to three leaflets. Theanterior leaflet has a semi-circular shape and attachesto two fifths of the annularcircumference. There iscontinuity between theanterior leaflet of themitral valve and the leftand non-coronary cusp ofthe neighboring aorticvalve, referred to as theaortic-mitral curtain.

BLOOD FLOW THROUGH THE HEART
Un-oxygenated bloodenters the atrium on theright side of the heartthrough the superior andinferior vena cava. Whilethe un oxygenated blood isin the right atrium, thetricuspid valve is closed tokeep the blood fromflowing down to theventricle. The atriumcontracts and the tricuspidvalve opens, forcing theblood down into the
ventricle. The tricuspidvalve closes again so thatblood can not move backup into the atrium.
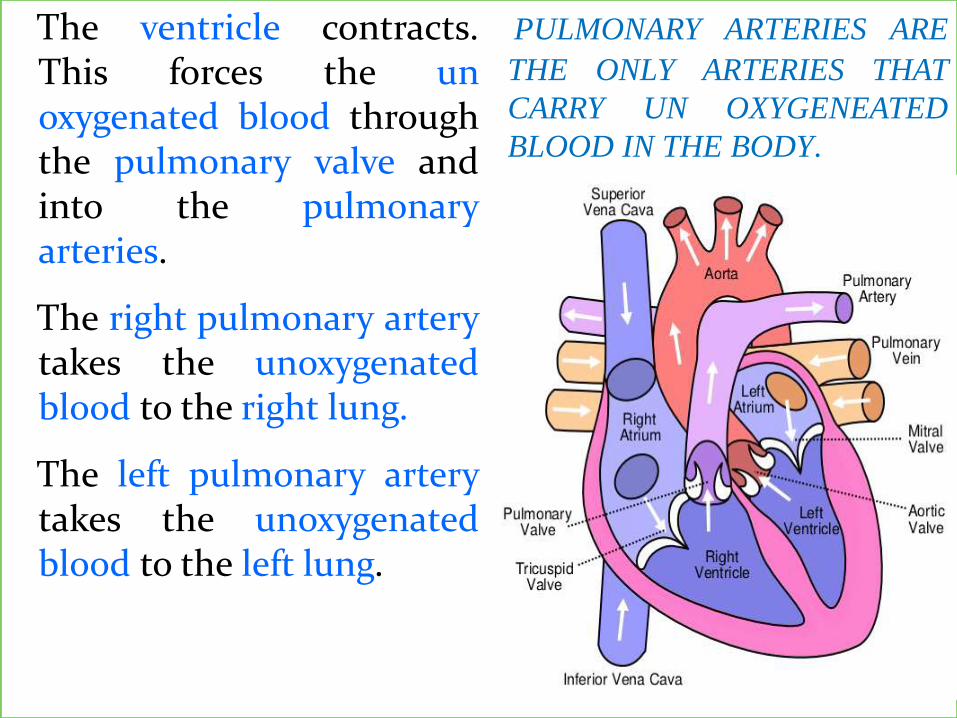
The ventricle contracts.This forces the unoxygenated blood throughthe pulmonary valve andinto the pulmonaryarteries.
The right pulmonary arterytakes the unoxygenatedblood to the right lung.
The left pulmonary arterytakes the unoxygenatedblood to the left lung.
PULMONARY ARTERIES ARE
THE ONLY ARTERIES THAT
CARRY UN OXYGENEATED
BLOOD IN THE BODY.
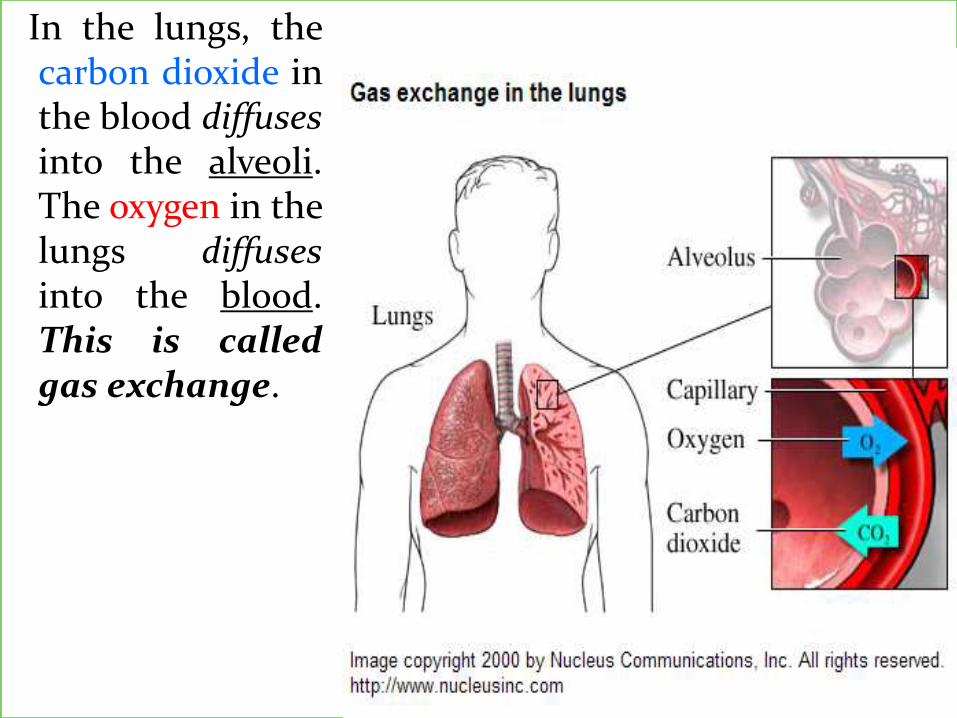
In the lungs, thecarbon dioxide inthe blood diffusesinto the alveoli.The oxygen in thelungs diffusesinto the blood.This is calledgas exchange.

