
Non-Allergic Rhinitis and Asthma - worldallergy.org Rhinitis... · RHINITIS Non-allergic...
45
Non-Allergic Rhinitis and Asthma Glenis Scadding Royal National Throat Nose &Ear Hospital London
-
Upload
vuongthien -
Category
Documents
-
view
248 -
download
0
Transcript of Non-Allergic Rhinitis and Asthma - worldallergy.org Rhinitis... · RHINITIS Non-allergic...
Non-Allergic Rhinitis and Asthma
Glenis Scadding
Royal National Throat Nose &Ear Hospital
London
Disclosures
�Research funds:
ALK-Abello, GSK ,
�Advisory Boards:
ALK-Abello, Allergen Therapeutics, GSK, Merck, Uriach, USB
�Speaker/Chair:
ALK-Abello, GSK , Merck, Uriach
Learning Objectives
�Classification & phenotypes NAR
�Co-morbid asthma association- or lack of it
� (Diagnosis and treatment of NAR-see www.bsaci.org)
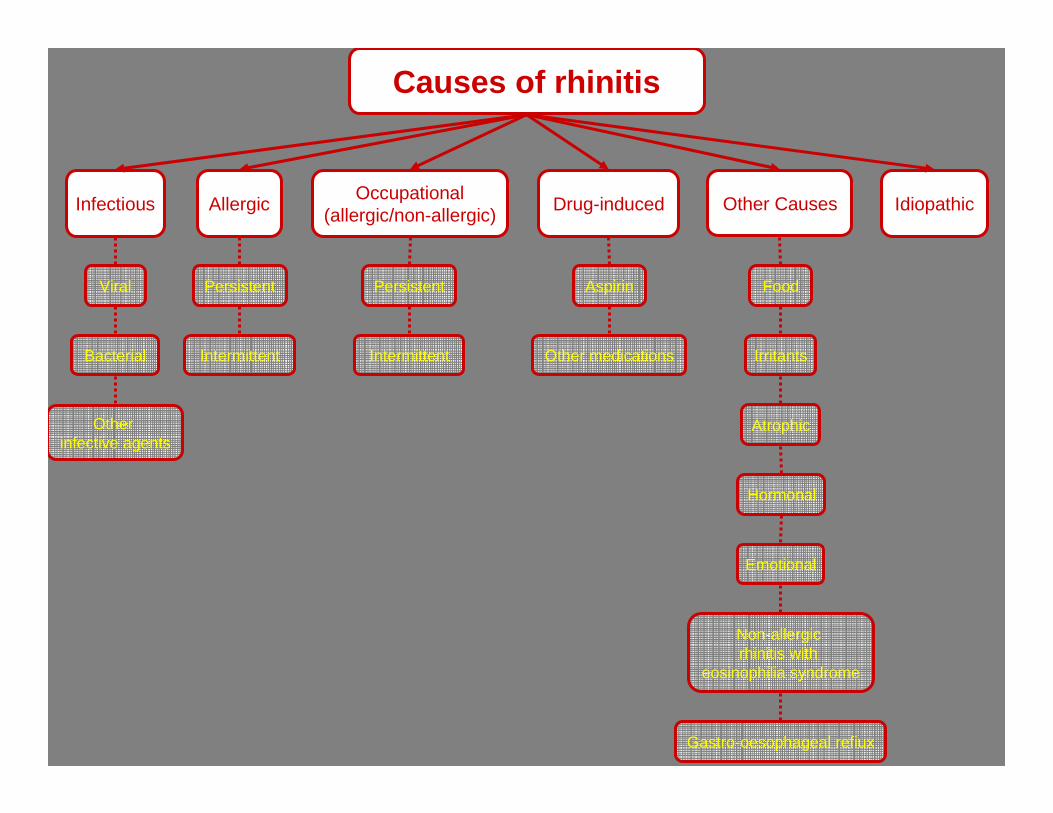
Causes of rhinitis
Aspirin
Other medications
Viral
Bacterial
Non-allergic rhinitis with
eosinophilia syndrome
Irritants
Food
Emotional
Other infective agents
Atrophic
Gastro-oesophageal refiux
Persistent
Intermittent Intermittent
Persistent
Infectious AllergicOccupational
(allergic/non-allergic)Drug-induced Other Causes Idiopathic
