Atopic eczema and emollients: guidance for GPNs · Atopic eczema (atopic dermatitis) is a common...
5
Atopic eczema and emollients: guidance for GPNs 36 GPN 2016, Vol 2, No 6 Atopic eczema is a common dry skin condition, and, as with any dry skin condition, emollients are a fundamental aspect of care. With so much choice there can be uncertainty around which product to use. Choosing one product over another can create confusion for both healthcare professionals and patients. This paper looks at emollients, the products available, how to use them and the current evidence and research relating to emollient use for atopic eczema. The reader is also directed to additional resources to support clinical practice. Sandra Lawton OBE Nurse consultant dermatology, Queen’s Nurse, Nottingham University Hospitals NHS Trust KEY WORDS: Atopic eczema Emollients Current research Prescribing Resources Copyright: Kaspars Grinvalds Long-term conditions: atopic eczema © 2016 Wound Care People Ltd
Transcript of Atopic eczema and emollients: guidance for GPNs · Atopic eczema (atopic dermatitis) is a common...

Atopic eczema and emollients: guidance for GPNs
36 GPN 2016, Vol 2, No 6
Atopic eczema is a common dry skin condition, and, as with any dry skin condition, emollients are a fundamental aspect of care. With so much choice there can be uncertainty around which product to use. Choosing one product over another can create confusion for both healthcare professionals and patients. This paper looks at emollients, the products available, how to use them and the current evidence and research relating to emollient use for atopic eczema. The reader is also directed to additional resources to support clinical practice.
Sandra Lawton OBENurse consultant dermatology, Queen’s Nurse, Nottingham University Hospitals NHS Trust
KEY WORDS:
Atopic eczema EmollientsCurrent researchPrescribingResources
Cop
yrig
ht: K
aspa
rs G
rinv
alds
Long-term conditions: atopic eczema
© 2016
Wou
nd C
are Peo
ple Lt
d
Atopic eczema (atopic dermatitis) is a common inflammatory, dry, itchy skin condition which usually develops in early childhood, with as many as one-fifth of children in developed countries now suffering from the condition (Flohr and Mann, 2014). Nationally, there is clear guidance on how to manage this condition (Box 1). However, for parents, coping with their child’s eczema can be challenging, and they need to be supported by competent healthcare professionals who can provide practical advice, demonstrate treatments and offer realistic plans of care (Lawton, 2014). One of the fundamental aspects of this care is the use of emollients.
EMOLLIENTS
The term emollient comes from a Latin word meaning to soften, and implies a substance that acts to smooth the skin’s surface. The word emollient and moisturiser are used interchangeably (Voegeli, 2007). Not all emollients are the same; emollient products are available in different formulations with additional ingredients which impact on skin hydration and acceptability for patients (Moncrieff et al, 2013), for example:
Simple emollients (occlusive), such as petrolatum or mineral oil, leave a fine occlusive layer of lipid or oil on the skin’s surface, which reduces the water loss from the stratum corneum (SC)Enhanced emollients which contain humectant ingredients such as urea and glycerol attract and hold water in the SC and have a longer-lasting hydrating effect on dry skinEmollients also contain lipids such as ceramides, cholesterol and free fatty acids, naturally found in the SC (Moncrieff et al, 2013) Some emollients contain a mixture of occlusive and
GPN 2016, Vol 2, No 6 37
humectant substances, with the humectant drawing and holding the water in the epidermis, and the occlusive element ensuring that it is trapped there (British Dermatological Nursing Group [BDNG], 2012
It is important that general practice nurses (GPNs) are aware of the different preparations and additional ingredients so that they can help patients to make an informed choice (Lawton, 2013). Prescribing should always be guided by clinical need and informed patient choice, with the following considerations:
Red Flag
Aqueous cream BP should never be used, either as a leave-on or wash product.
