Asma Murray
36
883 S ECTION I OBSTRUCTIVE DISEASES CHAPTER 38 ASTHMA Njira Lugogo, MD • Loretta G. Que, MD • Daniel Fertel, MD Monica Kraft, MD INTRODUCTION DEFINITION ASTHMA EPIDEMIOLOGY AND RISK FACTORS Introduction Prevalence of Asthma Risk Factors GENETICS OF ASTHMA Overview Linkage Analysis versus Candidate Gene Approaches Genome-Wide Association Studies Future Studies PATHOPHYSIOLOGY OF ASTHMA Etiology of Asthma Cellular Inflammation and Asthma Inflammatory Cytokines and Asthma Biochemical Mediators of Asthma AIRWAY REMODELING IN ASTHMA Introduction Epithelium Epithelial Basal Lamina Extracellular Matrix Airway Smooth Muscle Goblet Cell Hyperplasia and Mucus Hypersecretion Microvascular Changes Physiologic Manifestations of Asthma Effects of Treatment on Remodeling PHYSIOLOGY Introduction Physiology of Airflow Limitation Pulmonary Function Testing Provocative Challenges and Airway Hyperresponsiveness MANAGEMENT OF ASTHMA Introduction Assessment Treatment Additional Management Strategies Management of Acute Asthma Conclusion: Clinician-Patient Partnership INTRODUCTION Asthma is one of the oldest known diseases, but it has only been recognized as a major public health problem since the mid 1970s. The prevalence of asthma has increased dramatically and asthma is now recognized as a major cause of disability, medical expense, and pre- ventable death. Asthma has attracted the full spectrum of biomedical investigation, from studies of the preva- lence of asthmatic symptoms in different populations to studies of the effects of substitution of single base pairs in genes in animal models of allergic sensitization of the airways. These studies continue to refine the scientific understanding of asthma and suggest new approaches to diagnosis and treatment. The scope and depth of these studies present significant challenges in reviewing the topic of asthma. This chapter combines the perspectives of the authors with a “snapshot” of the body of knowl- edge, which is expanding at an explosive pace. DEFINITION Although asthma is a clearly recognized clinical entity, agreement on a precise definition of asthma has proved elusive. Asthma has been more often described than defined. The earliest feature described was the labored, rapid breathing typical of asthmatic attacks, because the word “asthma” is derived from the ancient Greek word for “panting.” As knowledge about asthma has grown, the features described as characteristic of asthma have expanded. Measurement of maximal expiratory flow led to recognition of reversible airflow obstruction as a characteristic feature; measurement of changes in airflow
Transcript of Asma Murray

883
S E C T I O N I
OBSTRUCTIVE DISEASES
C H A P T E R 3 8
ASTHMANjira Lugogo, MD • Loretta G. Que, MD • Daniel Fertel, MD
Monica Kraft, MD
INTRODUCTION
DEFINITION
ASTHMA EPIDEMIOLOGY AND RISK FACTORSIntroductionPrevalence of AsthmaRisk Factors
GENETICS OF ASTHMAOverviewLinkage Analysis versus Candidate Gene
ApproachesGenome-Wide Association StudiesFuture Studies
PATHOPHYSIOLOGY OF ASTHMAEtiology of AsthmaCellular Inflammation and AsthmaInflammatory Cytokines and AsthmaBiochemical Mediators of Asthma
AIRWAY REMODELING IN ASTHMAIntroductionEpithelium
Epithelial Basal LaminaExtracellular MatrixAirway Smooth MuscleGoblet Cell Hyperplasia and Mucus
HypersecretionMicrovascular ChangesPhysiologic Manifestations of AsthmaEffects of Treatment on Remodeling
PHYSIOLOGYIntroductionPhysiology of Airflow LimitationPulmonary Function TestingProvocative Challenges and Airway
Hyperresponsiveness
MANAGEMENT OF ASTHMAIntroductionAssessmentTreatmentAdditional Management StrategiesManagement of Acute AsthmaConclusion: Clinician-Patient Partnership
INTRODUCTION
Asthma is one of the oldest known diseases, but it has only been recognized as a major public health problem since the mid 1970s. The prevalence of asthma has increased dramatically and asthma is now recognized as a major cause of disability, medical expense, and pre-ventable death. Asthma has attracted the full spectrum of biomedical investigation, from studies of the preva-lence of asthmatic symptoms in different populations to studies of the effects of substitution of single base pairs in genes in animal models of allergic sensitization of the airways. These studies continue to refine the scientific understanding of asthma and suggest new approaches to diagnosis and treatment. The scope and depth of these studies present significant challenges in reviewing the topic of asthma. This chapter combines the perspectives
of the authors with a “snapshot” of the body of knowl-edge, which is expanding at an explosive pace.
DEFINITION
Although asthma is a clearly recognized clinical entity, agreement on a precise definition of asthma has proved elusive. Asthma has been more often described than defined. The earliest feature described was the labored, rapid breathing typical of asthmatic attacks, because the word “asthma” is derived from the ancient Greek word for “panting.” As knowledge about asthma has grown, the features described as characteristic of asthma have expanded. Measurement of maximal expiratory flow led to recognition of reversible airflow obstruction as a characteristic feature; measurement of changes in airflow

884 OBSTRUCTIVEDISEASES
after inhalation of chemical or physical irritants led to the definition of bronchial hyperresponsiveness. In addi-tion, studies of bronchial biopsies added a description of characteristic pathologic features. This evolution in the understanding of asthma is summarized in the definition offered in the National Heart, Lung, and Blood Institute’s 2007 Update on Asthma Pathophysiology and Treatment Guidelines.1
Asthma is a chronic inflammatory disorder of the airways in which many cells and cellular elements play a role, including mast cells, eosinophils, T lymphocytes, macrophages, neutrophils, and epithelial cells. In sus-ceptible individuals, inflammation causes recurrent epi-sodes of wheezing, breathlessness, chest tightness, and coughing, particularly at night or in the early morning. These episodes are usually associated with widespread but variable airflow obstruction that is often reversible either spontaneously or with treatment. The inflamma-tion also causes an associated increase in bronchial hyperresponsiveness to a variety of stimuli.
A feature found even more consistently than eosi-nophilia in bronchial biopsies from patients with asthma is thickening of the lamina reticularis immediately under-neath the subepithelial basement membrane, which is considered a hallmark of airway “remodeling,” however this feature has not yet been incorporated into consen-sus definitions of asthma’s features.
The consensus conference “definition” of asthma serves well as a description of the major features of asthma but does not hold up as a precise definition. No feature is unique to asthma, and no feature is universal in patients with the condition. For example, all tests of airway caliber may be normal between attacks, even in patients whose attacks are sudden and severe. Bronchial responsiveness may be normal over most of the year in patients with seasonal asthma, and bronchial hyperre-sponsiveness is often found in people with allergic rhin-itis but without asthma. Even the association between eosinophilic bronchial inflammation and asthma is incon-stant. Some patients with recurrent episodes of wheez-ing and dyspnea associated with reversible airflow obstruction and bronchial hyperresponsiveness have no evidence of eosinophilic inflammation on bronchial biopsies. Other patients have eosinophilic inflammation of the bronchial mucosa and chronic cough responsive to treatment with an inhaled corticosteroid but have neither airflow obstruction nor bronchial hyperrespon-siveness. Finally, some patients with severe asthma have a predominance of neutrophils, rather than eosinophils, in their bronchial mucosa.
The lack of firm, universally agreed-upon criteria for defining asthma complicates epidemiologic studies of the prevalence of asthma in different populations and of changes in prevalence in the same population over time, but agreement on “working definitions” of asthma has led to many informative studies.
Logically, studies of the genetic basis of asthma should be the most affected by lack of precise diagnostic crite-ria, but the approach developed by genetic researchers has refined concepts of the disease. Geneticists recog-nized that asthma is a complex trait, reflecting variations
in many genes and their interactions with the environ-ment, so they examined the genetic determinants of well-defined phenotypes rather than those of clinically defined asthma. This approach has clarified the role of genes as determinants of atopy, bronchial responsive-ness, and responsiveness to treatment, such as β-agonists. The recognition of asthma as a complex, multifactorial disorder has led to a greater focus on the individual and the varied disturbances in function that contribute to a more or less common clinical expression. Recent advances in science have not necessarily led to a more precise definition of asthma; rather, these advances have made the need for agreement on a definition seem less urgent.
ASTHMA EPIDEMIOLOGY AND RISK FACTORS
IntroductionThe epidemiology of asthma is complex and careful epi-demiologic studies are essential to enhancing our under-standing of a disease that affects millions of people worldwide. The challenges faced when studying asthma epidemiology begin with the lack of a universally accepted definition for the disease. Asthma was defined by the American Thoracic Society in 1962 as a disease characterized by increased hyperresponsiveness of the bronchi and trachea to various stimuli, involving wide-spread narrowing of the airways that changes in severity either spontaneously or as a result of therapy.1a,2 In 1975, the World Health Organization (WHO) described asthma as a chronic condition characterized by recurrent bron-chospasm resulting from a tendency to develop reversi-ble narrowing of airway lumina in response to stimuli of a level or intensity not causing such narrowing in normal individuals.2 The emphasis on bronchoconstriction or bronchospasm as the mechanism of asthma is warranted. However, recent advances in research techniques have shown that asthma is a complicated disease that involves both bronchoconstriction and inflammation.
Epidemiologic studies rely on questionnaire assess-ments of asthma symptoms, physician diagnosis of asthma, and use of asthma medications. Unfortunately, highly sensitive and specific physiologic tests to diag-nose asthma are not available. The methacholine chal-lenge test is highly sensitive but not specific. In 1991, the National Institutes of Health (NIH) and National Heart, Lung, and Blood Institute (NHLBI) described asthma as a chronic inflammatory disorder of the airways in which many cells and cellular elements are involved. The chronic inflammation causes an associated increase in airway hyperresponsiveness that leads to recurrent wheezing, breathlessness, chest tightness, and coughing, particularly at night and in the early morning. These episodes are usually associated with widespread but variable airflow obstruction that is often reversible, either spontaneously or with treatment. The NIH updated the asthma diagnosis and treatment guidelines in 2007.3 Current guidelines emphasize the role of inflammation

38 ASTHMA 885
22 countries. The countries covered a wide range of environments including both urban and rural areas. The relationship between atopic sensitization and current wheeze was not significant. However, there was a cor-relation between wheezing and atopy in countries with higher gross national income (typically in the developed world).9 Asthma prevalence rates are higher in affluent countries, an effect that is attributed to differential envi-ronmental exposures in industrialized countries as com-pared with developing countries, in which more people live in rural than in urban areas.10
ISAAC phase III aimed to identify temporal changes in asthma prevalence rates. The prevalence of asthma symptoms increased in Africa, Latin America, and parts of Asia during the observation period, but the overall prevalence of wheezing decreased in English-speaking countries and Western Europe.11
The European Community Respiratory Health Survey (ECRHS)12 was designed to collect data on asthma prev-alence, variation in symptoms, risk factors, and treat-ment patterns in Europe and several centers outside Europe. In 1996, the ECRHS reported a wide variation in the prevalence of asthma symptoms among countries. The lowest prevalence rates occurred in India and Algeria, whereas the highest prevalence rates occurred in the British Isles, New Zealand, Australia, and the United States.13 The increased prevalence of asthma has been substantiated by several large epidemiologic studies.14–18
Death from asthma was previously thought to be very uncommon; however, asthma-related deaths steadily increased in the United States and worldwide between 1980 and the mid-1990s.19–21 There was a sharp rise in asthma-related deaths in Australia and New Zealand in the early 1980s. This increased risk of death was attrib-uted to overuse of the β-agonist fenoterol.22 In 1999, a new diagnostic coding system was initiated, which is thought to have caused the apparent decline in death rates between 1998 and 1999. Although recent death rates have been declining, asthma-related morbidity and mortality continue to be a significant problem. World-wide, approximately 180,000 deaths are attributable to asthma each year, although considerable regional varia-tion exists.18
Approximately 4000 deaths/yr in the United States are attributed to asthma.23 The recent decline in asthma-related deaths is likely related to the increased use of inhaled corticosteroids, improved access to better medical care, and improved recognition and diagnosis of asthma. Disparities exist in asthma-related morbidity and mortality. In the United States, certain populations have a higher burden of asthma-related morbidity and mortality. Deaths from asthma are rare under the age of 18 years. The Morbidity and Mortality Weekly Report (MMWR)23 reported a plateau in asthma related deaths between 2001 and 2003. In 2003, 4055 asthma deaths occurred, suggesting a rate of 1.4/10,000 persons. Higher death rates were noted in persons older than age 65 years and in women (death rate 2.3/10,000 compared with 1.8/10,000 in men).23 Females had a 45% higher risk of dying from asthma than males. Puerto Ricans were the
in asthma and focus on evidence that the patterns and degrees of inflammation are variable, resulting in pheno-typic differences that have important influences on response to therapy.
Prevalence of AsthmaThe prevalence of asthma has been increasing world-wide over the past several decades.4 The etiology of this increase in prevalence is unclear but is likely multifacto-rial. Factors resulting in increased prevalence rates include obesity and exposure to allergens such as house dust mites, mold, and tobacco smoke. Exposure to envi-ronmental triggers results in increased bronchial hyper-responsiveness and asthma. Atopy and allergic rhinitis related to exposure to allergens at an early age likely contribute to the increased incidence of asthma.5 Obesity has also been increasing in prevalence since the mid 1980s.6 Although the available studies cannot address the direction of causality, they indicate that there are impor-tant relationships between environmental and individual factors that warrant further investigation.
In 2006, the National Health Interview Survey (NHIS) estimated that 16.1 million adults (7.3% of the popula-tion) and 6.8 million children (9.4% of the population) in the United States had a diagnosis of asthma.7 The prevalence of asthma in the United States increased from 3.1% in 1980 to 7.7% in 2005. The prevalence of asthma decreases with increasing age. There are important racial differences in the prevalence and morbidity of asthma. In 2005, Puerto Ricans had an asthma prevalence rate 125% higher than non-Hispanic whites and 80% higher than non-Hispanic blacks. Females had a 40% higher prevalence rate than males; however, boys under the age of 18 years old had a higher prevalence than girls.4
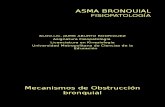
The International Study of Asthma and Allergies in Childhood (ISAAC) was performed between June 1996 and November 1997.5 This is the largest study to docu-ment the worldwide prevalence of asthma. The study involved 91 centers in 56 countries and over 6000 sub-jects. The study enrolled two cohorts of subjects: chil-dren aged 6 to 7 years old and 13 to 14 years old. The prevalence of asthma varied widely between countries, ranging from 2.1% to 4.4% in Albania, China, Greece, and Indonesia to 29.1% to 32.2% in Australia, New Zealand, and the United Kingdom. Lower prevalence rates were seen in Asia, Northern Africa, Eastern Europe, and Eastern Mediterranean areas (Fig. 38-1). The prevalence rates in the younger cohort ranged from an average of 4.1% in India, Indonesia, Iran, and Malaysia to 32.1% in Australia, Brazil, New Zealand, and Panama. The results of the ISAAC study indicate that atopy, allergic rhinoc-onjunctivitis, and atopic eczema are highly correlated with the prevalence and symptoms of asthma. Countries with lower rates of atopy had lower prevalence rates of asthma.
The goal of phase II of the ISAAC study was to further investigate the contribution of atopic sensitization to the large international variation in the prevalence of asthma.8 This was a cross-sectional study of random samples obtained from 8- to 12-year-old children in 30 centers in

886 OBSTRUCTIVEDISEASES
Risk FactorsHygiene Hypothesis
Several large epidemiologic studies have been designed to identify the risk factors that predispose individuals to developing asthma. In 1989, Strachan25 proposed that exposure to infections early in life results in the develop-ment of a predominately T-helper (Th)1-mediated immune response and down-regulation of the Th2-medi-ated response. The lack of exposure to microbes early in life results in an overactive Th2-mediated response
most likely to die of asthma, with a death rate 3.6 times higher than non-Hispanic whites. Non-Hispanic blacks had an asthma death rate twice as high as non-Hispanic whites.24 The disparate rates of death are attributed to variations in severity of disease, socioeconomic factors such as lack of access to quality health care, increased exposure to exacerbating factors in inner city areas, lack of access to medications, and differences in medications prescribed by medical professionals.20 Health care dis-parities contribute to the major differences in outcomes in different populations.
Republic of Ireland
IndonesiaAlbania
RomaniaGeorgiaGreece
ChinaRussiaTaiwan
IndiaEthiopiaMexico
MoroccoSouth Korea
AlgeriaPolandLatvia
PakistanItaly
OmanUzbekistan
PortugalMalaysia
SingaporeChile
SpainNigeriaEstonia
ArgentinaIran
AustriaBelgium
PhilippinesHong Kong
SwedenThailand
JapanFrance
GermanyKenya
LebanonFinland
MaltaSouth Africa
KuwaitPanamaUruguay
ParaguayUSA
BrazilCosta Rica
PeruCanada
AustraliaNew Zealand
UK
0 5 10 15 20 25 30 35 40
Cou
ntry
Prevalence of asthma symptoms (%)
FIGURE 38-1 n Prevalence of asthma symptoms as reported by written questionnaire. (Redrawn from The International Study of Asthma and Allergies in Childhood [ISAAC] Steering Committee. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjuncti-vitis and atopic eczema. ISAAC. Lancet 351:1225–1232, 1998; with permission.)

38 ASTHMA 887
might increase or decrease the incidence of asthma, depending on host factors and the timing, location, and type of microbial exposure.31,32 Using a birth cohort, Ramsey and coworkers found that having physician-diag-nosed croup or having two or more physician-diagnosed ear infections in the first year of life was inversely related to atopy at school age. In contrast, bronchiolitis in the first year of life was associated with increased odds of developing asthma at age 7 years.30
Respiratory syncytial virus (RSV) is the most common cause of bronchiolitis and is associated with an increased risk of developing subsequent wheezing or asthma.31,33–43 Recently, rhinovirus has been recognized as an impor-tant risk factor for the development of asthma. Rhinovi-rus infections are common in childhood and occur in the spring and fall. Rhinovirus is a known cause of bronchi-olitis and is the second most common cause of severe bronchiolitis resulting in hospitalizations. Until recently, little was known about the role of moderately severe outpatient lower respiratory tract infections in the devel-opment of asthma. Jackson and colleagues43 performed nasal sinus lavage, culture, and polymerase chain reac-tion (PCR) for microbial RNA on infants and children with outpatient wheezing illnesses. Viral etiologies were responsible for more than 90% of wheezing illnesses during early childhood. From birth to 3 years of age, wheezing with RSV, rhinovirus, or both resulted in odds ratios of 2.6, 9.8, and 10 for developing asthma by the age of 6 years.43 Other studies also support the increased risk of developing asthma following rhinovirus infec-tions.44 Rhinovirus is a very important predictor of asthma if the infection occurs early in life.
Understanding the mechanism by which viruses modify the risk of developing asthma is an area of intense research. In humans, severe viral infections and bronchi-olitis result in alterations in both Th1 and Th2 cytokine levels. RSV invades the respiratory epithelium through attachment and fusion proteins. Rhinovirus binds intrac-ellular adhesion molecule (ICAM)-1 and low-density lipo-protein receptors (LDLPRs) on the respiratory epithelium and is internalized with subsequent receptor upregula-tion. Downstream effects include the induction of inflam-matory chemokines and cytokines, including type 1 interferon (IFN), interleukin (IL)-12 and IL-18.45,46 Addi-tional factors that mediate the effects of acute viral infec-tions in the airways include neuropeptides, growth factors, and leukotrienes.47,48 The secretion of proinflam-matory cytokines causes airway inflammation, whereas growth factors result in airway remodeling, which may eventually increase the risk of wheezing. Although there is substantial knowledge about the mechanisms by which viruses induce acute airway inflammation, little is known about why these changes produce asthma months or years later. Severe respiratory infections may perma-nently alter the innate immune system, and up-regulation of Th2 cytokines49 acutely may cause irreversible changes in the airway that lead to increased airway hyperrespon-siveness (AHR) and asthma at later times.48
Atypical bacterial pathogens are implicated in trigger-ing acute asthma and propagating chronic asthma and airway inflammation.50 The role of these pathogens in
with increased allergic rhinitis and atopy and an increased risk of developing asthma.25,26 Modern environments are more likely to be hygienic, with smaller families, increased access to antibiotics, and decreased exposure to bacterial pathogens and microbes, leading to imbal-ance between the innate and the adaptive immune mechanisms. This maladaptive system increases the risk of developing allergic diseases such as asthma. The pres-ence of a predominantly allergic, Th2-driven milieu results in defective host defense mechanisms that make the host more susceptible to infection (Fig. 38-2).27 The hygiene hypothesis is supported by data obtained from several subsequent epidemiologic studies involving birth cohorts in the United Kingdom, Europe, and prospective studies worldwide.28,29 This association appears to be stronger in Europe than in other countries.10 For instance, the higher incidence of asthma in the inner city is not explained by this hypothesis. Von Mutius10 concluded that the hygiene hypothesis has led to important discov-eries about the etiology of asthma and the interaction between innate and adaptive immune mechanisms, even though it still lacks a unifying etiology. The practical implications of the hygiene hypothesis have not been fully tested.
Infections
The effect of respiratory infections on the incidence of asthma is incompletely understood. Exposure to microbes early in life may be protective against the development of asthma and allergic rhinitis later in life.25 Respiratory infections, particularly from viral pathogens, are especially common in infancy and childhood. The relationship between infection and the development of atopy and asthma is complex and highly dependent on the type of infection.30 Exposure to respiratory illness
• Presence of older siblings• Early exposure to daycare• Viral infection• Farm environment• Tuberculosis
• Widespread use of antibiotics• Western lifestyle• Urban environment• Diet• Aeroallergens
CD4CD4
Protectiveimmunity
Allergic diseasesincluding asthma
Cytokinebalance
Th1 Th2
FIGURE 38-2 n Determinants of the direction of differentiation of precursor T cells in early life. The concept is that environmental factors in early life can have key influences on the direction of differentiation of precursor T cells. Several factors favor devel-opment of a Th1 phenotype, leading to the absence of allergy and asthma.

888 OBSTRUCTIVEDISEASES
data demonstrate a significant link, important questions still remain.
Obesity
The role of obesity in the development of asthma is a new area of investigation. The obesity epidemic has been increasing for the past several decades and there are no signs that the trend will change in the near future. The recent Centers for Disease Control and Prevention (CDC) NHIS survey reported that 30% of adults over the age of 18 years are obese and about 68% of United States adults are either obese or overweight. The incidence of obesity has almost doubled since 1990.6 The incidence and prevalence of asthma also have increased, and current prevalence data suggest that asthma affects approximately 5% of the U.S. population. Many studies have examined whether the increased prevalence of obesity has resulted in the increasing incidence of asthma. More than 30 cross-sectional and case-control studies of the relationship between obesity and asthma have appeared since the 1990s.67–71 Almost without exception, these studies report an increased prevalence of asthma in obese and overweight individuals throughout the world. Although such studies do not address the direc-tion of causality, several large epidemiologic studies have found that obese individuals have an increased odds ratio or relative risk of developing asthma (defined as a body mass index [BMI] > 30).72,73 Obesity is associated with multiple comorbidities, including hypertension, hyperc-holesterolemia, diabetes mellitus, obstructive sleep apnea, gastroesophageal reflux disease (GERD), and depression.
The biologic basis for the relationship between obesity and asthma has not been established, but several mecha-nisms have been proposed, including common genetic etiologies, comorbidities, effect of obesity on lung mechanics, and the role of inflammatory mediators secreted by adipose tissue (adipokines). Weiss74 sug-gested that obesity and asthma share common etiologies, for example, common effects of fetal programming or common genetics. Obesity may increase the risk of asthma through its effects on other disease processes such as sleep-disordered breathing (SDB) and GERD. The effect of these disease processes on the development of asthma is controversial. In a community-based cohort study of almost 800 children, Sulit and coworkers75 reported that the association between obesity and asthma was strong even after adjusting for SDB. GERD is associ-ated with increased AHR and wheezing76–78 as a result of vagal nerve stimulation by acid refluxing into the distal esophagus and microaspiration of acid into the bronchi.79,80 Treatment of GERD with medications or sur-gical intervention with Nissen fundoplication improves asthma control and decreases bronchial hyperrespon-siveness.81–85 Whereas GERD and SDB may contribute to the development of bronchial hyperresponsiveness and affect asthma control, these diseases do not entirely account for the association between obesity and asthma.
Recently, there has been interest in the role of adipok-ines in the development and perpetuation of asthma.85a
initiating asthma is poorly defined.50 Johnston and Martin50 reported that with few exceptions, the majority of studies support the presence of a relationship between atypical pathogens and chronic stable asthma.50–55 Chlamydophila pneumoniae and Mycoplasma pneu-moniae are present in the airways of chronic asthmatics and are associated with increased airway inflammation and a more severe asthma phenotype.56–58 The interac-tion between pathogens and asthma is not necessarily causative but rather could indicate an increased suscep-tibility to infections associated with atopy and asthma. Further evidence is required to determine the role of infections in the development of asthma.
Atopy
The incidence of asthma in childhood is strongly and independently associated with hay fever and eczema.59–61 ISAAC phase I involved 155 centers in 56 countries and focused on the prevalence of asthma, allergic rhinitis, and atopic eczema in two childhood cohorts. This study found wide variations in the prevalence of asthma between countries and in different regions within coun-tries.5,7 The prevalence rates differed by more than 20-fold between study centers.5,7,26,60 This variability was likely to be explained by environmental or lifestyle factors.
ISAAC phase II was designed to determine the role of environmental and lifestyle factors on the observed dif-ferences in prevalence rates.8 This study included a smaller cohort of children 9 to 11 years old from 30 study centers in 22 countries and added objective measure-ments of atopy including skin examination, skin prick tests, bronchial challenge testing, and specific immu-noglobulin E (IgE) measurements. Study site selection was based on prevalence rates, and sites with high or low prevalence were included in the second phase of the study.8 Logistic regression modeling revealed no sig-nificant correlation between atopy and wheezing in this cohort of children. Subgroup analysis based on per capita income showed an increase in wheezing associ-ated with atopy and allergy in countries with higher gross national income.9 The association between mater-nal or paternal atopy and the occurrence of asthma in children is controversial. Paternal atopy or asthma is not strongly associated with the incidence of asthma in child-hood9; however, maternal AHR is associated with nonat-opic wheezing in children.62 In contrast, several studies show that a family history of atopy is an important risk factor for atopy in children.63,64
The type of allergen and duration of exposure may be important predictors of asthma in childhood and later life. Torrent and associates65,66 demonstrated that a threshold dose of environmental allergen exposure is required to induce sensitization or asthma, whereas no dose-response relationship existed above this threshold. The determinants of whether one develops allergic rhin-itis/atopy, asthma, or both are unclear. The role of early childhood atopy in the development of asthma contin-ues to be an area on ongoing research, and although the

