TROMBOEMBOLIA PULMONAR - Gmemi · En conclusión, sin tromboprofilaxis, la incidencia de TVP va de...
41
TROMBOEMBOLIA PULMONAR DRA. LINDA SÁNCHEZ PÉREZ RESIDENTE DE MEDICINA INTERNA
-
Upload
vuongquynh -
Category
Documents
-
view
217 -
download
0
Transcript of TROMBOEMBOLIA PULMONAR - Gmemi · En conclusión, sin tromboprofilaxis, la incidencia de TVP va de...

TROMBOEMBOLIA PULMONAR
DRA. LINDA SÁNCHEZ PÉREZ
RESIDENTE DE MEDICINA INTERNA


EPIDEMIOLOGÍA
▸ Tercera causa de enfermedad cardiovascular
▸ Incidencia anual de 100-200 por 100,000 habitantes / año
▸ 371 000 muertes
▸ 34% muerte súbita
▸ 54% sin diagnóstico
▸ 7% diagnóstico
▸ 40 años 2014 ESC Guidelines on the diagnosis and management of acute pulmonar embolism
PLoS One. 2016 Mar 1;11(3):e0150448. doi: 10.1371/journal.pone.0150448. eCollection 2016

95% CI: 0.51 to 7.89); results were similar at 6 months(59). In this context, it should also be borne inmind that cava filter placement is not free of compli-cations, which may include penetration of the cavalwall or embolization to the right heart cavitiesand occasionally require emergency treatment (60).Moreover, and importantly, the high success rates offilter retrieval (153 of 164 patients in whom it wasattempted) reported in the PREPIC 2 trial (59) willbe very difficult to reproduce in the real world,probably increasing the rate of long-term complica-tions. In conclusion, the evidence derived fromtrial data does not support the liberalization ofcava filter use beyond the strict indications listedpreviously.
IMPACT OF EVOLVING MANAGEMENT
STRATEGIES: TRENDS IN MORTALITY
AND THE ECONOMIC BURDEN OF
PULMONARY EMBOLISM
Evidence published in the past decade and continuingto accumulate consistently indicates a progressivereduction of case fatality rates among patients withacute PE (Figure 2). Data obtained from the U.S.Nationwide Inpatient Sample during the 8-year period
between 1998 and 2005 were used to investigate theoutcomes of patients with a primary or secondary PEdiagnosis who had been discharged from acute carehospitals. The number of patients increased from126,546 to 229,637 annually during that period; at thesame time, in-hospital case fatality rates for these pa-tients decreased from 12.3% to 8.2%, and the length ofhospital stay decreased from 9.4 to 8.6 days (65).Another study, using both the U.S. Nationwide Inpa-tient Sample cohort and the Multiple Cause-of-Deathdatabase, reported that the incidence of diagnosedPE increased by as much as 81% (from 62.1 to 112.3 per100,000) following the introduction of CT angiog-raphy, in comparison to the earlier reference period(1998 to 2006 vs. 1993 to 1998); in parallel, case fatalityrates decreased before (from 13.2% to 12.1%) and,particularly, in the era of CT angiography (from 12.1%to 7.8%). Over the entire observation period, mortalityrelated to PE dropped from 13.4 to 11.9 per 100,000(66). Similar trends were reported from Germany (67),and also on the basis of theNational Hospital DischargeDatabase, covering the entire Spanish population (68).In the latter study, in-hospital case fatality rates of PEdecreased from 12.9% in 2002 to 8.3% in 2011 in parallelwith a decrease in mean length of hospital stay from12.7 to 10 days.
FIGURE 2 Global Trends in PE Incidence and Case Fatality Rates
120
110
100
90
80
70
60
50
40
30
20
10
1997 1999 2001 2003 2005 2007 2009 2011 2013Year
Num
ber o
f Pul
mon
ary
Embo
lism
Dia
gnos
es /
100,
000
Inha
bita
nts
1997 1999 2001 2003 2005 2007 2009 2011 2013Year
26
24
22
20
18
16
14
12
10
8
6
4
2
Num
ber o
f In-
hosp
ital D
eath
s / 10
0 Pu
lmon
ary
Embo
lism
Dia
gnos
es (%
)
Incidence Rate Case Fatality Rate
U.S. (66)†
U.S. (66)*Italy (62)*
Australia (61)*
Spain (68)*
China (64)*
Italy (62)*
Spain (68)*U.S. (66)†
U.S. (70)†
U.S. (66)*U.S. (70)*
U.S. (63)*
(Left) Pulmonary embolism (PE) incidence. (Right) Case fatality rates. Data shown here were retrieved from studies of trends in pulmonary embolism (61–64,66,68,70).In case of duplicate or overlapping data, only the most recent publication was included. *Pulmonary embolism was listed as principal diagnosis. †Any listed code forpulmonary embolism was considered.
Konstantinides et al. J A C C V O L . 6 7 , N O . 8 , 2 0 1 6
Pulmonary Embolism Update M A R C H 1 , 2 0 1 6 : 9 7 6 – 9 0
984
JACC. VOL.67, NO.8. 2016

EPIDEMIOLOGÍA
▸ Aumento de mortalidad a los 3 meses
▸ 600, 000 casos en EU
▸ 200 000-300 000 muertes al año
▸ Complicaciones $13.5 a $69.3 billones
▸ Prevenir $4.5 a $39.3 billones
▸ 150, 000 sin diagnóstico
JAMA. 2014;311(23):2414-2421Journal of Intensive Care Medicine. 2010. 26(5) 275-294
JACC. VOL.67, NO.8. 2016
EPIDEMIOLOGÍA
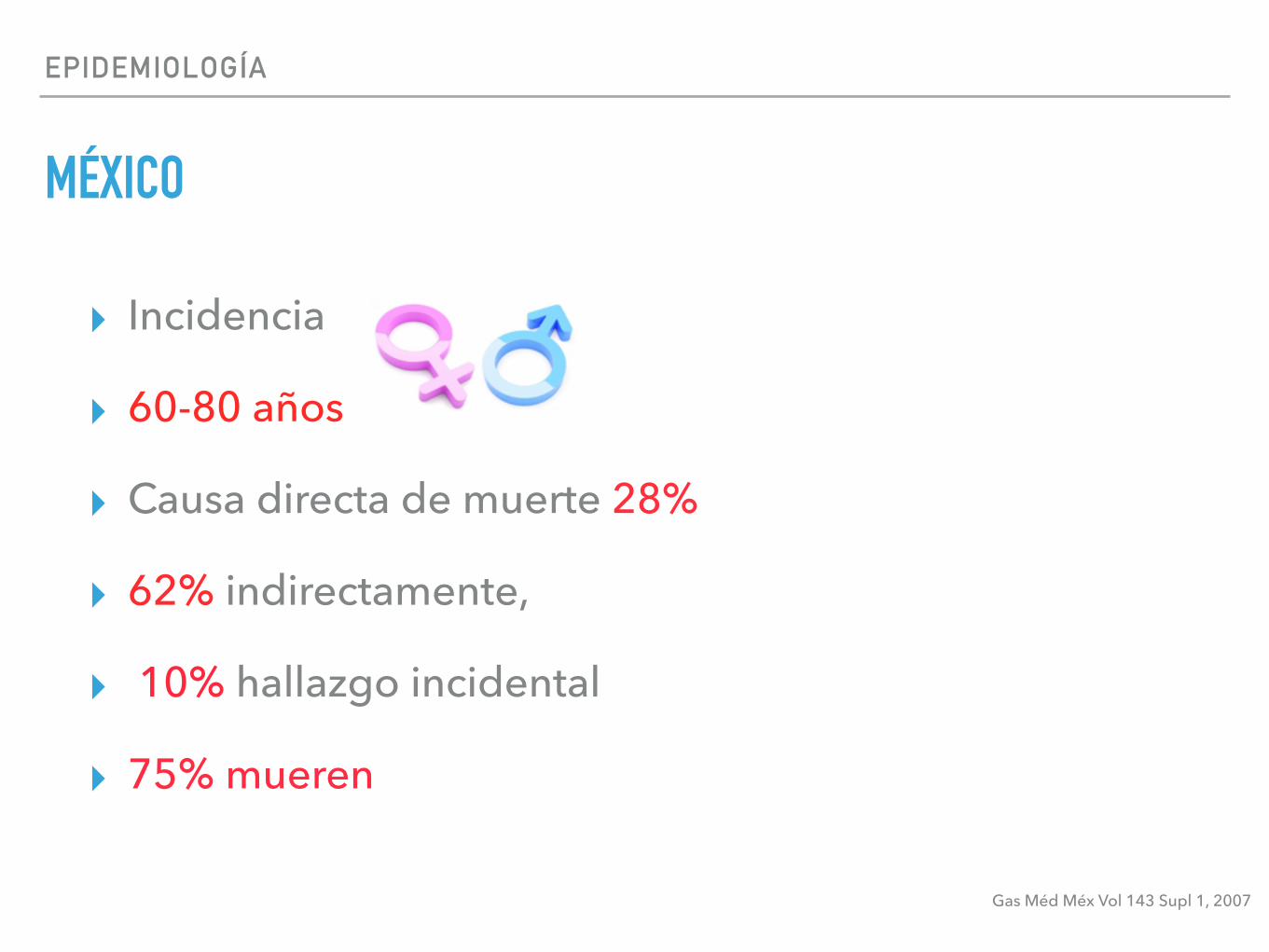
MÉXICO
▸ Incidencia
▸ 60-80 años
▸ Causa directa de muerte 28%
▸ 62% indirectamente,
▸ 10% hallazgo incidental
▸ 75% mueren
Gas Méd Méx Vol 143 Supl 1, 2007

EPIDEMIOLOGÍA
▸ INC
▸ 1032 autopsias/ 3751
▸ 231 TEP
▸ 100 masiva
▸ Sospecha 18%
▸ Tercera causa de mortalidad
▸ 82% TVP
Gas Méd Méx Vol 143 Supl 1, 2007
4 Gac Méd Méx Vol. 143 Supl 1, 2007
Datos nacionales
En México, de 1981 a 1990, en el Hospital General del CentroMédico Nacional del IMSS, se realizaron 1,685 necropsias. Seinformaron 252 casos con TEP (15%). La incidencia paraambos sexos fue similar y, aunque apareció en un rangoamplio de edad, la mayoría de casos se encontró entre los 60 y80 años. La TEP fue causa directa de muerte en 28%, contribuyóindirectamente en 62% y constituyó un hallazgo incidental en10%.4 En el Instituto Nacional de Cardiología Ignacio Chávez,entre 1985 y 1994, se realizaron 1,032 necropsias de 3,751defunciones. El diagnóstico de TEP se estableció en 231 casosy en 100 de ellos la TEP fue masiva; sin embargo, clínicamente,el diagnóstico sólo se sospechó en 18% de los pacientes. En estarevisión se informó como la tercera causa de mortalidad (10%),superada sólo por condiciones clínicas con falla circulatoriairreversible. La mayor incidencia se observó en menores de 10años en el postoperatorio inmediato de cirugía por cardiopatíacongénita.5
A pesar de la controversia con respecto a la relación entrela TVP asintomática y la TEP, estudios históricos sugieren quela TVP casi siempre precede a TEP y que ésta suele presen-tarse en el contexto de una TVP en la mayoría de las ocasionescomo asintomática. En 82% de los pacientes con TEP agudaratificada por angiografía se presenta al mismo tiempo TVPdemostrada por flebografía. En 21% de pacientes con diag-nóstico clínico de TVP se encuentran informes de gamagrafíapulmonar con alta posibilidad de TEP aguda.6
Estudios epidemiológicos.
Gran parte del conocimiento epidemiológico de la ETV seobtuvo de estudios en pacientes quirúrgicos. Aunque existenpocos análisis en pacientes con patología médica que permi-tan conocer la incidencia de ETV, uno de ellos, el estudioMedenox, incluyó 1,102 pacientes hospitalizados no quirúrgi-cos.7 Uno de los objetivos fue establecer la incidencia de ETVmediante flebografía bilateral o ultrasonido dóppler color (USD).En el día 14 de estudio, 236 pacientes se excluyeron por la faltade algún estudio por lo que sólo se incluyeron 866 pacientesen tres grupos. La incidencia de ETV fue mayor en el grupoplacebo vs. los grupos que recibieron 20 mg o 40 mg deenoxaparina (reducción del riesgo relativo = 0.37; p<0.001). Alfinal se registraron 4 TEP no fatales (3 en el grupo placebo y1 en el grupo de enoxaparina 20 mg). Por lo tanto, se consideraque los pacientes con patología no quirúrgica tienen un riesgomoderado para ETV. En otros estudios de pacientes noquirúrgicos, la incidencia de ETV alcanzó hasta 26%.8 Sinembargo, la incidencia de TEP fatal fue difícil de establecerdebido al bajo número de necropsias realizadas. En un estudiopostmortem, se informó que 7.6% de las muertes fueroncausadas por TEP.9
Los pacientes en las unidades de cuidados intensivos(UCI) tienen riesgo elevado de ETV al compararse con pacien-tes hospitalizados en otros servicios. A pesar de esto, 30 a100% de las TVP diagnosticadas en terapia intensiva por USDno se sospechan clínicamente. Se estima que los pacientescon ventilación mecánica y períodos de hipotensión, taquicardiae hipoxemia tienen un alto porcentaje de TEP no diagnostica-
da.10 En 268 pacientes en UCI con calificación promedio deAPACHE II de 25.5 puntos (+8.5), la prevalencia de TVP fuede 2.7% al momento del ingreso pero aumentó a 9.6% durantela estancia en el servicio (intervalo de confianza al 95% = 6.3-13.8).11 Se identificaron cuatro factores de riesgo independien-tes para desarrollar TVP: historia familiar o personal de TEP;ventilación mecánica prolongada (mediana = 9 días); estanciaprolongada en UCI (mediana = 17 días); y estanciaintrahospitalaria prolongada (mediana = 51 días).
Es importante considerar que los estudios epidemiológicosprovienen de sólo algunos países, utilizando diferentes clasi-ficaciones y criterios de diagnóstico; esto puede inducir un altomargen de error. Además, las necropsias no se realizan enforma sistemática y no es posible determinar con exactitud elporcentaje de casos sin expresión clínica.
En conclusión, sin tromboprofilaxis, la incidencia de TVP va de10% al 40% en pacientes con patología médica o con algún tipo decirugía general. Esta incidencia aumenta a 50% en pacientes conenfermedad vascular cerebral, hasta 60% en pacientes sometidosa cirugía ortopédica y hasta 80% en politraumatizados o pacientescríticamente enfermos (Cuadro I).12
Referencias1. Geerts WH, Heit JA, Claget GP, Pineo GF, Colwell CW, Anderson FA, et al.
Prevention of venous thromboembolism. Chest 2001;119:132S–175S.2. Spyropoulus AC. Emerging strategies in the prevention of venous
thromboembolism in hospitalized medical patients. Chest 2005;118:958-969.3. Carson JS, Kelley MA, Duff A, Weg JG, Fulkerson WJ, Palevsky HI, et al.
The clinical course of pulmonary embolism. N Engl J Med 1992;326:1240-1245.4. Sigler L, Romero T, Meillón LA, Gutiérrez L, Aguirre GJ, Esparza C.
Tromboembolia pulmonar en un período de 10 años. Rev Med IMSS 1996;34:7-11.
5. Sandoval ZJ, Martínez GML, Gómez A, Palomar A, Pulido T, Zevallos M.PAC Cardio-1. Tromboembolia pulmonar aguda. Sociedad Mexicana deCardiología. Editorial Intersistemas, México, DF. 1998;7-9.
6. Monreal M, Kakkar AK, Capriani JA, Barba R, Uresandi F, Valle R, et al. forthe RIETE investigators. Is the natural history of venous thromboembolismdifferent in surgery and non-surgery patients? Findings from the RIETE registry.Blood 2003;102:112b.
7. Alikhan R, Cohen AT, Combe S, Samama M, Desjardins L, Eldor A, et al.Risk factors for venous thromboembolism in hospitalized patients with acutemedical illnes: Analysis of the MEDENOX Study. Arch Intern Med 2004;164:963-968
8. Cade JF. High risk of the critically ill for venous thromboembolism. Crit Care Med1982;10:448-450.
Epidemiología de la enfermedad tromboembólica venosa
Cuadro I. Riesgo absoluto de TVP en pacientes hospitalizados*
Grupo de pacientes Prevalencia de TVP (%)
Padecimiento médico 10 – 20Cirugía general 15 – 40Cirugía ginecológica mayor 15 – 40Cirugía urológica mayor 15 – 40Neurocirugía 15 – 40Evento vascular cerebral 20 – 50Artroplastía de cadera o rodilla 40 – 60Trauma mayor 40 – 80Pacientes de terapia intensiva 10 – 80
*Modificado de referencia 12