Oxygenatedblood from theright lung returnsto the heartthrough the rightpulmonary veins.Oxygenatedblood from theleft lung returnsto the heartthrough the leftpulmonary veins.
THE PULMONARY VEINS
ARE THE ONLY VEINS THAT
CARRY OXY GENATED
BLOOD.
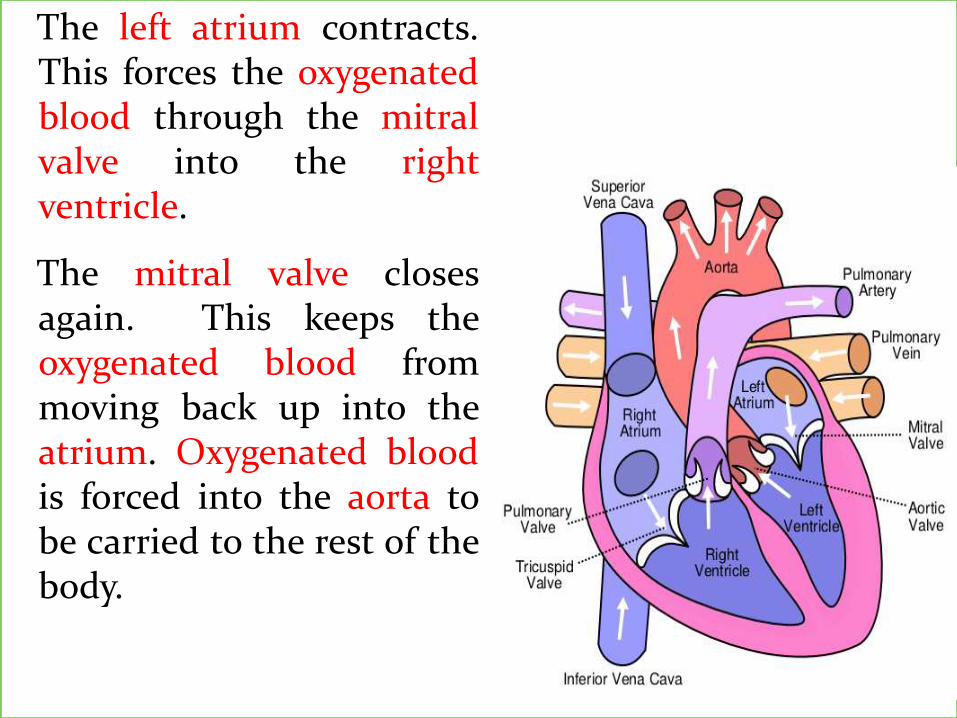
The left atrium contracts.This forces the oxygenatedblood through the mitralvalve into the rightventricle.
The mitral valve closesagain. This keeps theoxygenated blood frommoving back up into theatrium. Oxygenated bloodis forced into the aorta tobe carried to the rest of thebody.

Oxygenated blood iscarried to all body cellswhere oxygen diffuses intothe cells and carbondioxide diffuses into theblood. Blood carryingcarbon dioxide thenreturns to the heart.
And the cycle begins again.