38 ASTHMA 889
increasing evidence that both in utero and childhood exposure to tobacco results in detrimental effects on respiratory health. Studies have demonstrated that in utero and early childhood exposure to tobacco leads to an increased risk of abnormal lung function100,101 and wheezing illnesses in childhood,102–104 an effect that per-sists into adulthood.105 Population-based studies demon-strate that environmental tobacco exposure in childhood also results in an increased risk of asthma.106,107 These effects of tobacco exposure early in life are thought to be mediated by influences on early immune function, specifically alterations in TLR signaling, which result in an increased susceptibility to microbial infections and a decreased ability to activate regulatory pathways that inhibit allergic responses.108 The effect of early tobacco exposure on the development of allergic rhinitis and atopy is controversial; however, there is increasing evi-dence that a strong interaction exists.109 Gene-environ-ment interactions are important mediators of the effects of in utero exposure on the development of asthma.110 Polymorphisms of IL-13111 and β-receptors102 modify the effect of exposure to tobacco smoke on asthma and wheezing in childhood. Tobacco use is also associated with an increased risk of developing asthma.112 Polosa and colleagues113 found that the risk of developing asthma occurs in a dose-response manner in adults with allergic rhinitis. There was an odds ratio of 2.98 (95% confidence interval [CI], 1.81–4.92) of developing asthma in smokers with allergic rhinitis.113 Environmen-tal smoke exposure in adults results in increased morbid-ity and poorer asthma control.
Asthma is a complex disease that is the result of the interaction between genetic predisposition, environ-mental exposures, and responses of the innate and adaptive immune systems. Advances in research have led to the discovery of many possible mechanisms that underlie the development and persistence of asthma. These advances support the conclusion that asthma includes many distinct phenotypes that relate to the underlying pathophysiology and mechanisms of disease. Defining these phenotypes will enhance our ability to tailor therapies and improve outcomes for patients with asthma.
GENETICS OF ASTHMA
OverviewStudies of mono- and dizygotic twins were used initially to estimate the heritability of asthma. These studies showed a higher concordance rate for asthma in monozy-gotic than in dizygotic twins.114 Studies showing an increased prevalence of asthma in first-degree relatives115 lend further support to this hypothesis. Many efforts have been made to study the genetic etiology of asthma in order to better understand its pathogenesis and thereby improve strategies to prevent, diagnose, and treat asthma. Publication of the human genome in 2001 and completion of the International HapMap Project in
One link between obesity and asthma may be the effects of adipokines on airway inflammation. Adipose tissue is metabolically active and participates in energy homeos-tasis. Animal studies of obesity show that adipose tissue secretes biologically active cytokines, including tumor necrosis-α (TNF-α) and IL-6, and adipokines such as leptin, adiponectin, plasminogen activator inhibitor-1 (PAI-1), and resistin.86 Adiponectin, a potent anti-inflam-matory hormone secreted by adipose tissue, is found in low levels in the serum of obese individuals. Adiponectin attenuates allergen-induced airway inflammation and hyperresponsiveness in OVA sensitized and challenged mice.87 In humans, obesity results in systemic inflamma-tion characterized by elevated serum levels of these adi-pokines, chemokines, and acute phase proteins.88 Obesity is associated with increased leptin levels, which may be associated with increased inflammation in the airways of obese asthmatics. Guler and colleagues89 noted that serum leptin was predictive of asthma in boys, even after adjusting for BMI. Other studies reveal higher leptin levels in asthmatic women as compared with normal women; however, adjusting for serum leptin does not affect the association between BMI and asthma.90 The relationship between obesity and asthma does not appear to be mediated via leptin in spite the fact that leptin may be an independent predictor of asthma. The effect of obesity on the development of asthma remains incompletely understood, but these early studies are promising and more work in this area is needed.
Genetics
Genetics play a significant role in the development of asthma and allergic diseases and is discussed in greater detail in the “Genetics of Asthma” section. The interplay between genetic predisposition and environmental exposures underlies the development of asthma. Advances in genomics have led to the discovery of several polymorphisms that are important in the development of asthma91 and the response to therapy. Senthilselvan and associates92 studied a cohort of 915 nonsmoking students and identified an association between Toll-like receptor 4 (TLR4) polymorphisms and atopy in females. TLR4 polymorphisms reduced the odds of having hay fever by 88%.92,93 Conversely, Raby and coworkers94 found no associations between TLR4 polymorphisms and asthma or atopy-related phenotypes. Other polymorphisms of interest in asthma include polymorphisms in IL-4, IL-4 receptor-α, and IL-5 polymorphisms that contribute to susceptibility for bronchial asthma.95–98 The phenotypic and genetic het-erogeneity in asthma poses a challenge to discovering specific genetic mutations that solely increase the risk of asthma.99
Tobacco Use and Environmental Exposure
Exposure to environmental tobacco smoke is common and its role in the development of asthma and abnormal lung function in childhood is controversial. There is

890 OBSTRUCTIVEDISEASES
Furthermore, there is greater statistical power in study-ing case-control associations than in family-based linkage studies.
To test genes associated with a specific biologic hypothesis, candidate gene studies use case-control or family-based designs. Case-control designs compare allele frequencies between subjects with and without asthma. Case-control designs have been criticized because the recruitment of study populations can create differences in allele frequencies between cases and con-trols unrelated to disease status and introduce type I error. The family-based design, conversely, avoids issues of population structure and compares the alleles that parents transmit to children with asthma with alleles parents do not transmit. If an allele increases the risk for asthma, it should be more common among the transmit-ted alleles than the nontransmitted alleles.
More than 100 genes have been associated with asthma phenotypes. However, few reports of associa-tions between asthma and candidate genes have been replicated across studies. In a review of nearly 500 papers on disease association studies, Ober and Hoffjan130 identified 25 genes that are associated with asthma or atopy in six or more populations and 10 genes that have been associated with asthma or atopy in more than 10 studies (IL-4, IL-13, CD14, adrenergic receptor beta 2 [ADRB2], human leukocyte antigen [HLA]-DRB1, HLA-DQB1, TNF, FCER1B, IL-4Ra, and ADAM 33). These genes in general fall into four broad categories: innate immunity (CD14, HLA-DRB1, HLA-DQB1), Th2 cell signaling (IL-4, IL-13, IL-4Ra), cellular inflammation (TNF, FCEDR1B), and lung development (ADAM 33, ADRB2).
Genome-Wide Association StudiesThe completion of the International HapMap Project in 2005 laid the foundation for the next step in investigat-ing genetics in asthma, genome-wide association studies. In genome-wide association studies (GWAS), high-throughput screening of common genetic variations across the genome is used to genotype a single popula-tion. This unbiased approach has the potential to identify novel susceptibility genes and pathways not previously identified with asthma. The first GWAS for asthma was published in 2007131 and revealed an association between a gene on chromosome 17q21 locus and childhood asthma. This finding led to the identification of ORMDL3 as an asthma susceptibility gene. The potential role of this gene in asthma has not yet been defined, and further studies must be performed to determine its effect on susceptibility to asthma. The second GWAS on asthma was reported by Ober and colleagues132 and showed an association between a promoter variant in the chitinase 3-like 1 gene encoding YKL-40 and asthma, AHR, and decreased lung function. GWAS have also identified the 11p14 locus,133 5q23 locus,134 and chromosome 18135 as potential regions harboring asthma susceptibility loci that warrant further investigation.
2005 produced exponential growth in the field, and over 1 million markers of asthma have been identified. However, asthma is very heterogenous and varies not only in the age of onset, degree of severity, and response to therapy but also in the phenotype, which includes nonspecific AHR, atopy, eosinophilia, and mucus hyper-secretion. Moreover, these phenotypes change during life, which further complicates the search to find genetic risk factors for asthma.
Linkage Analysis versus Candidate Gene ApproachesStudies of asthma susceptibility genes have been carried out using two general approaches: linkage analysis and candidate gene association studies. Linkage analysis is a technique used to systematically scan the entire genome of various family members affected by a disease to iden-tify genetic regions associated or “in linkage” with a disease phenotype. Affected family members are hypoth-esized to share certain alleles located in the identified regions more frequently than would be expected by chance alone. Linkage analysis has been successful in identifying diseases in which the disease penetrance follows simple mendelian genetics but is limited because it has less power than association studies to detect weak genetic effects of loci involved in complex diseases that do not follow mendelian genetics.116,117 This approach, originally called “reverse genetics,” also called positional cloning, does not require a prior hypothesis about which genes cause asthma and has been successful in identify-ing candidate genes for asthma.118–121 ADAM 33 was the first gene identified as an asthma susceptibility gene using a positional cloning approach.120 ADAM 33 belongs to a family of proteins that are membrane-anchored met-alloproteases with diverse functions, including the shed-ding of cell-surface proteins. Increased immunostaining of ADAM33 has been found in the lungs of patients with severe asthma as compared with control subjects or those with mild asthma.122
Several studies also have identified linkage between regions of genes and asthma-associated phenotypes, including atopy, AHR, and elevated IgE levels.123–126 These studies have shown that, although asthma, ele-vated IgE, and AHR are genetically determined,127 no single gene controls inheritance of these phenotypes and heritability of the phenotypes is not the same.128,129
In contrast to linkage analysis, candidate gene asso-ciation studies select specific genes based on a biologic theory about their putative role. The gene of interest is chosen because it is believed to influence the expression of a phenotype because of its biologic role or because of its proximity to a region of linkage or association on a specific chromosome. Association studies are thought to be more powerful than linkage studies in detecting alleles that confer modest risk of disease.116 Furthermore, association studies take advantage of the fact that it is easier to recruit large populations of unrelated individu-als than it is to recruit large numbers of family numbers.

38 ASTHMA 891
strate heritability of genetic variations in the two tissues. This approach can be used to determine the effect of disease modifiers on asthma.
GWAS also have the potential to significantly affect medical care in the future by laying the groundwork for personalized medicine. Genetic profiling in subpopula-tions of asthmatics can be used to determine whether genetic polymorphisms predict response to therapy and adverse effects of therapy. The U.S. Food and Drug Administration (FDA) has approved several genetic tests for cytochrome 2D6 and 2C19 variants as part of its efforts to improve patient safety in the treatment of human immunodeficiency virus/acquired immunodefi-ciency syndrome (HIV/AIDS). Pharmacogenetics is also used in the treatment of childhood leukemia; however, tailored therapies for asthma are still under investigation. To date, the most studied genetic variations in asthma are the β2-adrenergic receptor polymorphisms. Three loci at amino acid positions 16, 27, and 164 have been found to significantly alter function.143–145 Genetic asso-ciation studies and linkage analyses in families have further established the importance of these polymor-phisms. Randomized placebo-controlled studies demon-strate that the polymorphism at position 16 may negatively influence response to short acting β2-agonists.146 However, the data with regard to the effect of the polymorphism and response to long-acting β-agonists (LABAs) are controversial147,148 because one small, retrospective study suggested a relationship,149 whereas two other larger retrospective studies did not.147,148 Two prospective, genotype-stratified studies are now in progress that should answer this question.
PATHOPHYSIOLOGY OF ASTHMA
Etiology of AsthmaAsthma is a complex inflammatory disease of the airways that involves many different cells (e.g., neutrophils, basophils, eosinophils, mast cells, macrophages, struc-tural cells) and mediators (e.g., cytokines, chemokines, histamine, leukotrienes, reactive oxygen species, and thromboxanes). The concepts about the pathogenesis of asthma have evolved since the mid 1980s, primarily due to new techniques that have linked various asthma phe-notypes to genotypic patterns. Based on this work, there is a general consensus that airway inflammation and remodeling are critical components of asthma. Further-more, environmental exposures throughout life can modulate the expression of asthma susceptibility genes, making asthma a dynamic disease.
Although asthma is multifactorial in origin, inflamma-tion is believed to be the cornerstone of the disease and is thought to result from inappropriate immune responses to a variety of antigens in genetically susceptible indi-viduals. Evidence from patients with asthma and animal models of bronchial hyperreactivity suggests that recruited CD4 lymphocytes orchestrate and implement immune responses and inflammation that contribute to asthma.
Future StudiesGWAS also have the ability to identify gene-gene interac-tions and gene-environment interactions. Gene-gene interactions identify whether one gene can modify the effect of another in a biologic pathway. Alone the variant has a modest effect; however, when combined with another genetic variant in the signaling pathway, the variant might amplify the impact on the disease.97 By analyzing steps in a pathway, discovery of new genes in an unbiased way can occur.
Gene-environment interactions can be used to study the effect that external factors have on influencing phe-notypic variance. This approach has shown that the influence of susceptibility genes for common diseases, such as asthma, might not become apparent unless the appropriate exposure to the environmental stimulus occurs. Miller and Ho136 listed 20 different reports as identifying specific gene-environment interactions with asthma. As an example, linkage of 5q to bronchial hyper-responsiveness was found in asthmatic children exposed to passive smoking, but not in children from non–smoke-exposed families.137
The future of GWAS also lies in studying the role of epigenetics in the etiology of asthma and the effect of disease modifiers, such as obesity. Epigenetic modifica-tions are defined as a collection of heritable changes in gene expression that do not directly alter DNA sequences. The most common epigenetic modifications of the human genome are DNA methylation and posttransla-tional modification of core histone proteins. DNA meth-ylation involves the covalent addition of a methyl group to a cytosine and usually occurs near CpG sites. Meth-ylation of CpG islands can affect gene expression. Post-translational modification of histones can involve acetylation, methylation, phosphorylation, and ubiquiti-nylation and can alter transcriptional activity. Both of these epigenetic modifications can be heritable and influ-ence gene expression during growth and develop-ment.138 If environmental exposures such as allergens, antibiotics, air pollution, diet, and tobacco exposure can induce epigenetic regulation in vivo, then epigenetics provides an attractive explanation for environmentally regulated alteration of gene expression. Indeed, evi-dence from two large prospective clinical studies indi-cates that prenatal exposure to tobacco smoke is associated with an increased incidence of asthma in young children and adolescents.139,140 Moreover, data also suggest that exposure to tobacco smoke can increase the risk of asthma across generations.141 Determining whether genetic or environmentally triggered epigenetic changes occur in the genome will be important in advancing understanding of the pathogenesis of asthma.
The first study to demonstrate genome-wide linkage and association of gene expression traits in tissues other than lymphoblastoid cell lines was published in 2008.142 Emilsson and associates142 showed that compared with the 10% correlation found in blood, more than 50% of all gene expression traits in adipose tissue correlated strongly with obesity-related traits. They then used genome-wide linkage and association studies to demon-

892 OBSTRUCTIVEDISEASES
factor-β (TGF-β) and their regulatory function is due to a TGF-β–dependent mechanism. TR1 cells are inducible and secrete high levels of IL-10, IFN-γ, and TGF-β but no IL-4 or IL-2.159 These cells do not overexpress FoxP3 and appear to be regulated through different pathways.
Epidemiologic studies demonstrate a higher preva-lence of asthma in industrialized Western societies than in less technologically advanced societies.7 These obser-vations are the essence of the “hygiene hypothesis.”160 The hygiene hypothesis proposes that increased hygiene and lack of exposure to environmental antigens, such as animal allergens, may be affecting the immune system by changing the relative balance of the Th1 and Th2 immunologic profile. Early exposures to various triggers that might occur at an increased frequency in a rural setting can tilt the balance to a Th1 dominant response that is protective against the allergic diathesis promoted by Th2 responses. Therefore, in more urban “cleaner” societies where early childhood exposures are less pro-nounced, a shift toward a Th2 immunologic profile occurs, resulting in a higher incidence of asthma and other allergic diseases.
Eosinophils
Eosinophils are prominent cells in the airways of many patients with asthma. Most asthma phenotypes are asso-ciated with increased numbers of eosinophils in blood, bone marrow, and lung, leading to the hypothesis that the eosinophil is a central effector cell in asthma that contributes to ongoing airway inflammation. The secre-tion of eosinophil peroxidase, leukotrienes, reactive oxygen species/reactive nitrogen species (ROS/RNS) by eosinophils can result in epithelial damage, bronchocon-striction, and mucus hypersecretion. Eosinophils also present antigens and secrete cytokines which can further amplify the Th2 response.161 Indeed, the number of eosi-nophils in bronchoalveolar lavage (BAL) and blood cor-relates with severity of disease in humans with asthma. However, whether the eosinophil is causal in the patho-genesis of asthma or an innocent bystander is still debated. Studies in mice blocking IL-5 either by targeted gene deletion or using anti-IL-5 monoclonal antibodies have produced conflicting results.162,163 Further studies in humans confirm that pharmacologic inhibition of IL-5 can result in eosinophil depletion, but this does not provide significant improvement in airway function or disease symptoms in asthma.164 Two published studies165,166 supported the concept that eosinophils are critical in allergic asthma in mice. In one study, Humbles and coworkers165 deleted the high-affinity GATA-1 binding site on the GATA-1 promoter, the transcription factor required for differentiation of immature myeloid cells, and found that despite eosinophil depletion, there was no effect on AHR and mucus production. In an entirely different approach, Lee and colleagues166 used an eosinophil peroxidase promoter to control transgenic expression of diphtheria toxin A chain, to destroy eosi-nophils, and found that eosinophils were essential for AHR and mucus production. The divergent findings in these two studies are difficult to explain and have been
Cellular Inflammation and AsthmaCD4 Lymphocytes
Four distinct subsets of CD4 lymphocytes, Th1, Th2, regulatory T cells (TReg), and T17 cells can differentiate from precursor T cells at the time of antigen presentation and influence cytokine production. The differentiated Th cells are characterized by the specific sets of cytokines they release when stimulated. For many years, it was believed that asthma and other allergic diseases resulted from an imbalance between Th1 and Th2 responses in favor of a Th2 response, promoting an allergic diathesis based on Th2 cell responses. The identification of tran-scription factors controlling Th1 and Th2 differentiation has provided further support for a predominant role of Th2 cells in the pathogenesis of asthma, because Tbet expression is reduced in the asthmatic lung150 and GATA 3 is overexpressed.151,152 However, recent discoveries and an improved understanding of the interaction between Th17 cells and regulatory T cells have shown that the simple Th1/Th2 hypothesis is not sufficient to explain asthma.
Th1 cells drive cell-mediated immune responses and are characterized by the production of IFN-γ, TNF-α, and IL-2 without production of IL-4, IL-5, IL-9, and IL-13. By contrast, Th2 cells mediate humoral responses and are characterized by their secretion of IL-4, IL-5, IL-9, and IL-13 in the absence of IFN-γ and TNF-α. Antigen recog-nition by naive T cells in the presence of IL-12 favors STAT4 and Tbet activation which promote Th1 cell dif-ferentiation. Early IL-4 production favors STAT6 and GATA3 activation, which lead to Th2 cell production. Th17 cells, a newly discovered subset, produce IL-17 and IL-22.153 These T cells are proinflammatory and have been studied primarily in mice. They express a charac-teristic transcription factor, retinoic acid orphan nuclear receptor (ROR-γ).154 In a murine model of allergic asthma, IL-17 was found to be necessary for the induction of allergic asthma. In healthy human subjects with asthma, IL-17 production increases in peripheral blood after aller-gen challenge. In addition to its proinflammatory role in asthma, Th17 cells also have been detected in other inflammatory autoimmune diseases such as Crohn’s disease, rheumatoid arthritis, and multiple sclerosis and have been shown to be important in host defense against bacterial pathogens.155
In contrast to Th1, Th2, and Th17 cells, TReg cells act directly or indirectly to suppress the function of effector T cell responses in allergic asthma. These cells have cytokine profiles that are distinct from Th1 and Th2 cells and appear to control development of autoimmune disease156 and are able to inhibit development of allergic Th2 responses. Several subsets of TReg cells have been identified, including natural CD4+CD25+TReg cells, Th3 cells, and inducible type 1 TReg (TR1) cells.157 A deficiency in CD4+CD25+TReg cells can result in the development of asthma.158 These cells originate in the thymus, require expression of the transcription factor FoxP3 for the devel-opment of the suppressive function, and do not produce cytokines. Th3 cells produce mainly transforming growth

38 ASTHMA 893
with the increased oxidants in asthma, the antioxidant activity in the lower airways is reduced, providing further indirect support for the importance of oxidants in asthma.183
Reactive Nitrogen Species
In addition to increased ROS, RNS also may be important in the pathogenesis of asthma. It is well-established that the exhaled breath of asthmatics contains higher concen-trations of nitric oxide (NO) than the exhaled breath of normal individuals.184 NO is produced by nitric oxide synthase (NOS). The three known isoforms of NOS are members of a family of different but related NOS pro-teins: neuronal NOS (NOS1), immunologic NOS (NOS2), and endothelial NOS (NOS3). NOS1 and NOS3 are con-stitutively expressed, although they can be regulated.185 NOS2 was originally described in macrophages and is inducible. All NOS isoforms are expressed in the lung.186 Whereas NOS1 is found primarily in the neuronal plexus; NOS3 is ubiquitous and expressed in respiratory epithe-lium, vascular endothelium, and neurons.187 In contrast, the expression of NOS2 is inducible in respiratory epi-thelium and macrophages.187 NO can react with oxygen or ROS to form oxidation products, NO2
−, NO3−, and per-
oxynitrite,188 which can induce tissue damage. The con-centrations of NO are increased in the exhaled breath of asthmatics, and measurements of expired NO can be used to monitor disease189 and titrate inhaled corticoster-oid therapy.190 Exhaled NO is a summation of airway NO formation, superoxide anion metabolism, changes in airway pH, and metabolism of S-nitrosoglutathione (GSNO), an endogenous bronchodilator present in the lung. GSNO is deficient in the airways of children with acute asthmatic respiratory failure. Mice deficient in GSNO-reductase (GSNOR), an enzyme that metabolizes GSNO, develop allergic airway inflammation, but do not develop AHR,191 which suggests that S-nitrosothiols may play a critical role in reducing bronchoconstriction in allergic asthma.
Arginase
Recent evidence indicates that arginine metabolism may also contribute to the development of AHR in allergic asthma. Increased arginase activity in allergic asthma was first described in a guinea pig model whereby administra-tion of an arginase inhibitor, N-hydroxy-nor-L-arginine (NOHA), reduced AHR and restored NO production.192 Arginase expression is also increased in BAL cells, inflam-matory cells, and airway epithelium obtained from bron-chial biopsies of asthmatic subjects.193 Furthermore, genetic polymorphisms in arginase have been identified, supporting a role for arginase in asthma and atopy in children.194
Arachidonic Acid Metabolism
Products of arachidonic acid metabolism are also increased in the exhaled breath of patients with asthma.195 Cysteinyl leukotrienes and other products of the 5-
attributed to background strain variability, controversy about the IL-5 antibody used in the studies, and indirect effects of diphtheria toxin A.167
Inflammatory Cytokines and AsthmaAtopic asthmatics have increased expression of Th2 cytokines in airway biopsies and BAL compared with healthy volunteers.168 Th2 cells regulate allergic inflam-mation via production of IL-3, IL-4, IL-5, IL-9, IL-10, and IL-13. IL-5 has an essential role in regulating eosinophilic inflammation in asthma and subsequent AHR.169 IL-9 appears to augment Th2-driven inflammation and be involved in mast cell release, IgE production, and mucus hypersecretion.170 IL-10 is an anti-inflammatory cytokine and acts to inhibit inflammatory cytokine expression, chemokines, IL-5171 and granulocyte-macrophage colony-stimulating factor (GM-CSF) production172 in asthma.
Although all Th2 cytokines contribute to the patho-genesis of asthma, IL-4 and IL-13 are particularly relevant. IL-4 is critical for the synthesis of IgE and is involved in eosinophil recruitment to the airways.173 Because IL-4 also acts to promote Th2 cell differentiation, it acts at a critical proximal site in the allergic response and is an attractive target for inhibition. This concept is supported by studies in IL-4–deficient mice, which show that IL-4 is essential for the development of allergic symptoms, because allergen-challenged IL-4–deficient mice do not develop an asthma phenotype.174
IL-13 has a similar structure to IL-4 and shares a func-tional receptor, IL-4Rα. A substantial body of evidence supports IL-13 as necessary and sufficient to induce aller-gic asthma.175,176 Acute administration of IL-13 to mice recapitulates many of the features of allergic asthma, including AHR, eosinophilia, mucus hypersecretion,175,176 and subepithelial fibrosis.177 Genetic evidence in humans further supports a role for IL-13 dysregulation in allergic asthma. Polymorphisms in the promoter region and coding regions of the gene are associated with increased risk of developing asthma.178,179
Biochemical Mediators of AsthmaReactive Oxygen Species
Asthma is characterized by altered airway redox chemis-try and increased oxidative stress in the airways.180 Lung inflammatory cells, including eosinophils, macrophages, and neutrophils, are increased in the asthmatic airway and able to release large quantifies of ROS and RNS.181 Furthermore, eosinophils, macrophages, and neutrophils isolated from asthmatics produce increased concentra-tions of ROS compared with normal subjects.182 Mye-loperoxidase and eosinophil peroxidase produced by these granulocytes are increased in BAL and peripheral blood in asthmatics and can produce large amounts of the potent ROS, hydroxyl radical,182 resulting in epithe-lial damage and increased AHR in asthmatic individuals. The observation that lung eosinophils in BAL and blood correlate with AHR in asthma provides further support for a proinflammatory role of ROS in asthma. Concurrent

