Uterine corpus. benign diseases: - endometritis - endometriosis and adenomyosis - endometrial polyps...
31
Uterine corpus
-
Upload
sheryl-bryant -
Category
Documents
-
view
237 -
download
1
Transcript of Uterine corpus. benign diseases: - endometritis - endometriosis and adenomyosis - endometrial polyps...
Uterine corpus
Uterine corpus
• benign diseases:• - endometritis• - endometriosis and adenomyosis• - endometrial polyps• precursor lesions of endometrial carcinoma• endometrial carcinoma• mesenchymal tumors of the uterus
Endometritis
Pregnancy-related• after a vaginal delivery 2-3%• after Cesarean delivery 13-
90%• - enterococcus• - streptococcus• - chlamydia …
• puerperal sepsis
Unrelated to pregnancy• usually ascending infection• IUD• acute• - neutrophils within endometrial
glands• - Neisseria gonorrhoeae• - Chlamydia trachomatis• chronic• - plasma cells• - pelvic inflammatory disease
Puerperal sepsis• bacterial infection• contracted during childbirth or abortion• usually treatable with antibiotics• can be fatal!
• between 1991 and 2001: 137 women died up to 42 day after the delivery (12,5 / 100 000 deliveries) - in the Czech Republic
• only 5 of them (4,3%) died because of infection
• common condition – historically• during the 18th century it took on
epidemic proportions• particularly when home delivery
practice changed to delivery lying-in hospital
• - at those times, there still was a total ignorance of asepsis
Endometriosis
• presence of endometrial tissue outside the endometrium and myometrium
• pathogenesis (two theories):• 1) metastatic theory: implantation of
endometrial tissue to its ectopic location• 2) metaplastic theory: development of the
endometrial tissue at the ectopic site
Endometriosis• true prevalence is unknown
as many patients are asymptomatic
• estimated prevalence in women of reproductive age is 10-15%
• >80% of patients are in reproductive age group
• sites of endometriosis: • - peritoneum• - urinary bladder• - ovaries• - uterine ligaments• - large bowel, skin• -lungs, bone, stomach
Adenomyosis• presence of endometrial
glands and stroma within the myometrium
• common condition, detected in 15-30% of hysterectomy specimen
• clinical features:• - pre- or perimenopausal
women• - abnormal bleeding and
dysmenorrhea• - uterus is enlarged
Endometrial polyps• common• 2-23% of patients undergoing
endometrial biopsy because of abnormal uterine bleeding
• probably related to hyperestrogenism
• may be single or multiple• increased frequency of polyps
in patients taking tamoxifen
Precursor lesions