Hormonal
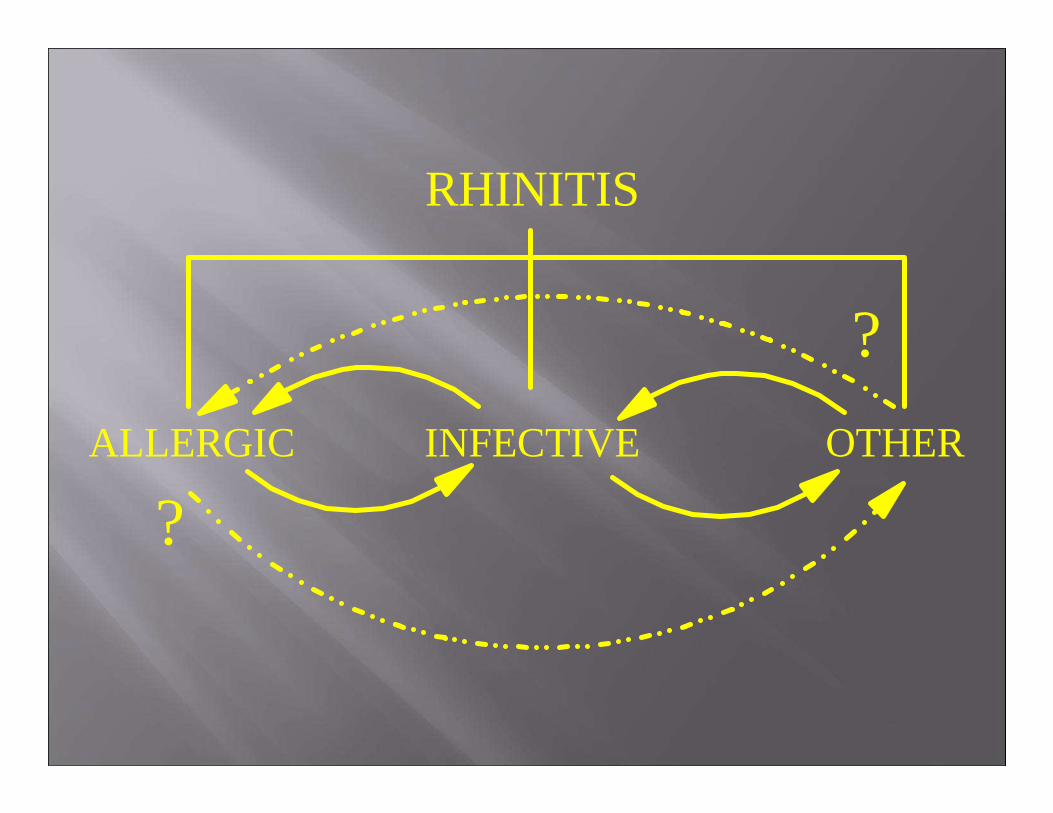
RHINITIS
ALLERGIC INFECTIVE OTHER
?
?
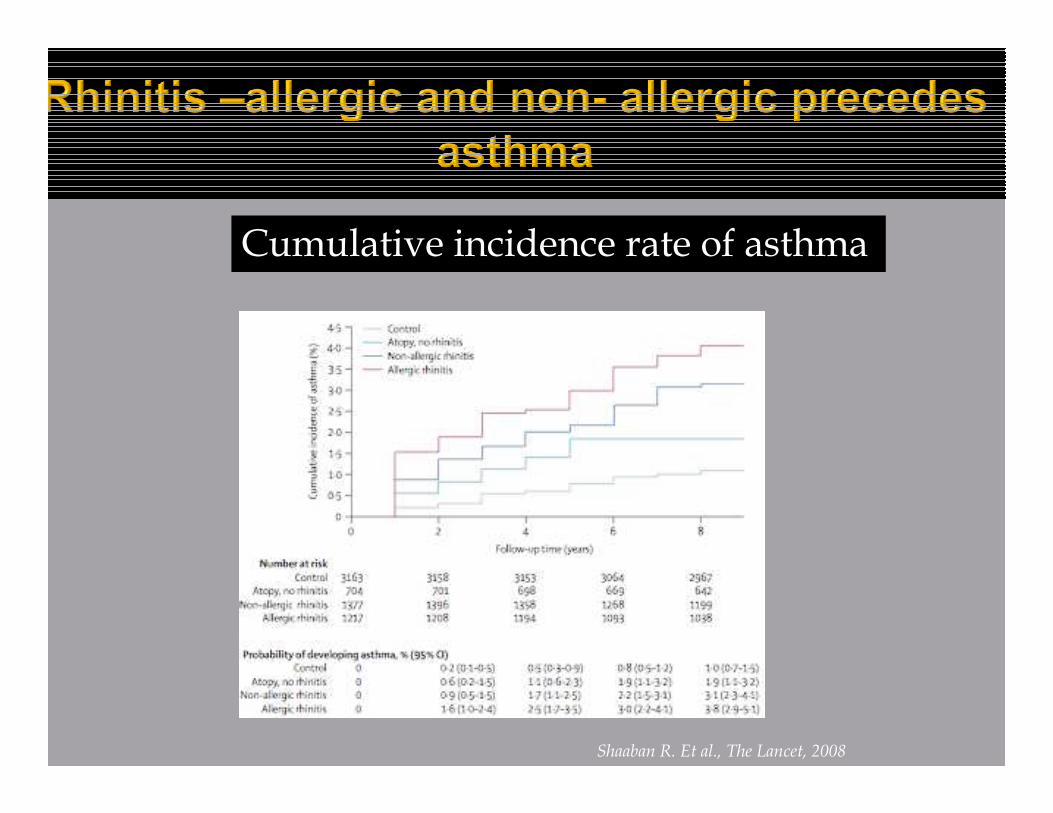
Cumulative incidence rate of asthma
Shaaban R. Et al., The Lancet, 2008
Non-allergic global AW disease
PROBLEMS
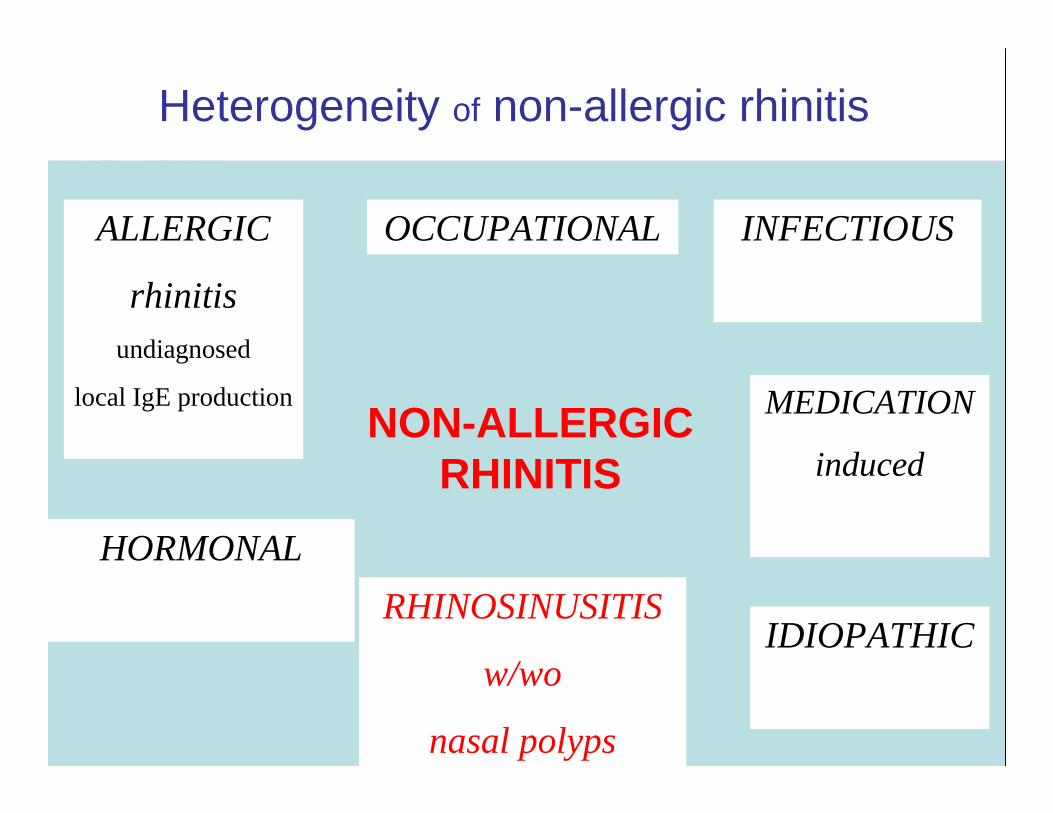
heterogeneity of non-allergic rhinitis
rhinitis - rhinosinusitis
NON-ALLERGIC
RHINITIS
ASTHMA
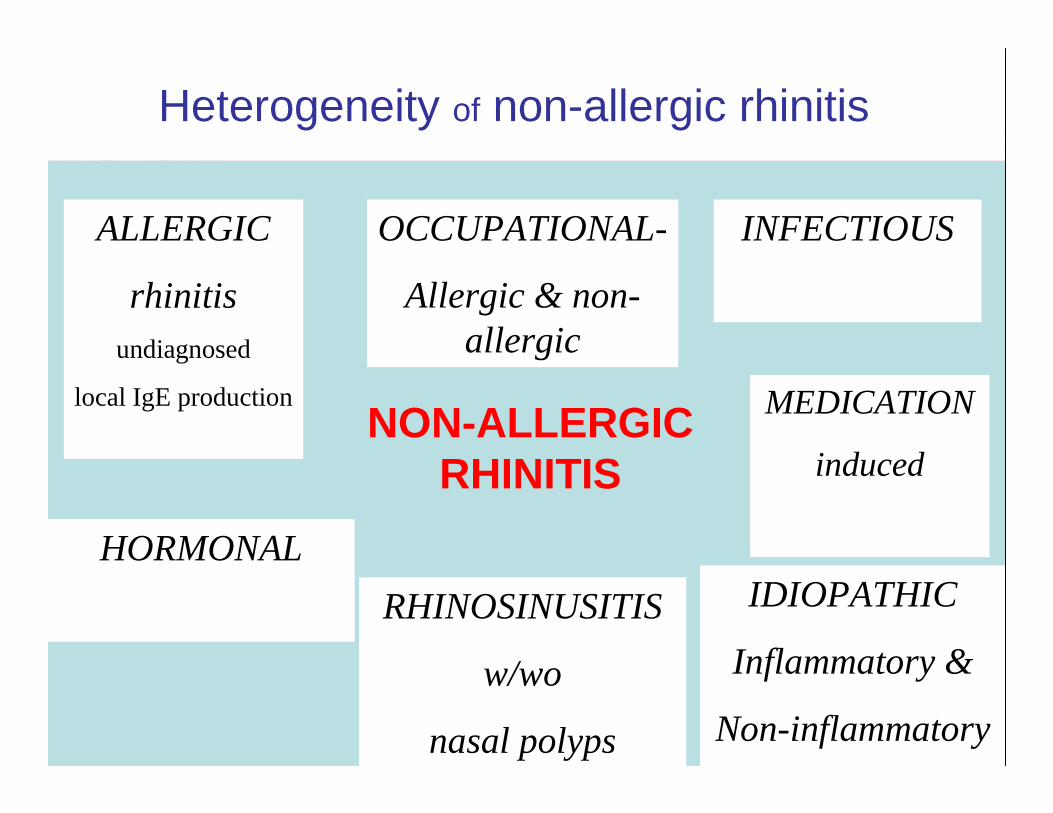
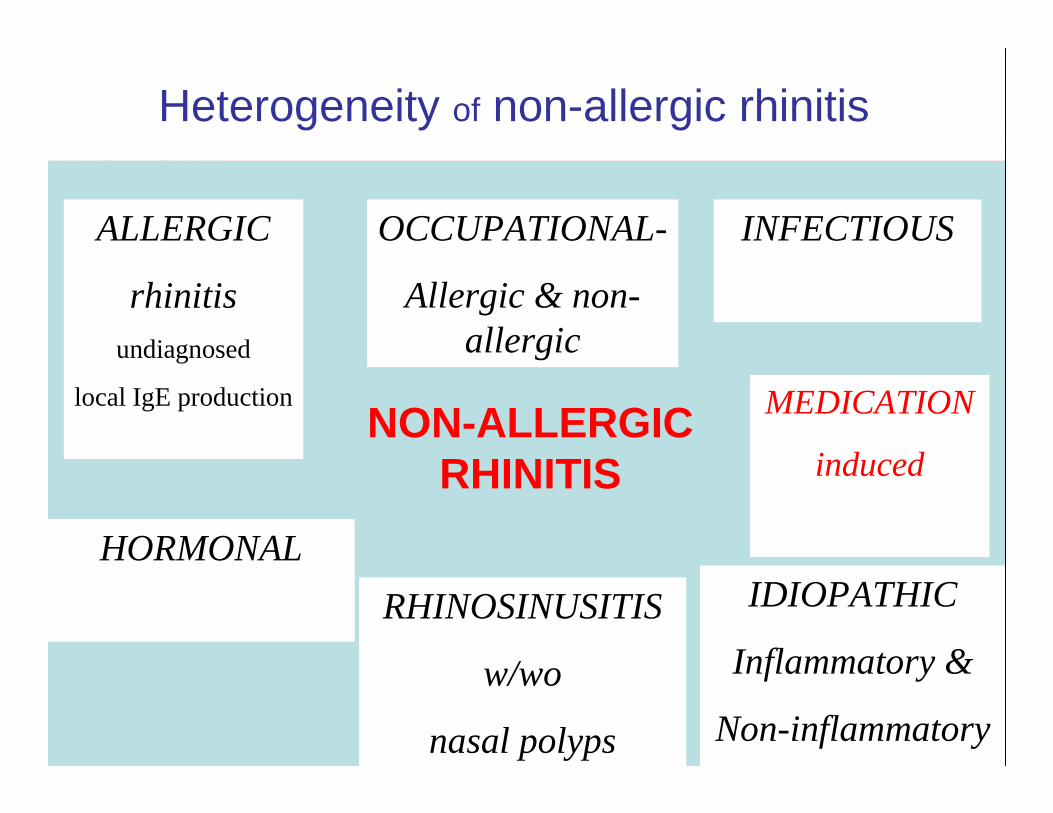
Heterogeneity of non-allergic rhinitis
ALLERGIC
rhinitisundiagnosed
local IgE production
OCCUPATIONAL-
Allergic & non-allergic
HORMONAL
INFECTIOUS
IDIOPATHIC
Inflammatory &
Non-inflammatory
RHINOSINUSITIS
w/wo
nasal polyps
MEDICATION
inducedNON-ALLERGIC
RHINITIS
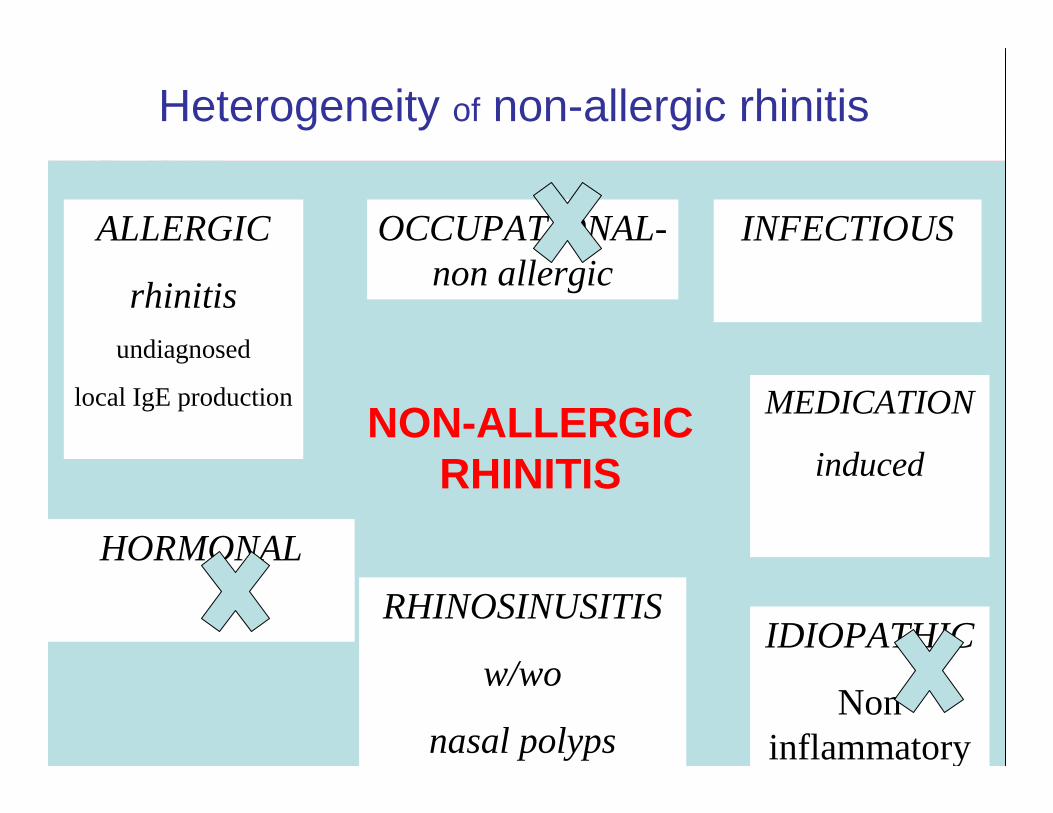
Heterogeneity of non-allergic rhinitis
ALLERGIC
rhinitisundiagnosed
local IgE production
OCCUPATIONAL-non allergic
HORMONAL
INFECTIOUS
IDIOPATHIC
Non inflammatory
RHINOSINUSITIS
w/wo
nasal polyps
MEDICATION
inducedNON-ALLERGIC
RHINITIS
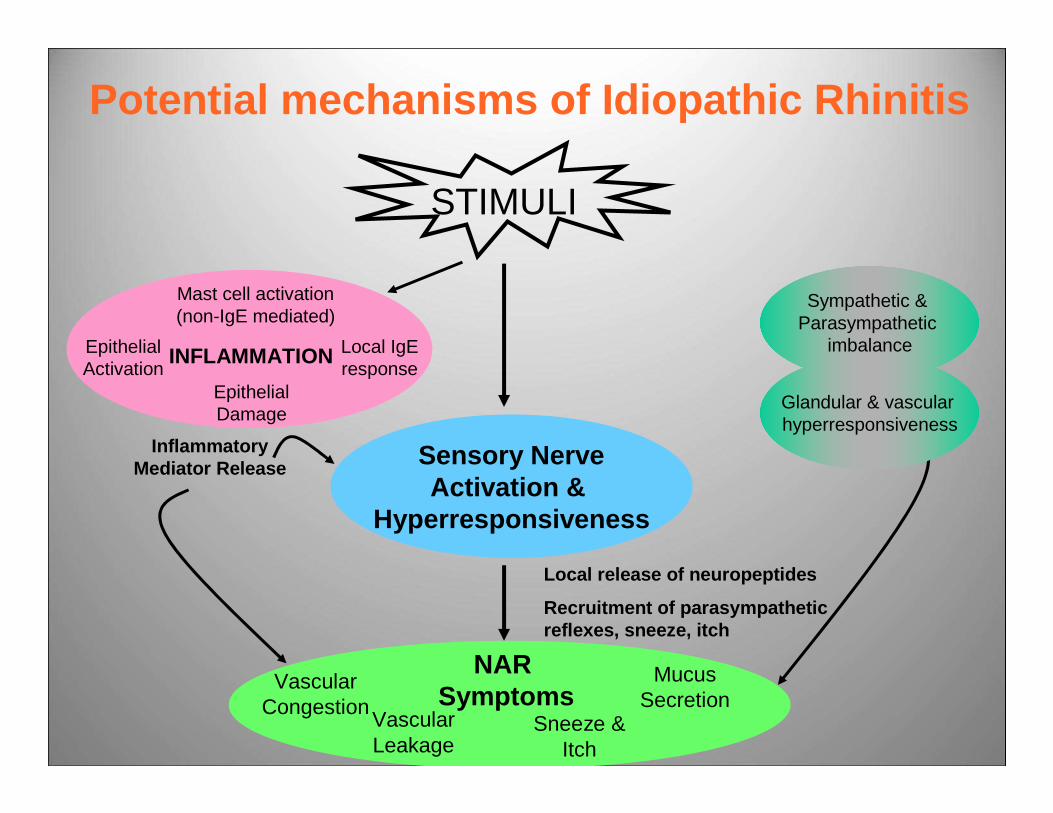
Potential mechanisms of Idiopathic Rhinitis
NAR Symptoms
Inflammatory Mediator Release
STIMULI
Sensory NerveActivation &
