Understanding BMT: Before, During, and After …...Understanding BMT: Before, During, and After...
14
Understanding BMT : Before, During, and After Transplant (BMT 101) Corey Cutler, MD MPH FRCP(C) Associate Professor of Medicine Harvard Medical School Dana-Farber Cancer Institute Boston, MA Definitions • Stem Cell Transplantation (aka BMT) – The transfer of Hematopoietic Stem Cells from Donor to Recipient • What is a Stem Cell? – Stem cells are defined by two characteristics: • They can make copies of themselves, or self-renew • They can differentiate, or develop, into more specialized cells Definitions • Are there different types of Stem Cells? – Embryonic / Pluripotent Stem Cells – Tissue Specific Stem Cells • Hematopoietic Stem Cells – A stem cell capable of giving rise to ALL cells in the blood and immune system 4 Rationale for Transplantation • Elimination AND Replacement of: – Diseased marrow – Poorly functioning marrow – Immune compromised marrow – Metabolically compromised marrow • Protection against ultra-high doses of chemoradiotherapy • Establish immunologic platform for immunotherapy 5 Types of Transplantation Autologous – High doses of chemotherapy and/or radiation – Designed to kill tumor; overcome resistance with dose intensity – Requires stem cell rescue – Not really a transplant Allogeneic – 2 mechanisms to cure: • Immunologic: Donor vs. Host (Graft vs. Tumor) • Chemotherapy and/or radiation Decision to use autologous/allogeneic marrow source is disease, stage and patient specific Indications for Transplantation • Autologous – Multiple Myeloma in remission • Prolongation of remission – Diffuse Large B Cell NHL in 2 nd remission – Hodgkin Disease in remission – Mantle Cell NHL – Some Germ Cell Tumors – AML, in very rare circumstances Curative Intent
Transcript of Understanding BMT: Before, During, and After …...Understanding BMT: Before, During, and After...

Understanding BMT: Before, During,
and After Transplant
(BMT 101)
Corey Cutler, MD MPH FRCP(C)
Associate Professor of MedicineHarvard Medical School
Dana-Farber Cancer Institute
Boston, MA
Definitions
• Stem Cell Transplantation (aka BMT)
– The transfer of Hematopoietic Stem Cells from Donor
to Recipient
• What is a Stem Cell?
– Stem cells are defined by two characteristics:
• They can make copies of themselves, or self-renew
• They can differentiate, or develop, into more
specialized cells
Definitions• Are there different types of Stem Cells?
– Embryonic / Pluripotent Stem Cells
– Tissue Specific Stem Cells
• Hematopoietic Stem Cells – A stem cell capable of
giving rise to ALL cells in the blood and immune system
4
Rationale for Transplantation
• Elimination AND Replacement of:
– Diseased marrow
– Poorly functioning marrow
– Immune compromised marrow
– Metabolically compromised marrow
• Protection against ultra-high doses of chemoradiotherapy
• Establish immunologic platform for immunotherapy
5
Types of Transplantation
Autologous – High doses of chemotherapy and/or radiation
– Designed to kill tumor; overcome resistance with dose intensity
– Requires stem cell rescue
– Not really a transplant
Allogeneic – 2 mechanisms to cure:
• Immunologic: Donor vs. Host (Graft vs. Tumor)
• Chemotherapy and/or radiation
Decision to use autologous/allogeneic marrow source is disease, stage and patient specific
Indications for Transplantation
• Autologous
– Multiple Myeloma in remission
• Prolongation of remission
– Diffuse Large B Cell NHL in 2nd remission
– Hodgkin Disease in remission
– Mantle Cell NHL
– Some Germ Cell Tumors
– AML, in very rare circumstances
Curative Intent
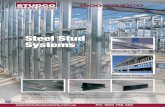
Indications for Transplantation -
Allogeneic
2,000
1,500
500
0
1,000
2,500
Num
ber
of
Tra
nspla
nts
MultipleMyeloma
NHLAML HDALL MDS/
MPD
AplasticAnemia
CML OtherLeuk
OtherCancer
Non-MaligDisease
Related Donor (Total N=3,282)
Unrelated Donor (Total N=3,389)
8
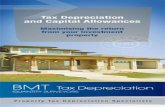
Stem Cell Transplant Decision Tree
Type of Transplant Autologous Allogeneic
Conditioning
Intensity
• High (Myeloablative) • High (Myeloablative)
• Reduced Intensity
9
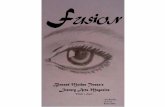
Conditioning Regimen
• Determined by:
– Primary tumor type
– Stage of disease at transplantation
– Graft vs. tumor effect in that disease
– Performance status/comorbidity of recipient
• Large variety of regimens exist
• Differ in intensity and toxicity
– Ablative is Hard; RIC is pretty easy
• We have “Recipes” for these regimens
9
0 2 61 3 4 5
Reduced-intensity conditioning, HLA-identical sibling
(N=232)
0
20
40
60
80
100
10
30
50
70
90
0
20
40
60
80
100
10
30
50
70
90
Myeloablative, HLA-identical sibling (N=318)
Years
Pro
bability o
f Surv
ival
CIBMTR, Age >50, 1998–2006
What is Better? Myeloablative or RIC?
