YG ED Student Induction Pack v1.2
20
Medical Student Information Pack v1.2 December 2015 Dr Linda Dykes Dr Helen Salter www.mountainmedicine.co.uk
-
Upload
ysbyty-gwynedd-emergency-department -
Category
Documents
-
view
166 -
download
1
description
An introduction to Ysbyty Gwynedd Emergency Department for students coming to us from Cardiff University, and also those on SSCs (Swansea & others), or Electives. Last updated December 2015.
Transcript of YG ED Student Induction Pack v1.2

Medical Student Information Pack
v1.2 December 2015 Dr Linda Dykes Dr Helen Salter
www.mountainmedicine.co.uk
Contents 2
2 Welcome & Contents
3/4/5 What to expect
6 Who’s Who
7/8 Practical Skills
9 How not to feel like a spare part
10 Seeing your own patients
11/12 FAQs
13 Final thoughts & extra activities
14 Map of the ED
Introduction Welcome to Ysbyty Gwynedd Emergency Department - better known as “Bangor ED”!
If you are here as an elective or SSC student, thank you for choosing to spend your placement with us! And if you’re here as a 3rd year (Hospital Front Door) or 5th year (Junior Student Assistantship) from Cardiff, then you are in luck: our ED is one of the most sought-after student placements in the UK! So even if you weren’t originally planning on coming up to Bangor, we intend to provide you with a fantastic introduction to EM.
This aim of this pack is to provide you with sufficient information that you can feel prepared for your placement with us, but if you’re feel a bit apprehensive, please don’t worry… all the
ED staff are used to welcoming and teaching students, and you’ll soon settle in.
A word about pre-reading: you don’t need to, but if you’d like to get a bit of flavour about Emergency Medicine in advance, we recommend the Oxford Handbook of Emergency Medicine, or Lecture Notes in Emergency Medicine. The “OHEM” is ideal for reading short chunks whilst sitting on the toilet, whereas “Lecture Notes” is better suited to an afternoon reclining on the sofa!
This information pack is a first edition and we’ve included the information previous students told us. If you can think what we should add, please tell us!
Linda Dykes & Helen Salter Consultants in EM
Follow us on Twitter! @YGEDBangor

3
What to expect 1. Elective students and SSC students without major written projects • Senior medical students • Placements at least 4 weeks long
The focus of your placement will be immersion in Emergency Medicine! After you have spent a day or two settling into the ED, you will start to see your own (stable) patients fresh off the pile, tackling the history and examination and then presenting the case to one of the doctors in the shop floor. We will help you develop your ability to produce a differential diagnosis and management/ investigation plan.
We’ll also take you into the Resus room where you will assist the doctors with sicker patients, have you “scribing” for the Trauma Team, and helping (supervised, of course) with chest compressions when we treat patients in cardiac arrest. You’ll also spend some time in our Minor Injuries area, where our highly-skilled Emergency Nurse Practitioner (ENP) team will introduce you to the art & science of musculoskeletal examination, documentation & extremity x-ray interpretation. This is also where you’ll learn about wound care and hopefully get the opportunity to suture - you’ll need to keep your eyes peeled for suitable cases.
Elective & SSC students are loaned these fetching Pistachio-coloured scrub tops
Other activities
During your time with us, there may be opportunities to assist with paramedic or Mountain Rescue training if you’re willing to “play casualty”. There’ll almost certainly be a pre-hospital simulation session you can attend (both these activities will need a car or lift).
If you can provide evidence of having had Violence & Aggression/breakaway training (and with advance notice) we can organise an observer shift with Welsh Ambulance, but you’ll need to do have done the V&A training before coming to Ysbyty Gwynedd. Sadly, we can no longer access any helicopter shifts.
Working pattern
You’ll be expected to work hard whilst in the ED, but we also expect you to enjoy yourself and hopefully get out and enjoy all that Snowdonia and Anglesey has to offer! You’ll work flexitime: your university will expect you to work for about 40 hours a week, and you’ll get the most to of your time in ED if this includes evenings, weekend and even a couple of night shifts. If you are here when we are also hosting multiple Cardiff students, we may ask you to arrange your shifts at times when they aren’t around, or to pop to the Minors area if Majors/Resus is overwhelmed with multiple students. You must adhere to EWTD (max 13 hours on duty, minimum of 11 hours off between shifts).
Supervision
Your nominated supervisor will usually be ED consultant Dr Linda Dykes, who has 10 years’ experience of supervising medical students. Linda will try to meet with you within your first week or two in order to draw up some individual learning goals for the placement, and again towards the end.
However, your main supervisors on a day-to-day basis will be the Clinical Fellows (our fantastic middle-grades/Registrar equivalents, some of whom have a specific interest in Medical Education) plus our SHO-tier doctors… hosting medical students is very much a team sport in the ED! Linda is less than full time in the ED and it’s possible that your shop floor shifts may not overlap at all.
Projects? Audit?
if you’d like to undertake a small project or audit whilst in the ED, this can sometimes be arranged, but please let Linda know about 4 weeks in advance if this is the case - [email protected] or Tweet her on @mmbangor
We can only supervise projects we are not anticipating when there are no other Elective/non-project SSC students in the ED (we can only manage one “project student” at a time).

