
The Role of Health and Health Promotion in Labour Force - RePub
153
The Role of Health and Health Promotion in Labour Force Participation Merel Schuring
Transcript of The Role of Health and Health Promotion in Labour Force - RePub

The Role of Health and Health Promotion
in Labour Force Participation
MerelSchuring

The printing of this thesis was financially supported by the Department of Public
Health,ErasmusMC,UniversityMedicalCentreRotterdam.
Schuring,M
TheRoleofHealthandHealthPromotioninLabourForceParticipation.ThesisEras-
musMC,UniversityMedicalCentreRotterdam
ISBN:978-90-8559-094-1
Lay-outandPrint:OptimaGrafischeCommunicatie
Cover-photograph:©GuidoBenschop
©2010,M.Schuring
All rights reserved. No part of this book may be reproduced or transmitted in any
formorbyanymeanswithoutwrittenpermissionofthecopyrightowner.Someofthe
chaptersarebasedonpublishedmanuscripts,whichwerereproducedwithpermis-
sionofthepublishersandco-authors.

The Role of Health and Health Promotion in Labour Force Participation
De rol van gezondheid en gezondheidsbevordering in arbeidsparticipatie
Proefschrift
terverkrijgingvandegraaddoctoraande
ErasmusUniversiteitRotterdam
opgezagvanderectormagnificus
Prof.dr.H.G.Schmidt
envolgensbesluitvanhetCollegevanPromoties.
Deopenbareverdedigingzalplaatsvindenop
donderdag14oktoberom11:30uur
door
Merel Schuring
GeborenteAlphenaandenRijn

PRomoTiecommissie
Promotoren: Prof.dr.J.P.Mackenbach
Prof.dr.ir.A.Burdorf
Overigeleden: Prof.dr.M.C.H.Donker
Prof.dr.W.R.F.Notten
Prof.dr.J.L.Severens

contents
1. GeneralIntroduction 7
2. Ethnicdifferencesinunemploymentandillhealth 19
International Archives of Occupational and Environmental Health
2009, 82:1023-30
3. TheimpactofillhealthonexitfrompaidemploymentinEurope
amongolderworkers
33
Occupational and Environmental Medicine, in press
4. Theeffectsofillhealthonenteringandmaintainingpaid
employment:evidenceinEuropeancountries
53
Journal of Epidemiology and Community Health 2007, 61:597-604
5. Theeffectofre-employmentonperceivedhealth 71
Journal of Epidemiology and Community Health, in press
6. Effectivenessofahealthpromotionprogrammeforlong-term
unemployedsubjectswithhealthproblems:arandomised
controlledtrial
87
Journal of Epidemiology and Community Health 2009, 63:893-899
7. Changesinphysicalhealthamongparticipantsina
multidisciplinaryhealthprogrammeforlong-termunemployed
persons
BMC Public Health 2009, 9:197
105
8. GeneralDiscussion 125
Summary 139
Samenvatting 143
Dankwoord 147
CurriculumVitae 148
Listofpublications 151
PhDPortfolio 153


1General introduction


Ch
apte
r1
Generalintroduction 9
1.1 inequaLiTies in HeaLTH
Duringthelastcentury,thecombinedeffectsofimprovementsinlivingandworking
conditionsandadvancesinmedicineandhealthcarehaveledtoaconsistentlyincreas-
inglifeexpectancyintheEuropeanUnion.[1]In2007intheEU,thelifeexpectancyofa
newbornboyatbirthwas76.1yearsandofanewborngirl82.2years.Lifeexpectancy
is,however,notequallydistributedinsociety.Personswithalowerlevelofeducation,
aloweroccupationalclass,oralowerlevelofincometendtodieatyoungerage,and
tohave,withintheirshorterlives,ahigherprevalenceofallkindsofhealthproblems.
Thisleadstotremendousdifferencesbetweensocioeconomicgroupsinthenumberof
yearsthatpersonscanexpecttoliveingoodhealth.InEurope,differencesinhealthy
lifeexpectancytypicallyamountto10yearsormore,countedfrombirth[2]According
tomany,suchdifferences inhealthareunacceptable,andrepresentoneofEurope’s
greatestchallengesforpublichealth.
Unemployed persons are a specific socioeconomically disadvantaged group. The
relationship between unemployment and poor health has been well established,
as demonstrated by a higher prevalence of illness and disability [3-4] and a higher
mortalityamongunemployedpersons.[5-6]Selectionandcausationmaycontributeto
theseinequalitiesinhealthamongemployedandunemployedpersons.Selectionmay
actthroughtwodifferentpathways:workerswithapoorhealthmaybemorelikelyto
leavethelabourforce,andunemployedpersonswithapoorhealthmaybelesslikely
to enter the workforce. Causation may also act in two different ways. Leaving the
workforcemayhaveanegativeinfluenceonhealthoftheex-workers.Theotherway
around,gainingpaidemploymentmayhaveapositiveinfluenceonhealth.
Paragraph1.2(HealthandWork)givesanoverviewofthecurrentstateofknowledge
concerningtheinfluenceofhealthonenteringorleavingtheworkforce.Paragraph1.3
(Work and Health) is focused on the effect of gaining paid employment on health.
Paragraph 1.4 (Health promotion among the unemployed) describes the current
evidenceontheeffectivenessofhealthpromotioninterventionsamongunemployed
personsforre-employment.
1.2 HeaLTH anD WoRk
Thereisampleevidencefortheselectionhypothesis.[7-11]Acommunitybasedsurvey
intheUnitedKingdomfoundevidenceforhealthrelatedjobloss,especiallyinrela-
tiontomusculoskeletaldisordersandmentalillness.[8]InaBritishhouseholdpanel
survey healthier persons were more likely to gain employment than persons with
minorpsychiatricmorbidity.[10]

10 Chapter1
In many industrialized countries the population is ageing, due to increasing life
expectancy and falling birth rates.[12] A rather paradoxical development is that,
despiteincreasesinlifeexpectancy,theaveragetimepersonsspendinpaidworkhas
decreased or been stable in most European countries. This paradox is explained by
prolongededucationamongyoungercohorts,and-evenamoreimportantcontribu-
tor-higherratesofexitfromthelabourmarketatolderages.[13]Asaconsequence,
manycountriesaredevelopingpoliciestoencourageolderworkerstoremainlonger
inthelabourmarketanddelayretirement.[14]In2009,theDutchgovernmentplanned
toincreasethestateretirementagefrom65to67.
Consequencesof illhealth for the likelihoodofbecomingor stayingunemployed
maydependonsocialandlabourmarketpolicieswhichvaryacrossEuropeancoun-
tries.Forexample,strikingdifferencesinaccesstobenefits,suchasearlyretirement
ordisabilitypension,fordisabledpersonshavebeendescribedwithintheEuropean
Union.IntheNetherlandslessthan10%ofdisabledpersonshavetheirmainsource
of incomethroughlabourwhereas inSwedenthisproportionamountstoover50%.
[15]Therearedifferentpathways thatmay leadworkersoutof theworkforce,such
as disability pension, retirement, unemployment or becoming a homemaker. There
maybedifferencesbetweencountrieswithrespecttothepathwaypersonswithhealth
problemstakeoutoftheworkforce.Healthproblemsaresurelyapredictorforexitout
ofthelabourforceintodisabilitypension.Evidencefortheinfluenceofhealthonexit
outofthelabourforceintoretirement,unemploymentortakingcareofthehousehold
islessclear.
Thereis littleevidenceaboutthetime-dynamicsofhealthrelatedselectionintoor
outofthelabourforce.Itmaytakesometimebeforehealthcomplaintsmayresultin
lossofpaidemployment.Similarly,improvementsinthehealthstatusofunemployed
personsmayneedsometimetoinfluencethelikelihoodofbecomingre-employed.
The associations between health and employment may not be similar across all
socio-economicgroups.Personalcharacteristics,suchasage,education,ethnicback-
groundand sex, andhousehold characteristics, suchasmarital statusorhousehold
income,willinfluencethesocialcontextofhealthandemploymentstatusand,thus,
influencetheassociationsbetweenhealthandemployment.[9]
1.3 WoRk anD HeaLTH
Thereisalsoevidenceforthecausationhypothesis.Joblossmayleadtoimpairedrole
andemotionalfunctioning,poorhealth,depression,andlowselfesteem.[16-17]Ina
recentstudyamongBritishhouseholdswith11yearfollow-upunemploymenthada
strongeffectontheincidenceofanylimitingillnessandre-employmentwasrelated

Ch
apte
r1
Generalintroduction 11
to recovery from these illnesses.[3] A review of 16 longitudinal studies concerning
mentalhealtheffectsofunemploymentconcluded that lossofemploymentaffected
mentalhealth,butalsothatgainingemploymentimprovedmentalhealth.[18]ABrit-
ishlongitudinalstudyfoundthattransitionsfrompaidemploymenttovariousforms
of non-employment (unemployment, long-term sick leave, maternity leave) had a
negative impact on mental health. Transitions from non-employment to formal em-
ploymentresultedinanimprovementofmentalhealth.[10]Thiswasalsofoundina
five-yearfollowupstudyamonglong-termunemployedNorwegianswhichreported
recoveryofmentalhealthwithinsixmonthsafterre-employment.[19]
In a review Waddel and Burton[20] concluded that re-employment leads to clear
benefits inpsychologicalhealthandsomemeasuresofwell-being,althoughthere is
adearthofinformationonphysicalhealth.Astudyonthepsychologicalandphysi-
cal well-being during unemployment also demonstrated that the bulk of research
is focused on mental health outcomes, suggesting that other aspects of health need
moreattention.[21]Researchisneededtoinvestigatewhetherre-employmentalsohas
beneficialeffectsonphysicalhealth,andifthisistrue,whetherre-employmenthasan
immediateeffectonphysicalhealth.
1.4 HeaLTH PRomoTion amonG THe unemPLoyeD
Apoorhealthwillactasabarriertoreturntopaidemployment.[16-17,22]Inorderto
increasethepossibilitiesforre-employment,improvementsinhealthofunemployed
personsmay,therefore,beanimportantstep.
Unemployed persons with chronic health complaints, such as musculoskeletal
disorders,maybecomeprogressivelylesshealthy,sincefearofpainandreinjurymay
leadtoreducedactivities[23],resultinginapassivelifestylewithlowlevelsofphysi-
calactivity.[7,24]Hence,exercisestoimprovephysicalactivitymaybebeneficial,not
only for those subjects with disorders of the locomotive system, but also for other
chronicdiseasesaswell,includingheartandpulmonarydiseasesanddepression.[25]
InareviewPedersenandSaltin[25]concludedthatexercisetherapyhaspositiveef-
fectsongeneralwell-being,physicalhealthanddepressivesymptomsofpersonswith
chronicdiseases.
Cognitive-behaviouraltherapymaybeneededtotargetspecificpain-relatedbeliefs
andcopingstrategiesformodification.[26]RoseandHarris[27]haveidentifiedcogni-
tive behavioural therapy as a promising intervention to improve the psychological
healthofpersonswhoareunemployed.Watsonandcolleagues [28]providedsome
indications that an occupationally oriented rehabilitation programme consisting
of physical exercise and cognitive behavioural training for long-term unemployed

12 Chapter1
persons with chronic low back pain improved physical fitness as well as increased
employmentamongunemployedparticipantswithhealthcomplaints.However,these
resultswerebasedonanobservationalstudy.
Thereisaneedforarandomisedcontrolledtrialtoinvestigatetheeffectsofacom-
bined physical exercise and cognitive behavioural programme among unemployed
persons with a poor health. In addition, factors that determine non-participation,
drop-out and non-compliance in a health promotion programme for unemployed
personsneedtobeaddressed.
1.5 objecTives
Theobjectivesofthisthesisarethreefold:
1. To study the influence of poor health on entering and maintaining paid employment
2. To study the influence of entering paid employment on different dimensions of perceived
health.
3. To evaluate the effectiveness of a health promotion programme among unemployed persons
with health complaints on physical and mental health and re-employment
1.6 DaTaseTs useD in THis THesis
The analyses of this thesis were based on four different datasets. Two large Euro-
peanlongitudinaldatasets(SHARE;ECHP)wereusedforsecondarydata-analyses.A
longitudinalstudywasconductedtoinvestigatetheassociationbetweenhealthand
re-employmentamongunemployedcitizensofthecityofRotterdam.Arandomised
controlled trial was conducted to evaluate the effectiveness of a health promotion
programmeforunemployedpersonswithhealthcomplaintsinthecityofRotterdam.
1.6.1SurveyonHealthandAgeinginEurope(SHAREstudy)
Inchapter3theeffectofillhealthonexitfromthelabourforceamongolderworkers
inEuropeisinvestigatedontwowaves(2004,2006)oftheSurveyonHealthandAge-
inginEurope(SHAREstudy).TheSHAREstudyisalongitudinalsurveythataimsto
collectmedical,social,andeconomicdataonthepopulationagedover50yearsin11
EuropeanUnioncountries(Sweden,Denmark,TheNetherlands,Belgium,Germany,
Austria,Switzerland,France,Italy,Spain,andGreece).[11,12]Thefirstwaveofdata
wascollectedbyinterviewsbetweenAprilandOctober2004.Theoverallhousehold

Ch
apte
r1
Generalintroduction 13
responseacrossthe11SHAREcountriesinwhichdatacollectiontookplacein2004was
approximately62%,althoughsubstantialdifferencesamongcountrieswereobserved.
[12]Theavailabledatasetfromthefirstwaveofdatacollection(SHARERelease2.0)
contains28,517participants,with12,965subjects(45%)agedbetween50and63years.
Aftertwoyears8,729subjectsparticipatedagaininthequestionnairesurvey(SHARE
Release 1.0), resulting in a response of 67%. Complete information on employment
status in 2006 was available for 8,568 subjects. For the longitudinal analysis of the
influence of ill health on exit of the labour market, a cohort was available of 4,611
subjectswithpaidemploymentin2004andcompleteinformationonindividualand
workrelatedcharacteristicsatbaselineandworkstatusatfollow-upin2006.
1.6.2EuropeanCommunityHouseholdPanel(ECHP)
Inchapter4theeffectofillhealthontransitionsbetweenpaidemploymentandvarious
formsofnon-employment,includingretirement,unemployment,andhomemaker,is
investigatedinfivewaves(1994-1998)oftheEuropeanCommunityHouseholdPanel
(ECHP). The ECHP study is a social survey, designed for the member states of the
EuropeanUnion,withauniformdesignthatallowsforadaptationtonationalrequire-
ments. Through its longitudinal design it aims to represent the social dynamics in
Europe,from1994,theyearofthefirstwave,throughouttheperiodthatiscoveredby
thesubsequentwaves.ThedatawerecollectedbyNationalInstitutesforStatisticsor
researchcenters,whiledatachecks,weightingsandimputationsweredonecentrally
by the Statistical Office of the European Communities (Eurostat).All surveys were
basedonanon-stratifiedrandomsamplingdesign.Thetargetpopulationwasmade
upofallnationalprivatehouseholds.Allpersonsinthepanelhouseholdwereindi-
viduallyinterviewed.Thedatacollectionwascarriedoutinmostcountriesbypaper-
and-pencil interviewing, but in four countries (United Kingdom, The Netherlands,
Portugal,andGreece)bycomputer-assistedpersonalinterviewing.Theoverallhouse-
hold response in the firstwavewas72%,butvariedconsiderablyamongcountries.
TheresponseinlaterwavesoftheECHPstudywashigher.Adetaileddescriptionof
samplingproceduresandresponserateshasbeenpublishedelsewhere.[16,17]
Forthelongitudinalanalysisoftheinfluenceofillhealthonenteringandmaintain-
ingpaidemployment,twodifferentpopulationsweredefined.Thefirststudypopula-
tionincluded4446personswhowereunemployedforatleasttwoconsecutiveyears
ofwhich1590(36%)personsenteredtheworkforceduringthelastyearoffollow-up.
Thesecondstudypopulationconsistedof57436workerswhowereemployedforat
leasttwoconsecutiveyearsofwhich6191(11%)personslefttheworkforceinthelast
yearoffollow-upduetounemployment(n=3000),retirement(n=2017),ortakingcare
ofthehousehold(n=1174).

14 Chapter1
1.6.3Re-employmentandhealthdataset
Inchapter5theassociationbetweenhealthandre-employmentwasstudiedinalongi-
tudinalstudywith6monthsfollow-upamongunemployedpersonsonsocialsecurity
benefits,whowerereferredtoare-employmenttrainingcentreforare-employment
trainingbytheEmploymentCentreoftheCityofRotterdam,TheNetherlands.Some
oftheparticipantsdidhavechronichealthproblems,butweredeclaredfitenoughto
becapableoffulltimeemploymentafterinvestigationbyaphysician,apsychologist,
andanemploymentspecialist.FromDecember2004untilDecember2007,everyweek
anaverageof19subjectswasenrolledinthestudy.Intotal,2754eligibleparticipants
were included in the study. Information about socio-demographic characteristics,
health related quality of life (measured by the SF-36), and psychological measures
ofparticipantswerecollectedwithpostalquestionnairesandface-to-faceinterviews
indifferent languages(Dutch,Turkish,Arabic(interview)).Atbaselinetheresponse
was 66% (1829/2754) and after a follow-up period of approximately 6 months the
response was 53% (965/1829). Information about start dates of a re-employment
training and start and end dates of social security benefits and reasons for ending
benefits were derived from registries of the Employment Centre of the City of Rot-
terdam. Re-employment was defined as leaving the social security benefit services
forat least threemonthsbecauseof startingwithpaidemployment,verifiedby the
nationalSocialSecurityAgency.
1.6.4.Randomisedcontrolledtrialdataset
Inchapter6theeffectivenessofahealthpromotionprogrammeamongunemployed
persons is investigated in a randomized controlled trial. The study population
consisted of persons on social security benefits in the City of Rotterdam, who did
havechronichealthproblems,butweredeclaredfitenoughtobecapableoffulltime
employmentafter investigationbyaphysician, apsychologist, andanemployment
specialist.FromDecember2004untilDecember2007,eligibleparticipantswereran-
domly assigned to the intervention (n= 465) or control group (n=456). Information
about socio-demographic characteristics, health related quality of life (measured by
theSF-36),psychologicalmeasures,workvalues,andjobsearchactivitiesofpartici-
pantswerecollectedwithpostalquestionnairesandface-to-faceinterviewsindiffer-
entlanguages(Dutch,Turkish,Arabic(interview)).Atbaseline,theresponsewas74%
(343/465) intheinterventiongroupand68%(310/456) inthecontrolgroup.Aftera
follow-upperiodofapproximately6months,theresponsewas51%(176/343)inthe
interventiongroupand48%(150/310) in thecontrolgroup. Informationaboutstart
datesofare-employmenttrainingandstartandenddatesofsocialsecuritybenefits

Ch
apte
r1
Generalintroduction 15
andreasonsforendingbenefitswerederivedfromregistriesoftheEmploymentCen-
treoftheCityofRotterdam.
1.7 ouTLine oF THis THesis
Followingthisgeneral introduction,chapter2willdescribe theassociationbetween
unemployment and health among different socioeconomic groups. Chapter 3 and 4
willaddressthefirstobjectiveofthisthesis,i.e.theinfluenceofpoorhealthonenter-
ingandmaintainingpaidemployment.Chapter5willfocusonthesecondobjective
ofthisthesis,i.e.theinfluenceofenteringpaidemploymentondifferentdimensions
ofperceivedhealth.Chapter6and7willfocusonthethirdobjectiveofthisthesis,i.e.
theeffectivenessofahealthpromotionprogrammeamongunemployedpersonswith
healthcomplaintsonphysicalandmentalhealthandre-employment.
Chapter 2 presents a cross-sectional study on the association between health and
employmentstatusamongdifferentsocio-economicgroupsintheCityofRotterdam,
theNetherlands.Chapter3presentsasecondarydata-analysiswithtwowaves(2004,
2006) of the SHARE study on the effect of ill health on exit from the labour force
amongolderworkers inEurope.Chapter4presentsasecondarydata-analysiswith
fivewaves(1994-1998)oftheEuropeanCommunityHouseholdPanel(ECHP)onthe
effectofillhealthontransitionsbetweenpaidemploymentandvariousformsofnon-
employment, includingretirement,unemploymentandhomemaker.Chapter5pres-
entsaprospectivestudyontheassociationbetweenhealthandre-employmentamong
965unemployedpersonsintheCityofRotterdam.Chapter6presentsarandomised
controlledtrialtoevaluatetheeffectivenessofahealthpromotionprogrammeamong
unemployedpersonswithhealthcomplaintsonphysicalandmentalhealthand re-
employment.Chapter7presentsanobservationalstudytoevaluatechangesinphysi-
calhealthamongparticipantsinahealthpromotionprogramme.Chapter8discusses
the main findings of the previous chapters within the light of the objectives of this
thesis.Methodologicalconsiderationsandrecommendationsforclinicalpracticeand
futureresearcharepresented.

16 Chapter1
ReFeRences
1. Mackenbach JP: Ziekte in Nederland. Gezondheid tussen politiek en biologie.Amsterdam:UitgeverijMouria2010:59-67.
2. MackenbachJP:HealthInequalities:EuropeinProfile.Anindependent,expertreportcom-missionedby,andpublishedundertheauspicesof,theUKPresidencyoftheEU2005.
3. BartleyM,SackerA,ClarkeP:Employmentstatus,employmentconditions,andlimitingillness:prospectiveevidencefromtheBritishhouseholdpanelsurvey1991-2001.Journal of epidemiology and community health 2004,58(6):501-506.
4. JanlertU:Unemploymentasadiseaseanddiseasesoftheunemployed.Scand J Work Environ Health 1997,23Suppl3:79-83.
5. MorrisJK,CookDG,ShaperAG:Lossofemploymentandmortality.BMJ (Clinical research ed 1994,308(6937):1135-1139.
6. Lundin A, Lundberg I, Hallsten L, Ottosson J, Hemmingsson T: Unemployment andmortality--alongitudinalprospectivestudyonselectionandcausationin49321Swedishmiddle-agedmen.Journal of epidemiology and community health 2010,64(1):22-28.
7. ClaussenB,BjorndalA,HjortPF:Healthandre-employmentinatwoyearfollowupoflongtermunemployed.Journal of epidemiology and community health 1993,47(1):14-18.
8. SolomonC,PooleJ,PalmerKT,CoggonD:Health-relatedjobloss:findingsfromacommu-nity-basedsurvey.Occup Environ Med 2007,64(3):144-149.
9. McDonoughP,AmickBC,3rd:Thesocialcontextofhealthselection:alongitudinalstudyofhealthandemployment.Soc Sci Med 2001,53(1):135-145.
10. ThomasC,BenzevalM,StansfeldSA:Employmenttransitionsandmentalhealth:ananalysisfromtheBritishhouseholdpanelsurvey.Journal of epidemiology and community health 2005,59(3):243-249.
11. JusotF,KhlatM,RochereauT,SermeC:Joblossfrompoorhealth,smokingandobesity:anationalprospectivesurvey inFrance. Journal of epidemiology and community health 2008,62(4):332-337.
12. IlmarinenJE:Agingworkers.Occup Environ Med 2001,58(8):546-552. 13. StattinM:Retirementongroundsofillhealth.Occup Environ Med 2005,62(2):135-140. 14. CaiL,KalbG:Healthstatusandlabourforceparticipation:evidencefromAustralia.Health
Econ 2006,15(3):241-261. 15. OECD:Transformingdisabilityintoability.Policiestopromoteworkandincomesecurityfor
disabledpeople.Paris, OECD,2003. 16. PriceRH,ChoiJN,VinokurAD:Linksinthechainofadversityfollowingjobloss:how
financialstrainandlossofpersonalcontrolleadtodepression,impairedfunctioning,andpoorhealth.Journal of occupational health psychology 2002,7(4):302-312.
17. EdenD,AviramA:Self-efficacytrainingtospeedreemployment:Helpingpeopletohelpthemselves.Journal of Applied Psychology 1993,78(3):352-360.
18. MurphyGC,Athanasou,J.A.:Theeffectofunemploymentonmentalhealth.Journal of Oc-cupational and Organizational Psychology 1999,72:83-99.
19. ClaussenB:Healthandre-employmentinafive-yearfollow-upoflong-termunemployed.Scand J Public Health 1999,27(2):94-100.
20. WaddellG,Burton,A.K.:Isworkgoodforyourhealthandwell-being?London: The Stationery Office 2006(www.tsoshop.co.uk):ISBN:9780117036949.

Ch
apte
r1
Generalintroduction 17
21. McKee-RyanF,SongZ,WanbergCR,KinickiAJ:Psychologicalandphysicalwell-beingdur-ingunemployment:ameta-analyticstudy.J Appl Psychol 2005,90(1):53-76.
22. CreedPA:Improvingthementalandphysicalhealthofunemployedpeople:whyandhow?Med J Aust 1998,168(4):177-178.
23. BendixAF,BendixT,OstenfeldS,BushE,Andersen:Activetreatmentprogramsforpatientswithchroniclowbackpain:aprospective,randomized,observer-blindedstudy.Eur Spine J 1995,4(3):148-152.
24. LakkaTA,KauhanenJ,SalonenJT:Conditioningleisuretimephysicalactivityandcardiore-spiratoryfitnessinsociodemographicgroupsofmiddle-agesmenineasternFinland.Int J Epidemiol 1996,25(1):86-93.
25. PedersenBK,SaltinB:Evidenceforprescribingexerciseastherapyinchronicdisease.Scand J Med Sci Sports 2006,16Suppl1:3-63.
26. TurnerJA,JensenMP,RomanoJM:Dobeliefs,coping,andcatastrophizingindependentlypredictfunctioninginpatientswithchronicpain?Pain 2000,85(1-2):115-125.
27. RoseV,HarrisE:Fromefficacytoeffectiveness:casestudiesinunemploymentresearch.J Public Health (Oxf) 2004,26(3):297-302.
28. WatsonPJ,BookerCK,MooresL,MainCJ:Returningthechronicallyunemployedwithlowbackpaintoemployment.Eur J Pain 2004,8(4):359-369.


2ethnic differences in unemployment
and ill health
SchuringM,BurdorfA,KunstAE,VoorhamAJJ,MackenbachJP.
international Archives of Occupational and Environmental Health 2009, 82:1023-30.

20 Chapter2
absTRacT
objective:Theaimofthestudyistoevaluatewhetherhealthinequalitiesassociated
withunemploymentarecomparableacrossdifferentethnicgroups.
method:Arandomsampleof inhabitantsofthecityofRotterdamfilledoutaques-
tionnaire on health and its determinants, with a response of 55.4% (n=2057). In a
cross-sectional design the associations of unemployment, ethnicity, and individual
characteristics with a perceived poor health were investigated with logistic regres-
sionanalysis.Theassociationsofthesedeterminantswithphysicalandmentalhealth,
measuredbytheShortForm36HealthSurvey,wereevaluatedwithlinearregression
analyses. Interactions between ethnicity and unemployment were investigated to
determine whether associations of unemployment and health differed across ethnic
groups.
Results: Ill health was more common among unemployed persons (OR 2.6; 95% CI
1.7-3.8) than workers in paid employment. Health inequalities between employed
and unemployed persons were largest among native Dutch persons (OR=3.2) and
Surinamese/Antilleanpersons(OR=2.6),andsmaller inTurkish/Moroccanpersons
(OR=1.6)andoverseasrefugees(OR=1.6).Theproportionsofpersonswithpoorhealth
thatcouldbeattributedtounemploymentwere14,26,14,and13%,respectively.
conclusions: Differences in ill health between employed and unemployed persons
were less profound in ethnic groups compared to the majority population, but the
prevalence of unemployment was much higher in ethnic groups. The population
attributable fractions varied between 14% and 28%, supporting the argument that
policiesforhealthequityshouldpaymoreattentiontomeasuresthatincludepersons
in the labourmarketandthatpreventworkerswith illhealth fromdroppingoutof
theworkforce.

Ch
apte
r2
Ethnicdifferencesinunemploymentandillhealth 21
inTRoDucTion
Thepresenceofsocioeconomicinequalitiesinhealthhasbeenwidelyacknowledged.
Lower education, unskilled labour, and a low income are associated with higher
mortalityandmorbidity. [1]Labour forceparticipation isan importantdeterminant
ofhealthinequalities,asdemonstratedbyahigherprevalenceof illness.[2]anddis-
ability [3] and a higher mortality among unemployed persons.[4] A poor health is
strongly associated with non-participation in the labour force, both unemployment
anddisability.[5-6]Theassociationbetweenhealthandemploymentisbi-directional:
unemploymentmaycausepoorhealth (causationhypothesis),andpoorhealthmay
increasetheprobabilityofbecomingunemployed(selectionhypothesis).[7-8]
Within many countries, substantial inequalities in health between ethnic groups
exist.[9-10]Theextent towhichsocioeconomic inequalitiesunderlieethnic inequali-
ties in health remains debated. Many researchers argue that ethnic inequalities in
health are predominantly determined by socioeconomic inequalities.[11-12] Others
argue that ethnicity is an independent risk factor for self-reported illness, with an
importanceequaltoriskfactorssuchassocialclass,age,havingapoorsocialnetwork,
nottakingregularexercise,andnotfeelingsecureindailylife.[13]Whenthestrength
oftherelationbetweensocioeconomicstatusandhealthvariesacrossethnicgroups,
this will have consequences for the extent to which socioeconomic inequalities can
underlie ethnic differences in health. A Canadian study found that socioeconomic
factorsweremoreimportanttoself-ratedhealthstatusandpresenceofchronicillness
among immigrants than in non-immigrants [14] There are some indications from a
Germanstudythatunemployedforeignworkerswerelesssatisfiedwiththeirhealth
than unemployed Germans.[15] Schuring et al.[8] observed that in countries with a
lownationalunemploymentrateapoorhealthwasstronglyassociatedwithentering
orretainingpaidemployment,whereasincountrieswithahighnationalunemploy-
ment rate the effect of a poor health on selection in and out of the workforce was
much smaller.A possible explanation is that with high unemployment various fac-
torsdeterminelabouropportunities,suchaseducation,training,andage,andthata
poorhealthonlyplaysaminor role relative to these socio-demographic factors.[16]
Withlowunemploymentpersonsofallageandeducationallevelareretainedinthe
workforce and, thus, the influence of a poor health becomes more prominent. This
reasoningwouldimplythat,withinagivencountry,amongthosegroupswithhigh
unemployment,suchasminoritygroups,socio-demographic factorswillexceedthe
importanceofhealth.Hence,ahighunemploymentrateinminoritygroupsmaymask
theassociationbetweenhealthandemploymentstatusinthesegroups.
Inorder tobetterunderstandtherelationbetweenethnicity,socioeconomicstatus
andhealth,itisimportanttoassesswhethersocioeconomicstatusisassociatedwith

22 Chapter2
healthinasimilarwayacrossethnicgroups.Inthispaperweexaminetheassociations
betweenunemploymentandhealthinthethreelargestethnicminoritygroupsofthe
Netherlandsandtheindigenouspopulation.Theaimsofthestudywere(1)toevaluate
whethertheassociationsbetweenpoorhealthandemploymentstatusarelessstrong
amongethnicgroupswithhighunemployment thanamongDutchpersons,and (2)
toassessthedifferencesinproportionsofunemploymentattributedtopoorhealth.
meTHoDs
Population
BetweenMarchandJune2003ahealthquestionnairesurveywasundertakenbythe
municipalhealthserviceofRotterdaminarandomsampleof6404inhabitantsofthe
cityofRotterdam,aged16to84.[17]Aquestionnairewassendtothehomeaddress,
followedbytworeminderstwoandfourweekslater,respectively.Atotalof3406sub-
jectsreturnedthequestionnaire(response55.4%).Thoserespondentswhowereaged
between16and65yearsoldandnotengagedas student ina secondaryor tertiary
educational programme were selected for the current study with a cross-sectional
design.Atotalof2057subjectsmettheseinclusioncriteria.
Socio-demographicvariables
Thesocio-demographicvariablesincludedinthisstudywerelabourforceparticipa-
tion, ethnic background, highest educational level, age, sex, and marital status. In
this study, labour status was based on self-reported current economic status with
five mutually exclusive categories: full-time employment (>32 h/week), part-time
employment(<32h/week),unemployment,disabilitypension,andhomemaker.
Theethnicbackgroundoftherespondentwasbasedonthecountryoforiginofthe
mother.IncasethemotherwasborninTheNetherlands,thecountryofbirthofthe
fatherwasleading.[18]Differentethnicgroupsweredefined,basedondifferencesin
experiencesofmigration(refugeesorlabourmigrants)anddifferencesingeographi-
cal and cultural distance from the Netherlands. Three ethnic minority groups were
defined: (1) Turks and Moroccans, (2)Antilleans and Surinamese, and (3) refugees.
TurksandMoroccans initiallycameas labourmigrants to theNetherlandsfromthe
early1960s,whilethemigrationofSurinameseandAntilleans/Arubansisrelatedto
thecolonialpast.Refugeesareanotherimportantgroupofmigrantsfromdesignated
countriesAfghanistan,Algeria,Angola,Bosnia,China,Chile,Croatia,DemocraticRe-
publicoftheCongo,Eritrea,HongKong,Iran,Iraq,Kosovo,Liberia,Nigeria,Sedan,

Ch
apte
r2
Ethnicdifferencesinunemploymentandillhealth 23
Serve, Sierra Leone, Somalia, South Korea, Syria, or former-Yugoslavia. Immigrants
fromothercountrieswerenotincludedintheanalysis(n=296).
Subjectsweredivided into threegroupsaccordingto theirhighest levelofeduca-
tionalattainment.Ahigheducationallevelwasdefinedashighervocationaltraining
oruniversity,intermediateeducationallevelwasdefinedashighersecondaryschool-
ing or intermediate vocational training, and low educational level was defined as
noeducation,primaryschool, lowerandintermediatesecondaryschoolingorlower
vocationaltraining.Maritalstatuswasusedtodistinguishthosesubjectsmarriedor
livingtogetherwithothers.
Healthmeasures
Self-reported health (SRH) was measured by asking subjects to rate their overall
healthonafive-pointscale,rangingfrom‘excellent’,verygood’,‘good’and‘fair’to
‘poor’.Thosereportinglessthan‘goodhealth’weredefinedashavingapoorhealth.
[16]Healthwasalsomeasuredwith theDutchversionof theShortForm36Health
Survey(SF-36).[19]TheSF-36consistsof36 itemsthatwereusedtocalculatescores
oneightdimensions:physicalfunctioning,generalhealth,mentalhealth,bodilypain,
socialfunctioning,vitality,rolelimitationduetoemotionalhealthproblems,androle
limitationduetophysicalhealthproblems.Scorescouldrangefrom0to100,witha
higherscoreindicatingabetterhealthrelatedqualityoflife.
Statisticalanalysis
Characteristicsofsubjectswereanalyzedusingdescriptivestatistics.Fortwosubscales
oftheSF-36,rolelimitationsduetophysicalhealthproblemsandrolelimitationsdue
toemotionalhealthproblems,astrongceilingeffectexistedandthevariableswerenot
normallydistributed.Therefore,thesesubscaleswereexcludedfromfurtheranalysis.
The statistical analysis was conducted on the study population with complete
informationonallvariablesincludedinthemultivariateanalyses.Sinceeducational
levelwasnotavailable for207subjects (10%)and forothervariablesa fewmissing
valuesoccurred,thenumberofsubjectsintheanalysesmayvaryslightly.Theassocia-
tionsbetweenunemployment,ethnicityandothersocio-demographiccharacteristics
and perceived poor health were investigated with logistic regression analysis, with
the odds ratio (OR) as measure of association. The analysis started with univariate
logisticregressionmodelstodeterminewhichindependentvariableswereofinterest
toconsiderinthefinalmodel.VariableswithaPvalueofatleast0.10wereselected
for further analysis. A multivariate logistic regression analysis was conducted to
determinetheassociationofemploymentstatus,ethnicbackground,sex,age,educa-

