Transient Hypogammaglobulinemia of Infancy
48
Transient Transient Hypogammaglobulinemia Hypogammaglobulinemia of Infancy of Infancy Vivek U. Rao, M.D. Fellow, Allergy & Immunology University of Pennsylvania Immunodeficiency Conference April 11, 2005
-
Upload
many87 -
Category
Health & Medicine
-
view
883 -
download
1
Transcript of Transient Hypogammaglobulinemia of Infancy

Transient Transient Hypogammaglobulinemia of Hypogammaglobulinemia of
InfancyInfancy
Vivek U. Rao, M.D.Fellow, Allergy & Immunology
University of PennsylvaniaImmunodeficiency Conference
April 11, 2005

Transient Transient Hypogammaglobulinemia of Hypogammaglobulinemia of
Infancy (THI)Infancy (THI) Medline search:
– Terms used “Transient hypogammaglobulinemia” “Transient hypogammaglobulinaemia” “Pediatric” and “hypogammaglobulinemia” “Pediatric” and “hypogammaglobulinaemia”
– 68 English articles found– 50 were available at the University of
Pennsylvania Biomedical Library or via E-journals; the relevant articles will be discussed during the remainder of today’s conference
THI: Historical BackgroundTHI: Historical BackgroundTransient hypogammaglobulinemia of
infancy– First described in 19561
– Characterized by abnormal delay in onset of immunoglobulin synthesis1
– Physiologic hypogammaglobulinemia in infants is prolonged
Usually occurs at 2-4 months, but lasts until 18-36 months in those with THI2
THI: IncidenceTHI: Incidence True incidence unknown Articles over the years have argued about how
common THI is Tiller and Buckley (Duke Univ.)3
– 1978 paper reported only 11 cases of THI out of 10,000 patients who underwent immunoglobulin studies over 12-year period
Used strict criteria for THI– At least one Ig class > 2 SDs below normal for
age on 2 specimens obtained during infancy– Subsequent labs must show definite increase in
values– No features to suggest other types of primary
immunodeficiency
THI: IncidenceTHI: IncidenceDressler et al.4
– Identified THI in only 5 patients after evaluating 8,000 sera in 2 clinics in Germany over 11 years

THI: IncidenceTHI: Incidence Royal Children’s Hospital in Victoria, Australia1
– Only pediatric immunology center in the state of Victoria (population 4 million)
– Study reviewed data from immunology lab collected between July 1979 and March 1990
Patients < 2 years of age with IgG levels < 5th percentile considered; those with known immunodeficiencies excluded
– 11 boys and 7 girls had “proved THI” (initial IgG low, subsequent level normal)
– 28 children had “probable THI” (initial IgG low, but no subsequent data available)
THI: IncidenceTHI: Incidence Royal Children’s Hospital in Victoria, Australia1
– Study Estimated incidence
– Proved THI: 23 per million births
– Probable THI: 61 per million births Estimated incidence of other immunodeficiencies
(previously calculated from data from same lab)
– XLA – 7 per million births
– CVID – 12 per million births
– Symptomatic absolute IgA deficiency – 24 per million births
– SCID – 14 per million births

THI: IncidenceTHI: IncidenceChildren’s Hospital, Sao Paulo, Brazil
(Grumach et al.)5
– 166 cases of primary immunodeficiency over 15 years
– Most common diagnosesIgA deficiency – 60THI – 14 (8 male, 6 female)Chronic granulomatous disease – 10Complement – 10

THI: IncidenceTHI: IncidenceJapan: Nationwide survey6
– Survey 1 1700 hospitals and institutes in Japan sent
questionnaires asking if they had patients with primary immunodeficiency syndrome 1966-1975
641 replied 628 cases reported
– THI – 116 (18.5%)
– IgA deficiency – 93 (14.8%)
– Selective immunodeficiency other than IgA – 77 (12.3%)
– XLA – 70 (11.1%)
THI: IncidenceTHI: IncidenceJapan: Nationwide survey6
– Survey 2 Physicians who took care of patients reported in first
survey, as well as ~ 100 physicians who might be willing to register new cases
497 patients registered– CVID – 79 – Selective IgA deficiency – 74– XLA – 58– CGD – 54– SCID – 46– Immunodeficiency with telangiectasia – 35– THI – 33 (23 male, 10 female)

