A parents guide to the management of Atopic Eczema
24
n The Leeds Teaching Hospitals NHS Trust A parents guide to the management of Atopic Eczema Information for parents and carers
Transcript of A parents guide to the management of Atopic Eczema
nThe Leeds
Teaching HospitalsNHS Trust
A parents guide to the management of
Atopic Eczema
Information for parents and carers
2
Atopic EczemaAtopic eczema (AE) is the commonest type of eczema. It is linked to the tendency to dry skin and a family (genetic) tendency to eczema, asthma or hayfever (atopy). It usually presents in the first year of life and rarely after the age of 5 years. Patients with AE are at higher risk of developing asthma, hayfever and/or an allergy.
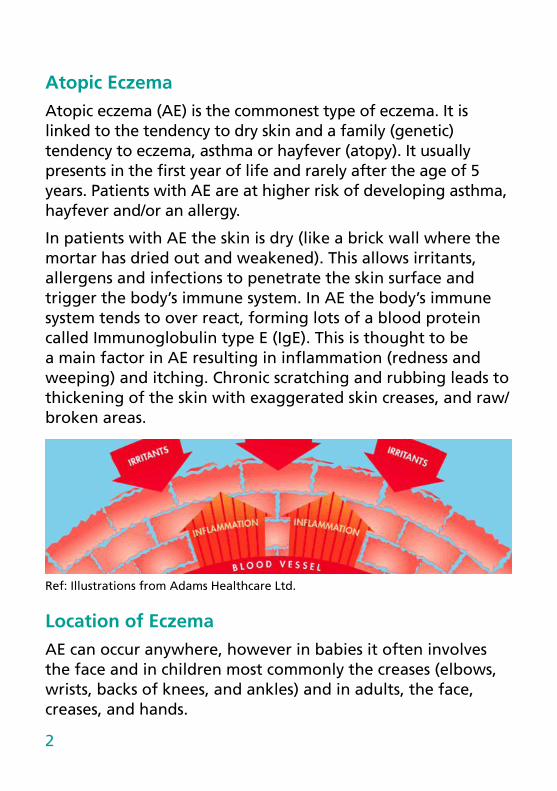
In patients with AE the skin is dry (like a brick wall where the mortar has dried out and weakened). This allows irritants, allergens and infections to penetrate the skin surface and trigger the body’s immune system. In AE the body’s immune system tends to over react, forming lots of a blood protein called Immunoglobulin type E (IgE). This is thought to be a main factor in AE resulting in inflammation (redness and weeping) and itching. Chronic scratching and rubbing leads to thickening of the skin with exaggerated skin creases, and raw/broken areas.
Ref: Illustrations from Adams Healthcare Ltd.
Location of EczemaAE can occur anywhere, however in babies it often involves the face and in children most commonly the creases (elbows, wrists, backs of knees, and ankles) and in adults, the face, creases, and hands.

3
TriggersThere are 4 main factors that can trigger a flare of AE:
1. Stresses
2. Dry Skin
3. Infection
4. Irritants & Allergies
StressStressful triggers include any tiredness, teething, illness and immunisation, as well as day-to-day stresses at home and school. Even children and babies can be affected by stress and can also have worries of their own which you may not realise e.g. new baby in the home, new nursery etc.
Dry SkinIn eczema the skin has lost its natural ability to moisturise, leaving it dry, and very itchy. This leads to breaks in the skin, worsened by scratching, rubbing and inflammation. Once the skin is broken, and with repeated scratching secondary infection is common, and the skin tends to become weepy, crusty and sore.
Ref: Illustrations from Adams Healthcare Ltd.
4
InfectionAny infection on the skin can trigger eczema to worsen however 3 infections are particularly common.
a) Impetigo-type bacteria
A bacterium called Staphylococcus Aureus can be found on many people’s skin and sometimes in the nose. However, it can cause active infection, particularly in AE skin. If the skin is dry, flaky or cracked the bacteria can multiply and trigger inflammation in the skin making the eczema worse, producing a vicious circle.