24 Chapter2
tionallevel,andmaritalstatuswiththedichotomousoutcomemeasureofpoorhealth.
Explanatoryvariableswere included into themainmodelonebyonebya forward
selection procedure, in order of magnitude of explained variance in the univariate
analyses,and independentvariableswithaPvalueofat least0.05wereretained in
the model. Interaction effects between ethnicity and unemployment were analyzed
inordertodeterminewhethertheeffectsofunemploymentonhealthdifferedacross
ethnicgroups.Theproportionofpersonswithpoorhealththattheoreticallycouldbe
attributedtounemploymentwascalculatedwiththepopulationattributablefraction,
expressed by the formula PAF% = 100 × [p × (OR-1)] / [1 + p × (OR-1)], whereby
p is the proportion of unemployed persons and the OR is the association between
unemploymentandpoorhealth.[20]
Table 2.1 Characteristicsandperceivedhealthofsubjectswithdifferentethnicbackgroundsinacommunity-basedhealthsurveyintheNetherlands(n=2057)
Dutchn=1448
T/mn=228
s/an=281
Refugeen=100
Women 808(55.9%) 119(52.2%) 170(60.5%) 50(50.0%)
Age*18-24yr25-44yr45-54yr55-65yr
96(6.6%)662(45.7%)347(24.0%)343(23.7%)
34(14.9%)137(60.1%)31(13.6%)26(11.4%)
39(13.9%)145(51.6%)68(24.2%)29(10.3%)
13(13.0%)54(54.0%)19(19.0%)14(14.0%)
Married* 882(61.8%) 168(74.3%) 113(40.8%) 56(57.1%)
Educationallevel*HighIntermediateLow
Missing
394(28.7%)350(25.5%)628(45.8%)76
10(6.3%)42(26.4%)107(67.3%)69
24(10.0%)59(24.7%)156(65.3%)42
18(22.5%)30(37.5%)32(40.0%)20
Employmentstatus*Employed>32h/wkEmployed<32h/wkUnemployedDisabilitypensionHomemaker
812(56.1%)289(20.0%)111(7.7%)111(7.7%)125(8.6%)
83(36.4%)28(12.3%)60(26.3%)14(6.1%)43(18.9%)
139(49.5%)56(19.9%)63(22.4%)13(4.6%)10(3.6%)
51(51.0%)13(13.0%)25(25.0%)3(3.0%)8(8.0%)
Poorhealth* 261(18.1%) 97(42.7%) 88(31.7%) 21(21.0%)
Generalhealth*Physicalfunctioning*Socialfunctioning*Bodilypain*Vitality*Mentalhealth*Rolelimitations,physical*Rolelimitations,emotional*
70.1(19.7)87.4(19.9)81.7(23.2)78.7(24.2)62.6(19.2)73.9(17.6)80.2(34.5)84.7(32.1)
55.7(22.8)69.1(27.0)69.4(24.7)65.1(28.3)50.6(18.0)61.8(18.8)66.3(36.9)69.8(39.6)
63.3(20.6)78.8(25.8)73.7(27.2)72.2(26.6)54.9(18.9)68.3(20.6)77.5(35.0)78.8(37.2)
65.5(19.5)79.2(26.3)75.9(24.6)73.5(24.7)55.0(18.9)66.4(18.0)80.6(31.6)81.4(33.8)
*chi-squaretestP<0.05,comparingminoritygroupstothenativeDutchpopulation

Ch
apte
r2
Ethnicdifferencesinunemploymentandillhealth 25
Theassociationsoflabourstatus,ethnicity,andothersocio-demographiccharacter-
isticswithphysicalandmentalhealthwereinvestigatedwithmultiplelinearregres-
sionanalysis,withasdependentvariablesthescoresonthesixsubscalesoftheSF-36;
general health, physical health, bodily pain, mental health, social functioning, and
vitality.
All statistical analyses were performed with the statistical package SPSS 11.0 for
Windows.
ResuLTs
CharacteristicsofsubjectsarepresentedinTable2.1,stratifiedbyethnicbackground.
Immigrantsubjectswereyoungerofage,moreoftenunemployedand,withtheexcep-
tionofrefugees,lowereducatedthannativeDutchsubjects.SubjectswithaTurkishor
Morrocanbackgroundweremoreoftenmarriedandhomemakercomparedwiththe
otherethnicgroups.HealthstatuswaslowerinmigrantsthannativeDutchsubjects
formostdimensionsofhealth.TurkishandMoroccansubjectshadtheworsthealth,
whereasthehealthstatusofrefugeesresembledthatofnativeDutchsubjectsforsome
dimensionsofhealth.
Figure 2.1 shows that within each ethnic group, with the exception of refugees,
unemployed subjects had a worse health than employed subjects. Subjects with a
0102030405060708090
100
native Dutch Turkish /Moroccan
Surinamsese /Antillean
Refugee
Employed >32 h/wk Employed <32 h/wkUnemployed Disability Homemaker
Figure 2.1 Perceivedhealthofsubjectswithdifferentethnicbackgroundsinacommunity-basedhealthsurveyintheNetherlands(n=2057)specifiedfordifferentcategoriesoflabourforceparticipationorbeingoutoftheworkforce

26 Chapter2
disabilitypensionhadtheworsthealth ineveryethnicgroup.Amongsubjectswith
aTurkishorMoroccanbackgroundthehealthstatusofhomemakerswasequaltothe
healthstatusofunemployedsubjects.
Table 2.2 shows that all socio-demographic variables in this study were included
inthemultivariatemodel.MigrantsmoreoftenhadapoorhealththannativeDutch
subjects,evenafteradjustingforage,sex,educationallevel,maritalstatus,andlabour
forceparticipation.ThehealthstatusofTurkishorMoroccansubjectswastheworst
(OR=3.9(2.6-6.0)),whereasthehealthstatusofrefugeeswasnotsignificantlydifferent
(OR=1.8(0.9-3.3))fromthatofnativeDutchsubjects.
Table2.3describestheassociationswithhealth-relatedqualityoflife,whichresem-
bles thepatternobservedforaperceivedpoorhealth in table2.Allmigrantgroups
hadsignificantlylowerscoresforthephysicalaswellasthementalhealthdimensions
of the SF36 than the native Dutch group, indicating a poorer health. Unemployed
personsandpersonsreceivingadisabilitypensionhadsignificantlylowerscoresfor
alldimensionsofphysicalandmentalhealthcomparedwithemployedpersons.The
magnitudeofthesedifferenceswascomparabletotheobserveddifferencesinhealth
acrossageandeducation.
Table 2.2 Associationsbetweendemographicfactorsandemploymentstatuswithpoorhealthofsubjectswithdifferentethnicbackgroundsinacommunity-basedhealthsurveyintheNetherlands(n=1815)bymultivariatelogisticregressionanalysis
n oR (95% ci)
NativeDutchTurkish/MoroccanSurinamese/AntilleanRefugee
134615723379
1.03.9(2.6-6.0)2.5(1.7-3.6)1.8(0.9-3.3)
Age18-24yr25-44yr45-55yr55-64yr
143886417369
1.02.4(1.3-4.3)5.5(2.9-10.4)4.7(2.5-9.1)
Women 1016 1.6(1.2-2.1)
EducationallevelHighIntermediateLow
443473899
1.01.6(1.0-2.5)3.2(2.1-4.9)
Married 1106 1.4(1.0-1.8)
EmploymentstatusEmployed>32h/wkEmployed<32h/wkUnemployedDisabilitypensionHomemaker
996349194119157
1.01.0(0.7-1.5)2.6(1.7-3.8)14.4(8.8-23.6)1.1(0.7-1.8)
ORoddsratio,CIconfidenceinterval

Ch
apte
r2
Ethnicdifferencesinunemploymentandillhealth 27
Theinteractionbetweenemploymentstatusandethnicbackgroundhadasignificant
contributiontothelogisticregressionmodel(χ2=10.4;df=3;p=0.018),demonstrat-
ingthattheassociationsbetweenemploymentstatusandhealthvariedwithinethnic
groups (Table2.4).Health inequalitiesbetweenemployedandunemployedsubjects
werelargestamongtheDutchsubjects(OR=3.2(1.9-5.4),followedbySurinameseand
Antilleans(OR=2.6(1.3-5.2),andlesspronouncedamongTurkish/Moroccansubjects
(OR=1.6(0.7-3.7))andrefugees(OR=1.6(0.4-6.2)).ThePAFofunemploymentinpoor
healthwas14%amongDutch,26%inSurinameseandAntilleans,14%amongTurkish
andMoroccan,and13%amongrefugees.
Discussion
Illhealthwassubstantiallymorecommonamongunemployedpersonsthanworkers
inpaidemployment.Healthinequalitiesassociatedwithemploymentdifferedwithin
ethnic groups, with the strongest association between employment and health for
Table 2.3 Associationsbetweendemographicfactorsandemploymentstatuswithhealthrelatedqualityoflife(sixsubscalesoftheSF-36)ofsubjectswithdifferentethnicbackgroundsinacommunity-basedhealthsurveyintheNetherlands(n=1845)bymultivariatelinearregressionanalysis
General health
Physical functioning
bodily pain mental health
social functioning
vitality
Intercept 81.8(2.3) 102.4(2.4) 100.0(2.9) 82.9(2.2) 97.5(2.8)* 77.5(2.3)*
NativeDutchTurkish/MoroccanSurinamese/AntilleanRefugee
0-11.0(1.6)*-6.5(1.4)*-4.5(2.2)*
0-13.1(1.7)*-8.2(1.4)*-7.0(2.3)*
0-9.6(2.0)*-5.0(1.7)*-6.5(2.7)*
0-8.2(1.5)*-3.9(1.3)*-5.9(2.0)*
0-9.5(2.0)*-7.3(1.6)*-6.6(2.6)*
0-7.3(1.6)*-5.5(1.4)*-7.5(2.1)*
Age18-24yr25-44yr45-54yr55-64yr
0-1.7(1.7)-5.5(1.8)*-6.6(1.9)*
01.0 (1.7)-4.2(1.9)*-6.0(1.9*
0-2.2(2.1)-7.1(2.3)*-4.9(2.3)*
0-0.2(1.6)-0.3(1.7)-1.6(1.8)
0-2.4(2.0)-3.9(2.2)-2.7(2.3)
0-3.5(1.6)*-3.0(1.8)-2.5(1.8)
Women -1.4(1.0) -2.9(1.0)* -6.6(1.2)* -2.8(0.9)* -4.9(1.2)* -4.3(1.0)*
EducationallevelHighIntermediateLow
0-1.9(1.2)-6.1(1.2)*
0-1.9(1.3)-8.7(1.2)*
0-3.5(1.5)*-7.2(1.5)*
0-0.5(1.1)-4.4(1.1)*
0-1.0(1.5)-4.0(1.4)*
0-1.3(1.2)-6.1(1.1)*
EmploymentstatusEmployed>32h/wkEmployed<32h/wkUnemployedDisabilitypensionHomemaker
00.2(1.2)-7.7(1.5)*-28.3(1.9)*-1.0(1.8)
0-1.1(1.3)-4.7(1.6)*-33.2(2.0)*-3.1(1.9)
0-0.3(1.6)-8.8(1.9)*-29.3(2.3)*-0.09(2.2)
0-0.1(1.2)-10.5(1.4)*-16.1(1.8)*0.6(1.7)
0-1.3(1.5)-9.3(1.8)*-31.9(2.3)*1.0(2.1)
0-1.1(1.2)-7.3(1.5)*-19.3(1.9)*0.04(1.7)
*P<0.05

28 Chapter2
nativeDutchpersons,followedbySurinameseandAntilleansandalesspronounced
associationbetweenemploymentandhealthforTurkish/Moroccanpersonsandrefu-
gees. The population attributable fraction varied between 13% and 26%, indicating
thatemploymentstatusisanimportantfactorinsocioeconomichealthinequalities.
Thedesignof this studywas cross-sectional, and thereforenoassumptioncanbe
madeaboutthedirectionoftheassociationbetweenpoorhealthandunemployment
amongmigrantgroups.Unemploymentmaycausepoorhealthandpoorhealthmay
increase the probability of becoming unemployed.[7-8]A another limitation of this
studywasthelackofinformationonnon-respondents.Withrespecttounemployment
in the study population, the proportion of unemployed persons within each ethnic
groupresembledcloselytheregisteredunemploymentinthecityofRotterdamand,
thus,responsedoesnotseembiasedtowardsemployedorunemployedpersons.
In this study ethnic groups reported higher prevalences of poor health and also
lower scoresonhealth-relatedqualityof life.There is awidespreadagreement that
a single question asking subjects to rate their overall health on a scale from excel-
lenttopoorprovidesausefulsummaryofhowsubjectsperceivetheiroverallhealth
status.[16]However,thevalidityofthissingle-itemquestioninsubjectswithdifferent
cultural backgrounds has been questioned.[21] Differences in self-concepts between
ethnicgroupsmayinfluencetheresultsofthesingleitemgeneralhealthquestion.The
Table 2.4 Associationsbetweenunemploymentandpoorhealthwithindifferentethnicbackgroundsinacommunity-basedhealthsurveyintheNetherlands(n=1558)
oR (95% ci)
Age18-24yr25-44yr45-55yr55-64yr
11.9(1.1-3.6)4.2(2.3-8.0)4.1(2.2-7.9)
Women 1.6(1.2-2.2)
EducationallevelHighIntermediateLow
11.8(1.1-3.1)3.7(2.3-6.0)
NativeDutchTurkish/MoroccanSurinamese/AntilleanRefugee
14.3(2.4-7.4)2.8(1.8-4.3)2.0(0.9-4.1)
Effectofunemploymentwithinethnicgroup:NativeDutchTurkish/MoroccanAntillean/SurinameseRefugee
3.2(1.9-5.4)1.6(0.7-3.7)2.6(1.3-5.2)1.6(0.4-6.2)
Employed(full-timeandpart-time)andunemployedpersonswereincluded,whereashomemakersendisabledpersons(n=327)werenotincludedinthisanalysis.ORoddsratio,CIconfidenceinterval

Ch
apte
r2
Ethnicdifferencesinunemploymentandillhealth 29
observationthatafteradjustingforthewell-establishedsocio-demographicdetermi-
nantsofhealthinequalities,stillsystematicdifferencesinoccurrenceofpoorhealthin
ethnicgroupsrelativetotheDutchgroupwereobserved,mayindicateover-estimation
of poor health. In the current study similar conclusions on unemployed, ethnicity,
andhealthweredrawnwhenusingthesinglequestiononperceivedgeneralhealth
questionandtheother35questionsonphysicalandmentalhealthdimensionsofthe
SF36.Thiscorroboratestheopinionthatthegeneralhealthquestionprovidesagood
summery of the mental and physical health in migrant groups and the indigenous
population.Thisfindingis,ofcourse,alsosupportedbythehighcorrelationsbetween
perceivedgeneralhealthandallhealthdimensionsintheSF-36.
A high proportion of persons with a poor health among ethnic groups has been
observed invariousstudies indifferent countries.[9-13]Differentexplanationshave
beenputforward.ASwedishstudyamongimmigrantsfromPoland,Turkey,andIran
foundthatacculturation(definedbytheknowledgeoftheSwedishlanguage)wasan
important mediator in the pathway between ethnicity and poor health.[22] Indeed,
in our study population differences in mastering the Dutch language may have
influencedhealth.ForSurinameseandAntilleansDutch isusuallya firstor second
language,whereasforTurksandMoroccansknowledgeoftheDutchlanguageisoften
limitedorabsent,especiallyamongolderwomen.Languageproblemsmayhamper
effective communication with physicians and also inhibit access to information on
healthandhealthcare.[23]Inthecurrentstudy,masteryof theDutchlanguagewas
notincludedintheanalyses,buttheobservationthatthehealthstatusofhomemakers
withaTurkishorMoroccanbackgroundwasworse thanthehealthstatusofhome-
makerswithanotherethnicbackgroundmayreflectaloweracculturation.
Differencesinmigrationexperiencesmayalsocontributetothedifferencesinhealth
betweentheethnicminoritygroups.Refugeeshaveadifferentmigrationhistorythan
Turks,Moroccans,Surinamese,andAntilleans.Forrefugees,experiencesofviolence,
theflightforasylumandforcedbrokensocialnetworksmayhaveaffectedhealth.[13]
However,inthisstudywefoundthatrefugeeshadarelativelygoodhealthcompared
with the other ethnic minority groups. The relatively good health of refugees can
partlybeexplainedbytherelativelyhigheducationallevelofrefugeesrelativetothe
otherethnicminoritygroups.
Employedmigrantsarestillconcentratedinbluecollarjobsinindustry.[15]Especially
foremployedrefugees,whohavearelativelyhigheducationallevel(87%intermedi-
ate/higheducated)comparedtotheemployednativeDutch(77%intermediate/high
educated), adverse health effects of unsatisfactory jobs have been suggested (Smith
2000).AnAustralianstudyhas shown thatunsatisfactory jobscanbeasdepressing
asunemployment.[24]Unfortunately,informationaboutthepotentialmisfitbetween
personalcapabilitiesandjobrequirementswasnotcollectedinthecurrentstudy.

30 Chapter2
It was hypothesized that the associations of poor health and employment status
would be less profound in ethnic groups with a high prevalence of unemployment
comparedtotheDutchpopulation.Whentheunemploymentrateishigh,theeffectof
healthselectionoutoftheworkforceisrelativesmallcomparedtootherfactorsthat
determinelabouropportunitiesforpeople.[16]Ingeneral,ourresultsindeedshowed
that the association between unemployment and poor health was strongest in the
Dutchpopulation(OR=3.2)withthelowestunemployment,whereastheassociations
between unemployment and health were less profound in ethnic minority groups
(ORsbetween1.6and2.6),whichwerecharacterisedbyahigherunemploymentlevel.
In the current study the logistic regressionanalysis showed that theassociationbe-
tweenunemploymentandhealthwasnotstatisticallysignificantwithintheTurkish/
Moroccan group. However, when adjustment for sex and educational level did not
takeplace,asignificantassociationbetweenunemploymentandhealth(OR=2.5)was
found.Hence,theabsenceofhealthinequalitiesacrossemploymentstatuswithinthis
ethnicgroupmaybeexplainedby thestrongcorrelationsbetweensexandemploy-
mentstatusandbetweeneducationallevelandemploymentstatus.Theseadditional
analyses showed that especially female, low educated Turkish/Moroccan persons
wereoftenunemployedandalsoreportedthehighestoccurrenceofapoorhealth.
ThePAFofunemploymentinpoorhealthwithinthefourethnicgroupsvariedbetween
13% among refugees to 26% among Surinamese/Antillean subjects. The PAF values
among Dutch persons (14%) was strongly influenced by the high OR for unemploy-
ment,whereasthePAFvaluesamongtheethnicminoritygroupsweremoreinfluenced
bythehighprevalenceofunemployment.Althoughthiscross-sectionalstudydoesnot
permitconclusionsoncausality,thesefindingssuggestthat,undertheassumptionthat
unemploymentleadstoapoorhealth,healthinequalitiesrelatedtounemploymentarea
majorpublichealthprobleminallethnicgroups.Thus,policiesforhealthequityshould
paymoreattentiontomeasuresthatincludepersonswithapoorhealthinthelabour
marketandthatpreventworkerswithillhealthfromdroppingoutoftheworkforce.
Acknowledgements
FundingforthisstudywasprovidedbythePublicHealthFund(FondsOGZ).
ReFeRences
1. MarmotMG,SmithGD,StansfeldS,PatelC,NorthF,HeadJ,WhiteI,BrunnerE,FeeneyA: Health inequalities among British civil servants: the Whitehall II study. Lancet 1991,337:1387-1393.

Ch
apte
r2
Ethnicdifferencesinunemploymentandillhealth 31
2. ClaussenB:Healthandre-employmentinafive-yearfollow-upoflong-termunemployed.Scand J Public Health 1999,27:94-100.
3. JanlertU:Unemploymentasadiseaseanddiseasesoftheunemployed.Scand J Work Environ Health 1997,23Suppl3:79-83.
4. MorrisJK,CookDG,ShaperAG:Lossofemploymentandmortality.BMJ (Clinical research ed 1994,308:1135-1139.
5. AlaviniaSM,BurdorfA:Unemploymentandretirementandill-health:across-sectionalanalysisacrossEuropeancountries.Int Arch Occup Environ Health 2008,82:39-45.
6. BootCR,HeijmansM,vanderGuldenJW,RijkenM:Theroleofillnessperceptionsinlaborparticipationofthechronicallyill.Int Arch Occup Environ Health 2008,82:13-20.
7. BartleyM,SackerA,ClarkeP:Employmentstatus,employmentconditions,andlimitingillness:prospectiveevidencefromtheBritishhouseholdpanelsurvey1991-2001.Journal of epidemiology and community health 2004,58:501-506.
8. SchuringM,BurdorfA,KunstAE,MackenbachJP:Theeffectofillhealthonenteringandmaintainingpaidemployment:evidenceinEuropeancountries.Journal of epidemiology and community health 2007,61:597-604.
9. SmithGD:Learningtolivewithcomplexity:ethnicity,socioeconomicposition,andhealthinBritainandtheUnitedStates.Am J Public Health 2000,90:1694-1698.
10. BosV,KunstAE,Keij-DeerenbergIM,GarssenJ,MackenbachJP:Ethnicinequalitiesinage-andcause-specificmortalityinTheNetherlands.Int J Epidemiol 2004,33:1112-1119.
11. NazrooJY:Thestructuringofethnicinequalitiesinhealth:economicposition,racialdiscrimi-nation,andracism.Am J Public Health 2003,93:277-284.
12. ChandolaT:EthnicandclassdifferencesinhealthinrelationtoBritishSouthAsians:usingthenewNationalStatisticsSocio-EconomicClassification.Soc Sci Med 2001,52:1285-1296.
13. SundquistJ:Ethnicity,socialclassandhealth.Apopulation-basedstudyontheinfluenceofsocialfactorsonself-reportedillnessin223LatinAmericanrefugees,333Finnishand126southEuropeanlabourmigrantsand841Swedishcontrols.Soc Sci Med 1995,40:777-787.
14. DunnJR,DyckI:SocialdeterminantsofhealthinCanada’simmigrantpopulation:resultsfromtheNationalPopulationHealthSurvey.Soc Sci Med 2000,51:1573-1593.
15. ElkelesT,SeifertW:Immigrantsandhealth:unemploymentandhealth-risksoflabourmi-grantsintheFederalRepublicofGermany,1984-1992.Soc Sci Med 1996,43:1035-1047.
16. FayersPM,SprangersMA:Understandingself-ratedhealth.Lancet 2002,359:187-188. 17. KuilmanM,vanDijkAP,vanderLeeG,SchrijversCTM:Resultatengezondheidsenquete
Rotterdam2003[ResultshealthquestionnaireRotterdam2003].internrapportGGDRot-terdameo2005.
18. CBS:Herkomstvanpersonen;allochtonenenmigratie[Countryoforiginofpersons;mi-grantsandmigration].CentraalBureauvoordeStatistiek,Voorburg/Heerlen2003.
19. WareJE,Jr.,SherbourneCD:TheMOS36-itemshort-formhealthsurvey(SF-36).I.Concep-tualframeworkanditemselection.Med Care 1992,30:473-483.
20. LastJM:Adictionaryofepidemiology,4thedn.OxfordUniversityPress,NewYork.2001. 21. AgyemangC,DenktasS,BruijnzeelsM,FoetsM:Validityofthesingle-itemquestionon
self-ratedhealthstatusinfirstgenerationTurkishandMoroccansversusnativeDutchintheNetherlands.Public health 2006,120:543-550.
22. WikingE,JohanssonSE,SundquistJ:Ethnicity,acculturation,andselfreportedhealth.Apopulation based study among immigrants from Poland, Turkey, and Iran in Sweden.Journal of epidemiology and community health 2004,58:574-582.

32 Chapter2
23. UnikenVenemaHP,GarretsenHF,vanderMaasPJ:Healthofmigrantsandmigranthealthpolicy,TheNetherlandsasanexample.Soc Sci Med 1995,41:809-818.
24. GraetzB:Healthconsequencesofemploymentandunemployment:longitudinalevidenceforyoungmenandwomen.Soc Sci Med 1993,36:715-724.

3The impact of ill health on exit from paid
employment in europe among older workers
vandenBergT.I.J.,SchuringM,AvendanoM,MackenbachJP,BurdorfA
Occupational and Environmental Medicine, in press

34 Chapter3
absTRacT
objective: To determine the impact of ill health on exit from paid employment in
Europeamongolderworkers.
methods: ParticipantsoftheSurveyonHealthandAgeinginEurope(SHARE)in11
Europeancountriesin2004and2006wereselectedwhenbetween50and63yearsold
andinpaidemploymentatbaseline(n=4611).Datawerecollectedonself-ratedhealth,
chronicdiseases,mobility limitations,behavioural factors (obesity,smoking,alcohol
use, andphysical activity), andworkcharacteristics.Participantswere followed for
twoyearsandclassifiedintoemployed,retired,unemployed,anddisabledatendof
follow-up.Multinomiallogisticregressionwasusedtoestimatetheeffectofdifferent
measuresofillhealthonexitfrompaidemployment.
Results: During the two-year follow-up period, 17% of employed workers quitted
paidemployment,primarilydue toearlyretirement.Controlling for individualand
workrelatedcharacteristics,poorself-perceivedhealthwasstronglyassociatedwith
exitfrompaidemploymentduetoretirement,unemployment,ordisability(ORsfrom
1.32to4.37).Adjustmentbyworkrelatedfactorsandlifestylereducedthesignificant
associations between ill health and exit from paid employment by 0 to 18.7%.Low
education,obesity,lowjobcontrol,andeffort-rewardimbalancewereassociatedwith
measuresofillhealth,butalsoriskfactorsforexitfrompaidemploymentafteradjust-
mentforillhealth.
conclusion:Poorself-perceivedhealthwasstrongestassociatedwithexitfrompaid
employment among European workers aged 50-63 years, compared to three other
measuresof illhealth.This studysuggests that theeffectsof illhealthonexit from
paid employment can be diminished by a variety of preventive measures towards
obesity,problematicalcoholuse,jobcontrol,andeffort-rewardbalance.

Ch
apte
r3
TheimpactofillhealthonexitfrompaidemploymentinEuropeamongolderworkers 35
inTRoDucTion
Inmanyindustrializedcountries thepopulation isageing,dueto increasing lifeex-
pectancyandfallingbirthrates.[1]Aratherparadoxicaldevelopmentisthat,despite
increasesinlifeexpectancy,theaveragetimepeoplespendinpaidworkhasdecreased
inmostEuropeancountries.Althoughpartofthisdecreaseisexplainedbyprolonged
educationamongyoungercohorts,amoreimportantcontributoristhehigherrateof
exit from the labourmarketatolderages.[2]Asa consequence,manycountriesare
developingpoliciestoencourageolderworkerstoremainlongerinthelabourmarket
anddelayretirement.[3]Clearly,thesuccessofthesepolicieswilldependonabetter
understandingofageingintheworkforceandtheparticularroleofhealthandwork
characteristics in continuing work or exit from the labour market. Recent evidence
suggeststhatworkcanbegoodforhealth,reversingtheharmfuleffectsoflong-term
unemploymentandprolongedsicknessabsence.[4]However,thecurrentassumption
seemsthatillnessisincompatiblewithbeinginwork.[4]
Thereisampleevidencethatillhealthmaycauseexitfromthelabourforce.[3,5-10]
Theearlieststudiesfocusedonpoorhealthasriskforunemployment,forexamplein
constructionworkers,wherebyseveralhealthproblemspredictedtheriskoflong-term
unemployment.[6]Morerecently, there isanincreasingawarenessthatamongolder
workers ill health does not only affect unemployment and disability, but may also
driveselectionoutoftheworkforceduetoearlyretirementandstayinghometotake
careofthefamily.[3,10]Forexample,inaFinnishcohortofmaleworkerswith11year
follow-up,self-assessedpoorhealthwasastrongpredictorofbothenrolmentintodis-
abilitybenefitaswellasnon-illnessbasedearlyretirement.[7]OntheEuropeanlevel
itwasshownthatillhealthwasariskfactorfortransitionsbetweenpaidemployment
and various forms of non-employment, including retirement, unemployment, and
takingcareofthehousehold.[5,9]
However,itremainsunclearwhichtypeofhealthmeasureismostpredictiveforfu-
tureexit,andhowlargethedirecteffectofpoorhealthisonfutureexit.Theaimofthe
studyistoexploretheroleofillhealthinexitfrompaidemployment.Thefollowing
researchquestionswereformulated.First,whichmeasuresofhealtharepredictivefor
exitfrompaidemployment?Second,howmuchoftheobservedassociationsbetween
illhealthandfutureexitcanbeexplainedbyworkrelatedfactorsandlifestyle?

36 Chapter3
meTHoDs
Studypopulation
ThestudypopulationconsistedofparticipantsoftheSurveyonHealthandAgeingin
Europe(SHAREstudy).SHAREisalongitudinalsurveythataimstocollectmedical,
social,andeconomicdataonthepopulationagedover50yearsin11EuropeanUnion
countries(Sweden,Denmark,TheNetherlands,Belgium,Germany,Austria,Switzer-
land, France, Italy, Spain, and Greece).[11-12] In the participating SHARE countries
theinstitutionalconditionswithrespecttosamplingweresodifferentthatauniform
samplingdesignfortheentireprojectwasnotfeasible.Differentregistriesofnational
orlocallevelwereusedthatpermittedstratificationbyage.Thesamplingdesignsvar-
iedfromsimplerandomselectionofhouseholdstocomplicatedmultistagedesigns.
ThefirstwaveofdatawascollectedbyinterviewsbetweenAprilandOctober2004.
Theoverallhouseholdresponseacrossthe11SHAREcountriesinwhichdatacollec-
tiontookplacein2004was57.4%,althoughsubstantialdifferencesamongcountries
wereobserved.[12]Theavailabledatasetfromthefirstwaveofdatacollection(SHARE
Release2.0)contains28,517participants,with12,965subjects(45%)agedbetween50
and 63 years. Individuals aged 63 years and older were excluded from the current
study,sinceitwasassumedthatworkersnormallyretiredwhentheybecame65years
oldattheendoffollow-up.Whilethisassumptioncertainlyhaslimitations,giventhe
complexity to define retirement at the individual level and the small proportion of
workersabovetheageof63yearsinthestudypopulation(about2%),itwasconsid-
eredtobe thedefinitionthatwasmostcomparableacrosscountries.For93persons
employmentstatuswasunknown,resultinginastudypopulationof12,872subjects,
ofwhich7119 (55%) subjectswithpaidemployment.After twoyears8,729 subjects
participated again in the questionnaire survey (SHARE Release 1.0), resulting in a
responseof67%.Completeinformationonemploymentstatusin2006wasavailable
for8,568 subjects.For the longitudinalanalysisof the influenceof illhealthonexit
ofthelabourmarket,acohortwasavailableof4,611subjectswithpaidemployment
in 2004 and complete information on individual and work related characteristics at
baselineandworkstatusatfollow-upin2006.
Labourforceparticipation
Theoutcomeof thisstudyisworkstatus,whichwasbasedonself-reportedcurrent
economic status that best described respondent’s situation based on four mutually
exclusivecategories:paidwork,retired,unemployed,disabled.Thedefinitionofbe-
ingemployedinSHAREencompassesallindividualswhodeclaredtohavedoneany

Ch
apte
r3
TheimpactofillhealthonexitfrompaidemploymentinEuropeamongolderworkers 37
kind of formal paid work in the last four weeks, including self-employed work for
familybusiness.Unemployedwerethosewhowerelaidofffromtheirlastjobbefore
beingabletobenefitfromnormalpensionbenefits,andthereforewereforcedtospend
some time in unemployment before effectively being retired. Sickness or disability
insurance applied to people who exited the labour force for reasons of recognized
health problems.[11] The category of disabled participants predominantly includes
persons whose health problems at work were an eligibility criterion for receiving a
disabilitypension.Total exit from theworkforcewasdefinedasexit either through
earlyretirement,unemploymentordisability.
Healthmeasurements
TheEuropeanversionofself-perceivedhealth,a5-pointscalequestionrangingbetween
verygoodto(very)bad,wasusedtodefinepoorhealth(lessthangood).Thisfrequently
usedquestionhasbeenshowntobeagoodindicatorofgeneralphysicalandmental
health.[13-14]Asecondhealthmeasurewashavingatleastoneofthefollowingchronic
diseases diagnosed by a doctor during lifetime; heart disease, stroke, diabetes, lung
disease,asthma,arthritisorrheuma,andosteoporosis.Functionallimitations,reflect-
ingtheabilityofindividualstoperformnormallyinsociety,werecharacterizedwith
twodichotomousmeasuresofhealth.Thefirstmeasureofinterest,mobilityproblems,
reflectslimitationswithmobility,armorfinemotorfunctions.Mobilityproblemswere
definedasoneormoreaffirmativeanswersonalistof10mobilityproblems,suchas
walking100metersandreachingorextendingarmsaboveshoulderlevel.Thesecond
measure,instrumentallimitations,waspositiveforsubjectswithoneormoreofthe13
instrumentalactivitiesofdailylife,suchaspreparingmealsandmakingphonecalls.
Individualcharacteristics
The highest education successfully completed was coded according to the 1997
International Standard Classification of Education (ISCED-97) and categorized into
low (pre-primary, primary and lower secondary education), intermediate (upper
secondaryeducation)andhigh (post secondaryeducation).Bodymass index (BMI)
wascalculatedbydividingbodyweightinkilogrambythesquareofbodyheightin
meters. BMI was recoded into normal (<25 kg/m2), overweight (>=25 and <30 kg/
m2), or obese (>=30 kg/m2). Marital status was used to categorize individuals into
thosewhowere livingwithaspouseorapartner in thesamehousehold (reference
category)andthoselivingalone.Smokersweresubjectswhowerecurrentlysmoking;
allotherswerecategorizedasnon-smokers.Problematicalcoholusewasdefinedby
analcoholconsumptionoftwoormoreglassesofalcoholicbeverageatleast5daysa

