Toolkit for PCBH in Pediatric Primary Care out Hirschprung’s Any constipating medications Diet...
50
Toolkit for PCBH in Pediatric Primary Care Lesley Manson, Psy.D., Assistant Chair of Integrated Initiatives, Clinical Assistant Professor, Arizona State University, Phoenix, AZ Tawnya Meadows, Ph.D., BCBA-D, Co-Chief of Behavioral Health in Primary Care-Pediatrics, Geisinger, Danville, PA Matthew Tolliver, PhD, Assistant Professor/Psychologist, Eastern Tennesee State University Pediatrics, Johnson City, TN Allison Allmon Dixson, Ph.D., Pediatric Psychologist, Gundersen Health System, La Crosse, WI Cody Hostutler, Ph.D., Psychologist, Nationwide Children's Hospital, OH Sarah Trane, PhD, Assistant Professor, Division of Integrated Behavioral Health (Pediatrics), Mayo Clinic Health System, La Crosse, WI Brian DeSantis, Psy.D., ABPP, VP, Behavioral Health, Peak Vista Community Health Centers, Colorado Springs, CO Session # PC 3 CFHA 20 th Annual Conference October 18-20, 2018 • Rochester, New York
-
Upload
duongkhuong -
Category
Documents
-
view
215 -
download
0
Transcript of Toolkit for PCBH in Pediatric Primary Care out Hirschprung’s Any constipating medications Diet...

Toolkit for PCBH in Pediatric Primary Care
Lesley Manson, Psy.D., Assistant Chair of Integrated Initiatives, Clinical Assistant Professor, Arizona State University, Phoenix, AZ
Tawnya Meadows, Ph.D., BCBA-D, Co-Chief of Behavioral Health in Primary Care-Pediatrics, Geisinger, Danville, PA
Matthew Tolliver, PhD, Assistant Professor/Psychologist, Eastern Tennesee State University Pediatrics, Johnson City, TN
Allison Allmon Dixson, Ph.D., Pediatric Psychologist, Gundersen Health System, La Crosse, WI
Cody Hostutler, Ph.D., Psychologist, Nationwide Children's Hospital, OH
Sarah Trane, PhD, Assistant Professor, Division of Integrated Behavioral Health (Pediatrics), Mayo Clinic Health System, La Crosse, WI
Brian DeSantis, Psy.D., ABPP, VP, Behavioral Health, Peak Vista Community Health Centers, Colorado Springs, CO
Session # PC 3
CFHA 20th Annual ConferenceOctober 18-20, 2018 • Rochester, New York

Toilet Talk• Cody Hostutler, PhD
• Pediatric Primary Care Psychologist at Nationwide Children’s Hospital• Assistant Professor at The Ohio State University
• Tawnya Meadows, PhD, BCBA-D• Co-Chief of Behavioral Health in Primary Care - Pediatrics at Geisinger• Assistant Professor at Temple University
Hayley Quinn, PsyD• Psychologist at West Seattle Pediatrics part of Swedish Pediatrics
CFHA 20th Annual ConferenceOctober 18-20, 2018 • Rochester, New York
Faculty Disclosure
The presenters of this session have NOT had any relevant
financial relationships during the past 12 months.

Potty TrainingANTICIPATORY GUIDANCE
Typical Potty Training• Start anticipatory guidance at 18 mos
• Average training period is 6 months• Earlier start -> longer training period• Starting before 27 months does not result in earlier completion
• 85% of 30 month olds are continent during the day, Bowel Control usually occurs by 36 months
• Nighttime control occurs months to years later and is expected at 5-7 years old

Fun Facts• Girls complete toilet training 2-3 mos earlier than boys
• First born usually takes longer
• Racial Differences• 50% of AA parents reported that it was important to have child toilet
trained by age 2 compared to 4% of Caucasian Families• AA parents start toilet training at 18 mos, Caucasian families start
around 25 mos
• Digo People in East Africa teach their children to urinate and stool on command by 4-5 months of age

Potty training readiness is based on development of readiness, not age
• Ability to stay dry for 2 hours or more
• Understand “wet” “dry” “pants” and able to tell parents when they are wet/dirty
• Showing interest: Asking for “big girl/boy” underwear; Asking about toilet
• Follows simple directions
• Able to recognize, express, and delay urge to use bathroom
• Regular BM schedule
• Able to pull down diapers/training pants/underwear
Potty Training Readiness

