PRE-IMPLANTATION GENETIC DIAGNOSIS AND ASSISTED ... 2007... · PRE-IMPLANTATION GENETIC DIAGNOSIS...
34
MELBOURNE IVF PRE-IMPLANTATION GENETIC DIAGNOSIS AND ASSISTED REPRODUCTIVE TECHNOLOGY IN HAEMOPHILIA DR PENELOPE FOSTER
Transcript of PRE-IMPLANTATION GENETIC DIAGNOSIS AND ASSISTED ... 2007... · PRE-IMPLANTATION GENETIC DIAGNOSIS...
MELBOURNE IVF
PRE-IMPLANTATION GENETIC DIAGNOSIS AND ASSISTED
REPRODUCTIVE TECHNOLOGY IN HAEMOPHILIA
DR PENELOPE FOSTER
MELBOURNE IVF
WHAT IS PGD ?
early embryo diagnosisallows selection of unaffected embryos for transfer to patientalternative to antenatal testing and termination of affected pregnancy

MELBOURNE IVF
TECHNIQUE OF PGD
standard IVF cyclebiopsy of 1 or 2 cells from day 3 embryodiagnostic testing on biopsied cellsselection of embryos for transfer

MELBOURNE IVF
PGD IN HAEMOPHILIA
OPTIONS Sex selection:
if affected husband, all male offspring unaffected, all females carriers = select male embryos for transferif carrier wife, 1/2 males affected, 1/2 females carrier = select female embryos for transfer
MELBOURNE IVF
PGD IN HAEMOPHILIA