38 Chapter3
weekinthelastsixmonths.Physicalactivitywasmeasuredwithsinglequestionson
regularparticipationinmoderateactivitiesandvigorousactivities,bothona4-point
scale ranging from ‘more than once a week’ to ‘hardly ever, or never’. Those who
reportedlessthanonceaweekmoderateorvigorousactivitywereconsideredtolack
inleisure-timephysicalactivity.[12]
Workrelatedcharacteristics
Workrelatedcharacteristicswereassessedbyashortbatteryofitemsderivedfrom(i)the
JobContentQuestionnairemeasuringthedemand-controlmodel[15]and(ii)theeffort-
rewardimbalancemodelquestionnaire[16].Allitemswereonafourpointscaleranging
from1‘stronglyagree’to4‘stronglydisagree’.Singleitemmeasuredhightimepressure
(“I’munderconstanttimepressureduetoaheavyworkload.”)Lackofjobcontrolwas
measuredby thesumscoreof two items (“Ihavevery little freedomtodecidehowI
domywork”,“Ihaveanopportunitytodevelopnewskills”).Country-specificmedian
valueswereusedtodefinethepresenceofhightimepressure,andlackofjobcontrol.
Effort-rewardimbalancewasmeasuredby2itemson‘effort’(‘physicallydemand-
ing’and‘timepressure’)and5itemson‘reward’(‘receiveadequatesupport’,‘receive
recognition’, ‘adequate salary’, ‘job promotion prospects’, ‘job security’). ‘Effort-re-
wardimbalance’wasdefinedbytheratioofthesumscoreofthe‘effort’itemsandthe
sumscoreofthe‘reward’items,adjustedforthenumberofitems.[17]Effort-reward
imbalancewasdefinedasascorewithintheuppertertileofthisratiopercountry.[17]
Ahighphysicalworkdemandwasmeasuredwithoneitem(“Myjobisphysically
demanding.”).Country-specificmedianvaluewasusedtodefinethepresenceofhigh
physicalworkdemand.
Statisticalanalysis
Logistic regression was used to evaluate cross-sectional associations at baseline be-
tween four measures of ill health as dependent variables and individual and work
characteristicsasindependentvariables,adjustingforcountry.
Risk factors for exit from paid employment during the two year follow-up were
evaluatedbymeansofamultinomiallogisticregressionanalysis.Thestudypopula-
tion consisted of subjects with paid employment at baseline and odds ratios were
calculatedforthelikelihoodoftransitiontoeverystateofnon-participation,i.e.early
retirement,unemployment,anddisabilityduringthe2yearfollow-up.Theresultsfor
homemakerswerenotshownasthisgroupwashighlydominatedbyfemalegender,
butsubjectswhoexitedpaidemploymentthroughbecomingahomeworkerremained
inthesample.Thefirststepintheanalysiswastoestablishunivariateassociationsbe-

Ch
apte
r3
TheimpactofillhealthonexitfrompaidemploymentinEuropeamongolderworkers 39
tweenthedependentvariableworkstatus,andhealthmeasures,socio-demographic
factors, lifestyle factors, and work characteristics as independent factors, including
country as fixed effect. In the second step multivariate analyses were conducted to
modelemploymentstatusat theendof follow-upasa functionof fourmeasuresof
health. For the initial selection of potential covariates for the multivariate model,
univariate associations with a significant level of p<0.05 were considered. For each
independent variable measure of health, we calculated odds ratios for dependent
variable exit for work, adjusted for age, sex and education (reference model) and
furtheradjustedforlifestylefactorsandworkrelatedcharacteristicsseparately,andin
combination.Foreachregressionmodelthepercentagechangeinoddsratioofeach
Table 3.1 Individualcharacteristics,lifestylefactors,healthstatus,andworkcharacteristicsamong4611employedpersonsaged50-63yearsoldin11EuropeancountriesduringthefirstwaveoftheSurveyonHealthandAgeinginEurope(SHARE)
employed(n=4611)
IndividualcharacteristicsFemaleAge
50-54yr55-59yr60-63yr
EducationlevelLowIntermediateHigh
Livingwithoutpartner
45%(2088)
48%(2224)40%(1826)12%(561)
31%(1443)33%(1513)36%(1655)20%(937)
LifestylefactorsBMI
<25kg/m2
25-30kg/m2
≥30kg/m2
CurrentsmokerProblematicalcoholuseLackofleisure-timephysicalactivity
44%(2011)41%(1910)15%(690)27%(1252)14%(664)56%(2561)
Work-relatedfactorsHightimepressureatwork(1/0)Highphysicalworkdemands(1/0)Lackofjobcontrol(1/0)Effort-rewardimbalanceatwork(1/0)
56%(2567)46%(2138)57%(2622)33%(1531)
PerceivedhealthVerygoodGoodFair(Very)bad
32%(1475)51%(2343)15%(708)2%(85)
Chronicdisease(1/0) 25%(1130)
Mobilityproblems(1/0) 28%(1287)
Instrumentallimitationsindailyactivities(1/0) 4%(170)
40 Chapter3
pathwayofexitwascalculated(100x[ORreferencemodel–OR+explanatoryfactors]/[ORreferencemodel-1].
[18]Oneofthemainadvantagesofthismethodisthatitcanbeusedtoestimatedirect
and indirectcontributionsofexplanatory factors.One limitation is that thepercent-
age change can be similar for different absolute changes in odds ratios. However,
allcontributionswerecalculatedrelativelytothesameoddsratios,whichwerealso
presented.Therefore,webelievethatthislimitationhasalimitedeffectonourresults.
Population Attributable Fractions were calculated for significant determinants of
exit from paid employment, using the formula PAF= Pe (OR-1)/(1+PE(OR-1))[19],
wherebyPerepresentstheprevalenceofexposureinthestudypopulation.
All statistical models were based on the number of persons with complete data
available.ThestatisticalanalyseswerecarriedoutwithSPSSversion15.0.[20]
ResuLTs
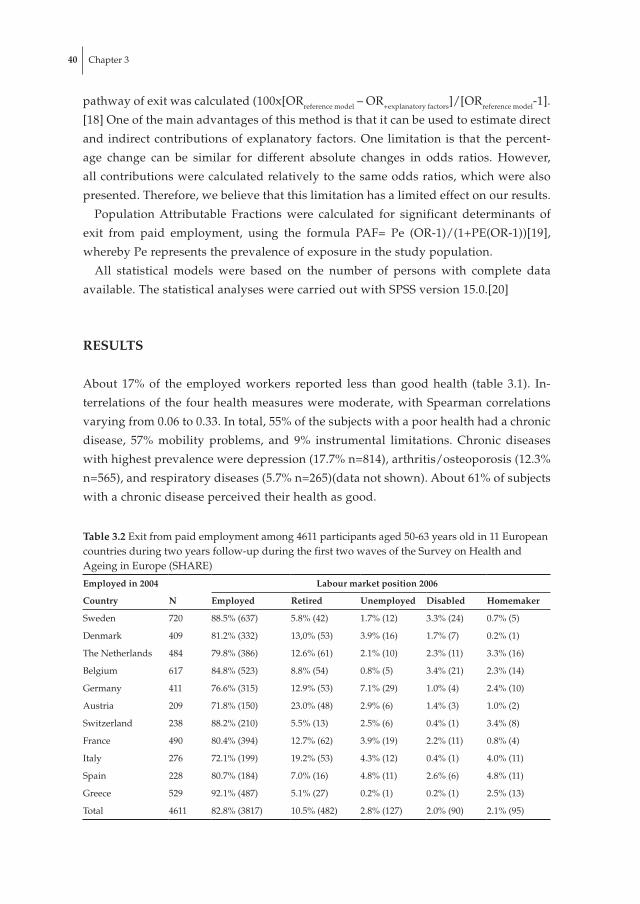
About 17% of the employed workers reported less than good health (table 3.1). In-
terrelationsof the fourhealthmeasuresweremoderate,withSpearmancorrelations
varyingfrom0.06to0.33.Intotal,55%ofthesubjectswithapoorhealthhadachronic
disease, 57% mobility problems, and 9% instrumental limitations. Chronic diseases
withhighestprevalenceweredepression(17.7%n=814),arthritis/osteoporosis(12.3%
n=565),andrespiratorydiseases(5.7%n=265)(datanotshown).About61%ofsubjects
withachronicdiseaseperceivedtheirhealthasgood.
Table 3.2 Exitfrompaidemploymentamong4611participantsaged50-63yearsoldin11Europeancountriesduringtwoyearsfollow-upduringthefirsttwowavesoftheSurveyonHealthandAgeinginEurope(SHARE)
employed in 2004 Labour market position 2006
country n employed Retired unemployed Disabled Homemaker
Sweden 720 88.5%(637) 5.8%(42) 1.7%(12) 3.3%(24) 0.7%(5)
Denmark 409 81.2%(332) 13,0%(53) 3.9%(16) 1.7%(7) 0.2%(1)
TheNetherlands 484 79.8%(386) 12.6%(61) 2.1%(10) 2.3%(11) 3.3%(16)
Belgium 617 84.8%(523) 8.8%(54) 0.8%(5) 3.4%(21) 2.3%(14)
Germany 411 76.6%(315) 12.9%(53) 7.1%(29) 1.0%(4) 2.4%(10)
Austria 209 71.8%(150) 23.0%(48) 2.9%(6) 1.4%(3) 1.0%(2)
Switzerland 238 88.2%(210) 5.5%(13) 2.5%(6) 0.4%(1) 3.4%(8)
France 490 80.4%(394) 12.7%(62) 3.9%(19) 2.2%(11) 0.8%(4)
Italy 276 72.1%(199) 19.2%(53) 4.3%(12) 0.4%(1) 4.0%(11)
Spain 228 80.7%(184) 7.0%(16) 4.8%(11) 2.6%(6) 4.8%(11)
Greece 529 92.1%(487) 5.1%(27) 0.2%(1) 0.2%(1) 2.5%(13)
Total 4611 82.8%(3817) 10.5%(482) 2.8%(127) 2.0%(90) 2.1%(95)

Ch
apte
r3
TheimpactofillhealthonexitfrompaidemploymentinEuropeamongolderworkers 41
Duringthetwoyearfollow-upperiod17%(n=794)ofemployedworkersexitedthe
workforce,primarilyduetoretirement(11%)(table3.2).Considerabledifferences in
prevalenceofexitfrompaidemploymentandpathwaysofexitwerefoundbetween
countries.At baseline all four measurements of ill health were associated with low
education (OR’s 1.27-2.00) (table 3.3). Obesity (ORs 1.53-2.74) and lack of physical
activity in leisure time (ORs 1.24-1.87) were associated with most health outcomes.
Effort-rewardimbalanceatworkwasincreasedforallfourhealthoutcomes(ORs1.25-
1.64).Hightimepressure(ORs0.98-1.09),andproblematicalcoholuse(ORs0.87-1.12)
werenotassociatedwithanyofthehealthoutcomes.
Table 3.3 Cross-sectionalmultivariateassociationsbetweenindividualcharacteristics,lifestyleandworkcharacteristics,anddifferenthealthoutcomesamong4611employedpersonsaged50-63yearsoldin11Europeancountries,duringthefirstwaveoftheSurveyonHealthandAgeinginEurope(SHARE)
Less than good perceived health (n=793)
chronic disease(n=1130)
mobility problems(n=1287)
instrumental limitations in daily activities(n=170)
oR 95%ci oR 95%ci oR 95% ci oR 95% ci
Age50-54yr55-59yr60-63yr
11.24*(1.04-1.47)1.35*(1.06-1.73)
11.55*(1.33-1.79)1.72*(1.39-2.13)
11.21*(1.05-1.40)1.43*(1.16-1.77)
11.33(0.95-1.85)1.40(0.86-2.29)
EducationallevelHighIntermediateLow
11.55*(1.26-1.90)2.00*(1.62-2.47)
11.21*(1.02-1.44)1.30*(1.08-1.58)
11.22*(1.03-1.44)1.27*(1.06-1.51)
11.34(0.90-2.03)1.61*(1.07-2.43)
Female 1.18(1.00-1.39) 1.34*(1.16-1.54) 2.05*(1.78-2.37) 2.44*(1.74-3.43)
Withoutpartner 0.99(0.81-1.21) 1.24*(1.05-1.46) 1.05(0.89-1.24) 1.17(0.81-1.68)
BMI<25kg/m2
25-30kg/m2
≥30kg/m2
11.03(0.86-1.24)2.01*(1.62-2.50)
11.18*(1.01-1.39)1.88*(1.55-2.29)
11.49*(1.28-1.74)2.74*(2.25-3.32)
11.13(0.79-1.61)1.53(0.99-2.35)
Currentsmoker 1.18(0.98-1.40) 0.93(0.80-1.09) 1.15(0.99-1.34) 1.55*(1.11-2.16)
Problematicalcoholuse
0.98(0.78-1.24) 1.12(0.92-1.37) 0.87(0.71-1.07) 0.98(0.60-1.60)
Lackofleisure-timephysicalactivity
1.46*(1.23-1.72) 1.24*(1.08-1.43) 1.57*(1.37-1.81) 1.87*(1.33-2.63)
Hightimepressureatwork
1.04(0.87-1.24) 0.98(0.84-1.15) 1.06(0.91-1.24) 1.09(0.76-1.56)
Highphysicalworkdemands
1.14(0.94-1.38) 1.09(0.92-1.28) 1.26*(1.08-1.48) 1.07(0.73-1.56)
Lackofjobcontrol 1.26*(1.06-1.49) 1.15*(1.00-1.33) 1.04(0.90-1.19) 1.23(0.88-1.71)
Effort-rewardimbalanceatwork
1.64*(1.33-2.01) 1.25*(1.04-1.50) 1.39*(1.17-1.66) 1.55*(1.03-2.33)
*P<0.05,ORoddsratio,CIconfidenceinterval

42 Chapter3
Table 3.4 Univariateassociationsbetweenhealth,individualcharacteristics,lifestyle,andworkcharacteristics,andtransitionsintounemployment,retirement,anddisabilityamong4611initiallyemployedsubjectsaged50-63yearsoldduringtwoyearsfollow-upintheSurveyonHealthandAgeinginEurope(SHARE)(stayinginpaidemploymentasreferencecategory)
unemployed (n=127)
Retired(n=482)
Disabled(n=90)
Total exit (n=699)
oR 95%ci oR 95%ci oR 95% ci oR 95% ci
Lessthangoodperceivedhealth(1/0)
2.49*(1.70-3.66) 1.50*(1.19-1.90) 5.04*(3.28-7.74) 2.08*(1.72-2.51)
Chronicdisease(1/0)
1.62*(1.10-2.37) 1.74*(1.42-2.14) 3.00*(1.96-4.59) 2.00*(1.68-2.37)
Mobilityproblems(1/0)
1.29(0.88-1.90) 1.37*(1.11-1.68) 3.44*(2.26-5.26) 1.56*(1.31-1.85)
Instrumentallimitationsindailyactivities(1/0)
1.69(0.76-3.73) 1.25(0.78-2.02) 3.52*(1.82-6.83) 1.73*(1.19-2.50)
Age50-54yr55-59yr60-63yr
11.72*(1.17-2.53)2.51*(1.42-4.43)
18.08*(5.91-11.04)33.30*(23.36-47.46)
12.36*(1.50-3.72)1.31(0.56-3.07)
13.96*(3.21-4.88)8.75*(6.83-11.21)
EducationallevelHighIntermediateLow
11.87*(1.17-3.00)2.80*(1.69-4.64)
11.12(0.89-1.43)1.65*(1.29-2.12)
11.56(0.89-2.72)2.20*(1.28-3.77)
11.39*(1.14-1.71)1.68*(1.37-2.05)
Female 1.16(0.81-1.66) 0.83(0.68-1.01) 0.95(0.62-1.45) 0.92(0.78-1.08)
Withoutpartner 1.36(0.90-2.05) 0.83(0.64-1.06) 0.78(0.45-1.37) 0.92(0.75-1.13)
BMI<25kg/m2
25-30kg/m2
≥30kg/m2
11.00(0.66-1.51)1.92*(1.21-3.07)
11.23*(1.00-1.52)1.40*(1.05-1.84)
10.97(0.60-1.56)1.71(0.98-2.97)
11.11(0.93-1.33)1.51*(1.20-1.89)
Currentsmoker 1.21(0.82-1.80) 0.87(0.70-1.09) 1.46(0.93-2.30) 0.97(0.81-1.17)
Problematicalcoholuse
1.04(0.63-1.72) 1.37*(1.07-1.76) 1.65(0.95-2.87) 1.57*(1.27-1.94)
Lackofleisure-timephysicalactivity
1.29(0.89-1.86) 1.24*(1.01-1.51) 0.98(0.64-1.49) 1.19*(1.01-1.44)
Hightimepressureatwork
0.72(0.50-1.04) 1.02(0.83-1.25) 1.23(0.80-1.90) 1.00(0.85-1.18)
Highphysicalworkdemands
1.04(0.73-1.50) 1.17(0.96-1.42) 1.57*(1.03-2.40) 1.19*(1.01-1.40)
Lackofjobcontrol 1.59*(1.07-2.37) 1.23*(1.00-1.51) 2.68*(1.59-4.54) 1.62*(1.37-1.91)
Effort-rewardimbalanceatwork
1.51*(1.05-2.16) 1.09(0.89-1.34) 1.62*(1.06-2.48) 1.22*(1.03-1.44)
*P<0.05,ORoddsratio,CIconfidenceinterval

Ch
apte
r3
TheimpactofillhealthonexitfrompaidemploymentinEuropeamongolderworkers 43
Table 3.5 Multivariateassociationsbetween4differenthealthmeasuresandtransitionsintounemployment,retirement,anddisabilityamong4611initiallyemployedsubjectsaged50-63yearsoldin11Europeancountriesduringtwoyearsoffollow-upintheSurveyonHealthandAgeinginEurope(SHARE)(stayinginpaidemploymentasreferencecategory)
unemployed (n=127)
Retired(n=482)
Disabled(n=90)
Total exit (n=699)
oR 95%ci oR 95%ci oR 95% ci oR 95% ci
Lessthangoodperceivedhealth(1/0)1
2.16*(1.47-3.19) 1.38*(1.07-1.79) 4.59*(2.97-7.10) 1.95*(1.59-2.39)
Adjustedforlifestylefactors 2.04*(1.37-3.02) 1.35*(1.04-1.76) 4.52*(2.91-7.02) 1.88*(1.53-2.31)
change 10.3% 7.9% 2.0% 7.4%
Adjustedforworkcharacteristics
2.09*(1.41-3.10) 1.35*(1.04-1.76) 4.36*(2.80-6.77) 1.87*(1.52-2.29)
change 6.0% 7.9% 6.4% 8.4%
Adjustedforlifestyle+work 1.96*(1.32-2.92) 1.32*(1.01-1.72) 4.24*(2.71-6.62) 1.78*(1.45-2.20)
change 14.7% 15.8% 6.1% 17.9%
Chronicdisease(1/0)1 1.42(0.96-2.09) 1.38*(1.10-1.73) 2.74*(1.78-4.22) 1.74*(1.45-2.09)
Adjustedforlifestylefactors 1.33(0.90-1.97) 1.36*(1.08-1.71) 2.71*(1.76-4.19) 1.67*(1.39-2.02)
change 21.4% 5.3% 1.7% 9.5%
Adjustedforworkcharacteristics
1.39(0.94-2.05) 1.36*(1.08-1.71) 2.66*(1.73-4.11) 1.69*(1.41-2.04)
change 7.1% 5.3% 4.6% 6.8%
Adjustedforlifestyle+work 1.30(0.88-1.93) 1.28*(1.01-1.62) 2.62*(1.69-4.07) 1.63*(1.35-1.96)
change 28.6% 13.2% 4.0% 14.9%
Mobilityproblems(1/0)1 1.15(0.78-1.71) 1.20(0.95-1.51) 3.32*(2.15-5.12) 1.46*(1.21-1.75)
Adjustedforlifestylefactors 1.07(0.71-1.59) 1.17(0.93-1.48) 3.35*(2.15-5.22) 1.40*(1.16-1.70)
change 53.3% 15.0% -1.3% 13.0%
Adjustedforworkcharacteristics
1.12(0.75-1.66) 1.18(0.94-1.49) 3.22*(2.08-4.99) 1.43*(1.19-1.72)
change 20.0% 10.0% 4.3% 6.5%
Adjustedforlifestyle+work 1.03(0.69-1.54) 1.15(0.91-1.46) 3.22*(2.06-5.03) 1.37*(1.13-1.65)
change 80.0% 25.0% 4.3% 19.6%
Instrumentallimitationsindailyactivities(1/0)1
1.43(0.64-3.19) 1.06(0.63-1.78) 3.19*(1.62-6.25) 1.55*(1.04-2.30)
Adjustedforlifestylefactors 1.35(0.60-3.02) 1.03(0.61-1.74) 3.19*(1.62-6.29) 1.48(0.99-2.20)
change 18.6% 50.0% 0% 12.7%
Adjustedforworkcharacteristics
1.39(0.62-3.11) 1.03(0.61-1.73) 3.00*(1.52-5.93) 1.47(0.99-2.20)
change 9.3% 50.0% 8.7% 14.6%
Adjustedforlifestyle+work 1.31(0.58-2.93) 0.99(0.59-1.69) 2.98*(1.50-5.91) 1.40(0.93-2.08)
change 18.6% 133.3% 18.7% 28.2%
1Adjustedforindividualcharacteristicsage,sexandeducationallevel

44 Chapter3
Table 3.4 shows that self-perceived poor health was a risk factor for transition to
unemployment(OR2.49),retirement(OR1.50),andworkdisability(OR5.04).Allfour
healthmeasureswereassociatedwithanyexitfromwork(ORs1.56-2.08).Alowedu-
cationallevelwasariskfactorforallthreepathwaysofnon-participation(ORs1.65-
2.80).Lifestylefactorsseemimportantforexittroughretirement.Exceptsmoking,all
lifestylefactorswereassociatedwithexitfrompaidemploymentthroughretirement
(ORs 1.23-1.40). Among work-related factors lack of job control showed increased
risksforallthreepathwaysofexit(ORs1.23-2.68).Highphysicalworkdemandswere
ariskfactoronlyforbecomingdisabled(OR1.57).Workrelatedfactorsseemedmost
importantforexitthroughworkdisabilityincomparisontootherpathways.
Table 3.5 shows that the observed associations between different measures of ill
healthandtransitionstonon-participation,afteradjustmentfor lifestyle factorsand
work characteristics. Significant odds ratios between ill health and exit from paid
employmentdecreasedby0%to10%afteradjustmentforlifestylefactors,4%to9%
afteradjustmentforworkfactors,and4%to19%afteradjustmentforlifestylefactors
andworkcharacteristicssimultaneously.Adjustmentwithlifestylefactorsandwork
related characteristics had a smaller influence on the association between ill health
andworkdisabilityleastcomparedtotheotherpathwaysofexitfrompaidemploy-
ment. Lifestyle factors and work related characteristics had a comparable influence
on the relation between ill health and exit from paid employment. In the fully ad-
justed models for each of the four health measures the lifestyle factors obesity and
problematicalcoholuseremainedsignificantinatleastoneofthemodels.Regarding
workrelatedcharacteristics,lackofjobcontrolandeffort-rewardimbalanceatwork
remainedsignificantafterfulladjustmentinatleastoneofthefourmodels.
Thepopulationattributablefractionsofaless-than-goodself-perceivedhealthfortran-
sitionintounemployment,retirement,anddisabledwere27%,9%,and61%,respectively.
Discussion
Duringatwoyearfollow-up,17%ofworkersemployedatbaselineleftpaidemploy-
ment,primarilyduetoearlyretirement.Controllingforindividualandworkrelated
characteristics,poorself-perceivedhealthwasstronglyassociatedwithexitfrompaid
employmentduetoretirement,unemployment,ordisability(OR’sfrom1.32to4.24).
In order of decreasing importance, chronic diseases, mobility problems and instru-
mentallimitationsalsoinfluencedexitfrompaidemployment,mostnotablythrough
disability.Significantassociationsbetweenillhealthandexitfrompaidemployment
changed0to19%afteradjustmentforlifestyleandworkcharacteristics.

Ch
apte
r3
TheimpactofillhealthonexitfrompaidemploymentinEuropeamongolderworkers 45
Some limitations must be taken into account in this study. First, although the at-
trition rate between baseline and follow-up was high (68%)[21], attrition was not
influencedby sex,but lower inhighagegroups.Except inGreeceandSwitzerland
therewasnorelationshipbetweenworkstatusandattrition,andthosereportinggood
orbetterhealthatbaselinehadahigherpropensitytoparticipateatthefollow-up.
Secondly,therearelargevariationsbetweenEuropeancountriesintheassociation
betweenillhealthandvariousformsofexit frompaidemployment.[5]Thesevaria-
tions may reflect differences between countries in institutional arrangements (e.g.
availability of disability benefit schemes for those with health problems), or other
factors (e.g. more or less selectivity of unemployment dependent on over-all levels
of unemployment). All analyses were therefore adjusted for country. Due to small
numbers,country-specificorregion-specificanalyseswerenotfeasible.
Third, all variables were based on self-reported data, which could have caused
reportingbias.Theproblemwithusingself-reportedhealthinanempiricalanalysisof
labourforceparticipationisthatitmaybeanendogenousexplanatoryvariable.[13,22-
23]Accordingtothejustificationhypothesisindividualsjustifytheirnon-participation
byclaimingthattheyareinillhealth.Subjectswithintentionsatbaselinetoquitpaid
employmentinthenearfuturemayalsohavebeenmorepronetoreporthighwork
demandsoralessbeneficialeffort-rewardbalanceinordertojustifytheirfutureexit
frompaidemployment.[17]
Fourth,thecurrentstudyusedafollow-upperiodoftwoyearsand,therefore,had
limiteddiscriminatorypoweranddoesnotgive insight in long-termeffectsofpoor
healthonexitfrompaidemploymentortherelevanttimewindowsfortheseeffects.
AEuropeanstudyshowed thatpoorhealthhad thestrongesteffectson leaving the
workforce in theyearbefore the transition.[8]Thus, it isexpected that the reported
influenceofillhealthonexitfrompaidemploymentisafairreflectionoftheeffectsof
illhealthonworkparticipation.
Severalstudieshaveanalyzedtheeffectsofhealthonexitfrompaidemploymentof
olderworkers.[3,5-7,9,24-27]Theresultsofthisstudysupporttheselectionhypoth-
esis,wherebypeoplewithpoorhealtharemorelikelytoquitpaidemployment.[28]
Theinfluenceoftypeofhealthmeasurediffersbyrouteofexit,butanoveralleffecton
totalexitwasconsistentlypresentforallmeasuresofillhealth.
Therelationbetweenpoorhealthandexitfrompaidemploymentmaybeexplained
byamismatchbetweenanindividual’scapacitiesandtherequirementsofthejob.[2]
Functional limitations might therefore be more important than self-perceived poor
healthforfuturelossofpaidemployment.However,theanalysesshowedthatapoor
self-perceived health was a stronger predictor for pathways of exit than functional
limitations,expressedbyeithermobilityproblemsorinstrumentallimitationsindaily
activities.Anexplanationcouldbethatself-perceivedhealthincludesmentalhealth

46 Chapter3
as well, whereas functional limitations concern primarily physical health. The high
prevalence of depression in the cohort may have contributed to the association be-
tweenself-perceivedhealthandfutureexitfrompaidemployment.
Theanalysesalsoshowedthathavingeverbeingdiagnosedwithachronicdisease
played a less profound role in exit from paid employment. This may be explained
by the fact that people diagnosed with these chronic conditions who remained in
paidemploymentareaselectionofthefittestsurvivors[29],whilethosewhoalready
leftpaidemploymentduetothesediseaseshavenotbeenincludedinoursampleas
theyhadalreadyleftpaidemploymentbeforethebaselineinvestigation.Analyseson
theroleofonsetofdiseaseduring the follow-upperiodwasnot feasibleasonly12
subjects reported that theonsetof their chronicdiseasehadbeendiagnosedduring
thefollow-upperiod.
The direct influence of ill health on exit from paid employment had odds ratios
varyingbetween1.37and5.04.Thecorrespondingpopulationattributablefractionsof
a less-than-goodself-perceivedhealthfortransitionintounemployment,retirement,
and disabled were 27%, 9%, and 61%, respectively. Under the assumption that the
observed associations represent a causal process, these associations and population
attributablefractionsindicatethatagoodhealthisanimportantfactorinmaintaining
paid employment. Based on this finding interventions aimed at prevention of exit
from paid employment should prevent or minimize ill health. Given the strong as-
sociationsatbaselinebetweenobesityandlackofleisuretimephysicalactivitywith
severalmeasuresof illhealth,healthpromotion interventionsshouldbeconsidered
that increase physical activity and support a healthy diet.[30-31] The consistent as-
sociationsatbaselinebetweenlackof jobcontrol,highphysicalworkdemands,and
effort-rewardimbalancewithseveralmeasuresofillhealth,outlinetheimportanceof
improvementofworkingconditionsandworkorganizationaswell.
Weobservedthatadjustmentwithlifestylefactorsandworkrelatedcharacteristics
showedreasonablechangesinhealthrelatedexitfrompaidemployment.Thechange
wasonlyimportantforstatisticallysignificantassociationsbecauseasmalldifference
inoddsratiocouldotherwiseresultinahighproportionofchange.Theinfluenceof
lifestylefactorsandworkcharacteristicsontheimpactofillhealthonlabourforceexit
pointsattheimportanceofprovidingworkerswithhealthproblemswithpossibilities
thatwillenablethemtocontinueworking,forexamplebyempoweringworkerswith
chronicdiseases.[32]
In the fullyadjustedmodelobesity,problematicalcoholuse, low job control, and
effort-rewardimbalanceremainedstatisticallysignificantforatleastoneofthepath-
waysofexitinatleastoneofthemodels.
Differentstudiessupporttheassociationbetweenunhealthylifestyles,suchaslack
ofphysicalactivity,obesity,andproblematicalcoholuse,andexitfrompaidemploy-

Ch
apte
r3
TheimpactofillhealthonexitfrompaidemploymentinEuropeamongolderworkers 47
ment.[5, 27, 33-35] In the fully adjusted multinominal models problematic alcohol
usewasconsistentlyassociatedwithenteringworkdisabilitywithORsvaryingfrom
1.84-1.88.Ithasbeensuggestedthatthismaybeexplainedbyproblemswithworking
times,workoutput,concentration,occupationalsafety,andcooperation,irrespective
ofhealthstatus.[8] In themultivariatemodelobesitywasassociatedwithbecoming
unemployed,(OR1.67).ThisisinagreementwithaFrenchstudythatreportedobesity
asariskfactorforunemploymentaftercontrollingforself-reportedhealth.[34]
Smokingwasnotassociatedwithearlyexit.Earlierstudieshaveshowncontradictory
results,withsignificantassociationsforsmoking[8,36-39]aswellasnon-significant
associationswithdifferentformsofexitfrompaidemployment.[34,40-41]
In the fully adjusted models lack of job control remained a significant predictor
forexitthroughretirementanddisability,whereaseffort-rewardimbalancepredicted
unemployment. Several studies have corroborated the observed direct influence of
strenuousworkingconditionsonexit frompaidemployment. [7, 27, 36, 42-43] Ina
cross-sectionalanalysisoftheSHAREsurveyatbaseline,ahighimbalancebetweenef-
fortsandrewardswasalsoassociatedwithintendedearlyretirementaftercontrolling
forpoorself-perceivedhealth[17].Hence,preventivemeasurestowardsproblematic
alcoholuse,obesity,jobcontrol,andeffort-rewardimbalancewillcontributetodimin-
ishtheoccurrenceofhealthrelatedearlyexitfrompaidemployment.
This study only focused on exit from paid employment, but poor health could
haveanadditionalimpactintermsofchangeofjobsandstalledcareers.TheHealth
andRetirementSurvey[25]showedthatworkersafter theonsetofhealthproblems
oftenchangedjobswithinseveralyears.Thismightalsobetruefortheonsetofpoor
health inearlierphasesof thecareer (youngerworkers).Poorhealthmayalsohave
adverseeffectsonperformanceatwork,asobservedintheinfluenceofpoorhealthon
sicknessabsence[44]andproductivitylossatwork.[45-46]Durationofemployment
contractcouldbeofinfluenceonsustainingpaidemployment.However,only7%of
thesubjectswithpaidemploymenthadatemporaryemploymentcontract,andthus
thisparametercouldnotbeevaluatedinthisstudy.
ThehealthstatusofolderEuropeanworkershasamajorinfluenceonthelikelihood
of sustaining paid employment. Self-perceived poor health and, to a lesser extent,
havingachronicdisease,perceivingmobilityproblemsandlimitationsseempredic-
tiveforfutureworkparticipation.Thereisconsistentevidencethatsocialinequalities
inhealthdependonwork related factorsaswellas lifestylebehaviours.[47-48]The
resultsofthisstudysuggestthatlabourmarketparticipationofolderworkerswithill
healthmaybesustainedbyinterventionsthatpromoteahealthierlifeandhealthier
workingconditions.Asexitfrompaidemploymentisoftenirreversibleatolderage,
prevention of work loss by improving worker’s health or improving ill workers’
work circumstances and lifestyles should be a key priority. Important entry-points

48 Chapter3
for policy could be lifestyle interventions, improvements of job control and effort-
reward balance, and social policies to encourage employment among older persons
withhealthproblems.
Acknowledgements
This paper uses data from release 2 of SHARE 2004 and release 1 of SHARE 2006.
The SHARE data collection has been primarily funded by the European Commis-
sion through the 5th framework programme (project QLK6-CT-2001-00360 in the
thematicprogrammeQualityofLife).AdditionalfundingcamefromtheUSNational
InstituteonAgeing(U01AG09740-13S2,P01AG005842,P01AG08291,P30AG12815,
Y1-AG-4553-01andOGHA04-064).DatacollectioninAustria(throughtheAustrian
ScienceFoundation,FWF),Belgium (through theBelgianSciencePolicyOffice)and
Switzerland (through BBW/OFES/UFES) was nationally funded. The SHARE data
collectioninIsraelwasfundedbytheUSNationalInstituteonAging(R21AG025169),
bytheGerman-IsraeliFoundationforScientificResearchandDevelopment(G.I.F.),and
bytheNationalInsuranceInstituteofIsrael.FurthersupportbytheEuropeanCom-
missionthroughthe6thframeworkprogram(projectsSHARE-I3,RII-CT-2006-062193,
andCOMPARE,CIT5-CT-2005-028857)isgratefullyacknowledged.Formethodologi-
cal details see Boersch-Supan and Juerges (2005). Mauricio Avendano is supported
by a grant from the Netherlands Organisation for Scientific Research (NWO, grant
no. 451-07-001) and a Bell Fellowship from the Harvard Center for Population and
Developmentstudies.

