Vertebral Artery Dissection Complicating Pregnancy and Puerperium: Case report and review of the...
25
Vertebral Artery Dissection Complicating Pregnancy and Puerperium: Case report and review of the literature Reza Pour N, Chuah S, Vo T, Department of Obstetric and Gynaecology, Liverpool Hospital, South Western Local Health District, Sydney
-
Upload
andrea-ferguson -
Category
Documents
-
view
216 -
download
2
Transcript of Vertebral Artery Dissection Complicating Pregnancy and Puerperium: Case report and review of the...

Vertebral Artery Dissection Complicating Pregnancy and
Puerperium: Case report and review of the
literature
Reza Pour N, Chuah S, Vo T, Department of Obstetric and Gynaecology,Liverpool Hospital, South Western Local Health District, Sydney

INTRODUCTION:
• Vascular dissections occur rarely during pregnancy. Spontaneous extracranial vertebral artery dissection (VAD) itself is very rare in general.
• The majority of pregnancy-related cerebrovascular diseases (CVD) occur during delivery or 6 weeks immediately after delivery. Recent data suggest that this increased risk may actually extend as long as 12 weeks postpartum.
• Risk factors for CVD: preeclampsia, eclampsia, chronic kidney disease, black race, pregnancy related hematologic disorders, advanced age

CLINICAL PRESENTATION:
Clinical presentation varies from patient to patient. Spontaneous VAD can present as:
• Headache• Neck pain • Diplopia • Transient ischaemic attack
(TIA) • Horner’s syndrome • Ischemic stroke
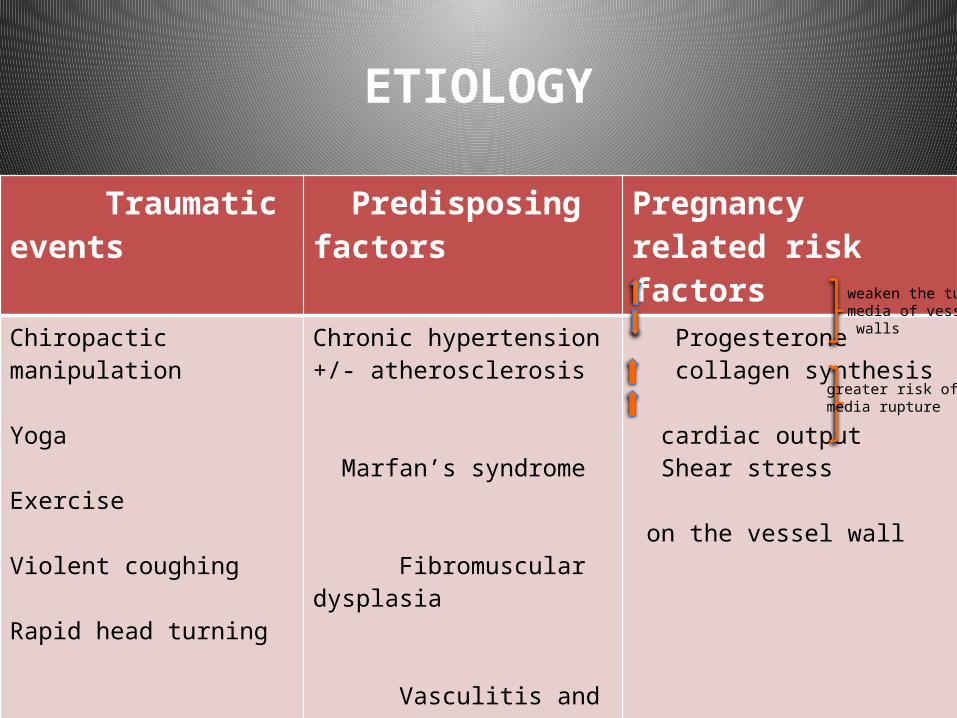
ETIOLOGY
Traumatic events Predisposing factors Pregnancy related risk factors
Chiropactic manipulation Yoga
Exercise Violent coughing Rapid head turning
Chronic hypertension +/- atherosclerosis Marfan’s syndrome Fibromuscular dysplasia Vasculitis and cystic medial necrosis
Oral contraceptives Migraine
Progesterone collagen synthesis
cardiac output Shear stress on the vessel wall
weaken the tunicamedia of vessel walls
greater risk of media rupture
CASE DESCRIPTION
Case 1:• 32-year-old• G1P0• 38+2/40 • No significant past
medical history• Low risk, midwifery
antenatal care