Hyperresponsiveness
Local release of neuropeptides
Recruitment of parasympathetic reflexes, sneeze, itch
Vascular Congestion
Mucus Secretion
Vascular Leakage
Sneeze & Itch
INFLAMMATIONEpithelial Activation
Mast cell activation (non-IgE mediated)
Epithelial Damage
Local IgE response
Sympathetic & Parasympathetic
imbalance
Glandular & vascular hyperresponsiveness
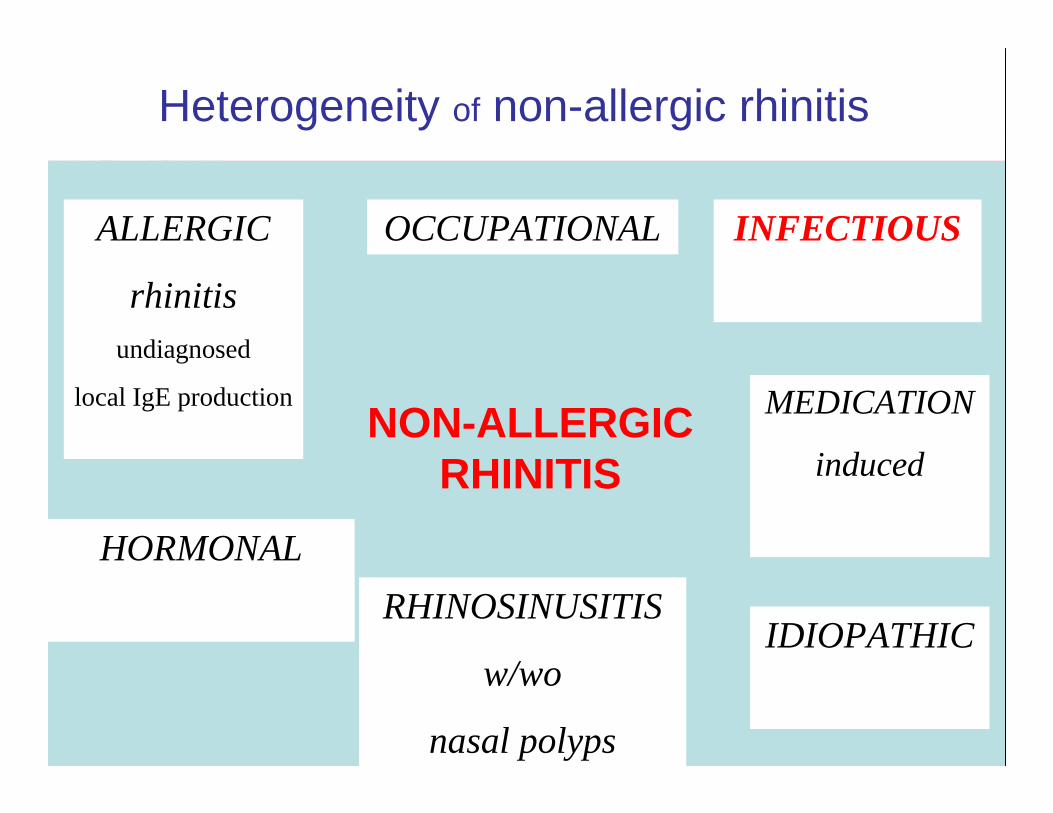
Heterogeneity of non-allergic rhinitis
ALLERGIC
rhinitisundiagnosed
local IgE production
OCCUPATIONAL
HORMONAL
INFECTIOUS
IDIOPATHICRHINOSINUSITIS
w/wo
nasal polyps
MEDICATION
inducedNON-ALLERGIC
RHINITIS
UUU
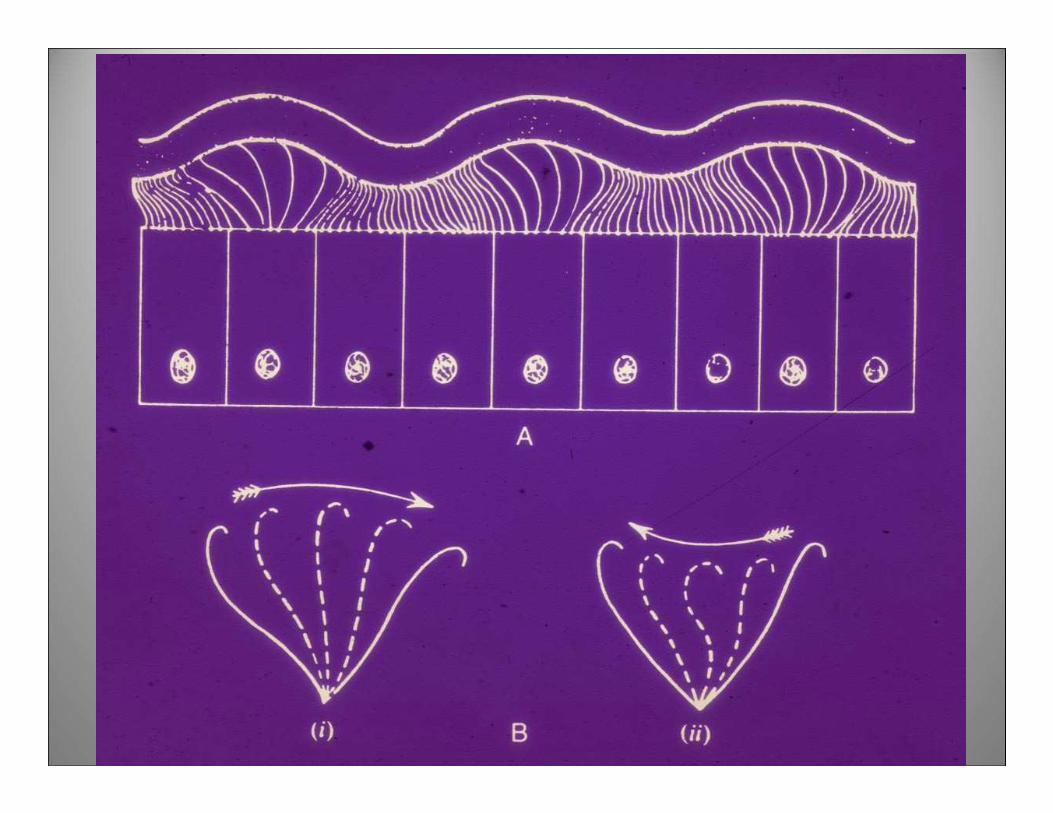
Physiologiccircumstances
Protection
air filteringair conditioning
air humidification
Physiologiccircumstances
Protection
air filteringair conditioning
air humidification
Nasaldisease
Trigger
TRIGGER SYNERGY IN ASTHMA
• AllergenIncreased BHR-most allergens stay in nose.
• Infection - viral rhinitis causes BHR Rhinovirus present in nose in asthma exacerbations.
• Both - synergy• Lemanske et al J. Clin. Invest.1989;83:1-10• Johnstone Pediatr.Pul Suppl.1991;16:88-9• Johnstone AJRCCM1995;152:S46-52.
