W120 Six Root Cause Analysis Tools for Performance Improvement Handouts/W120.pdf · Affinity...
17
1 Six Root Cause Analysis Tools For Performance Improvement Lisa Bridwell, Telligen Program Specialist September 2019 2 Today’s Objectives 1. Connecting QAPI and Root Cause Analysis 2. Identify Root Cause Analysis tools for adverse events 3. Recognize how to combine root cause analysis tools 4. Describe one method to prioritize root causes 3 A data‐driven, proactive approach to improving the quality of life, care and services in nursing homes • Involves members at all levels of the organization • Identify opportunities for improvement by addressing gaps in systems or processes developing and implement an improvement plan continuously monitoring effectiveness of interventions. QAPI
Transcript of W120 Six Root Cause Analysis Tools for Performance Improvement Handouts/W120.pdf · Affinity...

1
Six Root Cause Analysis Tools For Performance Improvement
Lisa Bridwell, Telligen Program Specialist
September 2019
2
Today’s Objectives
1. Connecting QAPI and Root Cause Analysis
2. Identify Root Cause Analysis tools for adverse events
3. Recognize how to combine root cause analysis tools
4. Describe one method to prioritize root causes
3
A data‐driven, proactive approach to improving the quality of life, care and services in nursing homes
• Involves members at all levels of the organization
• Identify opportunities for improvement by
addressing gaps in systems or processes
developing and implement an improvement plan
continuously monitoring effectiveness of interventions.
QAPI

2
4
• Prioritize
– Adverse events, high‐risk, high volume or problem prone areas
• Performance improvement activities must track
– Adverse Events, high‐risk, high volume or problem prone areas
• Regulatory mandate
– QAA committee, identifies root cause(s) of quality deficiencies and develops an action plan
Requirements of Participation
5
Find Out
1. What happened?
2. Why did it happen?
3. How to prevent it from
“happening again”?
Goal of Root Cause Analysis
Source: https://www.patientsafety.va.gov/professionals/onthejob/rca.asp
6
Impact of Process Failures
Swiss Cheese Model
1. Holes in cheese = individual process weaknesses
2. Holes continually vary in size and position in all slices
3. Failure = all holes in each slice align

3
7
Human Factors
8
1. Human failures are universal and inevitable
2. People cannot easily avoid those actions they did not intend to commit
3. Errors are consequences rather than causes
4. Many errors fall into recurrent patterns
5. The same or similar events have often occurred before
10 Facts About Human Failures1‐5
https://humanfactors101.files.wordpress.com/2016/09/ten‐facts‐on‐human‐failure‐humanfactors101.pdf
9
6. The best people can make the worst mistakes
7. Similar failures occur in all industries
8. Safety significant failures can occur at all levels of a system
9. There are certain situations/conditions that lead people into the same failure
10. You cannot change the human condition, but you can change the conditions in which they work
10 Facts About Human Failures6‐10
https://humanfactors101.files.wordpress.com/2016/09/ten‐facts‐on‐human‐failure‐humanfactors101.pdf

4
10
Impact of Human Factors
Human FactorsAre elements that influence the performance of people, systems and operating equipment
Human Factors
Principles & Systems Design• Avoid reliance on memory or
vigilance
– Checklists
– Protocols
• Simplify processes
• Standardize procedures to reduce unintended variation
• Use constraints and forcing functions
11
• Team Sport
• Effective problem solving method for
– System improvement
– Adverse events
• “No pain‐ No gain”
– It is not easy
Root Cause Analysis (RCA)
12
• Inter‐disciplinary– Leadership charters
– Involves those most familiar with situation/front line staff
– Facilitated
• A process that identifies necessary changes to systems by searching for the real problem
• Determine cause and effect – Dig deeper and ask “Why?” at each level of discovery
• A process that is as impartial as possible– Focus on process and not people
– Strive to create “A Just Culture”
Root Cause Analysis (RCA) Process
Source: https://www.patientsafety.va.gov/professionals/onthejob/rca.asp