Signs of Staphylococcal infection:
• broken, weeping skin
• yellow crusts or / and pus-filled spots
• sore skin
• red and hot skin
Treatment & Prevention: If the infected area is small antiseptics or antibiotics can be applied directly on to the skin (topically). Sometimes they may be added into other topical treatments e.g. steroids and moisturisers. If a large area or several areas are infected, or if the infection is more severe, antibiotic medicine or tablets are usually recommended. A skin swab is often taken before treatment is started.
The same bacterium can sometimes live in the skin lining the nose. If the bacterium that can cause infection is being carried in the nose, a swab will be taken and an antibiotic nasal ointment prescribed.
Antiseptic bath or shower gels together with soap substitutes help to prevent the risk of infection by reducing the number

5
of living bacteria on the skin. Antibacterial ointments can also be applied to broken/cracked skin to help prevent infection.
b) Herpes (cold sore) viral infection
A third of the population tend to get recurrent cold sores. These are due to an infection by a virus called Herpes Simplex type I. If this virus gets on to skin prone to eczema or worse, where eczema is active it tends to spread quickly and extensively to cause a much more severe infection. It can even spread in to the eye if the face is involved. The infection can leave permanent scarring. Contact with the cold sore virus should be avoided wherever possible and if infection is suspected you should seek urgent medical attention.
Signs of infection:
Painful small blisters often around the mouth, face and neck (occasionally fingers or other sites) spreading to other areas of the body. Blisters may be oozy and quickly crust.
Treatment: Antiviral medicine or tablets.
c) Candida (Thrush) fungal infection
Candida is a yeast that tends to live on the skin in the moist skin folds e.g. groins, nappy area, neck creases etc. Areas which are wet and warm are prone to this infection e.g. around the mouth or the neck in children who are dribbling or who suck a dummy. The infection can trigger/worsen eczema.
6
Signs of infection:
Infection tends to make the skin very red, shiny and sore and occasionally little pussy spots are seen. Occasionally infants may also have mouth soreness due to Candida.
Treatment: Antifungal cream or drops for the mouth.
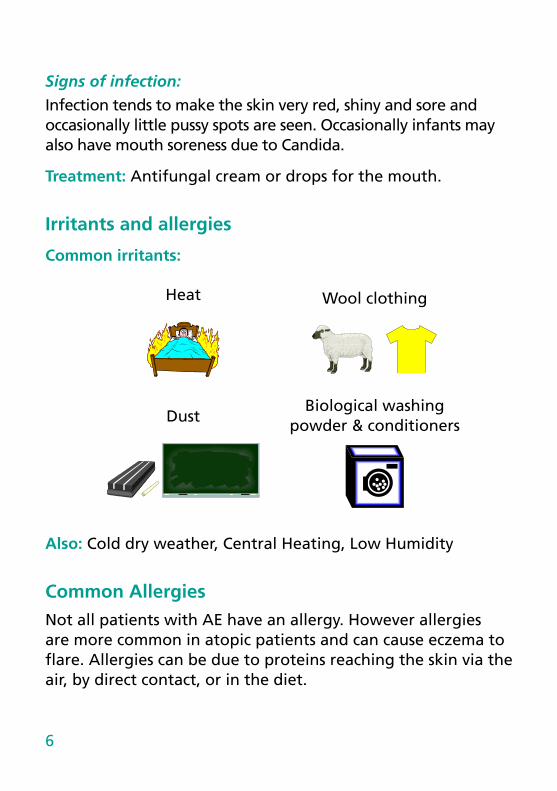
Irritants and allergies
Common irritants:
Heat Wool clothing
Dust
Biological washing powder & conditioners
Also: Cold dry weather, Central Heating, Low Humidity
Common AllergiesNot all patients with AE have an allergy. However allergies are more common in atopic patients and can cause eczema to flare. Allergies can be due to proteins reaching the skin via the air, by direct contact, or in the diet.
7
Airborne allergies1. Animals – House dust mite, Cat, Dog etc.
2. Plants – Grass and tree pollen
3. Moulds.
Contact allergiesEveryday products that come in contact with the skin can sometimes trigger allergy e.g. cheap metals in jewellery, fragrances, dyes, preservative chemicals in skin products and baby wipes etc. If contact allergy is suspected then patch tests can be arranged in the hospital dermatology department.