Two ApproachesParent led
•“Potty Party”
•Increase fluids
•Regular sit times
•Rewards for compliance• Sticker chart/M&Ms
•Over-correction for accidents
Child led
•Build vocabulary
•Presentation of the potty chair
•Shaping with positive reinforcement
•Transition to underwear
•Most consistent with AAP
Notes:- No head to head comparison trials - Independent trials show little difference in outcome- AAP approach most closely resembles child-led approach
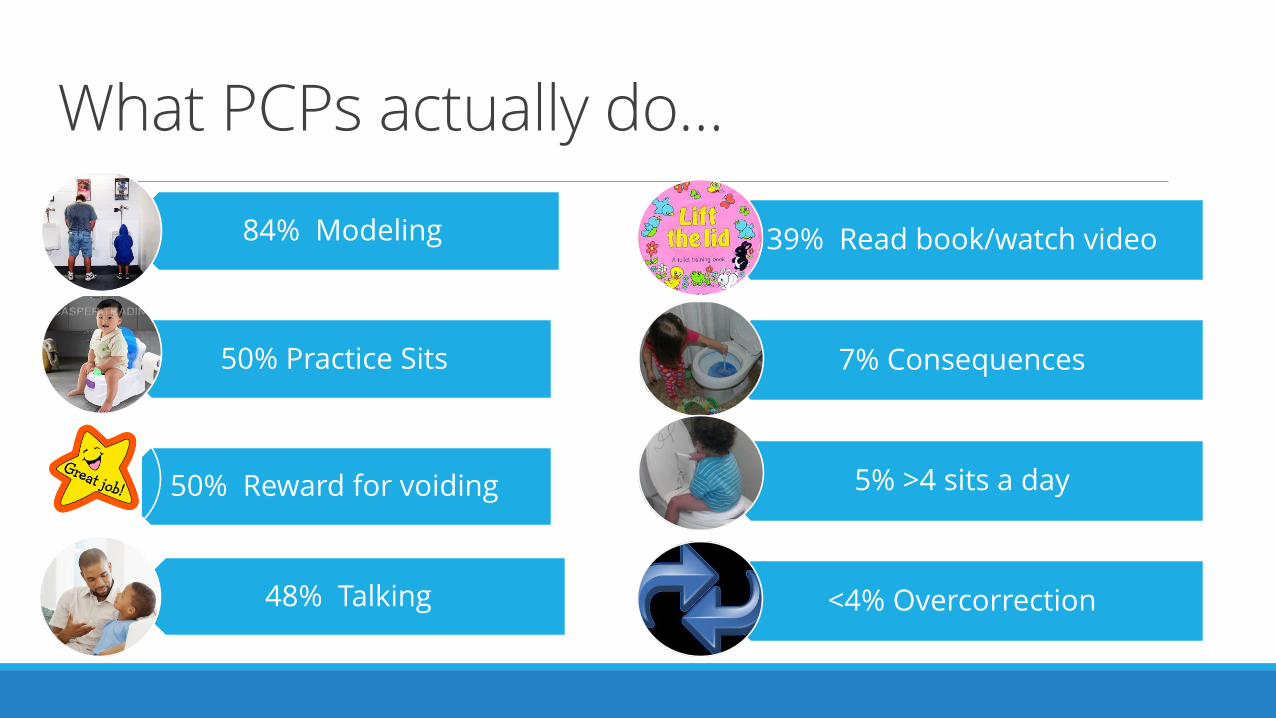
What PCPs actually do…
84% Modeling
50% Practice Sits
50% Reward for voiding
48% Talking
39% Read book/watch video
7% Consequences
5% >4 sits a day
<4% Overcorrection

Preliminary considerations (instructional readiness, physical readiness)
Pretraining considerations
Dry pants trials every 3-5 minutes
Push Fluid loading constantly (salty snacks, modeling, variety)
Pants up/down
Prompted potty trials
Immediate detection of urine
Motivation
Dealing with accidents
Cleanliness training
Azrin and Foxx (1974)
Middle-Ground Recommendations for Primary CareChild compliance not seen as a critical issue but it is huge
◦ Need instructional control before begin training
Multiple sits (at least every 30’)
Increase fluids to promote learning trials
Dry pants checks with consequences for wet/dry (at least every 15’)
Rewards for sits with additional rewards for being productive in the toilet
Have child participate in clean-up ◦ Not punitive◦ Socially sterile