4
What to expect II2. SSC students with a major written project • Senior medical students • Placements at least 4 weeks long
Your placement goals will be a mixture of all-round experience in Emergency Medicine, and producing a quality written project. Dr Linda Dykes will meet with you as soon as possible after you start to discuss your project with you (this will need to be done via email beforehand if she is due to be away when you start) and every couple of weeks through the placement.
You will have a learning contract and a timetable plan outlining the split between shop floor and project-time: there’s an example in the Appendix, from the 8-week Senior Clinical Project we used to host under the old Cardiff curriculum. See also Page 3 - this information
applies to you too!
We try really hard to help our “project students” produce a conference abstract from their project - the vast majority of students who have come to Bangor ED since 2005 achieved their first publication this way. We will support you every step of the way with this: it’s actually very easy when you know how!
How to keep Medical Students happy in your ED
Hannah Browne & Anna Woodman (Medical Students)Dr Linda Dykes (Consultant EM)
Ysbyty Gwynedd, Bangor, North Wales
“...it was the best placement of Medical School”
Objectives & BackgroundThe Emergency Department (ED) in Ysbyty Gwynedd, Bangor, has hosted Senior Clinical Projects (SCPs) for Cardiff medical students since 2005, and gained a reputation for providing unique student experiences. We wished to determine which aspects of these SCPs were most appreciated.
Method
Contact details were available for 25 of 45 former students who undertook their final-year SCP in Bangor ED. These individuals were invited to complete an online survey. Questions about specific aspects of the SCP were ranked from 0 (least value) to 5 (highest). 17 responses were received, 68% of those contacted.
Results ★ 12/17 undertook the Mountain Medicine SCP,
four “plain” Emergency Medicine (EM) and one Comparative Medicine.
★ 14/17 (82%) stated that their SCP identified Emergency Medicine as a possible future career; 2/17 (12%) said it confirmed Emergency Medicine as their intended career.
★ Bangor ED SCP was the “best placement of medical school” for 15/17 (88%)
★ Clerking, examining and practising clinical skills on patients was valued very highly (5/5) by 70%.
★ 100% of the 14 students who went flying with RAF Search and Rescue rated this highly (4/5 or 5/5).
★ 78% of those who shadowed an ambulance shift (n=9) rated the experience highly.
★ Of the now-qualified participants (n=13) 38% are currently working or applying for jobs in EM. The remaining 62% are working/applying for other acute specialties.
Conclusion
Emergency Department placements may be the highlight of medical school for some students, and can inspire future careers in EM. Students fortunate enough to undertaken their SCPs in Bangor ED rated local unique opportunities (notably the flying day with RAF SAR) exceptionally highly, alongside traditional EM exposure within the department.
We encourage any units hosting medical students to consider what unique opportunities they can offer their medical students: thinking outside the box helps optimise the student experience.
www.mountainmedicine.co.uk
Pelvic Fractures in Snowdonia Mountain Casualties:To splint or not to splint?Hannah Browne, Final Year Medical StudentDr Linda Dykes, Consultant in EMYsbyty Gwynedd, Bangor, North Wales
Background
Mountain Rescue Teams in Snowdonia endeavour to use pelvic splints as per JRCALC guidelines. However, mountain casualties with major mechanisms of injury are often found in precarious locations where application of splints is challenging.
We wondered whether the pelvic fractures seen in mountain casualties are of the type likely to benefit from splintage.
Method• The Bangor Mountain Medicine database (consist of all casualties brought to
Ysbyty Gwynedd following contact with MRT and/or RAF SAR helicopter) Jan 2004-October 2012 was interrogated and pelvic fracture cases identified.
• Fracture type was analysed from all available imaging using the Tile classification by a Consultant musculoskeletal radiologist.
• For fatalities, post-mortem reports were examined.
Results
• Of 913 casualties in the study period, 730 (80%) were injured rather than ill.
• 18/730 (2.5%) of trauma casualties had a confirmed pelvic fracture.
• 14/18 (78%) had fallen from height; 2 were mountain-biking; one crashed his paraglider and one sustained an acetabular fracture in a simple fall.
• 4.3% of casualties who had fallen from a height greater than standing sustained a pelvic fracture.
• 2/18 died at scene: post-mortem reports implied severe pelvic disruption but could not be classified further.
• In a further 3 cases, imaging was not available, leaving 13 cases for radiological analysis.
• 13/13 (100%) of fractures could be classified using the Tile system: 61% A1, 31% A2 and 8% C2.
Conclusion
Pelvic fractures are uncommon in Snowdonia mountain casualties, and, in survivors, the vast majority are stable (92%, cf. 55% in urban casualties1). Severe pelvic disruption was seen only in casualties declared dead at scene.
Only one casualty in a nine-year period had a pelvic fracture that might benefit from a pelvic splint.
Our data suggests that application of pelvic splints need not be considered a high priority in mountain casualties, especially in precarious locations.
Reference:1. Gansslen A, Pohlemann T et al. Epidemiology of pelvic ring injuries. Injury 1996;27(1):13-20
www.mountainmedicine.co.uk
Most of our students end up with a conference poster on their CV after an SSC in Bangor, but occasionally they go one step further & end up presenting at a conference. This is Naomi Dodds at a conference in Italy!

5
What to expect III
3. Junior Student Assistantships • Cardiff Final-years (18 students per block) • Each spend 2 shifts in the ED during JSA
As a JSA student, you will spend most of your time on the wards, but you will spend two shifts in the ED. To ensure maximum education benefit from this brief snapshot of life in the Emergency Department, these shifts will usually be spent with one of our MedEd Clinical Fellows, who will be free from shop-floor commitments enabling dedicated attention to your learning. You’ll see patients with your MedEd Fellow, either de novo to see the whole process, and/or popping in to see various patients in the ED with features in their history or physical examination that can be used as a springboard for discussion.
The EM MedEd Fellows will also facilitate some of your “MyPractice” sessions, and will assist in doing your workplace-based assessments. You will be timetabled for your ED shifts, and wear your own clothes plus your red Medical Student lanyard.
4. Hospital Front Door • 3rd year Cardiff Students • Spent 3 weeks based in ED, 3 weeks based in AMAU (+ one week in GP & intro week)
The HFD placement is completely new - it’s a feature of the new C21 Cardiff curriculum. We are looking forward to our “Pathfinders” arriving, and we will be standing by to evolve what we do pretty rapidly, but we are anticipating that our HFD students will start off by seeing patients with their supervising shop-floor ED doctor (usually an SHO- or middle-grade tier doctor) and then following that patients through their journey. For example, if the patient is admitted, you will go with them to the ward/attend the relevant post-take ward round etc.
During the Intro Week you will spend some time in all the acute clinical areas including the ED, Medical Assessment Unit (MAU, on Gogarth ward), Surgical Assessment Unit (SAU), theatres and ITU. This is to familiarise you with all these areas so you can follow the patient from arrival in ED to the next clinical area to follow their journey through the hospital.
You’ll then spent 3 weeks in MAU followed by ED (or vice versa). Towards the end of the three weeks in ED, we anticipate that students will want to see some patients “fresh” from the pile, and if we think you are ready, we will find you some suitable, stable patients for you to take a history from and examine.
During your HFD block, there are sessions on Thursdays (probably 11-2 but final confirmation awaited) where you will be issued with a new “virtual case” and discuss the previous week’s set case/homework: about four of these sessions will be with our ED MedEd Fellows. You have to present at three of these Thursday sessions during your HFC block, and also have three mini-CEXs to complete, so look out for suitable cases from the start of our HFD placement.
We hope to provide some MedEd Fellow sessions to work with you on the ED shop floor using a variety of teaching models to assist your learning.
You will be timetabled for your ED shifts, and issued with pale grey scrub tops to help ED (and other) hospital staff identify you as a 3rd year medical student. It may be possible for you to undertake additional time in ED if you wish (subject to EWTD compliance), but not if we have other students (Electives/SSCs) or clinical visitors who also require shop-floor ED exposure at the same time… we limit students and clinical visitors to two in the Majors & Resus area (plus one in Minors) at any one time, to maintain quality of clinical experience for everyone.
The ED Lead for the HFD programme is Dr Helen Salter, Consultant in EM. Finally, please don’t forget that we will be actively seeking your feedback and suggestions on the HFD module as it evolves.

