Anıl Sural - Globalization and Income Inequality and European Perspective
Journal of Neurology, Neurosurgery, and Psychiatry 1990;53:266-270
LETTERS TOTHE EDITOR
Persistent segmental cerebral arteryconstrictions in coital cephalgia
Onset of severe headache during sexual inter-course can result from subarachnoidhaemorrhage, but more commonly it has abenign aetiology."' In the majority of cases,such coital cephalgia has a vascular character,although it may also relate to muscular con-traction or, rarely, to low pressure in thecerebrospinal fluid.' There are similaritieswith the headache of phaeochromocytoma,4and a hyperdynamic circulation has beenimplicated in some instances.' In addition,coital cephalgia has been regarded as amigraine variant because of its character, itsresponse to beta blockade, the frequent pastor family history of migraine in affectedindividuals, and the rare development ofresidual neurological deficits."6 There haverecently been several reports of angiographicabnormalities in migraine consisting of mul-tiple segmental narrowings of cerebralarteries.7-'0 However, cerebral angiography incoital cephalgia has previously been reportedto be normal,2 to the extent that its use hasbeen reserved for those patients in whom amore sinister pathology is suspected.However, we now report a case of coitalcephalgia with radiological findings whichresembled those in migraine, but which werefound to persist when angiography wasrepeated after several months.A 55 year old right handed white woman
was admitted to hospital with a severe bifron-tal headache which began 10 days previously.
Initially there was a throbbing pain that laterbecame a dull ache which fluctuated in inten-sity. It was accompanied by vomiting butthere was no photophobia or neck stiffness.She later described its onset as associatedwith orgasm, and admitted that she hadexperienced similar headaches for 18 months,always precipitated in the same way.Previously they had resolved after a fewhours. There was no family history ofmigraine, but the patient described violent,unilateral, throbbing headaches during hertwenties which had not been associated withsexual intercourse. There was no history ofhead injury and she was not taking oralcontraceptives or any other regular medica-tions.
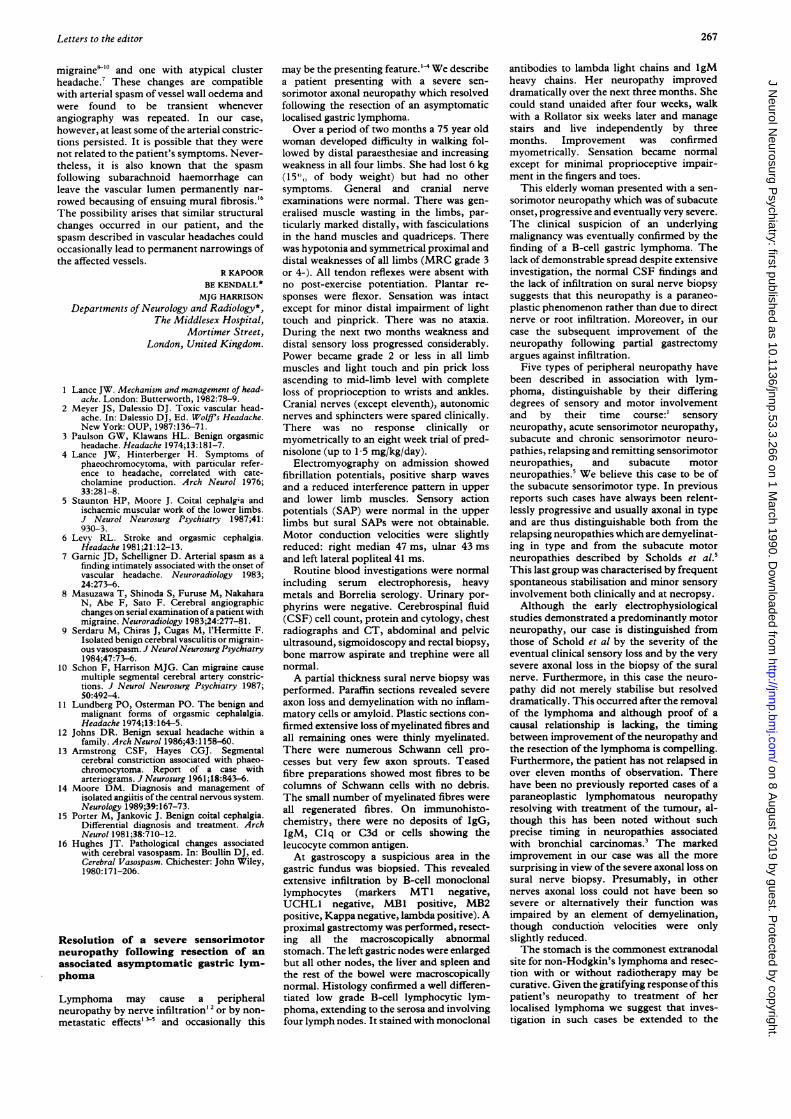
Initial examination showed no neck stiff-ness or Kernig's sign, normal fundi and nofocal neurological deficits. The blood pres-sure was 150/90 and subsequently remainedstable. Because of the duration of symptoms,it was thought necessary to exclude a sub-arachnoid haemorrhage. A cranial CT scanshowed no evidence of intracranial bleeding.At lumbar puncture the pressure was 175 mmCSF. The fluid was not xanthochromic andanalysis was otherwise normal. Four vesselangiography was performed under generalanaesthetic but this did not reveal angioma oraneurysm. However, there were segmentalnarrowings involving cortical branches ofmany of the vessels in thle supra- and infra-tentorial compartments bilaterally (fig).