Patients should be given the opportunity to choose emollients which are suitable for their skin. This includes a variety of formulations, such as oils, lotions, creams, ointments and sprays (Table 1) (Moncrieff et al, 2013)Emollient routines need to be realistic and achievable for the patient, who should be prescribed adequate quantities for optimal effect (250–600g per week) and be offered smaller quantity packs for use at work, school, etc in addition to their main prescription. Patients may require more than one emollient product, dependent on their lifestyle, time of day,
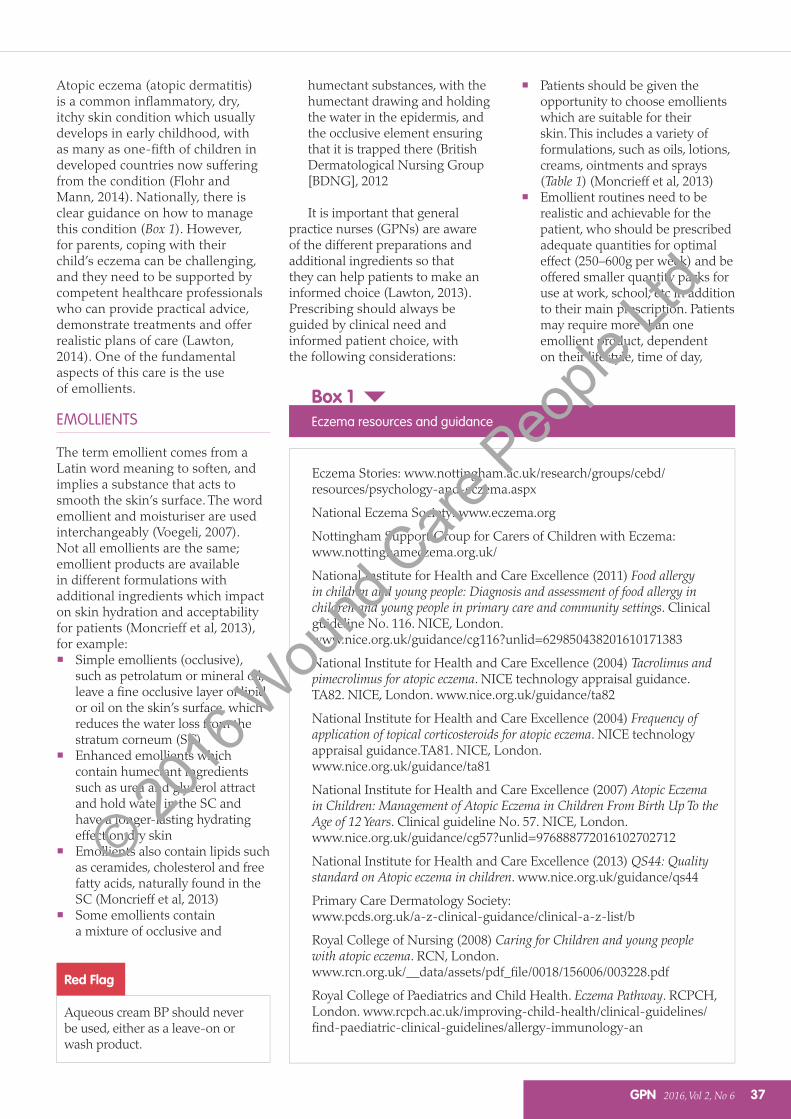
Eczema Stories: www.nottingham.ac.uk/research/groups/cebd/resources/psychology-and-eczema.aspx
National Eczema Society: www.eczema.org
Nottingham Support Group for Carers of Children with Eczema: www.nottinghameczema.org.uk/
National Institute for Health and Care Excellence (2011) Food allergy in children and young people: Diagnosis and assessment of food allergy in children and young people in primary care and community settings. Clinical guideline No. 116. NICE, London. www.nice.org.uk/guidance/cg116?unlid=629850438201610171383
National Institute for Health and Care Excellence (2004) Tacrolimus and pimecrolimus for atopic eczema. NICE technology appraisal guidance.TA82. NICE, London. www.nice.org.uk/guidance/ta82
National Institute for Health and Care Excellence (2004) Frequency of application of topical corticosteroids for atopic eczema. NICE technology appraisal guidance.TA81. NICE, London. www.nice.org.uk/guidance/ta81
National Institute for Health and Care Excellence (2007) Atopic Eczema in Children: Management of Atopic Eczema in Children From Birth Up To the Age of 12 Years. Clinical guideline No. 57. NICE, London.www.nice.org.uk/guidance/cg57?unlid=976888772016102702712
National Institute for Health and Care Excellence (2013) QS44: Quality standard on Atopic eczema in children. www.nice.org.uk/guidance/qs44
Primary Care Dermatology Society: www.pcds.org.uk/a-z-clinical-guidance/clinical-a-z-list/b