Who’s Who in the ED - medical staff
Consultants & Associate Specialists
We currently have five substantive EM Consultants, a locum (Mr Sabri) and two Associate Specialists (Mr Khalid & Dr Poeppinghaus) who are also on the Senior Doctor tier. In addition, Mrs Pauline Cutting - who was the senior EM consultant here for many years - does sessions for us regularly. She has a wealth of experience and you will learn a lot from her.
Name Supervisor of… Responsible for/interested in
Dr Rob Perry (Lead Clinician)
F2s (except Academic F2) Major Trauma Lead Complaints ED Ultrasound & ED Simulation lead
Dr Linda Dykes
Clinical Fellows (with Helen) ST4-6s
Anything to do with GP or PHEM/SAR Works with Welsh Ambulance one day a week (hence is less than full time in the ED) Medical Students (Electives & SSCs)
Dr Leesa Parkinson
Academic F2 ACCS trainees inc CT3
Anything to do with Paediatrics (dual-qualified in PEM) QAAC (our version of rapid assessment on arrival) Patient Safety Lead TARN
Dr Helen Salter Some Clinical Fellows (with Linda)
Audit Lead Appraisal - very popular appraiser choice for our middle grades Medical Students (Cardiff 3rd year programme)
Dr Pete Williams
TBC - he’s only just arrived!
Also works with EMRTS. Will be supporting Linda with the Clinical Fellows. Dual-accredited in Paediatric EM.
Dr Vanessa Poeppinghaus
GPSTs Rota master for SHO tier, plus oversees Middle Grade tier Locum co-ordinator (with Lou Lee our secretary)
Mr Khalid Arain ENP team Minor injuries (he is a real guru…)
Clinical Fellows (Middle Grades) NB - correctly referred to as “Clinical Fellow” or “Middle Grade” in medical notes, not “Registrar”
Our Clinical Fellows are post-ACCS doctors (i.e. at least 5 years post-graduation and equivalent to Specialty Registrars in terms of their seniority) who come to Bangor for 6-18 months.
Most of them do 20% pre-hospital EM, but those with an asterisk also have a Medical Education interest & those with two asterisks have dedicated MedEd sessions:
*Dr Niki Boyer *Dr Kim Hallam Dr Julie Hunt Dr Pooja Kathuria (till Feb 2016) Dr Ruth Watson Dr Mo Dingle **Dr Andrew Jacklin **Dr Madeleine Rowe Dr Jim Moonie (till Feb 2016) Dr Kimarnie Ki-Kydd (from Feb 2016) Dr Jamit M (from Jan 2016) Dr Gareth Thomas (from Jan 2016)
Other middle grades
Dr Rhiannon Lewis (Sessional Clinical Fellow) Dr Jo Boyd
Registrars
Dr Rio Talbot (ST6 - from Dec 2015) Dr Rich Griffiths (ST6 - from Feb 2016)
SHO-tier doctors
• F2 x 3 • ACCS x 1 • GPST x 3 • Junior Clinical Fellow x 1: usually an
anaesthetic trainee preparing for the Clinical Fellow post
• Academic F2 x1
Physio
Anne Harpum
6

7
Practical skills
Most students are keen to develop their practical skills whilst in the ED. Here’s some top tips!
Cannulation & venepuncture • There are endless opportunities to practice your cannulation in the ED! • “Blood trolleys” live in the Majors/Cubicle area, and in Resus. • For most patients, a green venflon is adequate (green is the minimum size for any patient
having a CT with contrast) • Students take maximum two tries at a cannula (only one if patient is unstable) before
asking for help. • Always wear gloves & pay attention to asepsis! • We are (currently) allowed to take blood from the back of venflons, including blood cultures
(though this is technically suboptimal). Have someone show you the kit.
• You will be expected to take bloods, but unfortunately, as a student you can’t use the computerised requesting system to generate the barcoded sticky labels. This can cause a problem with unlabelled blood samples loose in the ED! To get around this, either write name/D number on all bottles by hand (pink cross-match samples are always labelled by hand at the bedside anyway - see box, right) or lay a patient sticky label across all the bottles to keep them identifiable and together until they are formally labelled.
Cross-match samples We do allow students to take cross-match samples, but we also need to put the fear of God into you about getting it wrong. The procedure when taking samples for cross-matching (“XM”) is designed to stop the patient from getting the wrong blood and possibly dying, which in turn helps keep you (and your supervising doctor) out of prison for manslaughter. It really is that important.
So here goes:1. Before you start, check you have the right
patient - look on their wristband if they have one, or ask them to tell you their name/DOB/first line of home address. Never say to the patient “are you Jane Bloggs?” because anyone who is confused, anxious or hard of hearing is going to say “yes” just to please you!
2. Do not trust the sticky labels - they are frequently attached to the wrong Cas Card and it is very common to have several patients called Jones/Roberts/Williams in the ED at once!
3. Once you have taken the blood sample into the pink tube, stop right where you are. Label the bottle by hand, in full, before leaving the bedside.
4. Any pink bottles that are left lying around without their details filled in by hand will be discarded and you will have a very, very cross consultant to contend with. We take this seriously for the sake of both you and the patient!
5. Then do it all over again, from a second venepuncture & second site (unless patient is local & has had G&S in YG before)
Bottle colours
Purple: FBC, ESR Pink: XM
Blue: Coag, INR, D dimer
Yellow: Biochem, TnI, toxicology
Grey: Glucose

8
Practical skills II
Blood gasses • We do fewer Arterial Blood Gasses (ABGs) now than
we used to, but the sicker the patient the more important it is to know their ABG results (instead of venous blood gasses or VBG). The exception is DKA where VBG has basically replaced ABGs.
• ABGs taken at the radial artery are very painful: you should use local anaesthetic (especially for your early attempts!) - although many of our doctors are not in the habit of using lidocaine to take ABGs, so you may need to ask.
• We sometimes take blood from the femoral artery instead: it’s much bigger (so easier to hit!) and less painful. You do have to press hard for a good 5 minutes after, though.
• Always assemble everything you need before starting - including gauze & someone to press on the puncture site.
• Make yourself comfortable, have the wrist supported, take your time. • Always wear gloves: some of the senior docs learned to do ABGs without gloves and now
can’t do them with. Do not copy us! • You’ll need to find someone with a barcode to actually process the ABG sample (the
machine lives opposite rests but needs a barcode or PIN to work it) • Blood gas result sheets are stuck into the notes, usually on back of Cas Card front sheet -
please don’t stick them where they fall over written notes & make photocopying impossible!
ABG or VBG?Have a look at page 4 and 5 of our conference report from the 2014 CEM conference! Click here to see it.
BLS/Chest compressions
• When you hear a patient is coming to the ED in cardiac arrest, ask the Team Leader if you can help with chest compressions.
• Put on gloves and a plastic apron • If you are short, you’ll need to find the
small stool to stand on! • Find out who is your “buddy” (always at
least two people dedicated to doing chest compressions) and agree how you will communicate your changeovers
• The maximum time one person can do chest compressions for is two minutes… but very few people can keep good compressions up that long (it’s hard work!) so expect to change more frequently and do everything you can to minimise interruptions
• Listen to the Team Leader for when to pause, when to resume compressions whilst the defib is charging, and when to get off the chest for shocks to be delivered.
• Do 30:2 if using a BVM, continuous if patient is intubated, and it may be either if the patient has a supraglottic airway in situ (e.g. laryngeal mask airway/LMA or i-Gel) - ask the Team Leader what they want.
Urinary Catheters
• Most male nurses do male urinary catheters, all female nurses do female urinary catheters, all doctors can do male urinary catheters, but very few doctors can do female ones!
• Ask the Nurse In Charge and the nurses allocated to resus to tell you if they are going to do a catheter.
Suturing
• We suture a lot less often than we used to: tissue glue, steristrips and wound staples (especially good for scalps!) are much more common!
• Your best chance of getting suturing practice is either with the Emergency Nurse Practitioners (ENPs) who run the Minor Injuries department, or, an intoxicated patient with a cut head on a late or night shift.
• Practice first! Either go to the Clinical Skills lab, or bring a banana into the ED first thing in the morning (when the Minors area is usually quiet) and ask the ENPs very nicely if they would give you a refresher!