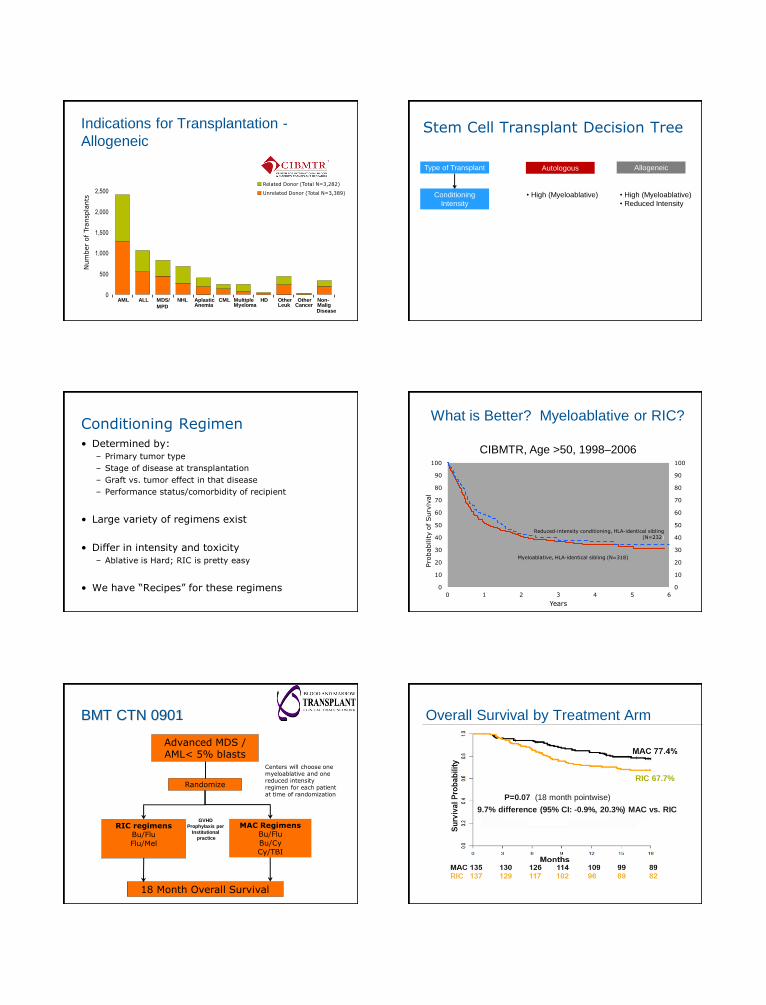
BMT CTN 0901
Advanced MDS /AML< 5% blasts
18 Month Overall Survival
Randomize
RIC regimensBu/Flu
Flu/Mel
MAC RegimensBu/Flu
Bu/CyCy/TBI
GVHD
Prophylaxis per
Institutional
practice
Centers will choose one myeloablative and one reduced intensity regimen for each patient at time of randomization
Overall Survival by Treatment Arm
12
9.7% difference (95% CI: -0.9%, 20.3%) MAC vs. RIC
P=0.07 (18 month pointwise)
RIC 67.7%

MAC 27 25 25 23 22 22 21
RIC 27 26 26 25 23 22 20
108 105 101 91 87 77 68
110 103 91 77 73 67 62
Su
rviv
al
Pro
ba
bilit
y
Months Months
Su
rviv
al
Pro
ba
bilit
y
Overall Survival by Disease Group
13
RIC 85.2%
RIC 63%
14
Stem Cell Transplant Decision Tree
Type of Transplant Autologous Allogeneic
Conditioning
Intensity
• High (Myeloablative) • High (Myeloablative)
• Reduced Intensity
Donor Type • Self • Related
• Unrelated
Degree of Match • Perfect • Matched
• Mismatched
• Highly Mismatched
Finding a Donor
• Goal is to MATCH donor-recipient pairs
– Not a problem in Autologous transplantation
– Identical Twins (Syngeneic Transplantation) not
commonly found nor used
• Matching performed for HLA (Human Leukocyte
Antigen) molecules, encoded by MHC complex
(Major Histocompatibility Complex)
• Matching at non-HLA loci also important, but not
done (yet).
The HLA System
Klein and Sato, NEJM 2000
Histocompatibility Histocompatibility – Unrelated Donors
HLA-A -B -C -DR -DP -DQ
2132 2798 1672 1196 179 158
HLA-A -B -C -DR -DP -DQ
2132 2798 1672 1196 179 158
Nearly Infinite Possible Combinations!!!

19
Courtesy Martin Maiers, NMDP Bioinformatics
“Perfect” Match Rates in the Adult
Donor Registry
20Courtesy Martin Maiers, NMDP Bioinformatics
“Perfect” and “Pretty Good” Match
Rates in the Adult Donor Registry
Does the Degree of Match Matter?
Weisdorf, BBMT 2008 22
Stem Cell Transplant Decision Tree
Type of Transplant Autologous Allogeneic
Conditioning
Intensity
• High (Myeloablative) • High (Myeloablative)
• Reduced Intensity
Donor Type • Self • Related
• Unrelated
Degree of Match
• Bone Marrow
• PBSC
• Bone Marrow
• PBSC
• Umbilical Cord Blood
Stem Cell Source
• Perfect • Matched
• Mismatched
• Highly Mismatched
Stem Cell Source
Bone MarrowPeripheral Blood
Stem Cells
Umbilical Cord
Blood
Ease of Collection Hard Easy Very Easy
Engraftment 18-21 days 12-15 days 21-40 days
Immune
ReconstitutionGood Better Very Poor
GVHD Rates Average Perhaps Higher Low
Graft-vs.Tumor Average Perhaps Higher ??