Royal College of Nursing (2008) Caring for Children and young people with atopic eczema. RCN, London. www.rcn.org.uk/__data/assets/pdf_file/0018/156006/003228.pdf
Royal College of Paediatrics and Child Health. Eczema Pathway. RCPCH, London. www.rcpch.ac.uk/improving-child-health/clinical-guidelines/find-paediatric-clinical-guidelines/allergy-immunology-an
Box 1Eczema resources and guidance
© 2016
Wou
nd C
are Peo
ple Lt
d
season and severity of eczema (Moncrieff et al, 2013). This may include a leave-on product and an emollient for washing, showering or bathing.
APPLICATION OF EMOLLIENTS
Emollients should replace detergents (soaps, shampoos, shower gels, bubble bath and hand washes, including so called ‘soap-free’ products, which should be avoided). Patients will require an emollient wash product and a leave-on emollient (Moncrieff et al, 2013). Bathing and cleansing the skin with emollients is an important aspect of any skincare routine. Emollients cleanse the skin, remove old treatments and scale, hydrate, and prepare the skin for the application of topical therapies us ed to treat eczema (Lawton, 2013). These include topical corticosteroids and topical immunomodulators. There should be a time interval of at least 30 minutes between the application of topical corticosteroids and two hours between tacrolimus and emollient. Emollients have a steroid-sparing effect and should be supplied in a 10:1 ratio of emollient to steroid to achieve the full benefit
38 GPN 2016, Vol 2, No 6
Long-term conditions: atopic eczema
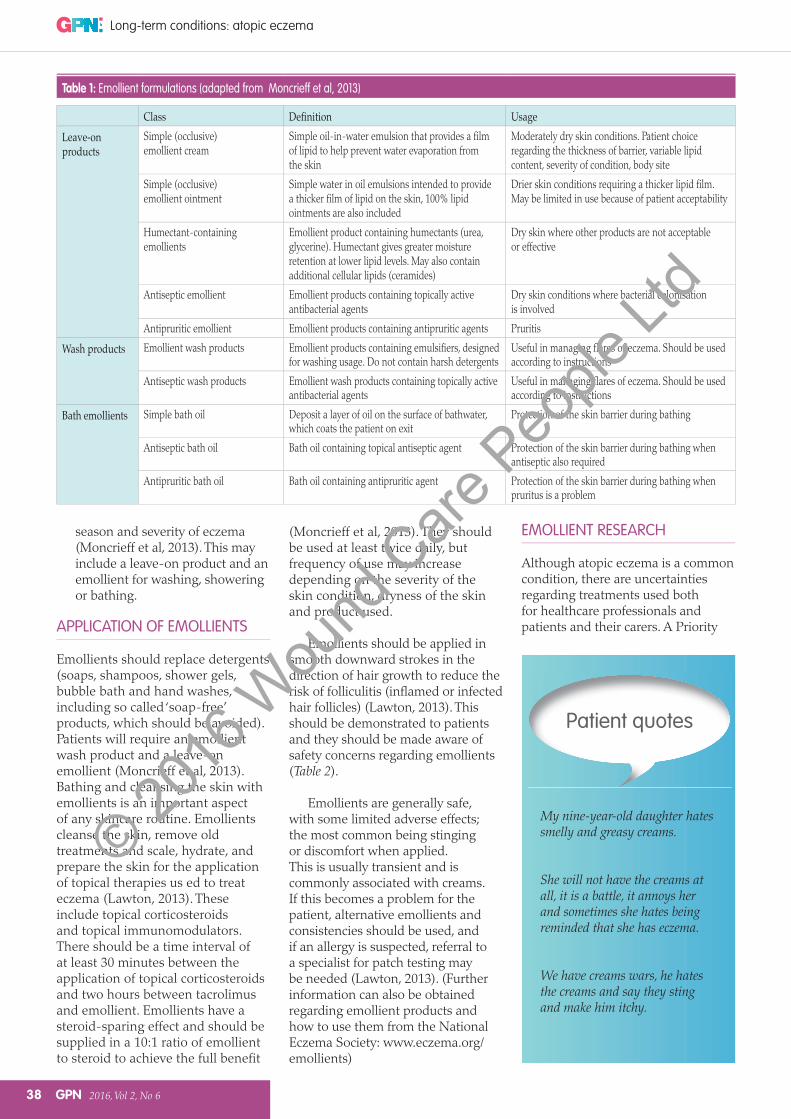
Table 1: Emollient formulations (adapted from Moncrieff et al, 2013)
Class UsageSimple (occlusive) emollient cream
Simple oil-in-water emulsion that provides a film of lipid to help prevent water evaporation from the skin
Moderately dry skin conditions. Patient choice regarding the thickness of barrier, variable lipid content, severity of condition, body site
Simple (occlusive) emollient ointment
Simple water in oil emulsions intended to provide a thicker film of lipid on the skin, 100% lipid ointments are also included
Drier skin conditions requiring a thicker lipid film. May be limited in use because of patient acceptability