Epidemiology
Approximately 600 000 PEs occur yearly in the United States,resulting in 200 000 to 300 000 deaths.5,6 Only 150 000 of allpatients with PE are actually diagnosed, indicating that thou-sands of PEs go undetected.7 Many deaths due to PE are unrec-ognized and the diagnosis is often made at autopsy.8 Manydeaths occur in hemodynamically unstable patients mistakenlythought to have myocardial infarction or arrhythmias.7
The risk of VTE is especially high in the critically ill. Withinthe first week of intensive care unit (ICU) admission, more than30% develop deep venous thrombosis (DVT) if they do notreceive prophylaxis.1 Of all patients in medical intensive careunits, 29% to 33% develop DVT. Inpatient mortality is 42%higher for patients with VTE compared to those without.1
Estimates of the percentage of PE patients presenting withhemodynamic instability range from 4.2% in the InternationalCooperative PE Registry (ICOPER)9 to as high as 22%.3,10,11
In patients with hemodynamic instability, inpatient mortalityis at least 15%; 25% for those with cardiogenic shock.7 Severalhereditary and acquired risk factors predispose individuals toVTE (Table 1). A detailed discussion of risk factors is beyondthe scope of this article and the reader is referred to an excellentreview for additional information.12
Definitions
It is helpful to divide PE into 3 categories: massive, sub-massive, and low risk. Those with massive PE are at highestrisk for death (Table 2).7,13 Key clinical features include hemo-dynamic compromise, shock, or need for cardiopulmonaryresuscitation.3 Hemodynamic compromise is defined by a sys-tolic arterial pressure <90 mm Hg or a drop in systolic arterialpressure by at least 40 mm Hg.7 Clinical evidence of shock may
include tissue hypoperfusion, hypoxia, metabolic (lactic)acidosis, altered mental status, oliguria, or cool extremities.7
Hemodynamic compromise must be caused by the PE not con-comitant illness.
Patients with sub-massive PE have normal blood pressureand evidence of right ventricular (RV) dysfunction.14 Evidenceof acute RV strain on electrocardiogram (EKG) may also helpdefine sub-massive PE. Right ventricular enlargement noted bycomputed tomographic pulmonary angiography (CTPA) canalso indicate sub-massive PE. Elevated cardiac biomarkers(brain natriuretic peptide [BNP] and troponin I for example)raise the suspicion for sub-massive PE. Patients with sub-massive PE comprise 31% of PEs diagnosed10 and have a5.0% to 12.6% in-hospital mortality rate, compared to 0.9%in patients with low-risk PE who have no evidence of RV dys-function (Table 2).3,15,16
Pathogenesis
Venous thromboembolism has long been considered one dis-ease, comprising DVT and PE.8 It was felt that PE most com-monly arises from the deep veins of the legs. Among patientswhose cause of death was due to PE by autopsy, approximately83% had evidence of DVT in their legs.17 In a retrospectivereview of hospitalized patients, 18% of all DVT presented inthe upper extremities.18 In all, 7% to 9% of upper extremityDVT may cause PE, mostly in those untreated.18 Lower extre-mity thrombi originate predominantly in venous valve pocketsand other sites of presumed venous stasis in the calves and pro-pagate above the knee.8 Once above the knee, thrombi are atgreatest risk of migrating.
A study of trauma patients found that PE was not associatedwith DVT in the pelvic or lower extremity veins.19 The authorsconcluded that some PE results from peripheral vein DVT but
Table 1. Risk Factors for VTEa
Acquired Risk Factors Hereditary Risk Factors Mixed/Unknown
Bed restTravelImmobilizer or castTrauma/spinal cord injuryMajor surgeryOrthopedic surgeryMalignancyOral contraceptivesHormonal replacement therapyAntiphospholipid syndromeMyeloproliferative disordersPolycythemia veraCentral venous cathetersAgeObesityChemotherapyHeparinsPregnancy/postpartum period
Antithrombin deficiencyProtein C deficiencyProtein S deficiencyFactor V leiden (FVL)Prothrombin gene mutationDysfibrinogenemiaFactor XIII 34valPlasminogen deficiency
High levels of factor VIIIHigh levels of factor IXHigh levels of factor XIHigh levels of factor fibrinogenActivated Protein C resistance in absence of FVLHyperhomocysteinemiaHigh levels of plasminogen activatorElevated levels of lipoprotein (a)Low levels of tissue factor pathway inhibitor
a N Engl J Med. 2008;358(10):1037-10528; Hematology Am Soc Hematol Educ Program. 200512.
276 Journal of Intensive Care Medicine 26(5)
at Universidad Nacional Aut Mexic on March 19, 2016jic.sagepub.comDownloaded from
Journal of Intensive Care Medicine. 2010. 26(5) 275-294
SEPSIS
SÍNDROME NEFRÓTICO
INSUFICIENCIA HEPÁTICA CHILD PUGH C

FISIOPATOLOGÍA
▸ Interferencia entre la circulación e intercambio de gases
▸ Sobrecarga del VD
▸ Falla del VD
▸ Aumento de la PAP 30-50%
▸ Vasoconstricción: Liberación de tromboxano A2 y serotonina
▸ Factor activador de plaquetas, trombina, C3,C5 e histamina
2014 ESC Guidelines on the diagnosis and management of acute pulmonar embolismJournal of Intensive Care Medicine. 2010. 26(5) 275-294

FISIOPATOLOGÍA
▸ Aumento de la RVP proporcional a la disminución de la compliance arterial
▸ Aumento de la RVP produce dilatación del VD
▸ Alteraciones en la contractilidad (Frank-Starling)
2014 ESC Guidelines on the diagnosis and management of acute pulmonar embolism

Revised Starling equation and the glycocalyx modelof transvascular fluid exchange: an improved paradigmfor prescribing intravenous fluid therapyT. E. Woodcock 1* and T. M. Woodcock 2
1 Critical Care Service, Southampton University Hospitals NHS Trust, Tremona Road, Southampton SO16 6YD, UK2 The Australian School of Advanced Medicine, Macquarie University, NSW 2109, Australia
* Corresponding author. E-mail: [email protected]
Editor’s key points
† The classic Starlingprinciple does not holdfor fluid resuscitation inclinical settings.
† The endothelialglycocalyx layer appearsto have a major role influid exchange.
† A revision of Starlingincorporating theglycocalyx modelappears to explain betterthe responses seenclinically.
Summary. I.V. fluid therapy does not result in the extracellular volume distribution expectedfrom Starling’s original model of semi-permeable capillaries subject to hydrostatic andoncotic pressure gradients within the extracellular fluid. Fluid therapy to support thecirculation relies on applying a physiological paradigm that better explains clinical andresearch observations. The revised Starling equation based on recent research considersthe contributions of the endothelial glycocalyx layer (EGL), the endothelial basementmembrane, and the extracellular matrix. The characteristics of capillaries in varioustissues are reviewed and some clinical corollaries considered. The oncotic pressuredifference across the EGL opposes, but does not reverse, the filtration rate (the ‘noabsorption’ rule) and is an important feature of the revised paradigm and highlights thelimitations of attempting to prevent or treat oedema by transfusing colloids. Filtered fluidreturns to the circulation as lymph. The EGL excludes larger molecules and occupies asubstantial volume of the intravascular space and therefore requires a new interpretationof dilution studies of blood volume and the speculation that protection or restoration ofthe EGL might be an important therapeutic goal. An explanation for the phenomenon ofcontext sensitivity of fluid volume kinetics is offered, and the proposal that crystalloidresuscitation from low capillary pressures is rational. Any potential advantage of plasmaor plasma substitutes over crystalloids for volume expansion only manifests itself athigher capillary pressures.
Keywords: fluid therapy; intensive care
Twenty-five years ago, Twigley and Hillman announced ‘theend of the crystalloid era’. Using a simplified diagram ofplasma, interstitial and intracellular fluid compartments,and their anatomic volumes, they argued that colloidscould be used to selectively maintain the plasma volume.1
Plasma volume being about 20% of the extracellular fluid(ECF), it was presumed that the volume equivalence for re-suscitation from intravascular hypovolaemia would be ofthe order of 20 ml colloid to 100 ml isotonic salt solution(ISS). Moreover, it was presumed from Starling’s principlethat transfusion of hyperoncotic colloid solutions wouldabsorb fluid from the interstitial fluid (ISF) to the intravascu-lar volume. This simple concept of colloid for plasma volumeand ISS for ECF replacement has been continued and devel-oped.2 – 4 Two trials in critically ill patients have found thatover the first 4 days of fluid resuscitation, 100 ml ISS is as ef-fective as 62–76 ml human albumin solution5 or 63–69 mlhyperoncotic plasma substitute.6 In blunt trauma patientsduring the first day of resuscitation, 100 ml ISS was as effect-ive as 97 ml isosmotic plasma substitute, while in gunshot orstabbing victims, 100 ml was as effective as 67 ml.7 A trial ofpaediatric resuscitation practices in resource-poor facilities in
Africa demonstrated no advantages of bolus therapy withalbumin compared with ISS, and a survival advantage forslow ISS resuscitation without bolus therapy.8 A series ofvolume kinetics experiments have demonstrated that thecentral volume of distribution of ISS is much smaller thanthe anatomic ECF volume,9 and an editorial had to concludethat ‘Fluid therapy might be more difficult than you think’.10
This review attempts to reconcile clinical trial data andbedside experience of fluid therapy with recent advances inmicrovascular physiology to improve our working paradigmfor rational prescribing.
Starling’s principleFrom experiments injecting serum or saline solution into thehindlimb of a dog, Starling deduced that the capillaries andpost-capillary venules behave as semi-permeable mem-branes absorbing fluid from the interstitial space.11 Thework of Krooh and colleagues12 developed Starling’s principlein human physiology. With adoption of reflection coeffi-cient13 and pore theories,14 the familiar paradigm of raisedvenous pressure and reduced plasma protein concentration
British Journal of Anaesthesia 108 (3): 384–94 (2012)Advance Access publication 29 January 2012 . doi:10.1093/bja/aer515
& The Author [2012]. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved.For Permissions, please email: [email protected]
by guest on April 5, 2013
http://bja.oxfordjournals.org/D
ownloaded from

leading to oedema in clinical practice emerged.12 15
Luft16 revealed ‘the fine structure of the capillary and theendocapillary layer’ in 1966, and Curry and Michel17 18 pro-posed a theory ‘that the molecular sieving properties of thecapillary wall reside in a matrix of molecular fibres whichcovers the endothelial cells and fills the channels throughor between them’ in 1980. Transvascular exchangedepends on a balance between hydrostatic and oncoticpressure gradients. Fluid is filtered to the interstitial spaceunder a dominant hydrostatic pressure gradient (capillarypressure Pc minus ISF pressure Pis) at the arteriolar portionof capillaries, and it was believed that it is absorbed backunder a dominant colloid osmotic pressure (COP) gradient(capillary COP pc minus ISF COP pis) at the venular end. In2004, Adamson and colleagues19 showed that the effect ofpis on transvascular fluid exchange is much less than pre-dicted by the standard Starling equation, which thereforehas to be revised.20 It is now established that non-fenestrated capillaries normally filter fluid to the ISF through-out their length. Absorption through venous capillaries andvenules does not occur. pc opposes, but does not reverse,filtration. Most of the filtered fluid returns to the circulationas lymph. Levick and Michel21 now propose that the smallpore system of the transvascular semi-permeable membraneis the endothelial glycocalyx layer (EGL) where it covers the
endothelial intercellular clefts, separating plasma from a‘protected region’ of the subglycocalyx space which isalmost protein-free. Subglycocalyx COP (psg) replaces pis asa determinant of transcapillary flow (Jv).19 22 Plasma pro-teins, including albumin, escape to the interstitial space bya relatively small number of large pores, which are respon-sible for the increased Jv observed in the early stage ofinflammation,21 and may be susceptible to pharmacologicalintervention.23 – 25 The fact that low protein concentrationwithin the subglycocalyx intercellular spaces accounts forthe low Jv and lymph flow in most tissues is a criticalinsight and the basis of the glycocalyx model.21
The endothelial glycocalyx layerThe EGL is a web of membrane-bound glycoproteins and pro-teoglycans on the luminal side of the endothelial cells,associated with various glycosaminoglycans (GAGs) (muco-polysaccharides) which contribute to the volume of thelayer (Fig. 1).26 It is the active interface between blood andthe capillary wall.27 Visualization of the EGL is technicallydemanding, but has helped to emphasize its physiologicalimportance.28 29 From indocyanine green dilution studies ofpatients given a large dose of i.v. colloid, the human EGLvolume was estimated to be about 700 ml,30 and presuming
Healthy glycocalyx layer whichcontains glycosaminoglycans
Compressed glycocalyx, sheddingor flaking glycosaminoglycans to theplasma
Endothelial cellErythrocyte
Endothelial glycocalyx layer
Glycosaminoglycans
Basement membrane/extracellular matrix
Fig 1 A cartoon illustrating that the intravascular volume contains the non-circulating glycocalyx fluid volume and the circulating plasmavolume. Red blood cells are excluded from the glycocalyx layer. Compaction of the glycocalyx layer increases plasma volume and the redcell dilution volume independently of changes in intravascular volume.
Transvascular exchange and fluid therapy BJA
385
by guest on April 5, 2013
http://bja.oxfordjournals.org/D
ownloaded from

pressure difference opposing filtration is maximal and Jv
becomes proportional to Pc, or transendothelial pressure dif-ference if Pis is not constant.
Table 1 Comparison of the original and revised paradigms for prescribing fluid therapy
Original Starling principle Revised Starling equation and glycocalyx model
Intravascular volume consists of plasma and cellular elements Intravascular volume consists of glycocalyx volume, plasma volume, andred cell distribution volume
Capillaries separate plasma with high protein concentration from ISFwith low protein concentration
Sinusoidal tissues (marrow, spleen, and liver) have discontinuous capillariesand their ISF is essentially part of the plasma volumeOpen fenestrated capillaries produce the renal glomerular filtrateDiaphragm fenestrated capillaries in specialized tissues can absorb ISF toplasmaContinuous capillaries exhibit ‘no absorption’The EGL is semi-permeable to anionic proteins and their concentration inthe intercellular clefts below the glycocalyx is very low
The important Starling forces are the transendothelial pressuredifference and the plasma–interstitial COP difference
The important Starling forces are the transendothelial pressure differenceand the plasma–subglycocalyx COP difference. ISF COP is not a directdeterminant of Jv
Fluid is filtered from the arterial end of capillaries and absorbed fromthe venous end. Small proportion returns to the circulation as lymph
Jv is much less than predicted by Starling’s principle, and the major routefor return to the circulation is as lymph
Raising plasma COP enhances absorption and shifts fluid from ISF toplasma
Raising plasma COP reduces Jv but does not cause absorption
At subnormal capillary pressure, net absorption increases plasmavolume
At subnormal capillary pressure, Jv approaches zero. Auto transfusion isacute, transient, and limited to about 500 ml
At supranormal capillary pressure, net filtration increases ISF volume At supranormal capillary pressure, when the COP difference is maximal, Jv isproportional to transendothelial pressure difference
Infused colloid solution is distributed through the plasma volume,and infused ISS through the extracellular volume
Infused colloid solution is initially distributed through the plasma volume,and infused ISS through the intravascular volumeAt supranormal capillary pressure, infusion of colloid solution preservesplasma COP, raises capillary pressure, and increases Jv
At supranormal capillary pressure, infusion of ISS also raises capillarypressure, but it lowers COP and so increases Jv more than the same colloidsolution volumeAt subnormal capillary pressure, infusion of colloid solution increasesplasma volume and infusion of ISS increases intravascular volume, but Jv
remains close to zero in both cases
Reduced COPNormal COPRaised COP
100
75
50
25
0
–25
10 20 mm Hg 30 40
Fig 3 Autotransfusion. Transendothelial filtration rate Jv is pro-portional to the capillary pressure, or transendothelial pressuredifference if interstitial pressure is not constant. Normal capillarypressure is nominally 20 mm Hg, and the scale for Jv is arbitrary,although studies show the rate of clearance from the intravascu-lar space during rapid infusion of Ringer’s acetate in humanscan be as much as 100 ml min21. Raising the plasma COPslows filtration (pink line), while reducing plasma COP increasesit (green line).
100
75
50
25
0
–25
Reduced COPNormal COPRaised COP
10 20 mm Hg 30 40
Fig 4 The no absorption rule. With less acute reduction in capil-lary pressure, the glycocalyx model preserves filtration at a verylow rate without a phase of absorption, the no absorption rule.We call the inflection on the filtration curve the J point.
BJA Woodcock and Woodcock
390
by guest on April 5, 2013
http://bja.oxfordjournals.org/D
ownloaded from

FISIOPATOLOGÍA
▸ Estiramiento de miocitos
▸ Activación neurohumoral: Estimulación inotrópica y cronotrópica
▸ Sistemas compensatorios: Catecolaminas- Taquicardia
▸ Desincronización ventricular
▸ Hipoxia. Aumento del gradiente a-A e hipocapnia
2014 ESC Guidelines on the diagnosis and management of acute pulmonar embolismJournal of Intensive Care Medicine. 2010. 26(5) 275-294

that RV ischaemia is of pathophysiological significance in the acutephase of PE.76 –78 Although RV infarction is uncommon after PE, itis likely that the imbalance between oxygen supply and demand canresult in damage to cardiomyocytes and further reduce contractileforces.
The detrimental effects of acute PE on the RV myocardium and thecirculation are summarized in Figure 1.
Respiratory failure in PE is predominantly a consequence ofhaemodynamic disturbances.79 Low cardiac output results in desat-uration of the mixed venous blood. In addition, zones of reducedflow in obstructed vessels, combined with zones of overflow in thecapillary bed served by non-obstructed vessels, result in ventila-tion–perfusion mismatch, which contributes to hypoxaemia. Inabout one-third of patients, right-to-left shunting through a patentforamen ovale can be detected by echocardiography: this is causedby an inverted pressure gradient between the right atrium and leftatrium and may lead to severe hypoxaemia and an increased risk ofparadoxical embolization and stroke.80 Finally, even if they do notaffect haemodynamics, small distal emboli may create areas of alveo-lar haemorrhage resulting in haemoptysis, pleuritis, and pleural effu-sion, which is usually mild. This clinical presentation is known as‘pulmonary infarction’. Its effect on gas exchange is normally mild,except in patients with pre-existing cardiorespiratory disease.
2.5 Clinical classification of pulmonaryembolism severityThe clinical classification of the severity of an episode of acute PE isbased on the estimated PE-related early mortality risk defined byin-hospital or 30-day mortality (Figure 2). This stratification, whichhas important implications both for the diagnostic and therapeuticstrategies proposed in these guidelines, is based on the patient’s clin-ical status at presentation, with high-risk PE being suspected or con-firmed in the presence of shock or persistent arterial hypotensionand not high-risk PE in their absence.
3. DiagnosisThroughout these Guidelines and for the purpose of clinical manage-ment, ‘confirmed PE’ is defined as a probability of PE high enough toindicate the need for PE-specific treatment, and ‘excluded PE’ as aprobability of PE low enough to justify withholding PE-specific treat-ment with an acceptably low risk.
3.1 Clinical presentationPE mayescapeprompt diagnosis since the clinical signs and symptomsare non-specific (Table 3). When the clinical presentation raises thesuspicion of PE in an individual patient, it should prompt furtherobjective testing. In most patients, PE is suspected on the basis of dys-pnoea, chest pain, pre-syncope or syncope, and/or haemoptysis.81–83
Arterial hypotension and shock are rare but important clinical pre-sentations, since they indicate central PE and/or a severely reducedhaemodynamic reserve. Syncope is infrequent, but mayoccur regard-less of the presence of haemodynamic instability.84 Finally, PE maybe completely asymptomatic and be discovered incidentally duringdiagnostic work-up for another disease or at autopsy.
Chest pain is a frequent symptom of PE and is usually caused bypleural irritation due to distal emboli causing pulmonary infarction.85
In central PE, chest pain may have a typical angina character, possiblyreflecting RV ischaemia and requiring differential diagnosis with acutecoronary syndrome (ACS) or aortic dissection. Dyspnoea may beacute and severe in central PE; in small peripheral PE, it is oftenmild and may be transient. In patients with pre-existing heart failureor pulmonary disease, worsening dyspnoea may be the onlysymptom indicative of PE.
Increased RV afterload
RV O2 deliveryTV insufficiency
RV wall tension
Neurohormonalactivation
Myocardialinflammation
RV O2 demand
RV ischaemia
RV coronaryperfusion
RV output RV contractility
Systemic BP
Cardiogenicshock
Death
RV dilatation
Low CO
LV pre-load
BP = blood pressure; CO = cardiac output; LV = left ventricular; RV = right ventricular; TV = tricuspid valve.
Figure 1 Key factors contributing to haemodynamic collapse inacute pulmonary embolism
Suspected acute PE
Shock or hypotensiona?
Yes No
High–riskb Not high–riskb
PE = pulmonary embolism.a
by ≥40 mm Hg, for >15 minutes, if not caused by new-onset arrhythmia, hypovolaemia, or sepsis.bBased on the estimated PE-related in-hospital or 30-day mortality.
Figure 2 Initial risk stratification of acute PE.
ESC Guidelines Page 7 of 48
by guest on September 8, 2014
http://eurheartj.oxfordjournals.org/D
ownloaded from