Timing Symptoms & Signs BP (mmHg) CTG Actions
On arrival
Early labour 130/70 Reassuring monitor at BU
During BU admission
-Dizziness -Severe frontal headache -blurry vision
150/110 Variable decelerations
Labetalo,l PO, STAT
15 minutes later -Stronger contractions-Unremarkable examination
238/120 Variable decelerations
Hydralazine IV, STAT
15 minutes later No neurological symptoms
140/80 Reassuring Close observation
2 hours later Eclamptic seizure 230/120 Variability complex variable decelerations Bradycardia (66bpm)
-Loading dose MgS04-Hydralazine IV, STAT-Emergency LSCS under GA
INTRAPARTUM HISTORY

A healthy male baby, BW 2.46 kg, APGAR scores of 4-7-10

Timing Symptoms & Signs
BP (mmHg)
Investigations Actions
Immediate Post-CS
Intubated for 12hrs Unstable Plt : 180Cr: 69ALT : 69 AST : 101
-ICU admission-BP management-Maintenance MgSO4 infusion
48hrs post-CS
-L sided neck pain -Occipital headache (refractory to simple analgesia)
Unstable -CT Head: NAD-CTA neck: L VAD-MRI: confirmed Dx
Low dose Aspirin
D10 post-CS asymptomatic Stable -Vasculitis screen: NAD-Placenta histopathology: NAD
-Discharged home-triple agents oral antihypertensive -aspirin-OPD follow up
POSTNATAL HISTORY

CTA of neck, Focal stenosis with thickened wall and an intramural thrombus of left vertebral artery at the level of C3.

MRI Brain, confirmed the presence of a short segment vertebral artery dissection at the level of C3.
L Vertebral Art

• After a detailed history, she reported sudden onset of left sided neck pain four days prior to the hospital presentation and had neck massage two days after the onset of pain, resulted in worsening of the symptoms which required taking regular simple analgesia.

• 33-year-old
• G2P0, TOP x 1
• No significant personal or family history
• She received appropriate antenatal care in the midwives clinic.
Case 2:

Timing Symptoms & Signs
BP (mmHg) Investigations Actions
35+5/40 - FMs- Mild headache- Pedal oedema
133/85 CTG reassuringPET bloods normal
-Discharged home-ANC follow up
36/40 -constant occipital headache -flashing lights in her visual field
155/105 -CTG reassuring-Growth USS normal-PET bloods normal- Urine PCR (296)
-Admit to the ANW-Expectant management of preeclampsia-Oral Labetalol
36+2/40 right-sided neck pain -refractory high DBP -fluctuant SBP
MRI neck: R VAD - Em LSCS under Spinal-ICU admission-Heparin infusion (6hrs post-op)
ANTENATAL HISTORY

Healthy female baby, BW 2.9kg,APGAR of 9 at 10 minutes

MRA neck, coronal view of the vertebral arteries confirms a 11mm C2-C3 right vertebral artery dissection
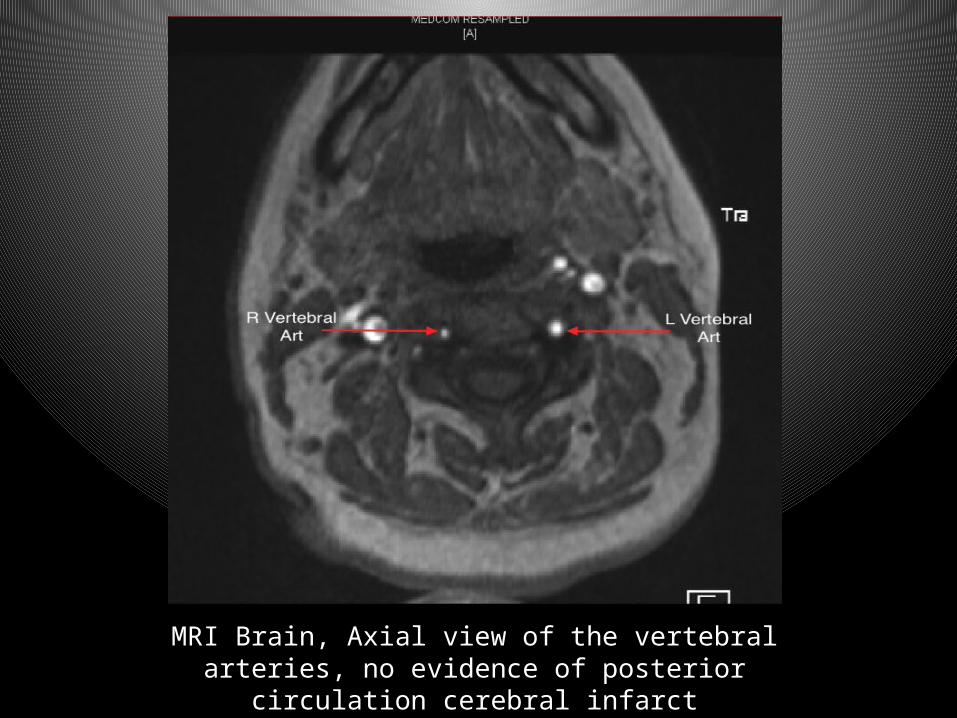
MRI Brain, Axial view of the vertebral arteries, no evidence of posterior circulation cerebral infarct