Humectant-containingemollients
Emollient product containing humectants (urea, glycerine). Humectant gives greater moisture retention at lower lipid levels. May also contain additional cellular lipids (ceramides)
Dry skin where other products are not acceptable or effective
Antiseptic emollient Emollient products containing topically active antibacterial agents
Dry skin conditions where bacterial colonisation is involved
Antipruritic emollient Emollient products containing antipruritic agents Pruritis
Emollient wash products Emollient products containing emulsifiers, designed for washing usage. Do not contain harsh detergents
Useful in managing flares of eczema. Should be used according to instructions
Antiseptic wash products Emollient wash products containing topically active antibacterial agents
Useful in managing flares of eczema. Should be used according to instructions
Simple bath oil Deposit a layer of oil on the surface of bathwater, which coats the patient on exit
Protection of the skin barrier during bathing
Antiseptic bath oil Bath oil containing topical antiseptic agent Protection of the skin barrier during bathing when antiseptic also required
Antipruritic bath oil Bath oil containing antipruritic agent Protection of the skin barrier during bathing when pruritus is a problem
My nine-year-old daughter hates smelly and greasy creams.
She will not have the creams at all, it is a battle, it annoys her and sometimes she hates being reminded that she has eczema.
We have creams wars, he hates the creams and say they sting and make him itchy.
Patient quotes
(Moncrieff et al, 2013). They should be used at least twice daily, but frequency of use may increase depending on the severity of the skin condition, dryness of the skin and product used.
Emollients should be applied in smooth downward strokes in the direction of hair growth to reduce the risk of folliculitis (inflamed or infected hair follicles) (Lawton, 2013). This should be demonstrated to patients and they should be made aware of safety concerns regarding emollients (Table 2).