Ch
apte
r3
TheimpactofillhealthonexitfrompaidemploymentinEuropeamongolderworkers 49
ReFeRences
1. IlmarinenJE:Agingworkers.Occupational and environmental medicine 2001,58:546-552. 2. StattinM:Retirementongroundsofillhealth.Occupational and environmental medicine 2005,
62:135-140. 3. CaiL,KalbG:Healthstatusandlabourforceparticipation:evidencefromAustralia.Health
economics 2006,15:241-261. 4. BlackC:Workingforahealthiertomorrow.2008. 5. AlaviniaSM,BurdorfA:Unemploymentandretirementandill-health:across-sectional
analysisacrossEuropeancountries.International archives of occupational and environmental health 2008,82:39-45.
6. BartleyM:Unemploymentandillhealth:understandingtherelationship.Journal of epidemiol-ogy and community health 1994,48:333-337.
7. KarpansaloM,ManninenP,KauhanenJ,LakkaTA,SalonenJT:Perceivedhealthasapredic-torofearlyretirement.Scandinavian journal of work, environment & health 2004,30:287-292.
8. Leino-ArjasP,LiiraJ,MutanenP,MalmivaaraA,MatikainenE:Predictorsandconsequencesof unemployment among construction workers: prospective cohort study. BMJ (Clinical research ed 1999,319:600-605.
9. SchuringM,BurdorfL,KunstA,MackenbachJ:Theeffectsofillhealthonenteringandmaintainingpaidemployment:evidenceinEuropeancountries.Journal of epidemiology and community health 2007,61:597-604.
10. ThomasC,BenzevalM,StansfeldSA:Employmenttransitionsandmentalhealth:ananalysisfromtheBritishhouseholdpanelsurvey.Journal of epidemiology and community health 2005,59:243-249.
11. Borsch-SupanA,JurgesH,MackenbachJ,SiegristJ,WeberG:Health,AgeingandRetirementin Europe. First results from the survey of Healht, Ageing and Retirement in Europe.Firstresults fromthesurveyofHealth,AgeingandRetirement inEurope. .Mannheim:MannheimResearchInstitutefortheEconomicofAgeing(MEA);2005.
12. Borsch-SupanA,KartsenH,JurgesH:Anewcomprehensiveandinternationalviewonage-ing:introducingthe‘SurveyofHealth,AgeingandRetirementinEurope’..Eur J Ageing 2005,2:245-253.
13. DwyerDS,MitchellOS:Healthproblemsasdeterminantsofretirement:areself-ratedmea-suresendogenous?Journal of health economics 1999,18:173-193.
14. IdlerEL,BenyaminiY:Self-ratedhealthandmortality:areviewoftwenty-sevencommunitystudies.Journal of health and social behavior 1997,38:21-37.
15. KarasekR,BrissonC,KawakamiN,HoutmanI,BongersP,AmickB:TheJobContentQues-tionnaire(JCQ):aninstrumentforinternationallycomparativeassessmentsofpsychoso-cialjobcharacteristics.Journal of occupational health psychology 1998,3:322-355.
16. SiegristJ:Adversehealtheffectsofhigh-effort/low-rewardconditions.Journal of occupational health psychology 1996,1:27-41.
17. SiegristJ,WahrendorfM,vondemKnesebeckO,JurgesH,Borsch-SupanA:Qualityofwork,well-being,and intendedearlyretirementofolderemployees:baselineresults fromtheSHAREStudy.European journal of public health 2007,17:62-68.
18. vanOortFV,vanLentheFJ,MackenbachJP:Material,psychosocial,andbehaviouralfactorsintheexplanationofeducationalinequalitiesinmortalityinTheNetherlands.Journal of epidemiology and community health 2005,59:214-220.

50 Chapter3
19. Hennekens C, Buring B, Mayrent S: Epidemiology in Medicine. Boston: LippincottWilliams&Wilkins;1987.
20. Statisticalpackageforsocialsciences(SPSS).15edition.Chicago,IL;2006. 21. Schröder M: Attrition. In Healt, ageing and retirement in Europe (2004-2007) Starting the
longitudinal dimension. Edited by Borsch-Supan A, Brugiavini A, Jürges H, KapteynA, Mackenbach J, Siegrist J, Weber G. Mannheim: Mannheim Research Institute for theEconomicsofAging(MEA);2008:325-330.
22. BoundJ:Self-reportedversusobjectivemeasuresofhealthinretirmentmodels.Journal of Human Resources 1991,26:106-138.
23. KalwijA,VermeulenF:HealthandlabourforceparticipationofolderpeopleinEurope:whatdoobjectivehealthindicatorsaddtotheanalysis?Health economics 2008,17:619-638.
24. BaandersAN,RijkenPM,PetersL:Labourparticipationof thechronically ill.Aprofilesketch.European journal of public health 2002,12:124-130.
25. BoundJ,SchoenbaumM,StinebricknerTR,WaidmannT:Thedynamiceffectsofhealthonthelaborforcetransitionsofolderworkers.Labour economic 1999,6:179-202.
26. McDonoughP,AmickBC,3rd:Thesocialcontextofhealthselection:alongitudinalstudyofhealthandemployment.Social science & medicine (1982) 2001,53:135-145.
27. FriisK,EkholmO,HundrupYA,ObelEB,GronbiekM:Influenceofhealth,lifestyle,workingconditions,andsociodemographyonearlyretirementamongnurses:TheDanishNurseCohortStudy.Scandinavian Journal of Public Health 2007,35:23-30.
28. ArrowJO:Estimatingtheinfluenceofhealthasariskfactoronunemployment:asurvivalanalysisofemploymentdurationsforworkerssurveyedintheGermanSocio-EconomicPanel(1984-1990).Social science & medicine (1982) 1996,42:1651-1659.
29. DetailleSI,HeerkensYF,EngelsJA,vanderGuldenJW,vanDijkFJ:Commonprognosticfactorsofworkdisabilityamongemployeeswithachronicsomaticdisease:asystematicreviewofcohortstudies.Scandinavian journal of work, environment & health 2009,35:261-281.
30. DauchetL,AmouyelP,HercbergS,DallongevilleJ:Fruitandvegetableconsumptionandriskofcoronaryheartdisease:ameta-analysisofcohortstudies.J Nutr 2006,136(10):2588-2593.
31. Matson-Koffman DM, Brownstein JN, Neiner JA, Greaney ML:A site-specific literaturereview of policy and environmental interventions that promote physical activity andnutritionforcardiovascularhealth:whatworks?Am J Health Promot 2005,19:167-193.
32. VarekampI,HeutinkA,LandmanS,KoningCE,deVriesG,vanDijkFJ:FacilitatingEm-powerment in Employees with Chronic Disease: QualitativeAnalysis of the Process ofChange.Journal of occupational rehabilitation 2009.
33. Biering-SorensenF,LundJ,HoydalsmoOJ,DarreEM,DeisA,KrygerP,MullerCF:Riskindicatorsofdisabilitypension.A15yearfollow-upstudy.Dan Med Bull 1999,46:258-262.
34. JusotF,KhlatM,RochereauT,SermeC:Joblossfrompoorhealth,smokingandobesity:anationalprospectivesurvey inFrance. Journal of epidemiology and community health 2008,62:332-337.
35. RissanenA,HeliovaaraM,KnektP,ReunanenA,AromaaA,MaatelaJ:Riskofdisabilityandmortalityduetooverweight inaFinnishpopulation.BMJ (Clinical research ed 1990,301:835-837.
36. EriksenW,NatvigB,RutleO,BruusgaardD:Smokingasapredictoroflong-termworkdisabilityinphysicallyactiveandinactivepeople.Occup Med (Lond) 1998,48:315-320.

Ch
apte
r3
TheimpactofillhealthonexitfrompaidemploymentinEuropeamongolderworkers 51
37. LiiraJ,Leino-ArjasP:Predictorsandconsequencesofunemploymentinconstructionandforestworkduringa5-yearfollow-up.Scandinavian journal of work, environment & health 1999,25:42-49.
38. LundT,CsonkaA:Riskfactorsinhealth,workenvironment,smokingstatus,andorganiza-tionalcontextforworkdisability.Am J Ind Med 2003,44:492-501.
39. RothenbacherD,ArndtV,FraisseE,ZschenderleinB,FliednerTM,BrennerH:Earlyretire-mentdue topermanentdisability inrelation tosmoking inworkersof theconstructionindustry.J Occup Environ Med 1998,40:63-68.
40. HaahrJP,FrostP,AndersenJH:Predictorsofhealthrelatedjobloss:atwo-yearfollow-upstudy inageneralworkingpopulation. Journal of occupational rehabilitation 2007,17:581-592.
41. LundT,IversenL,PoulsenKB:Workenvironmentfactors,health,lifestyleandmaritalstatusaspredictorsofjobchangeandearlyretirementinphysicallyheavyoccupations.Am J Ind Med 2001,40:161-169.
42. BlekesauneM,SolemPE:Workingconditionsandearlyretirement.Aprospectivestudyofretirementbehavior.Research on aging 2005,27(1):3-30.
43. SolomonC,PooleJ,PalmerKT,CoggonD:Health-relatedjobloss:findingsfromacommu-nity-basedsurvey.Occupational and environmental medicine 2007,64:144-149.
44. DuijtsSF,KantI,SwaenGM,vandenBrandtPA,ZeegersMP:Ameta-analysisofobserva-tionalstudiesidentifiespredictorsofsicknessabsence.Journal of clinical epidemiology 2007,60:1105-1115.
45. MeerdingWJ,WIJ,KoopmanschapMA,SeverensJL,BurdorfA:Healthproblemsleadtoconsiderable productivity loss at work among workers with high physical load jobs.Journal of clinical epidemiology 2005,58:517-523.
46. SchultzAB,EdingtonDW:Employeehealthandpresenteeism:asystematicreview.Journal of occupational rehabilitation 2007,17:547-579.
47. VahteraJ,VirtanenP,KivimakiM,PenttiJ:Workplaceasanoriginofhealthinequalities.Journal of epidemiology and community health 1999,53:399-407.
48. KuperH,MarmotM:Jobstrain,jobdemands,decisionlatitude,andriskofcoronaryheartdisease within the Whitehall II study. Journal of epidemiology and community health 2003,57:147-153.


4The effects of ill health on entering
and maintaining paid employment:
evidence in european countries
SchuringM,BurdorfA,KunstAE,MackenbachJP.
Journal of Epidemiology and Community Health2007,61:597-604.

54 Chapter4
absTRacT
objectives:Toexaminetheeffectsofillhealthonselectionintopaidemploymentin
Europeancountries.
methods:Fiveannualwaves(1994-8)oftheEuropeanCommunityHouseholdPanel
wereusedtoselecttwopopulations:(1)4446subjectsunemployedforatleast2years,
ofwhich1590(36%)subjectsfoundemploymentinthenextyear,and(2)57436sub-
jectsemployedforatleast2years,ofwhich6191(11%)subjectslefttheworkforcein
thenextyearbecauseofunemployment,(early)retirement,orhavingtotakecareof
household.Theinfluenceofaperceivedpoorhealthandachronichealthproblemon
employmenttransitionswasstudiedusinglogisticregressionanalysis.
Results:An interactionbetweenhealthandsexwasobserved,withwomen inpoor
health(oddsratio(OR)0.4),meninapoorhealth(OR0.6),andwomen(OR0.6)hav-
ing lesschance toenterpaidemployment thanmen ingoodhealth.Subjectswitha
poorhealthandlow/intermediateeducationhadthehighestriskofunemploymentor
(early)retirement.Takingcareofthehouseholdwasonlyinfluencedbyhealthamong
unmarried women. In most European countries, a poor health or a chronic health
problem predicted staying or becoming unemployed and the effects of health were
strongerwithalowernationalunemploymentlevel.
conclusion: In most European countries, socio-economic inequalities in ill health
were an important determinant for entering and maintaining paid employment. In
public health measures for health equity, it is of paramount importance to include
peoplewithpoorhealthinthelabourmarket.

Ch
apte
r4
Theeffectsofillhealthonenteringandmaintainingpaidemployment:evidenceinEuropeancountries 55
inTRoDucTion
Thepresenceofsocioeconomicinequalitiesinhealthhasbeenwidelyacknowledged.
[1] Lower education, unskilled labour and low income are associated with higher
mortalityandmorbidity.[2]Labourforceparticipationisanimportantdeterminantof
health inequalities,asdemonstratedbyahigherprevalenceof illnessanddisability
[3,4]andahighermortalityamongunemployedpeople.[5]Theassociationbetween
health and employment is bi-directional: unemployment may cause poor health
(causation hypothesis) and poor health may increase the probability of becoming
unemployed(selectionhypothesis)[6,7]
ThecausationmechanismisillustratedamongBritishhouseholds,whereunemploy-
menthadastrongeffectontheincidenceofanylimitingillnessandemploymentwas
relatedtorecoveryfromtheseillnesses.[6]Areviewoflongitudinalstudiesconcluded
that loss of employment affected mental health, but also that gaining employment
improvedmentalhealth.[8]
Thereisalsoevidencefortheselectionhypothesis.Amonglong-termunemployed
Norwegians,mentalmorbiditywasstronglyassociatedwithareductioninobtaininga
paidjob.[9]InaBritishstudy,healthierpeoplewerefoundmorelikelytogainemploy-
ment than people with minor psychiatric morbidity.[7] Ill health may also increase
otherformsofnon-employment,suchasearlyretirementandhavingtostayinghome
totakecareofthefamily.[7,10]InaFinnishcohortofmen,self-assessedpoorhealth
wasastrongpredictorofbothdisabilityaswellasnon-illnessbasedearlyretirement.
[11]
The associations between health and employment will not be similar across all
socio-economic groups, as age, education, sex, marital status or household income
may influence the social context of health and employment status.[12][13] The con-
sequencesofillhealthforthelikelihoodofbecomingorstayingunemploymentmay
dependonsocialandlabourmarketpolicies,whichvaryacrossEuropeancountries.
Forexample,strikingdifferencesinaccesstobenefits,suchasearlyretirementordis-
abilitypension,fordisabledpeoplehavebeendescribedwithintheEuropeanUnion.
In the Netherlands, < 10% of disabled people have labou as their main source of
incomewhereasinSwedenthisproportionamountstoover50%.[14]
Against thisbackground, theaimof thisstudywasto investigate theeffectsof ill
healthontheselectionprocessintopaidemploymentandwhethertheseeffectsinter-
actedwithsocioeconomicgroups.Thesecondaryaimofthestudywastoinvestigate
whetherobservedassociationsbetweenillhealthandemploymenttransitionsdiffered
amongEuropeancountries.

56 Chapter4
meTHoDs
Studypopulation
Thedatawerederivedfromthefirstfivewaves(1994-8)oftheEuropeanCommunity
Household (ECHP).[15] The ECHP is a social survey among member states of the
EuropeanUnionwithalongitudinaldesigntodescribethesocialdynamicsinEurope.
DatawerecollectedbyNationalInstitutesforStatisticsorresearchcenters,whiledata
checks, weightings and imputations were done centrally by the Statistical Office of
the European Communities (Eurostat). All surveys were based on a non-stratified
randomsamplingdesignamongallnationalprivatehouseholds.Allmembersofthe
householdwereindividuallyinterviewed.Thedatacollectionwascarriedoutinmost
countriesbypaper-and-pencil interviewing,butinfourcountries(UnitedKingdom,
TheNetherlands,Portugal,andGreece)bycomputer-assistedpersonalinterviewing.
Theoverallhouseholdresponserateinthefirstwavewas72%,butvariedconsiderably
amongcountries.Theresponserates in laterwavesoftheECHPstudywerehigher.
Adetaileddescriptionofsamplingproceduresandresponserateshasbeenpublished
elsewhere.[16,17]
For the purpose of this study, subjects aged between 16-65 years were selected,
with available information on employment status and health status during at least
three consecutive annual measurements, whereby the employment status remained
unchangedinthefirstandsecondmeasurementandapossibleemploymenttransition
hadoccurredinthethirdmeasurement.Althoughemploymentstatuswasascertained
annually,weconsideredthisstatusasrepresentativeforthewholeyearprecedingthe
administrationofthequestionnaire.Thisprocedureresultedinacohortwith3years
offollow-up,withtwoconsecutiveyearsbeforeapossibleemploymenttransition.For
asmallpartofthecohort,informationwasalsoavailableinthethirdandfourthan-
nualmeasurementbeforetheyearofemploymenttransition.Thus,foreverysubject,
anemploymenttransitionwaspossibleinagivenyearandlabourstatuswasregarded
asconstantinthe2-4yearsbeforepossibleemploymenttransition.
Self-defined employment status was classified into four mutually exclusive cat-
egories: employed (paid employment, paid apprenticeship or self-employment),
unemployment,retiredortakingcareofhousehold.[15]Employmentwasdefinedas
workinginajobforatleast15h/week.Subjectsworking<15h/weekwereautomati-
callyclassified intothecategoriesunemployed,retired, takingcareofhousehold, in
militaryservice,followingeducationoreconomicallyinactive.Unemployedsubjects
were defined as those people who worked <15 h/week and who considered them-
selves as being unemployed. Subjects who classified themselves into the last three
categorieswerenotselectedforanalysisinthisstudy,henceexcludingeconomically

Ch
apte
r4
Theeffectsofillhealthonenteringandmaintainingpaidemployment:evidenceinEuropeancountries 57
inactivepeoplewhoarewithoutworkandwhodonotwishtoconsiderthemselvesas
unemployed.Subjectswithadisabilitypensionasanotherformofnon-employment
were also excluded from the analysis, as poor health is an essential requirement to
qualifyforadisabilitypension.However,disabledpersonswithapaidjobfor>15h/
weekwereincludedinthecategory“employed”.
Two different populations were defined to study employment transitions. The
first studypopulation included4446peoplewhowereunemployed forat least two
consecutiveyears,ofwhich1590(36%)peopleenteredtheworkforceduringthelast
yearoffollow-up.Thesecondstudypopulationconsistedof57436workerswhowere
employedforatleasttwoconsecutiveyears,ofwhich6191(11%)peopleleftthework-
forceinthelastyearoffollow-upduetounemployment(n=3000),retirement(n=2017)
orhavingtotakecareofthehousehold(n=1174).
Questionnaire
Thequestionnairecomprisedquestionsonindividualandhouseholdcharacteristics,
perceived general health, chronic health problem, and employment status. Indi-
vidualcharacteristics includedage,sex,educationandpersonal income.Household
characteristics included marital status, the presence of children aged ≤12 years and
household income. Subjects were divided into three groups according to their level
ofeducationalattainmentonthebasisoftheInternationalStandardClassificationof
Education (ISCED).[18] Informationonmarital statuswasused tocomparesubjects
marriedorlivingwithothers.Householdandpersonalincomewerecategorizedinto
three percentile groups (<25th centile, 25-75th centile and >75th centile), relative to
theincomedistributionofthestudysampleineachcountry.Ifthepersonalincomeof
asubjectwas≥75%ofthehouseholdincome,thesubjectwasdefinedasbreadwinner
withinthehousehold.
Twomeasuresofself-reportedhealthwereused.First,subjectswereaskedtorate
their own general health on a five-point scale, ranging from “very good”, “good”,
“fair”and“bad”to“verybad”.Thosereportinglessthan“goodhealth”weredefined
ashavingapoorhealth.[19]Second,subjectswereaskedwhethertheyhadanychronic
physicalormentalhealthproblem, illnessordisability (yes/no).Anaffirmativean-
swerwasclassifiedaschronichealthproblem[15]
Statisticalmethods
Logisticregressionanalysiswasperformedtostudytheimpactofpoorhealthanda
chronichealthproblemonemploymentstatus,adjustedforcountryandpersonaland
householdcharacteristics.Thefirststepintheanalysiswastoestablishtheassociations

58 Chapter4
betweenpoorhealthandemploymentstatus,includingcountryasacategoricalvariable
(fixedfactor)toadjustfortheeffectofcountryontheassociationbetweenpoorhealth
and employment status. In the second step, other independent socio-demographic
variableswereincludedinthemodelbyastep-forwardprocedure.Thevariablewith
thestrongestassociationwithemploymentstatuswasputinthemodelfirst,followed
bythenextstrongest,andsoon.Variableswithasignificantreductionintheoverall
scaleddevianceofthemodelwereretainedinthemultivariatemodel.Inthethirdstep,
interactions between poor health and significant socio-demographic variables were
investigated for their influence on the overall fit of the model. The interaction with
thestrongesteffectonthescaleddevianceofthemodelwasincludedinthefinalmul-
tivariatemodel.Thus, interactiontermswithouthealthwerenotconsidered,thereby
excludingpossibleinteractionsamongsocio-demographicvariables.Forallanalyses,
fourdifferenttimewindowswereapplied,investigatingtheeffectsoftheindependent
variablesmeasured1,2,3,and4yearsbeforetheemploymenttransition.Allstatistical
modelswerebasedonthe(varying)numberofpeopleavailableforthethreedifferent
measuresofemploymentstatus,withoutweighingtheregressioncoefficientaccording
toattritionrateinthecountrysampleorpopulationsizeineachcountry.
Fortheanalysisontransitionfromemploymentto(early)retirement,onlysubjects
in the age group 55-65 years were used, as occurrence of retirement among those
aged≤54wasverylow.Owingtothisselection,agewasnotincludedinthisanalysis.
Likewise,theanalysisontransitionfromemploymenttohouseholdwasrestrictedto
women,asonlyveryfewmenclassifiedthemselvesastakingcareof thehousehold
withouthavinganypaidjob.
Thevariationamongcountriesintheassociationbetweenpoorhealthandemploy-
ment statuswas investigatedby introductionof the interaction termofpoorhealth
andcountry ineachmultivariatemodel.This interactiontermwasusedtoestimate
thecountry-specificassociationsforpoorhealthandemploymentstatus(expressedby
oddsratios (ORs)),adjustedforrelevantsocio-demographiccovariates.Allanalyses
wererepeatedwiththepresenceofachronichealthproblemasoutcomemeasure.The
analyseswerecarriedoutwiththestatisticalpackageSASV.8.2.
ResuLTs
Thebackgroundcharacteristicsofbothpopulationsarepresented inTable4.1.Both
health measures were strongly associated with almost 50% of all persons reporting
aperceivedpoorhealth,alsoindicatingthepresenceofachronicphysicalormental
healthproblem,illnessordisability.Illhealth,sex,education,havingyoungchildren
inhouseholdandbeingabreadwinnerwereassociatedwithemploymenttransition.

Ch
apte
r4
Theeffectsofillhealthonenteringandmaintainingpaidemployment:evidenceinEuropeancountries 59
Table 4.1 BackgroundcharacteristicsofsubjectsfromtheEuropeanHouseholdPanelSurveyintheyearofanemploymenttransitionafteratleasttwoconsecutiveyearsofunemploymentoremployment
characteristic
Subjectswithatleast2yearsofunemploymentwhoremainedunemployed(n=2856)orenteredemployment(n=1590)inthe3rdyear
Subjectswithatleast2yearsofemploymentwhoremainedemployed(n=51245)orlefttheworkforce(n=6191)inthe3rdyear
unemployed became employed employed Left workforce
n (%) n (%) n (%) n (%)
Age(years)16–2425–4445–5455–65
758(27)1241(45)463(17)291(11)
586(38)*785(49)170(11)38(2)*
5610(11)29344(60)10764(22)3240(7)
736(13)2200(38)*1102(19)1805(31)*
Sex(men) 1315(46) 886(56)* 31642(62) 3216(52)*
Married(yes) 1333(47) 700(44) 36347(71) 4399(71)
EducationallevelHighIntermediateLow
263(10)956(25)1507(55)
192(13)595(39)732(48)*
13297(27)18838(38)17594(35)
896(15)*2029(34)2982(51)*
Children<12years 800(28) 498(31)* 17797(35) 1674(27)*
Breadwinner 481(17) 251(16) 16341(32) 1585(26)*
Perceivedpoorhealth 968(34) 327(21)* 12437(24) 2311(37)*
Chronichealthproblem 662(23) 200(13)* 8100(16) 1544(25)*
*Waldχ2–test,P<0.05
40
45
50
55
60
65
70
75
80
85
4 3 2 1 *Years before employment transition
Perc
enta
ge o
f per
sons
with
go
od p
erce
ived
hea
lth (%
)
(Re)employed (n=183)Left workforce to take care of household (n=232)Left workforce due to unemployment (n=463)Continuously employed (n=30763)Continuously unemployed (n=850)Left workforce due to retirement (n=538)
Figure 4.1 ProportionofsubjectswithaperceivedgoodhealthamongrespondentswhocompletedallfivewavesoftheEuropeanHouseholdPanelSurveyandanemploymenttransitioninthelastyearofthesurvey
40
45
50
55
60
65
70
75
80
85
4 3 2 1 *Years before employment transition
Perc
enta
ge o
f per
sons
with
go
od p
erce
ived
hea
lth (%
)
(Re)employed (n=183)Left workforce to take care of household (n=232)Left workforce due to unemployment (n=463)Continuously employed (n=30763)Continuously unemployed (n=850)Left workforce due to retirement (n=538)

60 Chapter4
Figure4.1showsthatinallgroupstheproportionofpeopleingoodhealthdecreased
intheperiod1994-8.Theproportionofpeopleingoodhealthwasconsistentlyhigher
amongthosewhowereemployedorbecameemployedthanamongpeoplewhowere
notemployedorlefttheworkforce.
Table 4.2 shows that an interaction was observed between health status and sex.
Womenwithpoorhealth,menwithpoorhealthandwomenwithgoodhealthwere
significantlymorelikelytoremainunemployedinthenextyearthanmenwithgood
health.Thisinteractionwaspresentupto4yearsbeforeenteringpaidemployment.
Apositiveimpacton(re)employmentwasobservedforpeoplebeingmarried,being
ofyoungerage,havinghighereducationandhavinghigherpersonalincome.Beinga
breadwinner(OR0.9,95%CI0.8-1.2)andhavingchildren<12yearsinthehousehold
(OR1.0,95%CI0.8-1.2)werenotassociatedwithenteringpaidemployment.Chronic
healthproblemsshowedverysimilarresultsforalltimewindows(resultsnotshown).
Table4.3showsthatpoorhealthwasmoreimportantamongthosewithhigheredu-
cationthanamongthosewith lowereducationbecomingunemployed.Theeffectof
poorhealthwithinthestrataofintermediateandhighereducationbecamelessstrong
Table 4.2 Multivariatemodelswithdifferenttimewindowsofsignificantdeterminantsof(re)employmentamongsubjectsfromtheEuropeanHouseholdPanelSurveywithatleast2consecutivepreviousyearsofunemploymentbeforeenteringpaidemployment
Determinant
years before entering paid employment
1 yearoR (95% ci)
2 yearsoR (95% ci)
3 yearsoR (95% ci)
4 yearsoR (95% ci)
NstayedunemployedNenteredemployment
26341481
26461483
1444609
792174
Poorhealth-Women†
Goodhealth-WomenPoorhealth-MenGoodhealth-Men
0.4(0.3-0.5)*0.6(0.5-0.7)*0.6(0.4-0.7)*1
0.4(0.3-0.5)*0.6(0.5-0.7)*0.6(0.5-0.7)*1
0.6(0.4-0.8)*0.5(0.4-0.7)*0.6(0.4-0.8)*1
0.5(0.3-0.9)*0.7(0.5-1.0)*0.6(0.4-1.1)1
Age(years)16-2425-4445-5455-64
8.1(5.4-12.2)*5.7(3.9-8.3)*3.3(2.2-5.0)*1
9.0(6.0-13.5)*6.0(4.2-8.8)*3.4(2.3-5.0)*1
11.0(5.2-23.4)*8.3(4.1-17.0)*4.7(2.2-9.9)*1
4.7(1.4-14.9)*3.6(1.2-10.8)*1.7(0.5-5.7)1
Married 1.4(1.2-1.7)* 1.4(1.2-1.6)* 1.4(1.1-1.8)* 1.6(1.0-2.6)*
EducationallevelHighIntermediateLow
1.7(1.3-2.1)*1.6(1.3-1.8)*1
1.6(1.3-2.0)*1.5(1.3-1.8)*1
2.1(1.5-2.9)*1.6(1.3-2.0)*1
2.6(1.5-4.7)*1.9(1.2-2.8)*1
Personalincome>75thcentile25-75thcentile<25thcentile
1.6(1.3-1.9)*1.5(1.2-1.7)*1
1.9(1.6-2.3)*1.4(1.2-1.6)*1
1.8(1.4-2.5)*1.4(1.1-1.8)*1
1.4(0.9-2.3)1.0(0.6-1.6)1
*Waldχ2-test,P<0.05.†significantinteraction.

Ch
apte
r4
Theeffectsofillhealthonenteringandmaintainingpaidemployment:evidenceinEuropeancountries 61
inmoredistantyears. Job losswasalso influencedbyolderage,notbeingmarried,
havingchildren<12years (asper thepreviousyear)andhaving lowerpersonal in-
come.Beingbreadwinner(OR1.0,95%CI0.9-1.1)ormen(OR1.1,95%CI1.0-1.2)did
notinfluenceunemployment.Theimpactofchronichealthproblemswasremarkably
similartoaperceivedpoorhealth(resultsnotshown).
Among subjects aged ≥55 years, those with a poor health had a higher chance of
retiring the next year than subjects with a good health (table 4.4). Among highly
educatedsubjects,thisassociationwasnotobservedforthehealthstatus2,3,and4
yearsbeforetheyearofretirement.Beingmarriedseemedtoreducethelikelihoodof
retirement.Breadwinner,sex,andpersonalincomeallhadoddsratiosclosetounity.
Theinfluenceofachronichealthproblemon(early)retirementcloselymirroredthe
resultsofaperceivedpoorhealth.
Table4.5demonstratesthattakingcareofthehouseholdwasinfluencedbyhealth
amongunmarriedwomen(OR=1.6)butnotamongmarriedwomen.Thisassociation
wasonlyobservedinearlieryears.Leavingtheworkforcetotakecareofthehouse-
holdwasconsistentlyassociatedwitholderage,havingyoungchildren,lowpersonal
income,andloweducationallevel.
Table 4.3 MultivariatemodelswithdifferenttimewindowsofsignificantdeterminantsofbecomingunemployedamongsubjectsfromtheEuropeanHouseholdPanelSurveywithatleast2consecutivepreviousyearsofemploymentbeforebecomingunemployed
Determinant
years before becoming unemployed
1 yearoR (95% ci)
2 yearsoR (95% ci)
3 yearsoR (95% ci)
4 yearsoR (95% ci)
N(stayedemployed)N(becameunemployed)
473782700
366101629
30706515
28780427
Poorhealth-loweducation†
Goodhealth-loweducationPoorhealth-intermediateeducationGoodhealth-intermediateeducationPoorhealth-higheducationGoodhealth-higheducation
2.2(1.8-2.6)*1.9(1.7-2.2)*2.4(2.0-2.9)*1.4(1.2-1.6)*2.1(1.6-2.6)*1
2.5(2.0-3.1)*1.9(1.6-2.3)*2.1(1.7-2.6)*1.5(1.2-1.8)*1.6(1.2-2.2)*1
2.3(1.6-3.4)*2.2(1.6-3.1)*2.5(1.7-3.7)*1.6(1.2-2.3)*1.4(0.8-2.4)*1
2.5(1.6-3.9)*2.2(1.5-3.1)*2.3(1.5-3.5)*1.8(1.3-2.6)*1.2(0.7-2.3)1
Age(years)16-2425-4445-5455-64
1.0(0.9-1.3)0.8(0.7-0.9)*0.8(0.7-0.9)*1
1.0(0.8-1.3)0.8(0.6-1.0)*0.8(0.6-1.0)1
0.9(0.6-1.4)0.8(0.5-1.1)0.9(0.6-1.3)1
0.9(0.6-1.4)0.7(0.5-1.0)0.8(0.5-1.2)1
Married 0.7(0.6-0.7)* 0.7(0.6-0.8)* 0.7(0.6-0.9)* 0.8(0.6-0.9)*
Children<12years 1.2(1.1-1.3)* 1.1(1.0-1.3) 1.1(0.9-1.4) n/a
Personalincome>75thcentile25-75thcentile<25thcentile
0.2(0.2-0.3)*0.5(0.4-0.5)*1
0.2(0.2-0.3)*0.4(0.4-0.5)*1
0.3(0.3-0.5)*0.5(0.4-0.6)*1
0.4(0.3-0.6)*0.5(0.4-0.7)*1
n/a=notavailableindatacollection.*Waldχ2-test,P<0.05.†significantinteraction.

62 Chapter4
In table 4.6, the country-specific associations are presented for 11 countries (Lux-
embourgnotincludedasassociationswerenotestimabletherebecauseofverysmall
numbers).In9of11Europeancountries,aperceivedpoorhealthwasariskfactorfor
staying unemployed, varying from OR=0.2 in Denmark to OR=0.7 in Germany and
France,althoughthisassociationreachedtheconventionallevelofstatisticalsignifi-
canceinonlyfourcountries.In7of11countriesaperceivedpoorhealthincreasedthe
riskofbecomingunemployed,varyingfromOR=1.2inFrancetoOR=2.7intheNeth-
erlands.Amongolderworkers,aperceivedpoorhealthraisedthelikelihoodofretire-
mentinninecountries,withsmalleffectsobservedinFranceandtheUK(OR=1.1)and
significantlargeeffectsinBelgium(OR=2.6)andGermany(OR=2.6).Forpoorhealth
andachronichealthproblem,ingeneral,comparableassociationswerefound,with
theexceptionoftwocountries.InItaly,achronichealthproblempredictedremaining
unemployed (OR=0.4), but poor health had no discernable impact (OR=1.0). In the
Netherlands,achronichealthproblemseemedtoincreasethelikelihoodofretirement
amongolderworkers(OR=1.7),whereasapoorhealthdecreasedretirement(OR=0.6),
althoughbothassociationswerenotstatisticallysignificant.Figure4.2illustratesthat
a lower unemployment rate at national level in 1998 was associated with larger ef-
fectsofpoorhealthonnotenteringemployment(regressioncoefficient0.06,R2=0.46,
p=0.02)andlargereffectsofpoorhealthonbecomingunemployed(regressioncoeffi-
cient-0.10,R2=0.27,p=0.10).Thistrendovercountrieswasnotobservedfortheeffects
ofpoorhealthonretirementortakingcareofhousehold.
Table 4.4 Multivariatemodelswithdifferenttimewindowsofsignificantdeterminantsofretirementamongworkersaged55-65yearsintheEuropeanHouseholdPanelSurveywithatleast2consecutivepreviousyearsofemploymentbeforeretirement
Determinant
years before retirement
1 yearoR (95% ci)
2 yearsoR (95% ci)
3 yearsoR (95% ci)
4 yearsoR (95% ci)
N(stayedemployed)N(becameretired)
31401374
31671384
2097806
1778345
Poorhealth-loweducation†
Goodhealth-loweducationPoorhealth-intermediateeducationGoodhealth-intermediateeducationPoorhealth-higheducationGoodhealth-higheducation
1.7(1.4-2.2)*1.3(1.0-1.6)*2.0(1.6-2.7)*1.4(1.1-1.6)*1.5(1.0-2.2)*1
1.7(1.3-2.1)*1.2(1.0-1.5)1.8(1.3-2.4)*1.3(1.1-1.7)*1.1(0.8-1.6)1
1.4(1.0-1.9)*1.2(0.9-1.5)1.7(1.2-2.6)*1.2(0.8-1.7)0.8(0.5-1.3)1
1.6(1.0-2.4)*1.2(0.8-1.8)1.7(1.0-2.9)*1.1(0.7-1.7)*1.1(0.6-2.1)1
Married 0.8(0.7-1.0)* 0.8(0.7-1.0)* 0.8(0.7-1.0) 0.9(0.6-1.2)
*Waldχ2-test,P<0.05.†significantinteraction.

