Adjuvant Therapies in Endometrial Cancer - … Treatment...papillary and clear cell, 1C -2A grade 3,...
40
Adjuvant Therapies in Adjuvant Therapies in Endometrial Cancer Endometrial Cancer Emma Hudson Emma Hudson
Transcript of Adjuvant Therapies in Endometrial Cancer - … Treatment...papillary and clear cell, 1C -2A grade 3,...

Adjuvant Therapies in Adjuvant Therapies in
Endometrial CancerEndometrial Cancer
Emma HudsonEmma Hudson

Endometrial CancerEndometrial Cancer
�� Most common gynaecological cancerMost common gynaecological cancer
�� Incidence increasing in Western worldIncidence increasing in Western world
�� 11--2% cancer deaths2% cancer deaths
�� 75% patients postmenopausal75% patients postmenopausal
�� 97% epithelial tumours97% epithelial tumours
�� 3% sarcomas3% sarcomas

TreatmentTreatment
�� Total Abdominal Hysterectomy and Total Abdominal Hysterectomy and
Bilateral SalpingoBilateral Salpingo--oophorectomyoophorectomy
�� ?pelvic and para?pelvic and para--aortic Lymphadenectomyaortic Lymphadenectomy
�� Adjuvant TreatmentAdjuvant Treatment
�� ?Radiotherapy+/?Radiotherapy+/-- BrachytherapyBrachytherapy
�� ?Chemotherapy?Chemotherapy
�� ?Hormonal therapy?Hormonal therapy

Prognostic FactorsPrognostic Factors
�� StageStageIA : tumor limited to endometriumIA : tumor limited to endometriumIB : invasion to less than one half the myometriumIB : invasion to less than one half the myometriumIC : invasion to more than one half the myometriumIC : invasion to more than one half the myometrium
IIA : endocervical glandular involvement onlyIIA : endocervical glandular involvement onlyIIB : cervical stromal invasionIIB : cervical stromal invasion
IIIA: tumor invades serosa and/or adnexa, and/or positive IIIA: tumor invades serosa and/or adnexa, and/or positive peritoneal cytology/ascitesperitoneal cytology/ascites
IIIB : vaginal metastasesIIIB : vaginal metastasesIIIC : metastases of pelvic and/or paraIIIC : metastases of pelvic and/or para--aortic lymph nodesaortic lymph nodes
IVA : tumor invasion of bladder and/or bowel mucosaIVA : tumor invasion of bladder and/or bowel mucosaIVB : distant metastasesIVB : distant metastases

Prognostic FactorsPrognostic Factors
�� StageStage
�� Depth of myometrial involvementDepth of myometrial involvement
�� GradeGrade
�� Lymphovascular space invasionLymphovascular space invasion
�� Histological subtypeHistological subtype
�� Serous papillarySerous papillary
�� Clear cellClear cell
�� AgeAge

RadiotherapyRadiotherapy-- the Evidencethe Evidence
�� Adjuvant Radiotherapy for Stage 1 Adjuvant Radiotherapy for Stage 1 Endometrial Cancer:Systematic Review Endometrial Cancer:Systematic Review and Metaand Meta--analysisanalysis
�� PORTEC 1PORTEC 1
�� GOGGOG
�� Aalders (1968Aalders (1968--1974) 1974)
�� Soderini (abstract only)Soderini (abstract only)
�� 1770 patients1770 patients
Kong, A. et al. Ann Oncol 2007 18:1595-1604; doi:10.1093/annonc/mdm066

Systematic Review and MetaSystematic Review and Meta--
analysisanalysis
•• PORTEC,GOG and Soderini PORTEC,GOG and Soderini –– surgery surgery
+/+/--EBRTEBRT
•• Aalders Aalders –– surgery + brachytherapy +/surgery + brachytherapy +/--
EBRTEBRT
•• All reduced locoregional recurrence All reduced locoregional recurrence
raterate
•• No difference in distant recurrence or No difference in distant recurrence or
survivalsurvival
Kong, A. et al. Ann Oncol 2007 18:1595-1604; doi:10.1093/annonc/mdm066

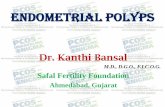
Meta-analysis on all stage I endometrial cancer patients who had adjuvant radiotherapy versus no radiotherapy
Kong, A. et al. Ann Oncol 2007 18:1595-1604; doi:10.1093/annonc/mdm066