Umbilical Cord Blood – A New Alternative
• Medical waste – Procured at the time of delivery
• Contains hematopoietic stem cells – Can be
used for transplantation
• Immunologically “immature” – Can be used with
less stringent matching
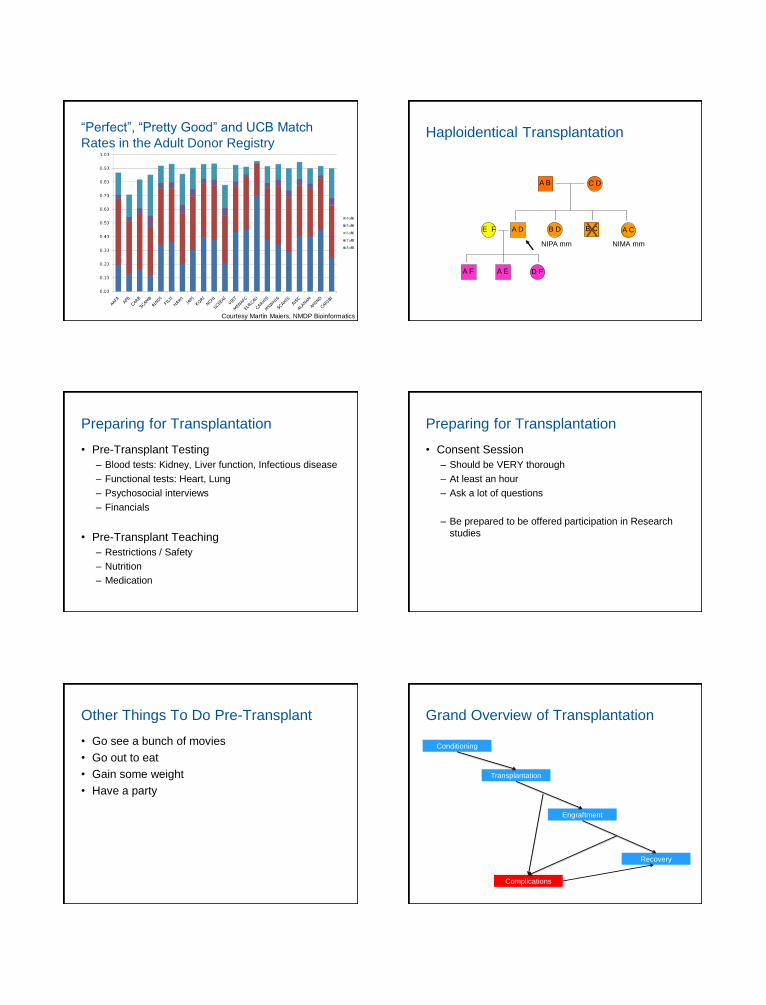
25Courtesy Martin Maiers, NMDP Bioinformatics
“Perfect”, “Pretty Good” and UCB Match
Rates in the Adult Donor RegistryHaploidentical Transplantation
A B C D
A E D F
E F B D
A F
B CA D A CXNIMA mmNIPA mm
Preparing for Transplantation
• Pre-Transplant Testing
– Blood tests: Kidney, Liver function, Infectious disease
– Functional tests: Heart, Lung
– Psychosocial interviews
– Financials
• Pre-Transplant Teaching
– Restrictions / Safety
– Nutrition
– Medication
27
Preparing for Transplantation
• Consent Session
– Should be VERY thorough
– At least an hour
– Ask a lot of questions
– Be prepared to be offered participation in Research
studies
28
Other Things To Do Pre-Transplant
• Go see a bunch of movies
• Go out to eat
• Gain some weight
• Have a party
29
Grand Overview of Transplantation
30
Conditioning
Transplantation
Engraftment
Recovery
Complications
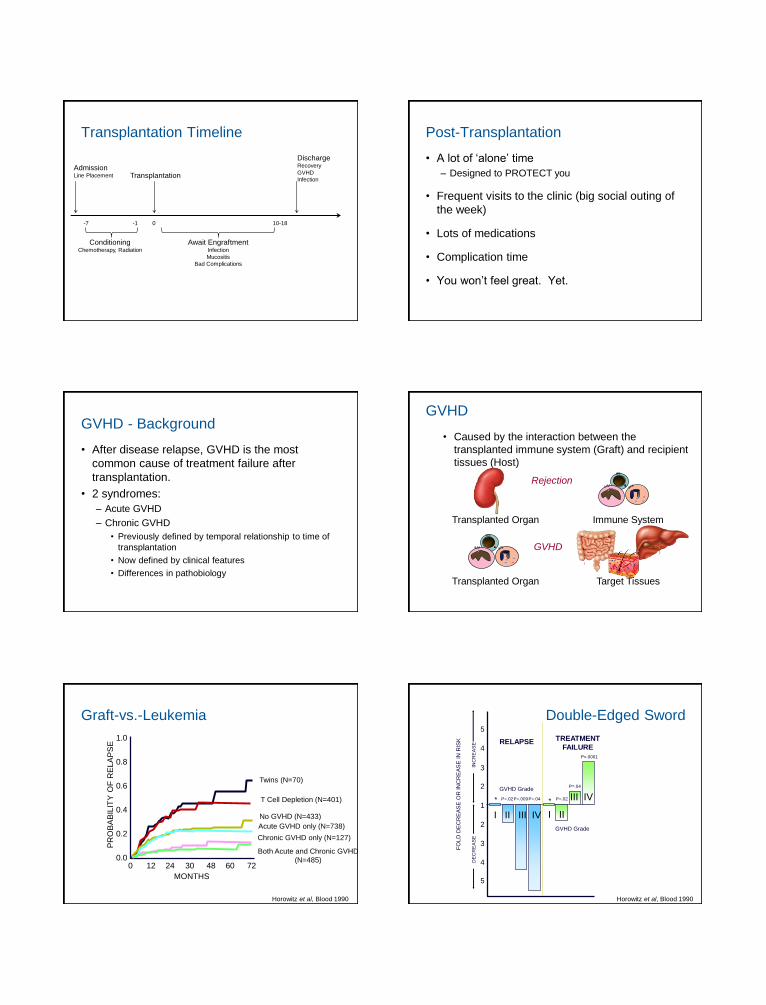
Transplantation Timeline
AdmissionLine Placement
ConditioningChemotherapy, Radiation
-7 -1 0
Transplantation
Await EngraftmentInfection
Mucositis
Bad Complications
10-18
DischargeRecovery
GVHD
Infection
Post-Transplantation
• A lot of ‘alone’ time
– Designed to PROTECT you
• Frequent visits to the clinic (big social outing of
the week)
• Lots of medications
• Complication time
• You won’t feel great. Yet.
GVHD - Background
• After disease relapse, GVHD is the most
common cause of treatment failure after
transplantation.
• 2 syndromes:
– Acute GVHD
– Chronic GVHD
• Previously defined by temporal relationship to time of
transplantation
• Now defined by clinical features
• Differences in pathobiology
GVHD
• Caused by the interaction between the
transplanted immune system (Graft) and recipient
tissues (Host)
Transplanted Organ Immune System
Transplanted Organ
Rejection
GVHD
Target Tissues
Graft-vs.-Leukemia
0 12 24 30 48 60 72
MONTHS
0.0
0.2
0.4
0.6
0.8
1.0
No GVHD (N=433)
T Cell Depletion (N=401)
Twins (N=70)
PR
OB
AB
ILIT
Y O
F R
ELA
PS
E
Acute GVHD only (N=738)
Chronic GVHD only (N=127)
Both Acute and Chronic GVHD
(N=485)
Horowitz et al, Blood 1990
*
5
4
3
2
1
2
3
4
5
P=.02P=.009P=.04 P=.02
P=.04
P=.0001
FO
LD
DE
CR
EA
SE
OR
IN
CR
EA
SE
IN
RIS
K
INC
RE
AS
ED
EC
RE
AS
E
TREATMENT
FAILURERELAPSE
*
I III II III IV
III IV
Double-Edged SwordDouble-Edged Sword
Horowitz et al, Blood 1990
