Update On Management Of Rhinitis - University of Hong...
7
Update On Management Of Rhinitis W K Ho,* FRCSEd, DLO, FHKAM(ORL) W I Wei, MS, FRCSEd, DLO, FHKAM(ORL) P K Y Lam, MBBS Division of Otorhinolaryngology Department of Surgery The University of Hong Kong Summary Rhinitis is common in Hong Kong. The aim of treatment is to control the symptoms and to allow an undisturbed lifestyle without the side-effects of therapy. A secondary goal is to prevent the complication of sinusitis and its sequelae. Most of these goals can be achieved by the combination of anti-allergy management, oral or topical medication and the occasional surgical intervention. (HK Pract 1998;20:319-326) Introduction Rhinitis is a common problem in Hong Kong. The local prevalence of hay fever, the classical allergic rhinitis, is reported to be 15.7% in a study of 1062 secondary school students. 1 In the United States, it is estimated that one in five persons suffers from allergic rhinitis 2 ' 3 and 3 percent of all medical consultations are for management of patients with nasal symptoms. Currently 30 to 40 million Americans suffer from nasal congestion, sneezing and runny nose and this prevalence is escalating both in the USA 4 and European countries. 5 ' 6 Rhinitis, rhinosinusitis and classification The mucosa of the nose is in continuity with that of the paranasal sinuses. In all forms of rhinitis, some degree of inflammation is also present in the paranasal sinuses. It is often difficult to differentiate rhinitis from sinusitis clinically. As a result, some physicians prefer to use the term rhinosinusitis instead of rhinitis or sinusitis. 7 However, isolated rhinitis and sinusitis, for example sinusitis due to odontogenic infection, do exist. Simple rhinitis may be acute or chronic. Chronic disease is arbitrarily defined as a persistence of symptoms for more than 12 weeks. 7 By aetiology, rhinitis can be of infective or non-infective in origin. The commonest acute infective rhinitis is common cold virus infection. Patients with non-infective rhinitis belong to one of the two groups. Those related to atopy may * Address for correspondence: Dr Ho Wai-kuen, Department of Surgery, the University of Hong Kong Medical Centre, Queen Mary Hospital, Hong Kong. 319
Transcript of Update On Management Of Rhinitis - University of Hong...

Update On Management Of Rhinitis
W K Ho,* FRCSEd, DLO, FHKAM(ORL)
W I Wei, MS, FRCSEd, DLO, FHKAM(ORL)
P K Y Lam, MBBSDivision of Otorhinolaryngology
Department of SurgeryThe University of Hong Kong
Summary
Rhinitis is common in Hong Kong. The aim of treatment is to control the symptoms and to allow an undisturbedlifestyle without the side-effects of therapy. A secondary goal is to prevent the complication of sinusitis and itssequelae. Most of these goals can be achieved by the combination of anti-allergy management, oral or topicalmedication and the occasional surgical intervention. (HK Pract 1998;20:319-326)
Introduction
Rhinitis is a common problem inHong Kong. The local prevalence ofhay fever, the classical allergicrhinitis, is reported to be 15.7% in astudy of 1062 secondary schoolstudents.1 In the United States, it isestimated that one in five personssuffers from allergic rhinitis2'3 and 3percent of all medical consultationsare for management of patients withnasal symptoms. Currently 30 to 40million Americans suffer from nasalcongestion, sneezing and runny noseand this prevalence is escalating
both in the USA4 and Europeancountries.5'6
Rhinitis, rhinosinusitis andclassification
The mucosa of the nose is incontinuity with that of the paranasalsinuses. In all forms of rhinitis,some degree of inflammation is alsopresent in the paranasal sinuses. It isoften difficult to differentiate rhinitisfrom sinusitis clinically. As a result,some physicians prefer to use theterm rhinosinusitis instead of rhinitis
or sinusitis.7 However, isolatedrhinitis and sinusitis, for examples inus i t i s due to odontogen icinfection, do exist.