Subgroup Analysis Subgroup Analysis
�� Patients with 1 Risk FactorPatients with 1 Risk Factor�� No statistically significant difference in deaths from all No statistically significant difference in deaths from all
causes or death from endometrial cancercauses or death from endometrial cancer
�� Patients with 2 Risk FactorsPatients with 2 Risk Factors�� Trend towards reduction in both deaths from all Trend towards reduction in both deaths from all
causes and endometrial cancercauses and endometrial cancer--related deaths but not related deaths but not statistically significant statistically significant
?Small number of patients?Small number of patients
�� Patients with No Risk FactorsPatients with No Risk Factors�� Statistically significant increased risk of endometrial Statistically significant increased risk of endometrial
related death (including treatment related deaths) related death (including treatment related deaths)
Kong, A. et al. Ann Oncol 2007 18:1595-1604; doi:10.1093/annonc/mdm066

Subgroup analysis of patients with at least 2 high risk factors, Stage Ic and grade 3
Kong, A. et al. Ann Oncol 2007 18:1595-1604; doi:10.1093/annonc/mdm066

Subgroup analysis of patients without high-risk features, i.e. patients with either stage Ia/b or grade 1/2
Kong, A. et al. Ann Oncol 2007 18:1595-1604; doi:10.1093/annonc/mdm066

ToxicityToxicity
�� PORTEC PORTEC
�� Late complications 26% vs 4%Late complications 26% vs 4%
�� GOGGOG
�� 6 cases intestinal obstruction vs 16 cases intestinal obstruction vs 1
�� 2 radiation related deaths2 radiation related deaths
Kong, A. et al. Ann Oncol 2007 18:1595-1604; doi:10.1093/annonc/mdm066

SummarySummary
�� Adjuvant Pelvic External Beam Adjuvant Pelvic External Beam
Radiotherapy Radiotherapy
�� Reduces locoregional recurrence (RR 0.28)Reduces locoregional recurrence (RR 0.28)
�� No difference in distant recurrenceNo difference in distant recurrence
�� No difference in overall survivalNo difference in overall survival
�� No difference in diseaseNo difference in disease--specific survivalspecific survival
Kong, A. et al. Ann Oncol 2007 18:1595-1604; doi:10.1093/annonc/mdm066

SummarySummary
�� Low Risk Early Endometrial CancerLow Risk Early Endometrial Cancer
�� Increased risk of endometrial cancer/ Increased risk of endometrial cancer/
treatment related deathstreatment related deaths
�� High Risk Early Endometrial CancerHigh Risk Early Endometrial Cancer
�� Trend towards reduction in risk of deathTrend towards reduction in risk of death
Kong, A. et al. Ann Oncol 2007 18:1595-1604; doi:10.1093/annonc/mdm066

SummarySummary
External Beam Pelvic Radiotherapy External Beam Pelvic Radiotherapy
should be considered in Patients with should be considered in Patients with
Multiple HighMultiple High--Risk Features but it carries Risk Features but it carries
an inherent risk of damage and toxicity an inherent risk of damage and toxicity
and should be avoided in Patients with and should be avoided in Patients with
no Risk Factorsno Risk Factors
Kong, A. et al. Ann Oncol 2007 18:1595-1604; doi:10.1093/annonc/mdm066

MRC ASTEC and NCIC CTG EN.5MRC ASTEC and NCIC CTG EN.5
�� 112 centres, 7 countries, 905 women112 centres, 7 countries, 905 women
�� Intermediate risk early stage diseaseIntermediate risk early stage disease--
FIGO stage 1A FIGO stage 1A --1B grade 3, 1C1B grade 3, 1C--2A grade 12A grade 1--
2 2
�� High risk early stage diseaseHigh risk early stage disease--serous serous
papillary and clear cell, 1Cpapillary and clear cell, 1C--2A grade 3, 2B2A grade 3, 2B
�� Randomised to observation vs EBRTRandomised to observation vs EBRT
�� Primary outcome Primary outcome -- overall survivaloverall survival
The Lancet:373;9658;137-146, 2009