894 OBSTRUCTIVEDISEASES
ASM cells, have been shown to produce mediators asso-ciated with remodeling in vitro and, to a lesser extent, in vivo.213,214 The precise relationship between remode-ling and inflammation is unclear.
EpitheliumNormal airway epithelium contains ciliated columnar, mucus-secreting goblet, and surfactant-secreting Clara cells that form a highly regulated and impermeable barrier made possible by tight junctions located on the apical surface of the columnar cells.215,216 The airway epithelium is altered in the airways of mild and severe asthmatics, because epithelial changes have been identified in biop-sies of airways of adults and children.217 Although initial pathologic studies in asthma attributed epithelial abnor-malities to bronchoscopy-related injury,218,219 recent studies have revealed that the airway epithelium is abnor-mal both in vitro and in vivo. The finding that damaged asthmatic epithelium is associated with up-regulated epi-dermal growth factor receptors and impaired prolifera-tion suggests a pattern of chronic injury and aberrant repair.220 This is hypothesized to lead to increased epithe-lial permeability due to dysfunction of the airway tight junctions221 and may in part be responsible for the increased susceptibility of asthmatic epithelium to oxidant injury.222
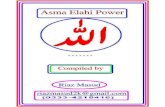
A great deal of evidence suggests that the airway epithelium is a central participant in innate and adap-tive immune responses.223 Disruption of the tight junc-tions allows easy entry of microparticles, allergens, and microbes into the subepithelial space with resultant activation of inflammatory cells, leading to the produc-tion of cytokines and chemokines and propagation of inflammation.215,224 Subsequent production of growth factors is thought to lead to subepithelial fibrosis and airway remodeling. Holgate225 proposed the concept of the epithelial mesenchymal trophic unit (EMTU) (Fig. 38-3), which is analogous to the “soil” that allows the “seed” of Th2 inflammation to persist. The activated EMTU is hypothesized to propagate Th2 inflammation through interactions with resident airway immune cells via proinflammatory mediators derived from the acti-vated structural cells of the EMTU.226 The cytokines produced by immune cells are proposed to feed back to the EMTU, contributing to a cycle of persistent chronic inflammation, with propagation of myofibrob-lasts, proliferation of smooth muscle, and alterations in microvasculature.
Epithelial Basal LaminaA characteristic feature of asthma in adults and children is the hyalinization and thickening of the basal lamina beneath a normal-appearing epithelial basement mem-brane.216 Accompanying this unique change in airway structure is an increased number of myofibroblasts capable of laying down matrix,227 including increased amounts of type III and V collagens, fibronectin, and tenascin.228,229 Asthma is not associated with basement membrane thickening but rather subepithelial fibrosis
lipoxygenase pathway are potent inflammatory media-tors implicated in the pathogenesis of asthma. Elevated concentrations of cysteinyl leukotrienes are produced in the airway of asthmatics196 and have been recovered from the urine of patients with allergen-induced asthma,197 exercise-induced asthma,198 and aspirin-induced asthma.199 Leukotrienes act by binding to receptors on the surface of structural and inflammatory cells. These receptors activate G protein–coupled receptors in the cytoplasm and increase intracellular calcium, resulting in bronchoconstriction and mucus secretion.200 Inhibitors of the 5-lipoxygenase pathway and cysteinyl leukotriene receptor 1 are used to treat asthmatics who remain symptomatic despite using inhaled corticosteroids.
AIRWAY REMODELING IN ASTHMA
IntroductionAirway remodeling is one of the cardinal pathologic fea-tures of chronic asthma and is defined as structural alter-ation of the airway with characteristic changes in the nature, content, and distribution of airway elements.201 The degree of remodeling is a function of disease sever-ity over time, because the degree of structural changes on biopsy and imaging studies correlates with the clini-cal severity of asthma.202–204 The major pathologic changes include increased deposition of subepithelial collagen, airway smooth muscle (ASM) hyperplasia, pro-liferation and hyperplasia of goblet cells and submucosal glands, and microvascular changes.205 These structural changes result in thickening of airway walls and decreased diameter of the airway lumen, which have been observed in pathologic and radiographic studies.206,207 Ultimately, remodeling contributes to the characteristic physiologic changes of asthma discussed previously, including airflow limitation, AHR, and mucus hypersecretion.
The primary hypothesis about the pathogenesis of airway remodeling is that remodeling is caused by exag-gerated airway inflammation in response to environmen-tal stimuli. The experimental support for this hypothesis includes animal data linking allergen-driven Th2 inflam-matory responses with extensive airway remodeling in mice.208,209 For example, overexpression of the Th2 cytokine IL-13 in transgenic mice leads to the character-istic changes of airway remodeling, including increased subepithelial collagen deposition, epithelial hyperpla-sia, enhanced mucus production, and microvascular changes.210 Similarly, in an ovalbumin challenge model of allergic asthma, inhibition of leukotriene formation substantially reduced airway remodeling and reduced the expression of Th2 cytokines.211 Nevertheless, the limited efficacy of anti-inflammatory treatment in pre-venting remodeling suggests that remodeling may not be entirely due to inflammation. Some evidence sug-gests that remodeling may occur independently of the recruitment of inflammatory cells.212 Native airway con-stituents, including epithelial cells, fibroblasts, and

38 ASTHMA 895
Extracellular MatrixExtracellular matrix (ECM) is increased in the airway walls of humans with asthma and is seen in experimental models. In ovalbumin challenge models, airway wall collagen, fibronectin, and proteoglycan deposition are increased.239,240 Loss of elastic fiber content in the small airway adventitial layer has been demonstrated in studies of severe and fatal asthma.241–243 Airway elastin, the matrix component whose degradation is central to emphysema, is also decreased in biopsy specimens from asthmatic patients.244–246 These changes appear to be mediated, at least in part, by exposure to Th2 cytokines. For example, IL-5 exposure increases allergen-induced collagen deposition, whereas allergen-chal-lenged IL-5 knockout mice have decreased collagen deposition.247,248 Mice with a knockout of Tbet, a Th1-specific transcription factor, have profound defects in the production of Th1 cytokines and increased produc-tion of Th2 cytokines. As a result, the mice develop a remodeled asthmatic phenotype, with high levels of Th2 cytokines and increased subepithelial collagen deposi-tion. The central role of IL-13 is illustrated by the amel-ioration of airway remodeling that occurs when IL-13 is neutralized.249
with deposition of collagen beneath the basement membrane.230 These changes have been reported in early asthma close to the beginning of the disease, suggesting that the changes in matrix deposition are not the result of chronic inflammation.216,225,231,232 Both the Tucson Children’s Respiratory Study and the Childhood Asthma Management Program demonstrated that reduced lung function can occur early in life and is unabated by conventional therapies.233,234 The mechanisms involved in remodeling of the basal lamina are unknown. However, murine models of asthma have suggested roles for plate-let-derived growth factor (PDGF), TGF-β, and IL-13.235 TGF-β promotes the differentiation of fibroblasts into myofibroblasts, which form collagen and secrete growth factors.236 In humans, PDGF has been implicated in airway remodeling by inducing airway fibroblasts to produce collagen and increase matrix formation. The PDGF-BB isoform enhances fibroblast procollagen I formation in subjects with severe asthma as compared to those with mild to moderate asthma.237,238 Additionally, PDGF and TGF-β have been shown to modulate expression of matrix metalloproteinases and regulation of migratory function of human airway smooth muscle cells.238a Further research is required to determine the mechanisms of airway fibrosis and to guide more specific therapy in asthma.
Dendritic cell
Mucus
Initiation
(Myo) fibroblasts Amplification
Propagation
Smooth muscle
Blood vessels
Environmental agentsInflammatory cell products
Th-2 and Th1cytokines
Chemoattractants eg IL-8,proinflammatory mediators
THE EPITHELIAL-MESENCHYMAL TROPHIC UNITIN ASTHMA
Th-2 cell
Neutrophil
EosinophilMast cell
TNF
IL-3,IL-5
GM-CSF
IL-9,IL-3, IL-4
FIGURE 38-3 n Schematic representation of the interaction between immune, inflammatory, and structural cells through the epithelial-mesenchymal trophic unit (EMTU) in the pathogenesis of asthma. (Adapted from Holgate ST: The airway epithelium is central to the pathogenesis of asthma. Allergol Int 57:1–10, 2008.)

896 OBSTRUCTIVEDISEASES
diameter associated with more severe asthma.259 Taken together, it seems likely that both hypertrophy and hyperplasia contribute to the increased smooth muscle mass characteristically seen in remodeled airways of patients with asthma.
Asthmatic ASM may be phenotypically different from ASM in nonasthmatic airways, with altered proliferative or contractile capacities. Smooth muscle cells exhibit phenotypic plasticity in vitro, with the ability to switch between a hyperproliferative and a hyperfunctional phe-notype, depending on culture conditions. This phenom-enon could theoretically explain the variable presence of both ASM hyperplasia and hypertrophy in asthma. To date, gene expression studies addressing this possibility are intriguing but inconclusive.266
In addition to alterations in quantity and function, asthmatic ASM appears to have an altered anatomic rela-tionship with inflammatory cells. Data demonstrate that smooth airway infiltration by mast cells is an important feature of asthmatic airway remodeling.267 Notably, this colocalization of mast cells and ASM is present in a cross section of asthma phenotypes and degrees of severity.268 Several mast cell products have the potential to adversely affect the growth and function of smooth muscle, and their localization in the smooth muscle may facilitate this interaction. For example, the mast cell–derived media-tors histamine, prostaglandin D2, and the cysteinyl leu-kotrienes are potent constrictors of airway smooth muscle.269 Human ASM promotes human lung mast cell (HLMC) survival in vitro, induces rapid HLMC prolifera-tion, and enhances constitutive HLMC degranulation, suggesting a smooth muscle–driven allergen-independ-ent mechanism of chronic mast cell activation.270
Goblet Cell Hyperplasia and Mucus HypersecretionGoblet cell hyperplasia is a hallmark of the pathology of asthma in mild, moderate, and severe disease. Mucin is secreted by goblet cells in the airway epithelium and mucus glands in the submucosal space. Airway mucus is a viscoelastic gel composed of cells, secreted polypep-tides, and cellular debris, which forms a thin film lining the airway surface.271 Under normal circumstances, airway mucus serves a protective function, trapping foreign debris, bacteria, and viruses, then working in concert with the ciliated epithelium to clear captured material. In asthma, excessive production of mucus con-tributes to airway obstruction. Secreted mucin levels in induced sputum are higher in patients with lower forced expiratory volume in 1 second (FEV1) values, indicating that mucus hypersecretion plays an important role in airway obstruction in asthma.272 Accumulation of intra-luminal mucus plays a significant role in fatal or near-fatal asthma, and widespread occlusion of airways by mucus is a common finding in autopsy studies of fatal asthma.273,274 Mucin is the major protein component of these plugs, which is a high-molecular-weight glycopro-tein produced by goblet cells in the epithelium and glands in the submucosa.275,276 Secreted and oligimerized
TGF-β, derived from eosinophils, macrophages, and other cells, is also strongly implicated in ECM remodel-ing. Mice treated with anti-TGF-β antibody have decreased ECM deposition,250 whereas treatment of asthmatics with anti-IL-5 antibody decreases ECM deposition and reduces BAL concentrations of TGF-β.251 In addition, the gene for TGF-β is up-regulated in allergen-challenged mice252 and Tbet/IFN-γ–deficient mice have elevated levels of TGF-β.249
Changes in the ECM appear to correspond with phys-iologic changes seen in asthma.253 Increased submucosal matrix protein deposition, in addition to contributing to luminal narrowing, changes the mechanical properties of the airway wall. Stiffening of the airway wall reduces forces exerted on lung parenchyma, leading to reduced distensibility. There are also data to suggest loss of elastic recoil in asthma, and early data suggest that loss of elastin may play a role.241,246,254
Airway Smooth MuscleAirway smooth muscle (ASM) mass is increased in humans with asthma and experimental animal models. The increased smooth muscle mass in airway walls con-tributes to airway luminal narrowing by occupying space and increasing the extent of narrowing for each degree of smooth muscle contraction.255,256 In animal models, increased ASM mass accounts for a significant percent-age of AHR257 and correlates with methacholine sensitiv-ity.258 In pathologic studies, increased ASM mass in large airways is linked with both severe and fatal asthma.259,260
In addition to the effects of increased smooth muscle mass on airway physiology, ASM cells have been shown to play a central role in the molecular events that initiate and propagate airway remodeling. The relationship of smooth muscle to the ECM is complex, with smooth muscle cells elaborating matrix proteins, as well as matrix metalloproteinases (MMPs) and their tissue inhib-itors (TIMPs), possibly via signaling between the ECM and cell surface receptors.261 Proof of this relationship comes from the ability of ASM cells to secrete ECM pro-teins in response to asthmatic sera, suggesting autocrine regulation of airway remodeling.262 Furthermore, ASM obtained from asthmatic airways secretes more ECM protein than nonasthmatic ASM and ECM from asthmat-ics induces a greater degree of cell proliferation.262
The relative contributions of smooth muscle hyper-trophy versus hyperplasia in increasing smooth muscle mass is not clear. Data from a Norway rat ovalbumin-challenge model shows that increases in ASM mass are associated with increased DNA synthesis, suggesting smooth muscle hyperplasia.263 More recent human biopsy data demonstrate that muscle mass increases along with the number of nuclei, providing additional support for the role of hyperplasia in smooth muscle remodeling.264 However, a second ovalbumin-challenge model showed increased muscle mass without a con-comitant increase in the number of smooth muscle cell nuclei.265 Furthermore, human biopsy studies support hypertrophy as the cause of increased smooth muscle mass in asthma, with greater smooth muscle cellular

38 ASTHMA 897
Physiologic Manifestations of AsthmaAirway Hyperresponsiveness
AHR is a characteristic feature of asthma. Hyperrespon-siveness can occur in response to a number of nonspe-cific environmental irritants, pharmacologic agonists, and inflammatory mediators. In the past, the predomi-nant view was that airway inflammation was the mecha-nism causing AHR. This concept has been criticized, because a number of studies have shown dissociation between AHR and inflammation,191,293 highlighting the fact that inflammation alone is insufficient as a mecha-nism of disease. Evidence suggests that a number of inflammatory Th2 cytokines, CD4 cells, and biochemical mediators contribute to the development of AHR in asthma. Exposure to Th2 cytokines in asthmatic airways can increase the isometric constrictor response of ASM by increasing calcium release from intracellular stores.294,295 In addition to the airway inflammation, factors contributing to mechanical airway obstruction have also been implicated in the pathogenesis of AHR, including epithelial permeability, smooth muscle hyper-trophy, mucus hypersecretion, and airway remodeling.
Epithelial Permeability
The airway epithelium is the source of many of the cytokines and inflammatory mediators contributing to airway inflammation and increased AHR in asthma. The airway epithelium serves several different functions within the lung. The airway epithelium is in a unique position, because it is exposed to the environment and is the primary target of viruses and inhaled agents known to cause or exacerbate asthma. In addition to barrier protection and mucociliary clearance of unwanted path-ogens, the epithelium can regulate the response of other lung cells involved in the inflammatory and fibrotic response of the lung to external stimuli.
In asthma, there is evidence that airway epithelial barrier function is impaired and epithelial tight junctions are disrupted. These cells show reduced transepithelial resistance indicating epithelial permeability, which is associated with AHR. Confocal microscopy with antibod-ies directed at adapter proteins (ZO-1) and tight junction proteins (occludin) support the concept that tight junc-tions are poorly developed in asthmatic epithelium. In addition to disruption of the tight junctions, epithelial desquamation has been described as a pathologic feature in patients with asthma who die from acute respiratory failure.296 Furthermore, markers of apoptosis indicating programmed cell death have also been noted in airway tissue of subjects with asthma and correlate with disease severity and chronicity.222
Smooth Muscle Hypercontractility
Hypercontractility of ASM is believed to be a key deter-minant of the development of AHR in asthma. It is still unclear whether contractile force is enhanced in the asthmatic airway, where inflammatory mediators accu-
mucins have an important role in determining the prop-erties of the extracellular mucus layer.
In patients with asthma, the number of mucus-secret-ing goblet and submucosal cells in the airway is increased compared with that in normal individuals.277 Although 19 human mucin genes (MUC) have been described, the major secreted mucus proteins include the gene prod-ucts MUC5AC and MUC5B. MUC5AC is the predominant gel-forming mucin and is disproportionately increased in asthma.278 In addition to quantitative differences in mucus gene products in asthma, asthmatic mucus may be functionally different. The increased viscosity seen in asthmatic mucus may be accounted for by variations in oligimerization and by incomplete release of mucins from goblet cells.279 The latter may lead to “tethering” of luminal mucins to the airway epithelium and increased adherence of mucus to airway walls.280
The increase in mucus production seen in asthma may be attributed to increased mucin production, increased exocytosis of previously formed mucus from airway cells, or both. The migration of mucus from preformed granules to the apical surface of epithelial cells is depend-ent on the presence of myristolated alanine-rich C kinase substrate (MARCKS protein), and activation of the MARCKS protein requires phosphorylation by protein kinase C.281 The strength of this relationship is bolstered by the observation that protein kinase C is up-regulated together with mucin production after stimulation of airway epithelial cells with neutrophil elastase.282 Binding of mycoplasma to TLR and subsequent expression of Th2 cytokines has also been shown to lead to increased mucus production in a murine model of asthma, possibly mediated by a nuclear factor-κB (NF-κB) binding site on the MUC5AC promoter.283 However, TLR2 knockout mice have increased mucus production, possibly due to decreased levels of IFN-γ and subsequently increased TGF-β levels.284
Microvascular ChangesBronchial neovascularization is a recognized feature of airway remodeling, with dilated and tortuous mucosal blood vessels present even in mild asthma.285 Function-ally, the airway microvasculature is more permeable, with leakage of plasma proteins into the extravascular space associated with mucosal edema.286 Mucosal edema results in airway narrowing, which may have a pro-nounced effect on airway function.286
Vascular endothelial growth factor (VEGF) appears to be a key mediator of the pathogenesis of airway vascular abnormalities in asthma. VEGF levels are increased in the asthmatic airway,287 with levels of VEGF staining corre-sponding to increasing bronchial vascularity.288 A number of different stimuli for VEGF expression are present in asthma. Th2 cytokine exposure prompts the release of VEGF from ASM cells,289,290 as does increased mechanical strain as seen in symptomatic airway obstruction.291 Trans-genic induction of VEGF in murine airway epithelial cells leads to increased pulmonary angiogenesis and increased expression of Th2 cytokines, suggesting the presence of a feedback loop increasing vascular remodeling.292

898 OBSTRUCTIVEDISEASES
toms suggest new therapeutic avenues targeting the underlying pathogenesis of airway remodeling in asthma.130
PHYSIOLOGY
IntroductionAs understanding of the pathogenesis of asthma improves and strategies for treatment evolve, it is important to recognize that the link between the pathophysiology and the treatment of asthma is functional, involving var-iable limitation of air flow. These two cardinal manifesta-tions of asthma, variability of symptoms in response to environmental factors and limitation of air flow, are crucial to making the diagnosis of asthma and distin-guishing asthma from other obstructive lung diseases.
Physiology of Airflow LimitationDuring asthma exacerbations, diffuse narrowing of the airways results in profound physiologic consequences. This narrowing has been thought to occur disproportion-ately in the small bronchi,307 although recent studies suggest a prominent role for large and medium airways.308 As a result, lung function tests are abnormal, with an increase in airway resistance and a decline in maximal expiratory flow. Airway narrowing also prevents the lungs from completely emptying (“air trapping”) due to resistance to expiratory flow and to bronchial closure at higher than normal lung volumes. The breath-to-breath variability of asthmatic obstruction and air trapping led to the concept of dynamic hyperinflation.309 As a result of dynamic hyperinflation, asthmatics breathe at higher total lung volumes, detectable as increased residual volume.310 Despite elevated total lung volumes, asthmat-ics typically have reduced tidal ventilation. Decreasing forced vital capacity (FVC) suggests worsening air trap-ping, whereas worsening of the FEV1/FVC ratio indicates increasing airway narrowing.311
At high lung volumes, flow limitation due to bronchial narrowing is offset by increased circumferential traction on the bronchial airways due to “tethering” of airways to inflated alveoli.312 This response may be less effective in asthma, because the altered mechanical properties of the ECM in asthmatic airways reduce the mechanical forces opposing ASM contraction.313 The net effect is that the work of breathing increases significantly, due in part to decreased lung and chest wall compliance at higher thoracic volumes and in part to the greater effort required to overcome the resistance of narrowed airways. The diaphragm and intercostal muscles are overloaded due to thoracic hyperinflation and mechanically disad-vantaged due to suboptimal positioning on their length-tension curves.314 As a result, accessory muscles of respiration, including the abdominal muscles and sterno-cleidomastoids, are required.315 A large proportion of the subjective dyspnea associated with asthma exacer-bations has been attributed to respiratory muscle fatigue.316
mulate, or whether smooth muscle is abnormal in asthma. Numerous reports have identified increased ASM mass in fatal and nonfatal asthma. The cellular mechanism of increased ASM mass in asthma represents a balance between smooth muscle hypertrophy and pro-liferation.297 Benayoun and associates259 found that patients with mild asthma had larger smooth muscle cell diameter in their airways than control subjects. The increase in ASM mass correlated with asthma severity, suggesting a causal role for smooth muscle hypertrophy in the development of AHR. Conversely, Woodruff and colleagues264 found that hyperplasia of smooth muscle occurs in mild to moderate asthma without changes in cell size or gene expression.
Excessive shortening of ASM also can result in exces-sive narrowing of the airways, and several different mechanisms have been proposed. One proposal sug-gests that exposure to chronic inflammatory mediators in the local asthmatic environment results in chronic shortening of ASM, so that further shortening occurs during activation.298 A second proposal suggests that the ECM surrounding ASM alters the ASM phenotype by increasing ASM mass and decreasing its secretory proper-ties.299 A third scenario suggests that abnormal relaxation of ASM occurs in asthma, which can contribute to increased bronchospasm,300 whereas a fourth scenario suggests that there is a change in the interdependence between the airway wall and the surrounding lung.300,300a
Effects of Treatment on RemodelingBecause of the importance of airway remodeling in the pathogenesis of asthma, efforts have been devoted to reversing airway remodeling. One hypothesis is that treatment of the inflammatory component of asthma may lessen airway remodeling. In a murine model of asthma, administration of corticosteroids in combination with allergen avoidance reduced airway fibrosis and smooth muscle mass.301 In another study comparing a leukotriene antagonist and a corticosteroid in an allergy-driven mouse model of asthma, the leukotriene inhibitor decreased ASM mass and subepithelial collagen deposition, whereas corticosteroids had no effect on remodeling.302
An alternative approach is to mechanically reduce smooth muscle mass in order to improve physiologic function. The application of controlled thermal energy via a radiofrequency catheter in order to reduce smooth muscle mass has been shown to reduce methacholine responsiveness in dogs.303 Early clinical trials in human subjects have shown beneficial effects on asthma symp-toms via reduction in smooth muscle mass, with results that were sustained for 1 year.304
With an increased understanding of the molecular mechanisms of asthma pathophysiology and airway remodeling, more focused therapeutic strategies can be explored.304a In vitro studies of compounds targeting putative mediators involved in remodeling suggest a promising role for novel agents in the treatment of asthma.253,305,306 Recent studies highlighting novel genes associated with airway remodeling and asthmatic symp-

38 ASTHMA 899
compared with an individual patient’s baseline measure-ment obtained when asymptomatic and well-control-led.327,328 Evaluation of peak flow measurements obtained during a trial of long- versus short-acting β-agonists suggests that individual peak flow is highly variable and that the variability in PEF has a greater predictive value for asthma exacerbations than the absolute PEF measurement.329,330
Spirometry
The best and most standardized test of airflow obstruc-tion is the FEV1. The FEV1 has the advantage of being an objective, non–patient-reported measurement of lung function. Improvement in FEV1 of more than 12% and 200 mL after bronchodilator treatment indicates revers-ible airflow obstruction and is suggestive, but not diag-nostic, of asthma.331 Prebronchodilator FEV1 is a strong predictor of decline in asthma control whereas postbron-chodilator FEV1 is a marker of future risk.332,333 However, accurate measurement requires stopping LABAs for at least 12 hours and short-acting bronchodilators for at least 6 hours. Furthermore, because the FEV1 may be normal or near-normal between asthma flares, it is a poor marker of response to bronchodilators in mild asthma. The absolute value of the FEV1 is dependent on FVC and also reflects the small airways. Interpretation of FEV1 therefore requires simultaneous FVC measurement. In asthma, the relative reduction in FEV1 is typically greater than the reduction in the FVC. As a result, the FEV1/FVC ratio in asthma is usually less than 70%. A characteristic flow-volume loop is created with scoop-ing of the expiratory loop consistent with airflow limita-tion (Fig. 38-4). However, in severe asthma, this ratio may actually increase as profound air trapping increases residual volume and reduces the FVC. This reversible restriction due to air trapping has been reported in asthma.311,334
The performance of the forced expiratory maneuver requires inhalation to total lung capacity prior to exhala-tion. In normal patients, the resultant stretch of intrapul-monary airways causes reflex bronchodilation and a shift
The airway obstruction and closure in asthma is non-uniform, with significant regional variability that may not be completely reflected by decreases in peak flow.317,318 Although pulmonary blood flow is reduced in areas of alveolar hypoventilation, the magnitude of this response in insufficient to offset more than moderate or severe airflow obstruction. Ventilation-perfusion mismatching leads to a widened alveolar-arterial oxygen difference that tracks with increasing asthma severity; the arterial oxygen tension in acute severe asthma typically falls below 70 mm Hg.319,320 Arterial carbon dioxide tension initially falls as alveolar ventilation increases, because CO2 elimination is less impaired than O2 uptake by ven-tilation-perfusion mismatching.321 As respiratory muscles fatigue, carbon dioxide tension increases, so that a normal or elevated PCO2 during an asthma exacerbation suggests impending respiratory failure.322 Worsening of airflow obstruction or any factor that decreases respira-tory drive (such as sedation) can drop alveolar ventila-tion precipitously; the resultant rise in PCO2 further inhibits respiratory drive and muscle performance and hastens respiratory failure.323
Pulmonary Function TestingEven between asthma exacerbations, pulmonary func-tion testing shows characteristic changes reflecting the reduced flow and air trapping of dynamic hyperinflation. Decreased expiratory flow can be easily and reproduci-bly detected with a peak flowmeter in ambulatory patients, and peak expiratory flow (PEF) measurement is an accepted method to correlate physiologic function with the clinical severity of asthma. However, peak flow measurements are not standardized and cannot be cor-related with other measures of lung function.324 PEF as a percentage of the predicted value is 10% higher than FEV1 on average, with a great deal of variability between measurements.325 PEF measurements tend to underesti-mate less severe obstruction and overestimate more severe obstruction.326 Currently, the recommended use of PEF measurement is for the daily monitoring of ambu-latory patients. In this situation, the values should be
Lung volume (L)
Flo
w r
ate
(L/s
ec)
A B C
FIGURE 38-4 n Flow-volume loops in asthma. A, The typical scooped appearance of the flow-volume loop in asthma is shown as the solid blue line. The predicted normal flow-volume loop is shown by the dashed line. B, The scooped appearance of the initial flow-volume loop (blue line) may show complete reversal following use of a bronchodilator (brown line). C, In some cases, the reversal of the scooped appearance following use of a bronchodilator is incomplete (brown line). (A-C, Adapted from Sameer KM: Asthma: Diagnosis and management. Med Clin North Am 90:39–60, 2006.)