9
How to not feel like a spare part
Get stuck in!
• Introduce yourself to the doctors (and nurses, especially the Nurse In Charge (NIC) every shift
• Make sure that all staff know what year you are - if you happen to be on attachment with someone two years further ahead in their training, supervising docs/nurses need to know this!
• If you’re an elective or senior SSC student, get stuck in seeing your own patients as soon as you have found your feet. You are welcome to see “fresh” patients, but the hospital rule is the patient must not be delayed to see a qualified doctor by you, so don’t take the top card on the pile… take one further down! See next page.
• Leave a marker card in the pile to make clear that the next patient to be seen is being seen by a student and the next doctor free should join you
• At peak periods of ED activity, it gets very busy, and it is difficult for the doctors to spend an additional 10-15 minutes for case teaching you. At these times, please stop seeing “your own” patients and switch to being the most helpful person you can be - usually, helping with bloods and venflons, and blood gases, and charting. Luckily, these are things most students need practice at!
• Take a good look at the Major Trauma Pack (it’s in the resus drawers, plus additional sheets on the lectures outside the relatives room) and have a go at scribing.
Find your way around resus
• If the sh**t hits the fan and resus kicks off, get in there to watch and learn.
• It’s OK to stand slightly out of the way if you’re not (yet!) sure what to do to help - if you stand at the top end of the trolley (by the patient’s left side) you are unlikely to get in the way, or else stand by the team leader. If someone does ask you to stand somewhere different, don’t get upset, it’s not that you aren’t welcome to watch! Just move somewhere else!
• If it’s a cardiac arrest, either watch and learn or get in there and help with chest compressions (make yourself known to the team leader)
• Help the nursing staff re-stock resus (usually in the morning) - that way, you’ll know where to find everything and if, in tense resuscitation situation, you can fetch what’s needed to do something (e.g. fluids, a blood gas syringe & the street and gauze) then you will free up vital nursing minutes, take the heat out of the situation and hopefully free up enough time for someone to teach you a little.
• Usually, however, the time to ask questions if someone is really, really sick is after things have calmed down. The team leader may look calm but they need all the cerebral “bandwidth” they can muster in order to direct the clinical care. Don’t distract them: wait until they are no longer making decisions in quick succession before asking questions.
• Make notes as you go along about things to ask afterwards.
To a certain extent, it’s unavoidable that students new to a unit will feel a little lost for the first few days… we try hard to minimise this, but by the time most medical students come to our ED on placement you’ve probably gotten a little used to it. Don’t worry, you’ll quickly settle in!
For those of you who are only with us for a couple of shifts (i.e. Cardiff JSAs) most of your time will be with one of our MedEd Fellows, so you won’t have chance to feel like a spare part - but it’s also your job to be an active learner. Don’t just stand there, do something…
For those on longer attachments, here’s our top tips for getting stuck in and feeling part of the team in the shortest possible time!

10
Seeing your own patients
How to find your patient
The “to-be-seen” pile of Cas Cards is on the racks close to the whiteboard. They are arranged in order of both both arrival & clinical priority (we use the Manchester Triage System to prioritise - send a few hours with the triage nurse to get a grasp of it) and doctors are expected to take the card on top of the pile.
As a student, however, you won’t take the top card: patients mustn’t wait longer to see a doctor as a result of seeing a student, so you have to take a card from further down the pile. You then use a “Student Seeing Patient” laminated card to mark the place in the pile you have taken the card from. In the event that this rises to the top before you have finished assessing the patient, the doctor should come and join you. If not, find a doctor to present the case to.
Writing on the Cas Card
There is a specific box for medical students to write their name (BLOCK CAPITALS unless your handwriting is wonderful) and time that you go to see the patient. Use it (24-hour clock please)!
We do appreciate that some students are reluctant to commit their physical examination findings to paper until they have been checked by the supervising doctor. That’s fine, but you can at least repeat & document the obs & whether the patient looks ill or well!
The responsibility of the supervising doctor
It is essential that it is 100% clear on the Cas Card which doctor has taken clinical responsibility for the patient: their name (and
time they see the patient) must be entered in the “Dr/ENP” box too. They must also write in & sign the Cas Card (and their name goes on the white board)
Occasionally, this will be just “Hx/Ex/Plan as above” but more usually the supervising doctor will write some brief additional notes.
What to do if you find a patient in significant pain (or who has deteriorated since triage)
Inform the Nurse In Charge (or a doctor) immediately. If you think the patient needs to be moved to resus, say so. If there are then no immediately available ED staff, then take a fresh set of obs yourself (practice with our Dynamaps!) and - if the patient requires analgesia urgently - enough history about the problem/allergies/PMHx/analgesia already given to help one of the doctors prescribe suitable analgesia as quickly as possible.
Beware handover times All patients in the ED must have a named doctor looking after them once they’ve been seen. This means “your” patients will need to be handed over when the doctor supervising the case goes off duty. Do not be left holding a patient without a supervising doctor: alert the doctor or nurse in charge if this happens, or better still, remind your supervising doctor to ensure the patient is handed over to another doctor!
We know that for many medical students, “seeing patients first” (and presenting the case to one of the on-duty ED doctors) is a highlight of ED placements, and this is a mainstay for how we host senior students on longer placements in the ED (e.g. SSCs and electives). It is a fantastic way to develop your skills & confidence in formulating a differential diagnosis and deciding upon a plan for management and (where required) investigations.
For more junior students (and/or those on very short placements) we take a totally different approach to make the best of the rich clinical environment of the ED. Such students generally won’t see patients on their own, unless we have a MedEd Fellow on duty (dark grey scrub top) doing a teaching shift, or, if the ED is exceptionally quiet. This means we avoid the frustrations caused by ED doctors dodging junior students who trying to present cases because - perfectly understandably - the doc then will have to repeat most of the evaluation we well as taking time to discuss the case.
The white board
Do not write your name on the white board in the slot for “doctor seeing” (and do not let the nurses do so either). It should remain as “TBS” (to be seen) until a doctor (or ANP) has seen the patient.