5
13
1. Credible– Participation: Leadership and those closely involved with process
– Consistent
– Include consideration of relevant literature
2. Data Driven– Gather/Interpret facts and information that lead to event
3. Thorough– Understanding of human and other factors
– Determination of related processes and systems
– Analysis of underlying cause and effect systems through a series of whyquestions
– Recognize risks and their potential contributions
– Identify potential improvement in processes or systems
RCA : Key Concepts
Source: https://www.patientsafety.va.gov/professionals/onthejob/rca.asp
14
Data
15
Pareto Chart

6
16
CMS Guidance for Performing RCA
1. Identify event
2. Charter and select a team/facilitator
3. Describe event
4. Identify contributing factors
5. Identify root causes
6. Design and implement changes
7. Measure the success
17
Examine a Process
18
Make Certain You Understand the Process
Adverse or Single Events Process Improvement

7
19
• Adverse or Single Events
Timeline
20
Adverse or Single Events
Time Line with Contributing Factors
Contributing Factors
21
• Flow chart/outline steps of the event or problem as it happened (current state)
• Flow chart /outline steps of the process as it should be (future state)
Process Flow Describe What Happened

8
22
Mismatches and gaps between what should have happened and what did happen.
Identify the Problem
23
Root Cause Analysis (RCA)
is a systematic process identifying unseen factors contributing to undesirable
outcomes
Identify Root Causes (RCA)
24
Avoid Jumping to SolutionsFocus on the Purpose of RCA
• Keeps us from jumping right to solution without really understanding the problem
• Keeps us from fixing the wrong thing
• Helps us find the right solution rather than a global, ‘one‐size‐fits‐all’ solution
• Focus is on the process, not the people
• Explore the cause‐and‐effect relationships underlying a particular problem
• Starts with data
9
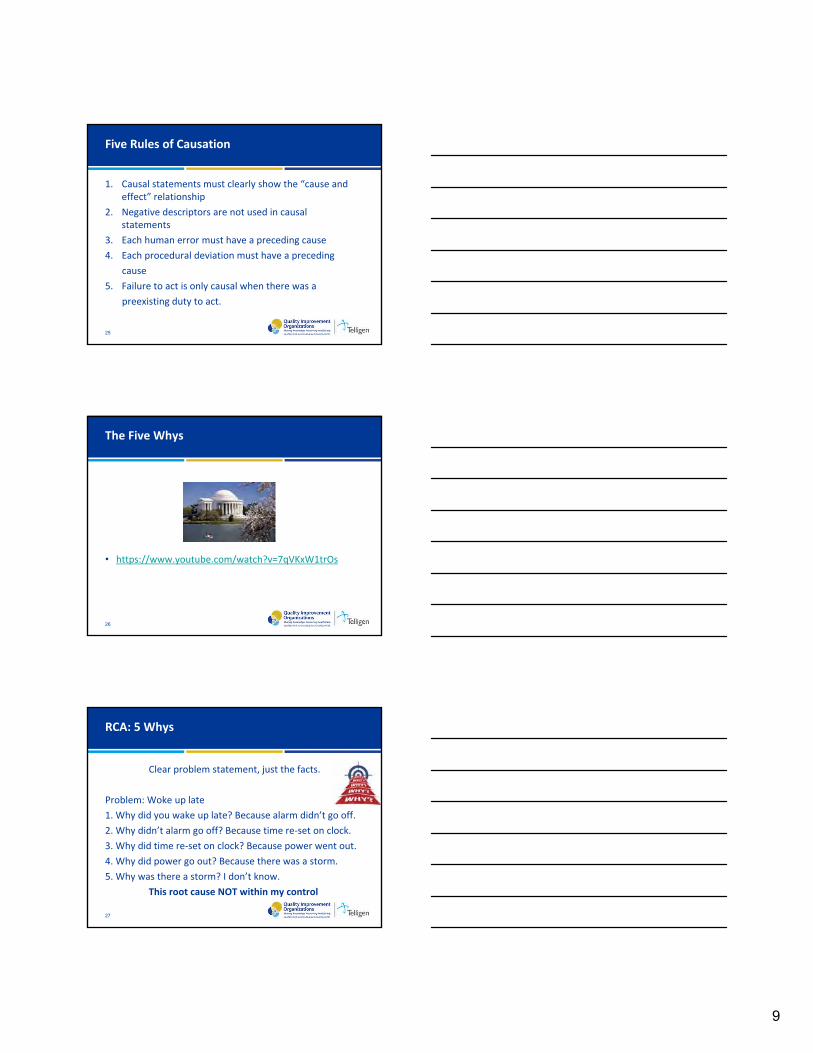
25
1. Causal statements must clearly show the “cause and effect” relationship
2. Negative descriptors are not used in causal statements
3. Each human error must have a preceding cause
4. Each procedural deviation must have a preceding
cause
5. Failure to act is only causal when there was a
preexisting duty to act.
Five Rules of Causation
26
• https://www.youtube.com/watch?v=7qVKxW1trOs
The Five Whys
27
Clear problem statement, just the facts.
Problem: Woke up late
1. Why did you wake up late? Because alarm didn’t go off.
2. Why didn’t alarm go off? Because time re‐set on clock.
3. Why did time re‐set on clock? Because power went out.
4. Why did power go out? Because there was a storm.
5. Why was there a storm? I don’t know.
This root cause NOT within my control
RCA: 5 Whys