CUADRO CLÍNICO
Knowledge of the predisposing factors for VTE is important in de-termining the likelihood of PE, which increases with the number ofpredisposing factors present; however, in as many as 30% of thepatients with PE, no provoking factors can be detected.86 In bloodgas analysis, hypoxaemia is considered a typical finding in acute PE,but up to 40% of the patients have normal arterial oxygen saturationand 20% a normal alveolar-arterial oxygen gradient.87,88 Hypocapniais also often present. The chest X-ray is frequently abnormal and, al-though its findings are usually non-specific in PE, it is useful for exclud-ing other causes of dyspnoea or chest pain.89 Electrocardiographicchanges indicative of RV strain, such as inversion of T waves inleads V1–V4, a QR pattern in V1, S1Q3T3 pattern, and incompleteor complete right bundle-branch block, may be helpful. These elec-trocardiographic changes are usually found in more severe cases ofPE;90 in milder cases, the only anomaly may be sinus tachycardia,present in 40% of patients. Finally, atrial arrhythmias, most frequentlyatrial fibrillation, may be associated with acute PE.
3.2 Assessment of clinical probabilityDespite the limited sensitivity and specificity of individual symptoms,signs, and common tests, the combination of findings evaluated byclinical judgement or by the use of prediction rules allows to classifypatients with suspected PE into distinct categories of clinical orpre-test probability that correspond to an increasing actual preva-lence of confirmed PE. As the post-test (e.g. after computed tomog-raphy)probabilityof PE dependsnot onlyon the characteristics of thediagnostic test itself but alsoonpre-testprobability, this hasbecomeakey step in all diagnostic algorithms for PE.
The value of clinical judgement has been confirmed in several largeseries,91– 93 including the Prospective Investigation On PulmonaryEmbolism Diagnosis (PIOPED).94 Note that clinical judgementusually includes commonplace tests such as chest X-ray and electro-cardiogram for differential diagnosis. However, clinical judgementlacks standardization; therefore, several explicit clinical predictionrules have been developed. Of these, the most frequently used
prediction rule is the one offered by Wells et al. (Table 4).95 Thisrule has been validated extensively using both a three-categoryscheme (low, moderate, or high clinical probability of PE) and a two-categoryscheme (PE likelyorunlikely).96–100 It is simple andbasedoninformation that is easy to obtain; on the other hand, the weight ofone subjective item (‘alternative diagnosis less likely than PE’) mayreduce the inter-observer reproducibility of the Wells rule.101 –103
The revised Geneva rule is also simple and standardized(Table 4).93 Both have been adequately validated.104– 106
More recently, both the Wells and the revised Geneva rule weresimplified in an attempt to increase their adoption into clinical prac-tice (Table 4),107,108 and the simplified versions were externally vali-dated.105,109 Whichever is used, the proportion of patients withconfirmed PE can be expected to be around 10% in the low-probability category, 30% in the moderate-probability category,and 65% in the high-clinical probability category when using thethree-level classification.104 When the two-level classification isused, the proportion of patients with confirmed PE in the PE-unlikelycategory is around 12%.104
3.3 D-dimer testingD-dimer levels are elevated in plasma in the presence of acute throm-bosis, because of simultaneous activation of coagulation and fibrin-olysis, The negative predictive value of D-dimer testing is high and anormal D-dimer level renders acute PE or DVT unlikely. On theother hand, fibrin is also produced in a wide variety of conditionssuch as cancer, inflammation, bleeding, trauma, surgery and necrosis.Accordingly, the positive predictive value of elevated D-dimer levelsis low and D-dimer testing is not useful for confirmation of PE.
A number of D-dimer assays are available.110,111 The quantitativeenzyme-linked immunosorbent assay (ELISA) or ELISA-derivedassays have a diagnostic sensitivity of 95% or better and can thereforebe used to exclude PE in patients with either a low or a moderatepre-test probability. In the emergency department, a negative ELISAD-dimer, in combination with clinical probability, can exclude thedisease without further testing in approximately 30% of patientswith suspected PE.100,112,113 Outcome studies have shown that thethree-month thromboembolic risk was ,1% in patients left untreatedon the basis of a negative test result (Table 5);99,112–116 these findingswere confirmed by a meta-analysis.117
Quantitative latex-derived assays and a whole-blood agglutinationassay have a diagnostic sensitivity ,95% and are thus often referredto as moderately sensitive. In outcome studies, those assays provedsafe in ruling out PE in PE-unlikely patients as well as in patientswith a low clinical probability.99,100,105 Their safety in ruling out PEhas not been established in the intermediate clinical probability cat-egory. Point-of-care tests have moderate sensitivity, and data fromoutcome studies in PE are lacking, with the exception of a recentprimary care-based study using the Simplify D-dimer assay,118 inwhich the three-month thromboembolic risk was 1.5% in PE-unlikelypatients with a negative D-dimer.
The specificity of D-dimer in suspected PE decreases steadily withage, to almost 10% in patients .80 years.119 Recent evidence sug-gests using age-adjusted cut-offs to improve the performance ofD-dimer testing in the elderly.120,121 In a recent meta-analysis,age-adjusted cut-off values (age x 10 mg/L above 50 years) allowedincreasing specificity from 34–46% while retaining a sensitivity
Table 3 Clinical characteristics of patients withsuspected PE in the emergency department (adaptedfrom Pollack et al. (2011)).82
Feature(n = 1880) (n = 528)
Dyspnoea 50% 51%
Pleuritic chest pain 39% 28%
Cough 23% 23%
Substernal chest pain 15% 17%
Fever 10% 10%
Haemoptysis 8% 4%
Syncope 6% 6%
Unilateral leg pain 6% 5%
Signs of DVT (unilateral extremity swelling) 24% 18%
DVT ¼ deep vein thrombosis.
ESC GuidelinesPage 8 of 48
by guest on September 8, 2014
http://eurheartj.oxfordjournals.org/D
ownloaded from
2014 ESC Guidelines on the diagnosis and management of acute pulmonar embolism

ABORDAJE
▸ Reglas de predicción estandarizada
▸ Wells o Ginebra
▸ Probabilidad clínica de la enfermedad
▸ 10% baja probabilidad
▸ 35% probabilidad intermedia
▸ 65% alta probabilidad
JACC. VOL.67, NO.8. 2016

above 97%.122 A multicentre, prospective management study evalu-ated this age-adjusted cut-off in a cohort of 3346 patients. Patientswith anormal age-adjustedD-dimer valuedidnotundergocomputedtomographic pulmonary angiography and were left untreated andformally followed up for a three-month period. Among the 766patients whowere75 years orolder, 673 had anon-high clinical prob-ability. On the basis of D-dimer, using the age-adjusted cut-off
(instead of the ‘standard’ 500 mg/L cut-off) increased the numberof patients in whom PE could be excluded from 43 (6.4%; 95% CI4.8–8.5%) to 200 (29.7%; 95% CI 26.4–33.3%), without any addition-al false-negative findings.123 D-dimer is also more frequently elevatedin patients with cancer,124,125 in hospitalized patients,105,126 andduring pregnancy.127,128 Thus, the number of patients in whomD-dimer must be measured to exclude one PE (number needed to
Table 4 Clinical prediction rules for PE
Items Clinical decision rule points
Wells rule Original version Simplified version
Simplified version
95 107
Previous PE or DVT 1.5 1
Heart rate ≥100 b.p.m. 1.5 1
Surgery or immobilization within the past four weeks 1.5 1
Haemoptysis 1 1
Active cancer 1 1
Clinical signs of DVT 3 1
Alternative diagnosis less likely than PE 3 1
Clinical probability
Three-level score
Low 0–1 N/A
Intermediate 2–6 N/A
High ≥7 N/A
Two-level score
PE unlikely 0–4 0–1
PE likely ≥5 ≥2
Revised Geneva score Original version93 108
Previous PE or DVT 3 1
Heart rate75–94 b.p.m.≥95 b.p.m.
35
12
Surgery or fracture within the past month 2 1
Haemoptysis 2 1
Active cancer 2 1
Unilateral lower limb pain 3 1
Pain on lower limb deep venous palpation and unilateral oedema 4 1
Age >65 years 1 1
Clinical probability
Three-level score
Low 0–3 0–1
Intermediate 4–10 2–4
High ≥11 ≥5
Two-level score
PE unlikely 0–5 0–2
PE likely ≥6 ≥3
b.p.m.¼ beats per minute; DVT ¼ deep vein thrombosis; PE ¼ pulmonary embolism.
ESC Guidelines Page 9 of 48
by guest on September 8, 2014
http://eurheartj.oxfordjournals.org/D
ownloaded from
2014 ESC Guidelines on the diagnosis and management of acute pulmonar embolism

above 97%.122 A multicentre, prospective management study evalu-ated this age-adjusted cut-off in a cohort of 3346 patients. Patientswith anormal age-adjustedD-dimer valuedidnotundergocomputedtomographic pulmonary angiography and were left untreated andformally followed up for a three-month period. Among the 766patients whowere75 years orolder, 673 had anon-high clinical prob-ability. On the basis of D-dimer, using the age-adjusted cut-off
(instead of the ‘standard’ 500 mg/L cut-off) increased the numberof patients in whom PE could be excluded from 43 (6.4%; 95% CI4.8–8.5%) to 200 (29.7%; 95% CI 26.4–33.3%), without any addition-al false-negative findings.123 D-dimer is also more frequently elevatedin patients with cancer,124,125 in hospitalized patients,105,126 andduring pregnancy.127,128 Thus, the number of patients in whomD-dimer must be measured to exclude one PE (number needed to
Table 4 Clinical prediction rules for PE
Items Clinical decision rule points
Wells rule Original version Simplified version
Simplified version
95 107
Previous PE or DVT 1.5 1
Heart rate ≥100 b.p.m. 1.5 1
Surgery or immobilization within the past four weeks 1.5 1
Haemoptysis 1 1
Active cancer 1 1
Clinical signs of DVT 3 1
Alternative diagnosis less likely than PE 3 1
Clinical probability
Three-level score
Low 0–1 N/A
Intermediate 2–6 N/A
High ≥7 N/A
Two-level score
PE unlikely 0–4 0–1
PE likely ≥5 ≥2
Revised Geneva score Original version93 108
Previous PE or DVT 3 1
Heart rate75–94 b.p.m.≥95 b.p.m.
35
12
Surgery or fracture within the past month 2 1
Haemoptysis 2 1
Active cancer 2 1
Unilateral lower limb pain 3 1
Pain on lower limb deep venous palpation and unilateral oedema 4 1
Age >65 years 1 1
Clinical probability
Three-level score
Low 0–3 0–1
Intermediate 4–10 2–4
High ≥11 ≥5
Two-level score
PE unlikely 0–5 0–2
PE likely ≥6 ≥3
b.p.m.¼ beats per minute; DVT ¼ deep vein thrombosis; PE ¼ pulmonary embolism.
ESC Guidelines Page 9 of 48
by guest on September 8, 2014
http://eurheartj.oxfordjournals.org/D
ownloaded from
2014 ESC Guidelines on the diagnosis and management of acute pulmonar embolism

that RV ischaemia is of pathophysiological significance in the acutephase of PE.76 –78 Although RV infarction is uncommon after PE, itis likely that the imbalance between oxygen supply and demand canresult in damage to cardiomyocytes and further reduce contractileforces.
The detrimental effects of acute PE on the RV myocardium and thecirculation are summarized in Figure 1.
Respiratory failure in PE is predominantly a consequence ofhaemodynamic disturbances.79 Low cardiac output results in desat-uration of the mixed venous blood. In addition, zones of reducedflow in obstructed vessels, combined with zones of overflow in thecapillary bed served by non-obstructed vessels, result in ventila-tion–perfusion mismatch, which contributes to hypoxaemia. Inabout one-third of patients, right-to-left shunting through a patentforamen ovale can be detected by echocardiography: this is causedby an inverted pressure gradient between the right atrium and leftatrium and may lead to severe hypoxaemia and an increased risk ofparadoxical embolization and stroke.80 Finally, even if they do notaffect haemodynamics, small distal emboli may create areas of alveo-lar haemorrhage resulting in haemoptysis, pleuritis, and pleural effu-sion, which is usually mild. This clinical presentation is known as‘pulmonary infarction’. Its effect on gas exchange is normally mild,except in patients with pre-existing cardiorespiratory disease.
2.5 Clinical classification of pulmonaryembolism severityThe clinical classification of the severity of an episode of acute PE isbased on the estimated PE-related early mortality risk defined byin-hospital or 30-day mortality (Figure 2). This stratification, whichhas important implications both for the diagnostic and therapeuticstrategies proposed in these guidelines, is based on the patient’s clin-ical status at presentation, with high-risk PE being suspected or con-firmed in the presence of shock or persistent arterial hypotensionand not high-risk PE in their absence.
3. DiagnosisThroughout these Guidelines and for the purpose of clinical manage-ment, ‘confirmed PE’ is defined as a probability of PE high enough toindicate the need for PE-specific treatment, and ‘excluded PE’ as aprobability of PE low enough to justify withholding PE-specific treat-ment with an acceptably low risk.
3.1 Clinical presentationPE mayescapeprompt diagnosis since the clinical signs and symptomsare non-specific (Table 3). When the clinical presentation raises thesuspicion of PE in an individual patient, it should prompt furtherobjective testing. In most patients, PE is suspected on the basis of dys-pnoea, chest pain, pre-syncope or syncope, and/or haemoptysis.81–83
Arterial hypotension and shock are rare but important clinical pre-sentations, since they indicate central PE and/or a severely reducedhaemodynamic reserve. Syncope is infrequent, but mayoccur regard-less of the presence of haemodynamic instability.84 Finally, PE maybe completely asymptomatic and be discovered incidentally duringdiagnostic work-up for another disease or at autopsy.
Chest pain is a frequent symptom of PE and is usually caused bypleural irritation due to distal emboli causing pulmonary infarction.85
In central PE, chest pain may have a typical angina character, possiblyreflecting RV ischaemia and requiring differential diagnosis with acutecoronary syndrome (ACS) or aortic dissection. Dyspnoea may beacute and severe in central PE; in small peripheral PE, it is oftenmild and may be transient. In patients with pre-existing heart failureor pulmonary disease, worsening dyspnoea may be the onlysymptom indicative of PE.
Increased RV afterload
RV O2 deliveryTV insufficiency
RV wall tension
Neurohormonalactivation
Myocardialinflammation
RV O2 demand
RV ischaemia
RV coronaryperfusion
RV output RV contractility
Systemic BP
Cardiogenicshock
Death
RV dilatation
Low CO
LV pre-load
BP = blood pressure; CO = cardiac output; LV = left ventricular; RV = right ventricular; TV = tricuspid valve.
Figure 1 Key factors contributing to haemodynamic collapse inacute pulmonary embolism
Suspected acute PE
Shock or hypotensiona?
Yes No
High–riskb Not high–riskb
PE = pulmonary embolism.a
by ≥40 mm Hg, for >15 minutes, if not caused by new-onset arrhythmia, hypovolaemia, or sepsis.bBased on the estimated PE-related in-hospital or 30-day mortality.
Figure 2 Initial risk stratification of acute PE.
ESC Guidelines Page 7 of 48
by guest on September 8, 2014
http://eurheartj.oxfordjournals.org/D
ownloaded from
2014 ESC Guidelines on the diagnosis and management of acute pulmonar embolism

contraindication toCT. Also,V/Qscintigraphy may bepreferredoverCT to avoid unnecessary radiation, particularly in younger and femalepatients in whom thoracic CT may raise the lifetime risk of breastcancer.139 V/Q lung scintigraphy is diagnostic (with either normalor high-probability findings) in approximately 30–50% of emergencyward patients with suspected PE.83,94,135,203 The proportion of diag-nostic V/Q scans is higher in patients with a normal chest X-ray, andthis supports the recommendation to use V/Q scan as the first-lineimaging test for PE in younger patients.204
The number of patients with inconclusive findings may also bereduced by taking into account clinical probability.94 Thus, patientswith a non-diagnostic lung scan and low clinical probability of PEhavea lowprevalence of confirmedPE.94,157,203 The negativepredict-ive value of this combination is further increased by the absence of aDVT on lower-limb CUS. If a high-probability lung scan is obtainedfrom a patient with low clinical probability of PE, confirmation byother tests may be considered on a case-by-case basis.
3.11 Areas of uncertaintyDespite considerable progress in the diagnosis of PE, several areas ofuncertainty persist. The diagnostic value and clinical significance ofsub-segmental defects on MDCT are still under debate.136,137 Arecent retrospective analysis of two patient cohorts with suspectedPE showed similar outcomes (in terms of three-month recurrence
and mortality rates) between patients with sub-segmental andmore proximal PE; outcomes were largely determined by comorbid-ities.205 The definition of sub-segmental PE has yet to be standardizedand a single sub-segmental defect probably does not have the sameclinical relevance as multiple, sub-segmental thrombi.
There is also growing evidence suggesting over-diagnosis ofPE.206 A randomized comparison showed that, although CTdetected PE more frequently than V/Q scanning, three-month out-comes were similar, regardless of the diagnostic method used.135
Data from the United States show an 80% rise in the apparent in-cidence of PE after the introduction of CT, without a significantimpact on mortality.207,208
Some experts believe that patients with incidental (unsuspected)PE on CT should be treated,144 especially if they have cancer and aproximal clot, but solid evidence in support of this recommendationis lacking. The value and cost-effectiveness of CUS in suspected PEshould be further clarified.
Finally, ‘triple rule-out’ (for coronary artery disease, PE and aorticdissection) CT angiography for patients presenting with non-traumatic chest pain appears to be accurate for the detection of cor-onary artery disease.209 However, the benefits vs. risks (includingincreased radiation and contrast exposure) of such a diagnostic ap-proach need thorough evaluation, given the low (,1%) prevalenceof PE and aortic dissection in the studies published thus far.
Suspected PE without shock or hypotension
Assess clinical probability of PEClinical judgment or prediction rulea
D-dimer
CT angiography
positive
CT angiography
negative
Low/intermediate clinical probabilityor PE unlikely
no PE PE confirmedc no PE PE confirmedc
High clinical probabilityor PE likely
No treatmentb Treatmentb No treatmentb
or investigate furtherd Treatmentb
CT = computed tomographic; PE = pulmonary embolism.a
two-level scheme (PE unlikely or PE likely). When using a moderately sensitive assay, D-dimer measurement should be restricted to patients with low clinical probability or a
use in suspected PE occurring in hospitalized patients.bTreatment refers to anticoagulation treatment for PE.cCT angiogram is considered to be diagnostic of PE if it shows PE at the segmental or more proximal level. d
Figure 4 Proposed diagnostic algorithm for patients with suspected not high-risk pulmonary embolism.
ESC GuidelinesPage 14 of 48
by guest on September 8, 2014
http://eurheartj.oxfordjournals.org/D
ownloaded from
2014 ESC Guidelines on the diagnosis and management of acute pulmonar embolism

