Upper Respiratory tract Obstruction
27
presented by : Dr. Mona Ahmed A/Raheem ENT Surgeon Khartoum National Center for Ear, Nose and Throat Diseases and Head and Neck Surgery Assistant Professor Faculty of Medicine & Health Sciences Alneelain University Upper Respiratory Upper Respiratory tract Obstruction tract Obstruction
description
presented by : Dr. Mona Ahmed A/Raheem ENT Surgeon Khartoum National Center for Ear, Nose and Throat Diseases and Head and Neck Surgery Assistant Professor Faculty of Medicine & Health Sciences Alneelain University. Upper Respiratory tract Obstruction. Definition. - PowerPoint PPT Presentation
Transcript of Upper Respiratory tract Obstruction

presented by : Dr. Mona Ahmed A/Raheem
ENT Surgeon Khartoum National Center for Ear, Nose and Throat Diseases and Head and Neck
SurgeryAssistant Professor
Faculty of Medicine & Health SciencesAlneelain University
Upper Upper Respiratory tract Respiratory tract
ObstructionObstruction

DefinitionDefinition
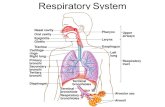
It is obstruction of the respiratory It is obstruction of the respiratory tract above the larynx.tract above the larynx.
The upper airway extends from The upper airway extends from the nares to the inferior end of the nares to the inferior end of the larynx.the larynx.
The lower airway extends from the The lower airway extends from the inferior end of the larynx to the inferior end of the larynx to the terminal bronchioles.terminal bronchioles.

Respiratory System DiagramRespiratory System Diagram

StridorStridor
•Is a physical sign common to Is a physical sign common to all causes of URT obstruction all causes of URT obstruction
• It is a harsh, raspy noise It is a harsh, raspy noise produced by the flow of air produced by the flow of air through partially obstructed through partially obstructed airwayairway

Stridor
Inspiratory stridor
Biphasic stridor
Expiratorystridor

• Inspiratory stridor:Inspiratory stridor:
Obstruction at the level of the larynx Obstruction at the level of the larynx or aboveor above
• Biphasic stridor:Biphasic stridor:
Obstruction in the tracheaObstruction in the trachea
• Expiratory stridor: Expiratory stridor:
0bstruction below the carena0bstruction below the carena

causes causes
1.1.LarynxLarynx- Supraglottic: Supraglottic: laryngomalacialaryngomalacia
webweb
cystic hygromacystic hygroma
laryngocelelaryngocele

– Glottic:Glottic: webweb
vocal cord paralysisvocal cord paralysis
• Subglottic:Subglottic: webweb
stenosisstenosis
haemangiomahaemangioma

Laryngeal Web (glottic)Laryngeal Web (glottic)

Laryngeal Web (endoscopic view)Laryngeal Web (endoscopic view)

2-2- Trachea & BronchiTrachea & Bronchi webweb stenosisstenosis tracheomalaciatracheomalacia3-3- Trauma Trauma thermal &chemicalthermal &chemical externalexternal surgicalsurgical intubationintubation

4-4- Foreign Body Foreign Body laryngeallaryngeal trachealtracheal bronchealbroncheal
5-5- Inflammtory Inflammtory acute laryngitisacute laryngitis laryngeotracheobronchitis (croup)laryngeotracheobronchitis (croup) acute epiglottitisacute epiglottitis diphtheriadiphtheria
6- 6- AllergyAllergy7-7- Neoplasm Neoplasm

ManagmentManagment
1- History1- History
2- secure the upper 2- secure the upper airwayairway

Foreign BodiesForeign Bodies
•History:History:• Usually there is definitive history of Usually there is definitive history of
choking followed by paroxysmal choking followed by paroxysmal coughing then subsides.coughing then subsides.
• After the initial paroxysm of coughing After the initial paroxysm of coughing the tracheobronchial mucosa becomes the tracheobronchial mucosa becomes tolerant to the F.B & cough ceases. tolerant to the F.B & cough ceases.

• The triad of symptoms of F.B The triad of symptoms of F.B inhalation are inhalation are
1.1. chockingchocking
2.2. ChoughingChoughing
3.3. WheezingWheezing
• Present in 91% OF pts.Present in 91% OF pts.
• Sudden onset of wheeze in a child not Sudden onset of wheeze in a child not known to be asthmatic especially if it known to be asthmatic especially if it is unilateral possibility of F.B is unilateral possibility of F.B inhalation inhalation

• Persistent fever with respiratory tract Persistent fever with respiratory tract infection not respond to treatment is infection not respond to treatment is possible to be F.B inhalation.possible to be F.B inhalation.
• Persistent or recurrent penumonia Persistent or recurrent penumonia needs Brochoscopy to execlude the needs Brochoscopy to execlude the presnce of F.Bpresnce of F.B

Clinical features:Clinical features: Patient present with variety of Patient present with variety of
symptoms depending on the location of symptoms depending on the location of the F.B & degree of obstructionthe F.B & degree of obstruction
• In the first few hoursIn the first few hours• Audible click may be heared by Audible click may be heared by
stethoscope due to movement of F.Bstethoscope due to movement of F.B• Unilateral respiratory wheeze & Unilateral respiratory wheeze &
reduced air entery indecate F.B reduced air entery indecate F.B bronchus.bronchus.
• If F.B not removed within the first 24 If F.B not removed within the first 24 hourshours

• Pneumotic signes may be foundPneumotic signes may be found
• Atelectasis of the distal lung Atelectasis of the distal lung
• Lung absces ( takes several months ) Lung absces ( takes several months )

InvestigationInvestigation
• Radiological, X RAY with extended Radiological, X RAY with extended neck both antroposterior & lateral neck both antroposterior & lateral viewsviews
• Sometimes may need CT SCAN in Sometimes may need CT SCAN in long standing F.Bslong standing F.Bs

TreatmentTreatment
laryngoscopy or laryngoscopy or bronchoscopybronchoscopy

F.B Right Main BronchusF.B Right Main Bronchus

F.B F.B

Tracheostomy Tracheostomy

Tracheostomy ProcedureTracheostomy Procedure

Plastic Tracheostomy Tube(Portics)Plastic Tracheostomy Tube(Portics)

Metalic Tracheostomy TubeMetalic Tracheostomy Tube