
Therapeutic targets of Alzheimer
29
Presented by Bondre Rameshwar B. M.Pharm (S.R.T.M.U) (Pharmacology), Nanded 1
-
Upload
rameshwar-bondre -
Category
Education
-
view
82 -
download
0
Transcript of Therapeutic targets of Alzheimer

Presented by
Bondre Rameshwar B.
M.Pharm (S.R.T.M.U)
(Pharmacology),Nanded1

Introduction
Risk factor for AD
symptoms of AD
Pathogenesis of AD
Therapeutic targets of AD
Treatment of AD
Conclusion
References
2

Alzheimer’s Disease (AD) is an irreversible, progressive brain disease
that slowly destroys memory, cognition, and abilities to function
In most cases, symptoms appear after Age 60
Alzheimer’s Disease is named after Dr. Alois Alzheimer.
In 1906, he noticed changes in the brain tissue of a woman who had died
of an unusual mental illness with symptoms of memory loss, language
problems, and unpredictable behavior.
He examined her brain and found many abnormal clumps and tangled
bundles of fibers (neurofibrillary tangles)..
3

Risk Factors for AD:
1. advancing age
2. family history
3. head trauma
4. lack of mental stimulation = “use it or lose it”
5. Down’s syndrome
6. environmental toxins: aluminum, mercury
7. oxidative stress due to accumulation of free radicals
and/or low antioxidant levels
8. abnormal protein processing
9. neurotransmitter deficit
10. genetic polymorphism
4

Repetitive questions or conversations.
Misplacing personal belongings.
Getting lost on a familiar route.
Poor understanding of safety risks.
Poor decision-making ability.
Inability to plan complex or sequential activities.
Speech, spelling, and writing errors.
Early: mild forgetfulness and short-term memory loss
Middle: problems speaking, understanding, reading, or writing
anxiety and aggression
Late: need complete care
complete memory loss, including inability to remember family
5

6

Alzheimer’s Disease
Neurofibrillary Tangles
Cortical Atrophy
Β-Amyloid Plaques
Diseased Neuron
Non-Diseased Neuron
8

Pathogenesis of AD
“The physiology of AD is “characterized by marked atrophy of the
cerebral cortex and loss of cortical and sub-cortical neurons.”
Amyloid Plaques in the spaces between the brain’s nerve cells.
“The senile plaques are extra cellular proteinaceous deposits of
amyloid-beta (Abeta) peptides.”
amyloid + dead brain cell = amyloid plaque
Neurofibrillary Tangles in the brain’s nerve cells.
“Neurofibrillary tangles consist of paired helical filaments which
are composed of hyperphosphorylated microtubule associated
protein tau.”
tau + dead brain cell = neurofibrillary tangle

1. Abnormalities in APP mutation leads
to its cleavage by β- and γ-secretase
enzymes
3. Deposits as Amyloid Plaques and
impairs synaptic function
2. Neurotoxic Aβ42 peptides released and
aggregate into Oligomers and Amyloid Fibrils
APP: Amyloid Precursor Protein
Aβ42: Toxic Aβ fragments
TARGETS
MK-8931
Solanezumab
12

The toxicity of oligomers and amyloid fibrils cause Tau-Hyperphosphorylation leading to
Neurofibrillary Tangles and eventually Neuronal Death.
Apoliopoprotein E gene ε4 allele has
been shown to be a genetic risk
Targets
Aβ pathology begins years before the
onset of Alzheimer’s
13

Neurofibrillary tangles
are due to the accumulation of Tau in the brain.
Tau is a microtubule-associated protein.
14

Acetylcholine (Ach) is a CNS messenger
important for learning and memory
Targets:
Ach is degraded by acetylcholinesterase
(AchE)
In AD, Ach level is low due to excessive
degradation by AchE.
Cholinesterase Inhibitors correct the
deficit of Ach by blocking the action of
AchE and thereby increasing the amount
of Ach that remains in the synaptic cleft.
Cholinesterase Inhibitor
1.
1.
2.
2.
3.
3.
Ach: Acetylcholine
AchE: Acetylcholinesterase
ChEIs: Cholinesterase Inhibitors
As disease progress, the brain gradually
produces less acetylcholine and ChEIs
may lost their effect.
4.
9

1. Glutamate is an excitatory
neurotransmitter involved in cognition
and higher mental function.
2. In AD, abnormalities in NMDA
receptors and excess glutamate in the
synapse due to failure of reuptake
3. Excess glutamate causes release of
excess excitatory ions leading to
excitotoxicity and neuronal death.
4. NMDA Antagonists modulates the
NMDA receptor during the excessive
glutamate stimulation
NMDA: N-Methyl D-Aspartate
NMDA-R: NMDA Receptors
10