Emollients are generally safe, with some limited adverse effects; the most common being stinging or discomfort when applied. This is usually transient and is commonly associated with creams. If this becomes a problem for the patient, alternative emollients and consistencies should be used, and if an allergy is suspected, referral to a specialist for patch testing may be needed (Lawton, 2013). (Further information can also be obtained regarding emollient products and how to use them from the National Eczema Society: www.eczema.org/emollients)
EMOLLIENT RESEARCH
Although atopic eczema is a common condition, there are uncertainties regarding treatments used both for healthcare professionals and patients and their carers. A Priority
© 2016
Wou
nd C
are Peo
ple Lt
d
Table 2: Emollient safety
Correct application It is important to demonstrate how to apply leave-on emollients (thinly, gently, quickly, frequently) in downward, sweeping strokes in the direction of hair growth to prevent folliculitis
Pots versus pumps If pots or tubs of emollient are used, advise against putting fingers directly into them to prevent contamination and infection (Carr et al, 2008). It is good practice to decant cream and ointment from open-lid pots using a clean spoon or spatula. Emollients in pumps or tubes reduce this risk. New supplies should be prescribed at the end of treatment for infected atopic eczema
Slipping There is a risk of slipping so care should be taken when using emollients in the bath, shower, or on a tiled floor. The floor should be protected with a towel or bath mat and after bathing or showering the bath/shower should be washed with hot water and washing-up liquid, rinsed well and dried with a kitchen towel. This prevents a build-up of the emollient, skin debris and reduces the risk of infection and slipping. Using hot water and detergent helps to clear the drains and prevents a build-up of grease
Fire hazard Patients should be advised to take care when near naked flames (fires and cigarettes) if they are using paraffin-based emollients, for example white soft paraffin, white soft paraffin plus 50% liquid paraffin or emulsifying ointment, as dressings and clothing soaked with the ointment can be easily ignited (National Patient Safety Agency [NPSA], 2007)
Medicines and Healthcare products Regulatory Agency (MHRA) alert: aqueous cream
Dermatologists do not recommend the use of aqueous cream, which contains sodium lauryl sulphate (SLS) as a wash or leave-on product. Recent evidence has shown that it causes burning, stinging, itching and redness, especially in children with atopic eczema, and has a detrimental effect on skin barrier (MHRA, 2013). There are better emollient formulations available that have a positive effect on skin barrier function
GPN 2016, Vol 2, No 6 39
Table 3: Top 14 treatment uncertainties for eczema (Batchelor et al, 2013)
Shared uncertainties
What is the best and safest way of using topical steroids for eczema: frequency of application, potency,length of time, alternating with other topical treatments and age limits for treatment?What is the long-term safety of applying steroids to the skin for eczema?What role might food allergy tests play in treating eczema?Which emollient is the most effective and safe in treating eczema?
Patient and carer
What is the best psychological treatment for itching/scratching in eczema?What is the best way for people with eczema to wash: frequency of washing, water temperature, bath versus shower?What are the best and safest natural products to apply to the skin for eczema?How much does avoidance of irritants and allergens help people with eczema?What is the role of diet in treating eczema: exclusion diets and nutritional supplements?
Healthcare professional
Which is most effective in the management of eczema: education programmes, GP care, nurse-led care, dermatologist-led care or multidisciplinary care?Which is safer and more effective for treating eczema: steroids or calcineurin inhibitors?How effective are interventions to reduce skin infections in the management of eczema?Which should be applied first when treating eczema, emollients or topical steroids?What is the best and safest way of using drugs that suppress the immune system when treating eczema?
excellent resources (Box 2) available to inform practice, and research is focusing on prevention, treatment and management of atopic eczema (Wedgeworth et al, 2013).
CONCLUSION
Emollients are first-line therapy for atopic eczema and should be used even when eczema is clear (National Institute for Health and Care Excellence [NICE], 2007).
Efficacy is dependent on usage and patient adherence and therefore informed patient choice is pivotal in determining which emollient is recommended. The patient’s age, individual needs, skin condition and preferences should be considered when selecting an emollient. An understanding of which emollient product (Table 1), additional ingredients, price, application frequency and safety issues are paramount. Appropriate use of emollients, prescribed at the right time and in sufficient quantities has the potential to improve patients’ quality of life and reduce prescribing costs (Moncrieff et al, 2013).
