Workshop 1: Lanziano Moderatori: E. Sagnelli, F. Suter Discussant: F.v. Schloesser La complessità...
14
Workshop 1: “L’anziano” Moderatori: E. Sagnelli, F. Suter Discussant: F.v. Schloesser La complessità della gestione terapeutica dell’anziano a lungo termine A. Castagna
-
Upload
nora-brunelli -
Category
Documents
-
view
218 -
download
0
Transcript of Workshop 1: Lanziano Moderatori: E. Sagnelli, F. Suter Discussant: F.v. Schloesser La complessità...

Workshop 1: “L’anziano”Moderatori: E. Sagnelli, F. SuterDiscussant: F.v. Schloesser
La complessità della gestione terapeuticadell’anziano a lungo termineA. Castagna

COHERE, Lancet 2010


1045 pts 12096 visits


2854 HIV + vs 8562 HIV-


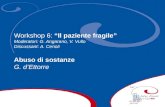
Prevalence of HIV associated type 2 diabetes in comparison with the italian population
<=50 >50 <=50 >500
3
6
9
12
15
HIV+ HIV-
FEMALES MALESage (years)
% o
f pa
tient
s w
ith ty
pe 2
dia
bete
s<=50 >50
0
3
6
9
12
HIV+ HIV-
age (years)
% o
f pa
tien
ts w
ith ty
pe
2 d
iab
etes
P=0.0006
P<0.0001 P<0.0001
P=0.153 P=0.002
P<0.0001
5509 1431
5877 3185
HIV+
HIV-
<=50 >50Number of pts
L. Galli, in preparation


Effects of Medical Therapies on Retinopathy Progression in Type 2 Diabetes
The ACCORD Study Group and ACCORD Eye Study Group
• In a randomized trial, we enrolled 10,251 participants with type 2 diabetes who were at high risk for cardiovascular disease to receive either intensive or standard treatment for glycemia (target glycated hemoglobin level, <6.0% or 7.0 to 7.9%, respectively) and also for dyslipidemia (160 mg daily of fenofibrate plus simvastatin or placebo plus simvastatin) or for systolic blood-pressure control (target, <120 or <140 mm Hg). A subgroup of 2856 participants was evaluated for the effects of these interventions at 4 years on the progression of diabetic retinopathy
• Intensive glycemic control and intensive combination treatment of dyslipidemia, but not intensive blood-pressure control, reduced the rate of progression of diabetic retinopathy
NEJM 2010

Clinical inertia
Recognising the problem but failure to act
Clinical inertia, defined as a failure to initiate or advance therapy in a patient who is not at the evidence-based goal, is a key contributing factor in the suboptimal rates of therapeutic target achievement for type 2 diabetes.
The causes of clinical inertia are multifactorial and interactive, arising among patients, providers, and health systems and from specific characteristics of available treatments.
Therapeutic non adherence is perhaps the most significant factor contributing to clinical inertia, with recent analyses demonstrating that providers are more likely to prescribe a dose escalation in patients who are adherent to therapy compared with those who are not.

Only high adherers reported a significantly decreased risk of acute cardiovascular events (HR 0.62)
Mazzaglia G, Circulation 2010


Encouraging patient-centered careContinuity of care
• Important to the integrity of the patient-provider relationship
•Being understood
•Being remembered