OPTIONSSpecific gene detection
avoids discarding unaffected male embryosavoids transfer of carrier female embryos

MELBOURNE IVF
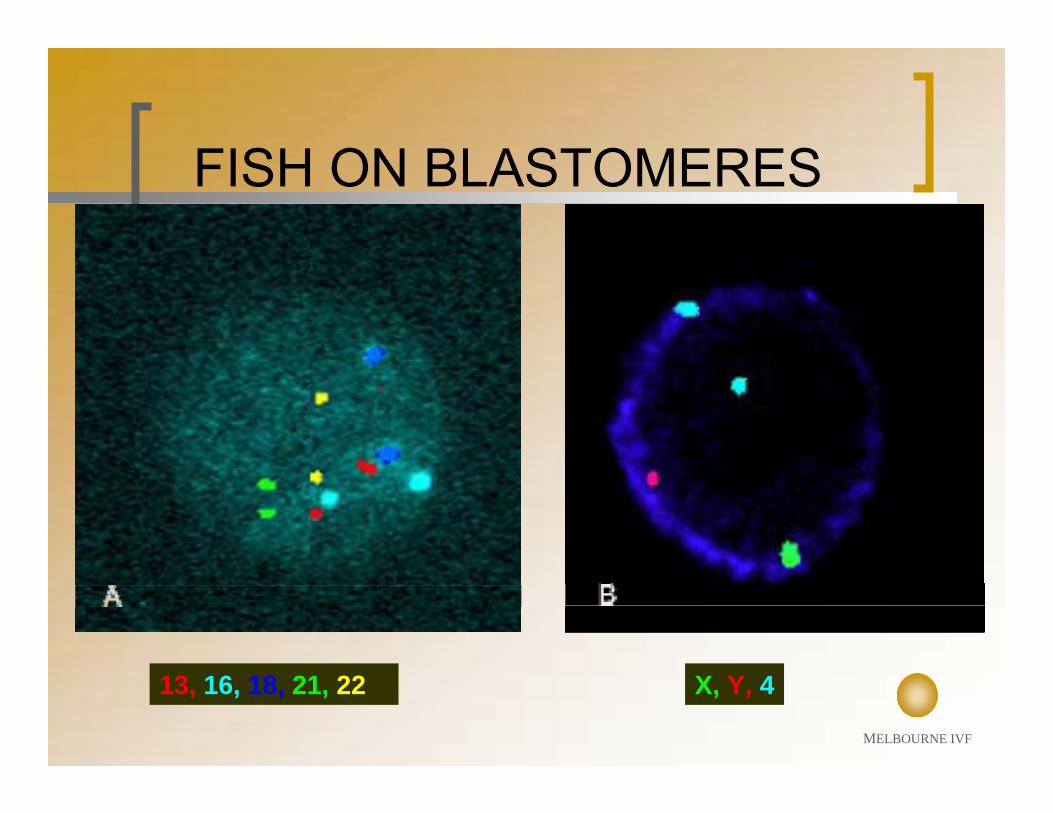
SEX SELECTION - FISH
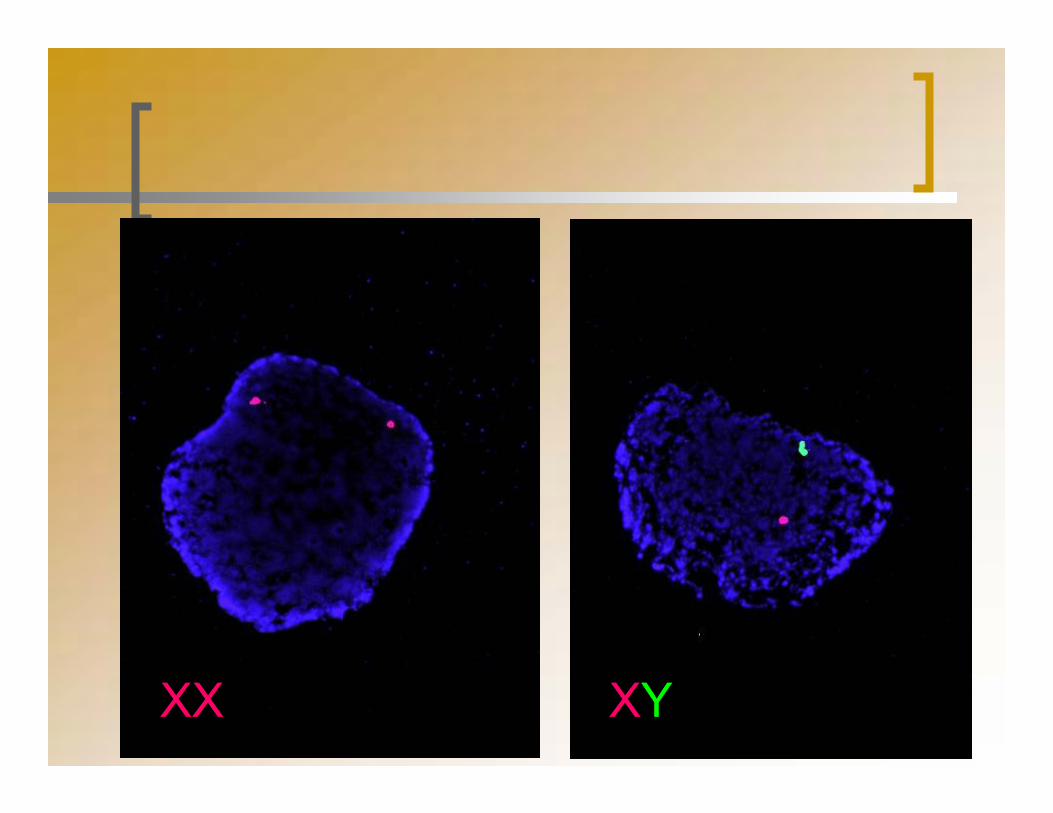
FLUORESCENT IN-SITU HYBRIDISATIONdetects chromosome number cell from embryo fixed to slideapply FISH probesDNA sequences complementary to small segment of particular chromosomeprobes labelled with coloured fluorochromescoloured spots indicate presence of sequence8-probe FISH – chromosomes 4,13,16,18,21,22,X,Yselect euploid XX or XY embryos for transfer
MELBOURNE IVF
13, 16, 18, 21, 22 X, Y, 4
FISH ON BLASTOMERES
MELBOURNE IVF
XX XY
MELBOURNE IVF
PGD FOR SPECIFIC GENE DETECTION
DNA amplification by PCR2 cells from embryofragment analysis on DNA sequencerinclusion of informative markersindividualised tests for each couplesignificant time and effort required for each test
MELBOURNE IVF
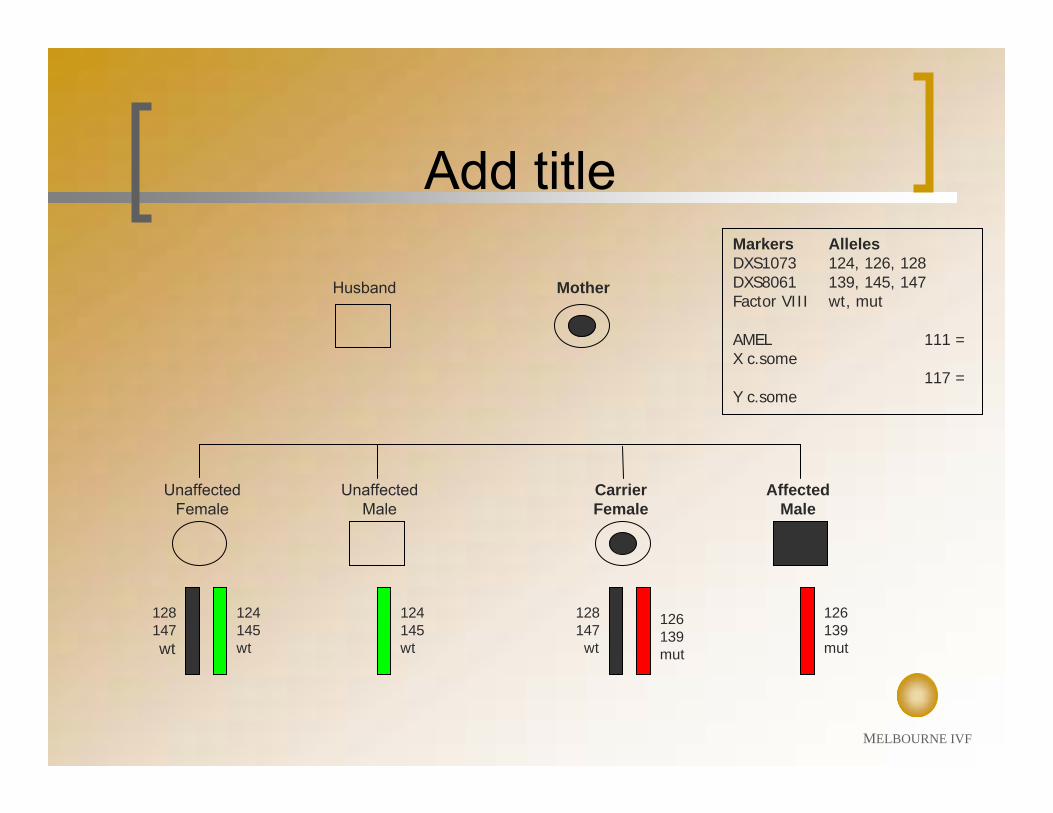
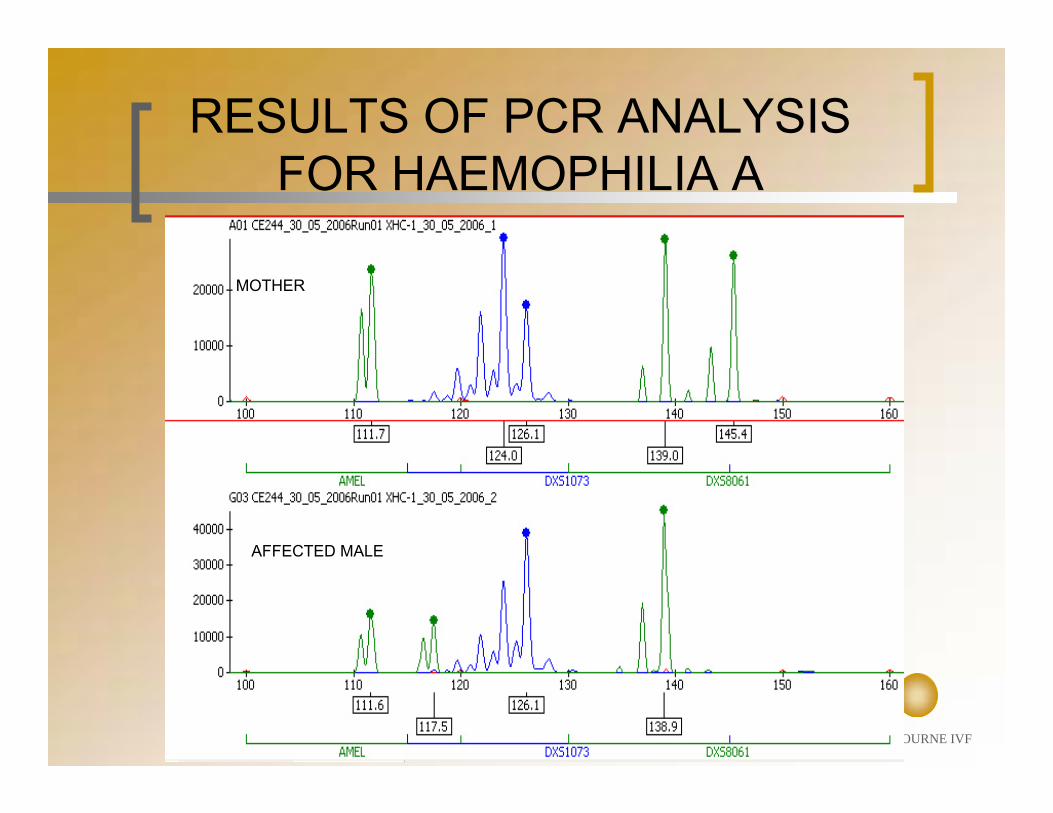
Markers AllelesDXS1073 124, 126, 128DXS8061 139, 145, 147Factor VIII wt, mut