GVHD Grade
GVHD Grade

Acute GVHD
Incidence:
– 35% after Related Donor Transplantation
– 50% after Unrelated Donor Transplantation
Despite prophylaxis
– Current Standard: Tacrolimus/Cyclosporine and
Methotrexate
Risk Factors for Acute GVHDFactor Condition That ↑ Risk of Acute GVHD
Donor-Recipient Factors
Major HLA Disparity (HLA Class I, II) HLA Mismatched donor > Matched Donor
Minor HLA Disparity (mHA) Unrelated Donor > Related Donor
Sex Matching Mismatch > Match
Donor Parity Multiparity > Nulliparity
Donor Age Older donor > Younger Donor
ABO type ABO Mismatch > ABO Match
Donor CMV Serostatus CMV positive > CMV Negative
Cytokine Gene Polymorphisms Numerous Associated with Acute GVHD
Stem Cell Graft Factors
Stem Cell Source PBSC > BM > UCB
Graft composition Higher CD34+ count > Lower CD34+ cell count*
Higher T cell dose > Lower T cell dose*
Transplantation Factors
Conditioning Intensity Myeloablative > Reduced-intensity Regimens
Acute GVHD
• Clinicopathologic syndrome
– Skin
Erythematous rash Bullae Desquamation
– Liver
Hyperbilirubinemia Hepatic failure
– Gut
Secretory diarrhea Ileus
Days after allogeneic HSCT
Marrow infusion
0 50 100 365
days
Host
Defense
Deficit
Bacterial
Fungal
Viral
Engraftment
CMV
Neutropenia
Mucositis
Acute GVHD + Rx Chronic GVHD + Rx
Gram Negative Rods
Low Risk High Risk
Pneumocystis jirovecii pneumonia
VZV
CMV
BK Virus HHV 6
Aspergillus
Respiratory and Enteric viruses - Epidemic
Candida sp
HSV / Resistant HSV
Gram Positive Cocci
Central Venous Catheters
Encapsulated Bacteria/Listeria/Salmonella/Nocardia
Aspergillus/Vasculotrophic Molds
Prophylaxis/preemptive/empiric
Infection
Post-Transplantation – Beyond 100 Days
• 2 Main issues
– Middle Term Complications
– Late Effects and Survivorship
Chronic GVHD - Background
• >50% of Related and Unrelated Recipients – Incidence increasing as early transplant outcomes
improve
• Important cause of morbidity in the later post-transplant period– Most have more than 1 organ system involved
• Median 2-3 years of treatment
• Associated with Quality of Life and functional deficits

Wt loss Diarrhea Lung Esophagus Joint
IBMTR-1 IBMTR-2 NMDP
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Cutaneous Oral Liver Eye
Organ Involvement
Adapted from Lee et al, 2002
Chronic GVHD – Organ Involvement
SYSTEM SIGNS SYMPTOMS
SKIN AND RELATED
STRUCTURES
Skin: Hyper/hypopigmentation,
lichenoid, sclerodermal,
papulosquamous, ichthyosiform and
psoriasiform changes. Atrophy,
poikiloderma and ulcers. Nails:
dystrophy, longitudinal ridging,
onycholysis, pterygium, destruction.