3.10.2 Suspected pulmonary embolism without shockor hypotensionStrategy based on computed tomographic angiography (Figure 4)
Computed tomographic angiography has become the main thor-acic imaging test for investigating suspected PE but, since mostpatients with suspected PE do not have the disease, CT should notbe the first-line test.
In patients admitted to the emergency department, plasmaD-dimer measurement, combined with clinical probability assess-ment, is the logical first step and allows PE to be ruled out inaround 30% of patients, with a three-month thromboembolic riskin patients left untreated of ,1%. D-dimer should not be measuredin patients with a high clinical probability, owing to a low negative pre-dictive value in this population.202 It is also less useful in hospitalizedpatients because the number needed to test to obtain a clinically rele-vant negative result is high.
In most centres, MDCT angiography is the second-line test inpatients with an elevated D-dimer level and the first-line test inpatients with a high clinical probability. CT angiography is considered
to be diagnostic of PE when it shows a clot at least at the segmentallevel of the pulmonary arterial tree. False-negative results ofMDCT have been reported in patients with a high clinical probabilityof PE;134 however, this situation is infrequent, and the three-monththromboembolic risk was low in these cases.99 Therefore, both thenecessity of performing further tests and the nature of these testsin such patients remain controversial.
Value of lower limb compression ultrasonographyUnder certain circumstances, CUS can still be useful in the
diagnostic work-up of suspected PE. CUS shows a DVT in 30–50%of patients with PE,116,192,193 and finding proximal DVT in a patientsuspected of PE is sufficient to warrant anticoagulant treatmentwithout further testing.194 Hence, performing CUS before CT maybe an option in patients with relative contraindications for CT suchas in renal failure, allergy to contrast dye, or pregnancy.195,196
Value of ventilation–perfusion scintigraphyIn centres in which V/Q scintigraphy is readily available, it
remains a valid option for patients with an elevated D-dimer and a
Suspected PE with shock or hypotension
CT angiography immediately available
Echocardiography
RV overloadb
Noa Yes
No
Search for other causesof haemodynamic instability
PE-specific treatment:primary reperfusionc
Search for other causesof haemodynamic instability
Yes
No other test availableb
or patient unstablepositive negative
CT angiographyCT angiography
available and
patient stabilized
CT = computed tomographic; PE = pulmonary embolism; RV = right ventricle.aIncludes the cases in which the patient’s condition is so critical that it only allows bedside diagnostic tests.b
chambers. Ancillary bedside imaging tests include transoesophageal echocardiography, which may detect emboli in the pulmonary artery and its main branches, and bilateral
cThrombolysis; alternatively, surgical embolectomy or catheter-directed treatment (Section 5).
Figure 3 Proposed diagnostic algorithm for patients with suspected high-risk PE, i.e. presenting with shock or hypotension.
ESC Guidelines Page 13 of 48
by guest on September 8, 2014
http://eurheartj.oxfordjournals.org/D
ownloaded from
2014 ESC Guidelines on the diagnosis and management of acute pulmonar embolism
IM - REVIEW
Risk stratification of patients with acute symptomatic pulmonaryembolism
David Jimenez1 • Jose Luis Lobo2 • Deisy Barrios1 • Paolo Prandoni3 •
Roger D. Yusen4
Received: 5 November 2015 / Accepted: 30 December 2015 / Published online: 14 January 2016! SIMI 2016
Abstract Patients with acute symptomatic pulmonaryembolism (PE) who present with arterial hypotension or
shock have a high risk of death (high-risk PE), and treat-
ment guidelines recommend strong consideration ofthrombolysis in this setting. For normotensive patients
diagnosed with PE, risk stratification should aim to dif-
ferentiate the group of patients deemed as having a low riskfor early complications (all-cause mortality, recurrent
venous thromboembolism, and major bleeding) (low-risk
PE) from the group of patients at higher risk for PE-relatedcomplications (intermediate-high risk PE), so low-risk
patients could undergo consideration of early outpatient
treatment of PE and intermediate-high risk patients wouldundergo close observation and consideration of thrombol-
ysis. Clinicians should also use risk stratification and eli-
gibility criteria to identify a third group of patients thatshould not undergo escalated or home therapy (intermedi-
ate-low risk PE). Such patients should initiate standard
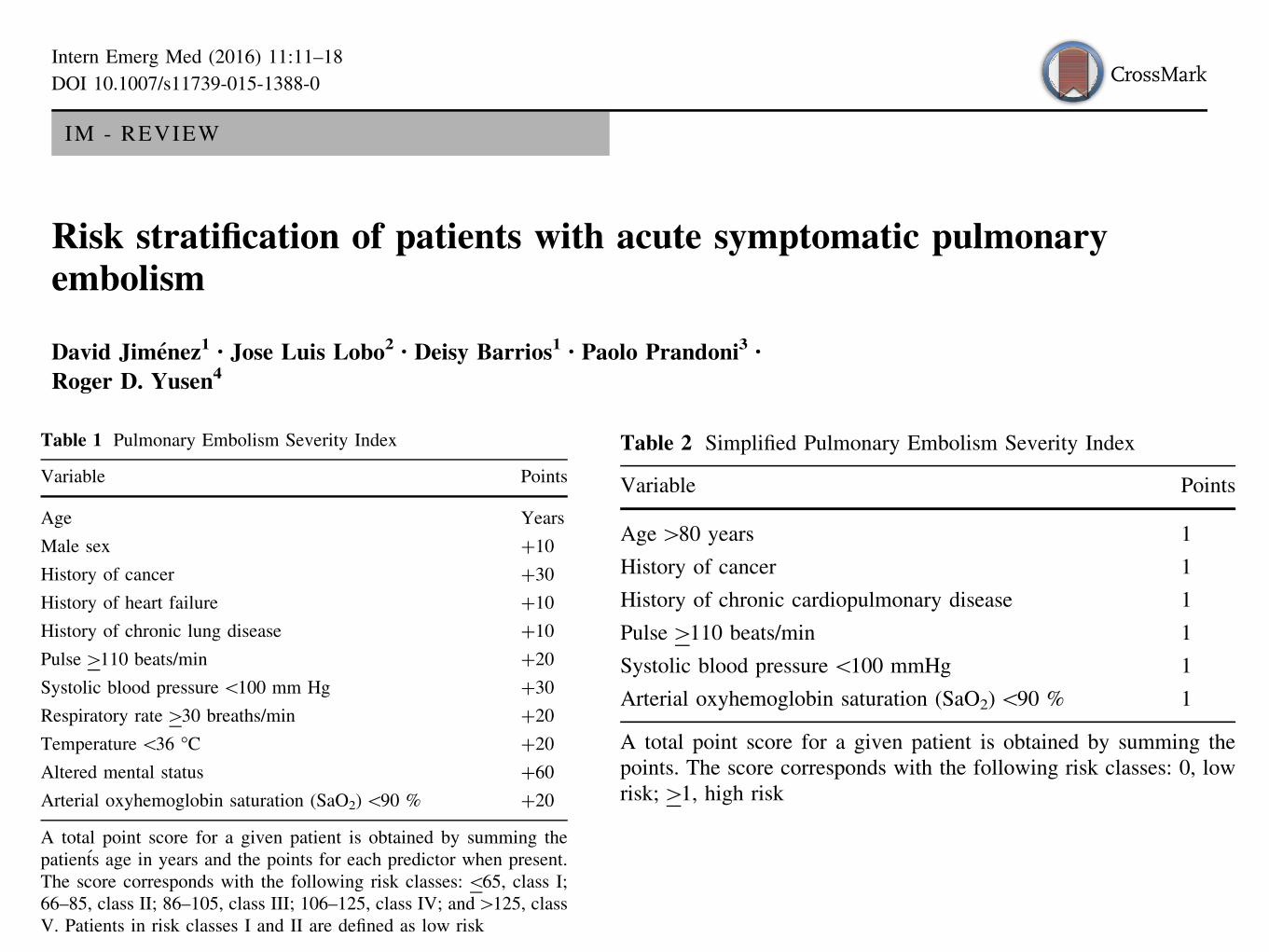
therapy of PE while in the hospital. Clinical models [e.g.,Pulmonary Embolism Severity Index (PESI), simplified
PESI (sPESI)] may accurately identify those at low risk ofdying shortly after the diagnosis of PE. For identification of
intermediate-high risk patients with acute PE, studies havevalidated predictive models that use a combination of
clinical, laboratory and imaging variables.
Keywords Pulmonary embolism ! Prognosis ! Mortality !Survival
Introduction
Pulmonary embolism (PE) remains one of the leadingcauses of cardiovascular morbidity and mortality. How-
ever, patients with PE have a heterogeneous presentation
and prognosis. While treated PE has a short-term mortalityof 2 % in normotensive patients who do not have evidence
of right ventricular (RV) dysfunction, the mortality rate
rises up to 30 % in patients with shock, and up to 65 % inpatients with cardiac arrest at presentation [1].
The key to an effective treatment of PE in the acute
phase lies in the assessment of the patient’s prognosis.High-risk PE is characterized by the presence of PE-asso-
ciated arterial hypotension or shock, and has a short-term
mortality of at least 15 % [2]. For patients with high-riskPE, guidelines generally recommend consideration of
treatment with thrombolytic agents [3–5]. For normoten-sive patients diagnosed with PE, risk stratification should
aim to differentiate the group of patients deemed as having
a low risk for early complications (low-risk PE) who mightbenefit from an abbreviated hospital stay or outpatient
therapy, from the group of patients with preserved systemic
arterial pressure deemed as having a high risk for a com-plicated course (intermediate-high risk PE) who might
benefit from an escalation of therapy. Clinicians should
also use risk stratification and eligibility criteria to identifya third group of patients who should not undergo escalated
& David [email protected]; [email protected]
1 Respiratory Department and Medicine Department, Ramon yCajal Hospital and Alcala de Henares University, IRYCIS,28034 Madrid, Spain
2 Respiratory Department, Hospital Araba, Vitoria, Spain
3 Department of Cardiovascular Sciences, Vascular MedicineUnit, University Hospital of Padua, Padua, Italy
4 Divisions of Pulmonary and Critical Care Medicine andGeneral Medical Sciences, Washington UniversitySchool of Medicine, St. Louis, MO, USA
123
Intern Emerg Med (2016) 11:11–18
DOI 10.1007/s11739-015-1388-0
through V) of increasing risk of mortality within 30 days of
hospitalization. Patients in classes I and II are categorizedas low risk, while patients in classes III, IV and V are
categorized as high risk. Multiple retrospective and
prospective studies have validated the prognostic accuracyof the PESI [14–16]. Furthermore, a trial that randomized
patients with acute PE and a low risk of complications
(according to the PESI) to receive low-molecular-weightheparin entirely out of the hospital (discharged within
24 h) vs. at least partly in hospital further validated the
PESI [17]. This study suggests that treating appropriatelyselected patients with acute PE at home does not increase
recurrent VTE, bleeding, or mortality.
Investigators derived and externally validated a simpli-fied version of the PESI [18]. The simplified PESI (sPESI)
includes the variables of age ([80 years vs. other), history
of cancer (yes/no), history of chronic cardiopulmonarydisease (yes/no), heart rate ([110 beats/min vs. other),
systolic blood pressure (\100 mmHg vs. other), and oxy-
hemoglobin saturation (\90 % vs. other). The sPESI cat-egorizes patients with none of the variables present as low
risk, and those with any variable present as high risk
(Table 2). In an external validation cohort of 7106 patientsincluded in the RIETE registry, the 36.1 % (2569/7106) of
patients classified by the sPESI as having a low risk of
death had a 30-day all-cause mortality of 1.1 % (28 of2569 patients; 95 % CI, 0.7–1.5 %), while the high-risk
group had a 30-day all-cause mortality of 8.9 % (95 % CI,
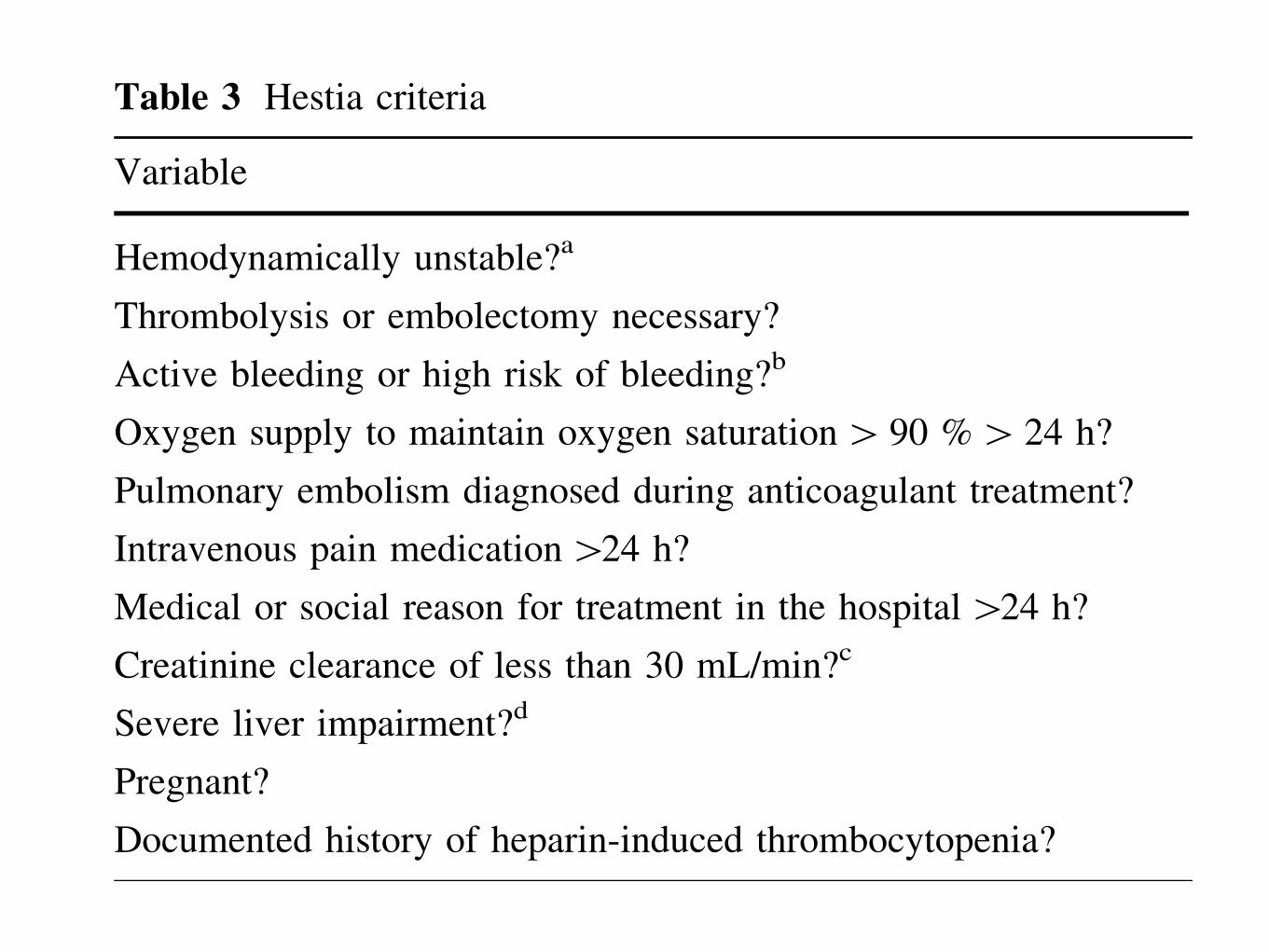
8.1–9.8 %).The Hestia criteria comprise a set of clinical parameters
that can easily be obtained at the bedside (Table 3). In a
single-arm management trial that used these criteria to
select candidates for home treatment, the rate of recurrent
VTE was 2.0 % (95 % CI, 0.8–4.3 %) in patients with
acute PE who were discharged within 24 h [19]. A vali-dation study of the Hestia criteria has not yet been
published.
A recent systematic review and metaanalysis assessedthe prognostic accuracy of different clinical prediction
rules to identify PE patients at low risk for early mortality,and thus, suitable for outpatient treatment or early hospital
Table 1 Pulmonary Embolism Severity Index
Variable Points
Age Years
Male sex ?10
History of cancer ?30
History of heart failure ?10
History of chronic lung disease ?10
Pulse[110 beats/min ?20
Systolic blood pressure\100 mm Hg ?30
Respiratory rate[30 breaths/min ?20
Temperature\36 !C ?20
Altered mental status ?60
Arterial oxyhemoglobin saturation (SaO2)\90 % ?20
A total point score for a given patient is obtained by summing thepatients age in years and the points for each predictor when present.The score corresponds with the following risk classes:\65, class I;66–85, class II; 86–105, class III; 106–125, class IV; and[125, classV. Patients in risk classes I and II are defined as low risk
Table 2 Simplified Pulmonary Embolism Severity Index
Variable Points
Age[80 years 1
History of cancer 1
History of chronic cardiopulmonary disease 1
Pulse[110 beats/min 1
Systolic blood pressure\100 mmHg 1
Arterial oxyhemoglobin saturation (SaO2)\90 % 1
A total point score for a given patient is obtained by summing thepoints. The score corresponds with the following risk classes: 0, lowrisk;[1, high risk
Table 3 Hestia criteria
Variable
Hemodynamically unstable?a
Thrombolysis or embolectomy necessary?
Active bleeding or high risk of bleeding?b
Oxygen supply to maintain oxygen saturation[ 90 %[ 24 h?
Pulmonary embolism diagnosed during anticoagulant treatment?
Intravenous pain medication[24 h?
Medical or social reason for treatment in the hospital[24 h?
Creatinine clearance of less than 30 mL/min?c
Severe liver impairment?d
Pregnant?
Documented history of heparin-induced thrombocytopenia?
If one of the questions is answered with YES, the patient can NOT betreated at homea Include the following criteria, but are left to the discretion of theinvestigator: systolic blood pressure \100 mmHg with heart rate[100 beats per minute; condition requiring admission to an intensivecare unitb Gastrointestinal bleeding in the preceding 14 days, recent stroke(less than 4 weeks ago), recent operation (less than 2 weeks ago),bleeding disorder or thrombocytopenia (platelet count\75 9 109/L),uncontrolled hypertension (systolic blood pressure[180 mm Hg ordiastolic blood pressure[110 mm Hg)c Calculated creatinine clearance according to the Cockcroft-Gaultformulad Left to the discretion of the physician
Intern Emerg Med (2016) 11:11–18 13
123
through V) of increasing risk of mortality within 30 days of
hospitalization. Patients in classes I and II are categorizedas low risk, while patients in classes III, IV and V are
categorized as high risk. Multiple retrospective and
prospective studies have validated the prognostic accuracyof the PESI [14–16]. Furthermore, a trial that randomized
patients with acute PE and a low risk of complications
(according to the PESI) to receive low-molecular-weightheparin entirely out of the hospital (discharged within
24 h) vs. at least partly in hospital further validated the
PESI [17]. This study suggests that treating appropriatelyselected patients with acute PE at home does not increase
recurrent VTE, bleeding, or mortality.
Investigators derived and externally validated a simpli-fied version of the PESI [18]. The simplified PESI (sPESI)
includes the variables of age ([80 years vs. other), history
of cancer (yes/no), history of chronic cardiopulmonarydisease (yes/no), heart rate ([110 beats/min vs. other),
systolic blood pressure (\100 mmHg vs. other), and oxy-
hemoglobin saturation (\90 % vs. other). The sPESI cat-egorizes patients with none of the variables present as low
risk, and those with any variable present as high risk
(Table 2). In an external validation cohort of 7106 patientsincluded in the RIETE registry, the 36.1 % (2569/7106) of
patients classified by the sPESI as having a low risk of
death had a 30-day all-cause mortality of 1.1 % (28 of2569 patients; 95 % CI, 0.7–1.5 %), while the high-risk
group had a 30-day all-cause mortality of 8.9 % (95 % CI,
8.1–9.8 %).The Hestia criteria comprise a set of clinical parameters
that can easily be obtained at the bedside (Table 3). In a
single-arm management trial that used these criteria to
select candidates for home treatment, the rate of recurrent
VTE was 2.0 % (95 % CI, 0.8–4.3 %) in patients with
acute PE who were discharged within 24 h [19]. A vali-dation study of the Hestia criteria has not yet been
published.
A recent systematic review and metaanalysis assessedthe prognostic accuracy of different clinical prediction
rules to identify PE patients at low risk for early mortality,and thus, suitable for outpatient treatment or early hospital
Table 1 Pulmonary Embolism Severity Index
Variable Points
Age Years
Male sex ?10
History of cancer ?30
History of heart failure ?10
History of chronic lung disease ?10
Pulse[110 beats/min ?20
Systolic blood pressure\100 mm Hg ?30
Respiratory rate[30 breaths/min ?20
Temperature\36 !C ?20
Altered mental status ?60
Arterial oxyhemoglobin saturation (SaO2)\90 % ?20
A total point score for a given patient is obtained by summing thepatients age in years and the points for each predictor when present.The score corresponds with the following risk classes:\65, class I;66–85, class II; 86–105, class III; 106–125, class IV; and[125, classV. Patients in risk classes I and II are defined as low risk
Table 2 Simplified Pulmonary Embolism Severity Index
Variable Points
Age[80 years 1
History of cancer 1
History of chronic cardiopulmonary disease 1
Pulse[110 beats/min 1
Systolic blood pressure\100 mmHg 1
Arterial oxyhemoglobin saturation (SaO2)\90 % 1
A total point score for a given patient is obtained by summing thepoints. The score corresponds with the following risk classes: 0, lowrisk;[1, high risk
Table 3 Hestia criteria
Variable
Hemodynamically unstable?a
Thrombolysis or embolectomy necessary?
Active bleeding or high risk of bleeding?b
Oxygen supply to maintain oxygen saturation[ 90 %[ 24 h?
Pulmonary embolism diagnosed during anticoagulant treatment?
Intravenous pain medication[24 h?
Medical or social reason for treatment in the hospital[24 h?
Creatinine clearance of less than 30 mL/min?c
Severe liver impairment?d
Pregnant?
Documented history of heparin-induced thrombocytopenia?
If one of the questions is answered with YES, the patient can NOT betreated at homea Include the following criteria, but are left to the discretion of theinvestigator: systolic blood pressure \100 mmHg with heart rate[100 beats per minute; condition requiring admission to an intensivecare unitb Gastrointestinal bleeding in the preceding 14 days, recent stroke(less than 4 weeks ago), recent operation (less than 2 weeks ago),bleeding disorder or thrombocytopenia (platelet count\75 9 109/L),uncontrolled hypertension (systolic blood pressure[180 mm Hg ordiastolic blood pressure[110 mm Hg)c Calculated creatinine clearance according to the Cockcroft-Gaultformulad Left to the discretion of the physician
Intern Emerg Med (2016) 11:11–18 13
123
through V) of increasing risk of mortality within 30 days of
hospitalization. Patients in classes I and II are categorizedas low risk, while patients in classes III, IV and V are
categorized as high risk. Multiple retrospective and
prospective studies have validated the prognostic accuracyof the PESI [14–16]. Furthermore, a trial that randomized
patients with acute PE and a low risk of complications
(according to the PESI) to receive low-molecular-weightheparin entirely out of the hospital (discharged within
24 h) vs. at least partly in hospital further validated the
PESI [17]. This study suggests that treating appropriatelyselected patients with acute PE at home does not increase
recurrent VTE, bleeding, or mortality.
Investigators derived and externally validated a simpli-fied version of the PESI [18]. The simplified PESI (sPESI)
includes the variables of age ([80 years vs. other), history
of cancer (yes/no), history of chronic cardiopulmonarydisease (yes/no), heart rate ([110 beats/min vs. other),
systolic blood pressure (\100 mmHg vs. other), and oxy-
hemoglobin saturation (\90 % vs. other). The sPESI cat-egorizes patients with none of the variables present as low
risk, and those with any variable present as high risk
(Table 2). In an external validation cohort of 7106 patientsincluded in the RIETE registry, the 36.1 % (2569/7106) of
patients classified by the sPESI as having a low risk of
death had a 30-day all-cause mortality of 1.1 % (28 of2569 patients; 95 % CI, 0.7–1.5 %), while the high-risk
group had a 30-day all-cause mortality of 8.9 % (95 % CI,
8.1–9.8 %).The Hestia criteria comprise a set of clinical parameters
that can easily be obtained at the bedside (Table 3). In a
single-arm management trial that used these criteria to
select candidates for home treatment, the rate of recurrent
VTE was 2.0 % (95 % CI, 0.8–4.3 %) in patients with
acute PE who were discharged within 24 h [19]. A vali-dation study of the Hestia criteria has not yet been
published.
A recent systematic review and metaanalysis assessedthe prognostic accuracy of different clinical prediction
rules to identify PE patients at low risk for early mortality,and thus, suitable for outpatient treatment or early hospital
Table 1 Pulmonary Embolism Severity Index
Variable Points
Age Years
Male sex ?10
History of cancer ?30
History of heart failure ?10
History of chronic lung disease ?10
Pulse[110 beats/min ?20
Systolic blood pressure\100 mm Hg ?30
Respiratory rate[30 breaths/min ?20
Temperature\36 !C ?20
Altered mental status ?60
Arterial oxyhemoglobin saturation (SaO2)\90 % ?20
A total point score for a given patient is obtained by summing thepatients age in years and the points for each predictor when present.The score corresponds with the following risk classes:\65, class I;66–85, class II; 86–105, class III; 106–125, class IV; and[125, classV. Patients in risk classes I and II are defined as low risk
Table 2 Simplified Pulmonary Embolism Severity Index
Variable Points
Age[80 years 1
History of cancer 1
History of chronic cardiopulmonary disease 1
Pulse[110 beats/min 1
Systolic blood pressure\100 mmHg 1
Arterial oxyhemoglobin saturation (SaO2)\90 % 1
A total point score for a given patient is obtained by summing thepoints. The score corresponds with the following risk classes: 0, lowrisk;[1, high risk
Table 3 Hestia criteria
Variable
Hemodynamically unstable?a
Thrombolysis or embolectomy necessary?
Active bleeding or high risk of bleeding?b
Oxygen supply to maintain oxygen saturation[ 90 %[ 24 h?
Pulmonary embolism diagnosed during anticoagulant treatment?
Intravenous pain medication[24 h?
Medical or social reason for treatment in the hospital[24 h?
Creatinine clearance of less than 30 mL/min?c
Severe liver impairment?d
Pregnant?
Documented history of heparin-induced thrombocytopenia?
If one of the questions is answered with YES, the patient can NOT betreated at homea Include the following criteria, but are left to the discretion of theinvestigator: systolic blood pressure \100 mmHg with heart rate[100 beats per minute; condition requiring admission to an intensivecare unitb Gastrointestinal bleeding in the preceding 14 days, recent stroke(less than 4 weeks ago), recent operation (less than 2 weeks ago),bleeding disorder or thrombocytopenia (platelet count\75 9 109/L),uncontrolled hypertension (systolic blood pressure[180 mm Hg ordiastolic blood pressure[110 mm Hg)c Calculated creatinine clearance according to the Cockcroft-Gaultformulad Left to the discretion of the physician
Intern Emerg Med (2016) 11:11–18 13
123