900 OBSTRUCTIVEDISEASES
pected finding of an increase in diffusing capacity should raise the possibility of undiagnosed asthma, whereas decreased diffusing capacity in a suspected asthmatic is suggestive of an alternate diagnosis or coexisting condition.347
Provocative Challenges and Airway HyperresponsivenessAHR to environmental stimuli is a hallmark of asthma. Patients suspected of having asthma despite normal lung function testing usually develop bronchoconstric-tion in response to a provocative stimulus. Direct stim-ulation, during which a substance known to induce bronchoconstriction via direct action on smooth muscle is inhaled into the airways, is the most widely used method of assessing bronchial hyperresponsiveness. Nebulized methacholine, delivered in doubling con-centrations until FEV1 falls by more than 20%, is the most commonly used agent. The concentration that causes a 20% fall is labeled the PC20 (provocative concentra-tion resulting in 20% fall in the FEV1) and can be used to measure the degree of AHR. A PC20 less than 16 mg/mL is consistent with mild AHR, less than 4 mg/mL is consistent with moderate AHR, and less than 1 mg/mL with severe AHR,348 with lower PC20 levels generally corresponding to more severe asthma.349 Bronchial hyperresponsiveness also has been associated with increased risk of developing persistent asthma and airway remodeling.350
Indirect stimuli, such as cold air exposure, exercise, inhalation of hypertonic saline, mannitol, and adenosine monophosphate, may also induce bronchoconstriction. Rather than working directly on smooth muscle, indirect stimuli cause the release of inflammatory mediators from airway cells that then interact with ASM to induce bron-choconstriction. Although the dose response is more difficult to assess with indirect stimuli, the results have direct applicability to daily asthma symptoms. For example, direct challenge of athletes suspected of having exercise-induced bronchospasm is less likely to uncover bronchospasm than indirect challenge using a surrogate for physical activity.351 There also may be differences between direct and indirect stimuli in the evaluation of response to treatment, with indirect challenge providing a better idea about response to therapy.352
MANAGEMENT OF ASTHMA
IntroductionThe inherent complexities in evaluating and treating asthma are evident from studies in the 1970s and 1980s documenting a significant number of asthma deaths that were attributable to failure of clinicians to recognize the clinical severity of asthma, leading to inadequate management. For example, a study of asthma deaths in the West Midland and Mersey regions of England in 1979 led to the conclusion that failure to recognize the
in the pressure-volume curve. This alteration in lung mechanics is generally attributed to a transient decrease in ASM tone.335 However, some asthmatics have the opposite response, developing bronchoconstriction during deep inspiration. The mechanism of this “spirom-etry-induced bronchoconstriction” is unknown, but some evidence suggests that it may be partly due to increased inflammation and remodeling of asthmatic airways.336
An alternative method for assessing airflow obstruc-tion is to evaluate midexpiratory flow, measured between 25% and 75% of the FVC (FEF25%–75%). Obtained at lower lung volumes, reductions in the FEF25%–75% may be more sensitive for identifying obstruction in small airways.337 Studies in patients at high risk for asthma based on atopic symptoms have shown that this index is valuable in pre-dicting AHR.338 Similarly, in childhood asthmatics who have become asymptomatic, the FEF25%–75% is a sensitive marker of residual physiologic abnormalities.339 The clin-ical utility of the FEF25%–75% is limited by the lack of acceptable standardized values. High numbers of false-positive and false-negative results occur when 80% of predicted FEF25%–75% is used for classification.340
The limitations of the FEF25%–75% are in part due to large variation in the duration of FVC maneuvers. To address this issue, measurement of the forced expiratory volume over the first 6 seconds (FEV6) has been proposed as an alternative to the FVC. The advantages of this maneuver over the FVC include ease of measurement, a more explicit end-of-test definition, and reduced risk of syncope.341 Data are available suggesting parameters that may be used for disease classification, although the sen-sitivity and specificity of the FEV1/FEV6 in comparison to the FEV1/FVC ratio remain controversial.342,343
Lung Volumes and Diffusing Capacity
As a result of dynamic hyperinflation and consequent air trapping, residual volume, functional residual capacity, and total lung capacity may be elevated in asthma. Exhaled gas dilution measures only the communicating volume of gas and may underestimate these volumes due to regional heterogeneity in the distribution of ventilation.344 For this reason, body plethysmography is often considered the method of choice for lung volume evaluation in severe asthma. However, because plethysmography measures the total volume of compressible gas within the thorax and abdomen, the inclusion of intra-abdominal gas may lead to overestimation of total lung capacity, particularly in severely obstructed asthmatics.345
Single-breath diffusing capacity is a marker of carbon monoxide gas transfer in the lungs and is reduced in most chronic lung diseases because of altered alveolar capillary surface area and/or maldistribution of inspired gas due to airflow obstruction. In asthma, the diffusing capacity is normal or elevated if airflow obstruction is not severe, and this can be useful in distinguishing asthma from other obstructive lung diseases.346 Elevated diffusing capacity in asthma has been attributed to improved perfusion of well-ventilated upper lung zones and is associated with large lung volumes. The unex-

38 ASTHMA 901
AssessmentAsthma Control
The assessment of patients with asthma involves five essential features: the current degree of control, based on symptoms, reliever medication use, recent exacerba-tions, and clinical lung function; and the risk of future adverse outcomes. With this in mind, the NHLBI recently updated guidelines, and the Global Initiative for Asthma (GINA) proposed a parallel scheme for asthma control based on expert opinion328 (Table 38-1). The NHLBI and GINA categorizations represent categorical interval vari-ables with threshold values. For example, the GINA guidelines accept some daytime symptoms (≤2 times/wk) in the definition of “controlled” asthma, whereas nocturnal symptoms move a patient to the “partially controlled” category. The importance of control indices is underscored by the relationship between poor asthma control and substantial degrees of physical impairment and diminished quality of life, even after taking the base-line severity of asthma into account.356
Several different validated instruments exist for assess-ing asthma, including the Asthma Control Questionnaire, Asthma Control Test, Asthma Therapy Assessment Ques-tionnaire, and Asthma Control Scoring System.357–360 All are useful because they direct history taking, provide
severity of asthma delayed treatment, that routine asthma management was unsatisfactory, and that 86% of the deaths might have been preventable.353 A similar study in 1988 included the observation that a large number of asthmatics admitted to the hospital for observation were discharged with no escalation in the management of their asthma.354 This ultimately led the NHLBI to convene the first expert panel to develop guidelines for the diagnosis and treatment of asthma, and the resulting recommendations were published in 1991.355 Other guidelines soon followed, extending the NHLBI’s initial recommendations. Subsequent revisions have provided clinicians with a reliable framework for evi-dence-based management of patients with asthma. These guidelines emphasize maintaining long-term control of symptoms through attention to environmental and social components of asthma and using treatment regi-mens tailored to the severity of each patient’s symptoms. Crucial components of management include initial eval-uation of severity and ongoing assessment of control; appropriate pharmacologic therapy to reverse bron-choconstriction and ameliorate inflammation; identifica-tion and control of environmental factors that worsen symptoms or trigger exacerbations; and creation of a partnership between the patient and the health care professional to ensure that therapy is tailored to symptoms.
TABLE 38-1. Classification of Asthma Control in Adults and Children Older than 12 Years of Age
Components of Control
CLASSIFICATION OF ASTHMA CONTROL (YOUTHS ≥ 12 YR OF AGE AND ADULTS)
Well-Controlled Not-Well-Controlled Very Poorly Controlled
IMPAIRMENT Symptoms ≤2 days/wk >2 days/wk Throughout the day
Nighttime awakening ≤2 times/mo 1-3 times/wk ≥4 times/wk
Interference with normal activity None Some limitation Extremely limited
Short-acting β-agonist use for symptom control (not prevention of EIB)
≤2 days/wk >2 days/wk Several times/day
FEV1 or peak flow >80% predicted/personal best
60%–80% predicted/personal best
<60% predicted/personal best
Validated questionnaires
ATAQ 0 1–2 3–4
ACQ ≤0.75* ≥1.5 N/A
ACT ≥20 16–19 ≤15
RISK Exacerbations 0-1/yr ≥2/yr†
Consider severity and interval since last exacerbation
Progressive loss of lung function Evaluation requires long-term follow-up care
Treatment-related adverse effects Medication side effects can vary in intensity from none to very troublesome and worrisome. The level of intensity does not correlate to specific levels of control but should be considered in the overall assessment of risk
*ACQ values of 0.76–1.4 are indeterminate regarding well-controlled asthma.†(1) The level of control is based on the most severe impairment or risk category. Assess impairment domain by patient’s recall of previous 2–4 wk and by spirom-
etry or peak flow measures. Symptom assessement for longer periods should reflect a global assessment, such as inquiring whether the patient’s asthma is better or worse since the last visit. (2) At present, there are inadequate data to correspond frequencies of exacerbations with different levels of asthma control. In general, more frequent and intense exacerbations (e.g., requiring urgent, unscheduled care, hospitalization, or intensive care unit admission) indicate poorer disease control. For treatment purposes, patients who had two or more exacerbations requiring oral systemic corticosteroids in the past year may be considered the same as patients who have not-well-controlled asthma, even in the absence of impairment levels consistent with not-well-controlled asthma.
ACQ, Asthma Control Questionnaire; ACT, Asthma Control Test; ATAQ, Asthma Therapy Assessment Questionnaire; EIB, exercise-induced bronchospasm; FEV1, forced expiratory volume in 1 second; N/A, not applicable.
Adapted from National Heart, Lung, and Blood Institute as a part of the National Institutes of Health and the U.S. Department of Health and Human Services, 2007.

902 OBSTRUCTIVEDISEASES
in normal, nonasthmatic patients.367,368 FeNO falls in a dose-dependent manner with steroid use, making FeNO less useful as an ongoing biomarker in patients using steroid therapy.369,370 A recent trial showed that an FeNO of more than 45 parts/billion excludes well-controlled asthma with a negative predictive value of nearly 90%. High FeNO suggests a severe, steroid-responsive pheno-type. A decline in FeNO of more than 40% between visits is a sign of improved control, and low levels of FeNO predicted lower risk of acute exacerbation.371 Measuring the FeNO during a period of good control can provide a baseline for comparing trends over time when following symptoms and response to treatment. Although the FeNO is a promising biomarker in asthma, the cost/benefit ratio of using FeNO to assess asthma control requires more study.
TreatmentOverview
Pharmacologic therapy for asthma is subdivided into acute, short-term “reliever” medications and chronic “controller” medications. Reliever medications target bronchoconstriction by relaxing ASM. The β-agonists such as inhaled albuterol are the most effective reliever medications. Other reliever medications include methyl-xanthines (e.g., theophylline) and short-acting anti-cholinergics such as inhaled ipatropium bromide. The most widely used controller medications are inhaled cor-ticosteroids, which have a localized anti-inflammatory effect. There is overlap in the use and mechanism of action of reliever and controller medications. LABAs, used in conjunction with an inhaled corticosteroid, provide additional control of symptoms. Theophylline, although primarily a bronchodilator, also has a sustained anti-inflammatory effect at low doses, whereas inhaled corticosteroids such as budesonide have been used in the acute treatment of asthma exacerbations.372,373 The introduction of omalizumab, a specific anti-IgE antibody, provided the first opportunity to treat and control asthma based on specific pathophysiologic characteristics. Tai-loring biologic therapy based on pathophysiologic mech-anisms in individual patients is an area of active clinical investigation, and additional agents addressing the aller-gic and nonallergic phenotypes of asthma are under investigation.
Specific Pharmacologic Agents
Current guidelines recommend adjusting therapy in a stepwise fashion to reduce daily symptoms and risk of exacerbations, while minimizing the use of medica-tions.374,375 The hierarchy of treatment recommendations is based on the available literature about efficacy and safety and provides a prominent role for controller med-ications at all levels of asthma treatment. In general, the strategy and recommendations in adults and children are similar. However, the increased risk of adverse effects and/or the lack of safety data in pediatric patients for theophylline, omalizumab, and the 5-lipoxygenase inhib-
goals for the management of symptoms, and guide adjust-ments in treatment.
Lung Function
Lung function testing is an important part of assessing asthma, both for making the initial diagnosis and as a means of evaluating the response to therapy. A recent study from the Genetics in Asthma Network361 suggested that FEV1 and FVC are useful components of a standard-ized scheme for identifying the contribution of genes and environments to disease expression. Further proof of the importance of lung function testing was provided by a recent finding that asthmatic patients with lower FEV1 values were at significantly higher risk of needing acute care.362 Although the FEV1, the FEV1/FVC ratio, and PEF are useful in the diagnosis and monitoring of asthma, the utility of these measurements in improving the outcome of asthma remains incompletely defined. FEV1 is an objective measurement of lung function. The pre-bronchodilator FEV1 is related to asthma control, whereas postbronchodilator FEV1 is related to future risk of exac-erbations. Accurate measurement requires stopping LABAs for 12 hours and short-acting bronchodilators for 6 hours. Because FEV1 is often normal or near-normal in mild asthma, FEV1 may be poorly responsive to bron-chodilators in mild asthma.
PEF measurement is a standard method to correlate physiologic function with asthma severity, and has been used as a marker of asthma control in many clinical trials. However, individual peak flow measurements are highly variable and the variability in peak flow has a greater predictive value for future exacerbations than individual PEF measurements themselves.329,330 The clinical useful-ness of peak flow measurements is also limited by patient resistance to home monitoring and difficulty with con-sistently maintaining peak flow records.
Biomarkers
The presence of sputum eosinophilia provides useful information about the asthma phenotype. Low sputum eosinophil counts predict response to inhaled corticos-teroids and decreased risk of exacerbations, whereas elevated sputum eosinophil counts (>10%) put the subject at high risk for future exacerbations.363,364 A change of 50% in sputum eosinophil counts is consid-ered to be clinically significant, whereas a decline in absolute eosinophil count predicts deterioration when inhaled corticosteroids are withdrawn.365,366 However, induced sputum eosinophils may be difficult to obtain in clinical practice. Furthermore, the lag between speci-men collection and processing may lead to delays in adjusting treatment.
Fractional excretion of nitric oxide (FeNO) has some advantages over counting the number of sputum eosi-nophils. Measurement of FeNO can be performed rapidly in a primary care setting, requires less technical exper-tise, and provides real-time objective physiologic data. However, the FeNO in stable, mild asthma after use of inhaled corticosteroids is often in the same range as that

38 ASTHMA 903
action than salmeterol, whereas salmeterol has a longer duration of action. Each has been shown to improve lung function, reduce symptoms, and reduce the frequency of exacerbations.382
Adverse events associated with the use of β2-agonists are primarily due to unwanted activation of β2-receptors on nonpulmonary tissue. Cardiac stimulation causes tachycardia and arrhythmias, whereas skeletal muscle stimulation causes tremors and hypokalemia. Since the introduction of β-agonists, there has been concern about the clinical implications of receptor desensitization. The short-acting β-agonist fenoterol was implicated in two epidemiologic studies of increased asthma deaths in the 1960s and 1970s383,384; later analysis suggested that this might have been due to excessive use, rebound bron-choconstriction due to short duration of action, or tach-yphylaxis. After fenoterol was withdrawn, mortality declined,385 and the safety profile of subsequent short-acting β2-agonists has been good. Clinical data suggest that “as-needed” versus scheduled short-acting β2-agonist treatment is associated with improved physiology386 and fewer, less severe exacerbations.387
Adverse events with long-acting β2-agonists also are of concern, particularly because of their long duration of action. In the Salmeterol Multicenter Asthma Research Trial (SMART),388 patients were randomized to salme-terol or placebo plus usual care, with approximately 13,000 patients in each arm. There was no significant difference in risk of death in either group, but subgroup analysis identified a small but increased risk of death that was more prominent in African American subjects in the salmeterol arm of the trial. However, the African Ameri-can patients also had poorer control of symptoms at baseline (with more exacerbations and hospitalizations) and a lower rate of inhaled corticosteroid use than the white patients.388 Importantly, the use of LABAs with inhaled corticosteroids in the same metered-dose inhaler has been shown to be safe and effective.389
Several studies have explored the relationship between polymorphisms in the β2-receptor and responses to β-agonist therapy. Specifically, the presence of the Arg/Arg mutation at the B16 locus has been associated with lower PEF, FEV1, symptoms, rescue inhaler use, and increased rate of exacerbations in patients treated with scheduled albuterol as compared with patients who lack the Arg/Arg mutation. All of these symptoms improve when regular albuterol is withdrawn.146,390,391 Use of LABAs (with and without inhaled corticosteroids) has been shown to worsen physiologic markers of respira-tory function in Arg/Arg patients in some studies, although these findings are not consistent.149,392 Two large randomized trials are currently underway that should shed light on this issue.
Other Bronchodilators. Anticholinergic agents act as bronchodilators via competition with acetylcholine at neuromuscular junctions, thereby blocking transmission of bronchoconstrictor reflexes.393 The short-acting anticholinergic ipratropium bromide is effective in patients with chronic obstructive pulmonary disease (COPD) but is considered a second-line agent for treating asthma, most likely because cholinergic tone contributes
itor zileuton, lead to their exclusion from current pedi-atric treatment guidelines.374
β2-Agonists. β2-Agonists have been used for thou-sands of years in the form of the ephedrine-containing herbal preparation ma huang.376 However, it was not until the 1940s, when the nonselective β-agonist isopro-terenol was introduced, that β-agonists became the standard of care for treating airway disease. The subse-quent development of the β2-selective agents albuterol and terbutaline, with improved side effect profiles, led to their current role as the cornerstone of asthma therapy.377
β2-Agonist activity is primarily mediated by binding to a specific G-coupled transmembrane receptor found in high abundance on ASM. Receptor binding leads to increased intracellular cyclic adenosine monophosphate (AMP) and relaxation of ASM.378 Notably, β2-receptors are also found on other resident airway cells, including airway epithelial cells and circulating immune cells, and binding to these sites may reduce vascular permeability and inflammatory mediator release.379 One concern raised about the chronic use of β2-agonists is that of receptor desensitization.380 As with most signaling recep-tors, repeated exposure to β2-agonists can lead to decreased responsiveness of membrane receptors through receptor down-regulation via receptor endocy-tosis and uncoupling of receptor from downstream trans-duction pathways. This response appears to be self-limited in ASM.
β2-Selective agonists are usually administered by aerosol, which maximizes delivery to target tissue (ASM), while minimizing the exposure of nontarget tissues. Both short-acting and long-acting agents are available, and the onset and duration of action are primarily related to lipophilicity.16 Short-acting agents are used for rescue or emergent treatment, whereas LABAs are used in combination with inhaled corticosteroids for chronic management.
A number of highly selective short-acting β2-agonists are now available, and all have a rapid onset of action with peak action between 60 and 90 minutes. Because they are inhaled directly into the airways, systemic side effects are minimal, even at high doses. A β2-agonist preparation containing only the active isomer of albuterol was developed in an attempt to minimize side effects. However, clinical trials have not shown significant dif-ferences in outcome or tolerability.381 Based on current guidelines, these medications should be used to treat symptoms not adequately controlled on a regimen of long-acting agents. Increased frequency of short-acting β2-agonist use is a sign of inadequate control of symp-toms or overreliance on rescue medication. Patients using more than one canister a month or requiring exces-sive doses of rescue inhalers (defined as >2 doses/wk) should be considered for a step-up in therapy.374,375
LABAs have minimal utility for treating acute asth-matic symptoms because of their delayed onset of action. However, in patients with inadequately controlled asthma, they can be added to an inhaled corticosteroid to improve symptoms. Formoterol and salmeterol are the two LABAs available. Formoterol has a shorter onset of

904 OBSTRUCTIVEDISEASES
ICS; although a small observational study suggested increased risk,408 a meta-analysis of several randomized controlled trials did not corroborate this finding.409 The risks of cataract formation410 and glaucoma411 are slightly increased, whereas hypothalamic-pituitary axis suppres-sion, gastrointestinal bleeding, and other complications of systemic steroids are not associated with inhaled prep-arations. The Towards a Revolution in COPD Health (TORCH) trial of the use of inhaled corticosteroids for COPD showed an increased risk of pneumonia, but this has not been demonstrated in patients with asthma.412 The use of inhaled corticosteroids in the pediatric popu-lation has raised concerns about growth suppression. However, available data show only a small and transient decrease in growth trajectory that does not translate into a reduction in adult height.404,413,414
Leukotriene Modifiers. Leukotrienes (LTs) are derived from cell membrane arachadonic acid metabo-lism. LT receptors on ASM and macrophages mediate bronchoconstriction, mucus hypersecretion, and mucosal edema.415 As a result, the LT pathway is a primary target for the development of novel asthma con-troller medications. Commercially available leukotriene modifiers (LTMs) work in one of two places in the LT pathway. Zileuton blocks 5-lipoxygenase, the enzyme that converts arachadonic acid to LTA4, which is the first step in LT synthesis. Montelukast, zafirlukast, and pran-lukast all inhibit LT receptors, blocking the final step in the LT pathway. All are taken orally as either once-daily or twice-daily doses.
LTMs have a modest bronchodilator effect and may improve asthma symptoms and exacerbation rates.416 Physiologic benefits have also been seen, with improve-ments in spirometry and measures of airway inflamma-tion.417 Whereas the subpopulation of patients with aspirin-sensitive asthma may derive great benefit from LTMs,418 data also suggest that LTMs are adequate as single agents in mild persistent asthma.419,420 Although LTMs treat multiple asthma symptoms, they are less effi-cacious than low-dose ICS. As a result, patients who require ICS for asthma control cannot be safely switched to LTM monotherapy. Therefore, the primary role of LTMs is as an adjunct to ICS, and the addition of LTMs typically leads to a reduction in the corticosteroid dose or an improvement in asthma control.421,422 Recent data suggest that the substitution of LTMs for ICS in smokers with asthma leads to similar symptomatic benefits, pos-sibly due to impaired therapeutic responses to ICS in this population. However, it is not clear whether this benefit would persist with the addition of LTMs to ICS in patients who smoke cigarettes.423 Overall, LTMs are less effective than LABAs as adjunctive therapy and do not seem to confer added benefits when added to a regimen that includes an ICS and an LABA.424,425
Overall, LTMs are well tolerated. Initial reports sug-gested a link between LTMs and Churg-Strauss syndrome, but this is now thought more likely to be due to an unmasking of the syndrome by a reduction in corticos-teroid dose with the introduction of an LTM.426 Zileuton is metabolized by the cytochrome P-450 system and has been associated with reports of hepatotoxicity. As a
less to bronchoconstriction in asthma. Although no trials have compared short-acting anticholinergics with short-acting β-agonists, randomized trials studying the addition of anticholinergics to β-agonists do not show any addi-tional benefit in patients with chronic asthma. However, specific asthma phenotypes might be more likely to respond to anticholinergic treatment, including patients with fixed airflow obstruction, advanced age,394 or longer duration of disease.395 Furthermore, anticholinergics may be an acceptable alternative for certain subgroups of patients who do not tolerate β-agonist treatment or for patients with the Arg/Arg-16 genotype, although this has not been studied directly.
Tiotropium, a long-acting anticholinergic agent, has been shown to be beneficial for treating the symptoms of COPD. The value of tiotropium in patients with asthma is not clear, but a randomized trial is in progress. Spiro-metric improvement has been demonstrated in case series of asthmatics who do not have sputum eosi-nophilia396 and asthmatics with concomitant COPD.397 Animal data suggest that tiotropium may have an antire-modeling effect comparable with that of budesonide.398
Inhaled Corticosteroids. With recognition of the central role of inflammation in the pathophysiology of asthma, contemporary treatment strategies now emphasize corticosteroids for long-term control of symp-toms. Corticosteroids suppress inflammatory responses through a broad influence on signal transduction and gene expression pathways. Corticosteroids bind to a specific cytoplasmic receptor that translocates to the nucleus, where it modulates expression of inflamma-tory genes through inhibition of histone acetyltrans-ferases and recruitment of histone deacetylases.399,400 Airway inflammatory cell influx and markers of airway inflammation in asthma are reduced by corticosteroid administration.401,402
Systemic corticosteroids have been used in the treat-ment of asthma since the 1940s and continue to be a cornerstone of the management of acute exacerbations. However, systemically administered corticosteroids are associated with a variety of undesirable side effects. The introduction of inhaled corticosteroids (ICS) in the 1970s ushered in a new era in the treatment of asthma. As with bronchodilators, delivery of drug directly into the lungs through the use of inhaled preparations minimizes sys-temic toxicity and improves therapeutic benefit.
The use of ICS improves all aspects of asthma control. ICS reduce asthmatic symptoms, improve lung function, decrease airway inflammation, and control AHR.403,404 A large meta-analysis showed that inhaled corticosteroids reduce asthma exacerbations by 55% as compared with placebo405 and reduce the risk of hospitalization by 50% as compared with use of as-needed β-agonists alone.406 Furthermore, risk of death from asthma is reduced in a dose-response manner with the use of ICS.407 As a result, ICS are considered to be first-line therapy for all patients requiring more than twice-weekly β-agonist use.375
The risk of systemic toxicity is diminished but not absent with the use of ICS, particularly at doses less than 400 µg budesonide daily or the equivalent. Data are conflicting about the risk of bone demineralization from

38 ASTHMA 905
Additional Management StrategiesControl of Triggers
Environmental factors have been shown to contribute to the pathogenesis of asthma, including occupational exposures, tobacco smoke, pollutants, respiratory infec-tions, allergen exposures, and comorbid conditions. Cigarette smoking decreases asthma control and reduces the efficacy of corticosteroids. All patients with asthma who smoke cigarettes should be strongly encouraged to quit.434 Certain comorbid conditions, including GERD and rhinosinusitis, may worsen asthma symptoms and severity. Because treatment of GERD and sinusitis often improves the control of asthma, all difficult-to-treat patients with asthma should be evaluated for these underlying conditions.435,436
Reduction of allergen exposure and provision of aller-gen immunotherapy are common strategies for treating asthma. Allergic asthmatics improve when removed from their domestic environment, but environmental control is often difficult to achieve.437 The most common allergens include dust mites and cat dander. Whereas avoiding environmental allergens is ideal, most patients do not like the idea of avoiding or giving away their pets. Although overall data are mixed, several studies have shown clinical benefits from dust mite control measures (i.e., impermeable mattress covers, frequent vacuuming, cockroach control).438,439 For patients with an allergic asthma phenotype, allergen-specific immunotherapy may reduce asthma symptoms and improve bronchial hyperreactivity.440,441 However, administration must take place under careful conditions owing to the risk of ana-phylaxis, and the optimal duration of treatment is not completely clear.
Medication Adjustment Based on Asthma Control
The definition of asthma severity is based on the severity of symptoms at the time of diagnosis. More recent defini-tions take into account the degree of treatment neces-sary to maintain control and the frequency of exacerbations. Asthma control, defined as the degree of symptoms present while on appropriate therapy, is more fluid. Depending on the extent of control, a more or less aggressive approach to symptom management may be needed. Recent studies support the importance of focus-ing on asthma control as a means of reducing exacerba-tions and morbidity.441a Published guidelines provide an up-to-date framework for medication choices when “stepping up” therapy to improve asthma control and “stepping down” therapy when control has been achieved (Fig. 38-5). For patients with mild, intermittent asthma, with symptoms that return to baseline between episodes, as-needed use of a short-acting bronchodilator is usually sufficient to maintain control of symptoms. For patients with chronic asthma (symptoms that occur >2 times/wk, nocturnal symptoms, or symptoms that affect activity), the addition of a controller medication is needed, and an ICS is the initial agent of choice.404,442,443
result, liver function should be monitored during its use. The availability of a sustained-release preparation of zileuton has made it a better option as adjunctive therapy. At present, zileuton is reserved for patients with refrac-tory asthma or who have an asthmatic phenotype sug-gesting benefit from the use of an LTM.427
Phosphodiesterase 4 Inhibitors (Theophylline). Theophylline is a well-established phosphodiesterase inhibitor that has mild anti-inflammatory properties. Because of its narrow therapeutic index, theophylline is not widely used in treating asthma. However, the discov-ery of additional anti-inflammatory properties, likely mediated by histone deacetylation, has led to a resur-gence of interest.428 Although no longer a first-line therapy, theophylline is currently used in low doses as adjunctive treatment for asthma that is difficult to control with steroids alone.429 The addition of theophylline to an existing drug regimen for poorly controlled asthma improves markers of control (rescue inhaler use, lung function) to a greater extent than LTMs.423 Dose-related side effects, such as anorexia, palpitations, dysrhythmias, and seizures, require careful clinical and laboratory monitoring.
Anti-Immunoglobulin E Treatment. The introduc-tion of omalizumab, a monoclonal antibody to IgE, rep-resents a new era of therapy targeted to specific asthma phenotypes. Omalizumab targets the receptor-binding portion of IgE, preventing it from interacting with immune cells to cause degranulation.430 The addition of omalizumab to ICS in poorly controlled allergic asthmat-ics is associated with improved asthma control and fewer exacerbations.431 Omalizumab is generally well tolerated, but rare reports of anaphylaxis have led to recommenda-tions that patients be observed for 2 hours after each of the first three injections to ensure safety.304 High cost, the requirement for monitoring during treatment, and the need to carefully select patients likely to benefit have limited the use of omalizumab. However, cost analysis suggests that anti-IgE therapy in patients with severe allergic asthma results in a cost-per-quality-adjusted life year that compares favorably with other uses of expen-sive health care resources.432
Nonpharmacologic Treatment
Bronchial thermoplasty is a novel intervention for asthma that is based on the observation that increased ASM mass is a characteristic feature of asthma. During thermo-plasty, controlled thermal energy is delivered to the airway wall, resulting in reduction of ASM mass. In patients with moderately severe asthma, thermoplasty been shown to reduce airway responsiveness to an inhaled constrictor and improve lung function.433 Treat-ment leads to improvements in symptoms and quality of life and reduction in the use of rescue medication in patients with moderate or severe asthma.304 However, treatment requires a series of three bronchoscopies, exposing patients to the concomitant procedural risk, and long-term outcome data are lacking. Nevertheless, the specific targeting of ASM in asthma remains an area of investigation.