THI: PathogenesisTHI: PathogenesisNormal values (n=296) (Stiehm)7
Age No. of subjects
IgG*
mg/dl
IgM*
mg/dl
IgA*
mg/dl
Newborn 22 1031 200 11 5 2 3
1-3 mo 29 430 119 30 11 21 13
4-6 mo 33 427 186 43 17 28 18
7-12 mo 56 661 219 54 23 37 18
13-24 mo 59 762 209 58 23 50 24
25-36 mo 33 892 183 61 19 71 37
3-5 yr 28 929 228 56 18 93 27
6-8 yr 18 923 256 65 25 124 45
9-11 yr 9 1124 235 79 33 131 60
12-16 yr 9 946 124 59 20 148 63
Adult 30 1158 305 99 27 200 61* Mean 1 SD.

THI: PathogenesisTHI: PathogenesisOne view: heterogenous group of errors in
immune system8
Alternative view: normal variant of the immune system in which some mature more slowly than others, just like those with delayed growth
THI: PathogenesisTHI: PathogenesisGenetic evidence
– Soothill et al.9
11 first-degree relatives of patients with hypogammaglobulinemia were followed from birth
4 developed sex-linked hypogammaglobulinemia 5 had probable THI
– Kilic et al.10
Followed 40 Turkish children with THI None had first-degree relatives with known
immunologic defects None had parents or siblings with abnormal IgG,
IgA, or IgM
THI: PathogenesisTHI: PathogenesisSiegel et al.: THI due to deficiency of
helper T cells11
– In vitro studies using lymphocytes from donors17 with THI6 who had recovered from THI13 age-matched healthy children11 parents of children with THI
THI: PathogenesisTHI: PathogenesisSiegel et al.11
– FindingsTHI patients had same number of circulating
B lymphocytes as healthy controlsTHI patients had decreased ability to
synthesize IgG (and to a lesser extent, IgM) in response to pokeweed mitogen (T-cell-dependent B-cell activator)
THI: PathogenesisTHI: PathogenesisSiegel et al.11
– FindingsTHI patients do not have increased
suppressor activity– Based on creating co-cultures with 1:1
ratio of THI patient’s lymphocytes to the parent’s, then stimulating with pokeweed
THI: PathogenesisTHI: PathogenesisSiegel et al.11
– FindingsTHI patients have deficient helper-T-cell
function– T and B cells were separated, recombined
1:1, and cultured for 7 days with pokeweed mitogen
• Parental T + parental B high IgG• THI T + THI B low IgG• Parental T + THI B high IgG• THI T + parental B low IgG
THI: PathogenesisTHI: PathogenesisSiegel et al.11
– FindingsIn THI, B cells are intrinsically intact
– In vitro infection with EBV (T-cell-independent B-cell activator) IgG and IgM production similar in THI patients and healthy controls
Absolute number of CD4+ helper cells decreased in THI patients compared to healthy controls and parents
– Number is normal in those who have recovered from THI
THI: PathogenesisTHI: PathogenesisKilic et al.10
– Findings26 patients with THI studied
– Normal CD4 numbers seen in all 26

THI: PathogenesisTHI: PathogenesisOther possibilities12
– Defective production of cytokines– Abnormal B-cell response to mediators– Inhibition of B cells by cytokines