normotensive patients with acute PE and evidence of rightventricle (RV) dysfunction and/or myocardial injury are clas-sified as having intermediate-risk PE (i.e., submassive PE) andcomprise a population at increased risk of adverse PE-relatedoutcomes and early mortality.4 Finally, patients with PE whohave a normal blood pressure and preserved RV functionrepresent the majority of patients with PE and have anexcellent prognosis when treatedwith anticoagulation alone.
This clinical review (1) updates the definition of interme-diate-risk PE, (2) reviews methods for estimating the proba-bility of short-termPE-related complications in normotensivePE patients (►Table 1), (3) compares benefits and harms ofavailable treatment strategies for patients with life-threaten-ing PE, and (4) integrates definitions, risk stratification, andmanagement alternatives into a practical clinical algorithm.
Updating the Definition of Intermediate-RiskPulmonary Embolism
The classical definition of intermediate-risk PE is the presenceof either RV dysfunction or myocardial injury in acute PEwithout systemic hypotension (systolic blood pressure ! 90mm Hg).4 Since identification of patients at high risk forcomplications associated with PEwould facilitate selection ofpatients for escalation of PE therapy (e.g., transfer to theintensive care unit, thrombolysis), we are proposing anupdated definition of intermediate-risk PE: confirmed PE,normal blood pressure, and a risk of PE-related complicationssimilar to patients with PE and cardiovascular instability.5
Estimating the Probability of PulmonaryEmbolism–Related Complications
Although the presence and severity of RV dysfunction, as-sessed by transthoracic echocardiography (TTE), is a majordeterminant of the clinical course of acute PE, the criteria forRV dysfunction have varied among studies.6 Thus, a universaldefinition of RV dysfunction on echocardiography is lacking.Moreover, the association between echocardiographic RVdysfunction and short-term PE-related complications is
weak. Sanchez et al performed ameta-analysis and calculatedan odds ratio (OR) for short-termmortality for RV dysfunctionon echocardiography of 2.53 (95% confidence interval [CI],1.17–5.50).7 Computed tomography (CT) allows the visuali-zation and measurement of the heart chambers, and ittherefore has the potential to provide an attractive alternativeto echocardiography for the assessment of RV function inpatients with acute PE.8–10 A recent systematic reviewshowed that RV dysfunction, assessed by CT, had an associa-tionwith increased risk ofmortality in normotensive patientswith PE.11 However, the relatively small increase (positivelikelihood ratio 1.27; 95% CI, 1.12–1.43) in the ability toclassify risk with this approach suggests that the usefulnessof basing therapeutic decision making solely on CT resultsdoes not appear warranted.
Studies of patients with acute PE have demonstrated anassociation between myocardial injury (assessed by elevatedserum levels of troponin) and short-term adverse in-hospitaloutcome. Becattini et al performed a meta-analysis of studiesin patients with acute PE to assess the prognostic value ofelevated troponin levels for short-termdeath and a compositeof adverse outcome events (composite of overall death andany of the following: shock, need for thrombolysis, endotra-cheal intubation, catecholamine infusion, cardiopulmonaryresuscitation, or recurrent PE).12 Elevated troponin levelswere associated with a high mortality in the subgroup ofhemodynamically stable patients (OR, 5.90; 95% CI, 2.68–12.95). However, troponin by itself did not appear to clinicallysignificantly change the pre- to posttest probabilities, and theusefulness of basing therapeutic decision making solely ontroponin levels does not appear warranted.
Thus, single markers of RV dysfunction (e.g., TTE, spiral CT,or brain natriuretic peptide [BNP] testing) and myocardialinjury (e.g., cardiac troponinTor I testing) have an insufficientpositive predictive value for PE-specific complications todrive decision making toward aggressive therapy.13 Whilethe American College of Chest Physicians (ACCP) guidelinessuggested that intermediate-risk patients should be identi-fied predominantly by clinical evidence of instability (e.g., adecrease in systolic blood pressure that still remains > 90mm Hg, tachycardia, elevated jugular venous pressure, clini-cal evidence of poor tissue perfusion, hypoxemia),14 obser-vational studies have suggested an incremental prognosticvalue of the association of markers of RV dysfunction andinjury over either alone.15 There is also incremental prog-nostic value for the combination of echocardiogaphy andclinical scores.16
A study of 591 normotensive patients diagnosed with PEassessed the test characteristics of cardiac troponin I (cTnI),TTE, and complete compression lower limb ultrasound (CCUS)testing for prediction of 30-day PE-related mortality.15 Athree-test strategy that combined all modalities (TTE, tropo-nin, and CCUS) improved prediction of PE-related death incomparison to use of any test by itself.
The PROgnosTic valuE of Computed Tomography scan inhemodynamically stable patients with acute symptomatic PE(PROTECT) study was designed to prospectively assess theprognostic significance of multidetector CT pulmonary
Table 1 Pulmonary embolism markers of severity
Clinical variables PESI37
Simplified PESI18
Right ventriculardysfunction
Echocardiogram7
Computed tomography11
BNP or NT-proBNP41
Clot burden Concomitant deep vein thrombosis42
D-dimer43
Computed tomography44
Myocardial injury cTnI or cTnT12
hsTnT45
H-FABP46
Abbreviations: BNP, brain natriuretic peptide; cTnI, cardiac troponin I;cTnT, cardiac troponin T; H-FABP, heart-type fatty acid binding protein;hsTnT, high-sensitivity troponin T; NT-proBNP, N-terminal pro-brainnatriuretic peptide; PESI, Pulmonary Embolism Severity Index.
Seminars in Respiratory and Critical Care Medicine Vol. 36 No. 6/2015
Controversies in the Management of Life-Threatening PE Marshall et al.836
Dow
nloa
ded
by: U
nive
rsid
ad N
atio
nal A
uton
oma
de M
exic
o (U
NAM
). C
opyr
ight
ed m
ater
ial.
Semin Respir Crit Care Med 2015;36:835-841

section titled Current Controversies and Areas ofOngoing Research.
Phase 3 trials investigating the new, non–vitamin K-dependent oral anticoagulant agents (NOACs) apix-aban (30), dabigatran (31,32), edoxaban (33), andrivaroxaban (34,35) in the treatment of VTE have beencompleted and published. A meta-analysis showedthat these agents are noninferior to the standard hep-arin/VKA regimen, in terms of prevention of VTErecurrence (relative risk [RR]: 0.90; 95% confidenceinterval [CI]: 0.77 to 1.06), and that they are probablysafer in terms of major bleeding (RR: 0.61; 95% CI: 0.45to 0.83), particularly intracranial (RR: 0.37; 95% CI:0.21 to 0.68) and fatal (RR: 0.36; 95% CI: 0.15 to 0.84)hemorrhage (36). As a result, NOACs are recommendedin the 2014 ESC Guidelines as an alternative to thestandard heparin/VKA treatment (4). All 4 NOACsmentioned earlier are now licensed for treatment ofVTE in the United States and the European Union(edoxaban still awaits approval in Canada); theapproved regimens are summarized in Table 1.
Post-marketing experience with these drugs in clinicalpractice (under “real-world” conditions) appearsreassuring in the setting of stroke prevention in atrialfibrillation, and has also begun to accumulate in VTE.In a prospective German registry of patients treatedwith rivaroxaban, rates of major bleeding for patientswith VTE were 4.1% per year (95% CI: 2.5% to 6.4% peryear), and case fatality rates were low (approximately5% at 30 days) (37). Importantly, available data suggestthat the first reversal agent against a NOAC, themonoclonal antibody idarucizumab, which binds thethrombin inhibitor dabigatran, is effective in emer-gency situations (38); this agent is expected to obtainU.S. Food and Drug Administration approval soon. Inparallel, phase 3 clinical trials are currently beingconducted with andexanet, a modified recombinantform of factor Xa, which is catalytically inactive (39)and may serve as a reversal agent for rivaroxaban,apixaban, and edoxaban.
Single oral drug regimens for PE might be expectedto improve (reduce) patients’ perceived burden of
CENTRAL ILLUSTRATION Acute PE: Current Risk Stratification
Risk Parameters and Scores
Early Mortality Risk
+
+
+
+ (+)(+)
Either 1 (or none) positive
Assessment optional:If assessed, both negative-
Both positive
Shock orHypotension
PESI Class III-Vor sPESI ≥1
Signs of RVDysfunction onan Imaging Test
CardiacLaboratoryBiomarkers*
--
-Low
Intermediate-high
Intermediate-low
High
Intermediate
Konstantinides, S.V. et al. J Am Coll Cardiol. 2016; 67(8):976–90.
*Markers of myocardial injury (e.g., elevated cardiac troponin or heart type-fatty acid-binding [H-FABP] plasma concentrations), or of right ventricular dysfunction(elevated natriuretic peptide plasma concentrations). Adapted with permission from the 2014 European Society of Cardiology Guidelines on the Diagnosis and Man-agement of Pulmonary Embolism (4). PE ¼ pulmonary embolism; PESI ¼ Pulmonary Embolism Severity Index; RV ¼ right ventricular; sPESI ¼ simplified PulmonaryEmbolism Severity Index.
Konstantinides et al. J A C C V O L . 6 7 , N O . 8 , 2 0 1 6
Pulmonary Embolism Update M A R C H 1 , 2 0 1 6 : 9 7 6 – 9 0
980
JACC. VOL.67, NO.8. 2016

TEXTO
OTROS MARCADORES DE RIESGO EN RIESGO INTERMEDIO
▸ Taquicardia
▸ Taquipnea
▸ Hipoxia
JACC. VOL.67, NO.8. 2016