Simple rhinitis may be acute orc h r o n i c . C h r o n i c disease i sarbitrarily defined as a persistence ofsymptoms for more than 12 weeks.7
By aetiology, rh in i t i s can be ofinfective or non-infective in origin.The commonest acute i n f ec t i ver h i n i t i s i s common cold v i rusinfection. Patients with non-infectiverhinitis belong to one of the twogroups. Those related to atopy may
* Address for correspondence: Dr Ho Wai-kuen, Department of Surgery, the University of Hong Kong Medical Centre, Queen Mary Hospital, Hong Kong.
319

Update on Management of Rhinitis
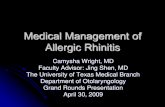
be sensi t ive to a l lergens such asp o l l e n s , h o u s e d u s t m i t e(Dermatophagoides species) (Figure1), animal dander, or food. Thesecond group inc ludes the non-allergic related disease entities suchas vasomotor rhini t is .
C l i n i c a l f ea tures anddifferential diagnosis
Rhinorrhoea, nasal blockage,itchiness and sneezing are cardinalsymptoms of rhinitis. Other commoncomplaints include hyposmia, post-nasal dripping, headache and facialpain. F requen t ly pat ients haveophthalmic symptoms such as eyeitchiness and epiphora as well.
The clue to the diagnosis ofa l l e r g i c r h i n i t i s i n c l u d e s t h eidentification of a specific triggersuch as a contact with cats, or onsetof symptoms after a t r i p to thecountryside. A consistent pattern ofseasonal a t tack of symptoms issuggestive of hay fever, whi le astrong personal or family history ofasthma or eczema contributes to thediagnosis. With the warm and humidclimate in Hong Kong, house dustmites, mould and air pollutants arethe likely causes of nasal allergy.Patients with definite disease entitiessuch as the aspirin hypersensitivity-asthma-nasal polyposis (ASA) triad;p r i m a r y c i l i a r y d y s k i n e s i a a n dKartagener syndrome, two diseasesdue to congen i t a l nasal c i l i a ryabnormality, also present initially aspersistent rhinit is . The ASA triadcan be diagnosed from the historyand physical examination but nasalmucosa c i l iary problems have to bediagnosed by electron microscopy.
In patients with non-al lergicrhinitis, non-specific stimuli such asi n h a l a t i o n of co ld , dry air oringestion of spicy food w i l l triggeran attack. Female pat ients oftenexperience an increase in severity ofsymptoms during pregnancy as aresult of hormonal changes.
Clinical assessment starts withanterior and posterior rhinoscopy,
Figure 1: House dust mite
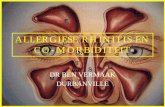
otological evaluation and a completehead and neck examination. Thepresence of anatomical abnormalitiessuch as enlarged turbinates, septald e f o r m i t i e s a n d n a s a l p o l y p s(Figure 2) should be recorded. Thepresence of thick mucus or frank pussignifies sinusitis.
Many diseases have symptomsand signs s imi l a r to rh inos inus i t i s
Figure 2: Endoscopic view of right nasal polyp
(Continued on page 322)
320

Update on Management of Rhinitis
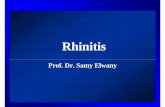
(Table 1). These include Wegener'sgranulomatos is , fungal infect ion(Figure 3), inverted papilloma of thenose (Figure 4 ) and n o t a b l ynasopharyngeal carcinoma (Figure
5) in southern Chinese. Most nasaldiseases can now be diagnosed withr i g i d ( F i g u r e 6 ) o r f l e x i b l en a s o e n d o s c o p y . X - r a y of theparanasal sinus is used for screening,
Mechanical factorsal septum
s, rhinoliths
Figure 3: Coronal CT scan of a patient with leukaemia andfungal sinusitis. (Note the loss of the right inferiorturbinate bone as a result of necrosis)
but a detailed examination of thenose and sinuses would need acomputer i sed tomography (CT)s c a n n i n g . A n a b n o r m a l r ena lf u n c t i o n test w i t h shadows ofg r a n u l o m a on chest x - ray maysuggest the possibility of Wegener'sgranulomatosis in a patient withchronic rhinosinusitis. Specialrequest for culture of nasal dischargefor mycobacterium and fungi, e.g.aspergillus, is required for immuno-compromised pa t ien ts who havea t y p i c a l n a s a l s y m p t o m s .Serological test for antibody againstEpstein-Barr virus is widely used forthe screening of nasopharyngealcancer. However, a nasal biopsy isrequired for the definitive diagnosisof neoplastic diseases.