Heterogeneity of non-allergic rhinitis
ALLERGIC
rhinitisundiagnosed
local IgE production
OCCUPATIONAL
HORMONAL
INFECTIOUS
IDIOPATHIC
inflammatory
RHINOSINUSITIS
w/wo
nasal polyps
MEDICATION
inducedNON-ALLERGIC
RHINITIS
Global Airway Disease
NON-ALLERGIC RHINITIS WITH EOSINOPHILS
ASTHMA
FACTS
similar pathophysiology
mucosal IgE
risk factor
?progression to AERD
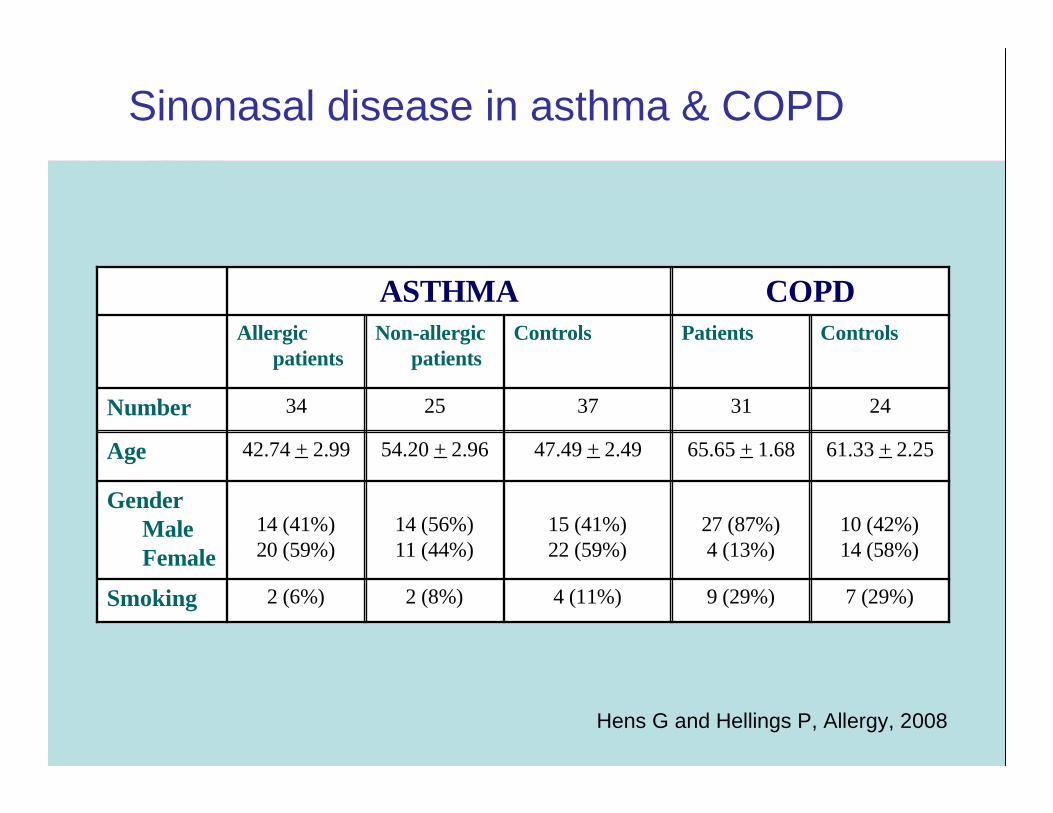
Sinonasal disease in asthma & COPD
7 (29%)9 (29%)4 (11%)2 (8%)2 (6%)Smoking
10 (42%)14 (58%)
27 (87%)4 (13%)
15 (41%)22 (59%)
14 (56%)11 (44%)
14 (41%)20 (59%)
Gender Male Female
61.33 + 2.2565.65 + 1.6847.49 + 2.4954.20 + 2.9642.74 + 2.99Age
2431372534Number
ControlsPatientsControlsNon-allergicpatients
Allergicpatients
COPDASTHMA
Hens G and Hellings P, Allergy, 2008
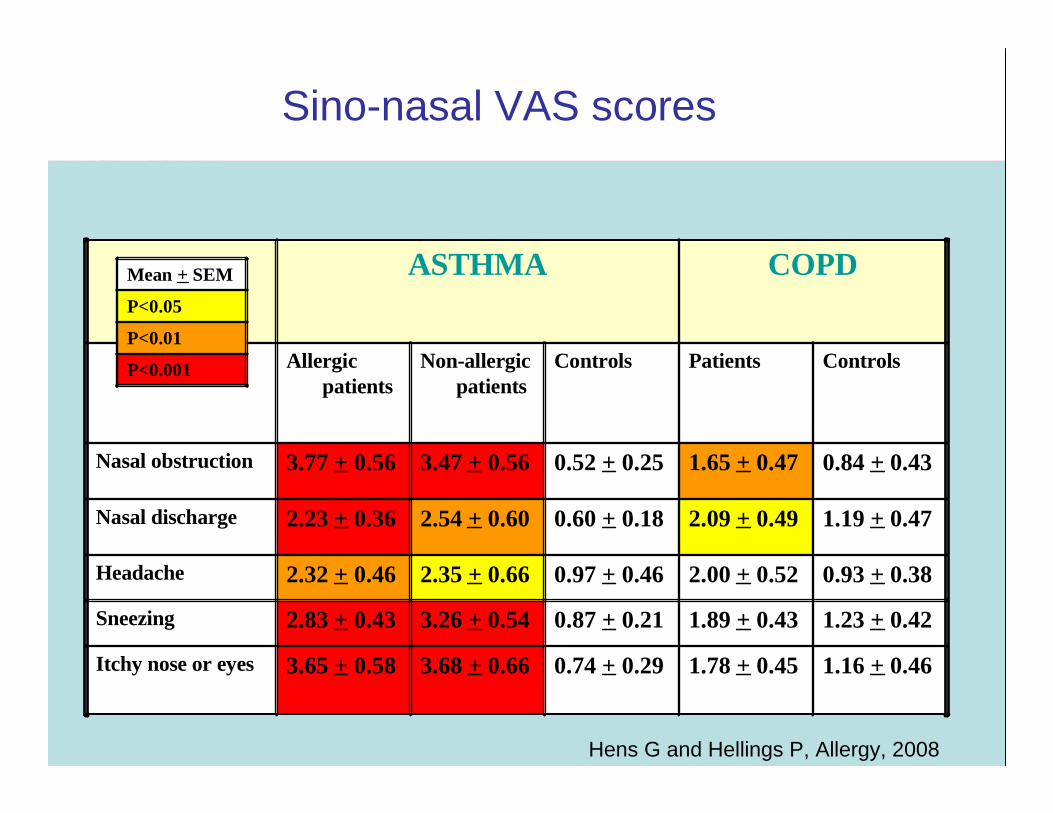
Sino-nasal VAS scores
Hens G and Hellings P, Allergy, 2008
1.16 + 0.461.78 + 0.450.74 + 0.293.68 + 0.663.65 + 0.58Itchy nose or eyes
1.23 + 0.421.89 + 0.430.87 + 0.213.26 + 0.542.83 + 0.43Sneezing
0.93 + 0.382.00 + 0.520.97 + 0.462.35 + 0.662.32 + 0.46Headache
1.19 + 0.472.09 + 0.490.60 + 0.182.54 + 0.602.23 + 0.36Nasal discharge
0.84 + 0.431.65 + 0.470.52 + 0.253.47 + 0.563.77 + 0.56Nasal obstruction
ControlsPatientsControlsNon-allergicpatients
Allergicpatients
COPDASTHMA
P<0.001
P<0.01
P<0.05
Mean + SEM
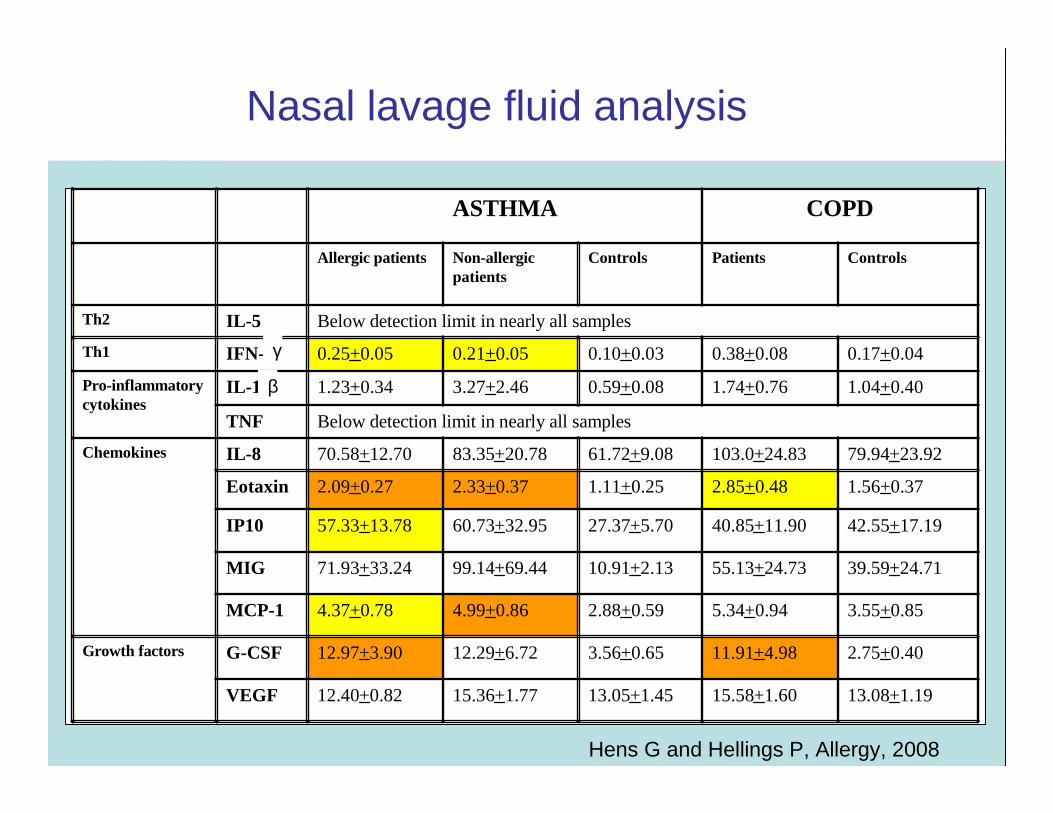
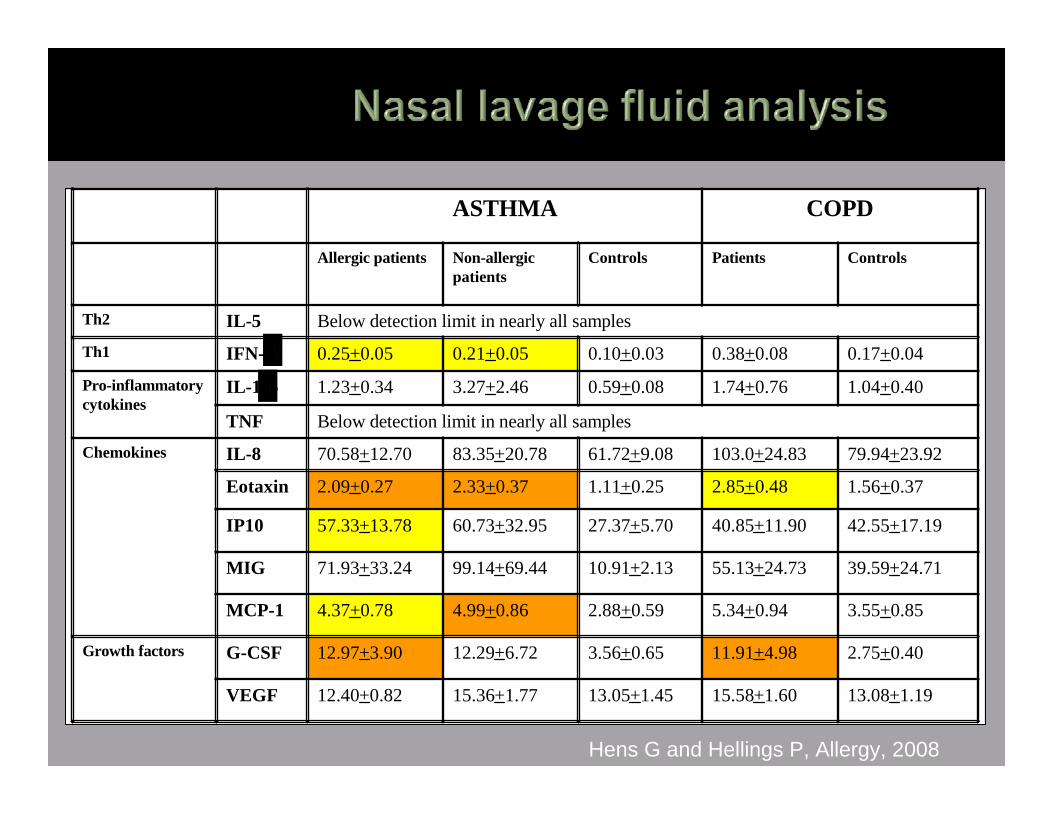
Nasal lavage fluid analysis
Hens G and Hellings P, Allergy, 2008
13.08+1.1915.58+1.6013.05+1.4515.36+1.7712.40+0.82VEGF
2.75+0.4011.91+4.983.56+0.6512.29+6.7212.97+3.90G-CSFGrowth factors
3.55+0.855.34+0.942.88+0.594.99+0.864.37+0.78MCP-1
39.59+24.7155.13+24.7310.91+2.1399.14+69.4471.93+33.24MIG
42.55+17.1940.85+11.9027.37+5.7060.73+32.9557.33+13.78IP10
1.56+0.372.85+0.481.11+0.252.33+0.372.09+0.27Eotaxin
79.94+23.92103.0+24.8361.72+9.0883.35+20.7870.58+12.70IL-8Chemokines