MRC ASTEC and NCIC CTG EN.5MRC ASTEC and NCIC CTG EN.5
�� Radiotherapy 40Radiotherapy 40--46Gy in 2046Gy in 20--25 daily 25 daily
fractionsfractions
�� BrachytherapyBrachytherapy-- clinicians preference similar clinicians preference similar
in both armsin both arms
�� Patient and tumour details well matched Patient and tumour details well matched
�� Slightly more high risk women in observation Slightly more high risk women in observation
group 25% vs 20%group 25% vs 20%
The Lancet:373;9658;137-146, 2009

MRC ASTEC and NCIC CTG EN.5MRC ASTEC and NCIC CTG EN.5
�� ResultsResults
�� No difference in OS HR 1.05No difference in OS HR 1.05
�� 5yr OS 84%5yr OS 84%
�� No difference in disease specific survival No difference in disease specific survival
90%(observation) vs 89% (EBRT) 90%(observation) vs 89% (EBRT)
�� No difference in disease specific recurrenceNo difference in disease specific recurrence--free free
survival 84.7%(observation) vs 85.3% (EBRT)survival 84.7%(observation) vs 85.3% (EBRT)
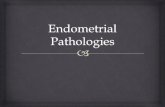
�� Reduction in isolated pelvic/vaginal recurrence Reduction in isolated pelvic/vaginal recurrence
HR 0.46HR 0.46
�� 5 year cumulative reduction 6.1% vs 2.9%5 year cumulative reduction 6.1% vs 2.9%The Lancet:373;9658;137-146, 2009

The Lancet:373;9658;137-146, 2009

Isolated Vaginal or Pelvic Initial Isolated Vaginal or Pelvic Initial
RecurrenceRecurrence
The Lancet:373;9658;137-146, 2009

SubgroupSubgroup AnalysisAnalysis
The Lancet:373;9658;137-146, 2009

MRC ASTEC and NCIC CTG EN.5: MRC ASTEC and NCIC CTG EN.5:
ToxicityToxicity
�� Increased acute toxicity 27% vs 57%Increased acute toxicity 27% vs 57%
�� Increased severe acute toxicity <1% vs 3%Increased severe acute toxicity <1% vs 3%
�� Increased late toxicity 45% vs 61%Increased late toxicity 45% vs 61%
�� Increased severe late toxicity 3% vs 7%Increased severe late toxicity 3% vs 7%
�� No treatment related deathsNo treatment related deaths
The Lancet:373;9658;137-146, 2009

MRC ASTEC and NCIC CTG EN.5: MRC ASTEC and NCIC CTG EN.5:
Updated MetaanalysisUpdated Metaanalysis
�� GOG and PORTEC includedGOG and PORTEC included
�� No effect on OS HR 1.04No effect on OS HR 1.04
�� Absolute benefit of >3% excludedAbsolute benefit of >3% excluded
The Lancet:373;9658;137-146, 2009

The Lancet:373;9658;137-146, 2009

MRC ASTEC and NCIC CTG EN.5: MRC ASTEC and NCIC CTG EN.5:
SummarySummaryThe ASTEC/EN.5 trial has shown The ASTEC/EN.5 trial has shown no evidenceno evidence of a benefit of a benefit for external beam radiotherapy for early endometrial cancer for external beam radiotherapy for early endometrial cancer at intermediate or high risk of recurrence, in terms of at intermediate or high risk of recurrence, in terms of overall, diseaseoverall, disease--specific, and diseasespecific, and disease--specific recurrencespecific recurrence--free survival. Combining these findings with data from other free survival. Combining these findings with data from other trials, we can exclude even a very small benefit of trials, we can exclude even a very small benefit of radiotherapy on overall survival radiotherapy on overall survival
With clear evidence from ASTEC/EN.5 that adjuvant With clear evidence from ASTEC/EN.5 that adjuvant external beam radiotherapy is associated external beam radiotherapy is associated with more acute with more acute and longand long--term toxicityterm toxicity than observation with or without than observation with or without brachytherapy, adjuvant radiotherapy after surgery to brachytherapy, adjuvant radiotherapy after surgery to achieve isolated local control is not justified as the achieve isolated local control is not justified as the treatment of choice.treatment of choice.
The Lancet:373;9658;137-146, 2009