Scalp: scaling, fibrosis, scarring and
non-scarring alopecia, papulosquamous
changes.
Pruritus, dryness, pain,
infection, rigidity,
decreased range of motion,
photosensitivity.
Nail and hair loss.
MOUTH Lichenoid changes, erythema, ulcers,
xerostomia, fibrosis, leukoplakia. Dental
caries.
Pain, odinophagia,
dysphagia, dysgeusia,
dryness, sensitivity to food.
EYES Keratoconjunctivis sicca, corneal
ulcerations.
Pain, dryness photophobia.
MUSCULOSKELETAL Polymyositis, muscle weakness,
myalgias, arthritis, arthralgias, fasciitis.
Weakness, arthralgias,
myalgias, decrease ROM
GI TRACT Upper: Abnormal motility, esophageal
fibrosis, ulcerations, strictures.
Lower: Mucosal
abnormalities/malabsorption,
submucosal fibrosis
Odynophagia and lower
dysphagia, pain, heartburn,
nausea, anorexia, vomiting,
abdominal pain,
diarrhea/malabsorption,
dehydration, weight loss
SYSTEM SIGNS SYMPTOMS
LIVER Hyperbilirrubinemia, elevated Alk P,
elevated ALT/AST, fibrosis.
Fatigue, jaundice, pruritus.
LUNG Obstructive (BO/BOOP) or restrictive
(scleroderma of the chest) dysfunction.
Air trapping, bronchiectasis,
pneumothorax, pneumomediastinum,
subcutaneous emphysema. Microbial
colonization or pneumonia.
Dyspnea, wheezing, productive or
non productive cough.
NEUROLOGIC Neuropathy, myasthenic syndromes. Pain, burning, dysesthesias,
paresthesias, muscle weakness
VAGINAL
MUCOSA
Erythema, lichenoid changes, dryness,
ulcers, strictures/stenosis.
Pain, burning, dryness,
Dyspareunia
SEROSAL Serositis, pericardial, pleural and
peritoneal effusions.
Dyspnea, chest pain, pleuritic
pain, abdominal pain, ascites.
HEMATOPOIETIC Isolated or combined cytopenias,
eosinophilia, hemolysis.
Fatigue, fever, infection, bleeding.
IMMUNOLOGIC Repeated infections of various
etiologies, lymphopenia,
Hyper/hypogammaglobulinemia
Increased susceptibility to
infection.
Treatment Strategy
• Local Symptoms Local Rx
– Early identification crucial
– Supportive vs. Local immunosuppressive
– National Institutes of Health Consensus
Development Project on Criteria for Clinical Trials
inChronic Graft-versus-Host Disease: The 2014
Ancillary Therapy and Supportive Care Working
Group Report.
Biology of Blood and Marrow Transplantation, 2015
• Can be accessed through ASBMT Website:
http://www.asbmt.org/?page=GuidelineStatements
Treatment Strategy
• Systemic Symptoms / Multiple Local Sites Systemic Rx
• Initial Rx:
– Prednisone 1 mg/kg/day
– Tacrolimus: 5-10 ng/ml or
– Cyclosporine: 200-400 µg/L
• Complete Response Rate: 50-55%
• Median Time to Discontinue Immune Therapy:
1.6 – 2.2 years!!
• Multiple Clinical Trials available – You should participate!!!