Ch
apte
r4
Theeffectsofillhealthonenteringandmaintainingpaidemployment:evidenceinEuropeancountries 63
Discussion
Thisstudyshowsthattheeffectsofhealthontransitionsbetweenpaidemploymentand
various formsofnon-employmentwere influencedbysocio-demographicvariables.
Apoorhealthwasariskfactorforremainingunemployedamongmen,buthadless
effectamongwomen.Apoorhealthwasalsoariskfactorforbecomingunemployed
or retiring, especially among highly educated workers. Finally, among women the
transitionfromemploymentintotakingcareofahouseholdwasinfluencedbyapoor
healthonlyamongwomennotmarried.InmostEuropeancountries,poorhealthand
achronichealthproblemwereriskfactorsfornotenteringtheworkforceorbecoming
unemployed,butlargedifferencesamongcountrieswereobservedthatcouldpartly
beexplainedbytheunemploymentrateatnationallevel.
TheseconclusionsarebasedontheEuropeanHouseholdPanelSurvey.Anobvious
disadvantageofthecurrentanalysisistherestrictiontotwomeasuresofself-reported
health.Bothmeasuresofhealthwerestronglycorrelated,asonewouldexpect.Unfor-
Table 4.5 MultivariatemodelswithdifferenttimewindowsofsignificantdeterminantsofleavingemploymentforhouseholdcareamongwomenintheEuropeanHouseholdPanelSurveywithatleast2consecutivepreviousyearsofemploymentbeforeleavingtheworkforcetotakecareofhousehold
years before leaving the workforce to take care of household
1 yearoR (95% ci)
2 yearsoR (95% ci)
3 yearsoR (95% ci)
4 yearsoR (95% ci)
N(stayedemployed)N(household)
181001000
13818608
11351229
10419193
Poorhealth-marriedGoodhealth-marriedPoorhealth-notmarriedGoodHealth-notmarried
2.6(2.0-3.3)*2.4(2.0-3.0)*1.6(1.1-2.3)*1
2.1(1.5-2.8)*1.9(1.4-2.4)*1.3(0.9-2.0)1
1.7(1.1-2.7)*1.7(1.1-2.6)*0.7(0.3-1.4)1
1.3(0.8-2.2)1.7(1.1-2.5)*0.9(0.4-1.7)1
Age16-2425-4445-54
0.5(0.4-0.7)*0.4(0.3-0.5)*0.4(0.3-0.5)*
0.4(0.3-0.7)*0.4(0.3-0.5)*0.4(0.3-0.6)*
0.6(0.3-1.2)0.4(0.3-0.7)*0.5(0.3-0.9)*
0.6(0.3-1.2)0.4(0.2-0.6)*0.4(0.2-0.7)*
EducationallevelHighIntermediateLow
0.6(0.5-0.8)*0.8(0.7-1.0)*1
0.7(0.5-0.9)*0.9(0.7-1.1)1
0.8(0.5-1.2)0.9(0.7-1.3)1
0.7(0.5-1.2)0.9(0.6-1.3)1
Children<12years 1.9(1.6-2.2)* 1.6(1.3-1.9)* 1.1(0.8-1.5) n/a
Personalincome>75thcentile25-75thcentile<25thcentile
0.3(0.2-0.4)*0.4(0.3-0.4)*1
0.2(0.2-0.4)*0.4(0.3-0.5)*1
0.4(0.2-0.6)*0.4(0.3-0.6)*1
0.3(0.2-0.6)*0.6(0.4-0.8)*1
n/a=notavailableindatacollection.*Waldχ2-test,P<0.05.†significantinteraction

64 Chapter4
tunately,noinformationwasavailableonself-reportedordiagnosedspecificdiseases
and,hence,itwasnotpossibletoevaluatewhichparticulardiseaseslargelyexplained
theroleofhealthinenteringorleavingtheworkforce.Theordinalmeasurementand
subsequentdichotomisingofself-perceivedhealthmayhampercomparabilityacross
countriesand,indeedinourstudypopulations,theprevalenceofpoorhealthvaried
fromabout8%inGreeceandIrelandtoover40%inPortugalandGermany.However,
themagnitudeoftheprevalencewasnotassociatedwiththeobservedORsforpoor
health.Inaddition,whenusingamorestringentcut-offpointforapoorhealth(only
Table 4.6 InfluenceofperceivedpoorhealthandchronichealthproblemsinthepreviousyearonemploymenttransitionsinthenextyearamongsubjectsfromtheEuropeanHouseholdPanelSurveyin11Europeancountries
country
From unemployed to employed
From employed to unemployed
From employed to retired (> 55 year)
n oR n oR n oR
GermanyPerceivedpoorhealthChronichealthproblem
4830.7(0.5-1.1)0.9(0.5-1.3)
95302.6(2.1-3.8)*2.2(1.8-2.7)*
7962.6(1.8-3.8)*2.4(1.7-3.4)*
DenmarkPerceivedpoorhealthChronichealthproblem
1300.2(0.1-0.7)*0.5(0.2-1.2)
25642.0(1.3-3.2)*1.2(0.8-1.8)
2231.6(0.8-3.0)1.1(0.7-2.0)
NetherlandsPerceivedpoorhealthChronichealthproblem
3440.3(0.2-0.6)*0.4(0.3-0.8)*
38042.7(1.8-4.0)*2.8(198-4.3)*
1300.6(0.1-5.8)1.7(0.3-10.8)
BelgiumPerceivedpoorhealthChronichealthproblem
2800.6(0.2-1.3)0.3(0.1-1.4)
26991.6(1.0-2.6)1.3(0.6-2.5)
1342.6(1.1-6.3)*1.5(0.6-4.4)
FrancePerceivedpoorhealthChronichealthproblem
4850.7(0.4-1.1)0.8(0.5-1.4)
56091.2(1.0-1.6)1.2(0.9-1.7)
3701.1(0.7-1.7)1.5(0.9-2.6)
UnitedKingdomPerceivedpoorhealthChronichealthproblem
2290.4(0.2-0.8)*0.4(0.2-0.8)*
71091.8(1.3-2.6)*1.2(0.9-1.8)
6051.1(0.7-1.8)1.5(1.0-2.3)
IrelandPerceivedpoorhealthChronichealthproblem
2600.6(0.3-1.3)0.7(0.3-1.6)
28600.6(0.2-1.5)0.8(0.4-1.7)
2991.4(0.7-2.7)1.4(0.7-2.7)
ItalyPerceivedpoorhealthChronichealthproblem
8911.0(0.7-1.5)0.4(0.2-0.9)*
62381.0(0.7-1.3)0.9(0.5-1.6)
5540.8(0.6-1.1)0.9(0.5-1.5)
GreecePerceivedpoorhealthChronichealthproblem
3851.2(0.5-2.5)0.7(0.2-2.1)
37401.3(0.8-2.0)1.0(0.6-1.8)
4891.3(0.9-2.0)0.9(0.6-1.6)
SpainPerceivedpoorhealthChronichealthproblem
7840.6(0.4-0.9)*0.4(0.3-0.7)*
48970.9(0.7-1.2)1.1(0.8-1.4)
4101.5(1.0-2.4)*1.3(0.8-2.0)
PortugalPerceivedpoorhealthChronichealthproblem
1910.5(0.3-1.0)*0.9(0.4-2.1)
48511.0(0.7-1.2)1.5(1.1-2.0)*
6691.5(1.0-2.4)1.8(1.2-2.7)*
*Waldχ2-test,P<0.05,adjustedforage,sex,maritalstatus,education,andpersonalincome.

Ch
apte
r4
Theeffectsofillhealthonenteringandmaintainingpaidemployment:evidenceinEuropeancountries 65
including subjects with bad or very bad health), results remained largely similar,
although the Ors for the effects of poor health and intermediate or high education
onbecomingunemployedorretiringweresomewhathigherthanthosepresentedin
tables4.3and4.4.This suggests that thedistributionaldifferencesamongcountries
havenotinvalidatedourfindings.
Aseconddrawbackwasthelargevariationinhouseholdresponses,whichinsome
countrieswereverylow,mostnotablyinGermany(48%)andIreland(56%).Inaddi-
tion,amongsubjectslosttofollow-upbetweenannualquestionnaires(attritionrate)
those with younger age, lower education, unmarried, and male gender were over-
represented.[16]Thelowhouseholdresponseinsomecountriescouldbeinfluenced
byhealth,butwhetherdifferentialbiasispresentremainsunknown.Asthenational
attritionratewasnotassociatedwiththeprevalenceofperceivedpoorhealthatbase-
line,wedonotexpectasubstantialbiasinthenon-responseduringthefollow-up.
Athirddisadvantagewastheuseofself-reportedlabourstatus,whichmaydiffer
fromofficialdefinitions.Forexample,apersonmayconsiderhimselfasunemployed
onlywhenheisactivelylookingforwork,whereasothersonunemploymentbenefit
may have categorized themselves as economically inactive.Another example is the
inability to distinguish illness-based unemployment or retirement from non-illness
based unemployment or retirement. Subjects becoming or remaining unemployed
0
0.5
1.0
1.5
2.0
2.5
3.0
0 5 10 15 20
OR
- va
lue
OR Poor health - unemploymentOR Poor health - employmentLinear (OR Poor health - unemployment)Linear (OR Poor health - employment)
Unemployment rate at national level
Figure 4.2 Themagnitudeoftheassociationbetweenaperceivedpoorhealthandbecomingunemployedorenteringemployment(OR)againstthenationalunemploymentratein1998among11countriesintheEuropeanHouseholdPanelSurvey

66 Chapter4
mayincludeasubstantialproportionofsubjectswith(workrelated)disability.Inthe
baselinesurvey,approximately2%oftherespondentsclassifiedasunemployedstated
thatthemainreasonfornotseekingworkwastheirownillness,injuryorincapacita-
tion.Hence,thiswillhaveonlyasmalleffectontheobservedinfluenceofpoorhealth
onthelikelihoodofenteringpaidemployment.
Theresultsofthisstudysupporttheexistenceofahealthselectionintheworkforce
ashealthierpeoplearemorelikelytobecomeorremainemployedthanlesshealthy
people.Severalstudieshavereportedasimilarimpactofhealthonenteringpaidem-
ploymentorleavingtheworkforce.IversenandSabroe[20]showedthatpsychological
healthremainedstableforthoseemployedorunemployedduringa2yearfollow-up,
whereas for those losingorgainingemployment,psychologicalhealthdecreasedor
increased,respectively.Thelikelihoodoffindingpaidworkwasnegativelyinfluenced
by mental health problems in British workers [7] and by health-related difficulties
in Finland.[21] A Swedish longitudinal study showed that subjects with limiting
longstandingillnesshadanincreasedriskofbecomingunemployed[10]andamong
Finnishmiddle-agedmen,apoorhealthpredictednon-illnessbasedearlyretirement.
[11]Theinfluenceofage,education,andmaritalstatusonemploymentstatusreflects
well-knownlabourmarketconditions-forexample,inallmosteveryEuropeancountry,
unemploymentishighestamongyoungerpeopleandamongthosewithalowlevel
of educational attainment.[22] The specific contribution of the current study is that
itshowsthatpoorhealthhadalong-termeffectonenteringpaidemployment,buta
muchmoretransienteffectonleavingtheworkforce.Poorhealthwasariskfactorfor
notenteringpaidemploymentalreadyfouryearsbeforethepotentialtransitioninto
theworkforce.Itisofinteresttonotethatinthecurrentstudytheeffectofpoorhealth
on entering paid employment was consistently present up to four years before the
actualtransitiontookplace.Thissuggeststhatthehealthstatusamongunemployed
subjectswithpoorhealthremainsstableovertimeand,hence,hasalong-termeffect
ontheprobabilityofenteringpaidemployment.Incontrast,theeffectsofpoorhealth
on unemployment, retirement or taking care of household were less pronounced in
moredistantyears,suggestingamoretransientpattern,withachangeinhealthbeing
theriskfactorratherthanpoorhealth.
Fewstudieshavereportedoninteractionsbetweenhealthstatusandsocioeconomic
position. McDonough and Amick[13] demonstrated that, in the USA, the effect of
perceivedillhealthonlabourmarketexitdependedonsex,race,andeducation.Poor
healthwasamoreimportantfactorinleavingtheworkforcethanamongwomen,and
theeffectofpoorhealthonlabourforceexitincreasedwitheducation.Bothfindings
werecorroboratedinourstudy(table4.2and4.3,respectively).Theeffectofhealthon
employmentstatuswilldifferacrossdifferentsocioeconomicpositionsastheconse-
quencesofpoorhealthalsodependonsocialandlabourmarketcircumstances.These

Ch
apte
r4
Theeffectsofillhealthonenteringandmaintainingpaidemployment:evidenceinEuropeancountries 67
lattercircumstancesvaryacrossthe11Europeancountriesinourstudy-forexample,by
thelevelofprotectionforworkerswithchronicdiseasesagainstworkforceexclusion
andrehabilitationpolicies,toincludepeoplewithpoorhealthinregularorsheltered
employment.[23]Itmaybehypothesizedthatcountrieswhereinapoorhealthstatus
wasastrongpredictorforlabourforceexitwerelesssuccessfulinretainingthosewith
apoorhealthstatusinthelabourforce.[14]Analternativeexplanationmaybethatin
countrieswherethisassociationwasnotobserved,healthislessimportantthanother
factorsindeterminingemploymentstatus.Figure2suggeststhat,incountrieswitha
lownationalunemploymentrate,healthwillcompetewithotherlabourmarketfactors
intheprocessofenteringorretainingpaidemployment,whereasincountrieswitha
highnationalunemploymentrate,theeffectofhealthselectionoutoftheworkforce
isrelativesmallcomparedwithotherfactorsthatdeterminelabouropportunitiesfor
people. However, this finding does not suggest that is these latter countries, health
selection per sé is not important, but rather that it cannot be demonstrated in the
currentanalysis.
An importantquestion iswhat society shoulddowithunhealthy job seekersand
unhealthy workers. Preventive public health interventions should not only address
thehealthselectionoutoftheworkforce,butalsotakeintoconsiderationthatbeing
unemployedcan lead to furtherdeteriorationof thehealth status, long-termunem-
ployment,andsocialexclusion.[23]Illhealthisanimportantdeterminantforentering
andmaintainingpaidemploymentinmanyEuropeancountries.Theseconsequences
of ill health will increase socioeconomic inequalities in health. It has been reported
before that unemployment, retirement, and work disability explain a great deal of
health inequalities across European countries.[24]. In policies for health equity, it is
ofparamountimportancetodeveloppublichealthmeasures,tailoredtosocio-demo-
graphiccharacteristics, that includepeoplewithapoorhealth in the labourmarket
andpreventworkerswithillhealthfromdroppingoutoftheworkforce.

68 Chapter4
ReFeRences
1. AchesonD.Independentinquiryintoinequalitiesinhealth.London:theStationaryOffice,1998.http://www.doh.gov.uk/ih/ih.htm(accessedOctober172005).
2. MarmotMG,SmithG,StansfieldS,etal.HealthinequalitiesamongBritishcivilservants:theWhitehallIIstudy.Lancet1991;337:1387-93.
3. ClaussenB.Healthandre-employmentinafive-yearfollowupoflong-termunemployed.Scand J Public Health1999;27:94-100.
4. JanlertU.Unemploymentasadiseaseanddiseasesoftheunemployed.Scand J Work Environ Health1997;23suppl3:79-83
5. MorrisJK,CookDG,ShaperAG.Lossofemploymentandmortality.BMJ1994;308:1135-9. 6. BartleyM,SackerA,ClarkeP.Employmentstatus,employmentconditions,andlimitingill-
ness:prospectiveevidencefromtheBritishhouseholdpanelsurvey1991-2001.J Epidemiol Community Health2004;58:501-506
7. ThomasC,BenzevalM,StansfeldSAEmploymenttransitionsandmentalhealth:ananalysisfromtheBritishhouseholdpanelsurvey.J Epidemiol Community Health2005;59:243-9.
8. MurphyGC,AthanasouJA.Theeffectofunemploymentonmentalhealth.J Occup Organ Psychol1999;72:83-99.
9. ClaussenB,BjorndalA,HjortPF.Healthandre-employmentinatwo-yearfollowupoflong-termunemployed.J Epidemiol Community Health1993;47:14-8.
10. LindholmC,Burström,DiderichsenF.Classdifferencesinthesocialconsequencesofillness?J Epidemiol Community Health2002;56:188-92.
11. KarpansaloM,ManninenP,KauhanenJ,LakkaTA,SalonenJ.Perceivedhealthasapredictorofearlyretirement.Scand J Work Environ Health2004;30:287-292
12. LoprestP,DavidoffA.Howchildrenwithspecialhealthcareneedsaffecttheemploymentdecisionsoflow-incomeparents.Matern Child HealthJ2004;8:171-82.
13. McDonoughP,AmickIIIBC.Thesocialcontextofhealthselection:alongitudinalstudyofhealthandemployment.Soc Science Med2001;53:135-45.
14. OECD.Transformingdisabilityintoability.Policiestopromoteworkandincomesecurityfordisabledpeople.Paris,OECD,2003.
15. Eurostat.(1999).EuropeanCommunityHouseholdPanel,Users’DatabaseManual(VersionofNovember1999),Luxembourg
16. PeracchiF.TheEuropeanCommunityHouseholdPanel:Areview.Emp Econ2002;27:63-90. 17. HuismanM,KunstAE,MackenbachJP.Inequalitiesintheprevalenceofsmokinginthe
EuropeanUnion:comparingeducationandincome.Prev Med2005;40:756-64. 18. UNESCO,(1997).InternationalStandardClassificationofEducation1997. 19. FayersPM,SprangersMAG.Understandingself-ratedhealth.Lancet2002;359:187-8. 20. IversenL,SabroeS.Psychologicalwell-beingamongunemployedanemployedpeopleafter
acompanyclosedown:alongitudinalstudy.J Soc Issues1988;44:141-52 21. PohjolaA.Healthproblemsandlong-termunemployment.Soc Work Health Care2001;34:101-12. 22. Eurostat.EuropeanUnionLabourForceStudy.http://forum.europa.eu.int/irc/dsis/em-
ployment/info/data/eu_lfs(accessedOctober172005) 23. GrammenosS.Illness,disabilityandsocialinclusion2003.EuropeanFoundationforthe
ImprovementofLivingandWorkingConditions.ISBN92-897-022104. 24. VanDoorslaerE,KoolmanX.Explainingthedifferencesinincome-relatedhealthinequalities
acrossEuropeancountries.Health Econom2004;13:609-28.

5The effect of re-employment on perceived health
SchuringM,MackenbachJP,VoorhamAJJ,BurdorfA.
Journal of Epidemiology and Community Health, in press.

70 Chapter5
absTRacT
background: Therelationshipbetweenunemploymentandpoorhealthhasbeenwell
established. Unemployment causes poor health and poor health increases the prob-
abilityofunemployment.
methods:A prospective study with 6 months follow-up was conducted among un-
employed subjects receiving social security benefits, who were capable of full time
employmentandwerereferred toa re-employment trainingcentre.Re-employment
was defined as ending social security benefits for at least three months because of
starting with paid employment. Health related quality of life was measured by the
ShortForm36HealthSurvey(SF-36).ACoxProportionalHazardsanalysiswasused
todetermine the factors thatpredicted re-employmentduring follow-up.The influ-
enceofre-employmentonchanges inperceivedhealthwas investigatedwith linear
regressionanalysis.
Results: Unemployedsubjectswithapoorhealthatbaselinewerelesslikelytoreturn
topaidemploymentduringfollow-up.Almostalldimensionsofhealthatbaselinehad
aninfluenceonthelikelihoodofbecomingemployed.Amongthere-employedsub-
jects,generalhealth,physicalfunctioning,socialfunctioning,vitality,mentalhealth,
bodily pain, and role-limitations due to emotional or physical problems improved,
withaneffectsizevaryingfrom0.11to0.66.
conclusion: Thisstudyprovidesevidencethatre-employmentleadstoimprovement
ofself-perceivedhealthwithinashorttimewindow.Thissuggeststhat labourforce
participationshouldbeconsideredastherapeuticinterventionwithinhealthpromo-
tionprogrammesamongunemployedpersons.

Ch
apte
r5
Theeffectofre-employmentonperceivedhealth 71
inTRoDucTion
Therelationshipbetweenunemploymentandpoorhealthhasbeenwellestablished,
as demonstrated by a higher prevalence of illness and disability[1-2] and a higher
mortalityamongunemployedpeople.[3]Theassociationbetweenhealthandemploy-
mentisbi-directional:unemploymentmaycausepoorhealth(causationhypothesis),
andpoorhealthmayincreasetheprobabilityofunemployment(selectionhypothesis).
There is evidence for the selectionhypothesis.A longitudinal studyamongEuro-
peancountries showed that in themajorityofEuropeancountriesaperceivedpoor
healthorachronichealthproblempredictedbecomingorstayingunemployed.[4]A
community based survey in the United Kingdom found that health related job loss
hadbecomeincreasinglycommon,especiallyinrelationtomusculoskeletaldisorders
andmentalillness.[5]Atwo-yearfollowupstudyoflongtermunemployedNorwe-
giansreportedthathealthrelatedselectionto longtermunemploymentexplaineda
substantialpartoftheexcessmentalmorbidityamongunemployedpeople.[6]
However, there is also evidence for the causation hypothesis. Various studies
haveshownthatunemploymentgaverise tohealtheffects,especiallypsychological
distress,depression,andreducedmentalhealth.Areviewof16longitudinalstudies
concerningmentalhealtheffectofunemploymentconcludedthatlossofemployment
affected mental health, but also that gaining employment improved mental health.
[7] A British longitudinal study found that transitions from paid employment to
various forms of non-employment (unemployment, long-term sick leave, maternity
leave)hadanegativeimpactonmentalhealth.Transitionsfromnon-employmentto
formalemploymentresultedinanimprovementofmentalhealth.Theeffectswerefelt
most stronglywithinsixmonthsafter the transition.[8]A five-year followupstudy
amonglong-termunemployedNorwegiansreportedrecoveryofmentalhealthafter
re-employment.[9]
“Work, matched to one’s knowledge and skills and undertaken in a safe, healthy
environment, can reverse theharmfuleffectsofprolongedsicknessabsenceor long
term unemployment, and promote health, well-being and prosperity”. This is the
main message of the so-called Black report, which reviewed the health of Britain’s
working-age population[10-11] In a review Waddel and Burton[12] concluded that
re-employment leads to clear benefits in psychological health and some measures
ofwell-being,althoughthere isadearthof informationonphysicalhealth.Ameta-
analytic study of the psychological and physical well-being during unemployment
also demonstrated that the bulk of research is focused on mental health outcomes,
suggesting that other aspects of health need more attention.[13] One study on re-
employmentindicatedthatphysicalaswellasmentalhealthimprovedamongthose
workingatoneyearfollow-upcomparedtothosenotworking.[14]Anotherstudyalso

72 Chapter5
showedapositiveassociationbetweengainingemploymentandphysicalfunctioning
among older workers who were displaced.[15] However, both studies were among
olderworkerswhowererecentlydisplacedorearlyretired.Itisnotknownwhether
theseresultscanbegeneralizedtothewholeworkingagepopulationwithadifferent
unemploymenthistory.
The impact of re-employment on mental health is reported by two meta-analytic
studies.[7,13]Thereislimitedinsightintotheeffectsizeofre-employmentonother
dimensions of health.[13] The aim of this study was to investigate the effect of re-
employment on different dimensions of health within a short period after entering
paidemployment.
meTHoDs
Studypopulation
A prospective study with 6 months follow-up was conducted among unemployed
subjects. The study population consisted of persons on social security benefits who
were capable of full time employment and who were referred by the Employment
CentreoftheCityofRotterdam,TheNetherlands,tooneofthefourre-employment
trainingcentresintheareaforare-employmenttraining.Someoftheparticipantsdid
havechronichealthproblems,butweredeclaredfitenoughtobecapableoffulltime
employmentafter investigationbyaphysician, apsychologist, andanemployment
specialist. From December 2004 until December 2007, every week an average of 19
subjectswasenrolledinthestudyafterreferraltoare-employmenttrainingcentre.In
total,2754eligibleparticipantswereincludedinthestudy.Participationinthisstudy
wasvoluntary.TheMedicalEthicsCommitteeofErasmusMCprovidedadeclaration
ofnoobjection.
Datacollection
Thefirstquestionnairewassenttoprospectiveparticipantsimmediatelyafterthere-
ferraltothere-employmenttrainingcentre.Thefollow-upquestionnairewassentsix
monthslater.Theprocedureofdatacollectionwassimilaratbaselineandfollow-up.
Thefirstquestionnairewassenttothehomeaddressoftheparticipants,followedby
tworeminderstworespectivelyfourweekslater.Additionalactionswereundertaken
to include more subjects.As a large part of the study population had a non-Dutch
background,thequestionnaireandcoveringletterweretranslatedinTurkishandsend
inadditiontotheDutchquestionnairetosubjectswithaTurkishsurname.Ifsubjects

Ch
apte
r5
Theeffectofre-employmentonperceivedhealth 73
ofthestudypopulationneededhelpwithfillinginthequestionnaire,theycouldgetin
touchwithaninterviewer.Subjectswhodidnotreplytothepostalquestionnairewere
visitedbyan interviewerat theirhomeaddresswith fourattemptsatdifferentday
times during a two week period. The interviewers were matched with the subjects,
basedonethnicity,age,andsex,andcouldofferan interview in themother tongue
(Dutch,Arabic,orTurkish).
Socio-demographicvariables
Socio-demographic variables, such as ethnic background, highest educational level,
age,sex,andmaritalstatuswereincludedinthequestionnaire.Ethnicbackgroundof
therespondentwasbasedonthecountryofbirthof themother. Incase themother
wasborninTheNetherlands,thecountryofbirthofthefatherwasleading.[16]Dif-
ferentethnicgroupsweredefined,basedondifferencesingeographicalandcultural
distancefromtheNetherlands.Threeethnicminoritygroupsweredefined:1)Turks
and Moroccans, 2) Antilleans and Surinamese, and 3) a miscellaneous group with
all other countries of origin. Subjects were divided into three groups according to
theirhighestlevelofeducationalattainment.Ahigheducationallevelwasdefinedas
highervocationaltrainingoruniversity,intermediateeducationallevelwasdefinedas
highersecondaryschoolingorintermediatevocationaltraining,andloweducational
levelwasdefinedasnoeducation,primaryschool,lowerandintermediatesecondary
schoolingor lowervocational training.Maritalstatuswasusedtodistinguish those
subjectsmarriedorlivingtogetherfromothers.
Psychologicalmeasures
Mastery was measured by the Personal Mastery Scale[17], which consists of seven
items (eg “I have little control over the things that happen to me”, “There is little
I can do to change many of the important things in my life”), answered on a four
point Likert scale (strongly agree to strongly disagree).Average scores across items
werecalculated,rangingfrom1to4,withahigherscoreindicatingahigherlevelof
mastery.Incasethreeormoreitemswereunanswered,noscorewascomputed.
Self-esteemwasmeasuredwiththeRosenbergSelf-EsteemScale[18],with10items
(e.g.,“Onthewhole,Iamsatisfiedwithmyself”,“Allinall,Iaminclinedtofeelthat
I am a failure”), answered on a four point Likert scale (strongly agree to strongly
disagree).Averagescoresacross itemswerecalculatedagain, ranging from1 to4;a
higherscoreindicatedahigherlevelofself-esteem.Incasethreeormoreitemswere
unanswered,noscorewascomputed.

74 Chapter5
Re-employmenttraining
Are-employmenttrainingcentreprovidedastandardizedapproachofare-employ-
ment training, characterizedbyabroadre-orientationonemploymentandemploy-
ability,enhancementofjobsearchskills,andintensificationofjobsearchefforts.
Re-employment
StartandenddatesofthesocialsecuritybenefitswereregisteredattheEmployment
Centre of the City of Rotterdam, The Netherlands. In these registers, additional in-
formationaboutreasonsforendingbenefitswasalsoadministered.Re-employment
was defined as leaving the social security benefit services for at least three months
because of starting with paid employment, verified by the national Social Security
Agency.Subjectswhoquittedtheirregistrationforasocialsecuritybenefitforother
reasons,forexamplemovinginwithapartnerormovingoutofthecityofRotterdam,
werecensoredfromthemomentthattheirbenefitpaymentwasquittedbythesocial
securityservices.
Healthmeasures
HealthrelatedqualityoflifewasmeasuredwiththeDutchversionoftheShortForm
36 Health Survey (SF-36).[19-20] Self-reported health (SRH) was measured with the
first itemof theSF-36byasking subjects to rate theiroverallhealthona five-point
scale,rangingfrom‘excellent’,verygood’,‘good’and‘fair’to‘poor’.Thosereporting
lessthan‘goodhealth’weredefinedashavingapoorhealth.[21]
Theother35itemsoftheSF-36wereusedtocalculatescoresoneightdimensions:
physical functioning, general health, mental health, bodily pain, social functioning,
vitality, role limitation due to emotional health problems, and role limitation due
to physical health problems. Scores could range from 0 to 100, with a higher score
indicatingabetterhealthrelatedqualityoflife.
Statisticalanalysis
AllstatisticalanalyseswereconductedbymeansofthestatisticalpackageSPSS(ver-
sion15)forWindowsandthelevelofsignificancewassetat0.05.
In the analyses two groups of respondents were compared, those who were still
unemployedatfollow-upandthosewhowerere-employedatfollow-up.Thebaseline
characteristics of both groups were compared with the chi-square test for dichoto-
mousdataandthet-testforcontinuousdata.Non-responsetothefirstquestionnaire

Ch
apte
r5
Theeffectofre-employmentonperceivedhealth 75
and loss-to-follow up during the six months until the second questionnaire were
investigated by logistic regression analysis with potential determinants; individual
characteristics, perceived health, participation in re-employment training, and re-
employment.
A Cox Proportional Hazards analysis was used to determine the factors that pre-
dicted re-employment during the follow-up period. The follow-up period was cen-
soredatdateofre-employment.Independentfactorswereindividualcharacteristics,
selfesteem,mastery,andtheeightdimensionsof theSF36.Variableswerecoded in
such a manner that a Hazard Ratio above 1 indicates an increased likelihood of re-
entering paid employment. For each dimension of the SF36 a standardized Hazard
Ratiowascalculatedbasedonanaveragescoreacrossitems,representingtheeffectof
anincreaseofonestandarddeviationintheaveragescoreatbaselineonthelikelihood
ofenteringpaidemployment.Individualcharacteristicswithasignificantunivariate
effectonre-employment,wereenteredfirstinthemultivariatemodel.Subsequently,
the health measure with the largest goodness-of-fit in the univariate analysis was
enteredinthemultivariatemodel.Afterthat,theeffectoftheothermeasuresofhealth
wereinvestigatedfortheiradditionaleffectongoodness-of-fit.
The association of re-employment with changes in perceived health was investi-
gated with linear regression analysis. The association of re-employment with each
dimensionofhealthwasadjustedforage,sex,ethnicbackground,education,duration
onbenefit,participationinare-employmenttraining,andalsoforthebaselinevalue
of the health dimension under study. For each dimension of health Cohen’s d was
calculated as measure of effect size by dividing the difference in health before and
afterre-employmentbytheirpooledstandarddeviation.[22]
ResuLTs
Figure5.1shows that2754subjectswereenrolled in thestudyafter referral toa re-
employmenttrainingcentre.Onethirdofthesubjects(n=932)hadchronichealthcom-
plaints,butweredeclaredtobefitenoughtobecapableoffulltimeemploymentafter
investigationbyaphysician,apsychologistandanemploymentspecialist.Fromthe
2754subjectswhoreceivedthefirstquestionnaire,1829subjects(66%)filledoutand
returnedthequestionnaire.Morethantwothirdoftherespondents(70%)returnedthe
baselinequestionnairebypost,whereasalmostonethirdoftherespondents(30%)had
a face-to-face interview. Non-response was statistically significantly higher among
youngersubjectsandmen.
Theresponseatfollow-upwas53%(965/1829).Loss-to-followupwasstatistically
significantlyhigheramongyoungersubjects,men,andsubjectsofnon-Dutchorigin,

76 Chapter5
butnotrelatedtomaritalstatus,employmenthistory,durationonbenefit,orhealthat
baseline.Subjectswhohadstartedwithare-employmenttraining(n=461)were less
oftenlosttofollowup(OR=0.8,95%CI0.7-1.0),whereassubjectswhohadreturned
topaidemployment(n=123)weremoreoftenlosttofollowup(OR=1.9,95%CI1.3-
2.7).However,amongthosewhoreturnedtopaidemployment,healthatbaselinedid
not differ significantly between non-respondents (n=76) and respondents (n=47) at
follow-up.
Table5.1showsthecharacteristicsoftherespondentstothefirstquestionnaire.The
meanageofrespondentswas39.7(sd9.5)years,49%wasman,57%hadalowlevelof
education,75%belongedtoanethnicminoritygroup,and43%receivedsocialsecurity
benefitsformorethanfiveyears.Duringthefollow-upperiod30%oftherespondents
hadstartedwithare-employmenttraining.
Figure5.2showsthathealthatbaselinewasbetteramongsubjectswhoreturnedto
paid employment during the follow-up period.All dimensions of health improved
Persons on social security benefits.Chronic health problems?
Referral to a re-employment training centerN=2754
Exemption from the obligation to work
Investigation by a physician, psychologist and an employment specialist.Capable of full time employment?
Enrollment in the studyN=2754
Response at baselineN=1829- 70% returned by post- 30% face-to-face interview
Non-response at baselineN=925
Response at follow-upN=965- 79% returned by post- 21% face-to-face interview
Non-response at baselineN=864
Yes
YesN=932
NoNoN=1822
Figure 5.1 Flowofparticipantsandresponseatbaselineandfollow-up

Ch
apte
r5
Theeffectofre-employmentonperceivedhealth 77
among re-employed subjects, whereas the health status of unemployed subjects re-
mainedunchanged.
Table5.2showsthatunemployedsubjectswithapoorhealthatbaselinewereless
likely to return to paid employment during follow-up (OR=0.39, 95% CI 0.2-0.7).
Alldimensionsofperceivedhealthatbaselinehadaninfluenceonthelikelihoodof
becomingemployed,exceptformentalhealth.Physicalfunctioninghadthestrongest
influence on the likelihood of becoming employed (OR=2.76, 95% 1.8-4.3). Ethnic
background,maritalstatus,selfesteem,mastery,andparticipatinginare-employment
trainingwerenotsignificantintheunivariatemodel.
Inthemultivariateanalysis,physical functioningatbaselinehadthestrongestas-
sociationwith re-employment.Due to the correlationsof theotherhealthmeasures
withphysicalhealth(generalhealthr=0.56,bodilypainr=0.62,mentalhealthr=
0.26, social functioning r=0.43, vitality r=0.41, role functioning, emotional r = 0.27,
rolefunctioning,physicalr=0.55),thesemeasuresofhealthdidnothaveasignificant
contributiontothemultivariatemodelincludingphysicalfunctioning.
Table5.3showsthatamongthere-employedsubjectsgeneralhealth,physicalfunc-
tioning, social functioning, vitality, mental health, bodily pain, and role-limitations
duetoemotionalorphysicalproblemsimprovedduringthefollow-upperiod,withan
effectsizevaryingfrom0.11to0.66.Thelargestrelativeimprovementswereobserved
Table 5.1 Characteristicsofrespondentstothefirstquestionnaire(n=1829)
variableRespondents n=1829
Age(n-%)18-44yr45-64yr
1230(67)599(33)
Men(n-%) 894(49)
Maritalstatuslivingwithpartner(n-%) 601(33)
Educationallevel(n-%)HigherandintermediatelevelLowerlevelMissing
634(35)1049(57)146(8)
Ethnicbackground(n-%)NativeDutchTurkish/MoroccanAntillean/SurinameseRefugee/Otherimmigrants
450(25)448(25)488(27)404(23)
Durationonsocialbenefit(n-%)LessthanoneyearBetween1and5years5yearsandmore
478(27)512(29)759(43)
Startedwithre-employmenttraining(n-%) 541(30)
Selfesteem(scale1-4:mean-sd) 2.48(0.6)
Mastery(scale1-4:mean-sd) 2.89(0.5)