The high risk PORTEC groupThe high risk PORTEC group
�� High risk patients excluded from randomisationHigh risk patients excluded from randomisation
�� 104 patients with stage IC, grade 3 endometrial 104 patients with stage IC, grade 3 endometrial
cancer registered, received adjuvant EBRT cancer registered, received adjuvant EBRT
�� Patients with Grade 3, 1C diseasePatients with Grade 3, 1C disease
�� Increased rate locoregional relapseIncreased rate locoregional relapse
�� Increased rate distant metastasesIncreased rate distant metastases
�� Decreased overall survivalDecreased overall survival
�� Grade 3 was the most important adverse prognostic Grade 3 was the most important adverse prognostic
factor for relapse and deathfactor for relapse and death
Creutzberg et al;J Clin Onc 2004;22:1234-1241

The High Risk PORTEC GroupThe High Risk PORTEC Group
58%58%31%31%14%14%Grade 3, Grade 3,
1C1C
74%74%20%20%11--3%3%Grade 3, Grade 3,
1B1B
8383--85%85%33--8%8%11--3%3%Grade 1Grade 1--22
Overall Overall
survivalsurvival
FiveFive--year year
distant distant
metastases metastases
ratesrates
Locoregional Locoregional
RecurrenceRecurrence
Rate Rate
Creutzberg et al;J Clin Onc 2004; 22:1234-1241

The high risk PORTEC groupThe high risk PORTEC group
�� CONCLUSION: Patients with stage IC, CONCLUSION: Patients with stage IC,
grade 3 endometrial carcinoma are at high grade 3 endometrial carcinoma are at high
risk of early distant spread and risk of early distant spread and
endometrial carcinomaendometrial carcinoma--related death. related death.
Novel strategies for adjuvant therapy Novel strategies for adjuvant therapy
should be explored to improve survival for should be explored to improve survival for
this patient group. this patient group.
Creutzberg et al;J Clin Onc 2004;22:1234-1241

BrachytherapyBrachytherapy
�� Prospective study Piver et al.Prospective study Piver et al.
�� 3 arm: post3 arm: post--op EBRT, pre and post op op EBRT, pre and post op
brachytherapybrachytherapy
�� No difference in OSNo difference in OS
�� 5 year DFS 99%5 year DFS 99%-- recurrences recurrences
salvageablesalvageable

BrachytherapyBrachytherapy
�� Portec 1 Portec 1 –– 75% pelvic recurrence treated 75% pelvic recurrence treated radicallyradically
�� ASTEC ASTEC �� Higher risk groupHigher risk group
�� Lower incidence locoLower incidence loco--regional recurrence regional recurrence 6.1%6.1%
�� ? Because of brachytherapy? Because of brachytherapy
�� Portec 2 awaitedPortec 2 awaited

ChemotherapyChemotherapy
�� GOG 34 GOG 34 �� Stage 1 and 2 disease, 224 patientsStage 1 and 2 disease, 224 patients
�� Adjuvant RT +/Adjuvant RT +/-- doxorubicindoxorubicin
�� Slow to recruit, No difference in OS or PFSSlow to recruit, No difference in OS or PFS
�� Italian StudyItalian Study�� Stage 1 and 2 disease, 345 patientsStage 1 and 2 disease, 345 patients
�� Adjuvant chemotherapy (cyclophosphamide, Adjuvant chemotherapy (cyclophosphamide, cisplatin and doxorubicin) vs pelvic EBRTcisplatin and doxorubicin) vs pelvic EBRT
�� No difference in OS or PFSNo difference in OS or PFS

ChemotherapyChemotherapy
�� EORTCEORTC--5599155991
�� High risk patients, 382 patientsHigh risk patients, 382 patients
�� Adjuvant EBRT +/Adjuvant EBRT +/-- chemotherapy (variety of chemotherapy (variety of
regimens)regimens)
�� 27% didn27% didn’’t complete chemotherapyt complete chemotherapy
�� Increase 5 yr PFS 7% (72%Increase 5 yr PFS 7% (72%--79%) 79%)
�� Increase in 5 yr OS of 8% (74%Increase in 5 yr OS of 8% (74%--82%)82%)
Hogberg T et al;J Clin Onc 2007 25(18S)