Possible dietary allergy factors:
Most Common food allergens:-
Eggs, Nuts, Wheat, Soya, dairy produce,cod fish
Also: Pulses (peas, lentils), sesame, kiwi
Most children with AD do not have a food allergy, however food allergies can be an exacerbating factor in some children. Food allergies usually trigger an urticarial (nettle-rash)
8
type skin reaction to the specific food(s), often with other symptoms such as vomiting, diarrhoea, swelling or wheezing. Food allergy is most common in little children. If food allergy is suspected further tests can be carried out under the supervision of a paediatric dietician.
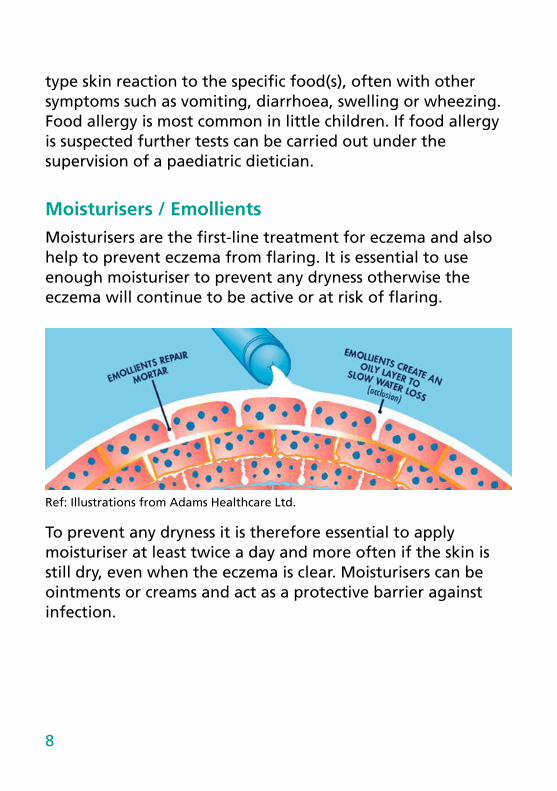
Moisturisers / EmollientsMoisturisers are the first-line treatment for eczema and also help to prevent eczema from flaring. It is essential to use enough moisturiser to prevent any dryness otherwise the eczema will continue to be active or at risk of flaring.
Ref: Illustrations from Adams Healthcare Ltd.
To prevent any dryness it is therefore essential to apply moisturiser at least twice a day and more often if the skin is still dry, even when the eczema is clear. Moisturisers can be ointments or creams and act as a protective barrier against infection.

9
Quantity of Emollient to be used per week
Amount (g)Infant 125-250Small Child 250-500Large Child 500+
Ointments: Ointments are the best for moisturising dry skin and less likely to sting/irritate eczematous skin. Ointments are preferred for very dry or cracked skin and during a severe flare.
During hot weather or if used excessively ointments can block pores and lead to small re bumps (folliculitis). Please contact a medical professinal for advice if this occurs.
Note: Paraffin based ointments are flammable! Avoid flame contact with skin or clothing covered with paraffin based ointment or emollient sprays!
CreamsCreams are white and lighter than ointments, they contain water. Creams tend to be less moisturising than ointments. Creams contain preservatives, therefore may sting. We therefore tend to avoid creams for those with moderate or severe eczema or where the skin is very dry or cracked.
Creams are less likely to block pores and cause folliculitis or in acne prone sites/ages acne. These are therefore preferable for eczema skin that is prone to acne or in hot or humid weather. They are also cosmetically nicer to use so are good for daytime moisturisation when eczema is not as severe or the skin not so dry.
10
Emolients and Moisturisers
Plain ointments and creams
Diprobase Ointment
Hydromol Ointment
Emulsifying Ointment
50/50 Emulsifying Ointment and liquid paraffin
50/50 Emulsifying Ointment and white soft paraffin
Vaseline
Double Base Gel
Epaderm Ointment
Creamy Paraffin
Aveeno Cream
Double Base Cream
Hydromol Cream
Diprobase Cream
Dermol 500 Lotion
E45 Cream
Imuderm
QV and QV Intensive
Balneum Cream
Zerobase Cream
N.B. creams contain preseravatives and these can somtimes cause stinging. If this occurs change to a greasy ointment (clear) emollient.