78 Chapter5
formentalhealth,socialfunctioning,androle-limitationsduetoemotionalorphysical
problems, whereas physical functioning showed the smallest relative improvement.
For those subjects who remained unemployed the effect sizes varied from -0.04 to
0.06,indicatingthattheirhealthstatusremainedvirtuallyunchangedduringthesix
monthsfollow-upperiod.Participation inare-employmenttrainingwasnotassoci-
atedwithchangeofhealthstatus(datanotshown).
Discussion
Unemployedsubjectswithapoorhealthatbaselinewerelesslikelytoreturntopaid
employment during follow-up.Almost all dimensions of health at baseline had an
influence on the likelihood of becoming employed. The strongest association was
foundbetweenphysical functioningatbaselineand re-employment.Among the re-
employed subjects, general health, physical functioning, social functioning, vitality,
mentalhealth,bodilypain,androle-limitationsduetoemotionalorphysicalproblems
improved,withaneffectsizevaryingfrom0.11to0.66.Hence,re-employmentposi-
tivelyinfluencedmentalhealthaswellasphysicalhealth.
0
20
40
60
80
100
120Se
lf-r
ated
hea
lth o
n 0-
100
scal
e
gene
ral
heal
th
role
lim
itatio
n-ph
ysic
alpr
oble
m
bodi
lypa
in
men
tal
heal
th
soci
alfu
nctio
ning
vita
lity
phys
ical
func
tioni
ng
baseline follow-up Re-entered paid employment (n=47)
baseline follow-up Continued to be unemployed (n=918)
role
lim
itatio
n-em
otio
nal
prob
lem
Figure 5.2 Healthatbaselineandfollow-upforsubjectswhocontinuedtobeunemployed(n=918)andsubjectswhore-enteredpaidemployment(n=47)duringthefollow-upperiodofsixmonths

Ch
apte
r5
Theeffectofre-employmentonperceivedhealth 79
Table 5.2 Theinfluenceofindividualcharacteristicsanddimensionsofself-perceivedhealthamonglong-termunemployedpersons(n=965)onthelikelihoodofre-employment(n=47)duringafollow-upperiodofsixmonths.(CoxProportionalHazardsanalysis)
Re-employment (univariate model)
Re-employment (multivariate model)
Hazard Ratio (95%ci) Hazard Ratio (95%ci)
Higherage(>45years) 0.40(0.20-0.83)** 0.45(0.19-1.10)*
Men 2.19(1.21-3.97)** 1.74(0.91-3.31)
Loweducationallevel 0.52(0.30-0.93)** 0.60(0.32-1.12)
Poorhealth 0.39(0.22-0.69)** -
Generalhealth† 1.57(1.20-2.07)** -
Physicalfunctioning† 2.76(1.80-4.24)** 2.18(1.40-3.38)**
Bodilypain† 1.92(1.42-2.60)** -
Mentalhealth† 1.19(0.89-1.59) -
Socialfunctioning† 1.54(1.13-2.10)** -
Vitality† 1.48(1.12-1.95)** -
Rolefunctioning,emotional† 1.44(1.06-1.96)** -
Rolefunctioning,physical† 1.72(1.25-2.37)** -
**P<0.05,*P<0.10†StandardizedHazardRatio,representingtheeffectofanincreaseofonestandarddeviationintheaveragescore.
Table 5.3 Theinfluenceofre-employmentonchangesineightdimensionsofhealthmeasuredbytheSF-36healthquestionnaireamonglong-termunemployedpersonsduringafollow-upperiodofsixmonths.
effect of re-employment change† (se)(n=965)
effect size‡(cohen’s d)(n=47)
Generalhealth +7.0(2.7)** +0.18
Physicalfunctioning +9.2(3.4)** +0.11
Bodilypain +11.3(3.6)** +0.20
Mentalhealth +11.0(2.7)** +0.66
Socialfunctioning +14.2(3.8)** +0.32
Vitality +7.8(2.5)** +0.26
Rolefunctioning,emotional +22.7(6.8)** +0.46
Rolefunctioning,physical +20.0(6.0)** +0.33
†.Eachlinearregressionmodelwasadjustedforage,gender,ethnicbackground,education,durationonbenefit,andhealthatbaseline.‡:Effectsizeswerebasedonthemeanvaluesofhealthatbaselineandfollow-upofthere-employedsubjects

80 Chapter5
Losstofollowupwassignificantlyhigheramongyoungersubjects,men,subjects
ofnon-Dutchoriginandsubjectswhohadreturned topaidemployment.However,
among those who found employment (n=123), health at baseline did not differ be-
tween non-respondents (n=76) and respondents (n=47) at follow up. Therefore, we
assumethattheeffectsofre-employmentonhealthwerenotinfluencedbyselective
losstofollowup.
Subjects who were referred to a re-employment training centre were included in
thestudy.ThepolicyoftheEmploymentCentreoftheCityofRotterdamwastorefer
everybodywhowasabletoworkandcouldusesomehelpwithsearchingforajob.
Hence,subjectswerenotincludedinthestudywhentheywerenotable(duetohealth
problems)ornotobliged(duetofamilyobligationsoreducation)towork.Inaddition,
recentlyunemployedpersonswhoweresupposedtobeabletofindpaidemployment
bythemselves,werenotincluded.Thismayhaveaffectedtheresultswithrespectto
healthstatusandre-employmentprobabilities.
There-employedworkersgottheirjobsatdifferenttimesduringthefollow-upperi-
odofthestudy.Therefore,somepersonsmayhavebeenbackatworkformuchlonger
thanothersandthus,thelengthofexposuretothehealthbenefitsofre-employment
variedamongstthere-employedsample.Unfortunately,duetothesmallnumberof
personswhogainedemploymentitisnotfeasibletoanalysetherelationbetweentime
atworkandhealthbenefitsduetore-employment.
Thestudyisbasedonself-reportedhealthstatus.Therefore, justificationbiasmay
haveinfluencedthepresentresults.Respondentswhowerestillunemployedatfollow
upmayhavereportedmoreeasilythattheyhadapoorhealththanthosewhofound
paidemploymentinordertojustifythefactthattheydidnotfindajob.[23]
Duetotheobservationaldesignofthestudytheresultsmayhavebeeninfluenced
by selection bias. Subjects who found employment differed from those who stayed
unemployed with respect to health at baseline and personal characteristics. These
variableswereadjustedfor intheanalysis,buttheremayhavebeenothervariables
thatinfluencedbothhealthchangeandre-employment,e.g.motivationtowork,that
were not included in the analysis. However, two psychological measures that were
includedinthestudy,selfesteemandmastery,didnothaveasignificantinfluenceon
the likelihoodof re-employment. Inaddition, thesepsychologicalmeasuresdidnot
influencetheestimatedeffectsofre-employmentonhealth.
To control for the systematic differences in health at baseline between the unem-
ployed and re-employed subjects, stratified analyses were conducted showing that
re-employmentresultedinanincreaseofhealthforbothsubjectswithapoorhealth
atbaselineaswellassubjectswithagoodhealthatbaseline.Ingeneral,subjectswith
apoorhealthatbaselineshowedalargerincreaseinhealthafterre-employmentthan
subjectswithagoodhealthatbaseline(datanotshown).However,afterfindingpaid

Ch
apte
r5
Theeffectofre-employmentonperceivedhealth 81
employmentthehealthstatusofrecentlyre-employedsubjectsstilllaggedthehealth
statusoflong-termemployedpersons.[24]
Unemployedsubjectswithagoodhealthweremorelikelytoreturntopaidemploy-
mentduringfollow-up.Therefore,theresultsofthisstudysupporttheselectionhy-
pothesis.ThesefindingsareinaccordancewithastudyoftheEuropeanCommunity
HouseholdPanel,whichfoundthatapoorhealthorchronichealthproblempredicted
staying or becoming unemployed in European countries.[4] A two year follow up
study of long term unemployed in Norway showed that health related selection to
longtermunemploymentexplainedasubstantialpartoftheexcessmentalmorbidity
amongunemployedpeople.[6]
This study also showed that the health status of re-employed subjects improved,
whereasthehealthstatusofunemployedsubjectsremainedunchanged.Re-employ-
ment did not only have a positive influence on mental health, but also on physical
functioning, which was in accordance with findings from two other studies[14-15]
Basedonthesefinding,itseemsmostlikelythatstartingwithpaidemploymentresults
inhealthimprovement.However,duetothedesignofthestudyitcannotberuledout
thatitistheotherwayaround;achangeinhealthstatusmayincreasethelikelihoodof
findingpaidemployment.However,areviewshowedthatanincreaseinhealthstatus
oflongtermunemployedisratherunlikely.[2]Therefore,itisassumedthatthehealth
statusofparticipantsincreasedshortlyafterre-employment,supportingthecausation
hypothesis.This is incongruencewith findings fromotherstudies,which foundan
increaseinmentalhealthstatusafterre-employment.[8-9]
Inthepresentstudy,aneffectsizeof0.66wasfoundfortheimprovementofmen-
tal health after re-employment. This result is in accordance with findings from two
meta-analytic studies [7,13], reporting thatgainingemployment impactsonmental
health with an effect size of 0.54 respectively 0.89. The effects on other dimensions
wereslightlylower,butsincedifferentdimensionsofhealthwereassociatedwitheach
other it is difficult to infer that mental health seems more important than physical
health.ThisisinaccordancewiththeresultsoftheWhitehallIIstudyofcivilservants,
whichshowedthatphysicalandmentalhealthwerecorrelatedforparticipantswitha
lowsocioeconomicposition.[25]
Inthecurrentstudyonly5%(47/965)oftheparticipantsfoundpaidemployment
withinsixmonths.Thislowre-employmentrateisinaccordancewithastudyamong
personsreceivingsocialsecuritybenefitsinthecityofAmsterdam,theNetherlands,
whichshowedthatonly8%ofthepersonsfoundpaidemploymentinatwo-yearpe-
riodfrom2004-2006.[26]Thecurrentstudypopulationischaracterisedbyalong-term
unemployment history. Long-term unemployed subjects often have much difficulty
infindingpaidemployment,especiallyforthosewithapoorhealth.Allparticipants
in the study were referred to a re-employment training centre for a re-employment

82 Chapter5
training.However,thisre-employmenttrainingdidnothaveapositiveeffectonthe
probabilityofre-employmentoronthehealthstatusofparticipants.Therefore,other
measuresseemtoberequiredtoincreasethechanceofre-employmentforlongterm
unemployedwithapoorhealth.
IntherecentBlackreportonthehealthoftheBritishworkingagepopulation,Black
appealedforchangingperceptionsoffitnessforwork.Insteadofstickingtotheidea
thatonecannotworkunless100%fit, itisrecommendedthatacampaignshouldbe
launchedtomakeemployers,healthcareprofessionalsandthegeneralpublicaware
thatworkis ingeneralgoodforhealth.[10]Thisstudyprovidesevidencethatwork
isindeedgoodforyourhealthand,thus,workshouldbeconsideredasanimportant
part of health promotion programmes among unemployed persons. In policies for
health equity public health measures are required to include persons with a poor
healthinthelabourmarketandtopreventworkerswithillhealthfromdroppingout
oftheworkforce.

Ch
apte
r5
Theeffectofre-employmentonperceivedhealth 83
ReFeRences
1. BartleyM,SackerA,ClarkeP:Employmentstatus,employmentconditions,andlimitingillness:prospectiveevidencefromtheBritishhouseholdpanelsurvey1991-2001.Journal of epidemiology and community health 2004,58:501-506.
2. JanlertU:Unemploymentasadiseaseanddiseasesoftheunemployed.Scand J Work Environ Health 1997,23Suppl3:79-83.
3. MorrisJK,CookDG,ShaperAG:Lossofemploymentandmortality.BMJ (Clinical research ed 1994,308:1135-1139.
4. SchuringM,BurdorfA,KunstAE,MackenbachJP:Theeffectofillhealthonenteringandmaintainingpaidemployment:evidenceinEuropeancountries.Journal of epidemiology and community health 2007,61:597-604.
5. SolomonC,PooleJ,PalmerKT,CoggonD:Health-relatedjobloss:findingsfromacommu-nity-basedsurvey.Occup Environ Med 2007,64:144-149.
6. ClaussenB,BjorndalA,HjortPF:Healthandre-employmentinatwoyearfollowupoflongtermunemployed.Journal of epidemiology and community health 1993,47:14-18.
7. MurphyGC,Athanasou,J.A.:Theeffectofunemploymentonmentalhealth.Journal of Oc-cupational and Organizational Psychology 1999,72:83-99.
8. ThomasC,BenzevalM,StansfeldSA:Employmenttransitionsandmentalhealth:ananalysisfromtheBritishhouseholdpanelsurvey.Journal of epidemiology and community health 2005,59:243-249.
9. ClaussenB:Healthandre-employmentinafive-yearfollow-upoflong-termunemployed.Scand J Public Health 1999,27:94-100.
10. BlackC:Workingforahealthiertomorrow.London: The Stationery Office 2008(http://www.workingforhealth.gov.uk/Carol-Blacks-Review/):ISBN:9780117025134
11. HulshofCT:Workingforahealthiertomorrow.Occup Environ Med 2009,66:1-2. 12. WaddellG,Burton,A.K.:Isworkgoodforyourhealthandwell-being?London: The Stationery
Office 2006(www.tsoshop.co.uk):ISBN:9780117036949. 13. McKee-RyanF,SongZ,WanbergCR,KinickiAJ:Psychologicalandphysicalwell-beingdur-
ingunemployment:ameta-analyticstudy.J Appl Psychol 2005,90:53-76. 14. PattaniS,ConstantinoviciN,WilliamsS:Predictorsofre-employmentandqualityoflife
inNHSstaffoneyearafterearlyretirementbecauseofillhealth;anationalprospectivestudy.Occup Environ Med 2004,61:572-576.
15. GalloWT,BradleyEH,SiegelM,KaslSV:Healtheffectsofinvoluntaryjoblossamongolderworkers: findingsfromthehealthandretirementsurvey.J Gerontol B Psychol Sci Soc Sci 2000,55:S131-140.
16. CBS:Herkomstvanpersonen;allochtonenenmigratie[Countryoforiginofpersons;mi-grantsandmigration].Centraal Bureau voor de Statistiek, Voorburg / Heerlen 2003.
17. PearlinLI,SchoolerC:Thestructureofcoping.J Health Soc Behav 1978,19:2-21. 18. RosenbergM:Societyandtheadolescentself-image.Princeton:PrincetonUniversityPress
1965. 19. WareJE,Jr.,SherbourneCD:TheMOS36-itemshort-formhealthsurvey(SF-36).I.Concep-
tualframeworkanditemselection.Med Care 1992,30:473-483. 20. VanderZeeKI,SandermanR:Hetmetenvandealgemenegezondheidstoestandmetde
RAND-36: een handleiding [Measuring health status with the RAND-36: a manual]. In

84 Chapter5
Groningen:NoordelijkCentrumvoorGezondheidsvraagstukken,RijksuniversiteitGron-ingen.1993.
21. FayersPM,SprangersMA:Understandingself-ratedhealth.Lancet 2002,359:187-188. 22. CohenJ:Statisticalpoweranalysisforthebehavioralsciences(2nded.).Hillsdale,NJ:Law-
renceEarlbaumAssociates1988. 23. KapteynA,SmithJP,vanSoestA:Dynamicsofworkdisabilityandpain.J Health Econ 2008,
27:496-509. 24. SchuringM,BurdorfA,KunstA,VoorhamT,MackenbachJ:Ethnicdifferencesinunemploy-
mentandillhealth.Int Arch Occup Environ Health 2009,82:1023-1030. 25. SackerA,HeadJ,GimenoD,BartleyM:SocialInequalityinPhysicalandMentalHealth
ComorbidityDynamics.Psychosom Med 2009. 26. Re-integratie-vanbijstandnaarwerk.Rekenkamer Amsterdam 2007.

6effectiveness of a health promotion programme
for long-term unemployed subjects with health
problems: a randomized controlled trial
SchuringM,BurdorfA,VoorhamAJJ,derWeduweK,MackenbachJP
Journal of Epidemiology and Community Health 2009, 63:893-899.

86 Chapter6
absTRacT
background:Employmentstatusisanimportantdeterminantofhealthinequalities.
Amongunemployedpersonsapoorhealthdecreasesthelikelihoodofre-employment.
methods:Arandomizedcontrolledtrialwith6monthsfollowupamongunemployed
personswithhealthcomplaintsreceivingsocialsecuritybenefitsfromthecityofRot-
terdam,theNetherlands.Intotal,456personswereassignedtothecontrolgroupand
465 persons to the intervention group. The intervention consisted of three sessions
weeklyover12weeks.Onesessionaweekwasfocusedoneducationtoenhancethe
abilitytocopewith(health)problemsandtwoweeklysessionsconsistedofphysical
activities. The primary outcome measures were perceived health, measured by the
ShortForm36HealthSurvey,andpsychologicalmeasuresmastery,selfesteem,and
pain-relatedfearofmovement.Secondaryoutcomemeasureswereworkvalues, job
searchactivities,andre-employment.
Results:Enrollmentintheinterventionprogrammewas65%and72%completedthe
programme with over 70% attendance to all sessions. The intervention had a good
reachamongsubjectswithlowereducation,buthadnoeffectonmentalandphysical
health,mastery,selfesteem,andpain-relatedfearofmovement.Participationinthe
programmehadnoinfluenceonworkvalues,jobsearchactivities,orre-employment.
conclusion:Theinterventionprogrammeaimedatpromotionofphysicalandmental
healthofunemployedpeoplewithhealthcomplaintsdidnotshowbeneficialeffects.
The lackof integration into regularvocational rehabilitationactivitiesmayhave in-
terferedwiththesefindings.Itcannotberecommendedtoimplementthisparticular
healthprogramme.

Ch
apte
r6
Effectivenessofahealthpromotionprogrammeforlong-termunemployedsubjectswithhealthproblems 87
inTRoDucTion
Therelationshipbetweenunemploymentandpoorhealthhasbeenwellestablished,
as demonstrated by a higher prevalence of illness and disability [1-2] and a higher
mortalityamongunemployedpeople.[3]Theassociationbetweenhealthandemploy-
mentisbi-directional:unemploymentmaycausepoorhealth(causationhypothesis),
andpoorhealthmayincreasetheprobabilityofunemployment(selectionhypothesis).
[4-6]
Workprovidesavarietyoffeatures,includingtheuseofskills,interpersonalcontact,
andprovisionofeconomicresources,thatareresponsibleforpsychologicalwell-being
andareadverselyinfluencedbyjoblossandunemployment.[7]Joblossmayleadto
impairedroleandemotionalfunctioning,poorhealth,anddepression.[8]Self-esteem
declineswithjobloss[9]andalowself-esteemisadeterminantofself-reportedpoor
health.[10]Apoorpsychologicalhealthwillactasabarriertoreturntopaidemploy-
mentthroughadecreasedmotivation,loweredexpectationsinfindingemployment,
andineffectivejobseeking.[8-9,11]Thus,unemploymentmayleadtoapoorerhealth,
whichinturnwillreducethelikelihoodofre-employment.
Inorderto increasethepossibilitiesforre-employment, improvementinhealthof
unemployedpersonsmay,therefore,beanimportantstep.Unemployedpersonswith
chronichealthcomplaints, suchasmusculoskeletaldisorders,maybecomeprogres-
sivelylesshealthy,sincefearofpainandreinjurymayleadtoreducedactivities[12],
resulting in a passive life style with low levels of physical activity.[13-14] Hence,
exercises to improvephysicalactivitymaybebeneficial,notonly for those subjects
withdisordersofthelocomotivesystem,butalsoforotherchronicdiseasesaswell,
including heart and pulmonary diseases and depression.[15] Cognitive-behavioural
therapymaybeneededtotargetspecificpain-relatedbeliefsandcopingstrategiesfor
modification.[16]RoseandHarris[17]haveidentifiedcognitivebehaviouraltherapy
asapromisinginterventiontoimprovethepsychologicalhealthofpersonswhoare
unemployed. Recently, Watson and colleagues [18] have provided some indications
that a combined physical exercise and cognitive behavioural programme improved
physical fitness as well as increased employment rates among unemployed partici-
pantswithhealthcomplaints.Theseresultsshouldbeinterpretedwithcaution,how-
ever,sincethevoluntaryparticipationintheprogrammemighthavebiasedtowards
participantswithahighmotivationandapositiveattitudetowards(returnto)work.
Hence,thereisaneedforrandomizedtrialsonmultidisciplinaryhealthintervention
onunemployedpersons.Theaimofthecurrentstudy(“Workonyourhealth”)was
toevaluatetheeffectivenessofahealthpromotionprogramme,consistingofphysical
exerciseandcognitivetraining,onphysicalandmentalhealthofunemployedsubjects
withhealthcomplaints.

88 Chapter6
meTHoDs
Designandstudypopulation
Thestudywasdesignedasarandomizedcontrolledtrial(RCT)andapprovedbythe
MedicalEthicsCommitteeoftheUniversityMedicalCenterRotterdamErasmusMC.
Personsonsocialsecuritybenefitswho(partly)attributedtheirinabilitytofindapaid
jobtotheirchronichealthproblems,werereferredbytheEmploymentCentreofthe
CityofRotterdam,TheNetherlands,forafit-to-worktest,conductedbyaphysician,
psychologist, and an employment specialist. All participants with health problems
anddeclaredtobecapableoffulltimeemploymentwereselectedastargetpopulation
forthisstudy.Formorethantwothirdofthepopulation(68%)thepresenceofchronic
painwasascertainedbyaphysician.Inaddition,subjectswererequiredtounderstand
andspeakDutchatbasiclevel.
Randomization
Randomization was performed by a researcher with a computer-generated list of
randomnumbers (SASSoftware,version8.12,Cary,NC).At the company thatper-
formed the fit-to-work tests, every week the researcher allocated all participants to
theinterventiongrouporthereferencegroup.FromDecember2004untilDecember
2007,everyparticipantwhomettheinclusioncriteriawasrandomized.Afterrandom-
izationeligibleparticipantswereapproachedby the research team forparticipation
in the study and asked to provide their written informed consent. This procedure
of informedconsentafterrandomizationwasnecessary,sincetheCityofRotterdam
requiredanimmediatereferraltoanemploymentserviceforvocationalrehabilitation
withoutfurtheradministrativedelay,andalsorequiredthatwillingnesstoparticipate
inthestudywouldnotinterferewithexistingrequirementsforjobsearch.
Theallocationsequencewasconcealeduntiltheparticipanthadbeenassigned.The
participants and the professionals providing the intervention could not be blinded.
However, the persons who were involved in data collection and data entry were
blinded,sincedatacollectionwasconductedcompletelyindependentfromtheinter-
ventionandregularvocationalrehabilitation.
Figure 6.1 shows the diagram of the flow of participants through the phases of
thetrial.Intotal,465subjectswereassignedtotheinterventionprogrammeand456
subjectstotheusualcaregroup.

Ch
apte
r6
Effectivenessofahealthpromotionprogrammeforlong-termunemployedsubjectswithhealthproblems 89
Intervention
Theinterventionwasaimedatchangingthewayunemployedpersonsperceiveand
cope with their health complaints. The rationale was based on the biopsychosocial
modelofchronicpainandsubsequentinterdisciplinarypainmanagementapproach.
Patients with chronic pain are at increased risk for emotional disorders (such as
anxiety,depressions,andanger),maladaptivecognitions(suchascatastrophizingand
poorcopingskills),functionaldeficitsandphysicaldeconditioning(duetodecreased
physicalactivityandfearofinjury).Theseeffectsareofteninterdependent,sothatone
cannotsimplytreatonetotheexclusionofothers.Interdisciplinarypainmanagement
Non-respons Q1N=122
Lost to follow-upN=111
Lost to follow-upN=160
No participation N=104
no longer benefit n=8reintegration programme n=22unknown n=74
Non-respons Q1N=146
Enrollment of eligible subjectsN=921
Randomization
Allocated to interventionN=465
Allocated to care as usualN=456
Filled out questionnaire Q1N=343
Filled out questionnaire Q1N=310
Filled out questionnaire Q2N=128
Filled out questionnaire Q2N=150
Analysis per protocolN=128
AnalysisN=150
Analysis intention to treatN=176
Initial participationN=239
Figure 6.1 Flowofparticipantsthroughthephasesofthetrial

90 Chapter6
embracesthefactthatthecomprehensivetreatmentofallthesedimensionsisneeded
inordertobeeffective.[19]
The intervention consisted of three sessions each week during a 12-week period.
Every week one session of three hours was focused on behavioural education and
twosessionswerefocusedonphysicalactivity.Thebehaviouraleducationalcompo-
nent was designed to enhance a participant’s insight in his/her health complaints,
to increasepositivecopingwithhealthproblemsbyreducingfearandavoidanceof
movement,toenhanceself-esteemandfeelingsofmastery,andtoimprovefunction-
ingbylearningtothinkpositivelyandenhancesocialskills.Thispartwasconducted
bytwopreventionworkers.
Thephysicalactivitycomponentconsistedoftwosessionsofthreehours.Thefirst
sessioncomprisedof1.5hours fitness training (cardioandweight training)and1.5
hoursofindoorsports(e.g.basketball,swimming).Thesecondsessioncomprisedof
1.5 hours fitness training and 1.5 hours of outdoor activities. The intervention was
designedtomaketheparticipantsawarethat itwassafe tomoveandhealthytobe
physically active, to extend the social network, to improve daily structure, and to
improvegeneralwellbeing.Theexerciseprogrammewasdevelopedaccordingtothe
graded-activity principle.[20-22] The exercises started below the average functional
capacity assessed during the first session and were increased gradually during the
courseoftheintervention,accordingtothetime-contingencyprinciple.Thesesessions
wereconductedbyphysicaleducationteachers.
Usualcare
Subjectsinthereferencegroupwerereferredtooneofthethreevocationalrehabilita-
tionservicesinthearea.Theyprovidedastandardizedapproachofvocationalreha-
bilitation,characterizedbyabroadre-orientationonemploymentandemployability,
enhancementof jobsearchskills,and intensificationof jobsearchefforts.Theusual
careapproachdidnotincludeanyactivityrelatedtohealth,suchashealthpromotion
toincreasephysicalactivityinleisuretime.
Datacollection
Aquestionnaireandan informedconsentwassendto thehomeaddressof thepar-
ticipants, followed by two reminders two respectively four weeks later.Additional
actions were undertaken to include more subjects. The questionnaire and covering
letterweretranslatedinTurkishandsendinadditiontotheDutchquestionnaireto
subjectswithaTurkishsurname.Ifsubjectsofthestudypopulationneededhelpwith
fillinginthequestionnaire,theycouldgetintouchwithaninterviewer.Subjectswho

Ch
apte
r6
Effectivenessofahealthpromotionprogrammeforlong-termunemployedsubjectswithhealthproblems 91
didnotreplytothepostalquestionnairewerevisitedbyaninterviewerattheirhome
address with four attempts at different day times during a two week period. The
interviewerswerematchedwithsubjects,basedonethnicity,age,andsex,andcould
offeraninterviewinthemothertongue(Dutch,Arabic,orTurkish).
Socio-demographicvariables
Socio-demographic variables, such as ethnic background, education, age, sex, and
maritalstatuswereincludedinthestudy.Ethnicbackgroundoftherespondentwas
basedonthecountryofbirthofthemother.IncasethemotherwasborninTheNeth-
erlands, the country of birth of the father was leading.[23] Different ethnic groups
were defined, based on differences in experiences of migration (refugees or labour
migrants)anddifferencesingeographicalandculturaldistancefromtheNetherlands.
Three ethnic minority groups were defined: 1) Turks and Moroccans, 2) Antilleans
and Surinamese, and 3) a miscellaneous group with all other countries of origin.
Subjectsweredividedintothreegroupsaccordingtothehighestlevelofeducational
attainment. A high educational level was defined as higher vocational training or
university, intermediate educational level was defined as higher secondary school-
ing or intermediate vocational training, and low educational level was defined as
noeducation,primaryschool, lowerandintermediatesecondaryschoolingorlower
vocationaltraining.Maritalstatuswasusedtodistinguishthosesubjectsmarriedor
livingtogetherfromothers.
Primaryoutcomemeasures
Health measuresHealthrelatedqualityoflifewasmeasuredwiththeDutchversionoftheShortForm
36HealthSurvey(SF-36).[24-25].Self-reportedhealth(SRH)wasmeasuredwiththe
first itemof theSF-36byasking subjects to rate theiroverallhealthona five-point
scale,rangingfrom‘excellent’,verygood’,‘good’and‘fair’to‘poor’.Thosereporting
lessthan‘goodhealth’weredefinedashavingapoorhealth.[26]
Theother35itemsoftheSF-36wereusedtocalculatescoresoneightdimensions:
physical functioning, general health, mental health, bodily pain, social functioning,
vitality, role limitation due to emotional health problems, and role limitation due
to physical health problems. Scores could range from 0 to 100, with a higher score
indicatingabetterhealthrelatedqualityoflife.

92 Chapter6
Psychological measuresMastery was measured by the Personal Mastery Scale [27], which consists of seven
items (eg “I have little control over the things that happen to me”, “There is little
I can do to change many of the important things in my life”), answered on a four
point Likert scale (strongly agree to strongly disagree).Average scores across items
were calculated, ranging from 1 to 4, with a higher score indicating a higher level
of mastery. In case three or more items were unanswered, no score was computed
(Cronbach’salpha=0.69).
Self-esteemwasmeasuredwiththeRosenbergSelf-EsteemScale[28]],with10items
(e.g.,“Onthewhole,Iamsatisfiedwithmyself”,“Allinall,Iaminclinedtofeelthat
I am a failure”), answered on a four point Likert scale (strongly agree to strongly
disagree).Averagescoresacross itemswerecalculatedagain, ranging from1 to4;a
higherscoreindicatedahigherlevelofself-esteem.Incasethreeormoreitemswere
unanswered,noscorewascomputed(Cronbach’salpha=0.84).
Kinesiophobia was measured with the Tampa Scale of Kinesiophobia [29], which
consists of 17 items on fear of movement and injury (e.g. “It’s really not safe for a
personwithaconditionlikeminetobephysicallyactive”,“PainalwaysmeansIhave
injuredmybody”)onafourpointLikertscale(stronglyagreetostronglydisagree).
Averagescoresacrossitemswereagaincalculated,rangingfrom1to4,withahigher
scoreindicatingahigherlevelofkinesiophobia.Incasefiveormoreitemswereunan-
swered,noscorewascomputed(Cronbach’salpha=0.80).
Secondaryoutcomemeasures
Attitudesandvalues towardspaidemploymentweremeasuredwith fivequestions
(e.g.,“Iwoulddoanythingtogetajob”,“Ifyoudon’twanttowork,youtakeadvan-
tageofothers”)onafivepointscale(stronglyagreetostronglydisagree).Asumscore
wasalsocalculated(Cronbach’salpha=0.30).Jobsearchactivitiesweremeasuredwith
fivequestionsconcerningdifferenttypesofjobsearchactivities(e.g.,“writinganap-
plicationletter”,“searchingforvacanciesinthenewspaperorontheinternet”).Asum
scorewascalculated,rangingfrom0(no jobsearchactivities) to5(many jobsearch
activities) (Cronbach’s alpha=0.68). Finally, re-employment was measured with one
question(“Doyoucurrentlyhaveapaidjob?”)onadichotomousscale(yes/no).
Processevaluation
At the end of the intervention programme semi-structured interviews were under-
taken with ten participants and ten trainers to obtain more qualitative insight into
differentaspectsoftheinterventionthatcouldbeimprovedinthefuture.

Ch
apte
r6
Effectivenessofahealthpromotionprogrammeforlong-termunemployedsubjectswithhealthproblems 93
Statisticalanalysis
Basedonthesamplesizecalculationwithaninitialparticipationof70%anda loss-
to-follow-upof30%(powerof80%,one-sidedsignificancelevel0.05),adifferenceof
5.0points(10%)inthescoresonhealthmeasuresbetweentheinterventiongroupand
referencegroupcouldbedetectedwith400personsassignedtoboth trialarmsand
196personswith completedata collection ineachgroup.With theseassumptionsa
differenceof10%inproportionofenteringpaidemploymentbetweenthe interven-
tion(15%)andcontrolgroup(5%)couldbedetected.
The effects of individual characteristics and physical and mental health on par-
ticipation in the intervention were investigated by logistic regression analysis. The
dependentvariableswerefailuretostartwiththeprogramme(yes/no)anddropping
outoftheprogramme(yes/no).Independentvariableswithap-valueof0.10orless
wereretainedinthemultivariatemodelsaswellasageandsexbydefault.Inorder
to compare both analyses, a variable retained in one multivariate model was also
includedintheothermultivariatemodel.
Thebaselinecharacteristicsofbothgroupswerecomparedwiththechi-squaretest
fordichotomousdataandthet-testforcontinuousdata.Theeffectsoftheinterven-
tion on outcome measures at 6 months follow-up were analyzed according to the
intention-to-treat principle, including all subjects regardless of whether or not they
actually received the complete intervention. The analysis was conducted with all
availablerespondentsatthetimeoffollow-upandanon-responseanalysiswascon-
ductedtoevaluatewhetherdrop-outduringthefollow-upperiodwasassociatedwith
healthstatusorinterventionstatus.Animputationtechniqueformissingresponseson
healthoutcomesduringfollow-upmeasurementswasnotused,sincethechoicefora
particularimputationmethodmayinfluencetheestimationoftheinterventioneffect.
[30]Theeffectsoftheinterventiononthecontinuousoutcomemeasureswereevalu-
atedwithamixedeffectmodelforrepeatedmeasurements,withtheinterventionas
fixedeffectandacompoundsymmetrycovariancestructurefortherandomvariation
betweenpersonsandacrosspersons.Thisapproachestimates thechange inanout-
comemeasurebetweenbaselineandfollow-up,takingintoaccountthebaselinevalue
oftheoutcomemeasureofinterestandthepotentialconfoundersage,sex,ethnicity,
education,andtimeonbenefits(SASversion8.12-procedureMixed).
Theeffectsoftheinterventiononthedichotomousoutcomemeasurere-employment
wasanalyzedbyachi-squaremethod (SASversion8.12 -procedureSurveymeans),
adjusted for sex and age.All analyses were carried out with the statistical package
SASversion8.12.