THI: PathogenesisTHI: PathogenesisKowalczyk et al. (1997)12
– 30 children with THI (IgG > 2 SD below mean)10 proved20 probable
– 15 children with IgA deficiency– 40 controls with recurrent infections but
negative immunodeficiency work-up– In vitro study took PBMCs, stimulated them
with phytohemagglutinin, and studied cytokines
THI: PathogenesisTHI: PathogenesisKowalczyk et al. (1997)12
– ResultsNormal numbers of CD3, CD4, CD8, CD19,
and CD22 lymphocytes in THI patientsIncreased TNF-alpha and TNF-beta in
proved and probable THIIncreased IL-10 in proved THINo change in IL-1, IL4, or IL-6When THI resolved, TNF-alpha and TNF-
beta were normal, but IL-10 remained elevated (at 6-12 month follow-up)

THI: PathogenesisTHI: PathogenesisKowalczyk et al. (1997)12
– ConclusionsTNF may affect B cells by arresting IgG and
IgA productionBalance between TNF and IL-10 may affect
development of IgG-producing B cells

THI: PathogenesisTHI: PathogenesisKowalczyk et al. (2002)13
– 14 with THI (IgG > 2 SD below mean with normal IgM and IgA)
All eventually had normalization of IgG– 20 with selective IgA deficiency– 29 controls with recurrent infections but
negative work-up for immunodeficiency– Examined Th1 (TNF-alpha, TNF-beta, IFN-
gamma) and Th2 (IL-4, IL-10) cytokines
THI: PathogenesisTHI: PathogenesisKowalczyk et al. (2002)12
– FindingsIncreased frequency of TNF-alpha- and
TNF-beta-positive CD3+/CD4+ in THISlightly increased frequency of CD4+/IL-10
(not significant) in THI with no difference in CD4+/IL-4
IL-12 but not IL-18 level (both needed for Th1 phenotype) significantly elevated in THI
– IL-12 level decreased significantly when IgG normalized
THI: PathogenesisTHI: PathogenesisKowalczyk et al. (2002)12
– FindingsTHI patients had an increased proportion of
IL-12+/CD33+ after stimulation with IFN-gamma/LPS
– ConclusionTHI associated with an excessive Th1
response in which IL-12 secretion is elevated
THI: Associated InfectionsTHI: Associated InfectionsCan be asymptomatic or have recurrent
infections2
– URIs– Otitis media– Sinusitis– Pneumonia (less common)

THI: Associated InfectionsTHI: Associated InfectionsKilic et al.10
– Prospective evaluation of 40 patients in Turkey with THI
– Criteria for diagnosis At least 1 major Ig class 2 SD below mean for
age Normal specific antibodies to polio antigen and
isohemagglutinins Intact cellular immunity Absence of features of other immunodeficiency
syndromes
THI: Associated InfectionsTHI: Associated InfectionsKilic et al.10
– Clinical features at presentation Upper respiratory tract infection 28 (70%) Lower respiratory tract infection 11 (27%) Otitis media 9 (22%) Gastroenteritis 5 (12%) Urinary tract infection 3 (7%) Lymphadenitis 1 (2%) GERD 1 (2%) Asthma, allergic bronchitis 11 (27.5%) Atopic dermatitis 2 (5%)
THI: Associated InfectionsTHI: Associated Infections Respiratory infections
– Cano et al.14
Followed 13 patients with THI; did further testing on 11
Antibodies to respiratory viruses tested – 9 of 11 THI patients tested prior to 17 months
lacked specific antibodies despite recurrent respiratory tract infections
– In contrast, 5 of 16 controls lacked specific antibodies
• 3 had no prior history of respiratory infections
• 1 had IgG checked and was found to have low level
THI: Associated InfectionsTHI: Associated Infections Respiratory infections
– Cano et al.14
13 patients with THI seen at follow-up between 20 and 44 months of age
– 2 never demonstrated positive viral serologies even though IgG normalized
– 1 became serology positive at same time IgG normalized
– 2 had IgG return to normal before becoming serology positive
– 8 demonstrated positive viral serologies prior to normalization of IgG
THI: Associated InfectionsTHI: Associated InfectionsClostridium difficile infection
– Gryboski et al.15
Retrospective review of records of infants and children with diarrhea and C. difficile seen over 4-year period
– 43 identified with diarrhea and C. difficile
– 2 sets of controls used
• 20 with abdominal pain and no diarrhea
• 40 with chronic diarrhea and no evidence of C. difficile