– www.clinicaltrials.gov
Post-Transplant Transitions
• You will experience a number of transitions post transplant– Gaining more independence and freedom - welcomed yet
very stressful
– Relationships with family/friends/loved ones-going through a time of adjustment
– Financial pressures – Going/not going back to work
• Acknowledge the enormity of your experience– The reality of your diagnosis
– The trauma inherent in transplant
– The loss of who you were and the security you previously felt
– Seek help if you are stuck
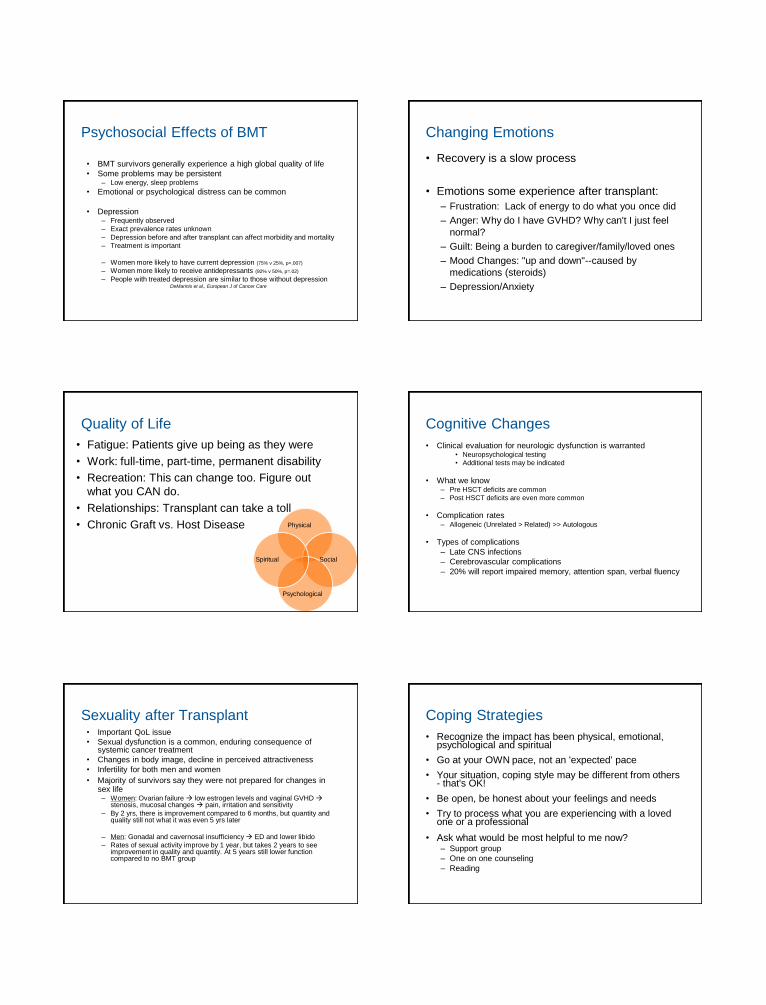
Psychosocial Effects of BMT
• BMT survivors generally experience a high global quality of life
• Some problems may be persistent– Low energy, sleep problems
• Emotional or psychological distress can be common
• Depression– Frequently observed
– Exact prevalence rates unknown
– Depression before and after transplant can affect morbidity and mortality
– Treatment is important
– Women more likely to have current depression (75% v 25%, p=.007)
– Women more likely to receive antidepressants (92% v 50%, p=.02)
– People with treated depression are similar to those without depressionDeMarinis et al., European J of Cancer Care
Changing Emotions
• Recovery is a slow process
• Emotions some experience after transplant:
– Frustration: Lack of energy to do what you once did
– Anger: Why do I have GVHD? Why can't I just feel
normal?
– Guilt: Being a burden to caregiver/family/loved ones
– Mood Changes: "up and down"--caused by
medications (steroids)
– Depression/Anxiety
Quality of Life
• Fatigue: Patients give up being as they were
• Work: full-time, part-time, permanent disability
• Recreation: This can change too. Figure out
what you CAN do.
• Relationships: Transplant can take a toll
• Chronic Graft vs. Host Disease Physical
Psychological
Spiritual Social
Cognitive Changes
• Clinical evaluation for neurologic dysfunction is warranted• Neuropsychological testing
• Additional tests may be indicated
• What we know– Pre HSCT deficits are common
– Post HSCT deficits are even more common
• Complication rates– Allogeneic (Unrelated > Related) >> Autologous
• Types of complications
– Late CNS infections
– Cerebrovascular complications
– 20% will report impaired memory, attention span, verbal fluency
Sexuality after Transplant• Important QoL issue
• Sexual dysfunction is a common, enduring consequence of systemic cancer treatment
• Changes in body image, decline in perceived attractiveness
• Infertility for both men and women
• Majority of survivors say they were not prepared for changes in sex life– Women: Ovarian failure low estrogen levels and vaginal GVHD
stenosis, mucosal changes pain, irritation and sensitivity
– By 2 yrs, there is improvement compared to 6 months, but quantity and quality still not what it was even 5 yrs later
– Men: Gonadal and cavernosal insufficiency ED and lower libido
– Rates of sexual activity improve by 1 year, but takes 2 years to see improvement in quality and quantity. At 5 years still lower function compared to no BMT group
Coping Strategies
• Recognize the impact has been physical, emotional, psychological and spiritual
• Go at your OWN pace, not an 'expected' pace
• Your situation, coping style may be different from others - that's OK!
• Be open, be honest about your feelings and needs
• Try to process what you are experiencing with a loved one or a professional
• Ask what would be most helpful to me now?– Support group
– One on one counseling
– Reading

Taking care of yourself
• Take your medications
• Make your appointments
• Respect your altered immune function
• Mind your emotional well being
• Get enough sleep
• Pay attention, keep lists, make associations
• Consider cognitive rehabilitation services
• Keep your perspective
– Do not over-generalize
– Time heals all?