94 Chapter6
ResuLTs
Figure 6.1 shows that at baseline 921 subjects were enrolled in the study. In the
intervention group 343 (74%) persons returned the first questionnaire, which was
statisticallysignificantlyhigherthanthe310(68%)respondentsinthereferencegroup.
Non-responsewasnotinfluencedbyageorsex.
The response at follow-up did not differ between the intervention group (n=176;
51%) and reference group (n=150; 48%). Loss-to-follow up was statistically sig-
nificantlyhigheramongmen,butnotrelatedtoage,maritalstatus,education,ethnic
Table 6.1 Characteristicsofthestudypopulationandbaselinevaluesofoutcomemeasures
variableintervention group(n=343)
usual care group(n=310)
Age(n-%)18-44yr45-64yr
194(52.8)149(43.4)
175(52.9)135(43.6)
Men(n-%) 172(50.2) 160(51.6)
Maritalstatuslivingwithpartner(n-%) 127(37.0) 119(38.4)
Educationallevel(n-%)HigherandintermediatelevelLowerlevel
113(32.9)230(67.1)
123(39.7)187(60.3)
Ethnicbackground(n-%)NativeDutchTurkish/MoroccanAntillean/SurinameseRefugee/Otherimmigrants
88(25.7)90(26.2)89(26.0)76(22.2)
65(21.0)87(28.1)90(29.0)68(21.9)
Employmentexperience(n-%)NeverworkedLessthan5years5yearsandmore
67(19.9)117(34.7)153(45.4)
60(19.8)107(35.3)136(44.9)
Durationonsocialbenefit(n-%)LessthanoneyearBetween1and5years5yearsandmore
58(16.9)85(24.8)200(58.3)
53(17.1)73(23.6)184(59.4)
Healthoutcomemeasures(mean-sd)Generalhealth(0-100)Physicalfunctioning(0-100)Bodilypain(0-100)Mentalhealth(0-100)Socialfunctioning(0-100)Vitality(0-100)
37.4(18.5)52.8(23.7)41.0(23.1)52.5(19.1)52.2(26.1)43.4(16.6)
37.4(19.8)53.5(24.8)43.0(24.5)54.0(20.0)52.6(27.7)45.7(18.1)
Psychologicaloutcomemeasures(mean-sd)Self-esteem(1-4)Mastery(1-4)Kinesophobia(1-4)
2.9(0.6)2.4(0.6)2.7(0.5)
2.9(0.6)2.4(0.6)2.7(0.5)
Poorhealth(n-%) 281(81.9) 252(81.3)

Ch
apte
r6
Effectivenessofahealthpromotionprogrammeforlong-termunemployedsubjectswithhealthproblems 95
background,workexperience,durationonbenefit,orhealthatbaseline.Within the
interventiongroup,participationintheinterventionwasnotassociatedwithresponse
onthefollow-upquestionnaire.
Table6.1showsthattherandomizationwassuccessfulincreatingstudygroupswith
similardemographiccharacteristicsandphysicalandpsychologicalhealthatbaseline.
Amongthe465subjectswhowereallocatedtotheinterventiongroup,300subjects
(65%)initiallystartedwiththehealthprogramme.Duringthehealthprogramme85
subjects(28%)droppedoutoftheinterventionduetoanattendancelevelbelow70%
ofallsessionoffered(table6.2). Initialparticipationwasnot influencedbyage,eth-
nicbackground,educational level,marital status, employmenthistory,orperceived
health. Men were more likely to not enter the intervention programme (OR=1.5).
Subjectsdroppingoutoftheprogrammereportedpoorerphysicalandmentalhealth
atbaseline(table6.3).Highfearofmovementatbaselinedidhaveasignificanteffect
ondroppingoutoftheprogrammeintheunivariatemodel(OR=2.095%CI1.0-3.9).
However,duetotheassociationsoffearofmovementwithmentalhealth(r=0.3)and
Table 6.2 Numberofsubjectswhostartedwiththehealthprogramme,whocontinuedtheirparticipationthroughouttheprogramme,andsubjectswhodroppedoutduringtheprogramme.
number of subjectsn (%)
number of respondents to the first questionnaire n
Allocatedtointervention 465 343
Initialparticipation 300(65) 239
Continuedparticipation(>70%attendancetoallsessions)
215(72) 172
Dropout:Between50-70%participationLessthan50%participation
41(14)44(15)
3037
Table 6.3 Logisticregressionanalysisontheeffectsofindividualcharacteristicsandmentalandphysicalhealthonfailuretostartwiththeprogrammeordroppingoutduringtheprogramme
variable not starting with programme(n=104/343)oR (95% ci)
Dropping out(n=67/239)
oR (95% ci)
Age18-44yr45-64yr
1.00.7(0.4-1.1)
1.00.9(0.5-1.7)
Men 1.5(0.9-2.5)* 0.9(0.5-1.7)
Healthoutcomemeasures(standardisedvalues)PhysicalfunctioningMentalhealth
1.0(0.8-1.3)1.0(0.8-1.3)
0.8(0.5-1.1)*0.7(0.5-1.0)*
*0.05<P<0.10ORoddsratio,CIconfidenceinterval.
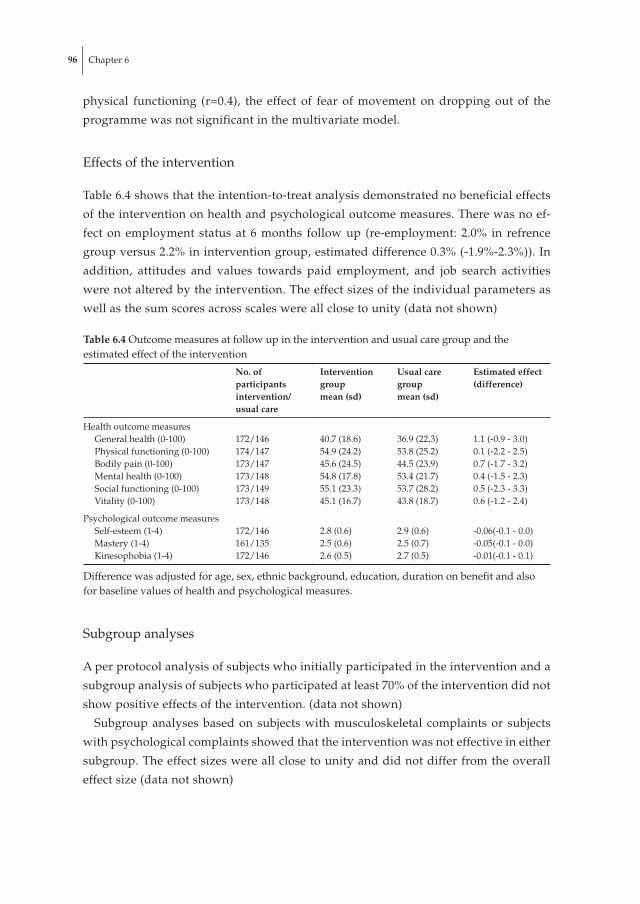
96 Chapter6
physical functioning (r=0.4), the effect of fear of movement on dropping out of the
programmewasnotsignificantinthemultivariatemodel.
Effectsoftheintervention
Table6.4showsthattheintention-to-treatanalysisdemonstratednobeneficialeffects
oftheinterventiononhealthandpsychologicaloutcomemeasures.Therewasnoef-
fectonemployment statusat 6months followup (re-employment: 2.0% in refrence
groupversus2.2%ininterventiongroup,estimateddifference0.3%(-1.9%-2.3%)).In
addition, attitudes and values towards paid employment, and job search activities
werenotalteredbytheintervention.Theeffectsizesoftheindividualparametersas
wellasthesumscoresacrossscaleswereallclosetounity(datanotshown)
Subgroupanalyses
Aperprotocolanalysisofsubjectswhoinitiallyparticipatedintheinterventionanda
subgroupanalysisofsubjectswhoparticipatedatleast70%oftheinterventiondidnot
showpositiveeffectsoftheintervention.(datanotshown)
Subgroupanalysesbasedonsubjectswithmusculoskeletal complaintsor subjects
withpsychologicalcomplaintsshowedthattheinterventionwasnoteffectiveineither
subgroup.Theeffectsizeswereallclosetounityanddidnotdifferfromtheoverall
effectsize(datanotshown)
Table 6.4 Outcomemeasuresatfollowupintheinterventionandusualcaregroupandtheestimatedeffectoftheintervention
no. of participants intervention/usual care
intervention groupmean (sd)
usual care groupmean (sd)
estimated effect (difference)
HealthoutcomemeasuresGeneralhealth(0-100)Physicalfunctioning(0-100)Bodilypain(0-100)Mentalhealth(0-100)Socialfunctioning(0-100)Vitality(0-100)
172/146174/147173/147173/148173/149173/148
40.7(18.6)54.9(24.2)45.6(24.5)54.8(17.8)55.1(23.3)45.1(16.7)
36.9(22.3)53.8(25.2)44.5(23.9)53.4(21.7)53.7(28.2)43.8(18.7)
1.1(-0.9-3.0)0.1(-2.2-2.5)0.7(-1.7-3.2)0.4(-1.5-2.3)0.5(-2.3-3.3)0.6(-1.2-2.4)
PsychologicaloutcomemeasuresSelf-esteem(1-4)Mastery(1-4)Kinesophobia(1-4)
172/146161/135172/146
2.8(0.6)2.5(0.6)2.6(0.5)
2.9(0.6)2.5(0.7)2.7(0.5)
-0.06(-0.1-0.0)-0.05(-0.1-0.0)-0.01(-0.1-0.1)
Differencewasadjustedforage,sex,ethnicbackground,education,durationonbenefitandalsoforbaselinevaluesofhealthandpsychologicalmeasures.

Ch
apte
r6
Effectivenessofahealthpromotionprogrammeforlong-termunemployedsubjectswithhealthproblems 97
Effectofaco-intervention
During the follow-up of 6 months, 80 subjects in the intervention group (23%) and
56 subjects in the reference group (19%) started with a job search training. This co-
interventiondidnotinfluencetheobservedlackofanyeffectoftheintervention.
Discussion
Thehealthpromotionprogrammedidnotshowpositiveeffectsonperceivedmental
andphysicalhealth,selfesteem,mastery,andfearofmovement.Inaddition,values
andattitudestowardspaidemployment,jobsearchactivities,andemploymentstatus
atsixmonthsfollowupwerenotaffectedbythehealthprogrammeeither.
Therearethreepossiblereasonswhytheinterventionwasnoteffective:1)thestudy
couldnotdemonstrateaneffectduetomethodologicallimitations;2)theintervention
wasnotsuccessfullyimplemented;or3)theinterventionwasindeednoteffectivein
thisform.
Methodologicallimitations
Eligibleparticipantswererandomizedbefore theywereapproachedbytheresearch
team for participation in the study. This procedure was necessary since the City of
Rotterdamrequiredanimmediatereferraltoanemploymentservicewithoutfurther
administrative delay.As a consequence of this procedure, the non response on the
firstquestionnaireafterrandomizationwasrelativelyhigh.Theresponsetothefirst
questionnairewasslightlyhigherintheinterventiongroup(74%)comparedwiththe
referencegroup(68%).Receivinganinvitationtoparticipate inahealthprogramme
mayhaveinfluencedthedecisiontofilloutthequestionnaire,butthishadlittleinflu-
enceonthecomparabilityofinterventionandreferencegroup.
Datacollectionwasconductedcompletelyindependentfromtheinterventionpro-
gramme and regular vocational rehabilitation, since participation in these activities
waspartlymandatory,whereasparticipationinthisstudywascompletelyvoluntary.
Asa consequence, somesubjectswho filledout thequestionnairedidnot takepart
in the intervention, whereas other subjects took part in the intervention but did
not respond on the questionnaire. For most subjects the reason for not taking part
in the intervention or the vocational rehabilitation was unknown, although a small
proportion was due to termination of the benefits for different reasons (moving in
withapartnerormovingoutofthecityofRotterdam).However,participationinthe
interventionwasnot influencedbypersonal characteristics, employmenthistory,or

98 Chapter6
perceived health. Therefore, it is assumed that there was no selection bias in initial
participationintheprogramme.
Thepowercalculationwasbasedon196subjectspergroupwithcompletedatacol-
lection.Infact,theachievedsamplewasconsiderablyless.Sincetheestimatedeffects
of the interventionwereclose tounity forallparameters,a largerstudypopulation
wouldnothaveresultedinstatisticallysignificanteffectsoftheintervention.There-
fore,itisassumedthatthefailuretodetectbetween-groupdifferencesisnotduetoa
lackofpowerofthestudy.
In this study perceived health was an important outcome measure, whereas the
focusoftheinterventionprogrammewasalsoonimprovingobjectivephysicalhealth.
Intheinterventiongroupitwasshownthatabettercardiorespiratoryfitnessdidnot
resultinabetterperceivedhealth.[31]
Anothermethodologicalreasonfornotfindinganyeffectofthehealthprogramme
mayhavebeentheabsenceofanassessmentofchangeimmediatelyaftertheendof
the intervention.Theoretically, there couldhavebeenapositiveeffectonhealthdi-
rectlyaftertheprogrammewasfinished,whichhadalreadyfadedawayatthetimeof
followup,onaverageaboutthreemonthsaftertheprogrammetermination.However,
thiswouldimplyalackofsustainabilityoftheintervention.Inthedesignofthestudy
avocational trainingdirectlyaftertheendof thehealthprogramwasthoughttobe
abletosustainpositiveeffectsoftheintervention.However,inpracticethevocational
trainingwasoftendelayedordidnotstartatall.Duetoorganisationalproblemsofthe
socialsecurityserviceandvocationalrehabilitationcentresonly23%oftheinterven-
tiongroupand19%ofthecontrolgroupstartedwithavocationaltrainingwithinthe
followupperiodofsixmonths.Thislackoffollow-upactivitiesconcerningvocational
rehabilitationcanbeconsideredasanimplementationfailureandmayhaveinterfered
withourresults.
Theinterventionwasnotsuccessfullyimplemented
The intervention was offered during two years in eight periods with three groups
perperiod.Intotal,22groupsstartedwiththeprogrammewith11to22participants
pergroup.Theoretically,eachprogrammeconsistedof12weeksofmultidisciplinary
rehabilitation.Inpractice,however,participantsreceivedonlynineweeksofeffective
training,sincethreeweekswerelostduetothetimeittookfortheintroductionand
intakeandouttakeactivities.
Participationinthehealthprogrammewasmandatory,butthesocialsecurityservice
ofthecityofRotterdamdidnotstrictlyenforceactualparticipation.Themandatory
naturehasundoubtedlyresultedinan increasedparticipation.Participantswhofell
obligedto join,maynothaveexperiencedaneedto improvetheirhealth.Feedback

Ch
apte
r6
Effectivenessofahealthpromotionprogrammeforlong-termunemployedsubjectswithhealthproblems 99
provided by the physical education teachers indicated that getting participants in-
volvedwasamajorchallengeinitselfandthatanincreaseintrainingeffortinatime-
contingentmannerwillcertainlynothavebeenachievedbyallparticipants.Hence,
thegradedactivityprinciplewasnotadheredtoforallparticipants.
Interviewswithtenparticipantsandthetrainersrevealedthatthecognitivetraining
wasnotwelladaptedtothisstudypopulationofpersonswithloweducationandlow
socio-economicstatus.Bothtrainersandparticipantsacknowledgedthatthecognitive
training should be improved with less focus on theory and being more adapted to
experiencesindailylifeoftheparticipants.
Among the persons who initially started with the intervention, 72% completed
the programme with more than 70% attendance to all sessions offered. Hence, the
interventionhadagoodreachamongsubjectswhoareusuallydifficulttoengagein
healthpromotionactivities.Only28%didnotsucceedtoparticipateinatleast70%
oftheprogrammeactivities.Participantswithapoorphysicalandmentalhealthand
high fear of movement at baseline had a higher chance of dropping out during the
programmecomparedtopersonswithagoodhealthandnofearofmovement.This
mayhaveaffectedtheeffectivenessofthehealthprogramme,becausethosepersons
whocouldpotentiallybenefit themostdroppedoutof theprogramme.However,a
subgroupanalysisof thesubjectswhoparticipated inat least70%ofall sessions in
theprogrammeversus thereferencegroup,didnotshowanypositiveeffectsof the
intervention.
Theinterventionwasindeednoteffectiveinthisform.
A systematic review concluded that only intensive (>100 hours) multidisciplinary
rehabilitationwillreducepainandimprovefunctioninpatientswithchroniclowback
pain.[32]Basedon this criterion, it is assumed that the intensityofourprogramme
was high enough (around 108 hours), but the subgroup analysis showed that par-
ticipantswithlowbackpaindidnotimproveintheirpain,physicalfunction,orany
of theotheroutcomemeasures in thecurrentstudy.Bendixetal.[12]showedthata
multidisciplinaryintensiveprogrammethatranfor3successiveweeksof39hoursper
weekwaseffective,whereasthehealthprogrammeunderstudyranfor12successive
weekswith9-12hoursperweek.Amoreintensiveprogrammewithashorterduration
maybemoreeffectivethanalessintensiveprogrammewithalongerduration.
Ananticipatedresultofthehealthprogrammewasahigherre-employmentinthe
interventiongroup.Amultidisciplinaryrehabilitationprogramme,describedbyWat-
sonetal.[18],withastrongfocusonimprovementintheabilitytoworkandonactual
return towork, showed thatat6months follow-up38%of subjectswereemployed
and another 23% were in voluntary work of education/training. In contrast, in the

100 Chapter6
healthprogrammeofferedinRotterdamreturntoworkwasnotpartoftheindividual
goalsetting.Thelackofastrongintegrationofthehealth-orientedinterventioninto
the regular vocational rehabilitation activities may have impeded beneficial effects.
Pateletal. [33]hassuggested thatmultidisciplinaryapproachesshouldnotonlybe
concerned with medical and psychological issues, but should also address the ob-
staclestoreturntoworkasseenbythepatient.
Theprocessevaluationshowedthatafter theendof theprogramme,mostpeople
fellbackintotheiroldlifestylewithlowlevelsofphysicalactivity. Inordertohave
sustainableeffectsofahealthpromotionprogramme,itisimportantthatparticipants
continuetobephysicallyactive.Theabsenceofasustainedeffortbyhealthcounsel-
lorsafterterminationoftheinterventiontoencourageparticipantstostayphysically
activemayhavecontributedtothefactthatnohealtheffectswerefound.
In conclusion, the intervention aimed at the promotion of physical and mental
healthofunemployedpersonswithhealthcomplaintsdidnotshowanybeneficialef-
fects.Thus,itcannotberecommendedtoimplementthisparticularhealthpromotion
programmetocounteractatindividuallevelthenegativeeffectsofunemploymenton
health.Measuresonsocietalleveltoreducethenegativeeffectsofunemploymenton
populationhealtharerequired [11]. Inpolicies forhealthequity, it remainsofpara-
mount importance todevelopmeasures to includepeoplewithapoorhealth in the
labourmarket.
Acknowledgements
FundingforthisstudywasprovidedbythePublicHealthFund(FondsOGZ)ofthe
Netherlands(reg.nr.P161).Wegratefullyacknowledgethededicationoftheprofes-
sionalsprovidingthehealthpromotionprogramme(Ergocontrol)andtheircontinu-
oussupporttothisstudy.

Ch
apte
r6
Effectivenessofahealthpromotionprogrammeforlong-termunemployedsubjectswithhealthproblems 101
ReFeRences
1. ClaussenB:Healthandre-employmentinafive-yearfollow-upoflong-termunemployed.Scand J Public Health 1999,27:94-100.
2. JanlertU:Unemploymentasadiseaseanddiseasesoftheunemployed.Scand J Work Environ Health 1997,23Suppl3:79-83.
3. MorrisJK,CookDG,ShaperAG:Lossofemploymentandmortality.BMJ (Clinical research ed 1994,308:1135-1139.
4. BartleyM,SackerA,ClarkeP:Employmentstatus,employmentconditions,andlimitingillness:prospectiveevidencefromtheBritishhouseholdpanelsurvey1991-2001.Journal of epidemiology and community health 2004,58:501-506.
5. SchuringM,BurdorfA,KunstAE,MackenbachJP:Theeffectofillhealthonenteringandmaintainingpaidemployment:evidenceinEuropeancountries.Journal of epidemiology and community health 2007,61:597-604.
6. ThomasC,BenzevalM,StansfeldSA:Employmenttransitionsandmentalhealth:ananalysisfromtheBritishhouseholdpanelsurvey.Journal of epidemiology and community health 2005,59:243-249.
7. WarrP,JacksonP:Adaptingtotheunemployedrole:alongitudinalinvestigation.Soc Sci Med 1987,25:1219-1224.
8. PriceRH,ChoiJN,VinokurAD:Linksinthechainofadversityfollowingjobloss:howfinancialstrainandlossofpersonalcontrolleadtodepression,impairedfunctioning,andpoorhealth.Journal of occupational health psychology 2002,7:302-312.
9. EdenD,AviramA:Self-efficacytrainingtospeedreemployment:Helpingpeopletohelpthemselves.Journal of Applied Psychology 1993,78:352-360.
10. CottCA,GignacMA,BadleyEM:DeterminantsofselfratedhealthforCanadianswithchronic disease and disability. Journal of epidemiology and community health 1999, 53:731-736.
11. CreedPA:Improvingthementalandphysicalhealthofunemployedpeople:whyandhow?Med J Aust 1998,168:177-178.
12. BendixAF,BendixT,OstenfeldS,BushE,Andersen:Activetreatmentprogramsforpatientswithchroniclowbackpain:aprospective,randomized,observer-blindedstudy.Eur Spine J 1995,4:148-152.
13. ClaussenB,BjorndalA,HjortPF:Healthandre-employmentinatwoyearfollowupoflongtermunemployed.Journal of epidemiology and community health 1993,47:14-18.
14. LakkaTA,KauhanenJ,SalonenJT:Conditioningleisuretimephysicalactivityandcardiore-spiratoryfitnessinsociodemographicgroupsofmiddle-agesmenineasternFinland.Int J Epidemiol 1996,25:86-93.
15. PedersenBK,SaltinB:Evidenceforprescribingexerciseastherapyinchronicdisease.Scand J Med Sci Sports 2006,16Suppl1:3-63.
16. TurnerJA,JensenMP,RomanoJM:Dobeliefs,coping,andcatastrophizingindependentlypredictfunctioninginpatientswithchronicpain?Pain 2000,85:115-125.
17. RoseV,HarrisE:Fromefficacytoeffectiveness:casestudiesinunemploymentresearch.J Public Health (Oxf) 2004,26:297-302.
18. WatsonPJ,BookerCK,MooresL,MainCJ:Returningthechronicallyunemployedwithlowbackpaintoemployment.Eur J Pain 2004,8:359-369.

102 Chapter6
19. Gatchel RJ, PengYB, Peters ML, Fuchs PN, Turk DC: The biopsychosocial approach tochronicpain:scientificadvancesandfuturedirections.Psychol Bull 2007,133:581-624.
20. LindstromI,OhlundC,EekC,WallinL,PetersonLE,FordyceWE,NachemsonAL:Theef-fectofgradedactivityonpatientswithsubacutelowbackpain:arandomizedprospectiveclinicalstudywithanoperant-conditioningbehavioralapproach.Phys Ther 1992,72:279-290;discussion291-273.
21. FordyceW:Behavioralmethodsforchonicpainandillness.StLouis:Mosby.1976. 22. OsteloRW,KokeAJ,BeurskensAJ,deVetHC,KerckhoffsMR,VlaeyenJW,WoltersPM,
Berfelo MW, van den Brandt PA: Behavioral-graded activity compared with usual careafterfirst-timedisksurgery:considerationsofthedesignofarandomizedclinicaltrial.J Manipulative Physiol Ther 2000,23:312-319.
23. CBS:Herkomstvanpersonen;allochtonenenmigratie[Countryoforiginofpersons;mi-grantsandmigration].CentraalBureauvoordeStatistiek,Voorburg/Heerlen2003.
24. WareJE,Jr.,SherbourneCD:TheMOS36-itemshort-formhealthsurvey(SF-36).I.Concep-tualframeworkanditemselection.Med Care 1992,30:473-483.
25. VanderZeeKI,SandermanR:HetmetenvandealgemenegezondheidstoestandmetdeRAND-36: een handleiding [Measuring health status with the RAND-36: a manual]. InGroningen:NoordelijkCentrumvoorGezondheidsvraagstukken,RijksuniversiteitGron-ingen.1993.
26. FayersPM,SprangersMA:Understandingself-ratedhealth.Lancet 2002,359:187-188. 27. PearlinLI,SchoolerC:Thestructureofcoping.J Health Soc Behav 1978,19:2-21. 28. RosenbergM:Societyandtheadolescentself-image.Princeton: Princeton University Press
1965. 29. VlaeyenJWS,KoleSnijdersAMJ,BoerenRGB,vanEekH:Fearofmovement/(re)injuryin
chroniclowbackpainanditsrelationtobehavioralperformance.Pain 1995,62:363-372. 30. HollisS,CampbellF:Whatismeantbyintentiontotreatanalysis?Surveyofpublished
randomisedcontrolledtrials.BMJ (Clinical research ed 1999,319:670-674. 31. SchutgensCAE,SchuringM,VoorhamAJ,BurdorfA:Changesinphysicalhealthamong
participantsinamultidisciplinaryhealthprogrammeforlong-termunemployedpersons.BMC Public Health2009,9:197.
32. GuzmanJ,EsmailR,KarjalainenK,MalmivaaraA,IrvinE,BombardierC:Multidisciplinaryrehabilitationforchroniclowbackpain:systematicreview.BMJ (Clinical research ed 2001,322:1511-1516.
33. PatelS,GreasleyK,WatsonPJ:Barrierstorehabilitationandreturntoworkforunemployedchronicpainpatients:aqualitativestudy.Eur J Pain 2007,11:831-840.
7changes in physical health among participants
in a multidisciplinary health programme
for long-term unemployed persons
SchutgensCAE,SchuringM,VoorhamAJJ,BurdorfA.
BMC Public Health 2009, 9:197

104 Chapter7
absTRacT
background: Therelationshipbetweenpoorhealthandunemploymentiswellestab-
lished.Healthpromotionamongunemployedpersonsmayimprovetheirhealth.The
aims of this study were to investigate characteristics of non-participants and drop-
outs inamultidisciplinaryhealthpromotionprogrammefor long-termunemployed
personswithhealthcomplaints,toevaluatechangesinphysicalhealthamongpartici-
pants,andtoinvestigatedeterminantsofimprovementinphysicalhealth.
methods:Alongitudinal,non-controlleddesignwasused.Theprogrammeconsisted
of twoweeklyexercisesessionsandoneweeklycognitivesessionduring12weeks.
Themainoutcomemeasureswerebodymassindex,bloodpressure,cardiorespiratory
fitness,abdominalmusclestrength,andlowbackandhamstringflexibility.Potential
determinantsofchangeinphysicalhealthweredemographicvariables,psychological
variables(self-esteem,mastery,andkinesiophobia),andself-perceivedhealth.
Results:Theinitialresponsewas73%and252personshadcompletedatacollection
at baseline. In total, 36 subjects were lost during follow-up. Participants were pre-
dominantly loweducated, long-termunemployed,and inpoorhealth.Participation
in theprogrammewasnot influencedbydemographicandpsychological factorsor
by self-reportedhealth.Drop-outswereyoungerandhada lowerbodymass index
at baseline than subjects who completed the programme.At post-test, participants’
cardio respiratory fitness, abdominal muscle strength, and flexibility had increased
by6.8%-51.0%,whereasdiastolicandsystolicbloodpressureshaddecreasedby2.2%-
2.5%.Theeffectsizesrangesfrom0.17-0.68.
conclusions: Participants with the poorest physical health benefited most from the
programmeandsexdifferencesinimprovementwereobserved.Physicalhealthofun-
employedpersonswithhealthcomplaintsimprovedafterparticipationinthishealth
promotionprogramme,butnotsufficiently,consideringtheirpoorphysicalhealthat
baseline.

Ch
apte
r7
Changesinphysicalhealthamongparticipantsinamultidisciplinaryhealthprogramme 105
inTRoDucTion
Therelationshipbetweenunemploymentandpoorerhealthhasbeenwellestablished.
[1-3] This relationship is bi-directional with both a selection mechanism with poor
health reducing the likelihood on paid employment, and a causation mechanism
wherebyunemploymentwillresultsinapoorerhealth.[1,4]Theseassociationsmay
bemediatedbyothervariables,suchashealthbehaviourandpsychosocialvariables.
Alowself-esteem,forinstance,isadeterminantofself-reportedpoorhealth[5]and
alsodecreasesthelikelihoodofemployment.[6-8]Thus,unemploymentmayleadto
poorerhealth,whichinturnreducesthechancesofreemployment.
In order to improve the possibility for reemployment, improvement in health of
unemployed persons may, therefore, be an important step. Pedersen and Saltin [9]
haveconcludedintheirextensivereviewthatexercisetherapyhaspositiveeffectson
maximumoxygenuptake(VO2max),musclestrength,generalwell-being,bloodpres-
sure,weight,bodyfatpercentage,anddepressivesymptomsofpersonswithchronic
diseases.Thereissomeevidencethatphysicalandmentalhealthareinterrelatedand
thatdeterminantsofphysicalhealthmayalsopositivelyaffectmentalhealthandvice
versa.Masteryorthesenseofcontroloverone’slife,andself-esteemhavebeenassoci-
atedwithabetterself-reportedphysicalhealth.[5]
There is, however, limited research into the effects of exercise-based programmes
among groups with a poor health in a low socio-economic position. A low socio-
economic position and a poor health have consistently been associated with non-
participation and drop-out in health programmes. [10-14] In addition to this, it is
importanttoidentifydeterminantsofnon-compliancewhichmayinfluencetheeffects
ofexerciseprogrammes.[15]
Watson and colleagues [16] provided some indications that a combined physical
exerciseandcognitivebehaviouralprogrammeimprovedphysical fitnessaswellas
increasedemploymentratesamongunemployedparticipants.Theseresultsshouldbe
interpretedwithcaution,however,sincethevoluntaryparticipationintheprogramme
mighthavebiasedtowardsparticipantswithahighmotivationandapositiveattitude
towards(returnto)work.
Thereisaclearneedformoreinsightintowaystoimprovehealthofpersonsina
lowsocio-economicposition.Anintensive,multidisciplinaryhealthprogrammewas
developedforunemployedpersonswithhealthcomplaints(“Workonyourhealth”),
consistingofphysicalexerciseandcognitivetraining,withthegoaltoimprovephysi-
calandmentalhealthasacontributiontoincreasetheopportunitiesonpaidemploy-
ment.Theaimsofthepresentstudywere(1)toidentifythefactorsthatdetermined
non-participation,drop-out, andnon-compliance inahealthpromotionprogramme

106 Chapter7
forunemployedpersons, (2) to evaluate the changes inphysicalhealthamongpar-
ticipants,and(3)toinvestigatethedeterminantsofimprovementinphysicalhealth.
meTHoDs
Studydesignandpopulation
A longitudinal, non-controlled design was used among participants in a health
promotion programme. Unemployed persons with chronic health complaints were
referred by the Employment Centre of the City of Rotterdam, The Netherlands, for
a fit-to-work test, conductedbyaphysician,psychologist,andanemploymentspe-
cialist.Participantswereselectedonthebasisofthefollowingcriteria:unemployed,
diagnosed with chronic health complaints by the physician or a psychologist, but
consideredtobecapableoffulltimeemployment,andbeingatleastmoderatelyable
to understand and speak Dutch. From December 2004 until December 2007 partici-
pantswereincludedinthestudy.Theinvitationtoparticipateinthehealthpromotion
programmewassendoutbytheproviderofthisprogramme,withasupportingletter
fromthecityofRotterdamstipulatingthatattendingtheprogrammeforatleast70%
wasmoreorlessmandatory,andthatrefusalmightresultinacutinthesocialbenefits
received.Theresearchgroupcarriedoutthecurrentevaluationstudyandparticipa-
tionwasstrictlyvoluntary.Beforethestartoftheprogramme,participantsweresenta
questionnaireandprepaidreturnenvelope.ForthosewithaTurkishlastname(alarge
ethnic minority), a Turkish version of the questionnaire was sent as well. Another
largeethnicminoritygrouparetheMoroccanpeople.However,itwasnotpossibleto
makeaMoroccan-ArabicquestionnairebecausethemajorityoftheMoroccansinthe
NetherlandsspeakBerber,whichisnotawrittenlanguage.Aftertwoandfourweeks,
reminderlettersandquestionnairesweresenttotheparticipants.If,afterfourweeks,
still no questionnaire had been sent back, an interviewer visited the home address.
Whenfourvisitsduringdifferenthoursinatwo-weekperiodwerenotsuccessful,a
participant was considered a non-respondent. The interviewers were matched with
subjects,basedonethnicity,age,andsex,andcouldofferaninterviewinthemother
tongue (Dutch, Arabic, or Turkish). The Medical Ethics Committee of the Erasmus
MC,Rotterdamapprovedthestudy.
Of the 465 subjects who were invited to take part in the health promotion pro-
gramme, 338 participated in an assessment to evaluate medical and psychological
eligibility tostart theprogramme(response73%).Thereasons fornon-participation
(n=127)werenotreceivingasocialsecuritybenefitanymore(n=14),beingallocatedto
areintegrationoreducationalprogramme(n=24),andunknown(n=89).Inaddition,

Ch
apte
r7
Changesinphysicalhealthamongparticipantsinamultidisciplinaryhealthprogramme 107
22individualsweredeclaredmedicallyunfittosuccessfullyparticipateinthephysical
trainingandanother5individualswereexcludedformajorpsychologicalproblems.
Intotal,311personsstartedtheprogramme,ofwhich252alsofilledoutthequestion-
nairesendoutbytheresearchteam.Intotal,216outof252individualscompletedthe
health promotion programme (86%) and 36 subjects were lost to follow-up (Figure
7.1).
Theprogramme
Theinterventionwasaimedatchangingthewayunemployedpersonsperceiveand
cope with their health complaints. The rationale was based on the biopsychosocial
modelofchronicpainandsubsequentinterdisciplinarypainmanagementapproach.
Patients with chronic pain are at increased risk for emotional disorders (such as
Invited to participate in programmeN= 465
Participated in intake (medical & psychological assessment)N = 338
No longer benefit (n=14)Reintegration programme (n=24)Unknown (n=89)
Started programmeN = 311
Declared medically unfit (n=22)Declared psychologically unfit (n=5)
Filled out questionnaire N = 252
No questionnaire (n=59)
Available post-testN = 216
Lost to follow-up (n=36)
Figure 7.1 Flowdiagramofparticipationinthehealthpromotionprogramme

108 Chapter7
anxiety,depressions,andanger),maladaptivecognitions(suchascatastrophizingand
poorcopingskills),functionaldeficitsandphysicaldeconditioning(duetodecreased
physicalactivityandfearofinjury).Theseeffectsareofteninterdependent,sothatone
cannotsimplytreatonetotheexclusionofothers.Interdisciplinarypainmanagement
embracesthefactthatthecomprehensivetreatmentofallthesedimensionsisneeded
inordertobeeffective.[17]
Thehealthpromotionprogrammeconsistedofthreesessionsofthreehoursevery
week during a twelve-week period. One session a week was focused on cognitions
andtwoweeklysessionswerefocusedonphysicalactivity.Thecognitivecomponent
wasdesignedtoenhanceparticipants’ insightintheirhealthcomplaints(e.g.move-
mentmaybepainful,thoughharmless)andhowtocopewiththesecomplaints,toen-
hanceself-esteemandfeelingsofmastery,toreducefearandavoidanceofmovement,
andtoimprovesocialfunctioningbylearningtothinkpositivelyandincreasesocial
skills.Thecognitivecomponent,conductedbytwopreventionworkers,wasprimar-
ilyfacilitatingthephysicalactivitypartoftheintervention.Theexerciseprogramme
consistedof1.5hoursfitnesstrainingtwiceaweek(cardioandweighttraining),1.5
hoursof indoorsportsweekly,and1.5hoursofoutdooractivitiesweekly.Thispart
of theprogrammewasprimarilydesigned to improvephysical fitness.Theexercise
programmewasdevelopedaccordingtothegraded-activityprinciple.Theexercises
started below the average functional capacity assessed during the first session and
wereincreasedgraduallyduringthecourseoftheintervention,accordingtothetime-
contingencyprinciple.Thesesessionswereconductedbyphysicaleducationteachers.
Theinterventioncostswereapproximately€2300perparticipantwhoenrolledinthe
programme.
Outcomemeasures
Sevenphysicalhealthindicatorsweremeasuredatstartandendoftheprogrammeby
theprovideroftheprogramme:BodyMassIndex(BMI)inkg/m²,bodyfatpercent-
age,systolicanddiastolicbloodpressure,cardiorespiratoryfitness,abdominalmuscle
strength,andlowbackandhamstringflexibility.Bodyfatpercentagewasdetermined
bymeansofabioelectricalimpedanceanalysiswithabodyfatmeter.[18]Bloodpres-
sure(mmHG)wasmeasuredwithanautomaticsphygmomanometerattheleftwrist.
Cardio respiratory fitness was measured by the Åstrand Ergometer Bicycle test
of maximum oxygen absorption (VO2max in ml/kg/minute) (Åstrand and Kodahl,
1986).Participantscycledonabicycleergometerwithaconstantpeddlingrateof70-
75rotations/minute.Theworkloadwasadjustedtotheparticipant’sheartrate,which
had tobeapproximately120beatsperminuteafter twominutes.Subsequently, the
participantcycledforsixminutes.Iftheheartratefluctuatedmorethanfivebeatsin