AMEL 111 = X c.some
117 = Y c.some
128147wt
126139mut
124145wt
124145wt
126139mut
128147wt
Add title
Unaffected Male
Unaffected Female
Carrier Female
Affected Male
Husband Mother
MELBOURNE IVF
MOTHER
AFFECTED MALE
RESULTS OF PCR ANALYSIS FOR HAEMOPHILIA A
MELBOURNE IVF
MONOGENIC PGD AT MELBOURNE IVF
Tests developed to date:Cystic fibrosis β-thalassaemiaα-thalassaemiaDuchennes muscular dystrophyα-1-antitrypsin deficiencyKennedys disease Fragile–X Motor neurone disease (exclusion)Huntington’s disease (direct)Huntington’s disease (exclusion)Neurofibromatosis 1Hirschprung’s diseaseX-linked hydrocephalusMyotonic dystrophyChronic granulomatous diseaseNiemann-Pick type COpitz syndromeRapp-Hodgkin ectodermal dysplasia
Multiple cases for many of these
Tests being developed:Congenital adrenal hyperplasiaTuberous sclerosisMultiple exostosis
Waiting:BRCA2Waardenburg syndromeNeurofibromatosis 2AR polycystic kidney diseaseTreacher-Collins syndromeMenkes diseaseFamilial adenomatous polyposisRetinoblastomaWHIM syndromeHaemophilia A
MELBOURNE IVF