Complications
In children, uncontrolled rhinitisis associated with snoring and sleepdis turbances which may lead todeterioration of school performanceand impairment of learning ability.8
The medical complications ofr h i n i t i s are acute and chron icsinusit is . Acute sinusitis typicallyo c c u r s a f t e r a s e v e r e u p p e rrespiratory tract infec t ion whichleaves the patient with a persistentye l lowish nasal discharge. Theremay be pain in the nose, tendernessover s i nus area and pe r s i s t en tsystemic symptoms such as fever andmalaise. Examination of the nosemay reveal inflammed nasal mucosawith yellowish purulent discharge.Acute maxillary sinusitis is relativelycommon in young adults, whereasacute frontal sinusitis occurs morefrequent ly in older children and
322

Hong Kong Practitioner 20 (6) June 1998
Figure 4: Inverted papilloma of the nose
Figure 5: Nasopharyngeal carcinoma in the right fossa ofRosenmuller
Figure 6: Rigid nasoendoscopes with light cable
teenagers. Acute ethmoidal sinusitisremains the commonest s inusi t isassociated with orbital complicationsin chi ldren. Early diagnosis andt r e a t m e n t of acute s i n u s i t i s ise s s e n t i a l t o p r e v e n t f u r t h e rcomplications of orbital cellulitis orsubperiosteal abscess (Figure 7).
The symptoms and s i g n s ofchronic sinusitis are less dramatic.There is usually a history of chronicrh in i t i s with or wi thout a l lergy.There may be long-standing purulentnasal discharge, nasal obstruction,hyposmia, recurrent facial pain andheadache. The patient often has hadrepeated episodes of increasing nasald i scharge w h i c h on ly respondpartially to antibiotics, and he is notcompletely well in between attacks.Examina t ion of the nose showscongested mucosa with thick nasaldischarge. Par t icu la r a t t e n t i o nshould be paid to the middle meatuswhere changes may indicate diseasesin the sinuses. Pus may be foundflowing into the nasopharynx. Inchi ldren, the presence of chronicinfection in the tonsils and adenoidss h o u l d be no ted . U n i l a t e r a lm a x i l l a r y s i n u s i t i s (Figure 8)occurring for the first time in adultlife may suggest that the infection isof dental origin. Besides causingchronic ill-health and persistentdiscomfort, chronic sinusitis carriesd e f i n i t e r i s k s o f o r b i t a l andintracranial complications.
Plain paranasal sinus x-rays helpto confirm the clinical suspicion ofacute or chronic maxillary or frontals i n u s i t i s (Figures 8 and 9).However, to define the extent ofinvolvement, CT of the sinuses in thecoronal plane is necessary. It canalso ident i fy the presence of any
323

Update on Management of Rhinitis
UPDATE ARTICLE
anatomical abnormalities which maya f f e c t t h e p l a n o f s u r g i c a lintervention. A simple nasal swabfor culture may reveal the causativeorganism and guide the choice ofantibiotics, but a more def in i t iveidentification may need a swab takenfrom the middle meatus or through amaxillary antral puncture.
Management of rhinitis
In patients with symptoms andsigns of hypersensitivity, an allergicwork-up should be performed. Thisincludes blood eosinophil count, totalserum IgE, skin prick test (Figure10) or specific serum IgE assay.Nasal p rovoca t ion test can beperformed in a specialist's clinicwhen a d e f i n i t i v e d i agnos i s isrequired before immunotherapy. Inthe simplest form of investigation,avoidance of a specific food for aperiod of time may give a clue tofood allergy.