11
FAQs - I
Where do I come on the first day? (electives/SSC students only)
• Unless instructed otherwise by the North Wales Clinical School team, go to the NWCS Office at 0900 on your first day with your ID, student ID etc.
• Once the paperwork is done, one of the NWCS team will bring you downstairs to the ED.
• If Dr Linda Dykes (your named supervisor) is around, she’ll try to meet with you, but this is not essential and can be done any time in the first week or two.
• Report to the Nurse In Charge, the Senior Doctor “Shop Floor Supervisor” and ask them to introduce you to the duty Clinical Fellow - these are register level doctors who will be your main point of contact in the ED.
Where do I leave my stuff?
• Please use the lockers upstairs in the Medical Student Common Room
• Do not bring valuables to the ED as we cannot guarantee their safety
Does it matter that I don’t speak Welsh?
• Not at all (very few of our doctors can speak Welsh), but don’t be surprised to find that many of the nursing staff speak to patients in Welsh.
• However, clinical conversations must be in English unless everyone involved in them speaks Welsh… and that includes you: you are a member of the clinical team.
• Pre-school children from Welsh-speaking families, and confused elderly patients may well give a history better in Welsh than English - just ask a Welsh speaking member of staff (or, if a child, the parent/carer) to translate.
• Learning even a few words of Welsh isn’t difficult and is much appreciated by patients and Welsh-speaking staff - see the box below!
Where can I get food?
• You are welcome to bring a packed lunch & use the fridges & microwaves in the staff coffee room in ED. There is no toaster.
• The canteen is open 12-2 and 5-7pm and also for breakfast
• If you miss that, the WRVS cafe near the hospital lifts is open in daytime, or there is a shop just across the road.
Is there any teaching I can attend?
• Every Thursday afternoon is our junior doctors’ teaching. This is often in the Postgrad Education Centre upstairs, but sometimes in Beuno Seminar Room (last on the right in Beuno ward)
• Every Friday lunchtime (1-2pm) in term-time is Grand Round - free lunch at 1230, go up to the education centre.
• Some weeks, Mr Mel Jones (consultant orthopaedic surgeon) runs a Trauma Meeting. This is a business meeting going through x-rays and orthopaedic admissions from the previous 24 hours. if you’d like to attend, call his secretary via switchboard to ask when and where.
• Also ask in the PG Education Centre about attending Foundation Programme teaching if you wish.
• The ED Monthly Meeting takes place in the second half of the month - watch out for flyers or ask Leesa Parkinson.
• If there’s sometime that particularly interests you - ask us. For example, we have a very friendly hand surgeon who may have space to host you in his hand fracture clinic.
How do I recognise the MedEd fellows?
• On days that our MedEd Fellows are 100% teaching (without any shop floor responsibilities of their own) they will wear dark-grey (pewter) scrub tops.
• Obviously, the same doctors also do normal clinical shifts! This doesn’t make them any less enthusiastic about teaching, but it does mean that they have to balance their own workload against finding time to teach: you will get shorter on-the-spot tutorials on these days!
I want to see X/YZ/Z & haven't yet…
• Talk to us: we can suggest when are the most likely times to see some problems and adjust your shifts to help you see what you want.
There are lots of websites where you can learn a few words of Welsh before you arrive - some have audio clips!
https://en.wikibooks.org/wiki/Welsh/Useful_Phraseshttp://gwybodiadur.tripod.com/phrases.htmhttp://www.heart-of-wales.co.uk/welsh.htm

12
FAQs - II
How do I gain consent from patients? • If you are seeing patient from the outset,
you must ask permission to do a “preliminary evaluation whilst you are waiting to see an ED doctor”.
• If you are seeing a patient (e.g. to look at signs) already seen by a member of the ED team, they should have asked the patient for permission to bring students to see them… but always check.
What if I have any Child Protection or Protection of Vulnerable Adult (POVA) concerns?
• Speak to the supervising doctor and/or Senior Doctor and/or NIC immediately.
Can I make referrals?
• Learning to make clear, succinct referrals is an important part of your attachment.
• Always discuss the patient with your supervising senior before making a specialty referral on their behalf.
• Practice with specialty teams who are already in the ED before trying by phone!
• Explain “I would like to refer an ED patient on behalf of Dr X, the ED Clinical fellow, who is right here next to me supervising my handover to you”.
• Listen to some referrals and copy the style of someone who does them succinctly and effectively.
• Or practice using a handover tool such as the SBAR.
How do I use the bleep system?
• Dial 81> bleep no you want>tel no you’re at
• There are lists of all specialty on-call bleeps strategically placed closed to phones!
How do I call switchboard?
• 100
How do I make a Cardiac Arrest call (also for trauma/paediatric emergency/massive haemorrhage - you need to state WHICH and WHERE)
• 222
What do I need to know about the 4-hour target?
• 95% of patients should be seen and either discharged or admitted within 4 hours of arriving at ED.
• In order to do this, any necessary investigations need to be done as early as possible, because blood results often take 90-120 minutes to become available.
• Therefore if you are seeing “your own patients”, discuss blood tests required with your supervising doctor as soon as you know (or suspect) they are needed.
How can I make best use of my supervising doctors?
• Different students have different preferences/learning styles and different doctors have different teaching styles… you’ll probably find some you prefer to learn from than others. That’s ok!
• Please be aware of your supervising doctor’s stress levels: carrying their own workload plus several patients of yours may be too much - use another doctor if necessary!
• All ED doctors of all levels of seniority have portfolios and appraisal folders to maintain and greatly appreciate written feedback on their supervision and teaching. If it’s positive, that’s fantastic, if you have identified a room for improvement, please be specific and constructive!
• In general, the doctor who is the Shop Floor Supervisor (or “head chef”) will not be able to fully supervise cases for you, so this will require another member of the team (quick questions are entirely appropriate). This refers to the designated SFS senior doctor (daytime/early evening) and the middle grade overnight.
• Don’t try to present patients to the QAAC doctor (but you can join the QAAC team and help)
WiFi
There’s free wifi in the whole hospital, and also in the residences.
Cardiff students can also access Cardiff Uni computers in the library.

13
Final thoughts
Your patients are having a bad day • Nobody plans to get ill or injured and need
to come to the ED - almost without exception, the patients & families you meet are, at best, having a badly disrupted day.
• For some, it may be the worst - or last - day of their lives
• A little kindness goes a long way… smile, always introduce yourself, offer to fetch a tea or coffee for relatives, look out for patients who need assistance with food/drink (or need to be offered some if their clinical condition permits and they are stuck in ED).
Sometimes, people die…
• Sadly, death is an almost-everyday occurrence in the ED.
• For many students, their ED attachment is their first experience of seeing someone passing from life to death. If that applies to you, it’s perfectly normal to find it a bit profound/odd/bizarre/upsetting. Talk to us.
• Not all lives can be saved… CPR isn’t always appropriate. Too many people whose lives are drawing to a natural close are inappropriately subjected to the indignity of CPR, which only stands a chance of working if the heart is the first thing to stop working (not the last)
PLEASE - answer the phone!From the profound to the mundane… ringing phones drive us all insane. Team members who ignore ringing phones drive us even more insane!
Just pick it up, say “Good morning, Emergency Department, Medical Student speaking, how can I help” - put on hold if necessary - and find someone to take the call. Simples!
Getting the best learning experience you can from your ED placement • The ED is a most fantastic environment for
learning: every patient is a goldmine. • Most students find that keeping a notebook
and writing down a few words about each case/presentation/condition enables them to spend a few minutes “reading round” the subjects each evening.
• If you think you’ve made a mistake, or are worried about something, just tell us - it’s our job to support you and sort it out :-)
What to wear
• Elective & SSC students, plus Hospital Front Door students, will get a loan scrub top. Wear with tidy trousers (Chinos or walking trousers, no jeans please) and closed-toe shoes (clean trainers OK, Crocs not ok). Please return the scrub top washed & ironed to the NWCS office (i.e. Kim & Myfanwy) at the end of your attachment.
• JSA students: you will wear your own clothes like any other clinical attachment. No jeans.
• Ladies: beware low-cut tops and short skirts - they aren’t practical in the ED setting and not a great idea if dealing with intoxicated and disinhibited patients!
Have we forgotten anything?
This is the first edition of our Medical Student handbook. Please email [email protected] if you can think of something we should add!
Follow us on Twitter! @YGEDBangor
Emergency DepartmentYsbyty GwyneddBangor, Gwynedd, LL57 2PW 01248 384001 (ED reception)01248 384005 (ED Staff “Hub”)01248 384003 (Consultants’ Secretary, Lou Lee)