Below detection limit in nearly all samplesTNF
1.04+0.401.74+0.760.59+0.083.27+2.461.23+0.34IL-1Pro-inflammatorycytokines
0.17+0.040.38+0.080.10+0.030.21+0.050.25+0.05IFN-Th1
Below detection limit in nearly all samplesIL-5Th2
ControlsPatientsControlsNon-allergicpatients
Allergic patients
COPDASTHMA
γ
β
Heterogeneity of non-allergic rhinitis
ALLERGIC
rhinitisundiagnosed
local IgE production
OCCUPATIONAL
HORMONAL
INFECTIOUS
IDIOPATHICRHINOSINUSITIS
w/wo
nasal polyps
MEDICATION
inducedNON-ALLERGIC
RHINITIS
Heterogeneity of non-allergic rhinitis
ALLERGIC
rhinitisundiagnosed
local IgE production
OCCUPATIONAL-
Allergic & non-allergic
HORMONAL
INFECTIOUS
IDIOPATHIC
Inflammatory &
Non-inflammatory
RHINOSINUSITIS
w/wo
nasal polyps
MEDICATION
inducedNON-ALLERGIC
RHINITIS
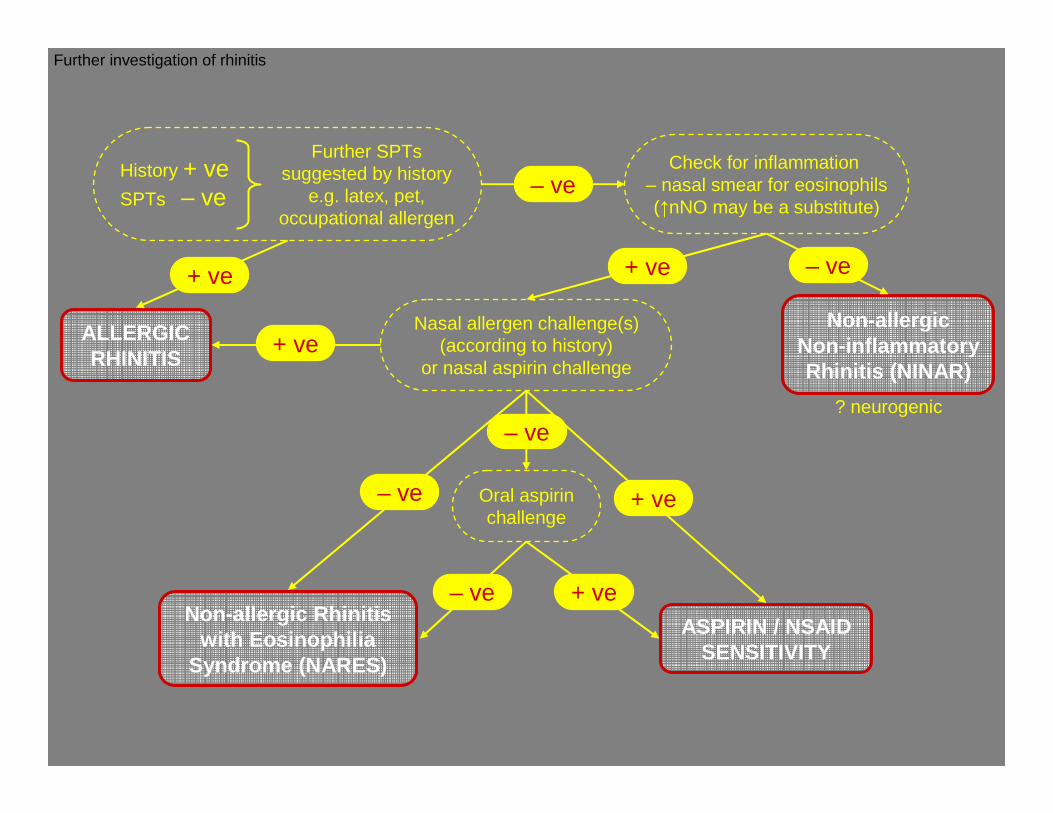
ALLERGICRHINITIS
Non-allergicNon-inflammatoryRhinitis (NINAR)
? neurogenic
Non-allergic Rhinitis with Eosinophilia
Syndrome (NARES)
Oral aspirinchallenge
Nasal allergen challenge(s)(according to history)
or nasal aspirin challenge
History + veSPTs – ve
Further SPTs suggested by history
e.g. latex, pet, occupational allergen
ASPIRIN / NSAIDSENSITIVITY
Check for inflammation – nasal smear for eosinophils(↑nNO may be a substitute)
+ ve
– ve
– ve
– ve+ ve+ ve
+ ve
+ ve– ve
– ve
Further investigation of rhinitis
Asthma
Nasal polyps
Aspirin hypersensitivity }First First
described described by Widal by Widal (1922)(1922)
1.AETIOLOGY & PATHOGENESIS
Site of disease onset
Availability for investigation
2. CLINICAL RELEVANCE
Need for treatment
Diagnosis-safest test for
aspirin sensitivity
Specific treatment-” desensitization”
� Persistent rhinitis, onset 29.7+- 12.5 years
then asthma, aspirin intolerance, nasal polyposis
� Earlier and more severe in females
� Atopics (1 in 3 ) earlier rhinitis and asthma
� ? Viral induction of disease
� Szczeklik A et al Eur. Respir. J 2000, 16, 432-6.