The heart sound
Lub
If you listen to yourheartbeat, it makes alub dub sound.
The lub (S1) is when blood ispushed out of the atria intothe ventricle and the dub(S2) is the reloading of theheart with more blood readyto push it out to the body
Dub
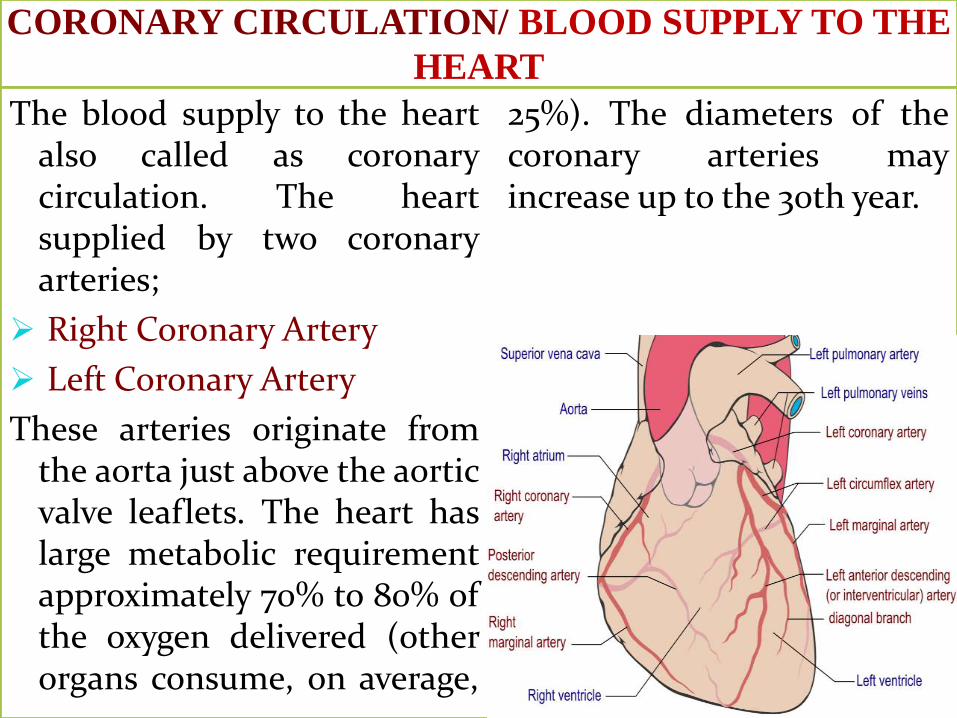
CORONARY CIRCULATION/ BLOOD SUPPLY TO THE
HEART
The blood supply to the heartalso called as coronarycirculation. The heartsupplied by two coronaryarteries;
Right Coronary Artery
Left Coronary Artery
These arteries originate fromthe aorta just above the aorticvalve leaflets. The heart haslarge metabolic requirementapproximately 70% to 80% ofthe oxygen delivered (otherorgans consume, on average,
25%). The diameters of thecoronary arteries mayincrease up to the 30th year.

Rt. Coronary Artery:
The right side of theheart is suppliedby the rightcoronary artery,which progressesaround to thebottom or inferiorwall of the heart.The posterior wallof the heart receiveblood supply by anadditional branchfrom the rightcoronary arterycalled Posterior
Descending Artery(PDA) The bottomsupply continuewith RightMarginal Artery(RMA).
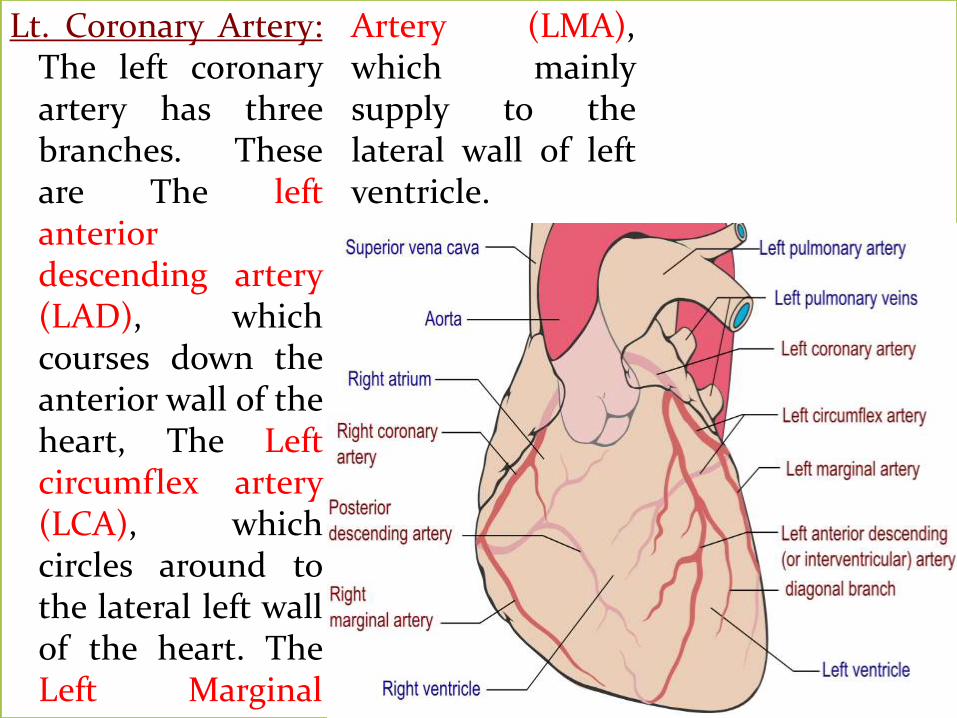
Lt. Coronary Artery:The left coronaryartery has threebranches. Theseare The leftanteriordescending artery(LAD), whichcourses down theanterior wall of theheart, The Leftcircumflex artery(LCA), whichcircles around tothe lateral left wallof the heart. TheLeft Marginal
Artery (LMA),which mainlysupply to thelateral wall of leftventricle.