Note: Paraffin based ointments are flammable! Avoid flame contact with skin or clothing covered with paraffin based ointment or emollient sprays!
11
SteroidsAlthough moisturisers are the first-line treatment for eczema, steroids are necessary to treat acutely inflamed or highly itchy areas of skin. Steroids should always be used with moisturisers and not instead of. When used correctly and monitored by a medical or nursing professional working in dermatology, steroids are safe to use and usually very effective.
(See Finger tip unit guide for steroids on next page)
When & where to use steroidsSteroids should ideally be used where eczema is active, even if the skin is broken or cracked, however they should be avoided where there is no eczema or if there is untreated infection (e.g. see impetigo or cold sore infection previously).
How to use steroidsSee the Finger Tip Unit guide for quantity use. Steroids should be applied up to 30 minutes before a moisturiser to enable the steroid to be absorbed into the skin and to avoid the spreading of the moisturiser moving the steroid onto healthy areas of skin. The steroid should be measured to a ‘Finger tip unit’ and dabbed along the appropriate size area of eczema, then smoothed together into the skin in the direction of the hair growth to reduce the risk of folliculitis.
12
Which steroid to useYou will usually be advised of a care plan for using steroids. When eczema is active steroids are often recommended once or twice daily for 1 to 2 weeks, however, if eczema is more severe, steroids may be recommended for longer, although we often recommended tailing off how often they should be applied or tailing off from a stronger to a weaker steroid.
For the face: Usually only mild steroids are recommended. Occasionally if eczema is more severe, a moderate strength steroid is recommended for a short period of time, reducing to a mild steroid as the eczema improves. It is very rare for strong (potent) steroids to be recommended for the face even for short periods. They should usually be avoided due to the risk of skin thinning and also of cataract if used near to the eye.
In general avoid using anything other than very mild steroids near the eye or on the eyelids.
For the body: The strength of steroid used will depend on how severe the eczema is. Your doctor or nurse will recommend which steroid should be used.
In general steroid ointments are preferable to steroid creams (for the same reason that ointment moisturisers are usually preferable to creams). Some steroids have extra ingredients in them, often antiseptics, antibiotics or antifungal treatments. These are often recommended if infection is suspected along with the eczema. It is important to continue to use the steroid until there are no signs of active eczema. This will reduce the risk of the eczema returning quickly and will also ensure that symptoms such as itching or soreness settle adequately.
Please see list of available topical steroids.
13
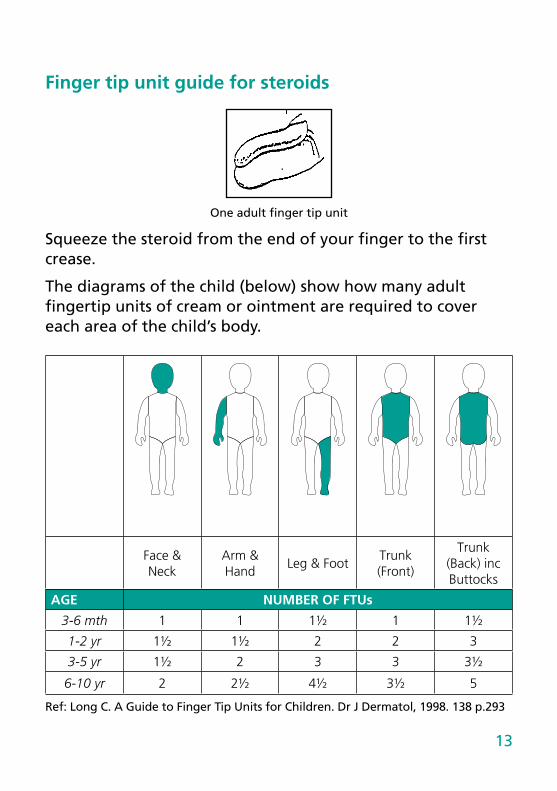
Finger tip unit guide for steroids
One adult finger tip unit
Squeeze the steroid from the end of your finger to the first crease.
The diagrams of the child (below) show how many adult fingertip units of cream or ointment are required to cover each area of the child’s body.