AIANE network-data from 500 patients from 16 centres in 10 European countries
Sequential pattern emerged:
Normal population
0.6-2.5%
Perennial Rhinitis 6%
Asthma-21% adult
onset
CRS & Nasal polyps 30-
40%Varga et al ,1994
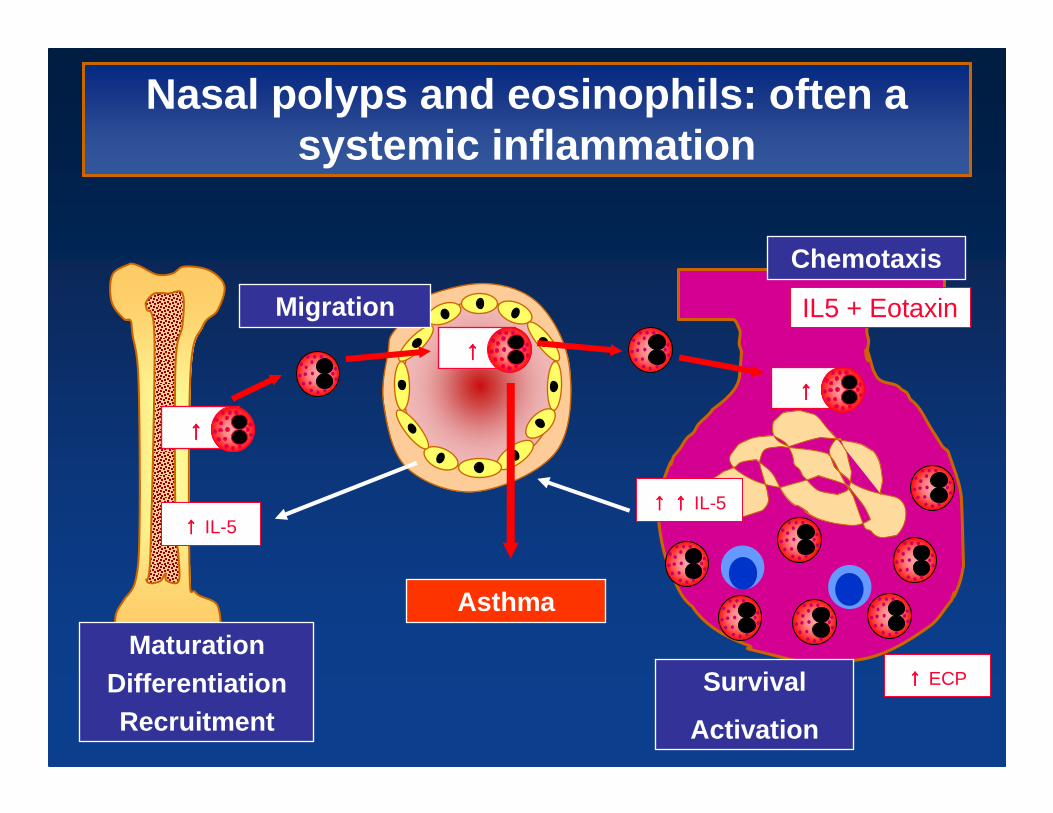
Nasal polyps and eosinophils: often a systemic inflammation
↑↑↑↑ ECP
↑↑↑↑ ↑↑↑↑ IL-5↑↑↑↑ IL-5
↑↑↑↑ ↑↑↑↑↑↑↑↑ ↑↑↑↑
↑↑↑↑ ↑↑↑↑Migration
Survival
Activation
MaturationDifferentiationRecruitment
IL5 + Eotaxin
Chemotaxis
Asthma
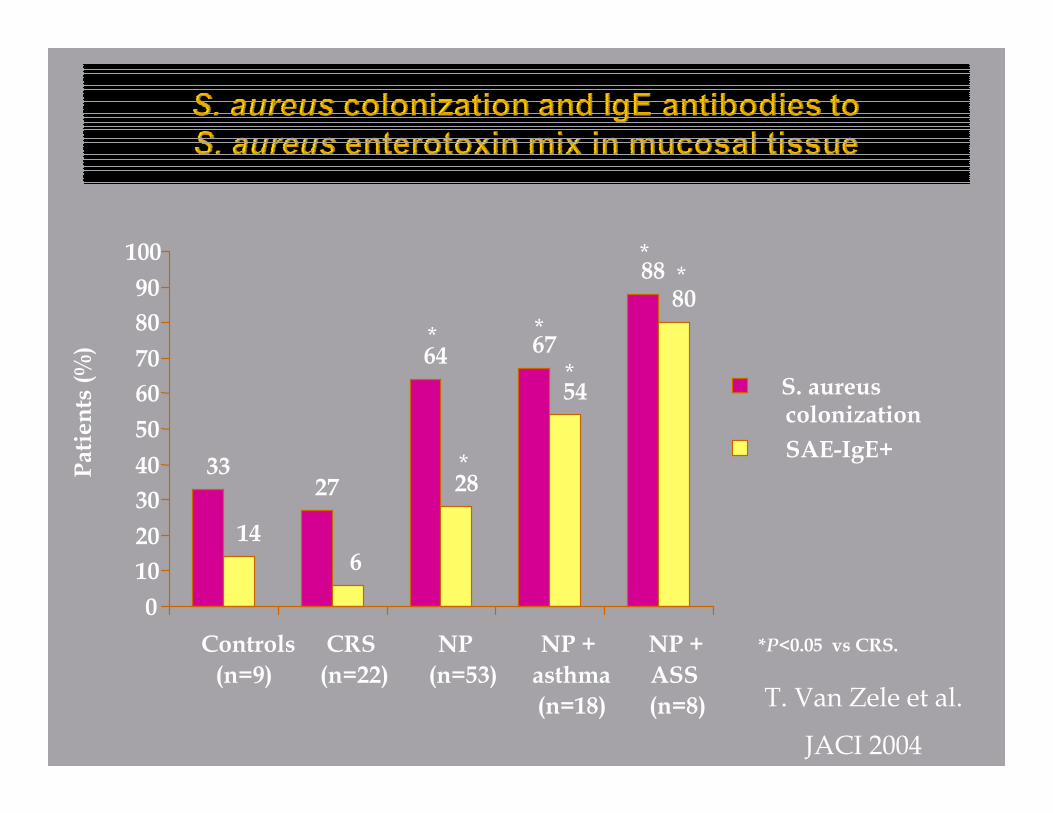
3327
64 67
88
146
28
54
80
0
10
20
30
40
50
60
70
80
90
100
Controls
(n=9)
CRS
(n=22)
NP
(n=53)
NP +
asthma
(n=18)
NP +
ASS
(n=8)
Patients (%)
S. aureuscolonization
SAE-IgE+
*
*
*
*
**
*P<0.05 vs CRS.
T. Van Zele et al.
JACI 2004
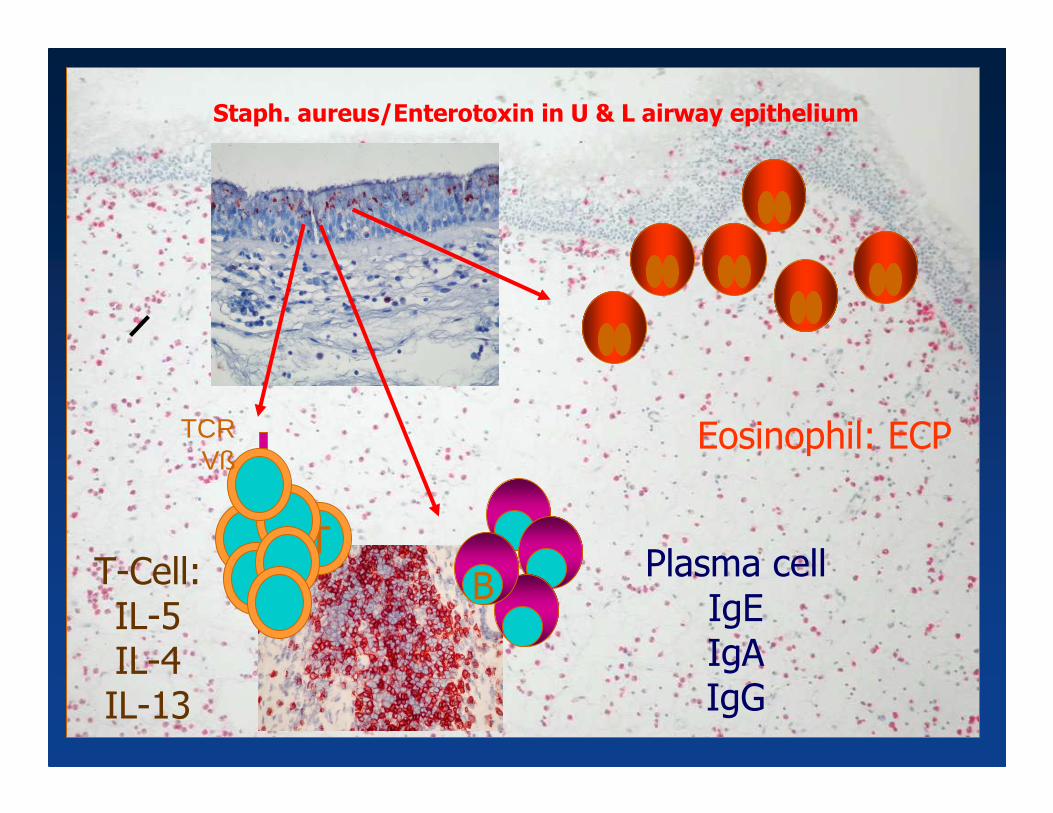
Staph. aureus/Enterotoxin in U & L airway epithelium
T
B
TCRVß
Eosinophil: ECP
Plasma cellIgEIgAIgG
T-Cell:IL-5IL-4IL-13
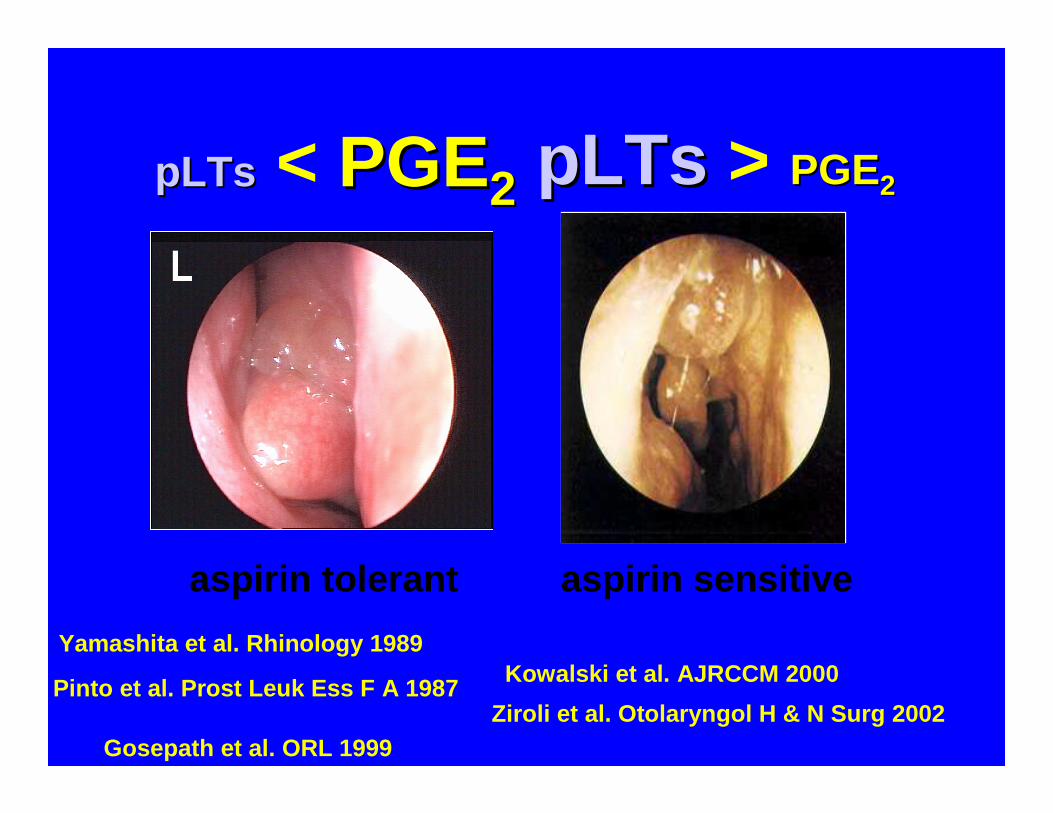
aspirin sensitiveaspirin tolerant
pLTspLTs < PGEPGE22 pLTs pLTs > PGEPGE22
Gosepath et al. ORL 1999
Yamashita et al. Rhinology 1989
Ziroli et al. Otolaryngol H & N Surg 2002
Kowalski et al. AJRCCM 2000Pinto et al. Prost Leuk Ess F A 1987
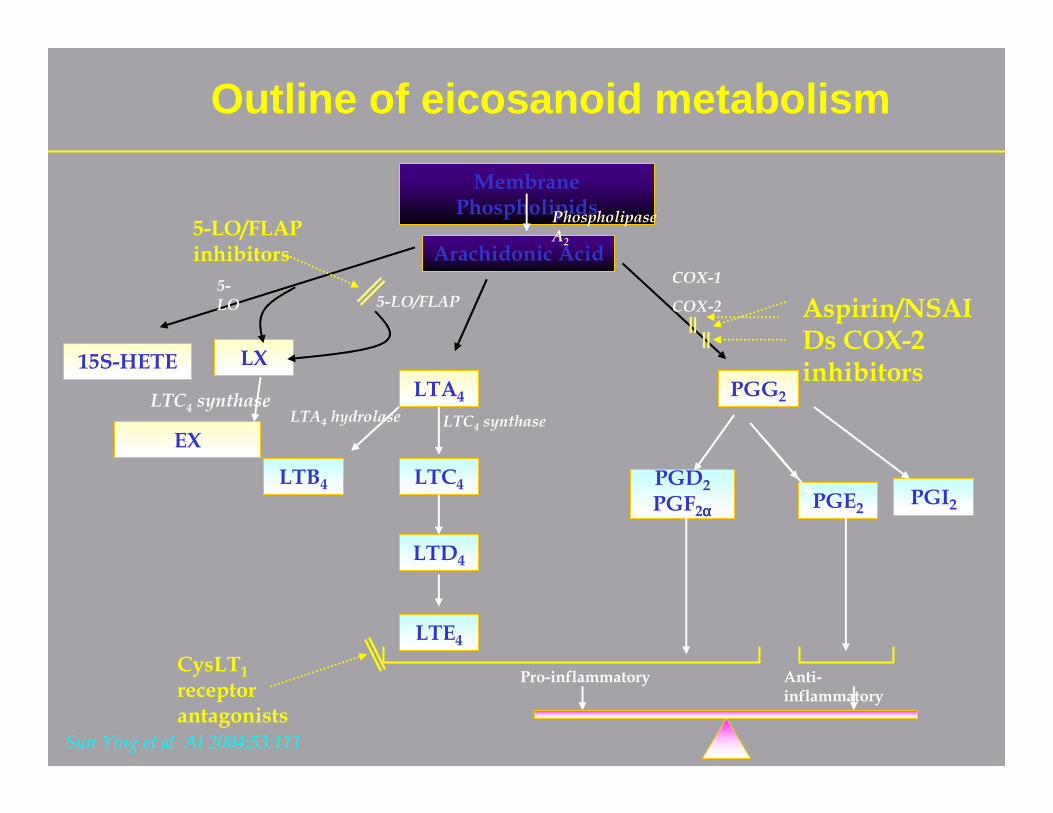
Membrane Phospholipids
Arachidonic Acid
15S-HETE LX
LTA4 PGG2
LTB4 LTC4
LTD4
LTE4
PGE2PGI2
PGD2
PGF2αααα
Pro-inflammatory Anti-inflammatory
LTC4 synthaseLTA4 hydrolase
Phospholipase A2
CysLT1
receptor antagonists
5-LO/FLAP inhibitors
Aspirin/NSAIDs COX-2 inhibitors
5-LO/FLAP5-LO
COX-1
COX-2
Sun Ying et al AI 2004;53:111
