2011 RYLA Participant Info and Health Forms

of 10
-
Upload
katie-mccarthy -
Category
Documents
-
view
215 -
download
0
Transcript of 2011 RYLA Participant Info and Health Forms
-
8/6/2019 2011 RYLA Participant Info and Health Forms
1/10
Rotary District 7500Rotary Youth Leadership Awards
June 25-28, 2011Monmouth University, West Long Branch, NJ
www.ryla7500.org
Congratulations! You made it!
What is RYLA?District 7500 RYLA is an intense and fun-filled four-day leadership training program runby Rotarians and previous RYLA participants who have demonstrated superior
leadership and training skills, within RYLA and in their communities. We hold our RYLAat Monmouth University in West Long Branch, NJ, usually the last weekend of June,from Saturday through Tuesday.
We teach a variety of leadership skills, such as team-building, problem-solving,cooperation and communication skills. Our program is designed to help train ethical,visionary leaders.
The RYLA conference is planned and run by the Rotary District 7500 RYLA Committee.Each team of about 16 RYLA participants is directly supervised by 3-4 counselors, whoare typically 1-2 years older then the participants, and one Advisor who is typically 4-10years older than the participants.
Who pays for RYLA?The cost for each participant in 2011 is $420. This price includes room, meals, a teeshirt and all program expenses. Most sponsoring Rotary Clubs are paying $395 of this
amount and asking the participants to contribute just $25. (Your local Rotary Club maybe doing it a little differently. Ask them.)
What to do now:
-
8/6/2019 2011 RYLA Participant Info and Health Forms
2/10
What to do now:
Rotary District 7500Rotary Youth Leadership Awards
June 25-28, 2011Monmouth University, West Long Branch, NJ
www.ryla7500.org
Participant Information SheetParticipant should keep this sheet and refer to it when getting ready for RYLA
Dates: Saturday, June 25, 2011 (8:45am) through Tuesday, June 28, 2011 (8:30pm)
Where: Monmouth University400 Cedar Avenue, West Long Branch, NJ 07764 (732) 571-3400
What youreally need
to bring:
Clothes for 4 days, three nights (Shorts & tee shirts are fine. Use common sense.) Sheets (for twin beds), blanket, pillow and/or sleeping bag Personal hygiene products: shampoo, soap, bath towel, washcloth, shower shoes, etc. Swim suit & swim towel, in a plastic shopping bag, labeled clearly with your name
(have this readily accessible when you arrive so we can take it to the pool for you)
Sunscreen (sunscreen is very important!)
Exercise clothes (sneakers, gym shorts, etc.) Sweater or sweatshirt (air conditioned rooms can sometimes be chilly) Reusable sports water bottle for drinking water (this is also very important!) Alarm clock Pen or pencils & notebook Personal medications in their original containers
Optional
items youmight want
to bring:
Second pair of shoes
Rain coat or umbrella Digital camera & charger No more than $20 spending money in small bills (for snacks, soft drinks, etc.) Musical instrument & sheet music or art supplies or sports equipment
-
8/6/2019 2011 RYLA Participant Info and Health Forms
3/10
Rotary District 7500Rotary Youth Leadership Awards
June 25-28, 2011Monmouth University, West Long Branch, NJ
www.ryla7500.org
Notice of Health Information PracticesParticipants Copy
This notice describes how medical information about you may be used and disclosed and how you can get access to this information.
Understanding Your Health Record InformationEach participant in the RYLA program must complete a health history form. This record contains health and medical information
generated by you for use if and when needed during the RYLA program. In this notice Notice of Health Information Practices, weshall refer to the information contained in your record as your health information. This term shall have the same meaning asprotected health information defined in the Health Insurance Portability and Accountabili ty Act of 1996, as amended (HIPAA).
Your Health Information RightsWithin the limits provided by federal and state law, you have the right to:
Request restrictions on certain uses and disclosures of your health information; Receive confidential communications of your health information. You may request that we communicate with you about
your health information by alternative means or at an alternative location;
Inspect and obtain a copy of your health information, except with regard to psychotherapy notes or information compiled inreasonable anticipation of certain civil, criminal or administrative proceedings;
Request an amendment to your health information that you have created. Obtain an accounting of certain disclosures of your health information; and Receive a paper copy of this Notice in addition to any electronic copy you may receive.
You may exercise any of the above rights by submitting a request in writing to our Registrar.