Figure 7: P a t i e n t w i t horbital cellulitis
l e f t
Figure 8: X-ray occipito-mental view: right maxillarysinusitis with opaque right maxillary antrum
Figure 9: X-ray showing air-fluid level in the right frontalsinus
Figure 10: Skin prick test
324

Hong Kong Practitioner 20 (6) June 1998
UPDATE ARTICLE
For patients with c o n f i r m e dallergy, it is logical and important toavoid the allergen. Pillows and bedsshould be covered by plastic bagsand changed at least weekly. Hotwater should be used for washing.Stuffed toys should be removed ormachine-washed frequently. Indoorcarpeting is not advisable and petsshould not be kept. Indoor humidityshould be kept below 40%. Cigarettefumes should be avoided.
In general, oral antihistamine ise f f e c t i v e for the symptoms ofsneezing and itchiness in allergicrhinitis. Unfortunately the classicala n t i h i s t a m i n e s , s u c h a schlorpheniramine, tripolidine, carrythe side-effects of drowsiness anddry m o u t h . The newer a n t i -histamines, loratadine, astemizole,cetirizine, fexofenadine, do not crossthe blood-brain barrier and havemuch lower incidence of centralnervous system side-effects and theirtherapeutic actions last longer. Ingeneral, they can be taken regularlydu r ing seasons of at tack or ondemand bas is in pa t ients wi thi n f r e q u e n t s y m p t o m s . T h eexperience with the new topical nasala n t i h i s t a m i n e s i s l i m i t e d .Theoretically, these topical agentsshould have minimal systemic ab-sorption and infrequent side-effects.The effect of their long-term use,however, needs further evaluation.
For patients with non-allergicvasomotor rhinitis, the rhinorrhoeamay only respond to antihistamineswith prominent an t i - cho l ine rg i caction. Patients wi th s ignif icantnasal blockage usually do not have agood response to antihistamines.Systemic deconges t an t may be
added. Local decongestant nosedrops should not be used for patientswith chronic nasal disease to avoidthe r i sk of d e v e l o p i n g r h i n i t i smedicamentosa (rebound conges-tion). For systemic decongestants,p r e c a u t i o n m u s t be t aken inpaediatric patients and in those withheart diseases and hypertension.
For pa t i en t s w i th f r e q u e n tattacks, topical nasal steroids areve ry e f f e c t i v e i n c o n t r o l l i n gsymptoms.9 Local steroids haveminimal systemic absorption and noeffect of adrenal suppress ion orgrowth retardation when used inrecommended dosages.10,11 In arecent Canadian study of elderlypatients, there is an increased risk ofocular hypertension in those takinghigh dose inha led s teroids forasthma.12 Although this risk is notassociated with nasal steroid spray,the dosage should be kept at therecommended level to avoid possiblecomplication.
Topical disodium cromoglycateacts by i n h i b i t i o n of mast cel lh i s tamine release. However, itsadministration has to precede theallergen challenge, and a 4 or 6 timesdaily administration is required. It isalso not very effective in alleviatingnasal blockage. All these factorslimit its use in patients with allergicrhinitis.
Nasal discharge is the result ofstimulation by acetylcholine releasedby the parasympathet ic nervoussystem. Antihistamines with anti-cholinergic action, however, haveside-effects such as dry mouth ,c o n s t i p a t i o n and d i f f i c u l t y i nurination, especially in elderly male
patients. They may be used only inse lec ted i n d i v i d u a l s . Topicala n t i c h o l i n e r g i c d r u g s u c h a sipratropium bromide can reduce thesecretion from nasal mucosal glandsand would benefit patients withsignificant rhinorrhoea.
W i t h t h e f i n d i n g o finflammation being important in thepathogenesis of rhinosinusitis, recentresearch has been directed towardsthe m o d i f i c a t i o n of c y t o k i n eac t i v i t i e s in the i n f l a m m a t o r ypathway. The use of leukotrien'em o d i f y i n g agents is now underclinical trial.