REFERENCES
Batchelor JM, Ridd MJ, Clarke T, et al (2013) The Eczema Priority Setting Partnership: A collaboration between patients, carers, clinicians and researchers to identify and prioritise important research questions for the treatment of eczema. Br J Dermatol 168(3): 577–82
British Dermatological Nursing Group (2012) Best practice in emollient therapy a statement for healthcare professionals. Available online: www.bdng.org.uk/resources/ (accessed November, 2016)
Carr J, Akram M, Sultan A, et al (2008) Contamination of emollient creams and ointments with Staphylococcus aureusin children with atopic dermatitis. Dermatitis 19(5): 282
Flohr C, Mann J (2014) New approaches to the prevention of childhood atopic dermatitis. Allergy 69: 56–61
Lawton S (2013) Safe and effective application of topical treatments to the skin. Nurs Standard 27(42): 50–8
Lawton S (2014) Managing difficult and severe eczema in children. Nurse Prescribing 12(1): 235–9
Setting Partnership (PSP) highlighted the top 14 uncertainties, which has provided guidance for future research. Of these, several focused on emollients and their use with other treatments (Table 3; Batchelor et al, 2013). GPNs need to be aware
of the current evidence base around the treatment and management of atopic eczema, as keeping up to date and implementing current guidance/research is the responsibility of every healthcare professional (Lawton, 2014). There are now
GPN
© 2016
Wou
nd C
are Peo
ple Lt
d
40 GPN 2016, Vol 2, No 6
Long-term conditions: atopic eczema
Lawton S (2014) Atopic eczema; the current state of clinical research. Br J Nurs 1061–66
Medicines and Healthcare products Regulatory Agency (2013) Drug safety update: aqueous cream: may cause skin irritation, particularly in children with eczema, possibly due to sodium lauryl sulfate content. Available online: www.mhra.gov.uk/safety-public-assessment-reports/CON251956 (accessed November, 2016)
Moncrieff G, Cork M, Lawton S, et al (2013) Use of emollients in dry-skin conditions: consensus statement. Clin Experiment Dermatol 231–8
National Patient Safety Agency (2007) Fire hazard with paraffin-based skin products. NPA, London. Available online: www.nrls.npsa.nhs.uk/resources/?EntryId45=59876 (accessed November, 2016)
National Institute for Health and Care Excellence (2007) Atopic Eczema in Children: Management of Atopic Eczema
in Children From Birth Up To the Age of 12 Years. Clinical guideline No. 57. NICE, London. Available online: www.nice.org.uk/guidance/cg57?unlid=976888772016102702712
Voegeli D (2007) The role of emollients in the care of patient’s with dry skin. Nurs Standard 62–8
Wedgeworth EK, Sharp H, Powell A, Flohr C (2013) What’s new in eczema? Part 2: Prevention, treatment and management. Dermatological Nurs 10–18
Wedgewood EK, Sharp H, Powell A, Flohr C (2012) What’s new in eczema? Part 1: Epidemiology and pathophysiology.Dermatol Nurs 9–1
Further reading
Santer M, Muller I, Yardley L, et al (2016) Parents’ and carers’ views about emollients for childhood eczema: qualitative interview study. BMJ Open e011887
Santer M, Burgess H, Yardley L, et al (2013)Managing childhood eczema: qualitative
Key points
Atopic eczema (atopic dermatitis) affects one fifth of children in developed countries.
The term emollient comes from the Latin meaning to soften and implies a substance that acts to smooth the skin’s surface.
All healthcare practitioners advising patients regarding skin disease should understand the ‘spectrum’ of emollient options.