14
Enjoying your stay in Bangor
Outdoor pursuits
If you are an active person, you’ll love your spell living in North Wales! For mountain bunnies, Snowdonia is only 15 minutes’ drive away, and if you like sailing or surfing or kitesurfing, it’s 15-20 minutes in the other direction. There are climbing walls both at the Beacon Climbing Centre in Caernarfon, or (much nearer) at Indy in Llanfair PG.
Not all students have cars, but there’s always doctors going off doing stuff, and other students who do have cars.
Fitness
There’s both a University Gym (Conolfan Brailsford) and DW Sports, both of whom usually accept short-term student members and are within 2-3km of the hospital.
Culture
The nearest Multiplex cinema is the Cineworld at Llandudno, about 20 minutes drive away. However, movies (and mass screening events such as RSC & NT Live) are also shown at the Galeri in Doc Victoria in Caernarfon and the Ucheldre Centre in Holyhead. The brand-new Pontio Centre at Bangor University is due to open in Autumn 2015 which will bring a new arts venue to Bangor. The main live theatre in the area is Venue Cymru in Llandudno which has a wide range of shows.
For other ideas, check out the Leisure Activities page on the unofficial ED website!
Ysbyty Gwynedd student facilities
• The residences are nice and warm (“plenty of hot water”), and there’s a basic kitchen.
• However, sound proofing isn’t great (“bring earplugs”) and the laundry facilities have been noted as expensive (£3 to wash and £3 to dry).
• There is free wifi all over the YG site (in residences and in the hospital itself) but beware poor phone reception on many networks.
• Library access is 24/7 (this is also where Cardiff University have terminals).
The North Wales Clinical School (West) are in the process of producing a guide to being a student in Bangor, so these are just a few interim pointers for you!
Getting here & getting around
• If you have a car, you’ll use the A55 to get here (from Cardiff, most people use A470)
• There are plenty of trains to and from Bangor, and if you look out about 6 weeks before you’ll find the bargain advance purchase fares. You can pop to London in as little as 3 hours 14 minutes.
• The hospital has a good bus service via Arriva Wales and the TravelineCymru online journey planner is rated as helpful.
Supermarkets
There’s a Tesco Extra (24/7) 1.8km walk from the hospital down a steep woodland path, but don’t try that after rain! Waitrose (wonderful but costly) is just across the landmark Menai Bridge, slightly further but the roads are weather-proof! Down in Bangor there is a Lidl, Morrisons, Asda and M&S Food.
ED Social events
You’ll find there are ED social events both planned an unplanned - they’re not frequent (every few months) but if there’s one on when you’re with us, you’d be very welcome!
On a Tuesday evening, many of the YG doctors attend the Pub Quiz at the Gardffon Inn in Felinheli - please do feel free to go and either back them up or take a rival team & beat them!
Coming from abroad?The nearest major airport is Manchester, but you can fly into London Heathrow or Gatwick and travel to Bangor from London’s Euston Station. See www.thetrainline.com for tickets. If you’re coming from an Australian summer straight into the UK winter, bring lots of warm clothes and a decent waterproof jacket - it can be pretty damp here in winter, and although our coastal location means heavy snow is unusual, if you’re used to daytime temperatures of 25C+ it’s going to feel cold here!
Don’t forget DublinYou can pop across to Dublin from Holyhead for a day-trip or overnight stay. Both Stena Line & Irish Ferries can take you there & back!
Many thanks to Ruby Kwong, Elective Student Winter 2014/15, University of Sydney.
15
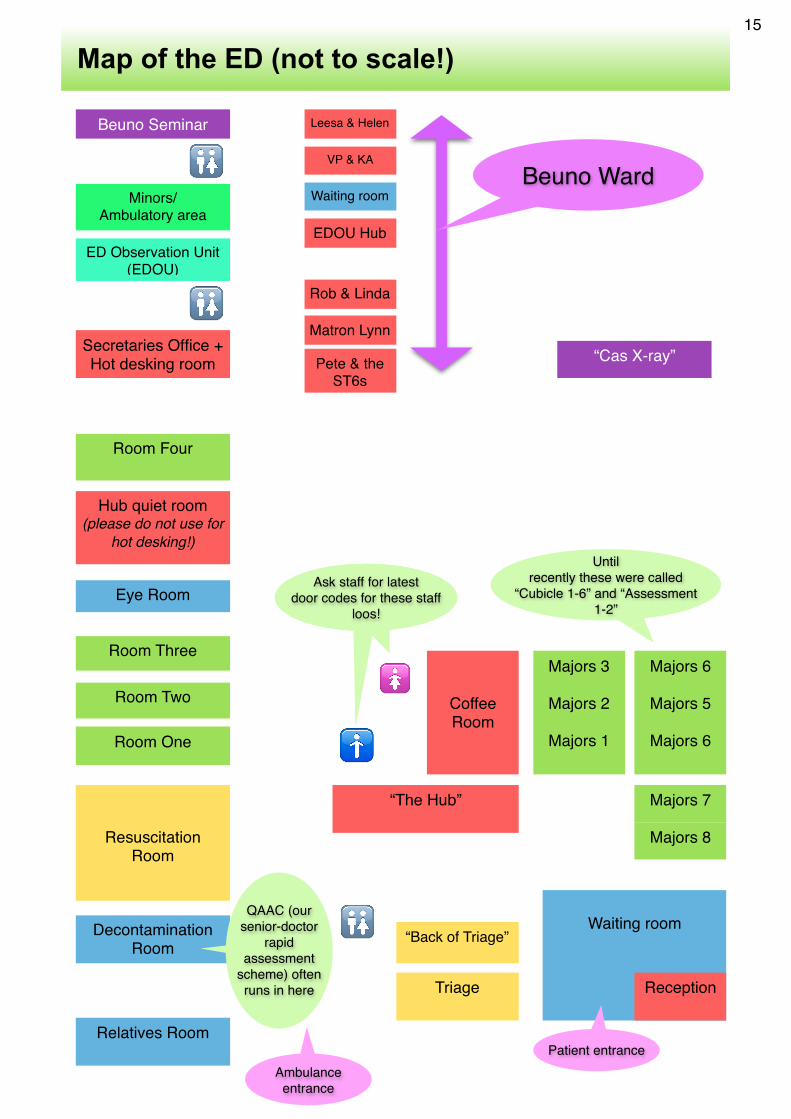
Map of the ED (not to scale!)
Waiting room
ReceptionTriage
Relatives Room
Decontamination Room
ResuscitationRoom
“The Hub”
Room One
Room Two
Room Three
Eye Room
Room Four
🚹
🚺Coffee Room
Hub quiet room (please do not use for
hot desking!)
🚻
Majors 8
Majors 7
Majors 3
Majors 2
Majors 1
Majors 6
Majors 5
Majors 6
Until recently these were called
“Cubicle 1-6” and “Assessment 1-2”
“Cas X-ray”Pete & the ST6s
Matron Lynn
Rob & Linda
EDOU Hub
Leesa & Helen
VP & KA
Waiting room
Beuno Seminar
Minors/Ambulatory area
ED Observation Unit (EDOU)
Beuno Ward
Patient entranceAmbulance entrance
🚻
🚻
Ask staff for latest door codes for these staff
loos!
“Back of Triage”
QAAC (our senior-doctor
rapid assessment
scheme) often runs in here
Secretaries Office + Hot desking room