906 OBSTRUCTIVEDISEASES
Prevention Program (NAEPP) guidelines give the options of increasing the dose of ICS or adding an LABA. This is also the preferred approach for pediatric patients. A third option is the addition of LTMs to low-dose ICS.422
If symptoms are still not controlled on one of the regimens just discussed, the next medication added depends on previous medication choices. For patients on increased doses of ICS, the recommended next step is the combination of a moderate- to high-dose ICS with an LABA. However, increasing the ICS dose for a patient already on an ICS/LABA combination is less likely to be effective.450,451 Other options include the addition of an LTM or sustained-release theophylline to an ICS.452 If symptoms remain uncontrolled on a full complement of standard medications, options include the addition of systemic corticosteroids or specific anti-IgE therapy for patients with allergic asthma.431
Once symptoms are controlled for a protracted period of time, therapy can be stepped down. Strategies for de-
As mentioned previously, when used properly, ICS amel-iorate all asthma symptoms, improve airway physiology, and reduce hospitalizations and asthma mortality. Failure to respond to ICS suggests nonadherence to medica-tions, uncontrolled trigger exposures and/or comorbidi-ties, or a steroid-nonresponsive phenotype. Approximately 30% of asthmatics fall into the last category. These patients typically have less airway inflammation and obtain their maximum response to a low-dose of ICS.444,445 LTMs are an alternative for patients who do not tolerate ICS and are the preferred agent for patients with con-comitant allergic rhinitis.416,417
For patients with persistent asthmatic symptoms despite the appropriate use of a controller medication, clinicians have several different options for “stepping-up” therapy. Some guidelines recommend the addition of an LABA to low-dose ICS (often in a combination inhaler) based on a large amount of efficacy data.446–449 However, because of concerns over the potential side effects of LABAs, the National Asthma Education and
Persistent asthma: daily medication
Consult with asthma specialist if step 4 care or higher is required.Consider consultation at step 3.
Intermittentasthma
Step 1
Preferred:SABA PRN
Each step: Patient education, environmental control, and management of comorbidities.Steps 2–4: Consider subcutaneous allergen immunotherapy for patients who have allergic asthma (see notes).
Quick relief medication for all patients• SABA as needed for symptoms. Intensity of treatment depends on severity of symptoms: up to 3 treatments at 20-minute intervals as needed. Short course of oral systemic corticosteroids may be needed.• Use of SABA >2 days a week for symptom relief (not prevention of EIB) generally indicates inadequate control and the need to step up treatment.
Step 2
Preferred:Low-dose ICS
Alternative:Cromolyn,
LTRA,Nedocromil,orTheophylline
Step 3
Preferred:Low-dose
ICS + LABAOR
Medium-doseICS
Alternative:Low-dose ICS+ either LTRA,Theophylline,
or Zileuton
Step 4
Preferred:Medium-doseICS + LABA
Alternative:Medium-doseICS + either
LTRA,Theophylline,
or Zileuton
Step 5
Preferred:High-dose
ICS + LABA
AND
ConsiderOmalizumabfor patientswho haveallergies
Step 6
Preferred:High-dose
ICS + LABA + oral
corticosteroid
AND
ConsiderOmalizumabfor patientswho haveallergies
Step up ifneeded
(first, checkadherence,
environmentalcontrol, andcomorbid
conditions)
Step down ifpossible
(and asthmais well
controlled at least
3 months)
Assesscontrol
Key: Alphabetical order is used when more than one treatment option is listed within either preferred or alternative therapy.EIB, exercise-induced bronchospasm; ICS, inhaled corticosteroid; LABA, long-acting inhaled beta2-agonist; LTRA, leukotrienereceptor antagonist; SABA, inhaled short-acting beta2-agonist.
FIGURE 38-5 n Medication recommendations for control of asthma in adults and children older than 12 years of age. (Adapted from the National Heart, Lung, and Blood Institute as a part of the National Institutes of Health and the U.S. Department of Health and Human Services, 2007.)

38 ASTHMA 907
suggests impending respiratory failure. Anion gap meta-bolic acidosis may also be present, which is usually due to elevated lactate levels. Patients who fail to respond to albuterol administration within 30 to 60 minutes, with persistent dyspnea and peak flow less than 70% of base-line, require hospital admission.374
Key pharmacologic components of treatment include repeated or continuous short-acting bronchodilator administration (via nebulizer or metered-dose inhaler with a spacer) and systemic glucocorticoids.457 The com-bination of short-acting β-agonists and ipratropium at the initiation of treatment is associated with physiologic improvements and reduced rate of hospitalization, but the benefits do not persist after hospitalization.458 Systemic corticosteroids are unequivocally associated with more rapid return to baseline function and are considered the first-line therapy for acute asthma. The initial dosing range for adult hospitalized patients is from 1.5 to 2.0 mg/kg of intravenous methylprednisolone or the equivalent.459 ICS are typically not used acutely, although some data suggest that the addition of inhaled budesonide to systemic corticosteroids following an emergency department visit leads to improved symp-toms and a decreased relapse rate.460,461 Intravenous mag-nesium sulfate, usually given as a 2-g bolus, may act as a smooth muscle relaxant and has been shown to reduce hospital admission rates.462 Supplemental oxygen to keep saturations above 90% helps maintain oxygen delivery to peripheral tissues and minimizes hypoxemic vasoconstriction.
Severe exacerbations of asthma are characterized by persistent reductions in peak expiratory flow of less than 40% predicted with poor response to initial treatment. These patients may demonstrate progressive hypercap-nia, fatigue, altered sensorium, and dysrhythmias and are at high risk for respiratory arrest. Low-level noninvasive positive-pressure ventilation without positive end-expira-troy pressure (PEEP) has been shown to reduce the rate of hospitalization and may be considered in alert, coop-erative patients who are not in immediate need of intuba-tion.463 Helium/oxygen mixtures increase flow through the airways and may be a useful adjunct in patients with severe exacerbations that do not respond to initial emer-gency treatment.464,465
Oral intubation and mechanical ventilation are manda-tory for patients in respiratory arrest or impending res-piratory arrest. Mechanical ventilation in patients with severe asthma exacerbations may be complicated by immediate postintubation worsening of gas exchange and hemodynamic instability due to increased airway and intrathoracic pressures from dynamic lung hyperin-flation. Provided that the patient is adequately oxygen-ated, briefly decreasing the mandatory respiratory rate to allow an extended expiratory phase is often success-ful. Initial ventilator settings should be focused on mini-mizing dynamic hyperinflation by using a relatively low minute ventilation (with respiratory rate between 12 and 14/min and tidal volumes in the 6-8 mL/kg range), a high inspiratory flow rate, and minimal to no PEEP.466 Aggres-sive sedation should be given to improve comfort and patient-ventilator synchrony. Short-term paralysis may be
escalation of therapy are determined by a patient’s con-troller regimen. Patients on an ICS alone can be considered for a decrease in dose or dosing interval. Some data suggest that conversion to as-needed com-bined short-acting β2-agonists/ICS may be effective with a lower total steroid dose.453,454 However, an as-needed regimen is not yet part of NHLBI guidelines. Similarly, for patients on a combined ICS/LABA regimen or LTM/ICS regimen, clinicians should focus first on reducing the ICS component.
Management of Acute AsthmaAsthma is a common cause of emergency room visits and hospital admissions. In 2004, asthma accounted for 1.8 million visits to emergency departments, or 64/10,000 people, with 497,000 asthma hospitalizations, or 17/10,000 people.24 The treatment of acute asthma is based on the cornerstones of chronic asthma therapy but typically requires greater attention to patient monitoring and an escalation in the aggressiveness of asthma care.
Asthma exacerbations are characterized by increased shortness of breath, coughing, and/or chest tightness, and airflow limitation (as measured by decreased peak flow or FEV1) is a cardinal feature. Increased symptoms typically precede a detectable decrease in air flow,455 although a subset of patients are at high risk of exacerba-tions due to poor perception of airflow limitations. In the outpatient setting, increased requirement for rescue inhalers, especially in a patient previously on a stable regimen, suggests an asthma flare.
Patients with asthma exacerbations require prompt evaluation and treatment in order to limit morbidity and mortality. Goals include relief of airflow obstruction and amelioration of respiratory symptoms. Patients with milder symptoms (with peak flow decrease <20%) may be evaluated in an outpatient setting but should be referred to an acute care facility if they fail to respond promptly to aggressive treatment with bronchodilators and systemic glucocorticoids.374 Conversely, certain patients are at high risk of asthma-related death and should be evaluated in the emergency department as soon as possible when their symptoms worsen. This includes patients with a history of recent exacerbation or previous near-fatal asthma, overutilization of short-acting β2-agonists or underutilization of ICS, recent oral glucocorticoid use, poor compliance with asthma action plans, or concomitant psychiatric disease.456
In the acute care setting, the severity of an asthma exacerbation should be assessed by physical examina-tion, including oximetry and measurement of peak expir-atory flow. Use of accessory muscles, ability to complete sentences, and arterial oxygen tension all should be eval-uated. Patients require close monitoring during the early stages of treatment, because it may take several hours for symptoms to resolve. Chest radiography is useful if pneumothorax is suspected but does not usually provide clues as to the etiology of an exacerbation. Arterial blood gas measurement typically reflects mild hypoxemia and respiratory alkalosis; the normalization of PaCO2 in the absence of significant symptomatic improvement

908 OBSTRUCTIVEDISEASES
allowing patients to titrate their own treatment based on changes in symptoms and peak expiratory flow with some degree of independence. The use of such guided self-management reduces asthma morbidity in different patient populations and patient care settings.467
Crucial components of self-management plans include education, self-monitoring with symptoms and/or peak flow, regular review, and patient directed self-manage-ment using a written action plan. Effective patient educa-tion is central to this approach. Better communication by health care providers translates into measurably better outcomes with no additional physician time commit-ment.468 Even for patients unable to engage in guided self-management, regular follow-up and medication review is beneficial, because approximately 50% of patients on long-term therapy fail to take medications as directed some of the time.469
necessary in patients for whom ventilator synchrony cannot be achieved with sedation alone. Bronchodilator administration should be continued until airway resist-ance decreases.
Conclusion: Clinician-Patient PartnershipFor chronic asthma, treatment should balance the best symptom control with the lowest possible dosage of medication.374 Effective management requires that the patients form a partnership with the health care provid-ers in order to ensure an appropriate flow of information, with the patients assuming a major role in the assessment and treatment of their disease. Through collaborative effort, a guided self-management plan can be developed,
KEY POINTS
• Asthma is an important cause of disability, death, and economic cost.
• Asthma is increasing in developed countries and appears to be increasing to epidemic proportions in non-Western societies that have adopted features of Western culture.
• On a fundamental level, asthma is a disease of misdirected immunity, with the direction of immune function being influenced by many genes and probably also by airway infections, especially with viruses, but established in the first few years of life. The cells most important in orchestrating this “misdirected” immune response in the airways are dendritic cells and CD4 Th2 lymphocytes.
• The cytokines produced by these lymphocytes, particularly IL-13, alter the function of immunological and structural cells in the airways, either directly through activation of specific receptors on the cells or indirectly through their effects on other cells, such as B lymphocytes, mast cells, eosinophils, and polymorphonuclear leukocytes. Repeated release of these cytokines alters the function and structure of the airways.
• The structural changes, often referred to as “remodeling,” are now recognized as potentially irreversible.
• The approach to the diagnosis, assessment, and treatment of asthma has changed in response to the recognition of asthma as a chronic inflammatory disease punctuated by intermittent exacerbations.
• The therapies available are effective in controlling asthma, but their efficacy depends on engaging the patient as a full partner in care.
• Before the most economical and effective approach for preventing asthma can be undertaken, more information is needed about the interplay between individual genotypes and environmental stimuli that are responsible for initiating and perpetuating the disease.
• Until a curative treatment is developed, only the combined use of anti-inflammatory and bronchodilator therapies, coupled with measures to reduce environmental exposures, can reduce the costs of asthma for the individuals affected. Applied widely, these measures can also reduce the consequences and costs for the health care system.
References1. http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm1a. Meneely GR, Ball CO, Ferguson JL, et al: Use of computers in
measuring body electrolytes by gamma spectrometry. Circ Res 11:539–548, 1962.
2. Tang EW, Wiesch D, Samet J: Epidemiology of asthma and allergic diseases. In Adkinson Jr NY, Yunginger JW, Busse WW, et al
(eds): Middleton’s Allergy: Principles and Practice. St. Louis: Mosby, 2003:1127–1144.
3. NHLBI/WHO Workshop Report: Global Strategy for Asthma Man-agement and Prevention. Publication 02-3659. Bethesda, MD: National Institutes of Health, 2006.
4. Eder W, Ege MJ, von Mutius E: The asthma epidemic. N Engl J Med 355:2226–2235, 2006.
5. Worldwide variation in prevalence of symptoms of asthma, aller-gic rhinoconjunctivitis, and atopic eczema: ISAAC. The Interna-

38 ASTHMA 909
31. Stein RT, Sherrill D, Morgan WJ, et al: Respiratory syncytial virus in early life and risk of wheeze and allergy by age 13 years. Lancet 354:541–545, 1999.
32. Illi S, von Mutius E, Lau S, et al: Early childhood infectious dis-eases and the development of asthma up to school age: A birth cohort study. BMJ 322:390–395, 2001.
33. Rooney JC, Williams HE: The relationship between proved viral bronchiolitis and subsequent wheezing. J Pediatr 79:744–747, 1971.
34. Gurwitz D, Mindorff C, Levison H: Increased incidence of bron-chial reactivity in children with a history of bronchiolitis. J Pediatr 98:551–555, 1981.
35. Hall CB, Hall WJ, Gala CL, et al: Long-term prospective study in children after respiratory syncytial virus infection. J Pediatr 105:358–364, 1984.
36. Mok JY, Simpson H: Outcome for acute bronchitis, bronchiolitis, and pneumonia in infancy. Arch Dis Child 59:306–309, 1984.
37. Mok JY, Simpson H: Symptoms, atopy, and bronchial reactivity after lower respiratory infection in infancy. Arch Dis Child 59:299–305, 1984.
38. Wright AL, Taussig LM, Ray CG, et al: The Tucson Children’s Respiratory Study. II. Lower respiratory tract illness in the first year of life. Am J Epidemiol 129:1232–1246, 1989.
39. Noble V, Murray M, Webb MS, et al: Respiratory status and allergy nine to 10 years after acute bronchiolitis. Arch Dis Child 76:315–319, 1997.
40. Sigurs N, Bjarnason R, Sigurbergsson F, et al: Respiratory syncytial virus bronchiolitis in infancy is an important risk factor for asthma and allergy at age 7. Am J Respir Crit Care Med 161:1501–1507, 2000.
41. Sigurs N, Gustafsson PM, Bjarnason R, et al: Severe respiratory syncytial virus bronchiolitis in infancy and asthma and allergy at age 13. Am J Respir Crit Care Med 171:137–141, 2005. Epub 2004;October 29.
42. Perez-Yarza EG, Moreno A, Lazaro P, et al: The association between respiratory syncytial virus infection and the develop-ment of childhood asthma: A systematic review of the literature. Pediatr Infect Dis J 26:733–739, 2007.
43. Jackson DJ, Gangnon RE, Evans MD, et al: Wheezing rhinovirus illnesses in early life predict asthma development in high-risk children. Am J Respir Crit Care Med 178:667–672. Epub 2008;June 19.
44. Lemanske RF Jr, Jackson DJ, Gangnon RE, et al: Rhinovirus ill-nesses during infancy predict subsequent childhood wheezing. J Allergy Clin Immunol 116:571–577, 2005.
45. Singh AM, Moore PE, Gern JE, et al: Bronchiolitis to asthma: A review and call for studies of gene-virus interactions in asthma causation. Am J Respir Crit Care Med 175:108–119, 2007. Epub 2006;October 19.
46. Peebles RS Jr, Graham BS: Pathogenesis of respiratory syncytial virus infection in the murine model. Proc Am Thorac Soc 2:110–115, 2005.
47. Dakhama A, Lee YM, Gelfand EW: Virus-induced airway dysfunc-tion: Pathogenesis and biomechanisms. Pediatr Infect Dis J 24(11 Suppl):S159–S169, 2005.
48. Hansbro NG, Horvat JC, Wark PA, et al: Understanding the mech-anisms of viral induced asthma: New therapeutic directions. Phar-macol Ther 117:313–353, 2008. Epub 2008;January 29.
49. Johnson TR, Graham BS: Secreted respiratory syncytial virus G glycoprotein induces interleukin-5 (IL-5), IL-13, and eosinophilia by an IL-4–independent mechanism. J Virol 73:8485–8495, 1999.
50. Johnston SL, Martin RJ: Chlamydophila pneumoniae and Myco-plasma pneumoniae: A role in asthma pathogenesis? Am J Respir Crit Care Med 172:1078–1089, 2005. Epub 2005;June 16.
51. Emre U, Roblin PM, Gelling M, et al: The association of Chlamy-dia pneumoniae infection and reactive airway disease in chil-dren. Arch Pediatr Adolesc Med 148:727–732, 1994.
52. Hahn DL, Golubjatnikov R: Asthma and chlamydial infection: A case series. J Fam Pract 38:589–595, 1994.
53. Cook PJ, Davies P, Tunnicliffe W, et al: Chlamydia pnuemoniae and asthma. Thorax 53:254–259, 1998.
54. Huittinen T, Hahn D, Anttila T, et al: Host immune response to Chlamydia pneumoniae heat shock protein 60 is associated with asthma. Eur Respir J 17:1078–1082, 2001.
tional Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Lancet 351:1225–1232, 1998.
6. Centers for Disease Control and Prevention: Obesity trends in the United States. Available at http://www.cdc.gov/nccdphp/dnpa/obesity/trend/index/htm
7. http://www.cdc.gov/hchs/fastats/asthma.htm8. Weiland SK, Bjorksten , Brunekreef B, et al: Phase II of the Inter-
national Study of Asthma and Allergies in Childhood (ISAAC II): Rationale and methods. Eur Respir J 24:406–412, 2004.
9. Weinmayr G, Weiland SK, Bjorksten B, et al: Atopic sensitization and the international variation of asthma symptom prevalence in children. Am J Respir Crit Care Med 176:565–574. Epub 2007; June 15.
10. Von Mutius E: Worldwide asthma epidemic. Immunol Allergy Clin North Am 22:701–711, 2002.
11. Pearce N, Ait-Khaled N, Beasley R, et al: Worldwide trends in the prevalence of asthma symptoms: Phase III of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax 62:758–766. Epub 2007;May 15.
12. Burney PG, Luczynska C, Chinn S, et al: The European Com-munity Respiratory Health Survey. Eur Respir J 7:954–960, 1994.
13. Variations in the prevalence of respiratory symptoms, self-reported asthma attacks, and use of asthma medication in the European Community Respiratory Health Survey (ECRHS). Eur Respir J 9:687–695, 1996.
14. Burr ML: Is asthma increasing? J Epidemiol Community Health 41:185–189, 1987.
15. Anderson HR: Is the prevalence of asthma changing? Arch Dis Child 64:172–175, 1989.
16. Anderson HR, Butland BK, Strachan DP: Trends in prevalence and severity of childhood asthma. BMJ 308:1600–1604, 1994.
17. Peat JK, van den Berg RH, Green WF, et al: Changing prevalence of asthma in Australian children. BMJ 308:1591–1596, 1994.
18. Masoli M, Fabian D, Holt S, et al: The global burden of asthma: Executive summary of the GINA Dissemination Committee report. Allergy 59: 469–478, 2004.
19. Anderson HR, Strachan DP: Asthma mortality in England and Wales, 1979–89. Lancet 337:1357, 1991.
20. Braman SS: The global burden of asthma. Chest 130(1 Suppl):4S–12S, 2006.
21. Tual S, Godard P, Piau JP, et al: Asthma-related mortality in France, 1980–2005: Decline since the last decade. Allergy 63: 621–623, 2008.
22. Pearce N, Crane J, Burgess C, et al: Fenoterol and asthma mortal-ity in New Zealand. N Z Med J 103:73–75, 1990.
23. Moorman JE, Rudd RA, Johnson CA: et al: National surveillance for asthma—United States, 1980–2004. MMWR Surveill Summ 56:1–54, 2007.
24. Akinbami L: Asthma prevalence, health care use and mortality: United States, 2003–05. 2008. Available at http://www.cdc.gov/hchs/products/pubs/pubd/hestats/asthma03-05/asthma03-05.htm
25. Strachan DP: Hay fever, hygiene, and household size. BMJ 299:1259–1260, 1989.
26. Strachan D, Sibbald B, Weiland S, et al: Worldwide variations in prevalence of symptoms of allergic rhinoconjunctivitis in children: The International Study of Asthma and Allergies in Childhood (ISAAC). Pediatr Allergy Immunol 8:161–176., 1997.
27. Beisswenger C, Bals R: Interaction of allergic airway inflammation and innate immunity: Hygiene and beyond. J Occup Med Toxicol 3(Suppl 1):S3, 2008.
28. Kiechl-Kohlendorfer U, Horak E, Mueller W, et al: Neonatal char-acteristics and risk of atopic asthma in schoolchildren: Results from a large prospective birth-cohort study. Acta Paediatr 96: 1606–1610. Epub 2007;September 19.
29. Stelmach I, Smejda K, Jerzynska J, et al: Decreased markers of atopy in children with presumed early exposure to allergens, unhygienic conditions, and infections. Ann Allergy Asthma Immunol 99:170–177, 2007.
30. Ramsey CD, Gold DR, Litonjua AA, et al: Respiratory illnesses in early life and asthma and atopy in childhood. J Allergy Clin Immunol 119:150–156, 2007. Epub 2006;October 23.