Emollients are first-line therapy for atopic eczema and should be used even when eczema is clear.
study exploring carers’ experiences of barriers and facilitators to treatment adherence. J Adv Nurs 2493–2501
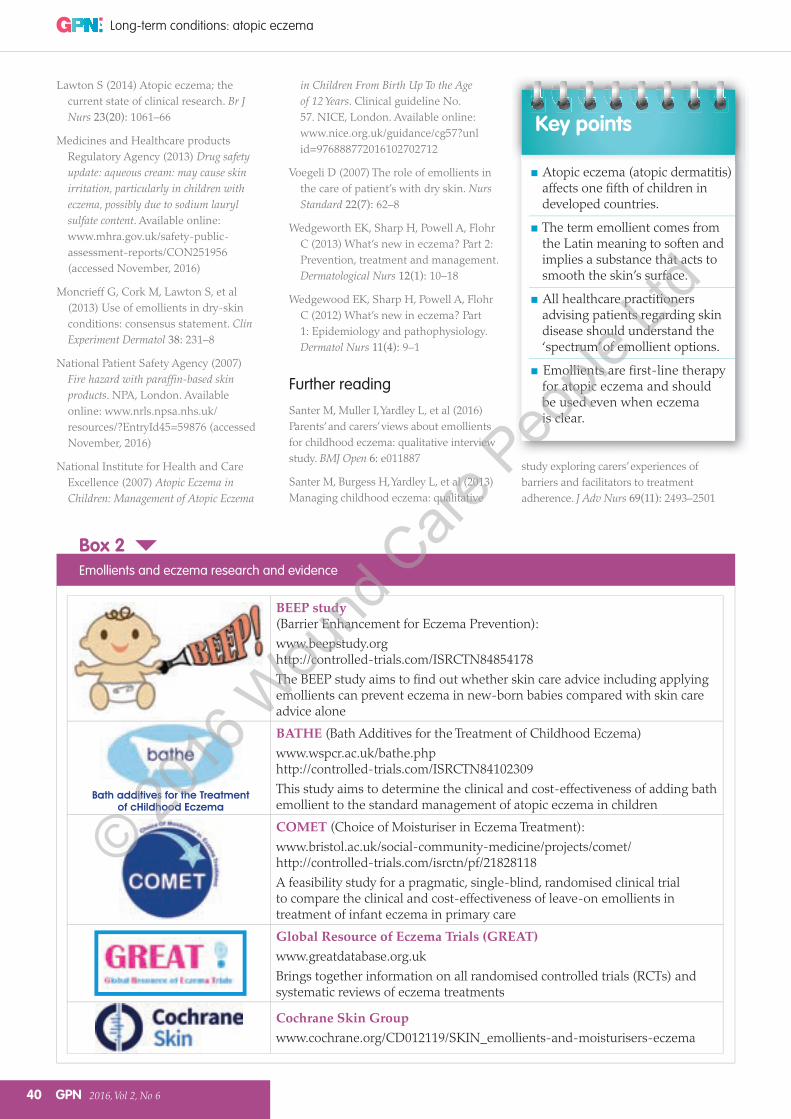
Box 2Emollients and eczema research and evidence
Bath additives for the Treatment of cHildhood Eczema
BEEP study (Barrier Enhancement for Eczema Prevention):www.beepstudy.org http://controlled-trials.com/ISRCTN84854178The BEEP study aims to find out whether skin care advice including applying emollients can prevent eczema in new-born babies compared with skin care advice alone
BATHE (Bath Additives for the Treatment of Childhood Eczema)www.wspcr.ac.uk/bathe.phphttp://controlled-trials.com/ISRCTN84102309This study aims to determine the clinical and cost-effectiveness of adding bath emollient to the standard management of atopic eczema in children
COMET (Choice of Moisturiser in Eczema Treatment):www.bristol.ac.uk/social-community-medicine/projects/comet/ http://controlled-trials.com/isrctn/pf/21828118A feasibility study for a pragmatic, single-blind, randomised clinical trial to compare the clinical and cost-effectiveness of leave-on emollients in treatment of infant eczema in primary care
Global Resource of Eczema Trials (GREAT)www.greatdatabase.org.ukBrings together information on all randomised controlled trials (RCTs) and systematic reviews of eczema treatments
Cochrane Skin Groupwww.cochrane.org/CD012119/SKIN_emollients-and-moisturisers-eczema
© 2016
Wou
nd C
are Peo
ple Lt
d