VENOUS DRAINAGE
Superficial to the coronaryarteries there are thecoronary veins. Venous bloodfrom these veins returns tothe heart primarily throughthe coronary sinus, which islocated posterior in the rightatrium.

FUNCTION OF THE HEART/ CONDUCTION SYSTEM
The specialized heart cells of the cardiac conduction system
generate and coordinate the transmission of electrical impulses to
the myocardial cells. The result is sequential atrioventricular
contraction, which provides for the most effective flow of blood,
thereby optimizing cardiac output. Three physiologic
characteristics of the cardiac conduction cells account for this
coordination:
Automaticity: ability to initiate an electrical impulse
Excitability: ability to respond to an electrical impulse
Conductivity: ability to transmit an electrical impulse from one cell
to another

The conduction system of heart has four elements;
Sinoatrial (SA) Node
Atrioventricular (AV) Node
Bundle of His
Purkinje Fibers


Sinoatrial node (SA Node): The Sinoatrial node (SANode) is the impulse-generating (pacemaker) tissue locatedin the right atrium of the heart. It is a group of cellspositioned on the wall of the right atrium, near the entranceof the superior vena cava. These cells are modified cardiacmyocytes. The SA node has a firing rate of 60 to 100 impulsesper minute, but the rate can change in response to themetabolic demands of the body. The electrical impulsesinitiated by the SA node are conducted along the myocardialcells of the atria via specialized tracts called internodalpathways. The impulses cause electrical stimulation andsubsequent contraction of the atria. The impulses are thenconducted to the atrioventricular (AV) node.
The Atrioventricular (AV) node: located in the right atrialwall near the tricuspid valve) consists of another group ofspecialized muscle cells similar to those of the SA node.

The AV node coordinates the incoming electrical impulsesfrom the atria and, after a slight delay (allowing the atria timeto contract and complete ventricular filling), relays theimpulse to the ventricles. This impulse is then conductedthrough a bundle of specialized conduction cells (bundle ofHis) that travel in the septum separating the left and rightventricles.
The bundle of His: divides into the right bundle branch(conducting impulses to the right ventricle) and the leftbundle branch (conducting impulses to the left ventricle). Totransmit impulses to the largest chamber of the heart, theleft bundle branch bifurcates into the left anterior and leftposterior bundle branches. Impulses travel through thebundle branches to reach the terminal point in theconduction system, called the Purkinje fibers. This is thepoint at which the myocardial cells are stimulated, causingventricular contraction.

PHYSIOLOGY OF CONDUCTION SYSTEM
Cardiac electrical activity is theresult of the movement ofions (charged particles suchas sodium, potassium, andcalcium) across the cellmembrane. The electricalchanges recorded within asingle cell result in what isknown as the cardiac actionpotential.
The normal electricalconduction of the heartallowed by electricalmovements to be transmittedfrom the SA Node through
both atria and forward to theAV Node. Normal physiologyallows further electricalchanges from the AV node tothe Ventricle. Both the SAand AV nodes stimulate theMyocardium. Time orderedstimulation of themyocardium allows efficientcontraction of all fourchambers of the heart.

A myocardial cell has anegative membrane potentialwhen at rest. Stimulationinduces the opening ofvoltage-gated ion channelsand cations into the cell. Thepositively charged ionsentering the cell cause thedepolarization characteristicof an action potential. Afterdepolarization, causesrepolarization to the restingstate.
Signals arising in the SA nodestimulate the atria tocontract. In parallel, action
potentials travel to the AVnode. After a delay, thestimulus is conductedthrough the bundle of His tothe bundle branches andthen to the purkinje fibersand to the ventricularmyocardium.