ABORDAJE
▸ sPESI
▸ BNP
▸ CCUS
▸ Combinación de variables:
▸ Daño miocardio
▸ Disfunción de VD
▸ Presencia de TVP concomitante
Semin Respir Crit Care Med 2015;36:835-841

for those patientswho received an IVC filter (relative risk withfilter, 2.00; 95% CI, 0.51–7.89; p ¼ 0.5).33
In summary, although some observational data suggestthat IVC filter placement in addition to anticoagulation mightimprove survival in patients with unstable PE or after throm-bolytic therapy, controlled data do not support its routine usein patients at high risk of death unless there is a contraindi-cation to anticoagulant therapy.34
Clinical Algorithm
Management algorithms need to incorporate the probabil-ity of PE-related complications, the accuracy of the avail-able prognostic tests, the potential benefits and harms ofaggressive treatments, the risk of bleeding, and patientpreferences. Based on information fromprospective studiesand on the authors’ clinical experience, we propose atreatment strategy according to risk stratification of pa-tients with acute PE (►Fig. 1). This algorithmwill change asthe evidence base evolves. The authors propose that thisdecision algorithm should supplement and not replaceclinical judgment.
Hemodynamic status remains the most important short-term prognostic factor for patients with acute PE. Guidelinesrecommend the use of thrombolytic therapy for patientswith acute symptomatic PE and hemodynamic instability (i.e., high-risk PE) that do not have major contraindications
owing to bleeding risk. Alternatively, if expertise is available,thrombus removal may be achieved by infusion of lowerdoses of thrombolytic drug directly into the thrombus, bycatheter-based fragmentation and aspiration of thrombus, byuse of these two modalities together, or by surgical embo-lectomy.35 These techniques may be preferred if there is ahigh risk of bleeding or a poor response to systemic throm-bolysis. Bolus systemic thrombolytic therapy could be con-sidered in urgent situations with hemodynamic instability,although fewer data have been published with this ap-proach.36 Intravenous unfractionated heparin should beadministered to high-risk PE patients as the preferredmode of initial anticoagulation.
For hemodynamically stable patients with PE, the catego-rization of risk for subgroupsmay assist with decisionmakingregarding PE therapy. Clinical models (e.g., Pulmonary Embo-lism Severity Index [PESI] or sPESI) may accurately identifythose at low risk of short-term death, and such patientsmightbenefit from an abbreviated hospital stay or outpatienttherapy.18,37 It has been suggested that only patients thathave tachycardia or borderline low blood pressure shouldproceed to further testing with cardiac biomarkers (e.g.,troponin) or RV imaging to identify those at intermediaterisk of PE-related complications.19 Careful monitoring andrescue fibrinolysis for intermediate-risk PE patients whoexperiencehemodynamic compromise or deteriorationwhilereceiving standard anticoagulant therapy can minimize
Fig. 1 Stepwise approach to identification and treatment of life-threatening pulmonary embolism. 1Markers of myocardial injury include cardiactroponins I and T, or heart-type fatty acid binding protein (H-FABP). 2Assessed by echocardiography, computed tomographic angiogram, brainnatriuretic peptide (BNP) or N-terminal pro-brain natriuretic peptide (NT-proBNP). 3For older patients, clinicians might consider half-dosethrombolytic therapy or catheter-directed thrombolysis. ¶Hemodynamically stable patients with negative test results have a good prognosis whenadequately treated with standard anticoagulation. "Patients with concomitant deep vein thrombosis are at increased risk of PE-relatedcomplications. Abbreviations: ICU, intensive care unit; PE, pulmonary embolism; PESI, Pulmonary Embolism Severity Index; sPESI, simplifiedPulmonary Embolism Severity Index; UFH, unfractionated heparin.
Seminars in Respiratory and Critical Care Medicine Vol. 36 No. 6/2015
Controversies in the Management of Life-Threatening PE Marshall et al. 839
Dow
nloa
ded
by: U
nive
rsid
ad N
atio
nal A
uton
oma
de M
exic
o (U
NAM
). C
opyr
ight
ed m
ater
ial.
Semin Respir Crit Care Med 2015;36:835-841

Page 4 of 8Meyer et al. Ann. Intensive Care (2016) 6:19
Hemodynamic management in the ICUAlthough data are lacking from clinical trials in humans, recent guidelines of the European Society of Cardiology recommended the following support: (1) to use volume expansion with caution, (2) to use norepinephrine infu-sion to improve RV function if necessary when blood pressure is low, (3) to ventilate patients, when required, with a low tidal volume and plateau pressure. A pro-posal for hemodynamic management is presented in Fig. 1. Historically, dobutamine was considered as the reference drug in case of hypotension/shock, although without strong evidence. Jardin et al. reported in a very small series of 10 patients spontaneously breathing that a 30-min dobutamine infusion (8.3 ± 2.7 µg/kg/min) sig-nificantly increases cardiac index and also reduces pul-monary vascular resistance [21]. Probably that the main interest of dobutamine compared to norepinephrine is that its infusion can easily done through a peripheral venous catheter.
One study performed in humans with intermediate-risk PE has reported that increase in cardiac output was inversely correlated with RV dilatation before fluid expansion [22]. The larger the right ventricle, the lower the positive effect on cardiac output and hemodynamics.
Moreover, an experimental study in PE has shown that volume expansion could be deleterious by increasing RV stress and then decreasing cardiac output and blood pressure by its deleterious consequences on the left ven-tricle [23].
Conversely, rather than increasing RV overload by flu-ids, norepinephrine infusion has been reported as very efficient to support the right ventricle and to increase the cardiac output when the blood pressure is low [23, 24]. It especially acts by restoring the coronary perfusion pres-sure [25]. A study performed in a canine model of PE with shock has also reported that all dogs treated with norepinephrine were resuscitated and remained hemo-dynamically stable for 1 h, whereas all dogs treated with volume or isoproterenol died [26].
It is very unusual to have patients with PE under mechanical ventilation. It mainly occurs after cardiac arrest or for refractory shock. Positive pressure ventila-tion may be avoided when possible because it is deleteri-ous by more increasing the RV afterload. If needed, it is recommended to limit the tidal volume and the plateau pressure.
A few treatments have been proposed but cannot be currently recommended due to the lack of data. In a few
Fig. 1 Proposal for hemodynamic management in high-risk PE: *in the absence of contraindication; **may improve the coupling between the right ventricle and the pulmonary circulation by increasing the RV contraction and decreasing the pulmonary vascular resistance. RV right ventricle, LV left ventricle, CTPA computed tomography pulmonary angiography, CO cardiac output, MV mechanical ventilation, NO nitric oxide inhalation, VA ECMO veno-arterial extracorporeal membrane oxygenation
Meyer et al. Ann Intensive Care (2016) 6:19
original article
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 370;15 nejm.org april 10, 20141402
Fibrinolysis for Patients with Intermediate-Risk Pulmonary Embolism
Guy Meyer, M.D., Eric Vicaut, M.D., Thierry Danays, M.D., Giancarlo Agnelli, M.D., Cecilia Becattini, M.D., Jan Beyer-Westendorf, M.D., Erich Bluhmki, M.D., Ph.D., Helene Bouvaist, M.D., Benjamin Brenner, M.D., Francis Couturaud, M.D., Ph.D., Claudia Dellas, M.D., Klaus Empen, M.D., Ana Franca, M.D., Nazzareno Galiè, M.D., Annette Geibel, M.D., Samuel Z. Goldhaber, M.D., David Jimenez, M.D., Ph.D., Matija Kozak, M.D., Christian Kupatt, M.D., Nils Kucher, M.D., Irene M. Lang, M.D., Mareike Lankeit, M.D., Nicolas Meneveau, M.D., Ph.D., Gerard Pacouret, M.D.,
Massimiliano Palazzini, M.D., Antoniu Petris, M.D., Ph.D., Piotr Pruszczyk, M.D., Matteo Rugolotto, M.D., Aldo Salvi, M.D., Sebastian Schellong, M.D.,
Mustapha Sebbane, M.D., Bozena Sobkowicz, M.D., Branislav S. Stefanovic, M.D., Ph.D., Holger Thiele, M.D., Adam Torbicki, M.D., Franck Verschuren, M.D., Ph.D.,
and Stavros V. Konstantinides, M.D., for the PEITHO Investigators*
The authors’ affiliations are listed in the Appendix. Address reprint requests to Dr. Konstantinides at the Center for Thrombosis and He mostasis, University Medical Center Mainz, Langenbeckstr. 1, 55131 Mainz, Germany, or at stavros [email protected].
* A complete list of the Pulmonary Embo-lism Thrombolysis (PEITHO) trial investi-gators is provided in the Supplementary Appendix, available at NEJM.org.
N Engl J Med 2014;370:1402-11.DOI: 10.1056/NEJMoa1302097Copyright © 2014 Massachusetts Medical Society.
A BS TR AC T
BackgroundThe role of fibrinolytic therapy in patients with intermediate-risk pulmonary embo-lism is controversial.MethodsIn a randomized, double-blind trial, we compared tenecteplase plus heparin with placebo plus heparin in normotensive patients with intermediate-risk pulmonary embolism. Eligible patients had right ventricular dysfunction on echocardiography or computed tomography, as well as myocardial injury as indicated by a positive test for cardiac troponin I or troponin T. The primary outcome was death or hemody-namic decompensation (or collapse) within 7 days after randomization. The main safety outcomes were major extracranial bleeding and ischemic or hemorrhagic stroke within 7 days after randomization.ResultsOf 1006 patients who underwent randomization, 1005 were included in the intention-to-treat analysis. Death or hemodynamic decompensation occurred in 13 of 506 pa-tients (2.6%) in the tenecteplase group as compared with 28 of 499 (5.6%) in the placebo group (odds ratio, 0.44; 95% confidence interval, 0.23 to 0.87; P = 0.02). Be-tween randomization and day 7, a total of 6 patients (1.2%) in the tenecteplase group and 9 (1.8%) in the placebo group died (P = 0.42). Extracranial bleeding occurred in 32 patients (6.3%) in the tenecteplase group and 6 patients (1.2%) in the placebo group (P<0.001). Stroke occurred in 12 patients (2.4%) in the tenecteplase group and was hemorrhagic in 10 patients; 1 patient (0.2%) in the placebo group had a stroke, which was hemorrhagic (P = 0.003). By day 30, a total of 12 patients (2.4%) in the ten-ec teplase group and 16 patients (3.2%) in the placebo group had died (P = 0.42).ConclusionsIn patients with intermediate-risk pulmonary embolism, fibrinolytic therapy prevented hemodynamic decompensation but increased the risk of major hemorrhage and stroke. (Funded by the Programme Hospitalier de Recherche Clinique in France and others; PEITHO EudraCT number, 2006-005328-18; ClinicalTrials.gov number, NCT00639743.)

▸ 2115 pacientes
▸ Hemodinámicamente estables, disfunción del VD (riesgo intermedio)
▸ 2115 pacientes
▸ Mortalidad y hemorragia mayor
▸ Disminución de mortalidad, incremento de hemorragia mayor
▸ NO pacientes estables sin datos de disfunción de VD
Copyright 2014 American Medical Association. All rights reserved.
Thrombolysis for Pulmonary Embolism and Risk of All-CauseMortality, Major Bleeding, and Intracranial HemorrhageA Meta-analysisSaurav Chatterjee, MD; Anasua Chakraborty, MD; Ido Weinberg, MD; Mitul Kadakia, MD; Robert L. Wilensky, MD;Partha Sardar, MD; Dharam J. Kumbhani, MD, SM, MRCP; Debabrata Mukherjee, MD, MS; Michael R. Jaff, DO;Jay Giri, MD, MPH
IMPORTANCE Thrombolytic therapy may be beneficial in the treatment of some patients withpulmonary embolism. To date, no analysis has had adequate statistical power to determinewhether thrombolytic therapy is associated with improved survival, compared withconventional anticoagulation.
OBJECTIVE To determine mortality benefits and bleeding risks associated with thrombolytictherapy compared with anticoagulation in acute pulmonary embolism, including the subset ofhemodynamically stable patients with right ventricular dysfunction (intermediate-riskpulmonary embolism).
DATA SOURCES PubMed, the Cochrane Library, EMBASE, EBSCO, Web of Science, andCINAHL databases from inception through April 10, 2014.
STUDY SELECTION Eligible studies were randomized clinical trials comparing thrombolytictherapy vs anticoagulant therapy in pulmonary embolism patients. Sixteen trials comprising2115 individuals were identified. Eight trials comprising 1775 patients specified inclusion ofpatients with intermediate-risk pulmonary embolism.
DATA EXTRACTION AND SYNTHESIS Two reviewers independently extracted trial-level dataincluding number of patients, patient characteristics, duration of follow-up, and outcomes.
MAIN OUTCOMES AND MEASURES The primary outcomes were all-cause mortality and majorbleeding. Secondary outcomes were risk of recurrent embolism and intracranial hemorrhage(ICH). Peto odds ratio (OR) estimates and associated 95% CIs were calculated using afixed-effects model.
RESULTS Use of thrombolytics was associated with lower all-cause mortality (OR, 0.53;95% CI, 0.32-0.88; 2.17% [23/1061] vs 3.89% [41/1054] with anticoagulants; number neededto treat [NNT] = 59) and greater risks of major bleeding (OR, 2.73; 95% CI, 1.91-3.91; 9.24%[98/1061] vs 3.42% [36/1054]; number needed to harm [NNH] = 18) and ICH (OR, 4.63;95% CI, 1.78-12.04; 1.46% [15/1024] vs 0.19% [2/1019]; NNH = 78). Major bleeding was notsignificantly increased in patients 65 years and younger (OR, 1.25; 95% CI, 0.50-3.14).Thrombolysis was associated with a lower risk of recurrent pulmonary embolism (OR, 0.40;95% CI, 0.22-0.74; 1.17% [12/1024] vs 3.04% [31/1019]; NNT = 54). In intermediate-riskpulmonary embolism trials, thrombolysis was associated with lower mortality (OR, 0.48;95% CI, 0.25-0.92) and more major bleeding events (OR, 3.19; 95% CI, 2.07-4.92).
CONCLUSIONS AND RELEVANCE Among patients with pulmonary embolism, including thosewho were hemodynamically stable with right ventricular dysfunction, thrombolytic therapywas associated with lower rates of all-cause mortality and increased risks of major bleedingand ICH. However, findings may not apply to patients with pulmonary embolism who arehemodynamically stable without right ventricular dysfunction.
JAMA. 2014;311(23):2414-2421. doi:10.1001/jama.2014.5990
Editorial page 2385
Supplemental content atjama.com
Author Affiliations: Division ofCardiology, St Luke’s-RooseveltHospital Center of the Mount SinaiHealth System, New York, New York(Chatterjee); Division of Pulmonologyand Critical Care, Thomas JeffersonUniversity Hospital, Philadelphia,Pennsylvania (Chakraborty); Institutefor Heart, Vascular, and Stroke Care,Massachusetts General Hospital,Boston (Weinberg, Jaff); Division ofCardiovascular Medicine, Universityof Pennsylvania Perelman School ofMedicine, Philadelphia (Kadakia,Wilensky, Giri); Division of Cardiology,Texas Tech University, El Paso (Sardar,Mukherjee); Division of Cardiology,University of Texas SouthwesternMedical Center, Dallas (Kumbhani).
Corresponding Author: Jay Giri, MD,MPH, Division of CardiovascularMedicine, Hospital of the Universityof Pennsylvania, Gates Pavilion, NinthFloor, 3400 Spruce St, Philadelphia,PA 19104 ([email protected]).
Research
Original Investigation
2414 jama.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ by a Universidad Nacional Autonoma de Mexico (UNAM) User on 03/19/2016

▸ Evaluación de mortalidad, hemorragia, recurrencia
▸ 1755 pacientes
▸ Disminución de la mortalidad, así como el riesgo a pesar del riesgo de hemorragia mayor y menor
Full Length Article
Thrombolysis for acute intermediate-risk pulmonary embolism:A meta-analysis
Guang-yuan Gao, Ping Yang, Miao Liu, Mei Ding, Guo-hui Liu, Ya-liang Tong, Chun-yan Yang, Fan-bo Meng ⁎Department of Cardiology, China-Japan Union Hospital of Jilin University, Changchun, China
a b s t r a c ta r t i c l e i n f o
Article history:Received 11 May 2015Received in revised form 14 August 2015Accepted 9 September 2015Available online 12 September 2015
Keywords:Thrombolytic therapyAnticoagulationAcute intermediate-risk pulmonary embolismMortalityBleeding riskRecurrent pulmonary embolism
Background: The use of thrombolytic therapy in patients with intermediate-risk pulmonary embolism iscontroversial. To compare with anticoagulation alone, no analysis before has determined whether thrombolytictherapy is associated with improved survival or lower incidence of adverse clinical outcomes for intermediate-risk pulmonary embolism.Objective: This meta-analysis was performed to assess mortality benefits, bleeding and recurrent pulmonaryembolism risks associated with thrombolytic therapy compared with anticoagulation in patients withintermediate-risk pulmonary embolism.Methods: The Web of Science, PubMed, Embase, EBSCO, and the Cochrane Library databases were searched forrandomized clinical trials comparing thrombolytic therapy with anticoagulation in intermediate-risk pulmonaryembolism patients (in which the mortality data were reported) from inception to August 5, 2014. Primaryoutcomes were all-cause mortality and major bleeding. Secondary outcomes were recurrent pulmonaryembolism and minor bleeding. The pooled relative risk (RR), Mantel–Haenszel corresponding method andfixed-effect model were used to estimate the efficacy and safety of thrombolytic therapy with 95% confidenceintervals.Results: Eight clinical randomized controlled trials involving 1755 patients with intermediate-risk pulmonaryembolism were included. Patients treated with thrombolytics presented lower mortality than patients in theanticoagulation cohort (RR, 0.52; 95% CI, 0.28–0.97; 1.39% [12/866] vs. 2.92% [26/889]). Compared withanticoagulation, thrombolytic therapy was associated with a higher risk of major (RR, 3.35; 95% CI, 2.03–5.54;7.80% [64/820] vs. 2.28% [19/834]) and minor (RR, 3.66; 95% CI, 2.77–4.84; 32.78% [197/601] vs. 8.94%[53/593]) bleeding. Furthermore, thrombolytic therapy was associated with a lower incidence of recurrentpulmonary embolism (RR, 0.33; 95% CI, 0.15–0.73; 0.73% [6/826] vs. 2.72% [23/846]).Conclusion: Comparedwith anticoagulation, thrombolytic therapy in patients with intermediate-risk pulmonaryembolism is associatedwith lower all-causemortality and recurrent pulmonary embolism risk despite increasedmajor and minor bleeding risks.
© 2015 Elsevier Ltd. All rights reserved.
1. Introduction
Acute pulmonary embolism (PE) is a life-threatening disorder associ-ated with a significant burden of morbidity andmortality. It is estimatedthat more than 100,000 PE cases occur annually, 20–25% of which
present as sudden death [4]. The annual incidence of PE is 0.1% inChinese hospitals from 1997 to 2008 [24].
PE is classified into three subgroups in order to better assessthe treatment and outcome of patients: high-risk PE, intermediate-riskPE and low-risk PE. The definition of intermediate-risk PE: acutePE patients without systemic hypotension (systolic blood pressure≥90 mm Hg) but with either right ventricular dysfunction (RVD) ormyocardial necrosis [12]. RVD means the presence of at least 1 of thefollowing: 1. right ventricular (RV) dilation (apical 4-chamber RVdiameter divided by left ventricular (LV) diameter N0.9) or RV systolicdysfunction on echocardiography; 2. RV dilation (4-chamber RVdiameter divided by LV diameter N0.9) on computed tomography(CT); 3. elevation of brain natriuretic peptide (BNP) (N90 pg/mL);4. elevation of N-terminal pro-BNP (N500 pg/mL) or electrocardio-graphic changes (new complete or incomplete right bundle-branchblock, anteroseptal ST elevation or depression, or anteroseptal T-wave
Thrombosis Research 136 (2015) 932–937
Abbreviations: RVD, right ventricular dysfunction; RV, right ventricular; LV, leftventricular; MI, myocardial injury; PE, pulmonary embolism; CT, computedtomography; V/Q, scanning, ventilation–perfusion lung scanning; Pang, pulmonaryangiography; ICH, intracranial hemorrhage; CTPA, computed tomography pulmonaryangiography; Hg, hemoglobin; cTn-I, cardiac troponin I; cTn-T, cardiac troponin T; BNP,brain natriuretic peptide; LMWH, low-molecular-weight heparin; UFH, unfractionatedheparin; RR, relative risk.⁎ Corresponding author.
E-mail addresses: [email protected] (G. Gao), [email protected] (P. Yang),[email protected] (M. Liu), [email protected] (M. Ding),[email protected] (G. Liu), [email protected] (Y. Tong), [email protected](C. Yang), [email protected] (F. Meng).
http://dx.doi.org/10.1016/j.thromres.2015.09.0120049-3848/© 2015 Elsevier Ltd. All rights reserved.
Contents lists available at ScienceDirect
Thrombosis Research
j ourna l homepage: www.e lsev ie r .com/ locate / th romres