Subsequent blood tests were normal, in-cluding the erythrocyte sedimentation rate(4 mm/hour), C-reactive protein (less than6 mg/L), antinuclear and rheumatoid factors.Twenty four hour urinary excretion ofvanillylmandelic acid (VMA) was also normal(31, 29 and 28 pmols/24 hr).The patient was treated with clonidine
(50 jg bd) with subsequent resolution of herheadaches despite resumption of sexualactivity. After three months, however, her
clonidine compliance became erratic and theheadaches recurred in an attenuated formwith orgasm. However, they again subsidedwhen treatment was resumed.
Intravenous digital subtraction angio-graphy was performed, eight months afterpresentation. Despite the poorer resolutionobtained by this method compared with thearterial study, some of the middle cerebralcortical branches were observed without sig-nificant overlap, and they still had regions ofnarrowing similar to those seen previously.
Despite the duration of her presentingheadache, its onset and character were typicalof this patient's coital cephalgia. This diag-nosis was further supported by the responseto migraine prophylaxis and the relation ofsymptoms to compliance with treatment.Lundberg and Osterman" regarded persis-tence of pain beyond 24 hours as favouringsubarachnoid haemorrhage rather thanbenign orgasmic cephalgia. However, sub-sequent authors have reported cases of thelatter experiencing pain for several days.'2 Inour case there was no evidence of intracranialbleeding and the clinical picture, negativeautoantibody tests, and normal erythrocytesedimentation rate did not support thepresence of a vasculitic illness to explain thesegmental cerebral arterial constrictions.These changes have also been reported inphaeochromocytoma," but again thepatient's blood pressure and normal urinaryVMA excretion were not in favour of thisdiagnosis. Finally, her benign clinical coursewas unlikely to be due to an isolated cerebralangiitis. 14
Patients with coital cephalgia usuallypresent after many attacks of pain, andangiography is not generally performed sincethe diagnosis is then apparent. Nevertheless,in at least 15 previous cases having cerebralangiography the appearances were nor-mal.' 3615 Segmental arterial narrowing hasbeen reported in three patients with
Figure Details of internal carotid (A,B) and vertebral (C) angiograms showing multiple sites of arterial narrowing.-,4,e
266
on 8 August 2019 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.3.266 on 1 M
arch 1990. Dow
nloaded from
Letters to the editor
migraine"'0 and one with atypical clusterheadache.7 These changes are compatiblewith arterial spasm of vessel wall oedema andwere found to be transient wheneverangiography was repeated. In our case,
however, at least some of the arterial constric-tions persisted. It is possible that they were
not related to the patient's symptoms. Never-theless, it is also known that the spasm
following subarachnoid haemorrhage can
leave the vascular lumen permanently nar-
rowed becausing of ensuing mural fibrosis.'6The possibility arises that similar structuralchanges occurred in our patient, and thespasm described in vascular headaches couldoccasionally lead to permanent narrowings ofthe affected vessels.
R KAPOORBE KENDALL*
MJG HARRISONDepartments of Neurology and Radiology*,
The Middlesex Hospital,Mortimer Street,
London, United Kingdom.