• Nutrition
• Exercise
Dietary Challenges after Transplant
• Weight gain or loss
• Appetite changes– Small, frequent meals
– Avoid eating snacks too close to meal times
– Choose nutrient dense foods
– Fortify foods to boost calories
– Try new recipes
• Lack of interest in food
• Taste alterations / Dry Mouth– Drink plenty of fluids, at least 8 cups per day
– Moisten foods with gravies, sauces, or broth
– Limit caffeine
– Artificial saliva products
• Steroids, GVHD
Post-Transplant Diet• Eat 5-10 servings fruits & veggies each day
– 1 serving = 1/2 cup cut, cooked or sliced; 1 piece medium fruit; 1 cup leafy greens
• Re-shape your plate– 1/2 veggies, 1/4 protein, 1/4 whole grains
• Emphasis on variety• Look for richly colored plant foods• Emphasize whole grains
– Reduce risk for certain cancers, diabetes and heart disease
– Keep weight off
– Lower cholesterol levels
– Promote digestive health
• Reduce consumption of saturated and trans- fats, increase monounsaturated and omega-3 Fats
Focus on Physical Activity
Physical Activity + Proper Diet = Healthy Weight• Create an individualized fitness plan
– Always talk with your doctor first
– Schedule time for activity each day, remember every bit counts
– Ensure intensity appropriate
– Choose activities you enjoy
– Find a workout “buddy”
• Incorporate key components
– Cardiovascular exercise, strength, flexibility and relaxation
Returning to Work• Up to 89% of BMT patients return to work or school within 5 years
after treatment.
• Influences that impact the ability to return to work are:– Age– Gender– Education– Personal values– Perceived advantages of work
• Influences that impact the INability to return to work:– Physical demands
– Job Lock
– Employer accommodation
– Fear of disclosure
– Perceived discrimination
• Data suggests BONE MARROW recipients more likely to return to work than PBSC recipients (Lee, ASH 2015)
Employer Accommodation
Accommodation: Aiding an employee to perform
their job by providing modifications.
“Reasonable” accommodations
– Change in duties
– Change in work hours
– Flexible work hours
– Periodic rest breaks
– Allow employees to work from home
– Modify dress code

Caregivers• Acknowledge the long haul of BMT caregiving
– Physical demands
– Feelings of loss, anger, fatigue, resentment, hope
• Change has been difficult, you have HAD to adapt to the change-shift in roles
• Sometimes paddling in the same direction as your loved one is difficult
• Every relationship/family functions differently
• As a caregiver, must adapt to what works best for you
• Make time for yourself
• Rely upon others (transportation, child care, meals)
• Say NO to non-essential needs – Prioritize!
Survivorship in BMT
After 1998
Before 1998
• Donor-recipient matching• GVHD prophylaxis anfd treatment• Supportive care
Survivorship in BMT
• 2 components:
– Surviving Malignancy
– Surviving Transplantation
• Different sets of risks and complications need
to be considered
Medical Monitoring after BMT
Majhail et al. Recommended screening and
preventive practices for long-term survivors after
hematopoietic cell transplantation.
Biology of Blood and Marrow Transplantation, 2012
Antin JH. Long term care after hematopoietic –cell
transplantation in adults.
New England Journal of Medicine, 2002
Medical MonitoringOrgan Risk Outcome What To Do?
Mouth Radiation, cGVHD Dryness, Caries Regular dental exams
Monitor for oral cancers
Eyes Radiation, cGVHD,
steroids
Dryness, Cataracts Regular eye exams
Schirmer test for dryness
Bones Radiation, steroids,
low estrogen/testost.
Osteoporosis, fracture Bone Densitometry
Calcium/Vitamin D
Hormone replacement
Lungs Radiation, Immune
suppression
Pneumonitis Quit smoking
Regular lung function test
Endocrine Radiation, Chemo,
steroids
Hypothyroidism
Hypoadrenalism
Hypogonadism
Screening
Slow steroid tapers
Hormone replacement
Medical MonitoringOutcome Risk What To Do?
Infection cGVHD, Immune Suppression Prophylaxis
Second Cancers Radiation, Chemotherapy,
cGVHD, Immune Suppression
Screening exams
Cardiovascular Steroids, Hypogonadal state,
Medications, Glucose
Intolerance
Routine BP monitoring
Routine Glucose monitory
General Health Survivorship See your PCP !

Allogeneic BMT Survivorship Clinic
• Target population– Allogeneic recipients of high-dose myeloablative
conditioning
– Alive, without malignancy, 12 months after transplantation
– May have evidence of chronic GVHD
– Total treatment considered• Chemotherapy to treat malignancy
• Focal radiotherapy to treat malignancy
• High-dose chemotherapy for transplant prep
• Total body irradiation for transplant prep
Allogeneic BMT Survivorship Clinic
• Multidisciplinary clinic– 1x/month, capture all patients (voluntary) for a one
time consultative visit
• Goals of the clinic– Develop wellness plan to address the needs of this
high risk group
– Develop an individualized follow up plan to address the non-GVHD related risks of transplant survivors
Allogeneic BMT Survivorship Clinic
• Providers– BMT Specialists: MD and NP – Endocrine,
cardiovascular, respiratory, bone, sexuality, cancer screening
– Dermatology– Oral Medicine– Ophthalmology– Exercise Physiology– Nutrition– Psychosocial Counselor
• Patients will be followed annually by NP for their survivorship needs, outlined in the wellness plan
• Research Agenda
Treatment summary
Diagnostic tests performed and results
Tumor characteristics (e.g. site, stage, grade, markers)
Dates of treatment initiation and completion Surgery, radiotherapy, chemotherapy, including agents used
Treatment regimen, total dosage, clinical trials (if any), and toxicities experienced during treatment
Psychosocial, nutritional, and other supportive services
Contact information on treating institutions and providers Identification of a key coordinator of continuing care
More Resources in BMT
• National Marrow Donor Program
– www.bethematch.org
– Smartphone app (excellent)
• BMT InfoNet
– www.bmtinfonet.org
• nbmtLink
– www.nbmtlink.org
• Questions?