Cystic fibrosisTay Sachs diseaseβ-thalassaemiaSickle cell anaemiaRh blood typingSpinal muscular atrophyAdrenogenital syndromeCongenital adrenal hyperplasiaPlakophilin-1 (PKP1)MCADCDG1C Epidermolysis bullosaGaucher’s disease Hyperinsulinemic hypoglycemia PHH1Fanconis anemiaHLA matchingFragile XMyotonic dystrophyHuntingtonsWiscott-Aldrich syndromeIncontinentia pigmentiOrnithine transcarbamylase def.Myotubular myopathyHunter syndromeFabry diseaseChoroideraemiaKallman syndromeCoffin-Lowy syndromeBarth syndromeHypospadiasGolabi-Rosen syndrome
Marfans syndromeCharcot-Marie-Tooth disease (type 1A)Amyloid polyneuropathyCrouzons syndromeNF2Osteogenesis imperfecta I and IVStickler syndromeTuberous sclerosis Central core disease Familial adenomatous polyposis coliLi Fraumeni syndromeLesch Nyhan syndromeDuchenne muscular dystrophyBecker muscular dystrophyHaemophilia ACharcot-Marie-Tooth disease Retinitis pigmentosaOrnithine Transcarbamylase DeficiencyAgammaglobulinemiaAlport syndrome Hunter’s syndrome MPSII Oro-facial-digital syndrome type 1AdrenoleukodystrophyChronic granulomatous diseaseMenkes diseaseLowe syndromeEctodermal dysplasiaEpilepsyBRCA1AtaxiaRenal agenesisNorrie disease