1 Lance JW. Mechanism and management of head-ache. London: Butterworth, 1982:78-9.
2 Meyer JS, Dalessio DJ. Toxic vascular head-ache. In: Dalessio DJ, Ed. Wolffis Headache.New York: OUP, 1987:136-71.
3 Paulson GW, Klawans HL. Benign orgasmicheadache. Headache 1974;13:181-7.
4 Lance JW, Hinterberger H. Symptoms ofphaeochromocytoma, with particular refer-ence to headache, correlated with cate-cholamine production. Arch Neurol 1976;33:281-8.
5 Staunton HP, Moore J. Coital cephalg'a andischaemic muscular work of the lower limbs.J Neurol Neurosurg Psychiatry 1987;41:930-3.
6 Levy RL. Stroke and orgasmic cephalgia.Headache 1981;21:12-13.
7 Garnic JD, Schelligner D. Arterial spasm as afinding intimately associated with the onset ofvascular headache. Neuroradiology 1983;24:273-6.
8 Masuzawa T, Shinoda S, Furuse M, NakaharaN, Abe F, Sato F. Cerebral angiographicchanges on serial examination of a patient withmigraine. Neuroradiology 1983;24:277-81.
9 Serdaru M, Chiras J, Cugas M, l'Hermitte F.Isolated benign cerebral vasculitis or migrain-ous vasospasm. J Neurol Neurosurg Psychiatry1984;47:73-6.
10 Schon F, Harrison MJG. Can migraine causemultiple segmental cerebral arterv constric-tions. J Neurol Neurosurg Psychiatry 1987;50:492-4.
11 Lundberg PO, Osterman PO. The benign andmalignant forms of orgasmic cephalalgia.Headache 1974;13:164-5.
12 Johns DR. Benign sexual headache within afamily. Arch Neurol 1986;43:1 158-60.
13 Armstrong CSF, Hayes CGJ. Segmentalcerebral constriction associated with phaeo-chromocytoma. Report of a case witharteriograms. J Neurosurg 1961;18:843-6.
14 Moore DM. Diagnosis and management ofisolated angiitis of the central nervous system.Neurology 1989;39:167-73.
15 Porter M, Jankovic J. Benign coital cephalgia.Differential diagnosis and treatment. ArchNeurol 1981;38:710-12.
16 Hughes JT. Pathological changes associatedwith cerebral vasospasm. In: Boullin DJ, ed.Cerebral Vasospasm. Chichester: John Wiley,1980:171-206.
Resolution of a severe sensorimotorneuropathy following resection of an
associated asymptomatic gastric lym-phoma
Lymphoma may cause a peripheralneuropathy by nerve infiltration'2 or by non-
metastatic effects' 3 and occasionally this
may be the presenting feature. '' We describea patient presenting with a severe sen-
sorimotor axonal neuropathy which resolvedfollowing the resection of an asymptomaticlocalised gastric lymphoma.Over a period of two months a 75 year old
woman developed difficulty in walking fol-lowed by distal paraesthesiae and increasingweakness in all four limbs. She had lost 6 kg(15',, of body weight) but had no othersymptoms. General and cranial nerve
examinations were normal. There was gen-
eralised muscle wasting in the limbs, par-
ticularly marked distally, with fasciculationsin the hand muscles and quadriceps. Therewas hypotonia and symmetrical proximal anddistal weaknesses of all limbs (MRC grade 3or 4-). All tendon reflexes were absent withno post-exercise potentiation. Plantar re-
sponses were flexor. Sensation was intactexcept for minor distal impairment of lighttouch and pinprick. There was no ataxia.During the next two months weakness anddistal sensory loss progressed considerably.Power became grade 2 or less in all limbmuscles and light touch and pin prick lossascending to mid-limb level with completeloss of proprioception to wrists and ankles.Cranial nerves (except eleventh), autonomicnerves and sphincters were spared clinically.There was no response clinically or
myometrically to an eight week trial of pred-nisolone (up to 1-5 mg/kg/day).
Electromyography on admission showedfibrillation potentials, positive sharp waves
and a reduced interference pattern in upper
and lower limb muscles. Sensory actionpotentials (SAP) were normal in the upperlimbs but sural SAPs were not obtainable.Motor conduction velocities were slightlyreduced: right median 47 ms, ulnar 43 msand left lateral popliteal 41 ms.