Face & Neck
Arm & Hand
Leg & FootTrunk (Front)
Trunk (Back) inc Buttocks
AGE NUMBER OF FTUs
3-6 mth 1 1 1½ 1 1½
1-2 yr 1½ 1½ 2 2 3
3-5 yr 1½ 2 3 3 3½
6-10 yr 2 2½ 4½ 3½ 5
Ref: Long C. A Guide to Finger Tip Units for Children. Dr J Dermatol, 1998. 138 p.293
14
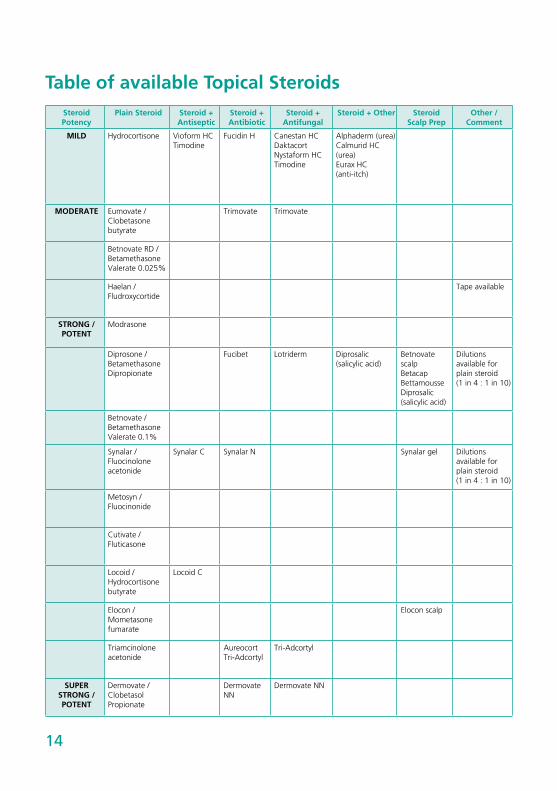
Table of available Topical SteroidsSteroid Potency
Plain Steroid Steroid + Antiseptic
Steroid + Antibiotic
Steroid + Antifungal
Steroid + Other Steroid Scalp Prep
Other / Comment
MILD Hydrocortisone Vioform HC Timodine
Fucidin H Canestan HCDaktacort Nystaform HCTimodine
Alphaderm (urea)Calmurid HC (urea)Eurax HC (anti-itch)
MODERATE Eumovate / Clobetasone butyrate
Trimovate Trimovate
Betnovate RD /BetamethasoneValerate 0.025%
Haelan / Fludroxycortide
Tape available
STRONG / POTENT
Modrasone
Diprosone /BetamethasoneDipropionate
Fucibet Lotriderm Diprosalic (salicylic acid)
Betnovate scalp BetacapBettamousseDiprosalic (salicylic acid)
Dilutions available for plain steroid (1 in 4 : 1 in 10)
Betnovate / BetamethasoneValerate 0.1%
Synalar / Fluocinolone acetonide
Synalar C Synalar N Synalar gel Dilutions available for plain steroid (1 in 4 : 1 in 10)
Metosyn / Fluocinonide
Cutivate / Fluticasone
Locoid / Hydrocortisone butyrate
Locoid C
Elocon / Mometasone fumarate
Elocon scalp
Triamcinoloneacetonide
Aureocort Tri-Adcortyl
Tri-Adcortyl
SUPER STRONG / POTENT
Dermovate / Clobetasol Propionate
Dermovate NN
Dermovate NN
15
Calcineurin Inhibitors (CI)CIs are topical treatments applied to the skin, which work like steroids to reduce inflammation (redness/soreness/itching). They are used similarly to steroids, once or twice a day where eczema is active. However, unlike steroids there is no risk of skin thinning (atrophy) or if used in the eye area of cataract, therefore they are often recommended for delicate sites like the face and creases.
CI are licensed for use in children 2 years and upward. Like steroids, they should be avoided on infected skin. It is also important to avoid sunburn/damage when using these treatments. It is quite common to get some contact stinging or sometimes a burning sensation when used on eczema skin. This is not a reason to stop the treatment unless these are not tolerable. CI’s also need to be stopped 4 weeks before and after live vaccines.
2 preparations are currently available:
Tacrolimus ointment (Protopic) and Pimecrolimus cream (Elidel).