Appendix 1 - Example SSC learning contract & timetable This example is from a last-block-of-final year SSC in 2012
LEARNING CONTRACT: Emergency Medicine SCP
This%is%an%educational%agreement%between:%
%
%
…………………………………………%……………………………..%%(Learner)%&%Dr%Linda%Dykes/Dr%Rob%Perry%
(SCP%Supervisor)%
%%
It%is%agreed%that%the%above%named%will%undertake%the%SCP%activities%outlined%below:%
%
1.####The#aims#of#the#project#are:#%
1. %To%gain%experience%of%Emergency%Medicine%in%a%busy%rural%ED%
2. Opportunity%to%practice%practical%skills%and%procedures%
3. To%produce%a%written%project%on%a%topic%relevant%to%Emergency%or%PreOHospital%EM.%%
%
2.####The#detailed#objectives#are:%
%
• The%student%will%revise%and%use%of%Microsoft%Excel%(and%possibly%SPSS)%
• The%student%will,%if%applicable%to%their%project,%be%able%to%describe%processes%surrounded%
handing%of%medical%records%
• The%student%will%gain%exposure%to%Emergency%Medicine%skills,%procedures%and%be%able%to%
describe%the%role%of%the%ED%in%the%modern%NHS.%%
• The%student%will%gain%an%appreciation%of%the%challenges%posed%by%rural%ED%when%tertiary%
facilities%are%100%miles%away%
• The%student%will%be%exposed%to%the%assessment%and%initial%management%of%a%wide%range%of%
unselected%patients%presenting%to%the%ED%
• The%student%will%gain,%practice%and%refine%practical%skills%such%as%cannulation,%
catheterisation,%blood%gasses,%CPR%
• The%student%will%be%able%to%describe%the%role%of%different%emergency%services%
• The%student%will%gain%handsOon%experience%of%the%process%of%abstract%preparation%&%
publication/presentation%of%findings%(if%the%student%wishes%and%assuming%a%suitable%
project%is%chosen)%
%
How do you say Ysbyty Gwynedd?You have two options. 1. Call it “YG” - or just “Bangor Hospital”.2. Take the plunge and learn how to say it. Try saying “Us-butty Gwyn-eth”!

%
3.####In#order#to#achieve#the#above#aims#and#objectives,#the#learners#will#undertake#the#following%
1)%ED%shop%floor%work:%minimum%of%21%shifts%(including%evenings/weekend%shifts)%over%the%8O
week%SCP%(see%appendix)%
%
2)%Choose%a%topic%after%discussion%with%Project%Supervisor%%
%3)%Update%your%supervisor(s)%at%least%weekly,%preferably%by%meeting%but%emailed%updates%may%be%
required%if%a%meeting%is%missed%due%to%tutor/student%sickness%or%tutor%being%on%leave.%(see%
Appendix)%%
%
4)%Maintain%a%personal%logbook%of%shifts%worked%and%cases%seen%in%the%ED,%plus%your%key%learning%
experiences%and%reflections%for%each%shift/session.%
%5)%Attend%the%ED%Junior%Doctors%teaching%on%Thursday%afternoon%(unless%excused%for%projectO
related%activities)%
%
4.####The#following#resources,#people#and#organisations#will#be#involved:%
Dr%Linda%Dykes%and/or%Dr%Rob%Perry%–%Consultants%in%Emergency%Medicine%and%your%SCP%
Supervisor%
At%least%one%of%the%Clinical%Fellows%
All%ED%doctors%and%ENPs%
North%Wales%Clinical%School%–%Kim%&%Myfanwy%
%
5.####The#endBproduct#of#the#project#will#be:%
1)%Submitted%SCP%project%
2)%Your%selfOmaintained%logbook%of%your%ED%experience%&%reflections%on%cases%&%learning%points%%
%
6.####It#is#agreed#the#project#will#be#evaluated#in#the#following#manner:%
1)%SCP%project%will%be%marked%as%per%Cardiff%University%procedures%2)%A%meeting%may%be%held%in%the%final%week%for%you%and%your%fellow%students%to%deObrief%your%
experiences%from%your%ED%attachment%(Clinical%and%Non%Clinical)%and%assist%the%ED%staff%with%
planning%next%years%SCP%programme.%%
%
%%
Date:%
%

%
APPENDIX Attendance#%%One%of%the%key%benefits%of%your%placement%at%Ysbyty%Gwynedd%is%the%opportunity%to%gain%experience%on%the%Emergency%Department%“shopOfloor”.%We%recognise%you%have%a%substantial%amount%of%activity%to%include%within%the%duration%of%the%placement,%especially%if%your%project%involves%a%significant%amount%of%data%collection,%and%as%a%final%year%SCP,%we%endorse%an%adult%approach%to%organising%your%own%learning%time.%Nevertheless%one%of%the%reasons%this%SCP%has%been%approved%by%Cardiff%University%is%for%the%educational%experience%gained%from%assessing%and%managing%ED%patients.%It%is%also%excellent%revision%–%just%spend%a%few%minutes%looking%up%every%condition%you%see!%%%You%are%expected%to%attend%at%least%21%ED%shifts.%A%shift%normally%lasts%for%eight%hours.%You%will%work%“flexiOtime”,%but%should%aim%for%a%variety%of%shift%times%in%order%to%maximise%the%breadth%of%your%experience.%You%should%definitely%include%at%least%four%late%shifts%(1800O0200)%and%at%least%two%shifts%on%either%a%Friday,%Saturday%or%Sunday%afternoon/evening%(1400O2200,%1600O0000%or%1800O0200),%as%well%as%ordinary%weekday%shifts.%We%highly%recommend%that%you%work%one%or%two%night%shifts%(2200O0800)%which%would%count%as%1.5%shifts%worked:%shadowing%and%assisting%one%of%the%SHOOtier%doctors.%However%please%ensure%that%you%meet%the%rest%requirements%of%the%EWTD:%a%minimum%of%11%hours%off%between%shifts.%%%%Notes:%1%–%With%good%reason,%two%halfOshifts%may%be%acceptable%in%place%of%one%full%shift,%with%the%agreement%of%your%mentor%or%supervisor.%2%–%ProjectOrelated%activities%such%as%collection%of%data%do(not%constitute%an%ED%shift,%unless%your%supervisor%has%specifically%agreed%that%the%two%can%be%combined.%3%–%The%above%are%not%utterly%prescriptive,%if%for%example%you%undertake%an%unusually%involved%project%or,%of%course,%if%you%unfortunately%experience%personal%difficulties%such%as%a%bereavement.%However,%deviation%from%the%above%should%be%discussed%with%and%agreed%by%your%supervisor%as%early%as%possible.%%Supervision#%Your%supervising%Consultant%is%either%Dr%Linda%Dykes%or%Dr%Rob%Perry%and%you%may%also%be%"coOsupervised"%by%an%experienced%middleOgrade%doctor%(Specialty%Registrar%or%Clinical%Fellow).%You%should%aim%to%undertake%at%least%some%of%your%ED%shifts%with%your%supervisor(s)%as%this%is%a%good%opportunity%to%ensure%s/he%is%aware%of%your%clinical%progress.%%You%must%keep%your%supervisor(s)%up%to%date%on%the%progress%of%your%project.%Most%weeks,%this%will%be%via%a%meetings:%if%you%are%being%supervised%by%Linda,%book%into%her%Thursday%afternoon%“clinic”%(ring%Eleri%the%ED%secretary%on%ext%4003,%or%first%door%on%right%going%onto%Beuno%ward)…%if%this%is%full/unavailable%in%the%required%week%(or%your%supervisor%is%Rob)%phone%or%email%to%arrange%a%meeting%time.%Alternatively,%and%only%if%you%are%certain%you%do%not%require%advice%or%guidance%from%your%supervisor%that%week,%you%may%send%a%formal%update%email.%See%box.%(%As%a%minimum,%you%should%aim%to%meet%with%your%Supervisor%during%week%2,%in%the%second%half%of%Week%3%and%during%the%second%half%of%Week%6.%This%will%include%a%detailed%review%of%your%project%to%date,%which%you%must%bring%with%you%to%the%meeting.%