10
28
Clear problem statement, just the facts.
Problem: Woke up late
1. Why did you wake up late? Because alarm didn’t go off.
2. Why didn’t alarm go off? Because time re‐set on clock.
3. Why did time re‐set on clock? Because clock lost power.
4. Why did clock loose power? Because back‐up battery was not installed.
5. Why was back‐up battery not installed? Because I didn’t know I needed to install one.
This root cause is within my control.
RCA: 5 Whys
29
• Identify the problem– Be very specific and include data
• Ask ‘Why did that happen?’
• “I know” vs “I think”– No speculation here
• Reason must be within your control – Stay away from medical diagnoses
Let’s Practice Using The 5 Whys
30

11
31
Fishbone Diagram for System Level Issues
Uses standard categories
Materials
Environment
People
Method
equipment
Different Tools for Different Needs
32
Fishbone Diagram
33
Audience Participation………
Hand Hygiene Barriers
Agency staff
Forgets
Policies
Empty Dispensers
Procedures
No Time
Lack of leadership
1‐Empty Dispensers2‐Agency Staff3‐Lack ofLeadership4‐No Time5‐Forgets6‐No safety audits
No Safety Audit

12
34
Affinity diagram
– Best for a system level issues. Something that affects everyone
Running out of supplies
Cold eggs in the morning
Missing laundry
Different Tools for Different Needs
35
Affinity Diagram
• Brainstorm ideas as to why the event/problem is happening
– Focus on people not process
• Write one idea per Post‐it note
• Group similar ideas together
• Things to consider
– Do we have control over the reason?
– Can we fix it?
– Will it solve the problem?
36
Failure Mode and Effects Analysis
• A structured way to identify potential problems or failures
• Address potential problems before they occur
– Potential bottlenecks
– Unintended consequences
– Impact on other process/systems

13
37
FMEA and Root Cause Analysis
Both Are:
• System focused
• Team Project
• Investigative Techniques
• Lead to Outcome Measure Development
Only FMEA
• Tries to Prevent Errors before they occur
• Allows YOU to choose what you investigate
• Focuses on Processes in the future
38
Guidance for Performing Failure Mode and Effects Analysis with Performance Improvement Projects
Steps
1. Select a process to analyze
2. Charter and select team facilitator and team members
3. Describe the process
4. Identify what could go wrong during each step of the process
5. Pick which problems to work on eliminating
6. Design and implement changes to reduce or prevent problems
7. Measure the success of process changes
39
Prioritizing Root Causes

14
40
Do actions meet the following?
• Unmistakable link to the root cause(s) including identified preceding causes?
• Specific?
• Easily understood and implemented using PDSA?
• Developed by the process owners/leaders?
• Measurable?
If no, go back and review root causes
Creating An Action Plan For Root Causes
41
PDSA
42
Weaker Actions
• Double checks
• Warnings and labels
• New procedure/memo/policy
• Training
• Additional study/analysis
Weak Actions for Process Change
Avoid using as a single actionIt can support other actions