A separate more detailed information sheet is available on these products.
Topical antibiotics Topical antifungals
(no steroid) (no steroid)
Bactroban Canesten
Metronidazole/Metrotop Nystatin
Daktarin
Terbinafine/Lamisil

16
Other scalp preparations
Shampoos
Descaling shampoos: Capasal, Alphosyl 2 in 1, Polytar, T GelAntifungal/antidandruff: Nizoral
Non-steroid Scalp Preparations
Descaling: Sebco, Cocois, Tar Pomade, SCC scalp preparation
Dressings Bandages:Duoderm Icthopaste (Icthammol)
Lyofoam Zincoband (Zinc)
Granuflex Zip-Zoc stocking (Zinc)
Aquacel Quinaband (Steroid)
Mepitel Tarband (Tar)
Allevyn
Handy Hints
Clothing:
• Try to wear cotton clothes whenever possible. Nylon and man-made fabrics make you sweat and wool clothes make you itch.
• Use non-biological washing powders without conditioners.
• Occasionally use biological washing powder on a hot rinse when empty to remove grease from your washing machine.
17
Environment
• Avoid heat as this increases the itching and central heating causes drying of the skin due to the lack of humidity.
• Use a high factor sunscreen for sensitive skin.
House Dust Mite (HDM)
• HDMs like warm places and thick textiles. Use lino, tiles or wooden flooring.
• Clean with a damp cloth rather than polishing.
• Wash clothes and bedding weekly at 60oC.
• Vacuum curtains weekly or replace them with blinds.
• Avoid fluffy toys or wash weekly at 60 oC. Alternatively place them in a plastic bag and place in the freezer over night.
• Keep a cover over the bed through the day, removing it carefully at night and shake the dust off outside.
• Special bedding covers can be purchased to protect from HD Mite.
Scratching • File fingernails and cut them regularly to keep them very
short.
• Cover hands with gloves/mittens overnight. Use tape to hold in place.
• Keep the bedroom cool to minimise itch. Use cotton sheets and blankets rather than quilts.
• Gently squeeze or pinch to relieve itchy skin rather than scratching it.
18
• Avoid products with fragrances and use hypoallergenic products. Try any new products first with a very small patch on your arm and wait for 2-3 days to make sure there is no reaction.