Timing Symptoms & Signs
Vital signs Investigations Actions
D2 post-CS -lower abdominal pain-severely tender and peritonitic abdomen
Haemodynamically unstable
- Hb despite blood transfusion-CT abdo/pelvis: haematoma of rectus muscle + several areas of acute bleeding
-Heparin infusion was ceased-Explorative laparotomy: haematoma evacuation - Low dose Aspirin: the next day post-op
D7 Post-CS Increasing abdominal symptoms.
Temp 38 C -Repeat CT abdo: rectus sheath + extraperitoneal haematoma
-IV antibiotics -CT-guided aspiration of pelvic collection
D15 post-CS
Improving symptoms
-afebrile -stable
- Aspirate MCS: negative
-discharged home-Low dose Aspirin-Oral antibiotics -oral antihypertensive-OPD follow up
POSTNATAL HISTORY

FOLLOW-UP PLAN
• Repeat MRI in 3 months postpartum • Cease Aspirin if the dissection stable or
resolved• Prophylactic antiplatlet or antithrombotic
therapy through the next pregnancy

DISCUSSION
• The actual incidence of VAD in the pregnancy and post partum period in association with preeclampsia/eclampsia is unknown as the current literature consists of case series and reports only.
• Because of collateral circulation, unilateral vertebral artery dissections may go unrecognized and may be more common than suspected. The outcome for most patients is benign, reflecting the adequacy of the collateral circulation in young patients. However, arterial compromise can result in brain injury by several mechanisms.

Literature Review
• One case was found to have posterior circulation stroke as a
result of bilateral VAD and labour was induced at 37 weeks gestation for preeclampsia.
• Another patient at 38 weeks with severe neck pain that
persisted after induction for elevated blood pressure and arteriography showed R VAD postpartum.
• A single case of lethal VAD in pregnancy with subsequent massive subarachnoid haemorrhage (SAH) has been reported that was confirmed by autopsy.
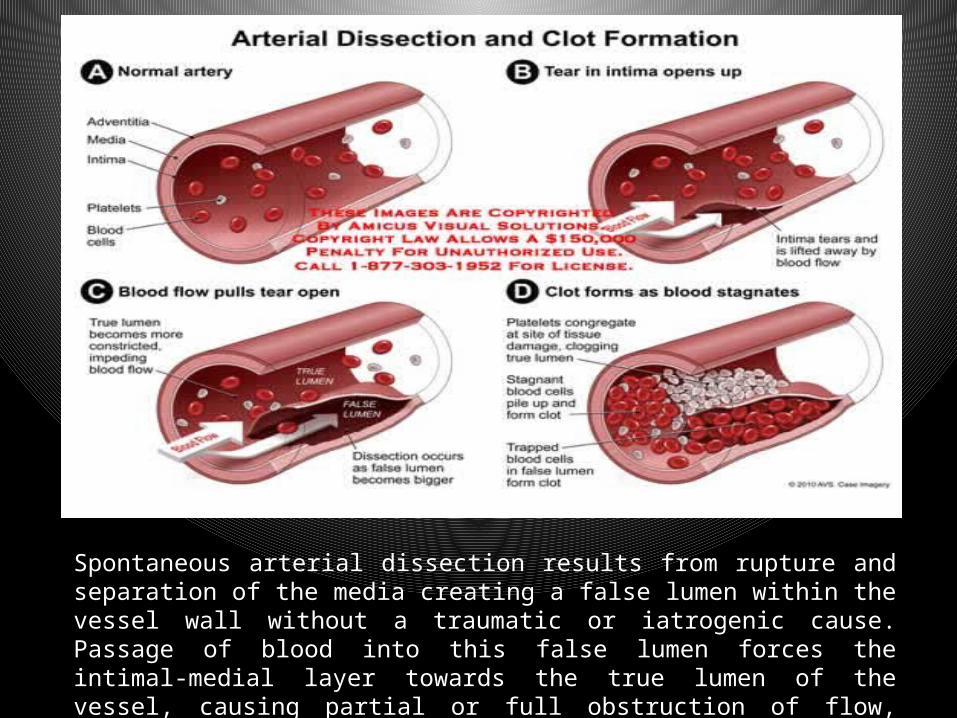
Spontaneous arterial dissection results from rupture and separation of the media creating a false lumen within the vessel wall without a traumatic or iatrogenic cause. Passage of blood into this false lumen forces the intimal-medial layer towards the true lumen of the vessel, causing partial or full obstruction of flow, ultimately leading to an ischaemic event.