Routine blood investigations were normalincluding serum electrophoresis, heavymetals and Borrelia serology. Urinary por-phyrins were negative. Cerebrospinal fluid(CSF) cell count, protein and cytology, chestradiographs and CT, abdominal and pelvicultrasound, sigmoidoscopy and rectal biopsy,bone marrow aspirate and trephine were allnormal.A partial thickness sural nerve biopsy was
performed. Paraffin sections revealed severe
axon loss and demyelination with no inflam-matory cells or amyloid. Plastic sections con-
firmed extensive loss of myelinated fibres andall remaining ones were thinly myelinated.There were numerous Schwann cell pro-cesses but very few axon sprouts. Teasedfibre preparations showed most fibres to becolumns of Schwann cells with no debris.The small number of myelinated fibres were
all regenerated fibres. On immunohisto-chemistry, there were no deposits of IgG,IgM, Clq or C3d or cells showing theleucocyte common antigen.At gastroscopy a suspicious area in the
gastric fundus was biopsied. This revealedextensive infiltration by B-cell monoclonallymphocytes (markers MT1 negative,UCHL1 negative, MBI positive, MB2positive, Kappa negative, lambda positive). Aproximal gastrectomy was performed, resect-ing all the macroscopically abnormalstomach. The left gastric nodes were enlarged
but all other nodes, the liver and spleen andthe rest of the bowel were macroscopicallynormal. Histology confirmed a well differen-tiated low grade B-cell lymphocytic lym-phoma, extending to the serosa and involvingfour lymph nodes. It stained with monoclonal
antibodies to lambda light chains and 1gMheavy chains. Her neuropathy improveddramatically over the next three months. Shecould stand unaided after four weeks, walkwith a Rollator six weeks later and managestairs and live independently by threemonths. Improvement was confirmedmyometrically. Sensation became normalexcept for minimal proprioceptive impair-ment in the fingers and toes.This elderly woman presented with a sen-
sorimotor neuropathy which was of subacuteonset, progressive and eventually very severe.The clinical suspicion of an underlyingmalignancy was eventually confirmed by thefinding of a B-cell gastric lymphoma. Thelack of demonstrable spread despite extensiveinvestigation, the normal CSF findings andthe lack of infiltration on sural nerve biopsysuggests that this neuropathy is a paraneo-plastic phenomenon rather than due to directnerve or root infiltration. Moreover, in ourcase the subsequent improvement of theneuropathy following partial gastrectomyargues against infiltration.
Five types of peripheral neuropathy havebeen described in association with lym-phoma, distinguishable by their differingdegrees of sensory and motor involvementand by their time course:' sensoryneuropathy, acute sensorimotor neuropathy,subacute and chronic sensorimotor neuro-pathies, relapsing and remitting sensorimotorneuropathies, and subacute motorneuropathies.' We believe this case to be ofthe subacute sensorimotor type. In previousreports such cases have always been relent-lessly progressive and usually axonal in typeand are thus distinguishable both from therelapsing neuropathies which are demyelinat-ing in type and from the subacute motorneuropathies described by Scholds et al.'This last group was characterised by frequentspontaneous stabilisation and minor sensoryinvolvement both clinically and at necropsy.Although the early electrophysiological
studies demonstrated a predominantly motorneuropathy, our case is distinguished fromthose of Schold et al by the severity of theeventual clinical sensory loss and by the verysevere axonal loss in the biopsy of the suralnerve. Furthermore, in this case the neuro-pathy did not merely stabilise but resolveddramatically. This occurred after the removalof the lymphoma and although proof of acausal relationship is lacking, the timingbetween improvement of the neuropathy andthe resection of the lymphoma is compelling.Furthermore, the patient has not relapsed inover eleven months of observation. Therehave been no previously reported cases of aparaneoplastic lymphomatous neuropathyresolving with treatment of the tumour, al-though this has been noted without suchprecise timing in neuropathies associatedwith bronchial carcinomas.3 The markedimprovement in our case was all the moresurprising in view of the severe axonal loss onsural nerve biopsy. Presumably, in othernerves axonal loss could not have been sosevere or alternatively their function wasimpaired by an element of demyelination,though conduction velocities were onlyslightly reduced.The stomach is the commonest extranodal
site for non-Hodgkin's lymphoma and resec-tion with or without radiotherapy may becurative. Given the gratifying response ofthispatient's neuropathy to treatment of herlocalised lymphoma we suggest that inves-tigation in such cases be extended to the
267
on 8 August 2019 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.53.3.266 on 1 M
arch 1990. Dow
nloaded from


