▸ 1833 pacientes
▸ No existe evidencia de reducción de mortalidad
▸ Incremento del riesgo de HIC y hemorragia mayor
Regular Article
Thrombolysis in hemodynamically stable patients with acute pulmonaryembolism: A meta-analysis
Antoni Riera-Mestre a,⁎, Cecilia Becattini b, Michela Giustozzi b, Giancarlo Agnelli ba Internal Medicine, Hospital Universitari de Bellvitge, IDIBELL, L’Hospitalet de Llobregat Barcelona Spainb Internal and Cardiovascular Medicine, Stroke Unit, University of Perugia, Perugia Italy
a b s t r a c ta r t i c l e i n f o
Article history:Received 8 August 2014Received in revised form 24 September 2014Accepted 3 October 2014Available online 13 October 2014
Keywords:Pulmonary thromboembolismThrombolytic therapyBleedingPrognosisVenous thromboembolism
Introduction: The role of thrombolysis in hemodynamically stable patients with acute pulmonary embolism (PE)remains controversial. We performed ameta-analysis of randomized trials to assess the effect of thrombolysis inthese patients.Materials andMethods:We searchedMEDLINE and EMBASE for randomized studies comparing thrombolysis andheparin for the initial treatment of hemodynamically stable PE patients. Pooled odds ratios (OR) and 95% confi-dence intervals (CI) were calculated. NNH to cause a major bleeding (MB) or an intracranial hemorrhage (ICH)and NNT to avoid one death were also calculated.Results: Eleven studies (1833 patients) were included seven with rt-PA, three with tenecteplase and one withurokinase. Patients randomized to thrombolysis had a significant increased risk for MB (5.9% vs 1.9%; OR 2.83,95% CI 1.68-4.76, I2 18.7%) and an increased risk for ICH (1.74% versus 0.6%; OR 2.36, 95% CI 0.98-5.71, I2 0%)and for fatal bleeding (1.3% versus 0.54%; OR 1.84, 95% CI 0.73-4.61, I2 0%). A not-significant reduction for all-cause death (1.74% vs 2.51%; OR 0.68, 95% CI 0.37-1.26, I2 0%) and a significant reduction for recurrent PE(1.1% vs 2.5%; OR 0.44, 95% CI 0.21-0.92, I2 0%) in favor of thrombolysis compared with heparin was found.NNH to cause a MB or an ICH were 27 and 91 patients, respectively. NNT to avoid one death was 125 patients.Conclusions: Due to increased risk for MB and ICH with no evidence of reduction in mortality, thrombolysisshould not be used for most normotensive PE patients.
© 2014 Elsevier Ltd. All rights reserved.
Introduction
Pulmonary embolism (PE) is a common disease associated with asubstantial risk for short-term mortality that can be as high as 30% inhemodynamically unstable patients [1]. The clinical management ofhemodynamically stable patients with acute PE is an everyday clinicalchallenge [2]. The wide range of short-term mortality observed inthese patients (from 15 to less than 1%) suggests the need for tailoringtheir clinicalmanagement according to the specific risk for death [1,3,4].
Thrombolytic treatment provides a more rapid lysis of pulmonaryemboli, reduction of pulmonary hypertension and improvement inright ventricle (RV) dysfunction than heparin [5,6]. A reduction inmortality has been shown with thrombolytic treatment in patientswith PE associated with hemodynamic compromise [7]. Whetherthrombolytic treatment results in an improved clinical outcome andoutweigh the potential increased risk of bleeding complications inhemodynamically stable patient with acute PE remains controversial.
A large randomized placebo controlled trial (PEITHO) aimed atassessing the clinical benefit of thrombolysis in normotensive patientswith acute PE, has recently been concluded [8]. In this trial, the clinicalbenefit of tenecteplase in terms of reduction in mortality and clinicaldeterioration at 7 days was counterbalanced by a high risk for majorbleeding (MB).
We performed a meta-analysis of randomized clinical trials (RCTs)to compare thrombolysis and heparin versus heparin alone in hemody-namically stable patients with acute PE.
Methods
Data sources and searches
We attempted to identify all RCTs which compared thrombolysisand heparin for the initial treatment of acute PE in hemodynamicallystable patients by computer aided search (MEDLINE and EMBASE),and scrutiny of the reference lists of original research and review arti-cles. We searched electronic databases MEDLINE and EMBASE usingthe terms “pulmonary embolism,” “thrombolysis”, and ”thrombolytictherapy,” in combinationwith generic names of individual thrombolyticagents.
Thrombosis Research 134 (2014) 1265–1271
⁎ Corresponding author at: Internal Medicine Department. Hospital Universitari deBellvitge - IDIBELL. C/Feixa Llarga s/n. L’Hospitalet de Llobregat (08907), BarcelonaSpain. Tel.: +34 93 260 76 99; fax: +34 93 260 79 67.
E-mail address: [email protected] (A. Riera-Mestre).
http://dx.doi.org/10.1016/j.thromres.2014.10.0040049-3848/© 2014 Elsevier Ltd. All rights reserved.
Contents lists available at ScienceDirect
Thrombosis Research
j ourna l homepage: www.e lsev ie r .com/ locate / th romres

should be given to patients who had syncope, whichmay represent transient hemodynamic instabilityand the potential for higher risk (9). Hemodynami-cally stable patients without evidence of RV strainare considered to be at low risk, may not requirePERT activation, and can be treated with anti-coagulation alone. That said, the PERT might help theclinical team define the level of risk and optimaltherapy for each individual patient.
Once the PERT has been activated, members typi-cally meet, either at the patient’s bedside or virtually,and review all patient-related data. The most impor-tant data include the presenting history, with a focuson symptoms and signs of hemodynamic instability,vital signs, CT, echocardiogram, and laboratory data.Team members should discuss indications and con-traindications to fibrinolytic therapy, catheter-basedintervention, and surgical embolectomy, followedby discussion with the patient and family members,including the risks and benefits of each therapy pro-posed. A sample algorithm to help in triaging patientspresenting to the emergency room of a hospital with aPERT is provided (Figure 1). The PERT shouldconsider the degree of hemodynamic compromiseand the existence of variable contraindications. Thesimplified PE severity index may be a useful aid whenfurther considering the risks and benefits of inter-ventional therapies (10).
SYSTEMIC FIBRINOLYSIS
Traditionally, intravenous (IV) fibrinolysis has beenconsidered the primary intensive therapy option inpatients with high-risk PE, although the data sup-porting its use in massive PE is poor. Most trials thatrandomized patients with PE to fibrinolytics versusstandard anticoagulation included submassive PEonly. A meta-analysis of trials including patients withmassive PE showed a reduction in the composite ofrecurrent PE and death with use of IV fibrinolyticagents, but not in death alone (11). Univariate analysisof a large inpatient sample found that among unsta-ble patients with PE, use of IV fibrinolytic therapy wasassociated with a lower mortality rate (12), but only30% of unstable patients received such therapy.
Patients with submassive PE were better repre-sented in randomized trials. The MAPPET (Manage-ment, Strategies and Prognosis of PulmonaryEmbolism)-3 trial (13) randomized 256 patients withPE and pulmonary hypertension or RV dysfunction to100 mg of IV alteplase or placebo infused over 2 h plusanticoagulation. IV alteplase was associated with alower risk of further need to escalate the treatment andwith a similar risk of death. Mortality was lower than
expected in both groups (3.4% in the alteplase and2.2% in the placebo group; p ¼ 0.71). More recently,the PEITHO (Pulmonary Embolism Thrombolysis) trial(14) randomized 1,006 patients with submassivePE (normal blood pressure, RV enlargement, andincreased troponin level) to tenecteplase or placebo.The PEITHO trial showed a reduction in the primaryendpoint of hemodynamic collapse at 7 days withtenecteplase, but a significant increase in hemorrhagicstroke (most in patients older than 75 years of age),with similar mortality in both groups. The smallerMOPETT (Moderate Pulmonary Embolism TreatedWith Thrombolysis) trial (15) randomized 121 patientswith moderate-risk PE to half-dose alteplase(maximum 50mg over 2 h) with anticoagulation versusanticoagulation alone. Low-dose alteplase was asso-ciated with lower pulmonary pressure at 28 monthsand no major bleeding. A 1,700 patient meta-analysis
CENTRAL ILLUSTRATION PERT Protocol
Medical therapy Catheter directed therapy
Surgicalembolectomy
Acute PE confirmed by Computed Tomography (CT) scan
Patient with suspected pulmonary embolism (PE)
Multidisciplinary PE response team (PERT) alerted:Interventionalist, cardiac surgeon,
radiology, pulmonary/critical care medicine
PERT members review the available medical informationand develop optimal treatment plan
Anticoagulation initiated, unless contraindicated
Jaber, W.A. et al. J Am Coll Cardiol. 2016; 67(8):991–1002.
Example of an intensive PE management pathway utilizing a single phone call to the PEteam leader. Further review with PERT members can occur while the patient is transferredto the critical care unit, interventional laboratory, or operating room. Adapted withpermission from Bloomer et al. (6). CT ¼ computed tomography; PE ¼ pulmonaryembolism; PERT ¼ pulmonary embolism response team.
J A C C V O L . 6 7 , N O . 8 , 2 0 1 6 Jaber et al.M A R C H 1 , 2 0 1 6 : 9 9 1 – 1 0 0 2 Pulmonary Embolism
993
JACC. VOL.67, NO.8. 2016
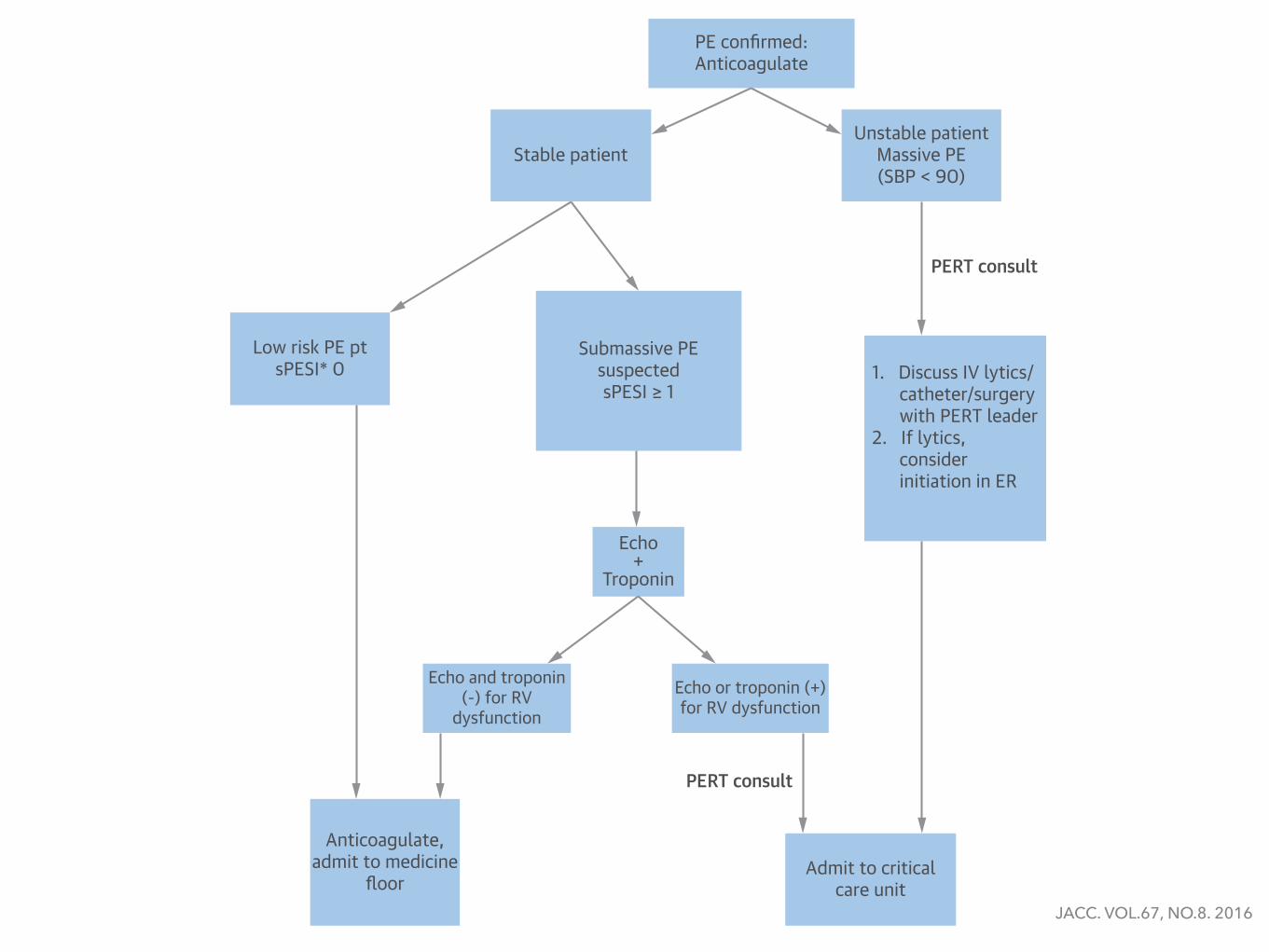
of all fibrinolysis trials, including patients withcatheter-directed fibrinolysis (CDF), demonstrated astatistically significant mortality benefit from fibrino-lysis in patients with intermediate-risk PE (16). Therewas a significantly increased risk of hemorrhage, butthe benefit appeared to outweigh the risk when theanalysis excluded patients older than 65 years of age.Importantly, subanalyses of patients younger than 65years of age were performed post hoc in the trialsincluded in the meta-analysis.
Taken together, these studies show that the use ofIV fibrinolytic therapy in patients with massive orsubmassive PE leads to improved hemodynamic sta-bilization and, possibly, a lower risk of recurrent PEand PE-attributed death. However, this benefit comes
with an increased risk of severe bleeding and intra-cranial hemorrhage (14).
CATHETER-BASED THERAPIES
Catheter-based therapies aim to relieve obstructionquickly and restore pulmonary blood flow, thusimproving cardiac output and converting a hemody-namically unstable situation into a stable one. Thisis accomplished with reduced or no doses of fibrino-lytic agents. Catheter-directed therapies (CDT) mightinclude clot fragmentation, aspiration, and low-dosefibrinolytic injection. The American Heart Associa-tion and American College of Chest Physiciansguidelines address catheter-based management of
FIGURE 1 ER PE Protocol Utilizing PERT Consultation and sPESI Score
PE confirmed:Anticoagulate
Stable patientUnstable patient
Massive PE(SBP < 90)
PERT consult
Low risk PE ptsPESI* 0
Submassive PEsuspectedsPESI ≥ 1
1. Discuss IV lytics/ catheter/surgery with PERT leader2. If lytics, consider initiation in ER
Echo+
Troponin
Echo and troponin(-) for RV
dysfunctionEcho or troponin (+)for RV dysfunction
Anticoagulate,admit to medicine
floorAdmit to critical
care unit
PERT consult
*Simplified pulmonary embolism severity index (sPESI) score ¼ 1 point for age >80 years, cancer, chronic heart failure or chronic pulmonarydisease, heart rate >110 beats/min, SBP <100 mm Hg, or O2 saturation <90%. Adapted with permission from Bloomer et al. (6). Echo ¼echocardiography; ER ¼ emergency room; IV ¼ intravenous; PE ¼ pulmonary embolism; PERT ¼ pulmonary embolism response team;RV ¼ right ventricular; SBP = systolic blood pressure.
Jaber et al. J A C C V O L . 6 7 , N O . 8 , 2 0 1 6
Pulmonary Embolism M A R C H 1 , 2 0 1 6 : 9 9 1 – 1 0 0 2
994
JACC. VOL.67, NO.8. 2016

DOSIS DE FIBRONOLÍTICOS ¿50 O 100 MG ALTEPLASE?
Semin Respir Crit Care Med 2015;36:835-841