910 OBSTRUCTIVEDISEASES
80. Harding SM: Gastroesophageal reflux, asthma, and mechanisms of interaction. Am J Med 111(Suppl 8A):8S–12S, 2001.
81. Kiljander T, Salomaa ER, Hietanen E, et al: Asthma and gastro-oesophageal reflux: Can the response to anti-reflux therapy be predicted? Respir Med 95:387–392, 2001.
82. Kiljander TO, Salomaa ER, Hietanen EK, et al: Gastroesophageal reflux and bronchial responsiveness: Correlation and the effect of fundoplication. Respiration 69:434–439, 2002.
83. Harding SM: Recent clinical investigations examining the associa-tion of asthma and gastroesophageal reflux. Am J Med 115(Suppl 3A):39S–44S, 2003.
84. Harding SM: Gastroesophageal reflux as an asthma trigger: Acid stress. Chest 126:1398–1399, 2004.
85. Harding SM: Gastroesophageal reflux: A potential asthma trigger. Immunol Allergy Clin North Am 25:131–148, 2005.
85a. Dixon AE: Adipokines and asthma. Chest 135:255–256, 2009.86. Milan G, Granzotto M, Scarda A, et al: Resistin and adiponectin
expression in visceral fat of obese rats: Effect of weight loss. Obes Res 10:1095–1103, 2002.
87. Shore SA, Johnston RA: Obesity and asthma. Pharmacol Ther 110:83–102, 2006. Epub 2005;November 17.
88. Straczkowski M, Dzienis-Straczkowska S, Stepien A, et al: Plasma interleukin-8 concentrations are increased in obese subjects and related to fat mass and tumor necrosis factor-alpha system. J Clin Endocrinol Metab 87:4602–4606, 2002.
89. Guler N, Kirerleri E, Ones U, et al: Leptin: Does it have any role in childhood asthma? J Allergy Clin Immunol 114:254–259, 2004.
90. Sood A, Ford ES, Camargo CA Jr: Association between leptin and asthma in adults. Thorax 61:300–305,, 2006. Epub 2006;March 15.
91. Vercelli D: Advances in asthma and allergy genetics in 2007. J Allergy Clin Immunol 122:267–271, 2008. Epub 2008;July 10.
92. Senthilselvan A, Rennie D, Chenard L, et al: Association of poly-morphisms of Toll-like receptor 4 with a reduced prevalence of hay fever and atopy. Ann Allergy Asthma Immunol 100:463–468, 2008.
93. Yang IA, Fong KM, Holgate ST, et al: The role of Toll-like recep-tors and related receptors of the innate immune system in asthma. Curr Opin Allergy Clin Immunol 6:23–28, 2006.
94. Raby BA, Klimecki WT, Laprise C, et al: Polymorphisms in Toll-like receptor 4 are not associated with asthma or atopy-related phenotypes. Am J Respir Crit Care Med 166:1449–1456, 2002.
95. Adjers K, Karjalainen J, Pessi T, et al: Epistatic effect of TLR4 and IL4 genes on the risk of asthma in females. Int Arch Allergy Immunol 138:251–256, 2005. Epub 2005;October 7.
96. Zhang H, Zhang Q, Wang L, et al: Association of IL4R gene poly-morphisms with asthma in Chinese populations. Hum Mutat 28:1046, 2007.
97. Howard TD, Koppelman GH, Xu J, et al: Gene-gene interaction in asthma: IL4RA and IL13 in a Dutch population with asthma. Am J Hum Genet 70:230–236, 2002. Epub 2001;November 14.
98. Freidin MB, Kobyakova OS, Ogorodova LM, et al: Association of polymorphisms in the human IL4 and IL5 genes with atopic bronchial asthma and severity of the disease. Comp Funct Genom-ics 4:346–350, 2003.
99. Denham S, Koppelman GH, Blakey J, et al: Meta-analysis of genome-wide linkage studies of asthma and related traits. Respir Res 9:38, 2008.
100. Wang L, Pinkerton KE: Detrimental effects of tobacco smoke exposure during development on postnatal lung function and asthma. Birth Defects Res C Embryo Today 84:54–60, 2008.
101. Moshammer H, Hoek, G, Luttmann-Gibson H, et al: Parental smoking and lung function in children: An international study. Am J Respir Crit Care Med 173(:1255–1263, 2006. Epub 2006;Feb-ruary 16.
102. Wang C, Salam MT, Islam T, et al: Effects of in utero and child-hood tobacco smoke exposure and beta2-adrenergic receptor genotype on childhood asthma and wheezing. Pediatrics 122:e107–e114, 2008. Epub 2008;June 16.
103. Goksor E, Amark M, Alm B, et al: The impact of pre- and post-natal smoke exposure on future asthma and bronchial hyper-respon-siveness. Acta Paediatr 96:1030–1035, 2007. Epub 2007;May 10.
104. Raherison C, Penard-Morand C, Moreau D, et al: In utero and childhood exposure to parental tobacco smoke, and allergies in
55. Sutherland ER, Brandorff JM, Martin RJ: Atypical bacterial pneu-monia and asthma risk. J Asthma 41:863–868, 2004.
56. Kraft M, Hamid Q, Cassell GH, et al: Mycoplasma and Chlamydia cause increased airway inflammation that is responsive to clari-thromycin. Am J Respir Crit Care Med 159:A517, 1999.
57. Kraft M, Cassell GH, Pak J, et al. Mycoplasma pneumoniae and Chlamydia pneumoniae in asthma: Effect of clarithromycin. Chest 121:1782–1788, 2002.
58. Kraft M, Adler KB, Ingram JL, et al: Mycoplasma pneumoniae induces airway epithelial cell expression of MUC5AC in asthma. Eur Respir J 31:43–46, 2008.
59. Strachan DP, Butland BK, Anderson HR: Incidence and prognosis of asthma and wheezing illness from early childhood to age 33 in a national British cohort. BMJ 312:1195–1199, 1996.
60. Strachan DP, Harkins LS, Johnston ID, et al: Childhood anteced-ents of allergic sensitization in young British adults. J Allergy Clin Immunol 99:6–12, 1997.
61. Strachan DP: Family size, infection and atopy: The first decade of the “hygiene hypothesis.” Thorax 55(Suppl 1):S2–S10, 2000.
62. Ozdemir C, Ceyhan BB, Yazi D, et al: Non-atopic asthma in chil-dren is related to maternal bronchial hyperreactivity. Pediatr Allergy Immunol 19:248–254, 2008.
63. Tariq SM, Matthews SM, Hakim EA, et al: The prevalence of and risk factors for atopy in early childhood: A whole population birth cohort study. J Allergy Clin Immunol 101:587–593, 1998.
64. Porsbjerg C, von Linstow ML, Ulrik CS, et al: Risk factors for onset of asthma: A 12-year prospective follow-up study. Chest 129:309–316, 2006.
65. Torrent M, Sunyer J, Garcia R, et al: Early-life allergen exposure and atopy, asthma, and wheeze up to 6 years of age. Am J Respir Crit Care Med 176:446–453, 2007. Epub 2007;June 15.
66. Celedon JC, Milton DK, Ramsey CD, et al: Exposure to dust mite allergen and endotoxin in early life and asthma and atopy in childhood. J Allergy and Clinical Immunol 120:144–149, 2007.
67. Nystad W, Meyer HE, Nafstad P, et al: Body mass index in relation to adult asthma among 135,000 Norwegian men and women. Am J Epidemiol 160:969–976, 2004.
68. Chen Y, Dales R, Tang M, et al: Obesity may increase the inci-dence of asthma in women but not in men: Longitudinal observa-tions from the Canadian National Population Health Surveys. Am J Epidemiol 155:191–197, 2002.
69. Bibi H, Shoseyov D, Feigenbaum D, et al: The relationship between asthma and obesity in children: Is it real or a case of over diagnosis? J Asthma 41:403–410, 2004.
70. Rizwan S, Reid J, Kelly Y, et al: Trends in childhood and parental asthma prevalence in Merseyside, 1991–1998. J Public Health (Oxf) 26:337–342, 2004.
71. von Kries R, Hermann M, Grunert VP, et al: Is obesity a risk factor for childhood asthma? Allergy 56:318–322, 2001.
72. Beuther DA, Sutherland ER: Overweight, obesity, and incident asthma: A meta-analysis of prospective epidemiologic studies. Am J Respir Crit Care Med 175:661–666, 2007. Epub 2007;January 18.
73. Shore SA: Obesity and asthma: Possible mechanisms. J Allergy Clin Immunol 121:1087–1093, 2008 [quiz 1094–1095]. Epub 2008;April 11.
74. Weiss ST: Obesity: Insight into the origins of asthma. Nat Immunol 6:537–539, 2005.
75. Sulit LG, Storfer-Isser A, Rosen CL, et al: Associations of obesity, sleep-disordered breathing, and wheezing in children. Am J Respir Crit Care Med 171:659–664, 2005. Epub 2004;December 10.
76. Hancox RJ, Poulton R, Taylor DR, et al: Associations between respiratory symptoms, lung function and gastro-oesophageal reflux symptoms in a population-based birth cohort. Respir Res 7:142, 2006.
77. Bagnato GF, Gulli S, Giacobbe O, et al: Bronchial hyperrespon-siveness in subjects with gastroesophageal reflux. Respiration 67:507–509, 2000.
78. Bagnato VJ: Laparoscopic Nissen fundoplication. Surg Laparosc Endosc 2:188–190, 1992.
79. Stein MR: Possible mechanisms of influence of esophageal acid on airway hyperresponsiveness. Am J Med 115(Suppl 3A):55S–59S, 2003.

38 ASTHMA 911
127. Bleecker ER, Amelung PJ, Levitt RC, et al: Evidence for linkage of total serum IgE and bronchial hyperresponsiveness to chro-mosome 5q: A major regulatory locus important in asthma. Clin Exp Allergy 25(Suppl 2):84–88, 1995 [discussion appears 95–96].
128. Koppelman GH, Stine OC, Xu J, et al: Genome-wide search for atopy susceptibility genes in Dutch families with asthma. J Allergy Clin Immunol 109:498–506, 2002.
129. Postma DS, Meyers DA, Jongepier H, et al: Genomewide screen for pulmonary function in 200 families ascertained for asthma. Am J Respir Crit Care Med 172:446–452, 2005. Epub 2005; May 18.
130. Ober C, Hoffjan S: Asthma genetics 2006: The long and winding road to gene discovery. Genes Immun 7:95–100, 2006.
131. Moffatt MF, Kabesch M, Liang L, et al: Genetic variants regulating ORMDL3 expression contribute to the risk of childhood asthma. Nature 448:470–473, 2007. Epub 2007;July 4.
132. Ober C, Tan Z, Sun Y, et al: Effect of variation in CHI3L1 on serum YKL-40 level, risk of asthma, and lung function. N Engl J Med 358:1682–1691, 2008. Epub 2008;April 9.
133. Guilloud-Bataille M, Bouzigon E, Annesi-Maesano I, et al: Evidence for linkage of a new region (11p14) to eczema and allergic dis-eases. Hum Genet 122:605–614, 2008. Epub 2007;October 18.
134. Choudhry S, Taub M, Mei R, et al: Genome-wide screen for asthma in Puerto Ricans: Evidence for association with 5q23 region. Hum Genet 123:455–468, 2008. Epub 2008;April 10.
135. Hui J, Oka A, James A, et al:. A genome-wide association scan for asthma in a general Australian population. Hum Genet 123:297–306, 2008. Epub 2008;February 6.
136. Miller RL, Ho SM: Environmental epigenetics and asthma: Current concepts and call for studies. Am J Respir Crit Care Med 177:567–573, 2008. Epub 2008;January 10.
137. Meyers DA, Postma DS, Stine OC, et al: Genome screen for asthma and bronchial hyperresponsiveness: Interactions with passive smoke exposure. J Allergy Clin Immunol 115:1169–1175, 2005.
138. Oates NA, van Vliet J, Duffy DL, et al: Increased DNA methylation at the AXIN1 gene in a monozygotic twin from a pair discordant for a caudal duplication anomaly. Am J Hum Genet 79:155–162, 2006. Epub 2006;May 22.
139. Alati R, Al Mamun A, O’Callaghan M, et al: In utero and postnatal maternal smoking and asthma in adolescence. Epidemiology 17:138–144, 2006.
140. Magnusson LL, Olesen AB, Wennborg H, et al: Wheezing, asthma, hayfever, and atopic eczema in childhood following exposure to tobacco smoke in fetal life. Clin Exp Allergy 35:1550–1556, 2005.
141. Li YF, Langholz B, Salam MT, et al: Maternal and grandmaternal smoking patterns are associated with early childhood asthma. Chest 127:1232–1241, 2005.
142. Emilsson V, Thorleifsson G, Zhang B, et al: Genetics of gene expression and its effect on disease. Nature 452:423–428, 2008. Epub 2008;March 16.
143. Israel E: Genetics and the variability of treatment response in asthma. J Allergy Clin Immunol 115(4 Suppl):S532–S538, 2005.
144. Liggett SB: Polymorphisms of the beta2-adrenergic receptor and asthma. Am J Respir Crit Care Med 156:S156–S162, 1997.
145. Reihsaus E, Innis M, MacIntyre N, et al: Mutations in the gene encoding for the beta 2-adrenergic receptor in normal and asth-matic subjects. Am J Respir Cell Mol Biol 8:334–339, 1993.
146. Israel E, Drazen JM, Liggett SB, et al: The effect of polymorphisms of the beta(2)-adrenergic receptor on the response to regular use of albuterol in asthma. Am J Respir Crit Care Med 162:75–80, 2000.
147. Bleecker ER, Postma DS, Lawrance RM, et al: Effect of ADRB2 polymorphisms on response to longacting beta2-agonist therapy: A pharmacogenetic analysis of two randomised studies. Lancet 370:2118–2125, 2007.
148. Bleecker ER, Yancey SW, Baitinger LA, et al: Salmeterol response is not affected by beta2-adrenergic receptor genotype in subjects with persistent asthma. J Allergy Clin Immunol 118:809–816, 2006. Epub 2006;August 28.
149. Wechsler ME, Lehman E, Lazarus SC, et al: Beta-Adrenergic recep-tor polymorphisms and response to salmeterol. Am J Respir Crit Care Med 173:519–526, 2006. Epub 2005;December 1.
schoolchildren. Respir Med 101:107–117, 2007. Epub 2006; June 2.
105. Landau LI: Tobacco smoke exposure and tracking of lung func-tion into adult life. Paediatr Respir Rev 9:39–43, 2008 [quiz 43–44]. Epub 2008;February 5.
106. Whu R, Cirilo G, Wong J, et al: Risk factors for pediatric asthma in the South Bronx. J Asthma 44:855–859, 2007.
107. Vork KL, Broadwin RL, Blaisdell RJ: Developing asthma in child-hood from exposure to secondhand tobacco smoke: Insights from a meta-regression. Environ Health Perspect 115:1394–1400, 2007.
108. Prescott SL: Effects of early cigarette smoke exposure on early immune development and respiratory disease. Paediatr Respir Rev 9:3–9, 2008 [quiz 10]. Epub 2008;February 5.
109. Guedes HT, Souza LS: Exposure to maternal smoking in the first year of life interferes in breast-feeding protective effect against the onset of respiratory allergy from birth to 5 yr. Pediatr Allergy Immunol 20:30–34, 2009. Epub 2008;January 12.
110. Thomson NC: The role of environmental tobacco smoke in the origins and progression of asthma. Curr Allergy Asthma Rep 7:303–309, 2007.
111. Sadeghnejad A, Karmaus W, Arshad SH, et al: IL13 gene polymor-phisms modify the effect of exposure to tobacco smoke on per-sistent wheeze and asthma in childhood, a longitudinal study. Respir Res 9: 2, 2008.
112. Plaschke PP, Janson C, Norrman E, et al: Onset and remission of allergic rhinitis and asthma and the relationship with atopic sen-sitization and smoking. Am J Respir Crit Care Med 162:920–924, 2000.
113. Polosa R, Knoke JD, Russo C, et al: Cigarette smoking is associ-ated with a greater risk of incident asthma in allergic rhinitis. J Allergy Clin Immunol 121:1428–1434, 2008. Epub 2008; April 24.
114. Sarafino EP, Goldfedder J: Genetic factors in the presence, sever-ity, and triggers of asthma. Arch Dis Child 73:112–116, 1995.
115. Lefkowitz RJ, Caron MG, Stiles GL: Mechanisms of membrane-receptor regulation. Biochemical, physiological, and clinical insights derived from studies of the adrenergic receptors. N Engl J Med 310:1570–1579, 1984.
116. Risch N, Merikangas K: The future of genetic studies of complex human diseases. Science 273:1516–1517, 1996.
117. Asthma mortality and hospitalization among children and young adults—United States, 1980–1993. MMWR Morb Mortal Wkly Rep 45:350–353, 1996.
118. Laitinen T, Polvi A, Rydman P, et al. Characterization of a common susceptibility locus for asthma-related traits. Science 304:300–304, 2004.
119. Nicolae D, Cox NJ, Lester LA, et al: Fine mapping and positional candidate studies identify HLA-G as an asthma susceptibility gene on chromosome 6p21. Am J Hum Genet 76:349–357, 2005. Epub 2004;December 20.
120. Van Eerdewegh P, Little RD, Dupuis J, et al: Association of the ADAM33 gene with asthma and bronchial hyperresponsiveness. Nature 418:426–430, 2002. Epub 2002;July 10.
121. Zhang M, Su X, Mileykovskaya E, et al: Cardiolipin is not required to maintain mitochondrial DNA stability or cell viability for Sac-charomyces cerevisiae grown at elevated temperatures. J Biol Chem 278:35204–35210, 2003.
122. Foley SC, Mogas AK, Olivenstein R, et al: Increased expression of ADAM33 and ADAM8 with disease progression in asthma. J Allergy Clin Immunol 119:863–871, 2007. Epub 2007;March 6.
123. Chen Y, Schnell AH, Rennie DC, et al: Segregation analyses of asthma and respiratory allergy: the Humboldt family study. Am J Med Genet 104:23–30, 2001.
124. Holberg CJ, Halonen M, Wright AL, et al: Familial aggregation and segregation analysis of eosinophil levels. Am J Respir Crit Care Med 160:1604–1610, 1999.
125. Sampogna F, Demenais F, Hochez J, et al: Segregation analysis of IgE levels in 335 French families (EGEA) using different strategies to correct for the ascertainment through a correlated trait (asthma). Genet Epidemiol 18:128–142, 2000.
126. Xu J, Levitt RC, Panhuysen CI, et al: Evidence for two unlinked loci regulating total serum IgE levels. Am J Hum Genet 57:425–430, 1995.

912 OBSTRUCTIVEDISEASES
172. Arock M, Zuany-Amorim C, Singer M, et al: Interleukin-10 inhibits cytokine generation from mast cells. Eur J Immunol 26:166–170, 1996.
173. Steinke JW, Borish L:. Th2 cytokines and asthma. Interleukin-4: Its role in the pathogenesis of asthma, and targeting it for asthma treatment with interleukin-4 receptor antagonists. Respir Res 2:66–70, 2001. Epub 2001;February 19.
174. Brusselle G, Kips J, Joos G, et al: Allergen-induced airway inflam-mation and bronchial responsiveness in wild-type and interleukin-4–deficient mice. Am J Respir Cell Mol Biol 12:254–259, 1995.
175. Wills-Karp M, Luyimbazi J, Xu X, et al: Interleukin-13: Central mediator of allergic asthma. Science 282:2258–2261, 1998.
176. Grunig G, Warnock M, Wakil AE, et al: Requirement for IL-13 independently of IL-4 in experimental asthma. Science 282:2261–2263, 1998.
177. Zhu Z, Homer RJ, Wang Z, et al: Pulmonary expression of inter-leukin-13 causes inflammation, mucus hypersecretion, subepithe-lial fibrosis, physiologic abnormalities, and eotaxin production. J Clin Invest 103:779–788, 1999.
178. van der Pouw Kraan TC, van Veen A, Boeije LC, et al: An IL-13 promoter polymorphism associated with increased risk of allergic asthma. Genes Immun 1:61–65, 1999.
179. Arima K, Umeshita-Suyama R, Sakata Y, et al: Upregulation of IL-13 concentration in vivo by the IL13 variant associated with bronchial asthma. J Allergy Clin Immunol 109:980–987, 2002.
180. Bowler RP, Crapo JD: Oxidative stress in allergic respiratory dis-eases. J Allergy Clin Immunol 110:349–356, 2002.
181. Nakamura H: Thioredoxin and its related molecules: Update 2005. Antioxid Redox Signal 7:823–828, 2005.
182. Bowler RP, Crapo JD: Oxidative stress in airways: Is there a role for extracellular superoxide dismutase? Am J Respir Crit Care Med 166:S38–S43, 2002.
183. De Raeve HR, Thunnissen FB, Kaneko FT, et al: Decreased Cu,Zn-SOD activity in asthmatic airway epithelium: Correction by inhaled corticosteroid in vivo. Am J Physiol 272:L148–L154, 1997.
184. Kharitonov SA, Barnes PJ: Exhaled markers of pulmonary disease. Am J Respir Crit Care Med 163:1693–1722, 2001.
185. Michel T, Feron O: Nitric oxide synthases: Which, where, how, and why? J Clin Invest 100:2146–2152, 1997.
186. Asano K, Chee CB, Gaston B, et al: Constitutive and inducible nitric oxide synthase gene expression, regulation, and activity in human lung epithelial cells. Proc Natl Acad Sci U S A 91:10089–10093, 1994.
187. Nathan C, Xie QW: Nitric oxide synthases: Roles, tolls, and con-trols. Cell 78:915–918, 1994.
188. Dweik RA, Comhair SA, Gaston B, et al: NO chemical events in the human airway during the immediate and late antigen-induced asthmatic response. Proc Natl Acad Sci U S A 98:2622–2627, 2001. Epub 2001;February 20.
189. Jones SL, Kittelson J, Cowan JO, et al: The predictive value of exhaled nitric oxide measurements in assessing changes in asthma control. Am J Respir Crit Care Med 164:738–743, 2001.
190. Smith AD, Cowan JO, Brassett KP, et al. Use of exhaled nitric oxide measurements to guide treatment in chronic asthma. N Engl J Med 352:2163–2173, 2005. Epub 2005;May 24.
191. Que LG, Liu L, Yan Y, et al: Protection from experimental asthma by an endogenous bronchodilator. Science 308:1618–1621, 2005. Epub 2005;May 26.
192. Meurs H, McKay S, Maarsingh H, et al: Increased arginase activity underlies allergen-induced deficiency of cNOS-derived nitric oxide and airway hyperresponsiveness. Br J Pharmacol 136:391–398, 2002.
193. Zimmermann N, King NE, Laporte J, et al: Dissection of experi-mental asthma with DNA microarray analysis identifies arginase in asthma pathogenesis. J Clin Invest 111:1863–1874, 2003.
194. Li H, Romieu I, Sienra-Monge JJ, et al: Genetic polymorphisms in arginase I and II and childhood asthma and atopy. J Allergy Clin Immunol 117:119–126, 2006. Epub 2005;November 28.
195. Montuschi P, Barnes PJ: Exhaled leukotrienes and prostaglandins in asthma. J Allergy Clin Immunol 109:615–620, 2002.
196. Samuelsson B, Dahlen S-E, Lindgren JÅ, et al: Leukotrienes and lipoxins: Structures, biosynthesis, and biological effects. Science 237:1171–1176, 1987.
150. Finotto S, Neurath MF, Glickman JN, et al: Development of spon-taneous airway changes consistent with human asthma in mice lacking T-bet. Science 295:336–338, 2002.
151. Nakamura Y, Christodoulopoulos P, Cameron L, et al: Upregula-tion of the transcription factor GATA-3 in upper airway mucosa after in vivo and in vitro allergen challenge. J Allergy Clin Immunol 105:1146–1152, 2000.
152. Nakamura Y, Ghaffar O, Olivenstein R, et al: Gene expression of the GATA-3 transcription factor is increased in atopic asthma. J Allergy Clin Immunol 103:215–222, 1999.
153. Harrington LE, Hatton RD, Mangan PR, et al: Interleukin 17-pro-ducing CD4+ effector T cells develop via a lineage distinct from the T helper type 1 and 2 lineages. Nat Immunol 6:1123–1132, 2005. Epub 2005;October 2.
154. Ivanov II, McKenzie BS, Zhou L, et al: The orphan nuclear receptor RORgammat directs the differentiation program of proinflammatory IL-17+ T helper cells. Cell 126:1121–1133, 2006.
155. Steinman: A brief history of T(H)17, the first major revision in the T(H)1/T(H)2 hypothesis of T cell-mediated tissue damage. Nat Med 13:139–145, 2007.
156. Gregori S, Giarratana N, Smiroldo S, et al: Dynamics of pathogenic and suppressor T cells in autoimmune diabetes development. J Immunol 171:4040–4047, 2003.
157. Akdis M, Blaser K, Akdis CA: T regulatory cells in allergy: novel concepts in the pathogenesis, prevention, and treatment of aller-gic diseases. J Allergy Clin Immunol 116:961–968, 2005 [quiz 969]. Epub 2005;October 10.
158. Lewkowich IP, Herman NS, Schleifer KW, et al: CD4+CD25+ T cells protect against experimentally induced asthma and alter pulmonary dendritic cell phenotype and function. J Exp Med 202:1549–1561, 2005. Epub 2005;November 28.
159. Levings MK, Sangregorio R, Roncarolo MG: Human cd25(+)cd4(+) t regulatory cells suppress naive and memory T cell pro-liferation and can be expanded in vitro without loss of function. J Exp Med 193:1295–1302, 2001.
160. Weiss ST: Eat dirt—The hygiene hypothesis and allergic diseases. N Engl J Med 347:930–931, 2002.
161. Leckie MJ, ten Brinke A, Khan J, et al: Effects of an interleukin-5 blocking monoclonal antibody on eosinophils, airway hyper-responsiveness, and the late asthmatic response. Lancet 356: 2144–2148, 2000.
162. Larson KA, Olson EV, Madden BJ, et al: Two highly homologous ribonuclease genes expressed in mouse eosinophils identify a larger subgroup of the mammalian ribonuclease superfamily. Proc Natl Acad Sci U S A 93:12370–12375, 1996.
163. Macias MP, Welch KC, Denzler KL, et al: Identification of a new murine eosinophil major basic protein (mMBP) gene: Cloning and characterization of mMBP-2. J Leukoc Biol 67:567–576, 2000.
164. Horton MA, Larson KA, Lee JJ, et al: Cloning of the murine eosi-nophil peroxidase gene (mEPO): Characterization of a conserved subgroup of mammalian hematopoietic peroxidases. J Leukoc Biol 60:285–294, 1996.
165. Humbles AA, Lloyd CM, McMillan SJ, et al: A critical role for eosinophils in allergic airways remodeling. Science 305:1776–1779, 2004.
166. Lee JJ, Dimina D, Macias MP, et al: Defining a link with asthma in mice congenitally deficient in eosinophils. Science 305:1773–1776, 2004.
167. Wills-Karp M, Karp CL: Biomedicine. Eosinophils in asthma: remodeling a tangled tale. Science 305:1726–1729, 2004.
168. Robinson DS, Hamid Q, Ying S, et al: Predominant TH2-type bronchoalveolar lavage T-lymphocyte activation in atopic asthma. N Engl J Med 326:298–304, 1992.
169. Greenfeder S, Umland SP, Cuss FM, et al: Th2 cytokines and asthma. The role of interleukin-5 in allergic eosinophilic disease. Respir Res 2:71–79, 2001. Epub 2001;March 8.
170. Longphre M, Li D, Gallup M, et al: Allergen-induced IL-9 directly stimulates mucin transcription in respiratory epithelial cells. J Clin Invest 104:1375–1382, 1999.
171. Schandene L, Alonso-Vega C, Willems F, et al: B7/CD28-depend-ent IL-5 production by human resting T cells is inhibited by IL-10. J Immunol 152:4368–4374, 1994.