%On%the%Thursday%afternoon%of%Week%4%or%5,%we%will%try%to%organise%a%meeting%for%all%Final%Year%SCP%students%with%their%supervisors%in%the%Clinical%School%or%Education%Centre.%Each%student%will%be%allocated%a%"slot"%of%twenty%minutes.%During%this%time%you%will%be%required%to%give%a%presentation,%lasting%around%ten%minutes,%in%which%you%outline%your%project%and%detail%your%progress%and%plan.%There%is%then%an%opportunity%for%your%colleagues%and%supervisors%to%discuss%the%project%with%you,%which%may%offer%solutions%to%difficulties%that%you've%encountered,%bring%out%entirely%new%ideas%and/or%help%to%identify%possible%problems%while%there%is%still%sufficient%time%to%act%upon%them.#%Progress Report Emails (same headings will be used for meetings) %1.#Project#O%A%summary%of%the%progress%on%your%project%so%far.%O%An%outline%of%how%you%intend%to%proceed%with%your%project%over%the%remaining%weeks%of%the%placement.%O%A%more%detailed%outline%of%how%you%intend%to%proceed%with%your%project%over%the%next%7%days.%%2.#Emergency#Department#Activity#O%A%clear%record%of%the%Emergency%Department%shifts%that%you%have%undertaken%in%the%preceding%week.%O%This%should%include%a%brief%summary%of%your%activity%during%each%of%those%shifts.%%3.#Other#Activities#O%A%summary%of%anything%else%that%you've%undertaken%within%the%previous%week.%%Example+Email+(end+of+Week+2)+(1.+Project+I(have(made(a(good(start(on(the(data(collection,(and(have(now(been(through(45(of(the(100(case(notes(that(I(need(to(review.(I(intend(to(complete(data(collection(by(the(end(of(Week(3,(which(will(give(me(a(week(to(undertake(my(data(analysis(and(then(four(weeks(to(write(up(the(project.(I(have(completed(my(literature(review(and(attach(it.(I(am(still(waiting(to(hear(back(from(the(RAF(about(the(audit(standards,(but(do(not(require(this(information(until(Week(4(anyway.(My(plan(for(next(week(is(to(complete(my(data(collection,(which(will(take(two(full(days.(As(we(agreed,(I(will(do(four(days(of(half(Emergency(Department(and(half(data(collection,(in(order(to(break(it(up(a(bit!((2.+Emergency+Department+Shifts+I(have(only(done(two(Emergency(Department(shifts(this(week,(but(I(will(be(doing(a(late(shift(tonight((Friday)(and(another(one(tomorrow.(Monday(0800P1600(P(spent(the(first(half(of(the(shift(with(the(triage(nurse(and(also(doing(some("See(and(Treat"(with(Dr(Smith.(Second(half(of(the(shift(in(resus,(almost(all(with(one(very(sick(patient.(Saw(the(placement(of(a(central((IJ)(line(with(Dr(Jones.(Tuesday(1400P2200(P(had(a(full(shift(with(Dr(Smith(in(minors.(Shadowed(for(the(first(half(of(the(shift,(then(started(seeing(patients(first(and(presenting(to(Dr(Smith.((3.+Other+Activities+P(Attended(the(Medical(Student(teaching(on(Tuesday(afternoon,(which(was(on(cardiovascular(examination.(P(Attended(F1(teaching(on(Thursday(afternoon,(which(was(on(consent(and(capacity.(P(Dr(Jones(invited(me(to(attend(the(registrar(teaching(on(Wednesday(so(I(could(have(a(go(at(placing(a(central(line(on(a(model.(This(was(really(useful(after(I'd(been(able(to(watch(the(procedure(for(real(on(Monday.%

IMPORTANT#%Your%Supervisors%(and,%if%applicable,%your%middleOgrade%mentors)%are%here%to%help%and%support%you.%Linda%is%quite%happy%to%be%texted%(10amO10pm),%facebook’d%or%emailed%at%home;%Rob%has%very%poor%mobile%reception%at%home%but%is%similarly%accessible.%Please,%please%don’t%sit%and%struggle%or%worry%about%anything%project%or%placement%related:%talk%to%us%and%help%us%make%this%the%best%placement%of%your%medical%school%career!%%%%Weekly#targets##
#Week## Suggested#shop#
floor#shifts#Project#activity## Comments##
1# 4% Look%at%previous%projects/posters;%chat%to%Supervisors%and%middleOgrade%mentor%(if%applicable).%Provisionally%choose%a%topic%and%start%reading%around%it%&%literature%searching.%%
Week%one%is%to%get%you%settled%into%the%ED%and%confident%working%on%the%shop%floor.%Book%literature%searching%tutorial%with%hospital%Librarian%if%you%are%not%confident%with%this%
2# 4%–%including%some%late%shifts%
Project%topic%must%be%chosen%by%end%of%Week%2%at%the%very%latest:%data%collection%may%be%underway%if%project%topic%chosen%by%end%of%week%1.%
Compulsory#meeting#with#your#supervisor#this#week#(replace#by#email#only#if#meeting#is#logistically#impossible)#%
3# 3% Data%collection%should%be%underway%(or,%if%waiting%for%notes,%prepare%your%background%&%literature%search%&%literature%review)%
Compulsory#meeting#with#your#supervisor#this#week#(replace#by#email#only#if#meeting#is#logistically#impossible)#%
4# 1%% Major%project%Work%week%Update(Afternoon(either(this(Thursday(or(next(Thursday((
ED%hosting%Acute%care%Module%Students%–%we’d%suggest%working%a%night%shift%this%week%%
5# 1% Major%project%Work%week%Update(Afternoon(if(it(wasn’t(last(Thursday%
ED%hosting%Acute%care%Module%Students%–%we’d%suggest%working%a%night%shift%this%week%%%
6# 3% Data%collection%should%be%almost%complete%by%end%of%this%week.%Your%Introduction,%Background%and%Literature%Review%section%draft%should%be%ready%for%your%supervisor%to%read.%%
Compulsory#meeting#with#your#supervisor#this#week#(replace#by#email#only#if#meeting#is#logistically#impossible)#%
7# 2% Absolute%deadline%for%data%collection%to%be%completed%by.%%Results,%Discussion%&%Conclusion%should%be%taking%shape%%
%
8# 2% Complete%writing%up:%finishing%early%is%ideal,%leaving%maximum%shop%floor/revision%time.%%
We%will%try%to%arrange%a%deObrief%meeting%in%the%final%week%for%all%SCP%students,%supervisors%and%middleOgrade%mentors%to%share%their%experiences.%%
#%


![1-S3=Y$2=S YG]H $GY,S%YG]H $GY3HSG Q]$ …](https://static.fdocuments.in/doc/165x107/620680590c66c662951a4918/1-s3y2s-ygh-gysygh-gy3hsg-q-.jpg)