15
43
Intermediate Actions
• Increase staffing/decrease workload
• Software enhancements/modification
• Eliminate/reduce distractions
• Checklist/Cognitive aid
• Eliminate look alike and sound alike terms
• “Read back” to assure clear communication
• Enhanced documentation/communication
Better Corrective Actions for Process Change
44
Stronger Actions
• Change physical surroundings
• Usability testing of devices before purchasing
• Engineering (forcing function) controls into system to force the user to complete an action
• Simplify process and remove unnecessary steps
• Standardize equipment or process
• Tangible involvement and action by leadership in support of resident safety
Best Corrective Actions for Process Change
45
Facilitator
• Gather and distribute data prior to meeting
• Create a schedule if multiple meetings are necessary
• Create an agenda with specific time frames and ground rules (1‐ 2 hours to complete RCA)
• Confirm attendance and participation
• Prepare participants
– provide PIP/RCA training/resources and information for the RCA prior to the meeting
• Prepare the workspace
– white boards markers, post it notes
Root Cause Analysis Facilitation Tips

16
46
• Introduce participants and describe meeting goals (list goals on agenda)
• Clarify meeting roles: facilitator, scribe, time keeper (list on agenda)
• Discuss event to be investigated (and why it was chosen for RCA)
• Set group norms
• Decide on process to be used to describe what happened
Collected and organize facts surrounding the event
Review findings
• Determine process that will be used to identify root causes
Thorough systematic analyses using tools such as fishbone, five whys
• Identify root causes
• Prioritize root cause for Improvement
• Select next meeting date to create action plan
Sample Agenda Items for RCA Meeting
Source: IIPC NCC “Effective QI meeting Management and Facilitation for Nursing Homes”, Stratis Health 2014
47
Questions
48
• Telligen QIN‐QIO Nursing Home Care https://telligenqinqio.com/our‐work/nursing‐home‐care/
• QAPI Process Framework Tools https://www.cms.gov/Medicare/Provider‐Enrollment‐and‐Certification/QAPI/Downloads/ProcessToolFramework.pdf
• CMS (Centers for Medicare and Medicaid Services https://www.cms.gov
• Root Cause Analysis Toolkit http://www.health.state.mn.us/patientsafety/toolkit/
• Institute for Healthcare Improvement http://www.ihi.org/
• Effective QI Meeting Management and Facilitation for Nursing Homes http://www.stratishealth.org/documents/Effective‐QI‐Mtg‐Mgmt‐Facilitation‐Slides‐2014‐07‐09.pdf
Resources

17
49
• Joint Commission: Root Cause Analysis in Health Care: Tools and Techniques https://www.jcrinc.com/assets/1/14/EBRCA15.pdf
• VA Center for Patient Safety: https://www.patientsafety.va.gov/professionals/onthejob/rca.asp
• Affinity Diagram http://asq.org/healthcare‐use/links‐resources/affinity‐diagram‐example.html
• Getting to the root of the root‐cause analysis problem https://www.americannursetoday.com/getting‐to‐the‐root‐of‐the‐root‐cause‐analysis‐problem/
Resources
50
Contact Us
Lisa Bridwell
lisa.bridwell@area‐d.hcqis.org
630‐928‐5831
Nell Griffin
nell.griffin@area‐d.hcqis.org
630‐928‐5813
Stacy Gordonstacy.gordon@area‐d.hcqis.org630‐928‐5812
Deanna Currydeanna.curry@area‐d.hcqis.org720‐554‐1479
This material was prepared by Telligen, the Medicare Quality Improvement Organization for Colorado, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. 11SOW-QIN-C2-06/04/2018-2782
Elizabeth Schulte Mullinselizabeth.schulte@area‐d.hcqis.org(720) 554‐1395
Gina Andersongina.anderson@area‐d.hcqis.org515‐223‐2900
Kristen Ives – NHSN supportkristen.ives@area‐d.hcqis.org720‐554‐1695
Sarah Wendelboe‐NHSN supportsarah.wendelboe@area‐d.hcqis.org(515) 267‐6227












![Sistema de alarma WiFi W120 Alarm System/(ES... · 2018. 11. 5. · Pulse el botón [+] de la página principal. Toque en [Alarma WiFi W120] y siga los pasos para configurar su centralita](https://static.fdocuments.in/doc/165x107/6102252e59a33b2a975b029e/sistema-de-alarma-wifi-w120-alarm-systemes-2018-11-5-pulse-el-botn.jpg)