THI: Associated InfectionsTHI: Associated InfectionsClostridium difficile infection
– Gryboski et al.15
Diarrhea + C. difficile
– 15/43 with hypogammaglobulinemia
– 12 with low IgA and IgG
– 3 with low IgA and normal IgG
– All 15 had normal levels 6-12 months later Abdominal pain but no diarrhea
– 0/20 with hypogammaglobulinemia Diarrhea but no C. difficile
– 3/40 with low IgA (all 3 had milk-protein allergy)
THI: Associated InfectionsTHI: Associated InfectionsClostridium difficile infection
– Gryboski et al.15
Conclusion: THI patients are at increased risk of diarrhea from C. difficile, due to increased use of antibiotics or inadequate local antibody response to organism
THI: Associated InfectionsTHI: Associated InfectionsBacterial gastroenteritis
– Melamed et al.16
Retrospective review of data from a bacteriology lab over 16-month period
Records of children with stool specimens positive for Campylobacter jejuni analyzed
51 cases found 5 were previously diagnosed with an
immunodeficiency– 1 combined immunodeficiency– 2 XLA– 1 agammaglobulinemia– 1 THI
THI: Associated InfectionsTHI: Associated InfectionsBacterial gastroenteritis
– Melamed et al.16
5 immunodeficiency patients
– More prolonged course of diarrhea (at least 1 week)
– Multiple pathogens isolated from stools 46 “normal” patients
– Diarrhea lasted 2-7 days
– No other organisms isolated THI patient
– Stool also grew Shigella, Salmonella, and E. coli
THI: Associated InfectionsTHI: Associated Infections Pneumocystis carinii pneumonia17
– Case report of 3.5 month old boy with PCP pneumonia (dx’ed by BAL)
Normal specific antibody production following tetanus, diptheria, and Hib immunization
Normal T cell numbers Normal IgM but borderline low IgG and absent IgA
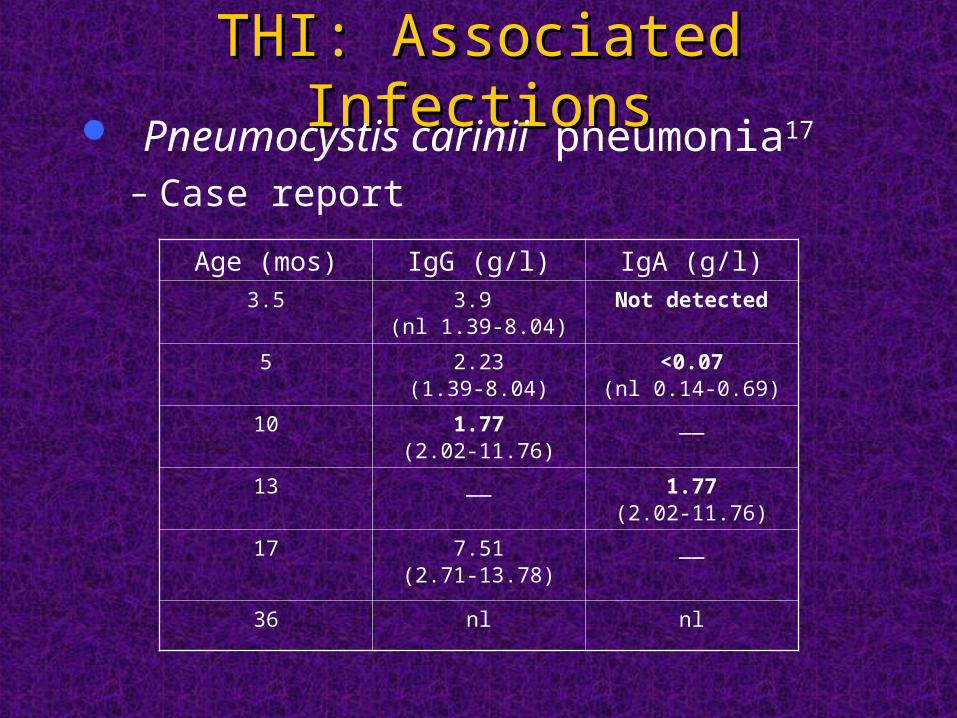
THI: Associated InfectionsTHI: Associated Infections Pneumocystis carinii pneumonia17
– Case report
Age (mos) IgG (g/l) IgA (g/l)3.5 3.9
(nl 1.39-8.04)Not detected
5 2.23(1.39-8.04)
<0.07(nl 0.14-0.69)
10 1.77(2.02-11.76)
__
13 __ 1.77(2.02-11.76)
17 7.51(2.71-13.78)
__
36 nl nl
THI: Associated InfectionsTHI: Associated Infections Poliomyelitis18
– Case report of 6-month old Japanese boy with THI and neurovirulent variation of Sabin type 2 oral poliovirus (based on PCR of CSF and stool)
Patient with febrile seizure at 4 months; abnormal eye movements (horizontal nystagmus-like) and no visual recognition at 5 months
Child never received OPV, but developed poliovirus meningoencephalitis (presumably from contact with someone who was shedding)
IgG normalized by age 2, with no subsequent episodes of unusual or severe infections