Our ResponsibilitiesThe RYLA program is required by law to:
Maintain the privacy of your health information; Provide you with this Notice of our legal duties and privacy practices with respect to health information we collect and
maintain about you;
Abide by the terms of this Notice, currently in effect, and as amended from time to time;
-
8/6/2019 2011 RYLA Participant Info and Health Forms
4/10
Rotary District 7500Rotary Youth Leadership Awards
June 25-28, 2011Monmouth University, West Long Branch, NJ
www.ryla7500.org
Notice of Health Information Practices(continued)
Participants Copy
More information or to Report a ProblemIf you would like to submit a comment or complaint about our privacy practices, please contact our Registrar:
Eric Stofman
RYLA Registrar1060 N. Kings Hwy, Suite 110
Cherry Hill, NJ 08034(856) 667-4567
You may also file your complaint with the Secretary of Health and Human Services. You will not be penalized or otherwise retaliatedagainst for filing a complaint.
Examples of Uses and Disclosures for Treatment, Payment and Health Operations
The following are examples of uses and disclosures of your health information which are permitted by law:
We will use your health information for treatmentWe will use your health information to provide medical services to you if necessary. Any of our staff involved in your care or seekingcare on your behalf will have access to your health information. We may also provide your health information to other health careproviders involved in your care to assist them in providing services to you. However, we will not disclose psychotherapy notes orinformation to health care providers who are not the originators of that information unless we have your written authorization to do so.
We will use your health information for regular health care operations.Members of our staff may review and use information from your record to assess the care and outcomes in your case and others like it.
Communication with Persons involved in Your Care:We may disclose your health information that is directly relevant to your care to individuals involved in your care and individuals youwish to receive such information, including family members, relatives, close personal friends, or other persons you identify. Before
-
8/6/2019 2011 RYLA Participant Info and Health Forms
5/10
Rotary District 7500Rotary Youth Leadership Awards
June 25-28, 2011Monmouth University, West Long Branch, NJ
www.ryla7500.org
Consent to Use or Disclose Information
for Treatment, Payment, and Health Care Operations
(Please type or print) Participants Name: ______________________________________________
Federal regulations allow us to use or disclose protected health information from your Health History form in order to providetreatment to you if necessary, and for other professional activities known as health care operations (for example, quality
improvement activities).
With this consent form, we are asking you to make the permission explicit. By signing this consent, you are giving us permission touse or disclose your protected health information for these activities.
These uses and disclosures are described more fully in our Notice of Health Information Practices. You have the right to review thatNotice before signing this consent. We reserve the right to revise our Notice of Health Information Practices at any time. If we do so,the revised Notice will be available at the registration desk on the first day of the RYLA program. You may ask for a printed copy ofour Notice at any time.
You may ask us to restrict the use and disclosure of certain information in your record that otherwise would be allowed for treatment,or health care operations. However, we do not have to agree to these restrictions. If we do agree to a restriction, that agreement isbinding.
I wish to have the following restrictions put on the use or disclosure of the health information:
-
8/6/2019 2011 RYLA Participant Info and Health Forms
6/10
Rotary District 7500Rotary Youth Leadership Awards
June 25-28, 2011Monmouth University, West Long Branch, NJ
www.ryla7500.org
Acknowledgement of Receipt of
Notice of Health Information Practices
(Please type or print) Participants Name: ___________________________________________
I have received a copy of the Notice of Health Information Practices for the Rotary District 7500-RYLA. I understand that RYLAreserves the right to modify these practices, if necessary, or as required by law.
Parent/Guardian Signature: ___________________________________________________________Date: _________________
Parent/Guardian Name: (please print) _______________________________________________________________
Parental/Guardian Authorization
I give my consent for my son/daughter, listed above, to participate in the Rotary District 7500-Rotary Youth Leadership Awardsprogram (hereinafter called RYLA) and do hereby release and hold harmless District 7500, the RYLA Committee, the RYLA staff,the sponsoring Rotary Clubs, and Monmouth University from any and all liability. In case of emergency I hereby give permission forRYLAs medical team to secure and provide whatever health services are determined necessary for our sons/daughters health,
including dispensing any medications that the medical team determines is in my son/daughters best interests. I understand that theRYLA staff will be taking photos of events at RYLA and understand that my son/daughter may appear in some of those photos and Igive permission to use these photos on the RYLA website, in RYLA brochures, etc. I understand that there are a few firm rules atRYLA, for example, attending all activities, not being out of the dorms after-hours, not texting during programs, respecting thecampus property, etc. and agree that if my son/daughter repeatedly breaks these rules that I am responsible to come get him/herimmediately and take them home.