When to not start
Traveling
Illness (of child or caregiver)◦ Especially GI-sickness/Constipation
Changes or transitions◦ Birth of sibling
◦ Changing from crib to bed
◦ Moving to new home
Other stressors◦ Death of parent
◦ Parent divorce or separation
If caregivers don’t have time to commit

Toileting Problems

Parents insist on training earlyProvide education on effects of training too early
Understand reasons and try to problem-solve reasons (e.g., daycare, cost, time)
Remember, behavior change suggests replacing rather than stopping behavior◦ Have parents train readiness skills rather than actual toileting

Toileting RefusalUp to 20% of developmentally typical children
Typically take longer to continence
Factors associated:◦ Training too early◦ Parent-child relational problem◦ Fear/Anxiety◦ Difficult Temperament◦ Painful Stools◦ Difficulty w/ limit setting
Recommendations◦ Do not punish/nag◦ Take a Break◦ Encourage child to imitate
family◦ Read books, watch videos◦ Encourage independence
(changing own diapers)◦ Treat large/hard stools◦ Reinforce successful
approximations

Toileting FearsFlushing (sound, object permanence), painful stools, separation fears
Graduated Exposure/Shaping w/ Reinforcement
• May work on tolerating being in the bathroom
• Being in bathroom when toilet is flushed by someone else
• Gradually work towards use of toilet

Diurnal EnuresisPrimary (never dry for 6 months) vs. Secondary (previously dry for 6 months)
Signs of possible medical concern:◦ Marked increase in drinking
◦ Stress incontinence (e.g., sneezing, laughing, coughing)
◦ Constantly damp underwear

Nocturnal EnuresisOccurs in 20% of 5yos and 10% of 6yos (DSM-V)
Spontaneous resolution occurs at rate of 15% per year
Organic etiology only found in 2-3% of children
Interventions◦ Medical evaluation
◦ Normalize
◦ Address the parental response
◦ The “night alarm” system
◦ Reinforcement/token economy system

Enuresis: EtiologyFamilial Factors
•15% No parental history of NE
•44% one parent with positive history of NE
•77% in children who have both maternal and paternal positive history for NE
Sleep Factors
•Parents of children with NE report remarkably heavy sleep
•Sleep EEG research suggests enuretic episodes indiscriminately transpire across the night
•Sleep patterns parallel between children with and without enuresis
Biological Factors
•Mean bone growth and height less developed among children with enuresis
•Small bladder capacity. Research suggests bladder capacity remains the same during day and night
•Increased nocturnal urine output. Differences in production of the antidiuretic hormone (ADH)
Enuresis: Assessment
Medical Assessment
Behavioral Assessment: Interview
Behavioral Assessment: Recording Data
Enuresis - Treatment
Medications
◦ Anti-cholinergic
◦ Tricyclic antidepressants
◦ Imipramine
◦ DDAVP

IMPRAMINE – SIDE EFFECTSUncommon with low dose◦ Anxiety◦ Insomnia◦ Adverse personality changes◦ Loss of appetite
Overdose from excess ingestion
Toxicity secondary to overdose – potentially fatal cardiac arrhythmias, hypotension, respiratory complications, convulsions.

DDAVP NASAL SPRAY TREATMENTSignificant improvement in several double-blind randomized trials
Decreased in mean frequency of wet nights ranging from 10% to 90% in 18
published control trials
Complete dryness achieved in 10% to 40% (average 25%)
Side effects minimal
Relapse rate high after short-term treatment
◦ Relapse rate varies from 50% to 95%

BEHAVIORAL INTERVENTIONS
◦ Most widely researched
◦ Assume nighttime continence can be acquired
◦ Do not assume there are no other problems
◦ Require that a general foundation of behavior management is already in place
◦ Require change on part of parent
BEHAVIORAL INTERVENTIONSIncentive system
Alarm◦ Combine with other interventions
Retention-control training
Waking schedules
Self-monitoring◦ Should be used in any kind of behavioral intervention◦ Effective when combined with pharmacotherapy
INCENTIVE SYSTEMSTask analysis◦ Several steps to allow contact with incentive◦ Effort required must be reasonable
Identify functional incentives with attainable goals – grab bag, connect dots for reward
Establish contingent relationships and present incentive immediately after response
Follow-up◦ 70% marked improvement◦ 25% cure rate

Moisture Alarm ◦ Classical Conditioning◦ Full bladder◦ Voids◦ Alarm sounds◦ Awakenings
◦ Operant Conditioning◦ Avoid aversive conditions during night (e.g., waking up to a wet bed,
cleaning up procedures, changing bed linens)
◦ Research suggests up to 70% successful outcomes
Downside to ALARMS
Possible embarrassment
“Rolling Over” pulls it off
May not wake child
May not wake in time to avoid a wet bed
Wakes other family members
Takes 2-4 months on average and a LOT of work!