Alzheimer’s Disease
PREVENT TANGLES BY DELAYING PLAQUE FORMATION
About 10-15 years after plaque formation, Neurofibrillary Tangles form and cause Neuronal
Death
TARGETED THERAPIES
Aβ Inhibitors
Immunotherapy
Diabetes Medications
EARLY PREVENTION OF DISEASE PROGRESSION
Delaying disease onset by targeting the underlying mechanism
Previous Prevention Treatments without Significant Results
Immunotherapy Bapineuzumab, AN-1792
Aβ Inhibitors Tramiprostate, Latrepirdine, Semagacestat
DM Medications Rosiglitazone
Others Hormone Replacement Therapy, NSAIDs, Gingko Biloba
11

Mechanism of action :
MK-8931 is a potent BACE 1 (β site APP Cleaving Enzyme 1)
Inhibitor
Reduces neurotoxic Aβ peptide production by inhibiting the β-
secretase from cleaving APP
Therefore reducing Amyloid Plaque formation and delaying
Tangle formation, neuronal degeneration and progression of
Alzheimer’s-aaCLI
NICAL DATA
15

Mechanism of Action:
Humanized anti-Aβ peptide immunoglobulin G-1 monoclonal
antibody
Binds with high affinity to the deposited soluble Aβ42 peptides
and mobilizes them
Thereby decreasing amyloid plaque formation and slowing the
progression to Alzheimer’s
Solanezumab
16

1. Glucose enters the brain via Glucose
Transporters (GLUT) at the BBB
2. Brain glucose is converted to ATP energy to
maintain normal neuronal functions such as
cognition and learning.
4. Cerebral energy depletion causing oxidative
stress and inflammation
3. In AD, significant reduction in brain glucose
metabolism and transport
5. Initiates neurodegeneration by amyloid
deposition and abnormal tau phosphorylation
6. Synaptic injury and dysfunction leading to
cognitive impairments
ATP: Adenosine Triphosphate
NFT: Neurofibrillary Tangles
BBB: Blood Brain Barrier
Blood Brain Barrier
17
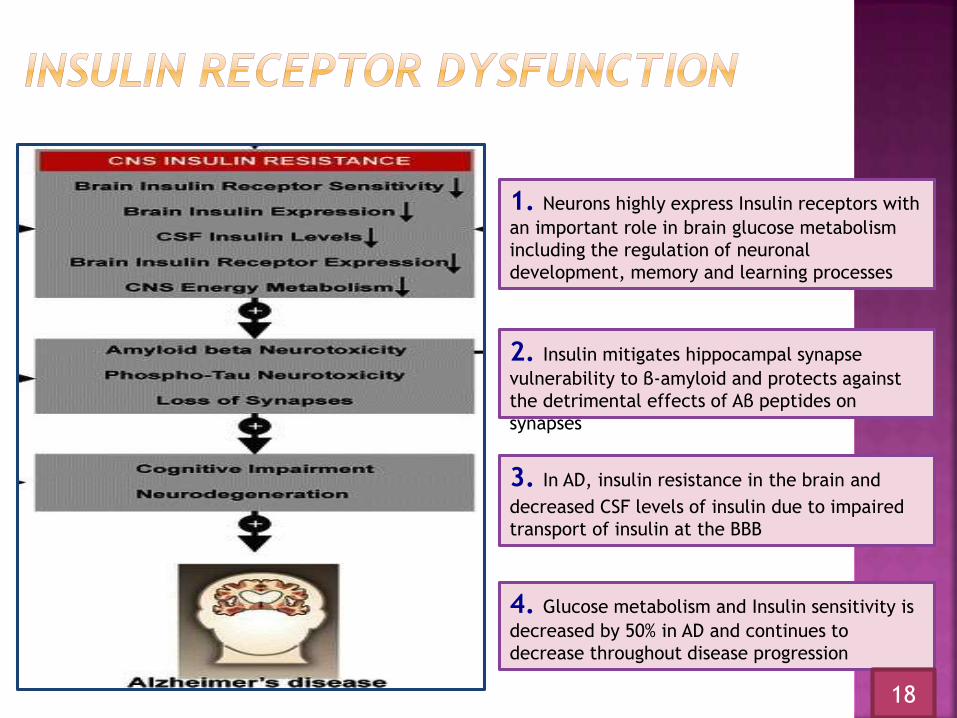
2. Insulin mitigates hippocampal synapse
vulnerability to β-amyloid and protects against
the detrimental effects of Aβ peptides on
synapses
3. In AD, insulin resistance in the brain and
decreased CSF levels of insulin due to impaired
transport of insulin at the BBB
4. Glucose metabolism and Insulin sensitivity is
decreased by 50% in AD and continues to
decrease throughout disease progression
1. Neurons highly express Insulin receptors with
an important role in brain glucose metabolism
including the regulation of neuronal
development, memory and learning processes
18

MECHANISM OF ACTION Potent agonist of PPAR-y (peroxisome proliferator-activated receptor
gamma), which is found in tissues sensitive to insulin action. Crosses the BBB and regulates glucose and lipid metabolism in
neuronal cells and prevents glucose deprivation-induced neuronaldeath.
MECHANISM OF ACTION
Brain insulin receptors are densely localized in the hippocampusand modulates the levels of Aβ and protects against thedetrimental effects of Aβ oligomers on synapses.
Peripheral administration of insulin is not viable due to the risk ofhypoglycemia.
INI provides rapid delivery of insulin to the CNS withoutadversely affecting blood insulin or glucose levels. (Expected toincrease insulin levels in CSF within 60 mins)
19