Conditions that have been diagnosed by PGD – worldwide
MELBOURNE IVF
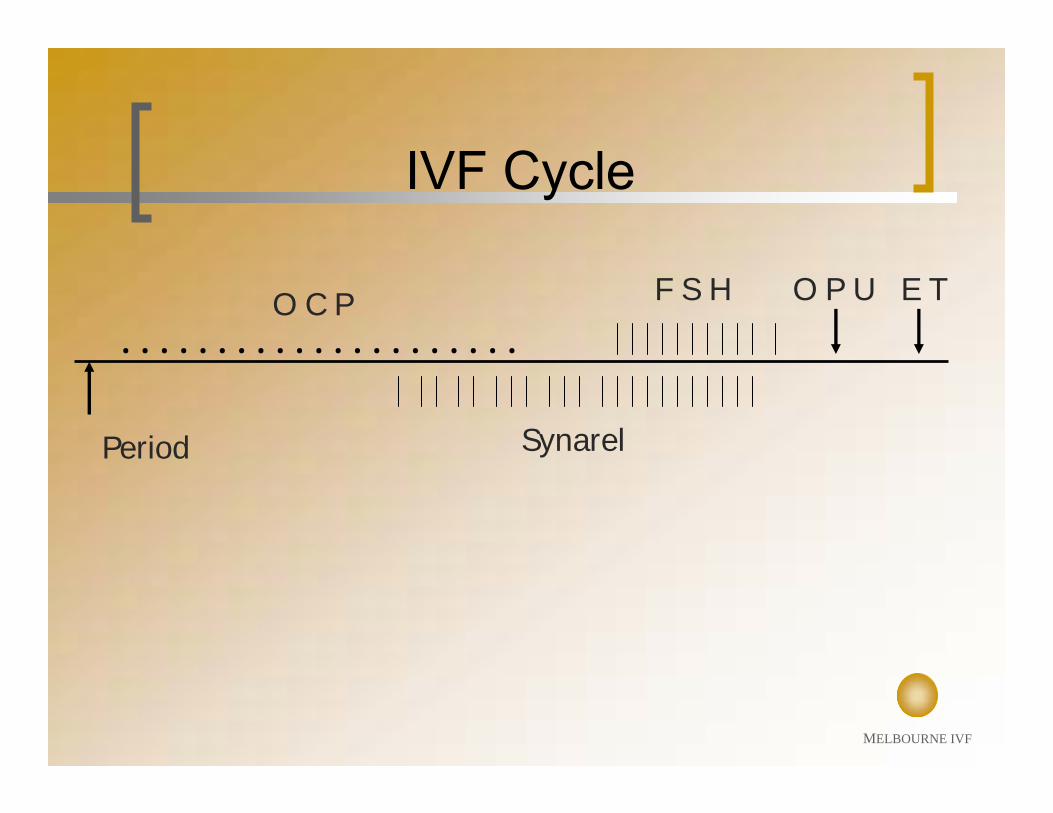
IVF Cycle
Pituitary down – regulation with OCP & GNRH agonist (gonadotrophin –releasing hormone)Ovarian stimulation with r FSH (follicle stimulating hormone)hCG triggerVaginal ultrasound – assisted OPU (ovum pick up)Embryo transfer (ET) 2 or 3 days after OPU
Monitor follicular maturation with vaginal ultrasoundAim for cohort of “leading follicles” of 18-20mm diameterAverage egg No./OPU = 11Fertilisation ~60%
MELBOURNE IVF
. . . . . . . . . . . . . . . . . . . . .
Period Synarel
O C P F S H O P U E T
IVF Cycle



MELBOURNE IVF
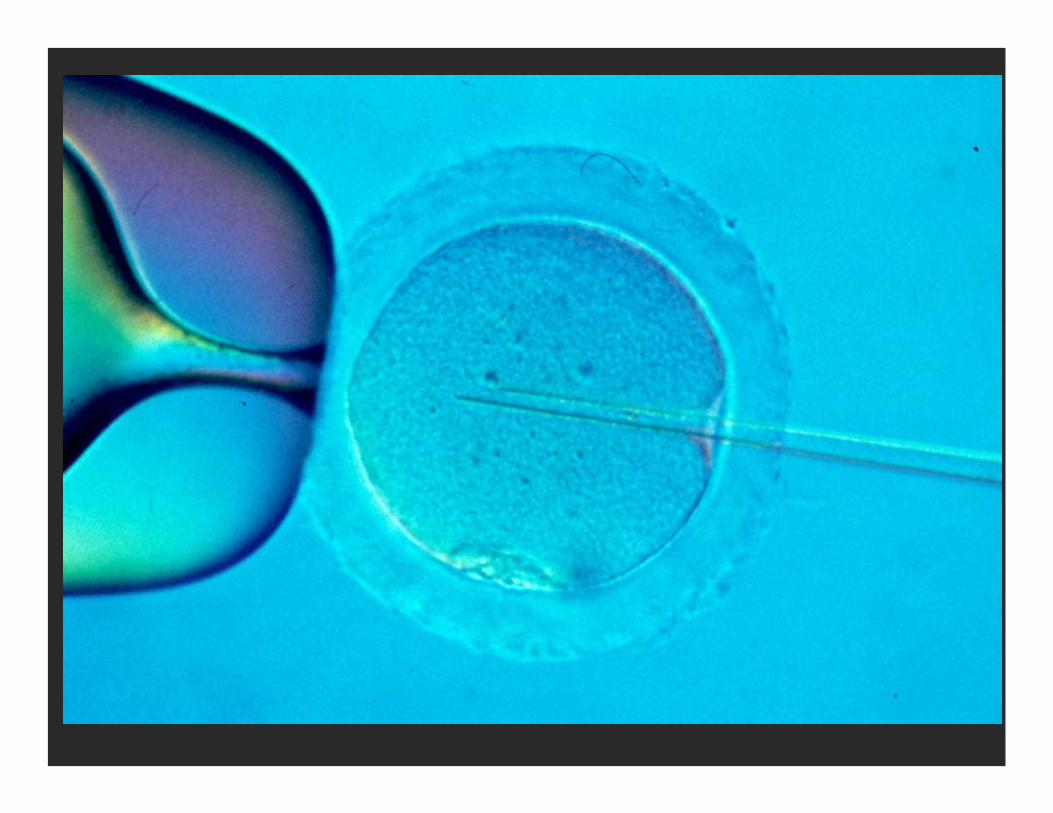
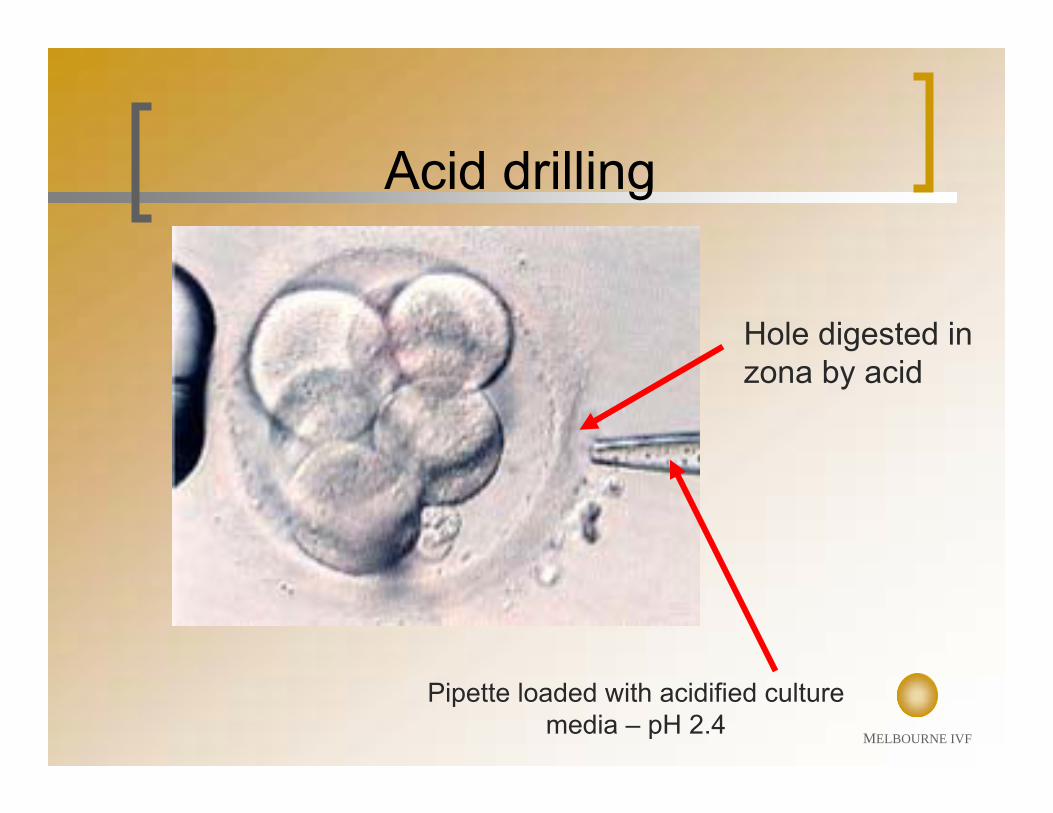
Pipette loaded with acidified culture media – pH 2.4
Hole digested in zona by acid
Acid drilling
MELBOURNE IVF
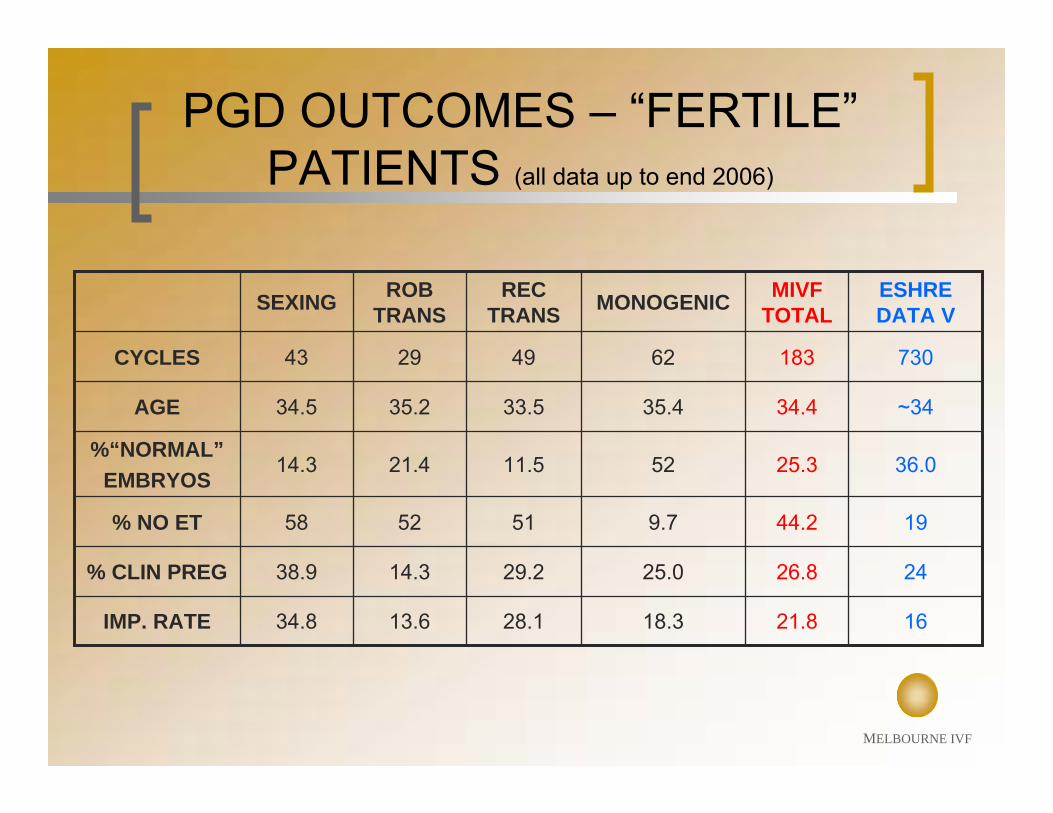
PGD OUTCOMES – “FERTILE”PATIENTS (all data up to end 2006)
13.6
14.3
52
21.4
35.2
29
ROB TRANS
1621.818.328.134.8IMP. RATE
2426.825.029.238.9% CLIN PREG