• Diagnosis: CT or MRI angiography
• Treatment: anticoagulation or antiplatelet therapy For a minimum of 3-6 months
• Reason for treatment: prevent future ischaemic events, allow the dissection to heal on its own • Safe MOD: UNKNOWN! We recommend LSCS

CONCLUSION
• We had 2 cases of VAD in the context of hypertensive disorders of pregnancy with an acceptable outcome. A high level of vigilance is required particularly with preeclamptic patients presenting with head/neck pain to allow an early diagnosis. This is as we hypothesise, early and aggressive management of vertebral artery dissection may potentially prevent further neurological complications.
• However, post operative recovery of our second patient was complicated by side effects of
anticoagulant that required further procedural interventions and prolonged hospital stay. • The use of anticoagulants may be questionable if antiplatelet therapy is effective enough to
prevent future ischaemic events specifically in an obstetric patient after caesarean delivery due to possible devastating complications.
• There is an undeniable need for further studies to find the best management of vertebral
artery dissection in pregnant and postpartum population. Since the incidence is very low, such a study would require the involvement of many different clinical centres and would take many years to accomplish.
• There is limited data on which mode of delivery is the safest. In our limited experience, we recommend caesarean section to hasten delivery so that we can reduce the period of elevated BP that theoretically may increase extension of the dissection and the subsequent neurological complications.

REFERENCES
1. Mass S, Cardonick E, Haas S, Gopalani S, Leuzzi R. Bilateral vertebral artery dissection causing a cerebrovascular accident in pregnancy. J Reprod Med. 1999;44:887-890
2. Cenkowski M, daSilva M, Bordun KA, Hussain F, Kirkpatrick ID, Jassal DS. Spontaneus dissection of the coronary and vertebral arteries post-partum: case report and review of the literature. BMC Pregnancy Childbirth. 2012 Nov 2;12:122.
3. Hovsepian DA, Sriram N, Kamel H, Fink ME, Navi BB. Acute Cerebrovascular Disease Occuring After Hospital Discharge for Labor and Delivery. Stroke. 2014 Jul;45(7):1947-50.
4. Glauser J, Hastings OM, Mervart M, et al: Dissection of vertebral arteries: Case report and discussion. J Emerg Med. 1994;12:307-315
5. Tuluc M, Brown D, Goldman B. Lethal Vertebral Artery Dissection in Pregnancy A Case Report and Review of the Literature. Arch Pathol Lab Med. 2006 Apr;130(4):533-5
6. O'Rourke N, Wollman L, Camann W. Bilateral spontaneous vertebral artery dissection: management during labor and vaginal delivery. Int J Obstet Anesth. 2004 Jan;13(1):44-6.
7. Moroz L, Airoldi J, Almario C et al. Prophylactic treatment during pregnancy for women with a history of vertebral artery dissection. American J of Obstetric and Gynaecology. 2006; 195; 104