INAPPROPRIATE PARENTAL ATTEMPTS TO “HELP” CHILDREN WHO WET THE BED
Displaying wet sheets
Making the child wash sheets
Punishing child
Withdrawing privileges
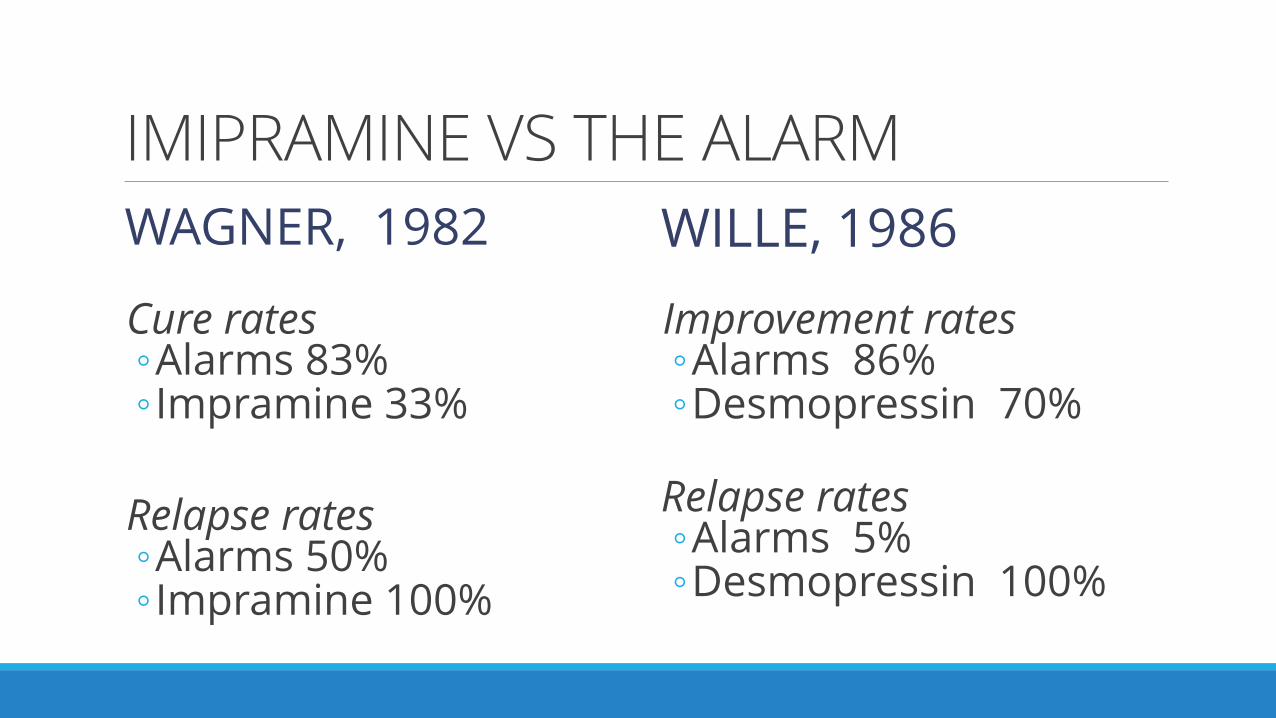
IMIPRAMINE VS THE ALARM
WAGNER, 1982
Cure rates ◦Alarms 83%◦ Impramine 33%
Relapse rates◦Alarms 50%◦ Impramine 100%
WILLE, 1986
Improvement rates◦Alarms 86%◦Desmopressin 70%
Relapse rates◦Alarms 5%◦Desmopressin 100%

Encopresis•Occurs in 2.8% of 4yos and 1.6% of 10yos
(Sood et al., 2016)
•1-2% of the child population
•Boys are 3-6 times more likely to have it than girls
•Mean onset is 7 years old
•95% of children referred for treatment of encopresis have constipation