72
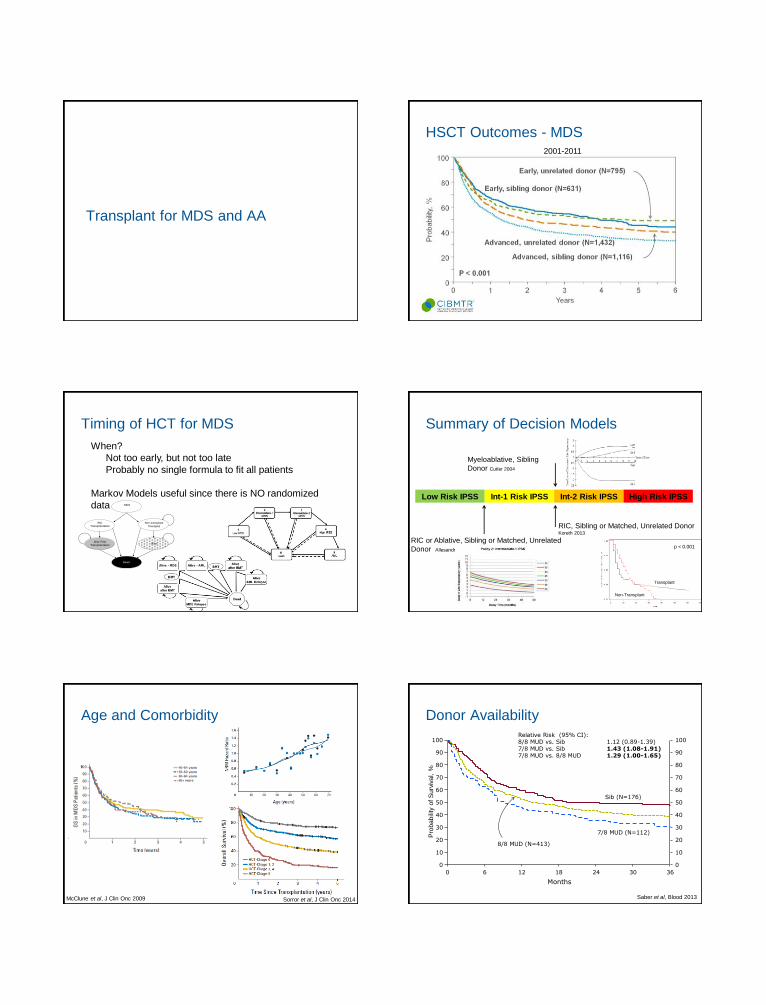
Transplant for MDS and AA
HSCT Outcomes - MDS2001-2011
Timing of HCT for MDS
Figure 1
MDS
RIC Transplantation
Non-transplant
Therapies
Dead
Alive Post Transplantation
Alive
When?
Not too early, but not too late
Probably no single formula to fit all patients
Markov Models useful since there is NO randomized
data
Summary of Decision Models
Low Risk IPSS Int-1 Risk IPSS Int-2 Risk IPSS High Risk IPSS
Myeloablative, Sibling
Donor Cutler 2004
RIC, Sibling or Matched, Unrelated Donor Koreth 2013
RIC or Ablative, Sibling or Matched, Unrelated
Donor Allesandrino 2013
Non-Transplant
Transplant
p < 0.001
Age and Comorbidity
McClune et al, J Clin Onc 2009 Sorror et al, J Clin Onc 2014
Donor Availability
Pro
ba
bili
ty o
f S
urv
iva
l, %
Months
0 6 12 362418
100
0
20
40
60
80
90
10
30
50
70
0
100
20
40
60
80
90
10
30
50
70
30
Sib (N=176)
8/8 MUD (N=413)
7/8 MUD (N=112)
Relative Risk (95% CI):8/8 MUD vs. Sib 1.12 (0.89-1.39) 7/8 MUD vs. Sib 1.43 (1.08-1.91) 7/8 MUD vs. 8/8 MUD 1.29 (1.00-1.65)
Saber et al, Blood 2013

Donor Availability
100
0
20
40
60
80
0
100
20
40
60
80
Pro
ba
bili
ty,
%
Years
0 2 94
Cord Blood (N=153)
861 3 75
Haploidentical donor (N=95)
Partially-matched UD (N=289)
Mismatched UD (N=65)
Log Rank p-value = 0.24
Courtesy W. Saber
HSCT Outcomes - SAA
>20 y, Unrelated Donor, (N = 114)
< 20 y, Unrelated Donor, (N = 244)
> 20y, Sibling Donor (N = 845)
>20 y, Sibling Donor (N = 844)
1994-19992001-2011
HCT for SAA
• This is an HCT EMERGENCY
• HLA type IMMEDIATELY
– Serologic family typing available often in 1-2 business
days
• Avoid Transfusion if possible
– Permissive anemia
– Permissive thrombocytopenia
Doney, Ann Intern Med 1997