Applied anatomy of adductor canal and popliteal fossa
19
Applied Anatomy of Applied Anatomy of Adductor Canal and Adductor Canal and Popliteal fossa Popliteal fossa Dhingra Harshita Roll no. 23 1 st year MBBS SSR Medical College
-
Upload
dikshat-pruthi -
Category
Health & Medicine
-
view
172 -
download
6
Transcript of Applied anatomy of adductor canal and popliteal fossa

Applied Anatomy of Applied Anatomy of Adductor Canal and Adductor Canal and
Popliteal fossaPopliteal fossa
Dhingra Harshita Roll no. 231st year MBBSSSR Medical College

ContentsContents
Adductor canal (Introduction)Clinical Anatomy-Adductor CanalPopliteal Fossa (Introduction)Clinical Anatomy - Popliteal FossaBibliography

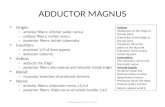
Adductor canalAdductor canal
Hunter’s canal or Subsartorial canalNarrow conical tunnel, located on the
medial side of middle one third of the thigh.Extends from apex of femoral triangle to
the hiatus of adductor magnusServes as a passage for structures passing
through the anterior thigh and posterior leg

Boundaries Boundaries Bounded by muscular structure Anterolaterally : vastus medialis,Posteromedially : adductor
longus, and distal to adductor longus, by adductor magnus.
Anteromedial (roof) : subsartorial fascia


Clinical AnatomyClinical AnatomyAdductor canal compression syndrome
Entrapment of Neurovascular bundle within adductor canal.
Rare conditionOccurs as a result of hypertrophy of adjacent
muscles, commonly vastus medialis.Most common in young males

Clinically patient may present with◦Intermittent claudication symptoms (pain on walking) More common Due to occlusion of femoral artery
◦Neurological symptoms Pain, numbness Due to entrapment of saphaneous Nerve

Adductor canal blockLocal anesthetic is administered in the
adductor canal to block the saphenous nerve in isolation, or together with the nerve to vastus medialis.
Used to provide sensory anesthesia for the surgical procedures involving distal thigh and femur, knee and lower leg on medial side.
Sartorius and femoral artery are used as anatomical landmark to locate the saphenous nerve.

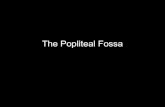
Popliteal fossaPopliteal fossaDiamond shape Located on posterior side of the
knee.Main pathway for the structures
moving from the thigh to the leg.

Boundaries Boundaries superolaterally:Biceps tendonsuperomedially:
Semimembranosus reinforced by
Semitendinosus;inferomedially the medial
head of Gastrocnemiusand inferolaterally: lateral
heads of Gastrocnemius & supplemented by Plantaris

The popliteal fossa. (a) Superficial dissection. (b) Deep dissection.

CONTENTSCONTENTS

Clinical AnatomyClinical Anatomyo Swelling in popliteal fossao Mass In popliteal fossa can occur
due to many causes:• Baker’s cyst • Popliteal artery aneurysm• Deep vein thrombosis • Neoplasm of the muscles
Major causes

Popliteal Lymph node enlargement (lymphadenitis)
There are usually six small lymph nodes embedded in the fat of the popliteal fossa. Inflammation of the popliteal nodes is often caused by lateral lesions of the heel resulting in enlargement of lymph nodes and pain.

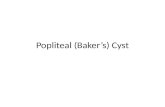
Baker’s cyst ( popliteal cyst )
Inflammation and swelling of the semimembranous bursa , a fluid filled sac found in the knee joint.
Usually arise in conjugation with arthritis.Usually resolves on its ownSome times may require surgery
MRI of knee showing Baker’s cyst


Popliteal artery aneurysm
Dialtation of an artery, which is greater than 50 % of the diameter
Due to tough fascia, aneurysm can not extend and compress the structures in the fossa .
Tibial nerve is more susceptible to compression, resulting in damage to nerve and patient may present as loss of sensory and motor function.

Bibliography• Textbook of Anatomy by B.D.
Chaurasia.• Clinical Anatomy by Vishram Singh.• Class notes.

Thank You!









![A Cystic Mass in the Popliteal Fossa and Its Differential ......[2]. Therefore, surgeons may mistake ganglionic cysts in the popliteal fossa for Baker’s cysts or meniscal cysts.](https://static.fdocuments.in/doc/165x107/5f8ba0d5beaa983e540e6dd7/a-cystic-mass-in-the-popliteal-fossa-and-its-differential-2-therefore.jpg)