Outline of eicosanoid metabolism
EX
LTC4 synthase
Hens G and Hellings P, Allergy, 2008
13.08+1.1915.58+1.6013.05+1.4515.36+1.7712.40+0.82VEGF
2.75+0.4011.91+4.983.56+0.6512.29+6.7212.97+3.90G-CSFGrowth factors
3.55+0.855.34+0.942.88+0.594.99+0.864.37+0.78MCP-1
39.59+24.7155.13+24.7310.91+2.1399.14+69.4471.93+33.24MIG
42.55+17.1940.85+11.9027.37+5.7060.73+32.9557.33+13.78IP10
1.56+0.372.85+0.481.11+0.252.33+0.372.09+0.27Eotaxin
79.94+23.92103.0+24.8361.72+9.0883.35+20.7870.58+12.70IL-8Chemokines
Below detection limit in nearly all samplesTNF
1.04+0.401.74+0.760.59+0.083.27+2.461.23+0.34IL-1Pro-inflammatorycytokines
0.17+0.040.38+0.080.10+0.030.21+0.050.25+0.05IFN-Th1
Below detection limit in nearly all samplesIL-5Th2
ControlsPatientsControlsNon-allergicpatients
Allergic patients
COPDASTHMA
γ
β
Rhinitis and COPD
Limited information !
Up to 88% of patients with COPD experience nasal symptomsUri N et al., J Laryngol Otol, 2002
Correlation between nasal symptoms and impairment of QOLHurst J et al., Respir Med, 2004
Involvement of upper airways in COPDHens G et al., Allergy, 2008
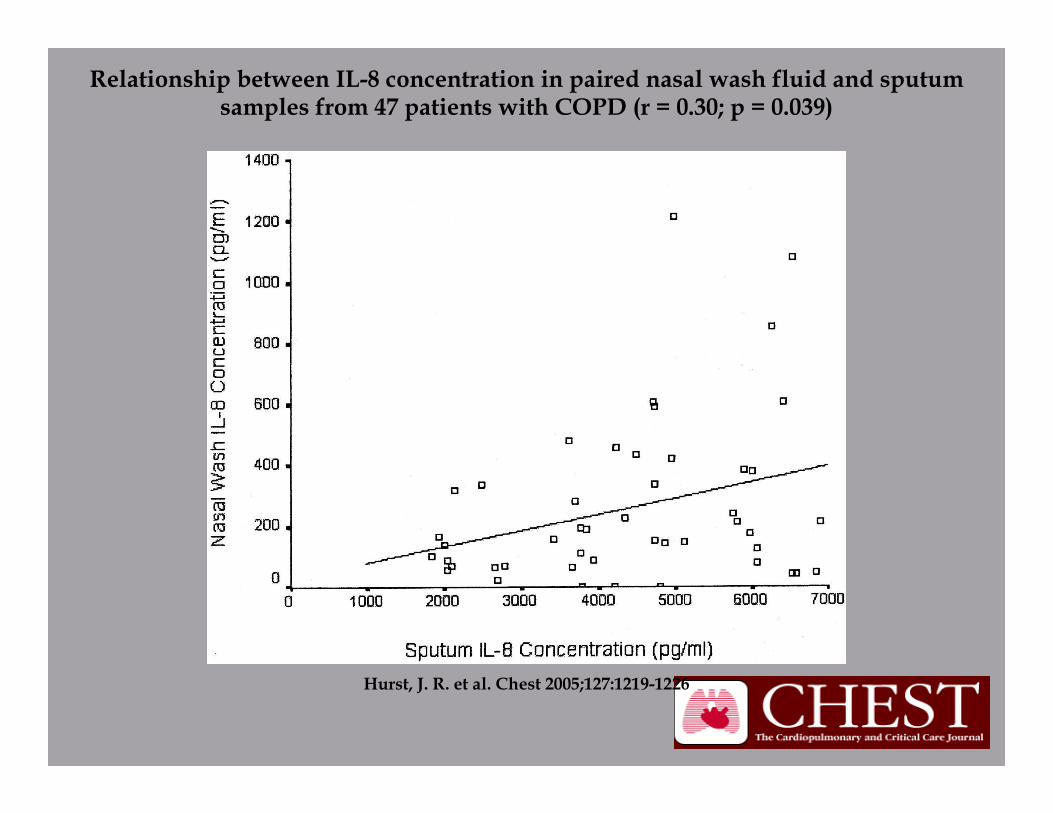
Hurst, J. R. et al. Chest 2005;127:1219-1226
Relationship between IL-8 concentration in paired nasal wash fluid and sputum samples from 47 patients with COPD (r = 0.30; p = 0.039)
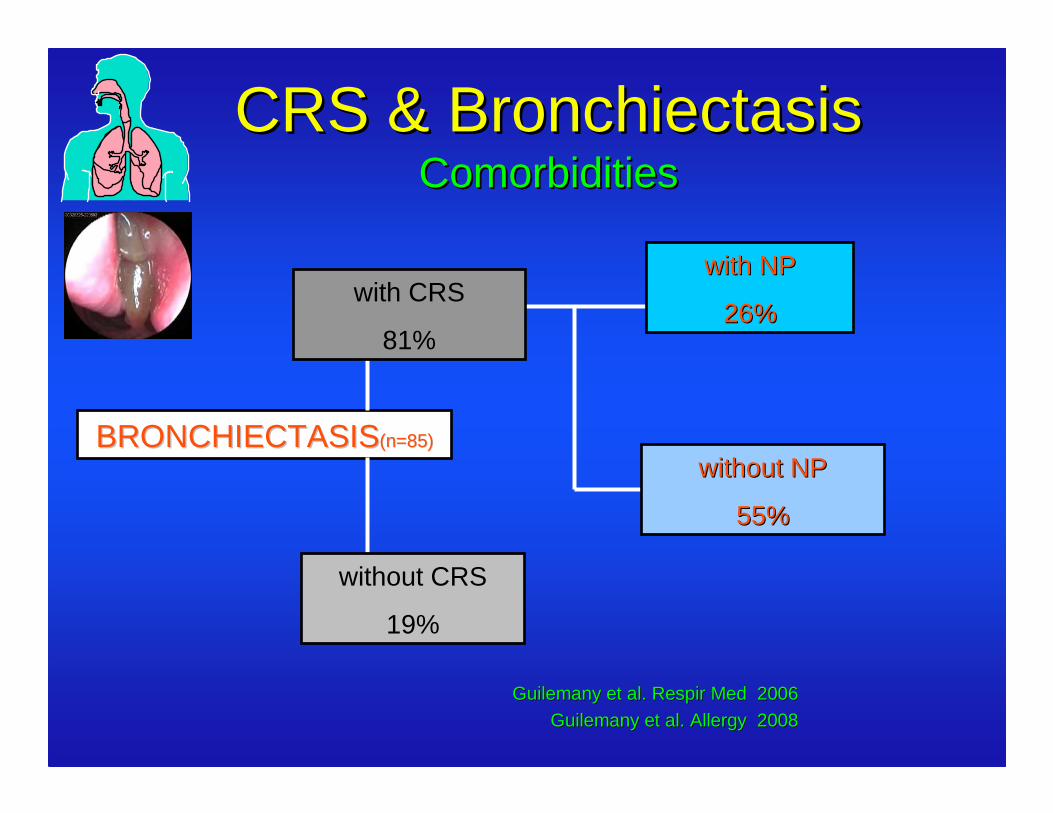
CRS & BronchiectasisCRS & BronchiectasisComorbiditiesComorbidities
BRONCHIECTASISBRONCHIECTASIS(n=85)(n=85)
with NPwith NP
26%26%
without NPwithout NP
55%55%
with CRS
81%
without CRS
19%