Constipation and Withholding

Clinical/Behavioral Signs of Encopresis
◦ Unusually large stools
◦ “Accidents” or “Streaks” in
underwear
◦ Unusually foul-smelling stools
◦ Painful Stools
◦ Kid doesn’t notice smell and
discomfort
◦ Infrequent bowel movements
(3-5 days)
◦ Hiding of underwear
◦ Complaints from family
members or peers
◦ Distended stomach
◦ Lethargy
Encopresis: Etiology◦ Little support for genetic basis for the disorder
◦ Little support for emotional and behavioral problems associated with encopresis
◦More a problem of dysfunction of the bowel

Encopresis: AssessmentMedical Assessment◦ Rule out Hirschprung’s
◦ Any constipating medications
◦ Diet (i.e., fiber intake, water)
Behavioral Assessment: Recording Data ◦ Provide Chart for recording bowel
movements
◦ Assess place, number of voids, size and consistency of void, reaction
◦ Record fiber intake and exercise
Behavioral Assessment: Interview◦ Toilet training history
◦ Any behavioral or emotional problems
◦ Recent stressful precipitating events
◦ Current status of toileting habits and bowel movements
◦ Environmental contributors (e.g., routine, diet and exercise)
◦ Consequences (e.g., parental reactions, child reactions)
◦ Child motivation for treatment

Bristol Stool Scale


Retentive Encopresis◦Patient Education◦Hang in there, it may take months◦ Most failure result from stopping Tx too soon
◦ May require 6 weeks to 6 months
◦Not purposeful behavior – won’t respond to punishment or rewards alone
◦ Long-term “psychotherapy” ineffective

Encopresis: TreatmentCombination of medical and behavioral treatment the most effective approach
Medical Treatment◦ Clean out the bowel/soften stools
◦ Enemas
◦ Laxatives
◦ Increase fiber and exercise
◦ Ensure regular bowel movements

Encopresis: Treatment
Behavioral Treatment
• Scheduled toilet sits • After meals or suppositories/laxatives
• Make relaxing
• Keep brief (e.g., 5-10 minutes)
• Reinforcers for sits and then poops in the toilet
• Minimize reaction to accidents
• Temporary discontinuation of toilet training
• Create a comfortable environment
Retentive Encopresis: Maintenance Therapy
Dietary education◦Balanced diet w/ Increased Fiber Intake◦ grains, fruits, veggies, fiber supplements
◦ 20 to 35 grams of fiber daily
◦ Juices that contain sorbitol◦ prune, pear, apple
◦ “Limit” dairy products that slow transit time

Retentive Encopresis: Maintenance
Daily record of bowel activity◦Frequency
◦“Texture”
◦Amount
◦“Accidents”
◦Time of Day

Encopresis: Guidelines for referral
To: GI Specialist:
◦ Soiling/constipation doesn’t resolve with standard treatment after
3-6 mos.
◦ Frequent soiling and child distress
◦ Primary Care Physician is in doubt as to the cause of the symptoms
◦ Concern over presence of organic disease

Using New Skills
Enuresis◦What would be a good behavioral protocol for a child who is wetting daily at daycare?

Nocturnal enuresis
What if the child won’t wake to the alarm?

Encopresis
What would be a good behavioral protocol for a child who is soiling daily after school?

Vignette
Parent of an African-American 18 month, natal female comes in to see
PCP for well-check. Mother expressed that she needs patient to be
potty trained as her siblings were trained by this age and she can’t deal
with the stress and financial costs of diapers. PCP provided education
on developmental expectations, but mother remains unsatisfied and
frustrated. PCP offers for mother to talk with BHC and she agrees
stating, “anything that get’s her out of diapers!”

Session Evaluation
Use the CFHA mobile app to complete the
evaluation for this session.
Thank you!

Toilet Talk• Cody Hostutler, PhD
• Pediatric Primary Care Psychologist at Nationwide Children’s Hospital• Assistant Professor at The Ohio State University
• Tawnya Meadows, PhD, BCBA-D• Co-Chief of Behavioral Health in Primary Care - Pediatrics at Geisinger• Assistant Professor at Temple University
Hayley Quinn, PsyD• Psychologist at West Seattle Pediatrics part of Swedish Pediatrics
CFHA 20th Annual ConferenceOctober 18-20, 2018 • Rochester, New York