Venturi-Bernoulli effect, using multiple high-velocity saline jets introduced through the distaltip, creating a low-pressure vacuum through smallslits in the catheter that can entrain and fragmentthrombi. A meta-analysis reported higher mortalityand morbidity, including massive hemoptysis, renalfailure, and death from bradycardia and apnea orfrom widespread distal embolization (18), whichresulted in a black-box warning from the Food andDrug Administration (FDA) for use of Angiojet inacute PE.
Additional embolectomy devices are discussed inthe following sections.AngioVac thrombectomy dev ice . The AngioVacCannula (Angiodynamics, Latham, New York), a 22-Fvenous catheter that can remove soft thrombi utiliz-ing the centrifugal pump and venous reinfusioncannula used in cardiopulmonary bypass (Figure 2), isFDA approved for the removal of undesirable
intravascular material, including fresh, soft thrombior emboli. The AngioVac catheter consists of aballoon-expandable, funnel-shaped distal tip, whichimproves removal of large clots en masse. Patients areprepped in 2 body locations that will allow for largevenous sheath placements (common femoral or in-ternal jugular veins). A 26-F sheath is placed in 1 veinand an 18-F reinfusion cannula is placed in anothervein. The AngioVac cannula is then attached to theinflow tubing of the centrifuge pump and the outflowtubing connected to the 18-F reinfusion cannula,creating a “veno-veno” bypass circuit. The cannula isinserted into the 26-F sheath and is advanced to thethrombus, which is suctioned out and captured by afiltration canister inserted proximal to the centrifugepump; filtered blood is returned continuously via thereinfusion cannula. Limitations of this device includethe large dual sheaths required for access, leading to ahigher likelihood of bleeding complications, and therelatively stiff suction catheter, which is difficult tomaneuver into the RV and PA. Furthermore, theactive participation of an experienced perfusionist isrequired for AngioVac setup and operation, as there isa learning curve for its use. AngioVac has been uti-lized in PE, although it is more commonly used toretrieve thrombi from the vena cava and right atrium(25). The rapidity of initiation may limit its use inmassive PE situations; future iterations may render itmore useful for PE.FlowTr iever dev ice . The FlowTriever catheter(Inari Medical, Irvine, California) is a recentlyreleased device that has FDA 510(k) approval forremoval of emboli and thrombi from blood vessels(Figure 3). The FlowTriever Infusion Aspiration Sys-tem requires a 22-F venous sheath and consists of3 parts: the Flow Restoration Catheter, which is madeup of 3 self-expanding nitinol disks; the AspirationGuide Catheter; and the Retraction Aspirator Device.The FlowTriever device is advanced over the wire andinto the thrombus, where the expandable disks aredeployed using a pin and pull method. The disks anddisrupted thrombus are then retracted and removedthrough the aspiration catheter. Set-up is rapid, andthere is a modest learning curve for device utilization.Limitations include the large size requirement of theaccess sheath, and manipulation of the large-borecatheter into the PA.Penumbra Ind igo thrombectomy system. TheIndigo mechanical thrombectomy system (Penumbra,Inc., Alameda, California) consists of a pump, 6- to8-F straight or angled catheters, and a Separator de-vice (Figure 4). It is approved for thrombus removalin both peripheral arterial and venous systems.An advantage is that it only requires an 8-F venous
FIGURE 2 AngioVac Device
AC
B AngioVac Cannula
Saline Bag
Filter
Centrifugal Pump Console
ReinfusionCannula
AngioVacCircuit
(A) AngioVac cannula. (B) Diagram of AngioVac insertion and reinfusion circuit. The cannulahas been inserted into the right internal jugular vein. Blood and thrombus is aspiratedthrough the filter canister, allowing clot capture utilizing a centrifugal pump canister,prior to return of blood to the patient via the reinfusion cannula placed into the femoralvein. (C) Example of thrombus captured in the filter canister. Images from Angiodynamics.
Jaber et al. J A C C V O L . 6 7 , N O . 8 , 2 0 1 6
Pulmonary Embolism M A R C H 1 , 2 0 1 6 : 9 9 1 – 1 0 0 2
996
sheath and can be placed into the PA system quickly,in an over-the-wire technique. Once placed proximalto the clot, the thrombectomy catheter is advancedwhile suction is supplied with the ACER pump. Theprovided Separator wire is used to clear the system ofthrombus as the catheter is manipulated inside theartery.
A distinct limitation of these last 3 devices is theabsence of published data on their overall success andsafety.
CATHETER-DIRECTED FIBRINOLYSIS. Genera lcons iderat ions . Given that full-dose systemic fibri-nolysis is helpful in stabilizing high-risk PE patientsand reducing pulmonary pressure, but at the cost ofincreased systemic bleeding, interest has risen in localdelivery of low-dose fibrinolytics close to or intothe PA thrombus. Unfortunately, data supportingsuch therapy is limited and mostly from smallcase series (18,26–28). One small trial randomized34 patients with angiographically large PE to IV- orcatheter-based infusion of t-PA at a dose of 50 mg over2 h (29), and showed similar safety and angiographicand hemodynamic results by both techniques. How-ever, the local fibrinolytic dose used in this older trialwas much higher than what is currently used. In amore recent prospective registry of 101 massive andsubmassive PE patients treated with catheter-basedtherapy (mostly local fibrinolysis), there was a sig-nificant decrease in PA pressure and improvement inRV function, with no reported major complications,major bleeding, or strokes (26). Given the low risk formajor complications, it is reasonable to consider CDFin patients with already stabilized massive PE whohave contraindications to systemic fibrinolysis and inpatients with intermediate-high–risk PE (those withRV dysfunction and increased biomarkers), particu-larly those deemed at increased bleeding risk withfull-dose systemic fibrinolysis. In a series of 52 PEpatients treated with CDF, a more prominent hemo-dynamic benefit was obtained in patients with symp-tom duration <14 days, as compared with those with alonger symptom duration (28).Techn ique . CT images, if available, are the basis forplanning the CDT procedure. Most high-risk patientshave bilateral PE, although some have a majorthrombus in 1 PA and only require unilateral treat-ment. Internal jugular or femoral venous access withultrasound guidance is obtained. For femoral access,ultrasound is used to rule out iliofemoral thrombus.A catheter (e.g., balloon-tipped, pigtail, or multipur-pose) is carefully advanced to the main PA, wherepressure and blood oxygen saturation sampling areobtained. Contrast injection into the main PA or
selectively into each PA can be performed to identifythe location of the thrombi; these are typically in themain and/or lower main PA branch (Figure 5). Ifthe location of the thrombi is not clear by manualinjection, or the anatomy has not been previouslyestablished by CT, and if the pulmonary pressure isnot severely elevated, a power injection may benecessary (e.g., at 15 to 20 m/s for a total of 30 mlselectively in each main PA, with a 15! to 20! leftanterior oblique projection for the left PA and 0! to20! right anterior oblique projection for right PA). Thevolume of contrast injected can be adjusted on thebasis of the CT findings. An exchange-length soft- orj-tipped wire is placed in the lower PA branch, and thediagnostic catheter is exchanged for an infusioncatheter, which has a treatment zone of 6 to 12 cmthrough which t-PA may be infused into the clot.A second infusion catheter may be placed in the
FIGURE 3 FlowTriever Device
A
B
AGC
FRC
RAD
(A) The flow restoration catheter (FRC) is used to enmesh clots and is pulled through theaspiration guide catheter (AGC) utilizing (B) the retraction aspirator device (RAD). Imagesfrom Inari Medical.
J A C C V O L . 6 7 , N O . 8 , 2 0 1 6 Jaber et al.M A R C H 1 , 2 0 1 6 : 9 9 1 – 1 0 0 2 Pulmonary Embolism
997
JACC. VOL.67, NO.8. 2016

contralateral PA through a second venous sheath, ifneeded, using the same technique. Alternatively, a10- to 12-F sheath may be placed at the beginning ofthe procedure and both catheters placed through thelarger sheath. A commonly used t-PA dose is 0.5 to 1.0mg/h per catheter. The total t-PA dose is typicallybetween 12 and 24 mg, delivered over 6 to 24 h. Low-dose, weight-adjusted heparin infusion is usuallycontinued during t-PA infusion, with a target partialthromboplastin time on the low end of the thera-peutic range (e.g., 40 to 60 s).
Commonly available infusion catheters used off-label for PE include the Cragg-McNamera catheter(ev3 Endovascular Inc.), the Fountain catheter (MeritMedical, South Jordan, Utah), and the Unifuse cath-eter (Angiodynamics). The EkoSonic catheter, (EKOSCorp., Brothell, Washington), discussed later, iscurrently the only catheter specifically approved byFDA for the treatment of high-risk PE.
The risk of serious complications, including majorhemorrhage, using CDT has been low in publishedstudies. The risk of intracranial hemorrhage is <0.2%(18,26–28).Ult rasound acce lerated fibr inolys i s . The Eko-Sonic catheter (Figure 6) consists of a 5.2-F con-ventional infusion catheter with an inner cablethat transmits high-frequency, low-power ultra-sound signals, designed to loosen the fibrin strandsand enhance thrombus penetration of the
fibrinolytic agent, hence theoretically achieving afaster thrombus breakdown (30). The techniqueused for in vivo insertion is similar to other infu-sion catheters, as described earlier. Once thecatheter is in position over the 0.035-inch guide-wire, the guidewire is replaced with the microsoniccable, which is then locked into place. The cath-eter has 2 infusion ports: 1 for the fibrinolyticinfusion, and the other for a coolant solution(normal saline at $35 ml/h).
Limited evidence supports the use of ultrasound-accelerated thrombolysis (discussed in detail byKonstantinides et al. [31]). It is uncertain whetherthis treatment is suitable for patients who arehemodynamically unstable and need faster resolu-tion of the PE or if there is long-term benefit of theprolonged treatment in prevention of future pulmo-nary hypertension, underscoring the need for moreevidence.
EXTRACORPOREAL MECHANICAL
OXYGENATION AND RV ASSIST DEVICES
Extracorporeal membrane oxygenator (ECMO) place-ment has been described in case reports of patientswith massive PE, as it has the potential to unloadthe RV and, importantly, provides oxygenation dur-ing massive PE to allow for RV recovery (32,33). Theability of the interventional team to place the ECMOunderscores the importance of a multidisciplinaryapproach. In many institutions, PERT membersare also ECMO service members.
Technologies such as the percutaneous RV assistdevice (Impella RP, Abiomed, Danvers, Massachu-setts) may one day be considered for use in massivePE, either as a bridge to definitive therapy, or tosupport RV recovery after thrombus removal.
SURGICAL EMBOLECTOMY
Currently, surgical therapy is considered a last resortfor acute PE and is offered only to patients inextremis. This concept is on the basis of data fromthe 1960s, when the surgical pulmonary embolec-tomy mortality rate was in excess of 50% (34). Thismay have been due, in part, to selection bias, as onlypatients with very poor prognosis were brought tothe operating room. Significant advances in cardiacsurgical techniques have led to an impressivereduction in operative mortality, which is as low as6% in the current era (35,36). Furthermore, there isevidence to support reduced long-term mortality inpatients undergoing pulmonary embolectomy(37,38). In a 2013 report on 27 consecutive surgicalpulmonary embolectomy patients, there was no
FIGURE 4 Penumbra Indigo Aspiration System
(A) The 6- to 8-F straight or angled aspiration catheter (CAT6 or CAT8, respectively)is advanced to the thrombus and aspiration performed with the (B) ACER pump. Separatorwires may be inserted into the catheter and utilized in a gentle back-and-forth motion toclear the catheter of thrombus. Images from Penumbra, Inc.
Jaber et al. J A C C V O L . 6 7 , N O . 8 , 2 0 1 6
Pulmonary Embolism M A R C H 1 , 2 0 1 6 : 9 9 1 – 1 0 0 2
998
by the PREPIC2 (Prevention of Recurrent PulmonaryEmbolism by Vena Cava Interruption 2) study,recently conducted in intermediate- and low-riskpatients (41). However, 3 large analyses, including aU.S. nationwide hospital sample (42) and a study fromJapan (43), suggest that IVC filters may result in betteroutcomes in patients with massive or intermediate-high–risk PE. In the International Cooperative Pul-monary Embolism registry, IVC filter use in patientswith massive PE was associated with reduced rates ofrecurrent PE and mortality at 90 days (44).
POST-INTERVENTION
Maintenance of anticoagulation post-intervention iscritical to prevent recurrent clot formation. However,patients who have had a recent catheter-based inter-vention are at risk of access site bleeding. One strategyto potentially reduce bleeding risk is to hold the hep-arin drip for 1 to 2 h after sheath removal, then restartwithout a bolus. Warfarin is administered on the nightof the procedure, and parenteral anticoagulation andwarfarin are overlapped until the internationalnormalized ratio is 2 to 3 for at least 24 h, as perAmerican College of Chest Physicians guidelines (7).
Low molecular weight heparin can be utilized inlieu of IV heparin. Alternatively, novel oral
anticoagulants, including rivaroxaban, dabigatran,apixaban, and edoxaban, can be used (45–48). How-ever, no guidelines indicate when or how theseagents should be initiated post-CDT, especially iffibrinolytic agents have been administered. If analternative anticoagulant agent is utilized, we suggestheparin alone for the first 24 to 48 h post-interventionand then discontinuation of the heparin at the time ofthe first alternative anticoagulant agent dosing. Thisstrategy does not include dabigatran or edoxabanusage, which require at least 5 days of parenteraltherapy before initiation.
Appropriate transition of the patient from theinpatient to the outpatient setting is important. Thisincludes assessment of adequacy of anticoagulationor affordability of novel anticoagulant agents, if pre-scribed. Outpatient follow-up with a medical providerfamiliar with PE care is imperative; several in-stitutions incorporate a PE follow-up clinic as part ofthe PERT program. To be addressed at follow-up are:monitoring of anticoagulation; assessment of lengthof anticoagulation and bleeding risk; retrieval of IVCfilter, if appropriate; screening for the developmentof chronic pulmonary hypertension in patients at risk;and completion of a hypercoagulable profile, whenindicated.
CONCLUSIONS
At this time, there is not enough evidence to stronglysupport routine utilization of any of the previouslydiscussed techniques in the management of sub-massive or massive PE, beyond anticoagulation. MostPE patients should continue to be treated conserva-tively, with aggressive treatment options reserved forthose at high- or intermediate-high–risk withoutcontraindications. Several studies have shown benefitfrom systemic fibrinolysis in this patient population,at the expense of an increased bleeding risk.Currently, CDF with use of the EKOS catheter is theonly FDA-approved catheter-based therapy for use intreatment of acute PE, although adequate compara-tive studies are lacking. Other catheter-based thera-pies focus on direct thrombus removal without use offibrinolytic agents and may be an option for patientswho either cannot receive fibrinolysis or cannot waitfor CDF to take effect. Although some centers havereported favorable outcomes with surgical embolec-tomy as a first-line management of intermediate-high– and high-risk PE, it is reasonable to reserve itfor patients with massive PE and shock, who havecontraindications to fibrinolysis, who have failedother treatments, or who have concomitant intracar-diac thrombus or paradoxical embolus.
FIGURE 6 EkoSonic Endovascular Device
The 5.2-F infusion catheter (A), which contains 3 lumens: 1 each for the inner ultrasoundcable, drug infusion, and normal saline as a coolant. The inner cable (B) is shown withultrasound crystals (arrows). Ultrasound energy separates fibrin strands, allowing forenhanced thrombus penetration of fibrinolytic agent. Images from EKOS Corporation.
Jaber et al. J A C C V O L . 6 7 , N O . 8 , 2 0 1 6
Pulmonary Embolism M A R C H 1 , 2 0 1 6 : 9 9 1 – 1 0 0 2
1000
JACC. VOL.67, NO.8. 2016

of acute PE is on the basis of the estimated earlydeath risk (Figure 1). It has been established that thepresence of right ventricular dysfunction and failureresulting from acute pressure overload is the prin-cipal determinant of the patient’s early clinicalcourse and risk of an adverse outcome (reviewedin [4,9]). Accordingly, high-risk or massive PE refersto the presence of shock or persistent arterialhypotension as a result of overt right ventricularfailure. This is clearly a life-threatening situation, inwhich prompt reperfusion treatment (as discussedlater) is needed, along with circulatory and res-piratory support in order to break the spiral of
hemodynamic deterioration and to increase thechances of survival (4,10,11).
More than 95% of patients with acute PE are (orappear to be) hemodynamically stable at presentationand are thus not considered to be at high risk (12).Within this large group, the next challenging step isto determine which patients will need hospitalizationand possibly initial monitoring, and to distinguishthem from those who are at truly low risk and mayqualify for early discharge and outpatient treatment.To be used as risk stratification tools for this purpose,baseline clinical parameters and prediction scoresderived from them should reliably exclude severe
FIGURE 1 PE: Risk-Adjusted Management in the Acute Phase and Over the Long Term
PREDICTORS OFEARLY ADVERSE OUTCOME
RISK FACTORS FORRECURRENT VTERISK FACTORS
FOR FIRST VTE
HORMONALCONTRACEPTION
TRAUMA OR FRACTURE
SURGERY
HORMONAL REPLACEMENTTREATMENT
PREGNANCYAND POSTPARTUM
IMMOBILIZATION
AGE
INFLAMMATORYBOWEL DISEASE
THROMBOPHILIA†
OBESITYCANCERCHEMOTHERAPY
PRIOR VTED-DIMERS
FIRST UNPROVOKEDVTE EVENT
MALE SEXCHRONIC HEART FAILURE
CHRONIC LUNG DISEASEACTIVE CANCER
VITAL SIGNSHYPOXEMIA
RV DYSFUNCTION(CT/ECHO)
BIOCHEMICAL MARKERS*
PRE-TESTCLINICAL ASSESSMENT DIAGNOSIS
ACUTE RISKSTRATIFICATION TREATMENT
LONG-TERMCLINICAL COURSE
Revised Geneva scoreWells ruleEmpirical assessment
(Age-adjusted) D-dimersCTPAV/Q scanEchocardiographyCUS
PESI and sPESIBiochemical markers*RV dysfunction(echocardiography)RV enlargment (CTPA)
Parenteral anticoagulantsOral anticoagulantsFibrinolyticsCatheter-directedtechniquesSurgical embolectomyVena cava filters
Assess bleeding riskPredict VTErecurrenceFocused screeningfor CTEPH insymptomatic patients
HIGH CLINICALPROBABILITY
LOW ORINTERMEDIATE
CLINICALPROBABILITY
Hemodynamicinstability
Absence ofhemodynamic
instability
Age-adjustedpositive
D-dimers
ALGORITHM FORHIGH-RISK PE
CTPA
CTPA
ALGORITHM FORNON HIGH-RISK PE
V/Q scan
HIGH RISK
INTERMEDIATE RISK
LOW RISK
PRIMARYREPERFUSION
ANTICOAGULANTTHERAPY
ANTICOAGULANTTHERAPY
ANTICOAGULANTTHERAPY
BLEEDING
RECURRENT VTE
CTEPH
Echocardiography (ifCTPA not readilyavailable or uncontrolledhypotension)
CUS-based algorithms
Hemodynamicinstability
INTERMEDIATE-HIGHINTERMEDIATE-LOW
plus
(Rescue reperfusion)
(Early discharge)
No validated predictionmodels for VTE patients
Standard-duration vs.extended (indefinite)treatment
Individualized follow-upprograms and intervals
*Biochemical markers include markers of myocardial injury (troponins, heart-type fatty acid-binding protein) and markers of heart failure (BNP or N-terminal-proBNP).†Only antiphospholipid syndrome and high-risk inherited thrombophilia (i.e., homozygosity for factor V Leiden, homozygosity for prothrombin G20210A mutation,double heterozygosity, antithrombin deficiency) are considered. Nevertheless, routine thrombophilia testing is not indicated in PE patients. BNP ¼ B-type natriureticpeptide; CT ¼ computed tomography; CTEPH ¼ chronic thromboembolic pulmonary hypertension; CTPA ¼ computed tomographic pulmonary angiogram; CUS ¼compression ultrasound; Echo ¼ echocardiography; N-terminal-proBNP ¼ N-terminal pro–B-type natriuretic peptide; PE ¼ pulmonary embolism; PESI ¼ pulmonaryembolism severity index; RV ¼ right ventricular; sPESI ¼ simplified pulmonary embolism severity index; V/Q scan ¼ ventilation/perfusion lung scan; VTE ¼ venousthromboembolism.
Konstantinides et al. J A C C V O L . 6 7 , N O . 8 , 2 0 1 6
Pulmonary Embolism Update M A R C H 1 , 2 0 1 6 : 9 7 6 – 9 0
978

CONCLUSIONES
▸ Alta sospecha diagnóstica
▸ Prevención
▸ Elevada mortalidad
▸ Toma de desiciones oportuna
▸ Intervencionismo, probable futuro