THI: DiagnosisTHI: DiagnosisNo definite criteria for diagnosis19
– Occurs in infancy and generally resolves by 24-36 months
– Usually characterized by serum IgG level 2 SDs below normal
– IgA (and IgM) may also be low– Antibody responses to protein antigens
(diptheria, tetanus) are normal
THI: DiagnosisTHI: DiagnosisDiagnosis can truly be made only
retrospectively20
– Individuals may have normalization of IgG but persistently low IgA levels, thus meeting criteria for selective IgA deficiency

THI and Risk for Other THI and Risk for Other DiseasesDiseases
Atopy– Not a prominent feature in most series1
– Exception: Fineman et al.21
Report of 4 infants seen within a 1-year period
All 4 had THI, food allergies, and elevated IgE
THI and Risk for Other THI and Risk for Other DiseasesDiseases
Atopy– Exception: Walker et al.1
Of 15 children with proved THI, 12 had either atopic disease or food allergy/intolerance
– 4 with cow milk protein intolerance
– 3 with asthma
– 2 with asthma and eczema
– 1 with asthma and immediate food hypersensitivity reaction

THI: TreatmentTHI: TreatmentIVIG: To give or not to give?
– Tiller and Buckley3
Followed 11 children with THI None received IVIG, and none had serious
infections
– Cano et al.14
Followed 13 patients with THI 5 received IM IG therapy (usually for a short period
of time – 9 months or so)– Therapy did not seem to delay onset of antibody
synthesis– Conclusion: IM IG should be considered in THI
since there is minimal evidence of harm
THI: Long-term OutcomeTHI: Long-term OutcomeLittle data availableLong-term follow-up needed to exclude
other etiologies, such as CVID2
THITHIReferences:1. Walker AM, Kemp AS, Hill DJ, Shelton MJ. Features of transient hypogammaglobulinaemia in
infants screened for immunological abnormalities. Archives of Disease in Childhood. 70(3):183-6, 1994 Mar.
2. Ballow M. Primary immunodeficiency disorders: antibody deficiency. Journal of Allergy & Clinical Immunology. 109(4):581-91, 2002 Apr.
3. Tiller TL Jr, Buckley RH. Transient hypogammaglobulinemia of infancy: review of the literature, clinical and immunologic features of 11 new cases, and long-term follow-up. Journal of Pediatrics. 92(3):347-53, 1978 Mar.
4. Dressler F, Peter HH, Muller W, Rieger CH. Transient hypogammaglobulinemia of infancy: Five new cases, review of the literature and redefinition. Acta Paediatrica Scandinavica. 78(5):767-74, 1989 Sep.
5. Grumach AS, Duarte AJ, Bellinati-Pires R, Pastorino AC, Jacob CM, Diogo CL, Condino-Neto A, Kirschfink M, Carneiro-Sampaio MM. Brazilian report on primary immunodeficiencies in children: 166 cases studied over a follow-up time of 15 years. Journal of Clinical Immunology. 17(4):340-5, 1997 Jul.
6. Hayakawa H, Iwata T, Yata J, Kobayashi N. Primary immunodeficiency syndrome in Japan. I. Overview of a nationwide survey on primary immunodeficiency syndrome. Journal of Clinical Immunology. 1(1):31-9, 1981 Jan.