Guilemany et al. Guilemany et al. Respir MedRespir Med 20062006
Guilemany et al. Guilemany et al. AllergyAllergy 2008 2008
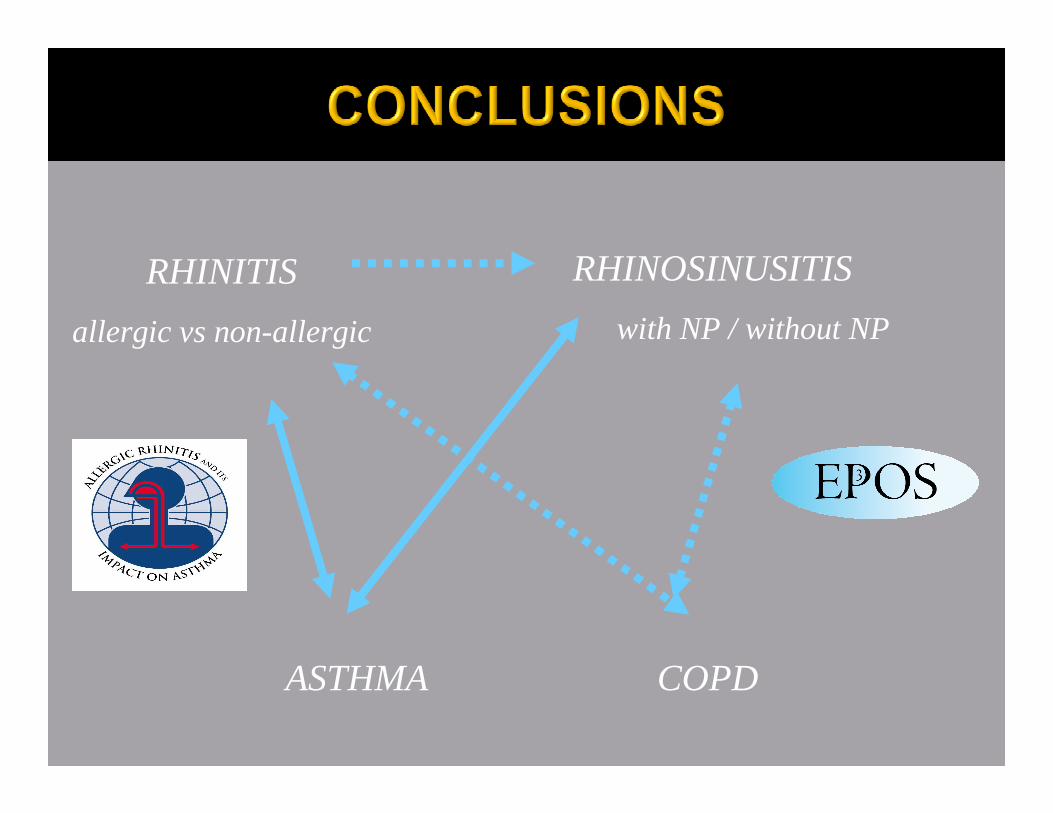
RHINITIS
allergic vs non-allergic
ASTHMA COPD
RHINOSINUSITIS
with NP / without NP
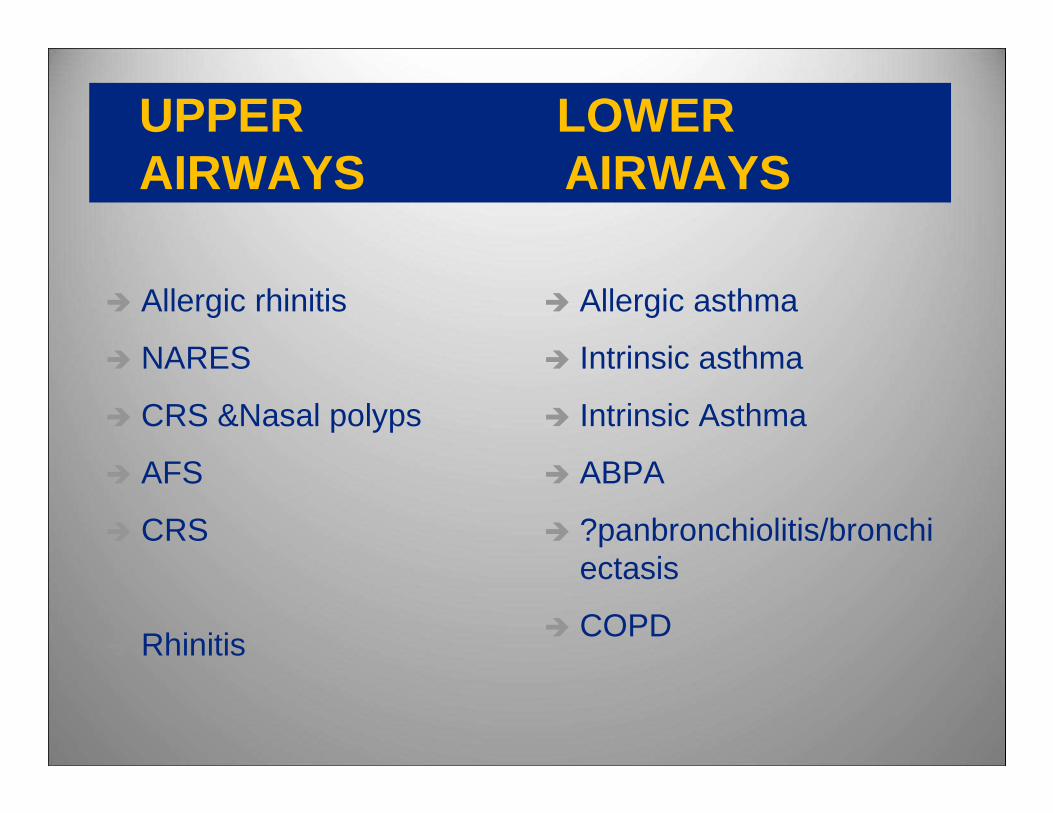
UPPER LOWER AIRWAYS AIRWAYS
� Allergic rhinitis
� NARES
� CRS &Nasal polyps
� AFS
� CRS
� Rhinitis
� Allergic asthma
� Intrinsic asthma
� Intrinsic Asthma
� ABPA
� ?panbronchiolitis/bronchiectasis
� COPD
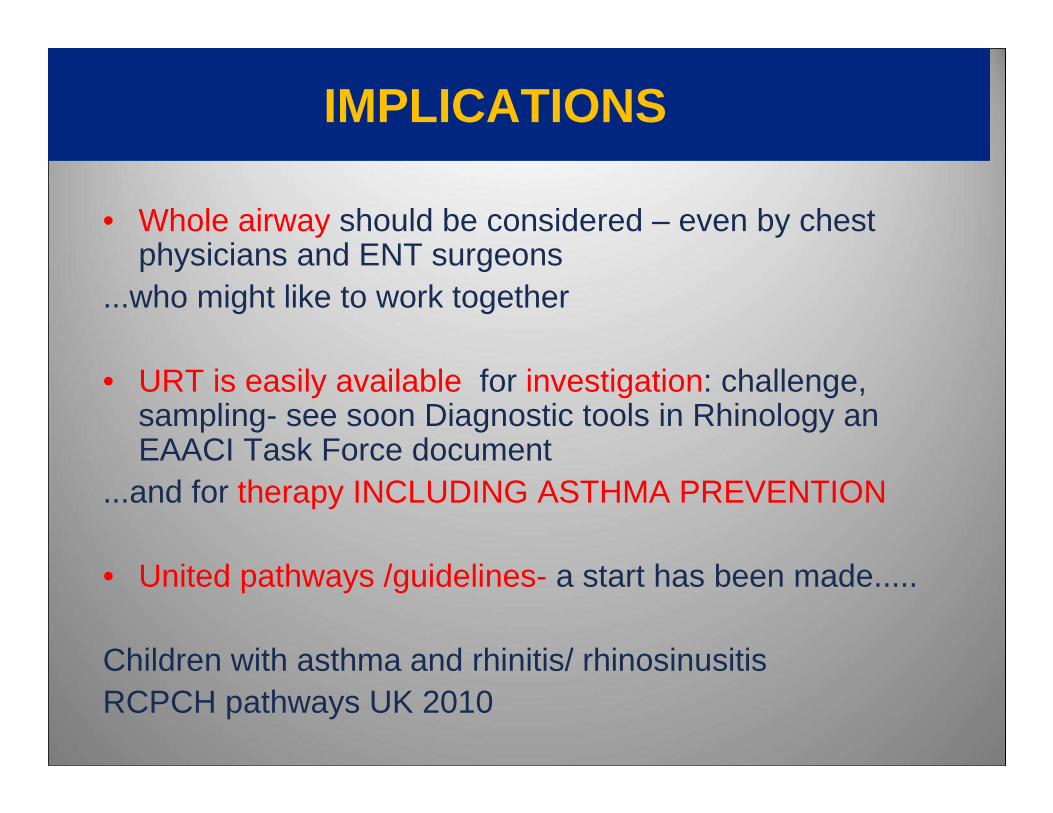
IMPLICATIONS
• Whole airway should be considered – even by chest physicians and ENT surgeons
...who might like to work together
• URT is easily available for investigation: challenge, sampling- see soon Diagnostic tools in Rhinology an EAACI Task Force document
...and for therapy INCLUDING ASTHMA PREVENTION
• United pathways /guidelines- a start has been made.....
Children with asthma and rhinitis/ rhinosinusitisRCPCH pathways UK 2010
ACKNOWLEDGEMENTS
Ideas and slides from
Peter Hellings Belgium
Peter Howarth, UK
Claus Bachert,Belgium
Further reading
Further marches: allergic and non-allergic
Scadding GK,CEA 2007.
Airways disease:just nosing around
ScaddingGK & Kariyawasam H Thorax 2009














![Diagnosis and Management of Rhinitis: Complete Guidelines ... · different forms of rhinitis (allergic, non-allergic, occupational rhinitis, hormonal rhinitis [pregnancy and hypothyroidism],](https://static.fdocuments.in/doc/165x107/5d61f07588c993197b8b51b8/diagnosis-and-management-of-rhinitis-complete-guidelines-different-forms.jpg)