Swimming • Apply moisturiser before and after swimming (shower to
remove chlorine from the skin first). Use a water-soluble product (e.g. emulsifying ointment).
Remember – Children with emollients are very slippery when wet!’
19
Contact details
Dematology Appointments:
Tel:
Dermatology Department:
Chapel Allerton Hospital
Chapeltown Road
Leeds
LS7 4SA
Paediatric Dermatology Nurses
Nurse Specialists: Michelle Ogundibo Tel: 0113 3924380
Nicola Maher Tel: 0113 3924846
Rachael Oller Tel: 0113 3924861
Senior Clinical Support Worker:
Sarah Brooke Tel: 0113 3924824
Paediatric Dermatology Consultants:
Dr SM Clark Tel: 0113 3924370 (Secretary)
Dr EG Taylor Tel: 0113 3923454 (Secretary)
Dr S Shanmugam Tel: 0113 3924356 (Secretary)
20
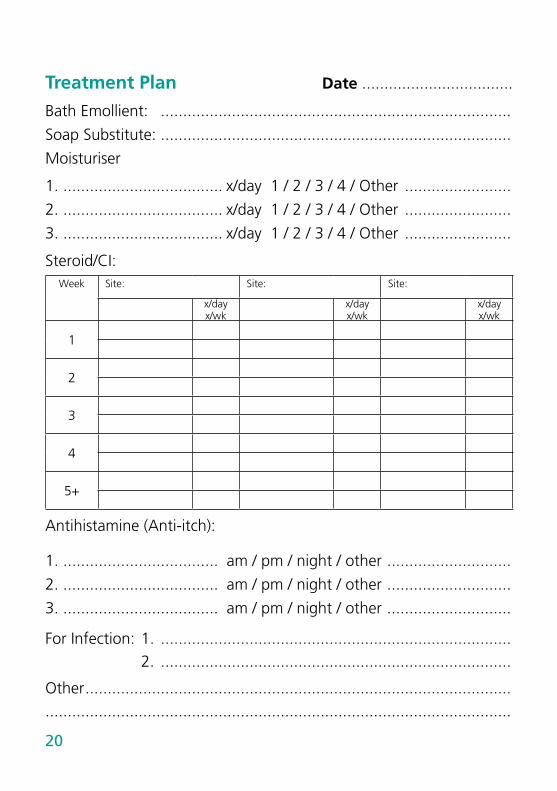
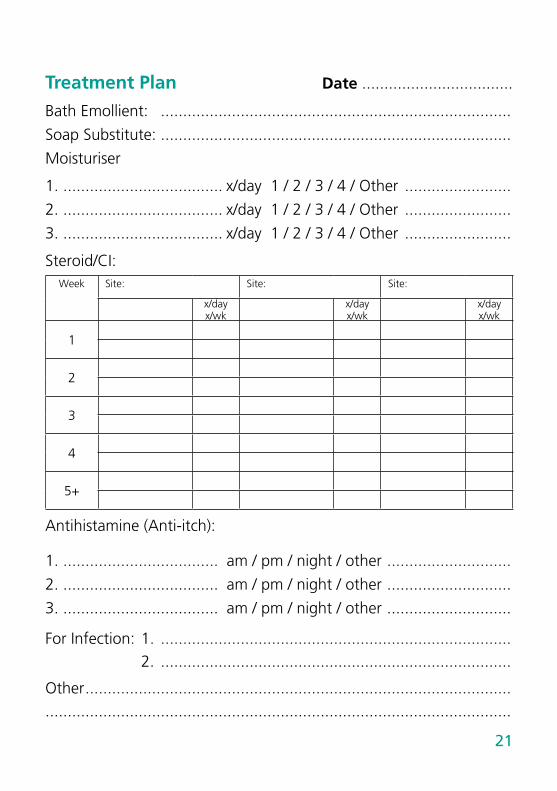
Treatment Plan Date ..................................
Bath Emollient: ...............................................................................
Soap Substitute: ...............................................................................
Moisturiser
1. .................................... x/day 1 / 2 / 3 / 4 / Other ........................
2. .................................... x/day 1 / 2 / 3 / 4 / Other ........................
3. .................................... x/day 1 / 2 / 3 / 4 / Other ........................
Steroid/CI:Week Site: Site: Site:
x/dayx/wk
x/dayx/wk
x/dayx/wk
1
2
3
4
5+
Antihistamine (Anti-itch):
1. ................................... am / pm / night / other ............................
2. ................................... am / pm / night / other ............................
3. ................................... am / pm / night / other ............................
For Infection: 1. ............................................................................... 2. ...............................................................................
Other .........................................................................................................................................................................................................
21
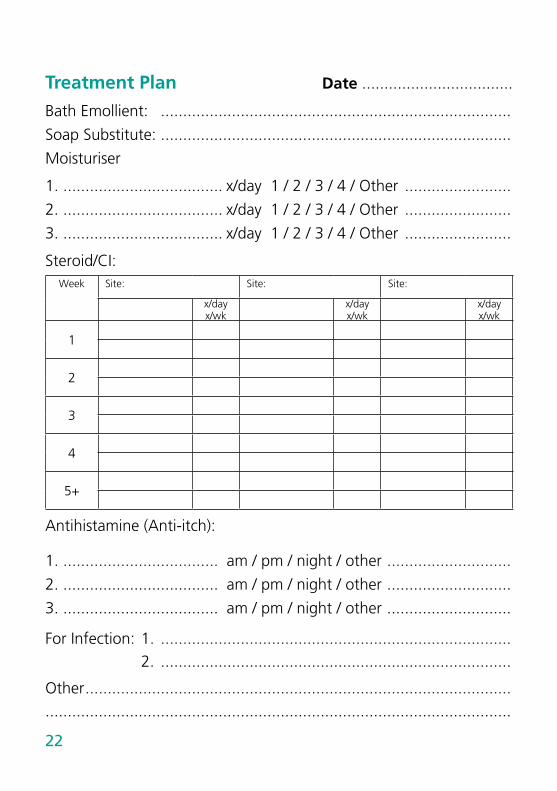
Treatment Plan Date ..................................