7. Stiehm ER, Fudenberg HH. Serum levels of immune globulins in health and disease: a survey. Pediatrics. 37(5):715-27, 1966 May.
8. Dalal I, Reid B, Nisbet-Brown E, Roifman CM. The outcome of patients with hypogammaglobulinemia in infancy and early childhood. Journal of Pediatrics. 133(1):144-146.
THITHIReferences:9. Soothill JF. Immunoglobulins in first-degree relatives of patients with
hypogammaglobulinaemia. Transient hypogammaglobulinaemia: a possible manifestation of heterozygocity. Lancet. 1(7550):1001-3, 1968 May 11.
10. Kilic SS, Tezcan I, Sanal O, Metin A, Ersoy F. Transient hypogammaglobulinemia of infancy: clinical and immunologic features of 40 new cases. Pediatrics International. 42(6):647-50, 2000 Dec.
11. Siegel RL. Clinical disorders associated with T cell subset abnormalities. Advances in Pediatrics. 31:447-80, 1984.
12. Kowalczyk D, Mytar B, Zembala M. Cytokine production in transient hypogammaglobulinemia and isolated IgA deficiency. Journal of Allergy & Clinical Immunology. 100(4):556-62, 1997 Oct.
13. Kowalczyk D, Baran J, Webster AD, Zembala M. Intracellular cytokine production by Th1/Th2 lymphocytes and monocytes of children with symptomatic transient hypogammaglobulinaemia of infancy (THI) and selective IgA deficiency (SIgAD). Clinical & Experimental Immunology. 127(3):507-12, 2002 Mar.
14. Cano F, Mayo DR, Ballow M. Absent specific viral antibodies in patients with transient hypogammaglobulinemia of infancy. Journal of Allergy & Clinical Immunology. 85(2):510-3, 1990 Feb.
15. Gryboski JD, Pellerano R, Young N, Edberg S. Positive role of Clostridium difficile infection in diarrhea in infants and children. American Journal of Gastroenterology. 86(6):685-9, 1991 Jun.
THITHIReferences:16. Melamed I, Bujanover Y, Igra YS, Schwartz D, Zakuth V, Spirer Z.
Campylobacter enteritis in normal and immunodeficient children. American Journal of Diseases of Children. 137(8):752-3, 1983 Aug.
17. Smart JM, Kemp AS, Armstrong DS. Pneumocystis carinii pneumonia in an infant with transient hypogammaglobulinaemia of infancy. Archives of Disease in Childhood. 87(5):449-50, 2002 Nov.
18. Inaba H, Hori H, Ito M, Kuze M, Ishiko H, Asmar BI, Komada Y. Polio vaccine virus-associated meningoencephalitis in an infant with transient hypogammaglobulinemia. Scandinavian Journal of Infectious Diseases. 33(8):630-1, 2001.
19. Yates AB, Shaw SG, Moffitt JE. Spontaneous resolution of profound hypogammaglobulinemia. Southern Medical Journal. 94(12):1215-6, 2001 Dec.
20. McGeady SJ. Transient hypogammaglobulinemia of infancy: need to reconsider name and definition. Journal of Pediatrics. 110(1):47-50, 1987 Jan.
21. Fineman SM, Rosen FS, Geha RS. Transient hypogammaglobulinemia, elevated immunoglobulin E levels, and food allergy. Journal of Allergy & Clinical Immunology. 64(3):216-22, 1979 Sep.