-
8/6/2019 2011 RYLA Participant Info and Health Forms
7/10
Rotary District 7500Rotary Youth Leadership Awards
June 25-28, 2011Monmouth University, West Long Branch, NJ
www.ryla7500.org
Participants Health History
(Please type or print) Participants Name: ___________________________________________
Date of Birth: _______________ Height: _______ Weight: ________ Sex: Male Female
Participants Mailing Address: __________________________________________________ Phone #:______________________
City: ______________________________________ State: NJ Zip: ____________ Another Phone #:____________________
Physician: __________________________________________________ Physician Phone #: _______________________________
Do you have, or have you had, any of the following? (Check yes or no)Allergies to Medication Yes NoAllergies to Food Yes NoAllergies (Seasonal) Yes No
Allergies to Bee Stings Yes NoAsthma Yes NoAsthma (Exercised Induced) Yes NoBack Problems Yes NoBleeding Disorders Yes NoDiabetes Yes NoDo you Smoke Yes NoEpilepsy Yes NoFractured Bones Yes No
Head Injury Yes NoHearing Problems Yes NoHeart Disease Yes NoHepatitis Yes No
Hernia Yes NoHigh Blood Pressure Yes NoInfectious Mononucleosis Yes No
Joint Problems Yes NoKidney Disease Yes NoSkin Diseases Yes NoSurgery Yes NoThyroid Disease Yes NoUnder Doctors Care Yes NoRecent Upper Respiratory Infection Yes NoVaricella (chicken pox) Yes NoWear Glasses or Contacts Yes No
Other:________________________________________________________________________________________________________________________________________________
-
8/6/2019 2011 RYLA Participant Info and Health Forms
8/10
Rotary Youth Leadership AwardsDistrict 7500
Program Book Order Form
The Rotary Youth Leadership Awards (RYLA) is a non-profit youthleadership development program available to high school studentsthrough Rotary International. Rotary is a worldwide organizationof more than 1.2 million business, professional, and communityleaders providing humanitarian service, encouraging high ethicalstandards in all vocations, and helping build goodwill and peace in
the world.
Each year, young men and women from Monmouth, Burlington andOcean Counties are trained in a variety of leadership skills. Some ofthese lessons include communication skills, goal setting, teambuilding, problem solving and many other personal developmentskills. District 7500 RYLA will take place June 25th - 28th atMonmouth University. You can learn more about our mission by
visiting our website atwww.ryla7500.org.
We are seeking local program support by selling ad space in our2011 Reflection Ceremony Program Book. By placing an ad inthis booklet, your company will have exposure to more than 250families in Monmouth, Burlington, and Ocean Counties.
Please send electronic copies of ads to: [email protected]
as a .JPEG, .PDF, or Word Doc. If you have trouble with thoseformats, please contact Kevin and he can work with you directly.
District 7500 would like to thank you in advance for yourib i O ld b ibl i h
http://www.ryla7500.org/http://www.ryla7500.org/http://www.ryla7500.org/http://www.ryla7500.org/ -
8/6/2019 2011 RYLA Participant Info and Health Forms
9/10
Directions to
FromBurlington
County:
NORTH on 295 (or NJTP) to 195 EAST to Garden State Pkwy (GSP) NORTHGSP NORTH to Exit 105 (Rt 36 East)See directions below from GSP Exit 105
FromOcean
County:
Take Garden State Pkwy NORTHto Exit 105 (Rt 36 East)See directions below from GSP Exit 105
From GSPExit 105:
From the Garden State Pkwy go EAST onRt 36 for about 3 milesTurn SOUTH onto Rt 71 (Monmouth Rd)Monmouth Rd becomes Cedar Ave(bear left at fork)Follow Cedar Ave to college
Monmouth University 400 Cedar Avenue, West Long Branch, NJ 07764 (732) 571-3400
-
8/6/2019 2011 RYLA Participant Info and Health Forms
10/10
Page 10 of 10
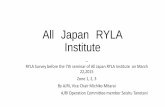
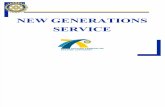
Map of Monmouth University
Main Entrance
Parking Dorms
Dining Hall
Wilson Hall
Student Center
Gym & PoolPollak Theatre
White Gates
Cedar Ave