1944.29.75158% NO ET
36.025.35211.514.3%“NORMAL”
EMBRYOS
~3434.435.433.534.5AGE
730183624943CYCLES
ESHRE DATA V
MIVF TOTALMONOGENICREC
TRANSSEXING
MELBOURNE IVF
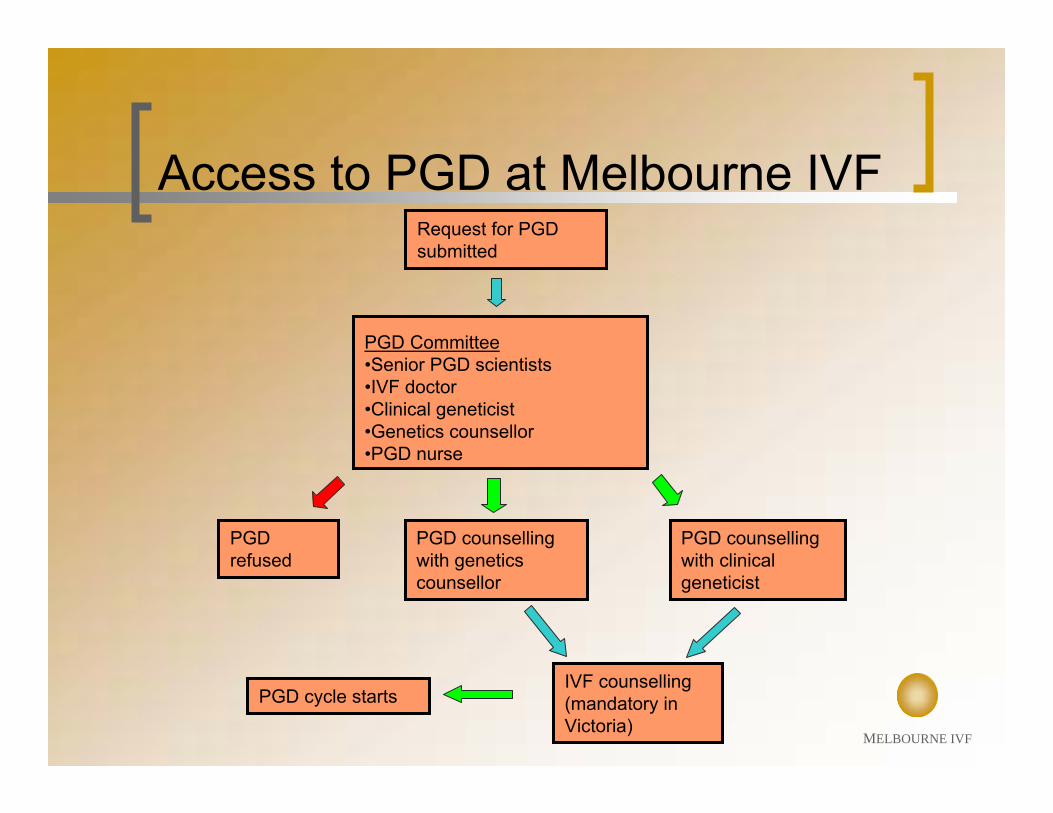
Request for PGD submitted
PGD Committee•Senior PGD scientists•IVF doctor•Clinical geneticist•Genetics counsellor•PGD nurse
PGD refused
PGD counselling with genetics counsellor
PGD counselling with clinical geneticist
IVF counselling (mandatory in Victoria)
PGD cycle starts
Access to PGD at Melbourne IVF
MELBOURNE IVF
Although the degree of accuracy of these tests is high, all tests have a failure rate, and the test results could be wrong.
A full genetic analysis is not being carried out and there are many other genetic conditions that are not being analysed or tested for.
Finding a normal cell using FISH testing does not mean that a baby resulting from the embryo will have the normal number of chromosomes or be of the expected sex.
In single gene defect testing, we cannot guarantee that the embryo will not have the disorder being tested for.
Consent to PGD
MELBOURNE IVF