Endometrial hyperplasia• hyperplasia without
atypia • atypical hyperplasia
Natural history of hyperplasia
• hyperplasia without atypia• fewer than 2% progress to carcinoma
• atypical hyperplasia• 23% progress to carcinoma
Endometrial intraepithelial carcinoma• precursor lesion of invasive
endometrial serous carcinoma• formerly also had been referred
to as „carcinoma in situ“• can be associated with
metastatic disease
• histological features:• - numerous mitotic figures• - high-grade nuclear atypias• - enlarged nuclei• - prominent nucleoli• - can be papillary arrangement
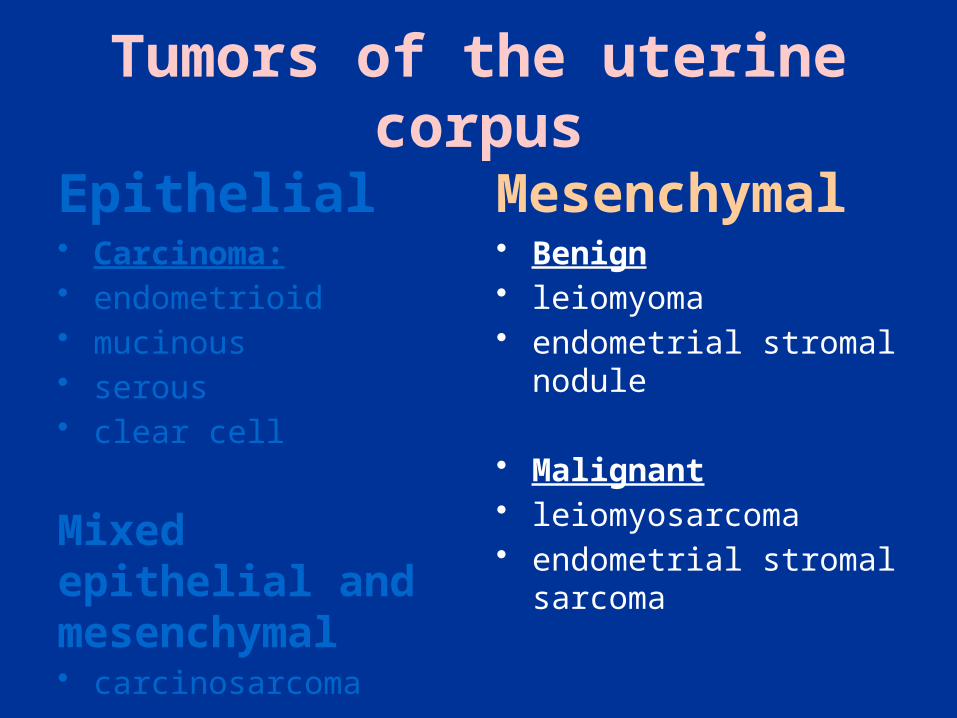
Tumors of the uterine corpus
Tumors of the uterine corpus
Epithelial• Carcinoma:• endometrioid • mucinous • serous • clear cell
Mixed epithelial and mesenchymal• carcinosarcoma
Mesenchymal• Benign• leiomyoma• endometrial stromal nodule
• Malignant• leiomyosarcoma• endometrial stromal
sarcoma
Endometrial carcinoma dualistic model of carcinogenesis
Type I• low-grade carcinomas• associated with estrogenic
stimulation• indolent behaviour• histologic subtypes:• - low grade endometrioid• - mucinous
• precursor lesion:• - atypical hyperplasia
Type II• high-grade carcinoma• not related to estrogenic
stimulation• aggresive behaviour• histologic subtypes:• - high-grade endometrioid• - serous• - clear cell
• precursor lesion:• - endometrial intraepithelial
carcinoma
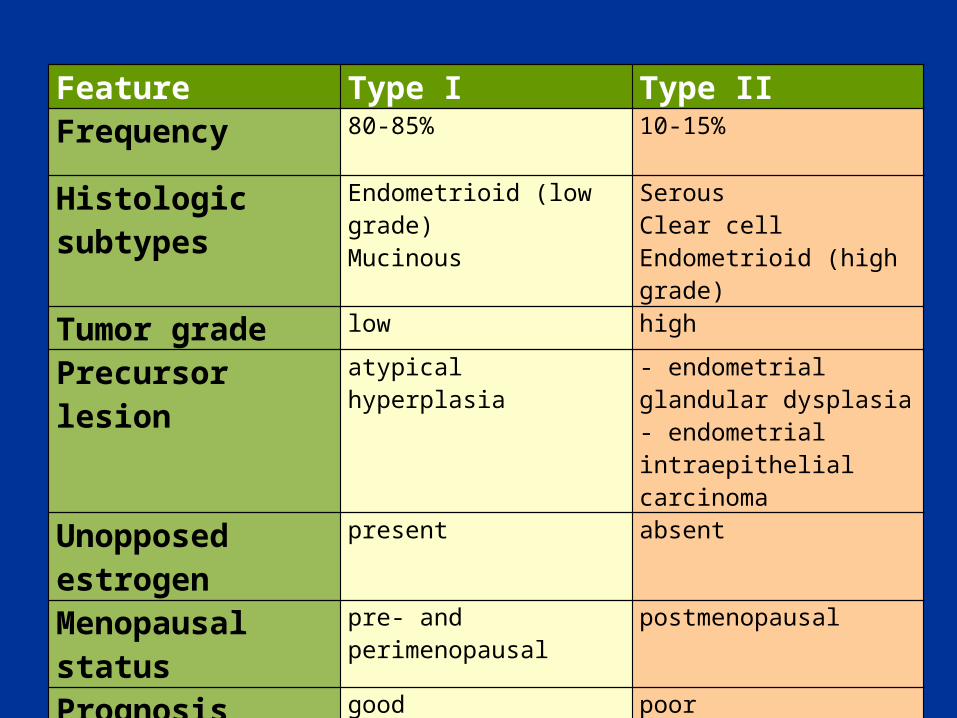
Feature Type I Type IIFrequency 80-85% 10-15%
Histologic subtypes Endometrioid (low grade)Mucinous
SerousClear cellEndometrioid (high grade)
Tumor grade low high
Precursor lesion atypical hyperplasia - endometrial glandular dysplasia- endometrial intraepithelial carcinoma
Unopposed estrogen present absent
Menopausal status pre- and perimenopausal postmenopausal
Prognosis good poor
Genetic alterations PTENMSIk-ras
p53Her2/neuE-cadherin

Etiology (type I)Risk factors• hormonal stimulation• - unopossed estrogen stimulation
(after 2 years – 2-3fold increase in the risk of EC)
• constitutional factors• - obesity• - diabetes mellitus• increased total caloric intake• high-fat diet• genetic alterations• - mutation of PTEN• - microstallite instability (HNPCC –
lynch syndrome)
Protective factors• increased physical exercise• addition of progestin to HRT• smoking• diet rich in vegetables• parity
Clinical features
• initial manifestation: • - abnormal vaginal bleeding• - rarely asymptomatic
• most women postmenopausal• in young women – generally low grade,
minimally invasive, excelent prognosis
Gross findings