ChemotherapyChemotherapy--High RiskHigh Risk
�� Retrospective study of stage 2 papillary serous Retrospective study of stage 2 papillary serous carcinomacarcinoma
�� 55 surgically staged patients, 1055 surgically staged patients, 10--observation, 26 observation, 26 EBRT alone, 19 platinum/taxane chemotherapy EBRT alone, 19 platinum/taxane chemotherapy + EBRT+ EBRT
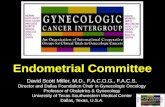
�� Reduction in risk of recurrence 11%(CT+/Reduction in risk of recurrence 11%(CT+/--RT) RT) VS 50% (RT alone) vs 50% (observation)*VS 50% (RT alone) vs 50% (observation)*
�� Increase PFS 86% (CT+/Increase PFS 86% (CT+/--RT) vs 41% (no RT) vs 41% (no chemo)*chemo)*
�� Increase OS 88% (CT+/Increase OS 88% (CT+/--RT) vs 64% (no chemo)RT) vs 64% (no chemo)
�� 70% recurrences extra pelvic and not 70% recurrences extra pelvic and not salvageablesalvageable
* Statistically significant
Fader A.N et al:Gynecologic Oncology 112 (2009) 558–562

PFS by chemotherapy versus no PFS by chemotherapy versus no
chemotherapy (RT alone+OBS group), chemotherapy (RT alone+OBS group),
p=0.028p=0.028
Fader A.N et al:Gynecologic Oncology 112 (2009) 558–562

PFS by OBS, RT alone and PFS by OBS, RT alone and
CT+/CT+/−−RT group, p=.081RT group, p=.081
Fader A.N et al:Gynecologic Oncology 112 (2009) 558–562

ChemotherapyChemotherapy
PORTEC 3PORTEC 3
Chemoradiotherapy with concurrent cisplatin Chemoradiotherapy with concurrent cisplatin
and adjuvant carboplatin AUC 5 and and adjuvant carboplatin AUC 5 and
paclitaxelpaclitaxel

Hormonal TherapyHormonal Therapy
�� Limited dataLimited data
�� Multicentre trial Multicentre trial
�� Stage 1B grade 1Stage 1B grade 1--2 :observation vs 2 :observation vs medroxyprogesterone acetate (MPA) medroxyprogesterone acetate (MPA) 100mg bd 12/12100mg bd 12/12
�� Stage 1C/ grade 3 :EBRT +/Stage 1C/ grade 3 :EBRT +/-- MPAMPA
�� Node positive pelvic/Node positive pelvic/paraaorticparaaortic RT +/RT +/--MPAMPA
�� No difference in DFSNo difference in DFS

What Adjuvant Therapy Should we What Adjuvant Therapy Should we
use?use?�� Low risk diseaseLow risk disease
�� >95% survival>95% survival
�� Adjuvant therapy maybe detrimentalAdjuvant therapy maybe detrimental
�� Intermediate risk, 1 risk factorIntermediate risk, 1 risk factor�� Decrease in local recurrence by EBRTDecrease in local recurrence by EBRT
�� No difference on OSNo difference on OS
�� High risk, 2 or more risk factorsHigh risk, 2 or more risk factors�� Decrease in local recurrence with EBRTDecrease in local recurrence with EBRT
�� Kong et al Kong et al –– trend to increasing OStrend to increasing OS
�� ASTEC no benefitASTEC no benefit
�� Increase PFS and OS with combination Increase PFS and OS with combination chemotherapychemotherapy

Treatment OptionsTreatment Options
EBRT +Vaginal Vault EBRT +Vaginal Vault
Brachytherapy Brachytherapy
Consider concurrent Consider concurrent
chemoradiation and chemoradiation and
adjuvant adjuvant
chemotherapy in chemotherapy in
context of PORTEC 3context of PORTEC 3
1C grade 31C grade 3
1C LVSI1C LVSI
Grade 3 LVSIGrade 3 LVSI
2A grade 32A grade 3
2B2B--3 any grade3 any grade
1B1B--3 with clear 3 with clear
cell/serous papillarycell/serous papillary
High risk, stage 1High risk, stage 1--2A2A
Advanced disease Advanced disease
stage 2Bstage 2B--33
Vaginal Vault Vaginal Vault
BrachytherapyBrachytherapy1A/B grade 31A/B grade 3
1C1C--2A grade 12A grade 1--22
Intermediate riskIntermediate risk
Stage 1Stage 1--2A2A
No further treatmentNo further treatment1A/B grade 11A/B grade 1--22Low riskLow risk
Stage 1Stage 1--2A2A
Proposed TreatmentProposed TreatmentRisk factorsRisk factorsEndometrial Endometrial
CarcinomaCarcinoma
Kong A et al. Clin Onc(2008)20:457-462

Thank youThank you
Questions?Questions?