Consent to PGDIt is strongly recommended that all women with PGD pregnancy consider DNA testing in early pregnancy ( CVS or amniocentesis ) to confirm the early embryo diagnosis.
Spontaneous conception may occur during a PDG cycle, and all couples having PGD should avoid any form of unprotected sex during the treatment cycle.
Rarely, some embryos may be destroyed during the biopsy procedure.
Rarely, it may not be possible to obtain a result on an embryo.
Embryos that are very poor quality will not be subjected to embryo biopsy and will be discarded.
MELBOURNE IVF
PGD - BENEFITSRELIABLE97% embryos diagnosed
ACCURATEmisdiagnosis rate ~ 2%
RAPIDembryo biopsy and diagnostic testing completed 8 –
30 hours
TREATMENT OPTIONalternative to antenatal testing and TOP
MELBOURNE IVF
PGD – PITFALLS
InvasiveHighly medicalised, requires IVFExpensiveSpecific feasibility testing can take monthsNo guarantee of pregnancy
MELBOURNE IVF
HIV AND ASSISTED REPRODUCTIVE TECHNOLOGY
Chronic Viral Illness Clinic at Royal Women’s Hospital Melbourne established 2002principle of harm minimisation (reduced risk of HIV transmission to partner and baby)Use of assisted reproductive technology (intra-uterine insemination or IVF/ICSI)
MELBOURNE IVF
HIV +ve MALE
Good healthUndetectable viral load for 2 monthsSemen screening for HIV
2 successive samples <50 copies=semen storage for IUI /IVF (all
semen samples tested for HIV RNA and DNA)risk of transmission to partner <1/2000
MELBOURNE IVF
CVI PROGRAMME RWH
33 referrals27 male HIV+ve4 female HIV+ve1 couple both HIV+ve
20 patients treated16 male HIV+ve - 12 pregnancies(7 delivered, inc 2 sets twins, 2 ongoing)3 female HIV+ve - 1 ongoing pregnancy
MELBOURNE IVF
ACKNOWLEDGEMENTSMIVF PGD TEAM
Leeanda WiltonSharyn Stock-MyerPam MatthewsMirjana MarticGreta GilliesKay OkeKate Pope
John McBainPenelope FosterMac GardnerDavid AmorStacey RoePeter ColemanRiddhi Marfatia
MELBOURNE IVF
ACKNOWLEDGEMENTSRWH CVI COMMITTEE
Janell ArcherGordon BakerHarold BourneKate CherryGary ClarkeSuzanne CrowePenelope FosterSuzanne Garland
Rachael Knight Hayley MaticAnne MijchSam PernaSepehr TabriziLoreto ValentVicky GreengrassMichelle Giles


