I n p a t i e n t s w i t h s e v e r es y m p t o m s , d e s e n s i t i s a t i o nprogramme or immunotherapy can beoffered for those with a specifical lergen. This involves weeklyinjections of the allergen to thepatient for a long period which maylast for years. Good result has beenreported particularly in patients withhay fever. This is popular in theUnited States while most patients inHong Kong prefer oral or topicalmedications.
For most patients, symptomsrelated to rhinitis can be controlledwith medical therapy alone. Whenthe symptoms are contr ibuted bys t r u c t u r a l a b n o r m a l i t i e s , e.g.hypertrophic turbinates and deviatednasal septum, surgical operationss u c h a s t u r b i n e c t o m i e s a n dseptoplasty may relieve the problemof nasal blockage. For pat ientscomplicated with chronic sinusitis, acombination of drug treatment andm i n i m a l l y i n v a s i v e f u n c t i o n a le n d o s c o p i c s i n u s s u r g e r y i srequired." •
325

Update on Management of Rhinitis
UPDATE ARTICLE
Rhinitis is becoming more common in Hong Kong. Proper management requires:
1. accurate diagnosis of different types of rhinitis, and differentiation it from other diseases of the nose;
2. alert on the possible complications of sinusitis and orbital or intracranial infections;
3. appropriate drug treatment;
4. environmental control; and
5. occasional surgical intervention.
References
Leung R, Ho P. Asthma, allergy and atopy in
three South-east Asian populations. Thorax.1994;49(12):1205-1210.Smith HM. Epidemiology and natural historyof asthma, allergic rhinitis, and atopic dermatitis
(eczema). Allergy: Principles and Practice. 3rded. St Louis. Mo: CV Mosby Co; 1988:891-929.
Naclerio RM. Allergic rhinitis. N Engl J HMed. 1991;325:860-869.Hagy GW, Settipane GA. Risk factors for thedevelopment of asthma and allergies rhinit is :a 7-year follow-up of college students. J AllergyClin Immunol 1976;58:330.
Aberg N. Asthma and al lergic r h i n i t i s in
Swedish conscripts. Clin Exp Allergy 1989; 19:
59-63.
Ninan TK, Russell G. Respiratory symptoms
and atopy in Aberdeen schoolchildren: evidence
from two surveys 25 years apart. BMJ 1992;
304:873-875.
Clement PAR, Bluestone CD, F Gordts.
Management of rhinosinusitis in children. Arch
Otolaryngol Head Neck Surg, 1998;124:31-34.
Simons FER. Learning impairment and allergic
rhinitis. Allergy and Asthma Proc, 1996;17:
185-189.
Svensson C, Klementsson H, Andersson M, et
al. Glucocorticoid-induced attenuation of
m u c o s a l e x u d a t i o n o f f i b r i n o g e n and
12.
b r a d y k i n i n s i n seasonal a l le rg ic r h i n i t i s .
Allergy 1994;49:177-183.Pipkorn U, Pukander J, Suonpaa J, et al.Long-term safety of budesonide nasal aerosal:
a 5.5 year follow-up study. Clin Allergy 1988;18:253-259.Mol le r C, Ek L, Svensson IL. Nasa lbudesonide to children for 5 years.Allergy Clin Immunol News 1994;6(Suppl 2):427.
Garbe E, LeLorier J, Boivin JF, et al. Inhaledand nasal glucocorticoids and the risks of ocularhypertension or open-angle glaucoma. JAMA1997:277:722-727.Kennedy DW. Prognostic factors, outcomes andstaging in ethmoid sinus surgery. Laryngoscope
1992:102(12 Pt 2 Suppl 57):1-18.
326





![Diagnosis and Management of Rhinitis: Complete Guidelines ... · different forms of rhinitis (allergic, non-allergic, occupational rhinitis, hormonal rhinitis [pregnancy and hypothyroidism],](https://static.fdocuments.in/doc/165x107/5d61f07588c993197b8b51b8/diagnosis-and-management-of-rhinitis-complete-guidelines-different-forms.jpg)