38 ASTHMA 913
221. Knight D: Increased permeability of asthmatic epithelial cells to pollutants. Does this mean that they are intrinsically abnormal? Clin Exp Allergy 32:1263–1265, 2002.
222. Bucchieri F, Puddicombe SM, Lordan JL, et al: Asthmatic bron-chial epithelium is more susceptible to oxidant-induced apopto-sis. Am J Respir Cell Mol Biol 27:179–185, 2002.
223. Schleimer RP, Kato A, Kern R, et al: Epithelium: At the interface of innate and adaptive immune responses. J Allergy Clin Immunol 120:1279–1284, 2007.
224. Hackett TL, Knight DA: The role of epithelial injury and repair in the origins of asthma. Curr Opin Allergy Clin Immunol 7:63–68, 2007.
225. Holgate ST: The airway epithelium is central to the pathogenesis of asthma. Allergol Int 57:1–10, 2008.
226. Phipps S, Benyahia F, Ou T-T, et al: Acute allergen-induced airway remodeling in atopic athma. Am J Respir Cell Mol Biol 31:626–632, 2004.
227. Roche WR, Beasley R, Williams JH, et al: Subepithelial fibrosis in the bronchi of asthmatics. Lancet 1:520–524, 1989.
228. Laitinen A, Altraja A, Kampe M, et al: Tenascin is increased in airway basement membrane of asthmatics and decreased by an inhaled steroid. Am J Respir Crit Care Med 156:951–958, 1997.
229. Karjalainen EM, Lindqvist A, Laitinen LA, et al: Airway inflamma-tion and basement membrane tenascin in newly diagnosed atopic and nonatopic asthma. Respir Med 97:1045–1051, 2003.
230. Slade DJ, Kraft M: Airway remodeling from bench to bedside: Current perspectives. Clin Chest Med 27:71–85, 2006.
231. Payne DN, Rogers AV, Adelroth E, et al: Early thickening of the reticular basement membrane in children with difficult asthma. Am J Respir Crit Care Med 167:78–82, 2003.
232. Saglani S, Malmstrom K, Pelkonen AS, et al: Airway remodeling and inflammation in symptomatic infants with reversible airflow obstruction. Am J Respir Crit Care Med 171:722–727, 2005.
233. Covar RA, Spahn JD, Murphy JR, et al: Progression of asthma measured by lung function in the Childhood Asthma Management Program. Am J Respir Crit Care Med 170:234–241, 2006. Epub 2004;March 17.
234. Martinez FD, Wright AL, Taussig LM, et al: Asthma and wheezing in the first six years of life. The Group Health Medical Associates. N Engl J Med 332:133–138, 1995.
235. Locke NR, Royce SG, Wainewright JS, et al: Comparison of airway remodeling in acute, subacute, and chronic models of allergic airways disease. Am J Respir Cell Mol Biol 36:625–632, 2007.
236. van den Toorn LM, Overbeek SE, de Jongste JC, et al: Airway inflammation is present during clinical remission of atopic asthma. Am J Respir Crit Care Med 164:2107–2113, 2001.
237. Lewis CC, Chu HW, Westcott JY, et al: Increased expression of platelet-derived growth factor receptor-beta in airway fibroblasts of severe asthmatics. Chest 123(3 Suppl):428S–429S, 2003.
238. Lewis CC, Chu HW, Westcott JY, et al: Airway fibroblasts exhibit a synthetic phenotype in severe asthma. J Allergy Clin Immunol 115:534–540, 2005.
238a. Ho I, Fixman ED, Asai K, et al: Platelet-derived growth factor and transforming growth factor-beta modulate the expression of matrix metalloproteinases and migratory function of human airway smooth muscle cells. Clin Exp Allergy 39:1370–1380, 2009.
239. Palmans E, Kips JC, Pauwels RA: Prolonged allergen exposure induces structural airway changes in sensitized rats. Am J Respir Crit Care Med 161:627–635, 2000.
240. Blyth DI, Wharton TF, Pedrick MS, et al: Airway subepithelial fibrosis in a murine model of atopic asthma: Suppression by dexamethasone or anti-interleukin-5 antibody. Am J Respir Cell Mol Biol 23:241–246, 2000.
241. Gelb AF, Licuanan J, Shinar CM, et al: Unsuspected loss of lung elastic recoil in chronic persistent asthma. Chest 121:715–721, 2002.
242. Mauad T, Xavier ACG, Saldiva PHN, et al. Elastosis and fragmenta-tion of fibers of the elastic system in fatal asthma. Am J Respir Crit Care Med 160:968–975, 1999.
243. Mauad T, Silva LFF, Santos MA, et al: Abnormal alveolar attach-ments with decreased elastic fiber content in distal lung in fatal asthma. Am J Respir Crit Care Med 170:857–862, 2004.
197. Kumlin M, Dahlen B, Bjorck T, et al: Urinary excretion of leuko-triene E4 and 11-dehydro-thromboxane B2 in response to bron-chial provocations with allergen, aspirin, leukotriene D4, and histamine in asthmatics. Am Rev Respir Dis 146:96–103, 1992.
198. Reiss TF, Hill JB, Harman E, et al: Increased urinary excretion of LTE4 after exercise and attenuation of exercise-induced bronchos-pasm by montelukast, a cysteinyl leukotriene receptor antagonist. Thorax 52:1030–1035, 1997.
199. Christie PE, Tagari P, Ford-Hutchinson AW, et al: Urinary leukot-riene E4 concentrations increase after aspirin challenge in aspirin-sensitive asthmatic subjects. Am Rev Respir Dis 143:1025–1029, 1991.
200. Kanaoka Y, Boyce JA:. Cysteinyl leukotrienes and their receptors: Cellular distribution and function in immune and inflammatory responses. J Immunol 173:1503–1510, 2004.
201. Bergeron C, Boulet LP: Structural changes in airway diseases: Characteristics, mechanisms, consequences, and pharmacologic modulation. Chest 129:1068–1087, 2006.
202. Boulet LP, Laviolette M, Turcotte H, et al: Bronchial subepithelial fibrosis correlates with airway responsiveness to methacholine. Chest 112:45–52, 1997.
203. Little SA, Sproule MW, Cowan MD, et al: High resolution com-puted tomographic assessment of airway wall thickness in chronic asthma: Reproducibility and relationship with lung func-tion and severity. Thorax 57:247–253, 2002.
204. Aysola RS, Hoffman EA, Gierada D, et al: Airway remodeling measured by multidetector computed tomography is increased in severe asthma and correlates with pathology. Chest 134:1183–1191, 2008.
205. Davies DE, Wicks J, Powell RM, et al: Airway remodeling in asthma: New insights. J Allergy Clin Immunol 111:215, 2003.
206. Paganin F, Séneterre E., Chanez P, et al: Computed tomography of the lungs in asthma: Influence of disease severity and etiology. Am J Respir Crit Care Med 153:110–114, 1996.
207. Nakano Y, Müller NL, King GG, et al: Quantitative assessment of airway remodeling using high-resolution CT. Chest 122(6 Suppl):271S–S275, 2002.
208. Leigh R, Ellis R, Wattie J, et al: Dysfunction and remodeling of the mouse airway persist after resolution of acute allergen-induced airway inflammation. Am J Respir Cell Mol Biol 27:526–535, 2002.
209. Ramos-Barbon D, Presley JF, Hamid QA, et al: Antigen-specific CD4+ T cells drive airway smooth muscle remodeling in experi-mental asthma. J Clin Invest 115:1580–1589, 2005.
210. Elias JA, Zheng T, Lee CG, et al: Transgenic modeling of inter-leukin-13 in the lung. Chest 123(3 Suppl): 339S–S345, 2003.
211. Henderson WR Jr, Tang LO, Chu SJ, et al. A role for cysteinyl leukotrienes in airway remodeling in a mouse asthma model. Am J Respir Crit Care Med 165:108–116, 2002.
212. Kuperman DA, Huang X, Koth LL, et al: Direct effects of inter-leukin-13 on epithelial cells cause airway hyperreactivity and mucus overproduction in asthma. Nat Med 8:885–889, 2002.
213. Cohn L, Elias JA, Chupp GL: Asthma: Mechanisms of disease persistence and progression. Annu Rev Immunol 22:789–815, 2004.
214. Pepe C, Foley S, Shannon J, et al: Differences in airway remode-ling between subjects with severe and moderate asthma. J Allergy Clin Immunol 116:544–549, 2005.
215. Roche WR, Montefort S, Baker J, et al: Cell adhesion molecules and the bronchial epithelium. Am Rev Respir Dis 148:S79–S82, 1993.
216. Holgate ST: Epithelium dysfunction in asthma. J Allergy Clin Immunol 120:1233–1244, 2007 [quiz 1245–1246].
217. Fedorov IA, Wilson SJ, Davies DE, et al: Epithelial stress and structural remodelling in childhood asthma. Thorax 60:389–394, 2005.
218. Ordonez C, Ferrando R, Hyde DM, et al: Epithelial desquamation in asthma: Artifact or pathology? Am J Respir Crit Care Med 162:2324–2329, 2000.
219. Shebani E, Shahana S, Janson C, et al: Attachment of columnar airway epithelial cells in asthma. Tissue Cell 37:145–152, 2005.
220. Kicic A, Sutanto EN, Stevens PT, et al: Intrinsic biochemical and functional differences in bronchial epithelial cells of children with asthma. Am J Respir Crit Care Med 174:1110–1118, 2006.

914 OBSTRUCTIVEDISEASES
267. Brightling CE, Bradding P, Symon FA, et al: Mast-cell infiltration of airway smooth muscle in asthma. N Engl J Med 346:1699–1705, 2002.
268. Berry M, Morgan A, Shaw DE, et al: Pathological features and inhaled corticosteroid response of eosinophilic and non-eosi-nophilic asthma. Thorax 62:1043–1049, 2007.
269. Page S, Ammit AJ, Black JL, et al: Human mast cell and airway smooth muscle cell interactions: Implications for asthma. Am J Physiol Lung Cell Mol Physiol 281:L1313–L1323, 2001.
270. Hollins F, Kaur D, Yang W. et al: Human airway smooth muscle promotes human lung mast cell survival, proliferation, and con-stitutive activation: Cooperative roles for CADM1, stem cell factor, and IL-6. J Immunol 181:2772–2780, 2008.
271. Williams OW, Sharafkhaneh A, Kim V, et al: Airway mucus: From production to secretion. Am J Respir Cell Mol Biol 34:527–536, 2006.
272. Fahy JV: Goblet cell and mucin gene abnormalities in asthma. Chest 122(6 Suppl):320S–326S, 2002.
273. Kuyper LM, Pare PD, Hogg JC, et al: Characterization of airway plugging in fatal asthma. Am J Med 115:6–11, 2003.
274. Aikawa T, Shimura S, Sasaki H, et al: Marked goblet cell hyper-plasia with mucus accumulation in the airways of patients who died of severe acute asthma attack. Chest 101:916–921, 1992.
275. Sheehan JK, Howard M, Richardson PS, et al: Physical charac-terization of a low-charge glycoform of the MUC5B mucin com-prising the gel-phase of an asthmatic respiratory mucous plug. Biochem J 338:507–513, 1999.
276. Rogers DF, Barnes PJ: Treatment of airway mucus hypersecretion. Ann Med 38:116–125, 2006.
277. Ordonez CL, Khashayar R, Wong HH, et al: Mild and moderate asthma is associated with airway goblet cell hyperplasia and abnormalities in mucin gene expression. Am J Respir Crit Care Med 163:517–523, 2001.
278. Kirkham S, Sheehan JK, Knight D, et al: Heterogeneity of airways mucus: Variations in the amounts and glycoforms of the major oligomeric mucins MUC5AC and MUC5B. Biochem J 361:537–546, 2002.
279. Sheehan JK, Richardson PS, Fung DC, et al: Analysis of respiratory mucus glycoproteins in asthma: A detailed study from a patient who died in status asthmaticus. Am J Respir Cell Mol Biol 13:748–756, 1995.
280. Shimura S, Andoh Y, Haraguchi M, et a: Continuity of airway goblet cells and intraluminal mucus in the airways of patients with bronchial asthma. Eur Respir J 9:1395–1401, 1996.
281. Li Y, Martin LD, Spizz G, et al: MARCKS protein is a key molecule regulating mucin secretion by human airway epithelial cells in vitro. J Biol Chem 276:40982–40990, 2001.
282. Park JA, Crews AL, Lampe WR, et al: Protein kinase C delta regu-lates airway mucin secretion via phosphorylation of MARCKS protein. Am J Pathol 171:1822–1830, 2007.
283. Chu HW, Balzar S, Seedorf GJ, et al: Transforming growth factor-beta2 induces bronchial epithelial mucin expression in asthma. Am J Pathol 165:1097–1106, 2004.
284. Wu Q, Martin RJ, Rino JG, et al: A deficient TLR2 signaling pro-motes airway mucin production in Mycoplasma pneumoniae–infected allergic mice. Am J Physiol Lung Cell Mol Physiol 292:L1064–L1072, 2007.
285. Li L, Kaplan J: Characterization of two homologous yeast genes that encode mitochondrial iron transporters. J Biol Chem 272:28485–28493, 1997.
286. Kanazawa H, Asai K, Hirata K, et al. Vascular involvement in exercise-induced airway narrowing in patients with bronchial asthma. Chest 122:166–170, 2002.
287. Hoshino M, Nakamura Y, Hamid QA: Gene expression of vascular endothelial growth factor and its receptors and angiogenesis in bronchial asthma. J Allergy Clin Immunol 107:1034–1038, 2001.
288. Chetta A, Zanini A, Foresi A. et al: Vascular endothelial growth factor up-regulation and bronchial wall remodelling in asthma. Clin Exp Allergy 35:1437–1442., 2005.
289. Faffe DS, Flynt L, Bourgeois K, et al: Interleukin-13 and inter-leukin-4 induce vascular endothelial growth factor release from airway smooth muscle cells: Role of vascular endothelial growth factor genotype. Am J Respir Cell Mol Biol 34:213–218, 2006. Epub 2005;October 6.
244. Shi W, Bellusci S, Warburton D: Lung development and adult lung diseases. Chest 132:651–656, 2007.
245. Slats AM, Janssen K, van Schadewijk A, et al: Expression of smooth muscle and extracellular matrix proteins in relation to airway function in asthma. J Allergy Clin Immunol 121:1196, 2008.
246. Pham DN, Chu HW, Martin RJ, et al: Increased matrix metallo-proteinase-9 with elastolysis in nocturnal asthma. Ann Allergy Asthma Immunol 90:72–78, 2003.
247. Kenyon NJ, Ward RW, McGrew G, et al: TGF-beta1 causes airway fibrosis and increased collagen I and III mRNA in mice. Thorax 58:772–777, 2003.
248. Cho JY, Miller M, Baek KJ, et al: Inhibition of airway remodeling in IL-5–deficient mice. J Clin Invest 113:551–560, 2004.
249. Finotto S, Hausding M, Doganci A, et al. Asthmatic changes in mice lacking T-bet are mediated by IL-13. Int Immunol 17:993–1007, 2005.
250. McMillan SJ, Xanthou G, Lloyd CM: Manipulation of allergen-induced airway remodeling by treatment with anti-TGF-beta antibody: Effect on the Smad signaling pathway. J Immunol 174:5774–5780, 2005.
251. Flood-Page P, Menzies-Gow A, Phipps S, et al: Anti-IL-5 treatment reduces deposition of ECM proteins in the bronchial subepithelial basement membrane of mild atopic asthmatics. J Clin Invest 112:1029–1036, 2003.
252. Kelly MM, Leigh R, Bonniaud P, et al: Epithelial expression of profibrotic mediators in a model of allergen-induced airway remodeling. Am J Respir Cell Mol Biol 32:99–107, 2005.
253. Lee JH, Haselkorn T, Borish L, et al: Risk factors associated with persistent airflow limitation in severe or difficult-to-treat asthma: Insights from the TENOR study. Chest 132:1882–1889, 2007.
254. Kraft M, Cairns CB, Ellison MC, et al: Improvements in distal lung function correlate with asthma symptoms after treatment with oral montelukast. Chest 130:1726–1732, 2006.
255. Armour CL, Black JL, Berend N, et al: The relationship between bronchial hyperresponsiveness to methacholine and airway smooth muscle structure and reactivity. Respir Physiol 58:223–233, 1984.
256. James AL, Pare PD, Hogg JC: The mechanics of airway narrowing in asthma. Am Rev Respir Dis 139:242–246, 1989.
257. Lambert RK, Wiggs BR, Kuwano K, et al: Functional significance of increased airway smooth muscle in asthma and COPD. J Appl Physiol 74:2771–2781, 1993.
258. Sapienza S, Du T, Eidelman DH, et al: Structural changes in the airways of sensitized brown Norway rats after antigen challenge. Am Rev Respir Dis 144:423–427, 1991.
259. Benayoun L, Druilhe A, Dombret MC, et al: Airway structural alterations selectively associated with severe asthma. Am J Respir Crit Care Med 167:1360–1368, 2003.
260. Carroll N, Elliot J, Morton A, et al: The structure of large and small airways in nonfatal and fatal asthma. Am Rev Respir Dis 147:405–410, 1993.
261. Black JL, Burgess JK, Johnson PR: Airway smooth muscle—Its relationship to the extracellular matrix. Respir Physiol Neurobiol 137:339–346, 2003.
262. Johnson PR, Burgess JK, Underwood PA, et al: Extracellular matrix proteins modulate asthmatic airway smooth muscle cell proliferation via an autocrine mechanism. J Allergy Clin Immunol 113:690–696, 2004.
263. Panettieri RA Jr, Murray RK, Eszterhas AJ, et al: Repeated aller-gen inhalations induce DNA synthesis in airway smooth muscle and epithelial cells in vivo. Am J Physiol 274:L417–L424., 1998.
264. Woodruff PG, Dolganov GM, Ferrando RE, et al: Hyperplasia of smooth muscle in mild to moderate asthma without changes in cell size or gene expression. Am J Respir Crit Care Med 169:1001–1006, 2004.
265. Moir LM, Leung SY, Eynott PR, et al: Repeated allergen inhalation induces phenotypic modulation of smooth muscle in bronchioles of sensitized rats. Am J Physiol Lung Cell Mol Physiol 284:L148–L159, 2003.
266. Woodruff PG: Gene expression in asthmatic airway smooth muscle. Proc Am Thorac Soc 5:113–118, 2008.

38 ASTHMA 915
reversal of obstruction with bronchodilation. J Appl Physiol 104:394–403, 2008.
312. Adler A, Cowley EA, Bates JH, et al: Airway-parenchymal interde-pendence after airway contraction in rat lung explants. J Appl Physiol 85:231–237, 1998.
313. Bai TR, Knight DA: Structural changes in the airways in asthma: Observations and consequences. Clin Sci 108:463–477, 2005.
314. Martin J, Powell E, Shore S, et al: The role of respiratory muscles in the hyperinflation of bronchial asthma. Am Rev Respir Dis 121:441–447, 1980.
315. McFadden ER Jr, Kiser R, DeGroot WJ: Acute bronchial asthma. Relations between clinical and physiologic manifestations. N Engl J Med 288:221–225, 1973.
316. O’Donnell DE, Bertley JC, Chau LK, et al: Qualitative aspects of exertional breathlessness in chronic airflow limitation: Patho-physiologic mechanisms. Am J Respir Crit Care Med 155:109–115, 1997.
317. Venegas JG, Schroeder T, Harris S, et al: The distribution of ventilation during bronchoconstriction is patchy and bimodal: A PET imaging study. Respir Physiol Neurobiol 148:57–64, 2005.
318. Wagner PD, Hedenstierna G, Rodriguez-Roisin R: Gas exchange, expiratory flow obstruction and the clinical spectrum of asthma. Eur Respir J 9:1278–1282, 1996.
319. Tai E, Read J: Blood-gas tensions in bronchial asthma. Lancet 1:644–646, 1967.
320. Rodriguez-Roisin R, Roca J: Contributions of multiple inert gas elimination technique to pulmonary medicine.3. Bronchial asthma. Thorax 49:1027–1033, 1994.
321. Mcfadden E: Hypoxemia and hypocapnia in asthma. N Engl J Med 278:1068, 1968.
322. Cherniack RM: Physiologic diagnosis and function in asthma. Clin Chest Med 16:567–581, 1995.
323. McFadden ER Jr: Acute severe asthma. Am J Respir Crit Care Med 168:740–759, 2003.
324. Brand PL, Duiverman EJ, Waalkens HJ, et al: Peak flow variation in childhood asthma: Correlation with symptoms, airways obstruction, and hyperresponsiveness during long-term treat-ment with inhaled corticosteroids. Dutch CNSLD Study Group. Thorax 54:103–107, 1999.
325. Llewellin P, Sawyer G, Lewis S, et al: The relationship between FEV1 and PEF in the assessment of the severity of airways obstruc-tion. Respirology 7:333–337, 2002.
326. Aggarwal AN, Gupta D, Jindal SK: The relationship between FEV1 and peak expiratory flow in patients with airways obstruction is poor. Chest 130:1454–1461, 2006.
327. Reddel HK, Marks GB, Jenkins CR: When can personal best peak flow be determined for asthma action plans? Thorax 59:922–924, 2004.
328. Bateman ED, Hurd SS, Barnes PJ, et al: Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J 31:143–178, 2008.
329. Taylor DR, Town GI, Herbison GP, et al: Asthma control during long-term treatment with regular inhaled salbutamol and salme-terol. Thorax 53:744–752, 1998.
330. Frey U, Brodbeck T, Majumdar A, et a: Risk of severe asthma episodes predicted from fluctuation analysis of airway function. Nature 438:667–670, 2005.
331. Pellegrino R, Viegi G, Brusasco V, et al: Interpretative strategies for lung function tests. Eur Respir J 26:948–968, 2005.
332. Nowak RM, Tomlanovich MC, Sarkar DD, et al: Arterial blood gases and pulmonary function testing in acute bronchial asthma. Predicting patient outcomes. JAMA 249:2043–2046, 1983.
333. Fuhlbrigge AL, Weiss ST, Kuntz KM, et al: Forced expiratory volume in 1 second percentage improves the classification of severity among children with asthma. Pediatrics 118:e347–e355, 2006.
334. Moore WC, Bleecker ER, Curran-Everett D, et al: Characterization of the severe asthma phenotype by the National Heart, Lung, and Blood Institute’s Severe Asthma Research Program. J Allergy Clin Immunol 119:405, 2007.
335. Burns GP, Gibson GJ: A novel hypothesis to explain the bronch-constrictor effect of deep inspiration in asthma. Thorax 57:116–119, 2002.
290. Simcock DE, Kanabar V, Clarke GW, et al: Induction of angiogen-esis by airway smooth muscle from patients with asthma. Am J Respir Crit Care Med 178:460–468, 2008. Epub 2008;June 12.
291. Hasaneen NA, Zucker S, Lin RZ, et al: Angiogenesis is induced by airway smooth muscle strain. Am J Physiol Lung Cell Mol Physiol 293:L1059–L1068, 2007. Epub 2007;August 10.
292. Lee JW, Ovadia B, Azakie A, et al: Increased pulmonary blood flow does not alter surfactant protein gene expression in lambs within the first week of life. Am J Physiol Lung Cell Mol Physiol 286:L1237–L1243, 2004.
293. Crimi E, Spanevello A, Neri M, et al: Dissociation between airway inflammation and airway hyperresponsiveness in allergic asthma. Am J Respir Crit Care Med 157:4–9, 1998.
294. Grunstein MM, Hakonarson H, Leiter J, et al: IL-13–dependent autocrine signaling mediates altered responsiveness of IgE-sensi-tized airway smooth muscle. Am J Physiol Lung Cell Mol Physiol 282:L520–L528, 2002.
295. Hakonarson H, Herrick DJ, Serrano PG, et al: Autocrine role of interleukin 1beta in altered responsiveness of atopic asthmatic sensitized airway smooth muscle. J Clin Invest 99:117–124, 1997.
296. Hogg JC: Pathology of asthma. J Allergy Clin Immunol 92:1–5, 1993.
297. Ebina M, Takahashi T, Chiba T, et al: Cellular hypertrophy and hyperplasia of airway smooth muscles underlying bronchial asthma. A 3-D morphometric study. Am Rev Respir Dis 148:720–726, 1993.
298. McParland BE, Tait RR, Pare PD, et al: The role of airway smooth muscle during an attack of asthma simulated in vitro. Am J Respir Cell Mol Biol 33:500–504, 2005. Epub 2005;July 29.
299. Hirst SJ, Martin JG, Bonacci JV, et al: Proliferative aspects of airway smooth muscle. J Allergy Clin Immunol 114(2 Suppl):S2–S17, 2004.
300. An SS, Bai TR, Bates JH, et al: Airway smooth muscle dynamics: A common pathway of airway obstruction in asthma. Eur Respir J 29:834–860, 2007.
300a. Blach JL, Roth M: Intrinsic asthma: Is it intrinsic to the smooth muscle? Clin Exp Allergy 39:962–965, 2009.
301. Cho W, Stahelin R: Membrane protein interactions in cell signal-ing and membrane trafficking. Annu Rev Biophys Biomol Struct 34:119–151, 2005.
302. Henderson WR Jr, Chiang GK, Tien YT, et al: Reversal of allergen-induced airway remodeling by CysLT1 receptor blockade. Am J Respir Crit Care Med 173:718–728, 2006.
303. Danek CJ, Lombard CM, Dungworth DL, et al: Reduction in airway hyperresponsiveness to methacholine by the application of RF energy in dogs. J Appl Physiol 97:1946–1953, 2004.
304. Cox L, Platts-Mills TA, Finegold I, et al: American Academy of Allergy, Asthma & Immunology/American College of Allergy, Asthma and Immunology Joint Task Force Report on omalizumab-associated anaphylaxis. J Allergy Clin Immunol 120:1373–1377, 2007.
304a. Holgate ST: Novel targets of therapy in asthma. Curr Opin Pulm Med 15:63–71, 2009.
305. Ratnovsky A, Mellema M, An SS, et al: Airway smooth muscle proliferation and mechanics: Effects of AMP kinase agonists. Mol Cell Biomech 4:143–157, 2007.
306. Simoes DCM, Vassilakopoulos T, Toumpanakis D, et al: Angiopoi-etin-1 protects against airway inflammation and hyperreactivity in asthma. Am J Respir Crit Care Med 177:1314–1321, 2008.
307. Kessler GF, Austin JH, Graf PD, et al: Airway constriction in experimental asthma in dogs: Tantalum bronchographic studies. J Appl Physiol 35:703–708, 1973.
308. Brown RH, Pearse DB, Pyrgos G, et al: The structural basis of airways hyperresponsiveness in asthma. J Appl Physiol 101:30–39, 2006.
309. Pellegrino R, Violante B, Nava S, et al: Expiratory airflow limita-tion and hyperinflation during methacholine-induced bronchoc-onstriction. J Appl Physiol 75:1720–1727, 1993.
310. Wagers SS, Jaffe EF, Irvin CG: Development structure and physiol-ogy in normal and asthmatic lung. In Adkinson Jr NY, Yunginger JW, Busse WW, et al (eds): Middleton’s Allergy: Principles and Practice. St. Louis: Mosby, 2003.
311. Sorkness RL, Bleecker ER, Busse WW, et al: Lung function in adults with stable but severe asthma: Air trapping and incomplete