• almost uniformly exophytic
• focal or diffuse• myometrial invasion
may result in enlargement of the uterus
• involvement of the cervix – approximately 20% cases
Tumors of the uterine corpus
Epithelial• Carcinoma:• endometrioid • mucinous • serous • clear cell
Mixed epithelial and mesenchymal• carcinosarcoma
Mesenchymal• Benign• leiomyoma• endometrial stromal nodule
• Malignant• leiomyosarcoma• endometrial stromal
sarcoma
PrognosisUterine factors• histologic type• grade• hormone receptor status• depth of myometrial
invasion• cervical involvement• vascular invasion
Extrauterine factors• adnexal involvement• intraperitoneal metastasis• lymph node metastasis
PrognosisUterine factors• histologic type• grade• hormone receptor status• depth of myometrial
invasion• cervical involvement• vascular invasion
Extrauterine factors• adnexal involvement• intraperitoneal metastasis• lymph node metastasis
stage
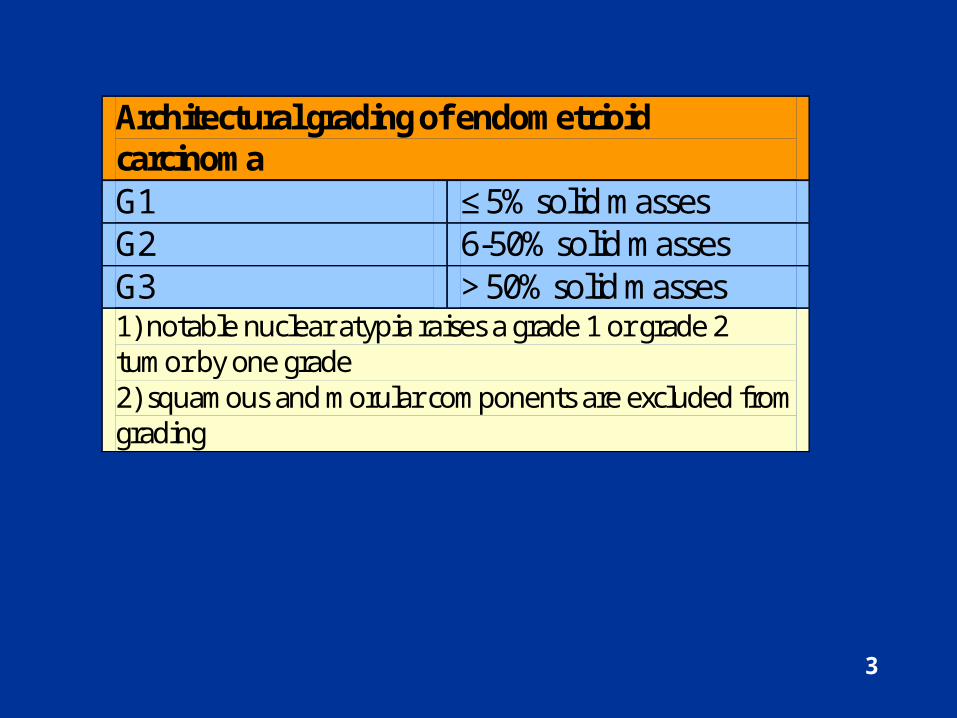
Architectural grading of endometrioid carcinoma G1 ≤ 5% solid masses G2 6-50% solid masses G3 > 50% solid masses 1) notable nuclear atypia raises a grade 1 or grade 2 tumor by one grade 2) squamous and morular components are excluded from grading
3
Tumors of the uterine corpus
Epithelial• Carcinoma:• endometrioid • mucinous • serous • clear cell
Mixed epithelial and mesenchymal• carcinosarcoma
Mesenchymal• Benign• leiomyoma• endometrial stromal nodule
• Malignant• leiomyosarcoma• endometrial stromal
sarcoma
Leiomyoma
• the most common uterine tumors• noted clinically in 20-30% of women over 30
years of age• when systematically searched – 75% of
women
Gross findings• location:• - submucosal (rare pedunculated)• - intramural (most common)• - subserosal (can be pedunculated)• multiple tumors in 2/3 of women• spherical, firm• sharply demarcated• cut surface: • - white to tan• - whorled trabecular pattern
Clinical features
• most asymptomatic, only a minority requires treatment
• therapy is indicated if:• - tumors are symptomatic (metrorrhagia,
abdominal pain, urination problems)• - interfere with fertility• - rapidly enlarge• - pose a diagnostic problem
Leiomyosarcoma
• about 1.3% of uterine malignancies• more than 50% of uterine sarcomas• most intramural• averages 6-9 cm in diameter• soft, fleshy, poorly defined margins• cut surface: gray-yellow or pink, often with areas of
necrosis and hemorrhage• poor prognosis: 5 year survival rate 15-25%
Carcinosarcoma (malignant mixed Müllerian tumor)
• composed of malignant epithelial and mesenchymal components
• frequently polypoid• poor prognosis