Bath Emollient: ...............................................................................
Soap Substitute: ...............................................................................
Moisturiser
1. .................................... x/day 1 / 2 / 3 / 4 / Other ........................
2. .................................... x/day 1 / 2 / 3 / 4 / Other ........................
3. .................................... x/day 1 / 2 / 3 / 4 / Other ........................
Steroid/CI:Week Site: Site: Site:
x/dayx/wk
x/dayx/wk
x/dayx/wk
1
2
3
4
5+
Antihistamine (Anti-itch):
1. ................................... am / pm / night / other ............................
2. ................................... am / pm / night / other ............................
3. ................................... am / pm / night / other ............................
For Infection: 1. ............................................................................... 2. ...............................................................................
Other .........................................................................................................................................................................................................
22
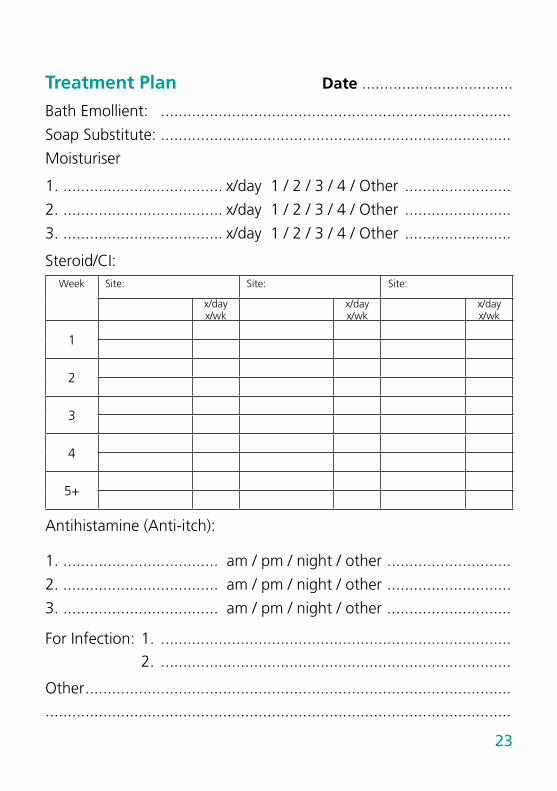
Treatment Plan Date ..................................
Bath Emollient: ...............................................................................
Soap Substitute: ...............................................................................
Moisturiser
1. .................................... x/day 1 / 2 / 3 / 4 / Other ........................
2. .................................... x/day 1 / 2 / 3 / 4 / Other ........................
3. .................................... x/day 1 / 2 / 3 / 4 / Other ........................
Steroid/CI:Week Site: Site: Site:
x/dayx/wk
x/dayx/wk
x/dayx/wk
1
2
3
4
5+
Antihistamine (Anti-itch):
1. ................................... am / pm / night / other ............................
2. ................................... am / pm / night / other ............................
3. ................................... am / pm / night / other ............................
For Infection: 1. ............................................................................... 2. ...............................................................................
Other .........................................................................................................................................................................................................
23
Treatment Plan Date ..................................
Bath Emollient: ...............................................................................
Soap Substitute: ...............................................................................
Moisturiser
1. .................................... x/day 1 / 2 / 3 / 4 / Other ........................
2. .................................... x/day 1 / 2 / 3 / 4 / Other ........................
3. .................................... x/day 1 / 2 / 3 / 4 / Other ........................
Steroid/CI:Week Site: Site: Site:
x/dayx/wk
x/dayx/wk
x/dayx/wk
1
2
3
4
5+
Antihistamine (Anti-itch):
1. ................................... am / pm / night / other ............................
2. ................................... am / pm / night / other ............................
3. ................................... am / pm / night / other ............................
For Infection: 1. ............................................................................... 2. ...............................................................................
Other .........................................................................................................................................................................................................
© The Leeds Teaching Hospitals NHS Trust • 3rd edition Ver 2Developed by: Dr S M Clark, Consultant Paediatric Dermatologist
Produced by: Medical Illustration Services • MID code: 20200716_001/RC
LN002861Publication date
07/2018Review date
07/2021
What did you think of your care?Scan the QR code or visit bit.ly/nhsleedsfft
Your views matter