916 OBSTRUCTIVEDISEASES
360. Boulet LP, Boulet V, Milot J: How should we quantify asthma control? A proposal. Chest 122:2217–2223, 2002.
361. Pillai SG, Tang Y, van den Oord E, et al: Factor analysis in the Genetics of Asthma International Network family study identifies five major quantitative asthma phenotypes. Clin Exp Allergy 38:421–429, 2008.
362. Osborne ML, Pedula KL, O’Hollaren M, et al: Assessing future need for acute care in adult asthmatics: The Profile of Asthma Risk Study: A prospective health maintenance organization-based study. Chest 132:1151–1161, 2007.
363. Bacci E, Cianchetti S, Bartoli M, et al: Low sputum eosinophils predict the lack of response to beclomethasone in symptomatic asthmatic patients. Chest 129:565–572, 2006.
364. Green RH, Brightling CE, McKenna S, et al: Asthma exacerbations and sputum eosinophil counts: A randomised controlled trial. Lancet 360:1715–1721, 2002.
365. Kips J: Managing a variable disease. Pulm Pharmacol Ther 15:485–490, 2002.
366. Deykin A, Lazarus SC, Fahy JV, et al: Sputum eosinophil counts predict asthma control after discontinuation of inhaled corticos-teroids. J Allergy Clin Immunol 115:720–727, 2005.
367. Travers J, Marsh S, Aldington S, et al: Reference ranges for exhaled nitric oxide derived from a random community survey of adults. Am J Respir Crit Care Med 176:238–242, 2007.
368. Olin AC, Rosengren A, Thelle DS, et al: Height, age, and atopy are associated with fraction of exhaled nitric oxide in a large adult general population sample. Chest 130:1319–1325, 2006.
369. Kharitonov SA, Yates DH, Barnes PJ: Inhaled glucocorticoids decrease nitric oxide in exhaled air of asthmatic patients. Am J Respir Crit Care Med 153:454–457, 1996.
370. Silkoff PE, McClean P, Spino M, et al: Dose-response relationship and reproducibility of the fall in exhaled nitric oxide after inhaled beclomethasone dipropionate therapy in asthma patients. Chest 119:1322–1328, 2001.
371. Michils A, Baldassarre S, Van Muylem A: Exhaled nitric oxide and asthma control: A longitudinal study in unselected patients. Eur Respir J 31:539–546, 2008.
372. Sun JG, Deng YM, Wu X, et al: Inhibition of phosphodiesterase activity, airway inflammation and hyperresponsiveness by PDE4 inhibitor and glucocorticoid in a murine model of allergic asthma. Life Sci 79:2077–2085, 2006.
373. Volovitz B: Inhaled budesonide in the management of acute wors-enings and exacerbations of asthma: A review of the evidence. Respir Med 101:685, 2007.
374. NHLBI/NIH. (National Institutes of Health, National Asthma Education and Prevention Program, 2007). Managing asthma long term in children 0–4 years of age and 5–11 years of age. Available at http://www.nhlbi.nih.gov/guidelines/asthma/08_Sec4_lt_0-11.pdf
375. GINA Report: Global Strategy for Asthma Management and Pre-vention, Global Initiative for Asthma (GINA), 2007. Available at http://www.ginasthma.com/Guidelineitem.asp?l1=2&l2=1&intId=60. Bethesda, MD: NIH, Publication No. 02-3659.
376. Bielory L, Lupoli K: Herbal interventions in asthma and allergy. J Asthma 36:1–65, 1999.
377. Sears MR, Lotvall J: Past, present and future—Beta2-adrenoceptor agonists in asthma management. Respir Med 99:152–170, 2005.
378. Johnson M: Molecular mechanisms of [beta]2-adrenergic receptor function, response, and regulation. J Allergy Clin Immunol 117: 18, 2006.
379. Zink S, Rosen P, Sackmann B, et al: Regulation of endothelial permeability by beta-adrenoceptor agonists: Contribution of beta 1- and beta 2-adrenoceptors. Biochim Biophys Acta 1178:286–298, 1993.
380. Johnson M: The beta-adrenoceptor. Am J Respir Crit Care Med 158:146S–153S, 1998.
381. Ahrens R, Weinberger M: Levalbuterol and racemic albuterol: Are there therapeutic differences? J Allergy Clin Immunol 108:681–684, 2001.
382. Walters EH, Gibson PG, Lasserson TJ, et al: Long-acting beta2-agonists for chronic asthma in adults and children where back-ground therapy contains varied or no inhaled corticosteroid. Cochrane Database Syst Rev 1:CD001385, 2007.
336. Lutchen KR, Jensen A, Atileh H, et al: Airway constriction pattern is a central component of asthma severity. The role of deep inspirations. Am J Respir Crit Care Med 164:207–215, 2001.
337. McFadden ER, Linden DA: A reduction in maximum and mid-expiratory flow rate. A spirometric manifestation of small airway disease. Am J Med 52:725–737, 1972.
338. Marseglia GL, Cirillo I, Vizzaccaro A, et al: Role of forced expira-tory flow at 25–75% as an early marker of small airways impair-ment in subjects with allergic rhinitis. Allergy Asthma Proc 28:74–78, 2007.
339. Chiang CH, Hsu K: Residual abnormalities of pulmonary function in asymptomatic young adult asthmatics with childhood-onset asthma. J Asthma 34:15–21, 1997.
340. Hansen JE, Sun XG, Wasserman K: Should forced expiratory volume in six seconds replace forced vital capacity to detect airway obstruction? Eur Respir J 27:1244–1250, 2006.
341. Ferguson GT, Enright PL, Buist AS, et al: Office spirometry for lung health assessment in adults: A consensus statement from the National Lung Health Education Program. Chest 117:1146–1161, 2000.
342. Vandevoorde J, Verbanck S, Schuermans D, et al: Obstructive and restrictive spirometric patterns: fixed cut-offs for FEV1/FEV6 and FEV6. Eur Respir J 27:378–383, 2006.
343. Hansen JE, Sun XG, Wasserman K: Discriminating measures and normal values for expiratory obstruction. Chest 129:369–377, 2006.
344. Punjabi NM, Shade D, Wise RA: Correction of single-breath helium lung volumes in patients with airflow obstruction. Chest 114:907–918, 1998.
345. Brown R, Hoppin FG Jr, Ingram RH Jr, et al: Influence of abdom-inal gas on the Boyle’s law determination of thoracic gas volume. J Appl Physiol 44:469–473, 1978.
346. Saydain G, Beck KC, Decker PA, et al: Clinical significance of elevated diffusing capacity. Chest 125:446–452, 2004.
347. Collard P, Njinou B, Nejadnik B, et al: Single breath diffusing capacity for carbon monoxide in stable asthma. Chest 105:1426–1429, 1994.
348. Guidelines for Methacholine and Exercise Challenge Testing—1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med 161:309–329, 2000.
349. Josephs LK, Gregg I, Mullee MA, et al: Nonspecific bronchial reactivity and its relationship to the clinical expression of asthma. A longitudinal study. Am Rev Respir Dis 140:350–357, 1989.
350. Jansen DF, Schouten JP, Vonk JM, et al: Smoking and airway hyperresponsiveness especially in the presence of blood eosi-nophilia increase the risk to develop respiratory symptoms: A 25-year follow-up study in the general adult population. Am J Respir Crit Care Med 160:259–264, 1999.
351. Holzer K, Brukner P, Douglass J: Evidence-based management of exercise-induced asthma. Curr Sports Med Rep 1:86–92, 2002.
352. Benckhuijsen J, van den Bos JW, van Velzen E, et al: Differences in the effect of allergen avoidance on bronchial hyperresponsive-ness as measured by methacholine, adenosine 5′-monophos-phate, and exercise in asthmatic children. Pediatr Pulmonol 22:147–153, 1996.
353. Death from asthma in two regions of England. British Thoracic Association. Br Med J (Clin Res Ed) 285:1251–1255, 1982.
354. Bucknall CE, Moran F, Stevenson RD: A retrospective survey of asthma management in hospital. Scott Med J 33:328–330, 1988.
355. Sheffer AL: The National Asthma Education Program attacks asthma. J Allergy Clin Immunol 87:468–469, 1991.
356. Chen H, Gould MK, Blanc PD, et al: Asthma control, severity, and quality of life: Quantifying the effect of uncontrolled disease. J Allergy Clin Immunol 120:396–402, 2007.
357. Juniper EF, O’Byrne PM, Guyatt GH, et al: Development and validation of a questionnaire to measure asthma control. Eur Respir J 14:902–907, 1999.
358. Nathan RA, Sorkness CA, Kosinski M, et al: Development of the asthma control test: A survey for assessing asthma control. J Allergy Clin Immunol 113:59–65, 2004.
359. Vollmer WM, Markson LE, O’Connor E, et al: Association of asthma control with health care utilization and quality of life. Am J Respir Crit Care Med 160:1647–1652, 1999.

38 ASTHMA 917
407. Suissa S, Ernst P, Benayoun S, et al: Low-dose inhaled corticoster-oids and the prevention of death from asthma. N Engl J Med 343:332–336, 2000.
408. Israel E, Banerjee TR, Fitzmaurice GM, et al: Effects of inhaled glucocorticoids on bone density in premenopausal women. N Engl J Med 345:941–947, 2001.
409. Halpern MT, Schmier JK, Van Kerkhove MD, et al: Impact of long-term inhaled corticosteroid therapy on bone mineral density: Results of a meta-analysis. Ann Allergy Asthma Immunol 92:201–207, 2004 [quiz 207–208, 267].
410. Cumming RG, Mitchell P, Leeder SR: Use of inhaled corticoster-oids and the risk of cataracts. N Engl J Med 337:8-–14, 1997.
411. Garbe E, LeLorier J, Boivin JF, et al: Inhaled and nasal glucocor-ticoids and the risks of ocular hypertension or open-angle glau-coma. JAMA 277:722–727, 1997.
412. Calverley PM, Anderson JA, Celli B, et al: Salmeterol and flutica-sone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med 356:775–789, 2007.
413. Skoner DP, Szefler SJ, Welch M, et al: Longitudinal growth in infants and young children treated with budesonide inhalation suspension for persistent asthma. J Allergy Clin Immunol 105:259–268, 2000.
414. Agertoft L, Pedersen S: Effect of long-term treatment with inhaled budesonide on adult height in children with asthma. N Engl J Med 343:1064–1069, 2000.
415. Henderson WR Jr: The role of leukotrienes in inflammation. Ann Intern Med 121:684–697, 1994.
416. Barnes NC, Miller CJ: Effect of leukotriene receptor antagonist therapy on the risk of asthma exacerbations in patients with mild to moderate asthma: An integrated analysis of zafirlukast trials. Thorax 55:478–483, 2000.
417. Drazen JM, Israel E, O’Byrne PM: Treatment of asthma with drugs modifying the leukotriene pathway. N Engl J Med 340:197–206, 1999.
418. Dahlen B, Nizankowska E, Szczeklik A, et al: Benefits from adding the 5-lipoxygenase inhibitor zileuton to conventional therapy in aspirin-intolerant asthmatics. Am J Respir Crit Care Med 157:1187–1194, 1998.
419. Leff J.A, Busse WW, Pearlman D, et al: Montelukast, a leukotriene-receptor antagonist, for the treatment of mild asthma and exer-cise-induced bronchoconstriction. N Engl J Med 339:147–152, 1998.
420. Nelson H, Kemp J, Berger W, et al: Efficacy of zileuton controlled-release tablets administered twice daily in the treatment of mod-erate persistent asthma: A 3-month randomized controlled study. Ann Allergy Asthma Immunol 99:178–184, 2007.
421. Lofdahl CG, Reiss TF, Leff JA, et al:. Randomised, placebo control-led trial of effect of a leukotriene receptor antagonist, montelu-kast, on tapering inhaled corticosteroids in asthmatic patients. BMJ 319:87–90, 1999.
422. Vaquerizo MJ, Casan P, Castillo J, et al: Effect of montelukast added to inhaled budesonide on control of mild to moderate asthma. Thorax 58:204–210, 2003.
423. Clinical trial of low-dose theophylline and montelukast in patients with poorly controlled asthma. Am J Respir Crit Care Med 175:235–242, 2007. Epub 2006;September 22.
424. Fish JE, Israel E, Murray JJ, et al: Salmeterol powder provides significantly better benefit than montelukast in asthmatic patients receiving concomitant inhaled corticosteroid therapy. Chest 120:423–430, 2001.
425. Deykin A, Wechsler ME, Boushey HA, et al: Combination therapy with a long-acting beta-agonist and a leukotriene antagonist in moderate asthma. Am J Respir Crit Care Med 175:228–234, 2007.
426. Wechsler ME, Finn D, Gunawardena D, et al: Churg-Strauss syn-drome in patients receiving montelukast as treatment for asthma. Chest 117:708–713, 2000.
427. Wenzel S, Busse W, Calhoun W, et al: The safety and efficacy of zileuton controlled-release tablets as adjunctive therapy to usual care in the treatment of moderate persistent asthma: A 6-month randomized controlled study. J Asthma 44:305–310, 2007.
428. Barnes PJ: Theophylline: New perspectives for an old drug. Am J Respir Crit Care Med 167:813–818, 2003.
429. Evans DJ, Taylor DA, Zetterstrom O, et al: A comparison of low-dose inhaled budesonide plus theophylline and high-dose inhaled
383. Stolley PD: Asthma mortality. Why the United States was spared an epidemic of deaths due to asthma. Am Rev Respir Dis 105:883–890, 1972.
384. Hancox RJ: Concluding remarks: Can we explain the association of beta-agonists with asthma mortality? A hypothesis. Clin Rev Allergy Immunol 31:279–288, 2006.
385. Pearce N, Beasley R, Crane J, et al: End of the New Zealand asthma mortality epidemic. Lancet 345:41–44, 1995.
386. Drazen JM, Israel E, Boushey HA, et al: Comparison of regularly scheduled with as-needed use of albuterol in mild asthma. Asthma Clinical Research Network. N Engl J Med 335:841–847, 1996.
387. Taylor DR, Sears MR, Herbison GP, et al: Regular inhaled beta agonist in asthma: Effects on exacerbations and lung function. Thorax 48:134–138, 1993.
388. Nelson HS, Weiss ST, Bleecker ER, et al: The Salmeterol Multi-center Asthma Research Trial: A comparison of usual pharmaco-therapy for asthma or usual pharmacotherapy plus salmeterol. Chest 129:15–26, 2006.
389. Donohue JF: Safety and efficacy of beta agonists. Respir Care 53:618–622, 2008 [discussion appears 623–624].
390. Taylor DR, Drazen JM, Herbison GP, et al: Asthma exacerbations during long term beta agonist use: Influence of beta(2) adreno-ceptor polymorphism. Thorax 55:762–767, 2000.
391. Israel E, Chinchilli VM, Ford JG, et al: Use of regularly scheduled albuterol treatment in asthma: Genotype-stratified, randomised, placebo-controlled cross-over trial. Lancet 364:1505–1512, 2004.
392. Bleecker ER, Emmett A, Crater G, et al: Lung function and symptom improvement with fluticasone propionate/salmeterol and ipratropium bromide/albuterol in COPD: Response by beta-agonist reversibility. Pulm Pharmacol Ther 21:682-–688, 2008. Epub 2008;May 1.
393. Beakes DE: The use of anticholinergics in asthma. J Asthma 34:357–368, 1997.
394. Cazzola M, Centanni S, Donner CF: Anticholinergic agents. Pulm Pharmacol Ther 11:381–392, 1998.
395. Partridge MR, Saunders KB: Site of action of ipratropium bromide and clinical and physiological determinants of response in patients with asthma. Thorax 36:530–533, 1981.
396. Iwamoto H, Yokoyama A, Shiota N, et al: Tiotropium bromide is effective for severe asthma with noneosinophilic phenotype. Eur Respir J 31:1379–1380, 2008.
397. Magnussen H, Bugnas B, van Noord J, et al: Improvements with tiotropium in COPD patients with concomitant asthma. Respir Med 102:50–56, 2008.
398. Bos IST, Gosens R, Zuidhof AB, et al: Inhibition of allergen-induced airway remodelling by tiotropium and budesonide: A comparison. Eur Respir J 30:653–661, 2007.
399. Barnes PJ: How corticosteroids control inflammation: Quintiles Prize Lecture 2005. Br J Pharmacol 148:245–254, 2006.
400. Adcock IM, Ito K, Barnes PJ: Glucocorticoids: Effects on gene transcription. Proc Am Thorac Soc 1:247–254, 2004.
401. van Rensen EL, Straathof KC, Veselic-Charvat MA, et al: Effect of inhaled steroids on airway hyperresponsiveness, sputum eosi-nophils, and exhaled nitric oxide levels in patients with asthma. Thorax 54:403–408, 1999.
402. Olivieri D, Chetta A, Del Donno M, et al: Effect of short-term treatment with low-dose inhaled fluticasone propionate on airway inflammation and remodeling in mild asthma: A placebo-controlled study. Am J Respir Crit Care Med 155:1864–1871, 1997.
403. Juniper EF, Kline PA, Vanzieleghem MA, et al: Effect of long-term treatment with an inhaled corticosteroid (budesonide) on airway hyperresponsiveness and clinical asthma in nonsteroid-depend-ent asthmatics. Am Rev Respir Dis 142:832–836, 1990.
404. Long-term effects of budesonide or nedocromil in children with asthma. The Childhood Asthma Management Program Research Group. N Engl J Med 343:1054–1063, 2000.
405. Sin DD, Man J, Sharpe H, et al: Pharmacological management to reduce exacerbations in adults with asthma: A systematic review and meta-analysis. JAMA 292:367–376, 2004.
406. Donahue JG, Weiss ST, Livingston JM, et al: Inhaled steroids and the risk of hospitalization for asthma. JAMA 277:887–891, 1997.

918 OBSTRUCTIVEDISEASES
toms on existing inhaled corticosteroid. Allen & Hanburys Limited UK Study Group. Lancet 344:219–224, 1994.
449. Shrewsbury S, Pyke S, Britton M: Meta-analysis of increased dose of inhaled steroid or addition of salmeterol in symptomatic asthma (MIASMA). BMJ 320:1368–1373, 2000.
450. Bateman ED, Boushey HA, Bousquet J, et al: Can guideline-defined asthma control be achieved? The Gaining Optimal Asthma ControL study. Am J Respir Crit Care Med 170:836–844, 2004.
451. Pauwels RA, Lofdahl CG, Postma DS, et al: Effect of inhaled for-moterol and budesonide on exacerbations of asthma. Formoterol and Corticosteroids Establishing Therapy (FACET) International Study Group [published erratum appears in N Engl J Med 338:139, 1998]. N Engl J Med 337:1405–1411, 1997.
452. Virchow JC Jr, Prasse A, Naya I, et al: Zafirlukast improves asthma control in patients receiving high-dose inhaled corticosteroids. Am J Respir Crit Care Med 162:578–585, 2000.
453. Peters SP, Anthonisen N, Castro M, et al: Randomized comparison of strategies for reducing treatment in mild persistent asthma. N Engl J Med 356:2027–2039, 2007.
454. Papi A, Canonica GW, Maestrelli P, et al: Rescue use of beclom-ethasone and albuterol in a single inhaler for mild asthma. N Engl J Med 356:2040–2052, 2007.
455. Chan-Yeung M, Chang JH, Manfreda J, et al: Changes in peak flow, symptom score, and the use of medications during acute exacer-bations of asthma. Am J Respir Crit Care Med 154:889–893, 1996.
456. Turner MO, Noertjojo K, Vedal S, et al: Risk factors for near-fatal asthma. A case-control study in hospitalized patients with asthma. Am J Respir Crit Care Med 157:1804–1809, 1998.
457. Beasley R, Miles J, Fishwick D, et al: Management of asthma in the hospital emergency department. Br J Hosp Med 55:253–257, 1996.
458. Rodrigo GJ, Rodrigo C: First-line therapy for adult patients with acute asthma receiving a multiple-dose protocol of ipratropium bromide plus albuterol in the emergency department. Am J Respir Crit Care Med 161:1862–1868, 2000.
459. Manser R, Reid D, Abramson M: Corticosteroids for acute severe asthma in hospitalised patients. Cochrane Database Syst Rev 1:CD001740, 2001.
460. Rowe BH, Bota GW, Fabris L, et al: Inhaled budesonide in addition to oral corticosteroids to prevent asthma relapse following dis-charge from the emergency department: A randomized control-led trial. JAMA 281:2119–2126, 1999.
461. Edmonds ML, Camargo CA, Saunders LD, et al: Inhaled steroids in acute asthma following emergency department discharge. Cochrane Database Syst Rev 3:CD002316, 2000.
462. Rowe BH, Bretzlaff JA, Bourdon C, et al: Magnesium sulfate for treating exacerbations of acute asthma in the emergency depart-ment. Cochrane Database Syst Rev 2:CD001490, 2000.
463. Soroksky A, Stav D, Shpirer I: A pilot prospective, randomized, placebo-controlled trial of bilevel positive airway pressure in acute asthmatic attack. Chest 123:1018–1025, 2003.
464. Ho AMH, Lee A, Karmakar MK, et al. Heliox vs air-oxygen mix-tures for the treatment of patients with acute asthma: A system-atic overview. Chest 123:882–890, 2003.
465. Rodrigo G, Pollack C, Rodrigo C, et al: Heliox for nonintubated acute asthma patients. Cochrane Database Syst Rev 4:CD002884, 2006.
466. Williams TJ, Tuxen DV, Scheinkestel CD, et al: Risk factors for morbidity in mechanically ventilated patients with acute severe asthma. Am Rev Respir Dis 146:607–615, 1992.
467. Cote J, Cartier A, Robichaud P, et al. Influence on asthma morbid-ity of asthma education programs based on self-management plans following treatment optimization. Am J Respir Crit Care Med 155:1509–1514, 1997.
468. Clark GJ, Angel N, Kato M, et al: The role of dendritic cells in the innate immune system. Microbes Infect 2:257–272, 2000.
469. Coutts JA, Gibson NA, Paton JY: Measuring compliance with inhaled medication in asthma. Arch Dis Child 67:332–333, 1992.
budesonide for moderate asthma. N Engl J Med 337:1412–1418, 1997.
430. Ayres JG, Higgins B, Chilvers ER, et al: Efficacy and tolerability of anti-immunoglobulin E therapy with omalizumab in patients with poorly controlled (moderate-to-severe) allergic asthma. Allergy 59:701–708, 2004.
431. Humbert M, Beasley R, Ayres J, et al: Benefits of omalizumab as add-on therapy in patients with severe persistent asthma who are inadequately controlled despite best available therapy (GINA 2002 step 4 treatment): INNOVATE. Allergy 60:309–316, 2005.
432. Brown R, Turk F, Dale P, et al: Cost-effectiveness of omalizumab in patients with severe persistent allergic asthma. Allergy 62:149–153, 2007.
433. Cox G, Miller JD, McWilliams A, et al: Bronchial thermoplasty for asthma. Am J Respir Crit Care Med 173:965–969, 2006.
434. Chaudhuri R, Livingston E, McMahon AD, et al: Effects of smoking cessation on lung function and airway inflammation in smokers with asthma. Am J Respir Crit Care Med 174:127–133, 2006.
435. Rachelefsky GS, Katz RM, Siegel SC: Chronic sinus disease with associated reactive airway disease in children. Pediatrics 73:526–529, 1984.
436. Patterson PE, Harding SM: Gastroesophageal reflux disorders and asthma. Curr Opin Pulm Med 5:63–67, 1999.
437. Platts-Mills TA, Tovey ER, Mitchell EB, et al: Reduction of bron-chial hyperreactivity during prolonged allergen avoidance. Lancet 2:675–678, 1982.
438. Morgan WJ, Crain EF, Gruchalla RS, et al: Results of a home-based environmental intervention among urban children with asthma. N Engl J Med 351:1068–1080, 2004.
439. Gotzsche PC, Johansen HK, Schmidt LM, et al. House dust mite control measures for asthma. Cochrane Database Syst Rev 4:CD001187, 2004.
440. Calamita Z, Saconato H, Pela AB, et al: Efficacy of sublingual immunotherapy in asthma: Systematic review of randomized-clinical trials using the Cochrane Collaboration method. Allergy 61:1162–1172, 2006.
441. Abramson MJ, Puy RM, Weiner JM: Allergen immunotherapy for asthma. Cochrane Database Syst Rev 4:CD001186, 2003.
441a. Haselkorn T, Fish JE, Zeiger RS, et al: Consistently very poorly controlled asthma, as defined by the impairment domain of the Expert Panel Report 3 guidelines, increases risk of future severe asthma exacerbations in the Epidemiology and Natural History of Asthma: Outcomes and Treatment Regimens (TENOR) Study. J Allergy Clin Immunol 2009 [Epub ahead of print].
442. Pauwels RA, Pedersen S, Busse WW, et al: Early intervention with budesonide in mild persistent asthma: A randomised, double-blind trial. Lancet 361:1071–1076, 2003.
443. Adams NP, Bestall JB, Malouf R, et al: Inhaled beclomethasone versus placebo for chronic asthma. Cochrane Database Syst Rev 1:CD002738, 2005.
444. Bousquet J, Ben-Joseph R, Messonnier M, et al. A meta-analysis of the dose-response relationship of inhaled corticosteroids in ado-lescents and adults with mild to moderate persistent asthma. Clin Ther 24:1-–20, 2002.
445. Szefler SJ, Martin RJ, King TS, et al: Significant variability in response to inhaled corticosteroids for persistent asthma. J Allergy Clin Immunol 109:410–418., 2002.
446. Lazarus SC, Boushey HA, Fahy JV, et al: Long-acting beta2-agonist monotherapy vs continued therapy with inhaled corticosteroids in patients with persistent asthma: A randomized controlled trial. JAMA 285:2583–2593, 2001.
447. Lemanske RF Jr, Sorkness CA, Mauger EA, et al: Inhaled corticos-teroid reduction and elimination in patients with persistent asthma receiving salmeterol: A randomized controlled trial. JAMA 285:2594–2603, 2001.
448. Greening AP, Ind PW, Northfield M, et al: Added salmeterol versus higher-dose corticosteroid in asthma patients with symp-