Normal Brain Alzheimer’s Brain
20
1. Symptomatic Treatments:
- Acetylcholinesterase Inhibitors
- NMDA-receptor Antagonists
- Nicotinic-receptor Agonists
2. Disease-modifying Treatments:
- Inhibition of amyloid formation: beta and gamma-secretase inhibitors
- Inhibition of abeta aggregation
- Tau phosphorylation inhibitors
3. Other Therapies:
- Cholesterol-lowering therapies
- Anti-inflammatory therapies
- Therapies involving antioxidants: vitamin E and gingko biloba
- Therapies involving neurotrophic factors: nerve growth factor (NGF) and estrogen
4. The “Do-It-Yourself” Approach:
- Diet control
- Use of exercise
- Stress control
- Herbal remedies
- Use it or Lose it!
5. Psychotic Treatments:
- Antidepressants [depression]
- Anxiolytics [anxiety]
- Antipsychotics [severe confusion, paranoia, and hallucinations]
22
1. Symptomatic Treatments:
Treatment of mild to moderate dementia of the Alzheimer's type
- Acetylcholinesterase Inhibitors
- tacrine [Cognex®]
- donepezil [Aricept®]
- rivastigmine [Exelon®]
- galantamine [Razadyne®, formerly Reminyl®]
- NMDA-receptor Antagonists
- memantine [Namenda®]
- Nicotinic-receptor Agonists
23

2. Disease-modifying Treatments:
Treatment of moderate to severe dementia of the Alzheimer's type
- Inhibition of amyloid formation
1. gamma-secretase inhibitors
-Semagacestat,avagacestat(ongoing)
2.Beta-secretase inhibitors
-GRL-834,TAK-070
- Inhibition of abeta aggregation
1.solanezumab 2.ponezumab,Curcumin(ongoing)
- Tau phosphorylation inhibitors
1.Methylene blue,NAP,
2.Lithium salts,valproate
24

3. Other Therapies:
- Cholesterol-lowering therapies
- Anti-inflammatory therapies
- aspirin
- ibuprofen
- COX-2 inhibitors: Celebrex
- naproxen sodium
- Rx drugs used for arthritis
- Therapies involving antioxidants
- vitamin E
- gingko biloba
- Therapies involving neurotrophic factors
- nerve growth factor (NGF)
- estrogen25

5. Psychotic Treatments:
- Antidepressants [depression]
- bupropion [Wellbutrin]
- desipramine [Norpramin or Pertofrane]
- fluvoxamine [Luvox]
- Anxiolytics [anxiety]
- Antipsychotics [severe confusion, paranoia, hallucinations]
- carbamazepine [Tegretol]- olanzapine [Zyprexa]
- divalproex [Depakote] - risperidone [Risperdal]
- Haloperidol [Haldol]
26
28

The pathogenesis of AD is a complex process
involving both genetic and environmental factors;
therefore development of effective disease-modifying
drugs is proving to be a difficult task. Current therapies
for patients with AD may ease symptoms by providing
temporary improvement and reducing the rate of
cognitive decline. The concurrent treatment & drug
agent for AD are under research.
27

1. Alzheimer’s Disease. Alzheimer’s Disease Education & Referral Center. National Institute on Aging. National
Institutes of Health. NIH Publication. 11-6423.
2. Alzheimer’s Disease Medications. Alzheimer’s Disease Education & Referral Center. National Institute on
Aging. National Institutes of Health. NIH Publication. 08-3431
3. Tomohiro C. Emerging Therapeutic Strategies in Alzheimer’s Disease. InTech.
4. Christensen D. Alzheimer‘s Disease: Progress in the Development of Anti-amyloid Disease-Modifying
Therapies
5. Francis P, Parsons C, Jones R. Rationale for Combining Glutamatergic and Cholinergic Approaches in the
Symptomatic Treatment of Alzheimer’s Disease. Neurotherapeutics. 2012;12(11):1351-1365
6. Alzheimer’s Disease Trials. ClinicalTrials.gov
7. Kaushik S, DeSilva S, Abbruscato T. The Role of Glucose Transporters in Brain Disease: Diabetes and
Alzheimer’s Disease. International Journal of Molecular Sciences. 2012;13(10):12629-12655
8. Craft S, Baker L, Montine T, et al. Intranasal Insulin Therapy for Alzheimer Disease and Amnestic Mild
Cognitive Impairment. JAMA Neurology. 2012;69(1):29-38
9. Ivan Aprahamian*, Florindo Stella*+ & Orestes V. Forlenza*. New treatment strategies for Alzheimer’s disease .
Indian J Med Res 138 October 2013, pp 449-460
28
Alzheimer’s Disease
THANK YOU!
29


