Ch
apte
r7
Changesinphysicalhealthamongparticipantsinamultidisciplinaryhealthprogramme 109
thelastminute,thetestwasprolongeduntilasteadypulsewasobtainedforatleast
oneminute.VO2maxwasestimatedonbasisoftheaverageheartrateinthelastmin-
ute,workload,sex,andage.Thetestwascarriedoutunderstandardizedconditions
withthetemperaturebetween18and20°Candatmospherichumiditybetween40and
60%.Beforethetest,participantsrestedfiveminutes,andtheyhadtoabstainfromeat-
ing,drinkingcoffee,andsmokingfortwohours,fromalcoholfortwelvehours,and
fromvigorousphysicalactivityandsunbathingforsixhours. If theparticipantwas
notabletocyclewithaheartrateof120beatsperminuteoriftheheartrateexceeded
170beatsperminute,thetestwasterminated.
Abdominalmusclestrengthwasdeterminedasthenumberofsit-upsperminute,
withkneesbent(90°)andfootsandhandsonthefloor.Shouldershadtostayabove
thefloorduringthetest.Handshadtoreachalineat7.5cmfromthestartingposi-
tion (Fitness Canada). Low back and hamstring flexibility (cm) was measured with
a sit-and-reach test, selecting the best of three trials. Participants placed their foot
soles, without shoes, against the end of a box.Arms were stretched forward as far
aspossiblewithunbentkneesand the reachwasdetermined (cm)on thebox scale
(FitnessCanada).
Determinants
Determinants of (change in) health were demographic characteristics (sex, age,
educationallevel,ethnicity,andmaritalstatus),durationofunemployment,mastery,
self-esteem,kinesiophobia,andself-perceivedhealth.Educationallevelwasmeasured
asthehighestlevelofeducationalattainmentinthreecategories.Ahigheducational
level was defined as higher vocational training or university, intermediate educa-
tionallevelashighersecondarytrainingorintermediatevocationaltraining,andlow
educationallevelasnoeducation,primaryschool,lowerandintermediatesecondary
trainingorlowervocationaltraining.Ethnicitywasbasedonthemother’scountryof
origin;incasethemotherwasnativeDutch,thefather’scountryoforiginwaslead-
ing.Fourethnicgroupsweredefined:NativeDutch,TurkishandMoroccan,Antillean
andSurinamese,andother.TurkishandMoroccanpeoplehaveasimilarimmigration
history with limited acculturation.Antillean and Surinamese people originate from
former Dutch colonies and are reasonably integrated in Dutch society by virtue of
speakingDutch.Theotherethnicgroupisaheterogeneousmixtureofalargenumber
ofnationalities.Maritalstatusdistinguishedbetweensubjectslivingwithoutapartner
andsubjectsbeingmarriedorlivingwithapartner.
MasterywasmeasuredbythePersonalMasteryScale[19],whichconsistsofseven
items (eg “I have little control over the things that happen to me”, “There is little
I can do to change many of the important things in my life”), answered on a four

110 Chapter7
point Likert scale (strongly agree to strongly disagree).Average scores across items
were calculated, ranging from 1 to 4, with a higher score indicating a higher level
of mastery. In case three or more items were unanswered, no score was computed
(Cronbach’salpha=0.69).
Self-esteemwasmeasuredwiththeRosenbergSelf-EsteemScale[20],with10items
(e.g.,“Onthewhole,Iamsatisfiedwithmyself”,“Allinall,Iaminclinedtofeelthat
I am a failure”), answered on a four point Likert scale (strongly agree to strongly
disagree).Averagescoresacross itemswerecalculatedagain, ranging from1 to4;a
higherscoreindicatedahigherlevelofself-esteem.Incasethreeormoreitemswere
unanswered,noscorewascomputed(Cronbach’salpha=0.84).
Kinesiophobia was measured with the Tampa Scale of Kinesiophobia [21], which
consists of 17 items on fear of movement and injury (e.g. “It’s really not safe for a
personwithaconditionlikeminetobephysicallyactive”,“PainalwaysmeansIhave
injuredmybody”)onafourpointLikertscale(stronglyagreetostronglydisagree).
Averagescoresacrossitemswereagaincalculated,rangingfrom1to4,withahigher
scoreindicatingahigherlevelofkinesiophobia.Incasefiveormoreitemswereunan-
swered,noscorewascomputed(Cronbach’salpha=0.80).
Self-perceivedhealthwasmeasuredwiththeShortForm36HealthSurvey(SF-36)
[22]. The SF-36 consists of 36 questions about health, covering eight dimensions:
physical functioning, general health, mental health, bodily pain, social functioning,
vitality,role limitationduetoemotionalhealthproblems,androle limitationdueto
physicalhealthproblems.Scoresmayrangefrom0to100withahigherscoreindicat-
ingabetter self-perceivedhealth.
Tomeasureprogrammecompliance,participants’trainingattendancerecordswere
kept.Subjectswereconsideredcompliantwhentheyattendedatleast70%ofallses-
sions.Thecut-offpointof70%attendanceofallsessionswasinlinewiththepolicy
of the social security services, which demanded an attendance of at least 70% from
participants.
Statisticalanalyses
AllstatisticalanalyseswereconductedbymeansofthestatisticalpackageSPSS(ver-
sion13)forWindowsandthelevelofsignificancewassetat0.05.
Differences between participants and non-participants, between drop-outs and
completers,andbetweencompliersandnon-complierswereevaluatedbychisquare
testsandone-wayanalysesofvariance.
The dependent measures of physical health in the statistical analyses were BMI,
bodyfatpercentage(%),systolicanddiastolicbloodpressures(mmHg),VO2max(ml/
kg/minute),abdominalmusclestrength(sit-ups/minute),andflexibility(cm).Toin-

Ch
apte
r7
Changesinphysicalhealthamongparticipantsinamultidisciplinaryhealthprogramme 111
vestigatewhichdeterminantswereassociatedwiththesemeasuresofphysicalhealth
atbaseline,univariate linearregressionanalyseswereconductedwithdemographic
characteristics,psychological factors,andself-perceivedhealthas independentvari-
ables.Subsequently,independentvariablesofinterest(p-value<0.10)wereincluded
inthemultipleregressionanalysisforeachphysicaloutcomemeasureandvariables
were retained in the final multivariate linear regression model when statistically
significant (p < 0.05) or statistically significant in a multivariate model on another
outcome measure. For each independent variable based on an average score across
items also the standardized regression coefficient was calculated, representing the
effectofanincreaseofonestandarddeviationintheaveragescoreonthemagnitude
oftheoutcomemeasure.Allanalyseswerecorrectedforthedurationbetweenthedate
offillingoutthequestionnaireandthedateofcollectingthephysicalhealthmeasures
inthetest.BodyfatpercentagecorrelatedhighlywithBMI(r=0.72)and,hence,only
BMI was further analysed. Mastery correlated with self-esteem (r = 0.46) and the
inclusionofbothvariablesinthesamemodelcreatedproblemswithmulticollinear-
ity, resulting in substantially higher confidence intervals and, thus, non-significant
results. Self-esteem was strongest associated with the outcome measures of interest
and selected for further presentation. The SF-subscales were interrelated (r varying
from0.25to0.63).Basedontheunivariateanalyses,physicalfunctioningwaschosen,
sinceithadthestrongestassociationswithseveraloutcomemeasures.
The changes in physical health during the health promotion programme were
evaluatedbysixpaired-samples t-testsandCohen’sdwascalculatedasmeasureof
effectsizebydividingthedifferencesbetweenpre-testandpost-testbytheirpooled
standarddeviation.[23]Duetoregressiontothemean,thephenomenonthatextreme
scoresfallbacktowardstheaveragewhenmeasuredagain,theinitialvalueatbaseline
willbeassociatedwiththeobservedchangeovertime.[24-25]Inordertoinvestigate
whetherchanges inphysicalhealthwereduetoregressionto themeanor todiffer-
entialresponsetothehealthpromotionprogramme,themeasuresofphysicalhealth
at baseline were classified into three categories: below 25% percentile, interquartile
range (p25-p75), and above 75% percentile. Regression to the mean will be present
when subjects with a poor physical health (lower quartile) improve and subjects
withagoodphysicalhealth(upperquartile)deterioratelikewise.Inlinearregression
analyseswithrepeatedmeasurements,thedeterminantsofimprovementinphysical
healthwereevaluatedbyintroducinginteractiontermsoftheinitialphysicalhealth
values,expressedascategoricalvariables,withtimeofmeasurementasfixedeffects
in the analysis. Similarly, interaction terms of significant determinants of physical
health at baseline with time of measurement were investigated, adjusted for initial
values of physical health. In these analyses the random variance components were
pooledacrossalldeterminantsandassumedtobeequalacrosstime.Thisassumption

112 Chapter7
ofacompoundsymmetrycovariancestructureresulted in themost restrictiveerror
structure possible, necessary because of the small number of subjects available for
somephysicalhealthmeasures.
ResuLTs
Baselinecharacteristicsoftheparticipants
Ofallparticipantswithcompletebaselineinformation(n=252),46%wasmale,75%
belongedtoanethnicminority,68%hadalowlevelofeducation,and72%reported
beingunemployedforat least5yearsorhadneverworked(Table7.1).Onaverage,
participants had a low self-perceived health, a low VO2max, and the prevalence of
overweight and obesity was high. No correlations were found between SF-36 sub-
scalesandphysicalhealthoutcomemeasures,exceptforabdominalmusclestrength
(physicalfunctioning:r =0.24,mentalhealth:r =0.20,generalhealth:r =0.16).
Characteristicsofnon-participants,drop-outs,andnon-compliers
Based on the information obtained by the questionnaires, subjects who started the
healthprogrammedidnotdifferstatisticallysignificantlyfromnon-participantswith
respect to demographic and psychological variables and self-perceived health. Sub-
jectswhocompletedtheprogramme(ie,attendedbothpre-testandpost-test)hada
higherBMIatbaseline(2.33,95%CI0.26-4.41)andwereolder(3.98,95%CI0.78-7.18)
thandrop-outs.Ofallsubjectswhocompletedtheprogramme,82%attendedatleast
70%ofthesessions.Compliantpersonshadastatisticallysignificantlyhigherphysical
functioning(7.97,95%CI0.15-15.78)andlesskinesiophobia(0.23,95%CI0.07-0.39)at
baselinethannon-compliantpersons.
Determinantsofphysicalhealthatbaseline
Sex, age, marital status, self-esteem, and self-perceived physical functioning were
determinants forphysicalhealthatbaseline,althoughnot foralloutcomemeasures
(Table7.2).Ethnicity,levelofeducation,unemploymentduration,andkinesiophobia
didnothaveasignificantcontribution.Theexplainedvariancewas lowest for flex-
ibility(R²=7.4%)andhighestforVO2max(R²=31.8%).Halfofthesubjectswerenot
abletofinishtheÅstrandErgometerBicycletestandfailurewasassociatedwitholder
age,lowerselfesteemandlowerphysicalfunctioning.

Ch
apte
r7
Changesinphysicalhealthamongparticipantsinamultidisciplinaryhealthprogramme 113
Table 7.1 Characteristicsofunemployedpersonswithhealthcomplaints(n=252)whoenrolledinahealthpromotionprogramme
variable
Demographiccharacteristics
Men 46.4%
Age(yr) 42.11(9.12)
Marriedorlivingwithpartner 35.2%
EthnicbackgroundNativeDutchTurkish/MoroccanSurinamese/AntilleanOther
24.9%25.7%29.0%20.4%
LevelofeducationLowIntermediateHigh
67.9%28.8%3.3%
Unemploymentduration(n=245)<5years>5yearsNeverworked
27.4%53.5%19.1%
Psychologicalmeasures
Self-esteem(1-4) 2.85(0.56)
Mastery(1-4) 2.45(0.55)
Kinesiophobia(1-4)(n=239) 2.68(0.47)
Self-perceivedhealth(SF-36)
Physicalfunctioning 52.69(23.11)
Rolefunctioning(physical) 32.18(39.66)
Bodilypain 41.39(23.42)
Vitality 43.74(16.03)
Socialfunctioning 53.64(25.88)
Rolefunctioning(emotional) 48.43(44.58)
Mentalhealth 53.00(18.85)
Generalhealth 37.62(18.23)
Physicalmeasures
BMI(kg/m2)overweight(25<=BMI<30)obese(BMI>=30)
27.61(5.68)32.9%29.4%
VO2max(ml/kg/minute)(n=130) 24.60(7.85)
Abdominalmusclestrength(sit-ups/minute)(n=216) 21.13(13.69)
Flexibility(cm)(n=223) 23.70(10.94)
Systolicbloodpressure(mmHg) 130.33(17.42)
Diastolicbloodpressure(mmHg) 82.96(10.89)

114 Chapter7
Changesinphysicalhealth
Participantsintheprogrammeshowedsignificantdecreasesindiastolicandsystolic
blood pressure by 2.2%-2.5% and significant increases in cardio respiratory fitness,
flexibility,andabdominalmusclestrengthby6.8%-51.0%(Table7.3). Effectsizeswere
smalltomedium(Cohen’sdrangedfrom0.17to0.68).Inaddition,theproportionof
participantsthatwasabletocompletethebicycletestincreasedfrom52%atbaseline
to71%atfollow-up.
Table 7.2 Determinantsofphysicalhealth†atbaselineamongunemployedpersonswhoenrolledinahealthpromotionprogramme(n=252)basedonmultivariatelinearregressionanalyses
bmi vo2max(n = 130)
abdominal muscle strength
Flexibility systolic blood pressure
Diastolic blood pressure
Constant 26.26 41.08 14.13 17.97 97.66 67.04
Female 2.51** -3.91** -4.50** 4.04** -4.03 -0.51
Age(yr) 0.05 -0.36** -0.22** -0.09 0.52** 0.19**
Marriedorlivingwithpartner 2.08** -1.04 -6.67** -1.59 1.66 -0.28
Self-esteem(1-4) 0.71 -1.49 0.20 0.64 3.85* 3.79**
Physicalfunctioning(0-100) -0.01 0.05* 0.12** 0.08* -0.02 -0.05
Explainedvariance(R²) 8.9% 31.8% 15.6% 7.4% 9.8% 8.9%
*0.05<=P <=0.10,**P <0.05.†BMI(kg/m2),VO2max(ml/kg/minute),abdominalmusclestrength(sit-ups/minute),flexibility(cm),diastolicandsystolicbloodpressures(mmHg).
Table 7.3 Changesinphysicalhealthamongunemployedpersonswhoparticipatedinahealthpromotionprogramme
outcome measure Pre-test mean (sD)
Post-test mean (sD)
change (95% ci)
effect size (cohen’s d)
change (%)
BMI(n=216) 27.93(5.76) 27.86(5.70) -0.03(-0.12-0.06) 0.01 -0.1%
VO2max(n=97) 24.27(7.77) 25.60(8.08) 1.64**(0.53-2.76) 0.21 6.8%
Abdominalmusclestrength(n=196)
21.56(13.97) 31.24(17.94) 10.99**(9.02-12.96) 0.68 51.0%
Flexibility(n=191) 23.83(11.00) 25.10(10.68) 1.99**(1.17-2.81) 0.18 8.4%
Systolicbloodpressure(n=216)
130.63(17.57) 127.23(16.20) -3.28**(-5.48--1.08) 0.19 -2.5%
Diastolicbloodpressure(n=216)
83.39(10.98) 81.57(10.79) -1.83**(-3.40--0.26) 0.17 -2.2%
*0.05<=P <=0.10,**P <0.05,pairedt-test.

Ch
apte
r7
Changesinphysicalhealthamongparticipantsinamultidisciplinaryhealthprogramme 115
Determinantsofimprovementinphysicalhealth
Significant interactiontermsofsexwithtimeandbaselinevaluesofphysicalhealth
and time were consistently observed. Table 7.4 shows that men improved more in
VO2max, flexibility,andsystolicbloodpressure,whereaswomen improvedmore in
abdominal muscle strength. The effect of the category 25%-75% percentile of initial
physicalhealthdescribestheaverageimprovementinthestudypopulation,adjusted
forage,andwasclosetotheobserveddifferencesintable3.ForVO2max,abdominal
muscle strength, and flexibility, a statistically significant trend was observed with
subjectswithaninitiallylowerscoreonphysicalhealthimprovingmorethansubjects
with a better physical health. For systolic and diastolic blood pressure a strong re-
gressiontothemeanwasobservedwiththelowestgroupimprovingandthehighest
groupdeteriorating.
Discussion
Atthestartoftheprogramme,participantswereinpoorphysicalhealth,considering
theirlowVO2maxandthehighprevalenceofoverweightandobesity.Physicalhealth
oftheparticipantsimprovedsignificantly,exceptforBMI.Participants’cardiorespira-
toryfitness,abdominalmusclestrength,andflexibilityhadincreasedby6.8%-51.0%,
whereasdiastolicandsystolicbloodpressureshaddecreasedby2.2%-2.5%.Theeffect
sizesrangesfrom0.17-0.68,indicatingsmalltomoderateeffects.Participantswiththe
poorest physical health benefited most from the programme and sex differences in
improvementwereobserved.
Table 7.4 Determinantsofchangesinphysicalhealth†amongunemployedpersonswhoparticipatedinahealthpromotionprogramme(n=216)estimatedbymultivariatelinearregressionanalyseswithrepeatedmeasurements
change in vo2max
change in abdominal muscle strength
Flexibility systolic blood pressure
Diastolic blood pressure
Baselinevalue<25%percentile25%-75%percentile>75%percentile
3.37**2.06**-0.85
13.44**10.59**9.31**
3.61**2.00**0.25
8.33**-3.10-13.80**
5.22**-1.84-8.06**
SexMenWomen
2.19**1.23
10.30**11.59**
2.57**1.53**
-4.23**-2.46
-1.31-2.27**
*0.05<=P <=0.10,**P <0.05,pairedt-test.†VO2max(ml/kg/minute),abdominalmusclestrength(sit-ups/minute),flexibility(cm),diastolicandsystolicbloodpressures(mmHg).

116 Chapter7
Theparticipationinthishealthprogrammewas73%(n=338),whichwashigherthan
reportedinotherstudiesamonglowsocio-economicgroups[10,14]orinthegeneral
population.[13]Thehighparticipationwaspartlyduetothemoreorlesscompulsory
nature,whichmayalsoexplainthelackofanydifferencesbetweenparticipantsand
non-participants on demographic, psychological, or self-perceived health measures.
ParticipantswhocompletedtheprogrammehadahigherinitialBMIthandrop-outs,
indicatingthatthesubjectswhoneededtheprogrammethemostwerealsomostlikely
tofinishit.
Participantsintheprogrammewereaparticularlyunhealthygroup.Theprevalence
ofoverweightandobesitywas33%(n=83)and29%(n=74)respectively,ascompared
to40%and10%inthegeneralDutchpopulation.[26]Cardiorespiratoryfitnesswason
average30%lowerthaninhealthy,untrainedreferencegroups.[27]Inaddition,self-
perceivedhealthwasapproximately30%lowerthanarandomsampleofinhabitants
ofthesamecity(datanotshown).Althoughtheparticipants’physicalimprovements
werepromising,thechangesweregenerallymodest,andconsideringthepoorhealth
at baseline, the programme did not succeed to improve the participants’ physical
health to theaveragevalue in thegeneralDutchpopulation.Approximately25%of
therequiredimprovementwasreached.
Previous studies have shown similar improvements in physical health with flex-
ibilityincreasingwith9%afteraworksitehealthpromotionprogramme[28]anda3%
decreaseinsystolicanddiastolicbloodpressureafteranexerciseprogrammeamong
adults. [29] Slightly higher increases in maximum oxygen absorption have been re-
portedafterexerciseprogrammesamongdiabeticpatients(11.8%)[30]inobesewomen
(15%)[31],andstrokepatients (10%). [32]Bodymass indexremainedunchangedin
ourstudy,whichmaybeexplainedbythefactthatfoodintakewasnotaddressedin
theprogramme[28].Animportantconsiderationiswhetheralongerdurationofthe
programmeormoresessionsaweekwouldhaveresultedinlargergainsinphysical
health.Arecentreviewonseveralmodalitiesofphysicaltrainingprogrammesamong
diabeticpatientsshowedthattheinfluenceofprogrammedurationwaslimited,but
ahigherexerciseintensitywasassociatedwithgreaterincreaseinVO2max.[30]This
maybeconsideredasaguidelineforfutureexerciseprogrammes.
The improvement in physical health was predominantly associated with sex and
initialvalueofphysicalhealth,whereastrainingattendancenoranyofthedetermi-
nantsofphysicalhealthatbaselinewerenotassociatedwithimprovementsinphysi-
calhealth.Thefindingthatindividualsinpoorestphysicalconditionbenefitedmost
fromtheinterventionisinaccordancewithpreviousresearchintodecreasesinblood
pressure. [29,33]Forbloodpressureastrongregression to themeanwasobserved,
whereby subjects with high blood pressure decreased and subjects with low blood
pressureincreased.[24]Despitethisregressiontothemean,theimprovementamong

Ch
apte
r7
Changesinphysicalhealthamongparticipantsinamultidisciplinaryhealthprogramme 117
subjectswith intermediatebloodpressure indicates theoverall improvementdueto
participationinthehealthpromotionprogramme.
Theresultsarepromising,however, since theyare inaccordancewith findingsof
similar exercise interventions, even though subjects were not voluntarily enrolled
in the programme, and participants’ health improved consistently on all outcome
measures.Anearlier studyonunemployedpeoplewith lowbackpain [16] showed
improvements inphysicalhealthaswell,butmayhavebeenbiasedduetotheself-
selectionofmotivatedsubjects.Anotherlimitationisthelackofappropriateprocess
information on the implementation of the graded-activity principle in the physical
exercises.Feedbackprovidedbythephysicaleducationteachersindicatesthatgetting
theparticipantsinvolvedwasamajorchallengeinitselfandthatanincreaseintrain-
ingeffortwill certainlynothavebeenachievedbyallparticipants.Thismaypartly
explaintherathermoderategainsincardiorespiratoryfitness.Athirdweaknessofthis
studywasthechoiceforthebicycletestasmeasureofcardiorespiratoryfitness.At
baseline,halfoftheparticipantswerenotabletocarryoutthebicycletest.Thelackof
bikingskillsamongnon-Dutchpeoplemayhaveplayedarole,butalsoamongnative
Dutchpersonsatoolowcardiorespiratoryfitnesswasobservedtocarryoutthetest.
Personswhowerenotabletocarryoutthebicycleergometerpre-testdidnotdropout
oftheintervention,butwereallowedtoparticipateintheintervention.However,for
estimatingtheeffectoftheinterventiononcardiorespiratoryfitnesstheseparticipants
werenotincluded.Atpost-testsomeoftheparticipantswhowerenotabletocareout
the pre-test, where indeed able to carry out the post-test. The higher proportion of
participantcompleting this testat follow-up indicates that the improvement inVO-
2maxwillhavebeenunderestimated.Furthermore,itcannotbeexcludedthatpractice
effectsunderlietheimprovementsonabdominalmusclestrengthandflexibility.
Datacollectionwasconductedcompletelyindependentfromtheinterventionpro-
gramme,sinceattendingtheprogrammewasmoreorlessmandatorywhereaspartici-
pationinthisstudywascompletelyvoluntary.Asaconsequence,somesubjectswho
filledoutthequestionnairedidnottakepartintheprogramme,whereasothersubjects
tookpartintheprogrammebutdidnotrespondonthequestionnaire.Therefore,the
evaluationisbasedonlesspersons(46%,n=216)thanwhatwouldbeexpectedbased
ontheparticipation(73%)anddrop-outs(14%).
Persons with a low educational level and/or a non-Dutch origin may have had
difficultieswithfillingoutthequestionnaireduetoilliteracyordifficultieswiththe
Dutch language. To overcome these problems interviewers were used in this study.
The interviewers could offer an interview in the mother tongue (Dutch,Arabic, or
Turkish). However, the validity of the questionnaires may be less good for persons
withanon-Dutchoriginorlowliteracy,duetodifferencesininterpretationofques-
tionscausedbyculturaldifferences.

118 Chapter7
No associations between objective physical health and self-perceived health (SF-
36)werefoundinthisstudy.Itwasassumedthatbyimprovingphysicalhealthand
fitness, self-perceived physical and mental health would also increase. The lack of
anyassociationbetweenperceivedhealthandobjectivephysicalhealth,asmeasured
by cardio respiratory fitness, has been observed in several other studies. [34-35]
Perceivedhealthmaybeinfluencedbycognitions,forexamplethewaypeoplecope
with theirhealthproblems.Althoughphysicalhealthand self-reportedhealthwere
notmeasuredatexactly thesameday, timebetweenbothmeasurementsatbaseline
hadnoinfluenceonthelackofassociation.Duetothislackofassociation,itmightbe
questionedwhetherfocusingonphysicalhealthisthebestwaytoachievethemuch
needed improvement in self-reported health in this study population with health
complaintsthatwereoftenmentionedasabarriertostriveat(re)employment.Nev-
ertheless,improvementofphysicalhealthbyobjectivemeasurementsisbeneficialfor
thehealthstatus.
Toinvestigatetheeffectofthisinterventiononre-employmentasubstantiallylonger
follow-upperiodisneeded.However,weexpectthattheeffectoftheprogrammeon
re-employmentwillbemodestduetothefactthatphysicalfunctioningattheendof
theprogrammeisstillbelowtheaveragevalueinthegeneralDutchpopulation.
Thisstudyaddressesphysicalhealthwithinparticipantsofanexerciseprogramme.
TheoverallresultsoftheRCTongeneralhealthandsocialfunctioningispublished
elsewhere.[36]Schuring[36]foundthatthecurrenthealthpromotionprogrammedid
notshowbeneficialeffectsonperceivedhealth,psychologicalmeasures,workvalues,
job search activities or re-employment. This lack of positive effects of the interven-
tion, despite of the increased physical health, may be due to the fact that physical
functioningattheendoftheprogrammeisstillbelowtheaveragevalueinthegeneral
Dutchpopulationandthedurationoftheinterventionwasquitelimitedwithrespect
tosecondaryoutcomemeasuressuchasre-employment.Inadditiontothis,theseout-
comemeasureswereinvestigatedatleastthreemonthsaftertheendoftheprogram,
thebeneficialeffectsofthehealthprogrammemaybefadedawaybythattimedueto
alackoffollowupactivitiestosustainpossiblehealthbenefits.
Attheendoftheinterventionprogrammesemi-structuredinterviewswereunder-
taken with ten participants and ten trainers to obtain more qualitative insight into
differentaspectsoftheinterventionthatcouldbeimprovedinthefuture.Theprocess
evaluationshowedthataftertheendoftheprogramme,mostsubjectsfellbackinto
their old lifestyle with low levels of physical activity. In order to have sustainable
effects of a health promotion programme, it seems important for these participants
tohavecontinuedsupervisionandsupporttobeabletomaintainamorephysically
activelifestyle.

Ch
apte
r7
Changesinphysicalhealthamongparticipantsinamultidisciplinaryhealthprogramme 119
Thehealthsituationofunemployedpeoplemaydependonsocialandlabourmarket
policieswhichvaryacrossEuropeancountries.InthepastdecadesintheNetherlands,
healthproblemswereoftenalegitimatereasonforreceivingunemploymentbenefits.
Thesebenefitsareregardedsufficientlyhightocoverbasiccostsforalllivingexpenses.
Therefore,lessthan10%ofdisabledpersonshavetheirmainsourceofincomethrough
labour,whereasinSwedenthisproportionamountstoover50%.[37]Hence,results
fromstudiesconcerninghealthandemploymentstatusintheNetherlandsmaynotbe
easilybegeneralizedtoanotherEuropeancountry.
Conclusions
This study showed that (1) participation in a health promotion programme among
unemployed persons was not influenced by individual characteristics, but younger
personsweremorelikelytodropout,(2)physicalhealthmeasuredbycardiorespira-
toryfitnessincreasedonaverageby7%,and(3)participantswiththepooresthealth
at baseline benefited most from the programme. Although the health programme
consisting of an exercise and a cognitive component improved the health of unem-
ployedpersons,thisimprovementwasnotsufficientlyenoughtoraisephysicalhealth
tolevelsobservedamongindividualsinthegeneralpopulation.
Acknowledgements
FundingforthisstudywasprovidedbythePublicHealthFund(FondsOGZ)ofthe
Netherlands.

120 Chapter7
ReFeRences
1. BartleyM,SackerA,ClarkeP:Employmentstatus,employmentconditions,andlimitingillness:prospectiveevidencefromtheBritishhouseholdpanelsurvey1991-2001.Journal of epidemiology and community health 2004,58:501-506.
2. ThomasC,BenzevalM,StansfeldSA:Employmenttransitionsandmentalhealth:ananalysisfromtheBritishhouseholdpanelsurvey.Journal of epidemiology and community health 2005,59:243-249.
3. WilsonSH,WalkerGM:Unemploymentandhealth:areview.Public health 1993,107:153-162. 4. SchuringM,BurdorfA,KunstAE,MackenbachJP:Theeffectofillhealthonenteringand
maintainingpaidemployment:evidenceinEuropeancountries.Journal of epidemiology and community health 2007,61:597-604.
5. CottCA,GignacMA,BadleyEM:DeterminantsofselfratedhealthforCanadianswithchronic disease and disability. Journal of epidemiology and community health 1999, 53:731-736.
6. VinokurAD,SchulY:MasteryandinoculationagainstsetbacksasactiveingredientsintheJOBSinterventionfortheunemployed.Journal of Consulting and Clinical Psychology 1997,65:867-877.
7. CreedPA:Improvingthementalandphysicalhealthofunemployedpeople:whyandhow?Med J Aust 1998,168:177-178.
8. WatersLE,MooreKA:Self-esteem,appraisalandcoping:Acomparisonofunemployedandre-employedpeople.Journal of Organizational Behavior 2002,23:593-604.
9. PedersenBK,SaltinB:Evidenceforprescribingexerciseastherapyinchronicdisease.Scand J Med Sci Sports 2006,16Suppl1:3-63.
10. ChinnDJ,WhiteM,HowelD,HarlandJO,DrinkwaterCK:Factorsassociatedwithnon-participationinaphysicalactivitypromotiontrial.Public health 2006,120:309-319.
11. OleskeDM,KwasnyMM,LavenderSA,AnderssonGB:Participationinoccupationalhealthlongitudinalstudies:predictorsofmissedvisitsanddropouts.Annals of epidemiology 2007,17:9-18.
12. ProctorTJ,MayerTG,TheodoreB,GatchelRJ:Failuretocompleteafunctionalrestorationprogram for chronic musculoskeletal disorders: a prospective 1-year outcome study.Archives of physical medicine and rehabilitation 2005,86:1509-1515.
13. ToftUN,KristoffersenLH,AadahlM,vonHuthSmithL,PisingerC,JorgensenT:Dietandexerciseinterventioninageneralpopulation--mediatorsofparticipationandadherence:theInter99study.European journal of public health 2007,17:455-463.
14. WilburJ,McDevittJ,WangE,DancyB,BrillerJ,IngramD,NicolaT,LeeH,ZenkSN:Re-cruitmentofAfricanAmericanwomentoawalkingprogram:eligibility,ineligibility,andattritionduringscreening.Research in nursing & health 2006,29:176-189.
15. WinterEM,FowlerN:ExercisedefinedandquantifiedaccordingtotheSystemeInternationald’Unites.Journal of sports sciences 2009,27:447-460.
16. WatsonPJ,BookerCK,MooresL,MainCJ:Returningthechronicallyunemployedwithlowbackpaintoemployment.Eur J Pain 2004,8:359-369.
17. Gatchel RJ, PengYB, Peters ML, Fuchs PN, Turk DC: The biopsychosocial approach tochronicpain:scientificadvancesandfuturedirections.Psychol Bull 2007,133:581-624.

Ch
apte
r7
Changesinphysicalhealthamongparticipantsinamultidisciplinaryhealthprogramme 121
18. LukaskiHC,JohnsonPE,BolonchukWW,LykkenGI:Assessmentoffat-freemassusingbioelectricalimpedancemeasurementsofthehumanbody.The American journal of clinical nutrition 1985,41:810-817.
19. PearlinLI,SchoolerC:Thestructureofcoping.J Health Soc Behav 1978,19:2-21. 20. RosenbergM:Societyandtheadolescentself-image.Princeton: Princeton University Press
1965. 21. VlaeyenJWS,KoleSnijdersAMJ,BoerenRGB,vanEekH:Fearofmovement/(re)injuryin
chroniclowbackpainanditsrelationtobehavioralperformance.Pain 1995,62:363-372. 22. WareJE,Jr.,SherbourneCD:TheMOS36-itemshort-formhealthsurvey(SF-36).I.Concep-
tualframeworkanditemselection.Med Care 1992,30:473-483. 23. CohenJ:Statisticalpoweranalysisforthebehavioralsciences(2nded.).Hillsdale, NJ: Law-
rence Earlbaum Associates 1988. 24. BlandJM,AltmanDG:Someexamplesofregressiontowardsthemean.BMJ (Clinical research
ed 1994,309:780. 25. ChesterMR,BlandM,ChenL,KaskiJC:Therelationshipbetweenchangeandinitialvalue:
thecontinuingproblemofregressiontothemean.European heart journal 1995,16:289-290. 26. BlokstraA,SchuitAJ:Factsheetovergewicht.Prevalantieentrend[Factsheetoverweight.
Prevalenceandtrend].Bilthoven: Rijksinstituut voor Volksgezondheid en Milieu 2003. 27. ShvartzE,ReiboldRC:Aerobicfitnessnormsformalesandfemalesaged6to75years:a
review.Aviation, space, and environmental medicine 1990,61:3-11. 28. LiCL,TsengHM,TsengRF,LeeSJ:Theeffectivenessofanaerobicexerciseintervention
on worksite health-related physical fitness--a case in a high-tech company. Chang Gung medical journal 2006,29:100-106.
29. WheltonSP,ChinA,XinX,HeJ:Effectofaerobicexerciseonbloodpressure:ameta-analysisofrandomized,controlledtrials.Annals of internal medicine 2002,136:493-503.
30. BouleNG,KennyGP,HaddadE,WellsGA,SigalRJ:Meta-analysisoftheeffectofstructuredexercisetrainingoncardiorespiratoryfitnessinType2diabetesmellitus.Diabetologia 2003,46:1071-1081.
31. KraemerWJ,VolekJS,ClarkKL,GordonSE,IncledonT,PuhlSM,Triplett-McBrideNT,Mc-BrideJM,PutukianM,SebastianelliWJ:Physiologicaladaptationstoaweight-lossdietaryregimenandexerciseprogramsinwomen.J Appl Physiol 1997,83:270-279.
32. PangMY,EngJJ,DawsonAS,McKayHA,HarrisJE:Acommunity-basedfitnessandmobil-ityexerciseprogramforolderadultswithchronicstroke:arandomized,controlledtrial.Journal of the American Geriatrics Society 2005,53:1667-1674.
33. PescatelloLS,FranklinBA,FagardR,FarquharWB,KelleyGA,RayCA:AmericanCollegeofSportsMedicinepositionstand.Exerciseandhypertension.Medicine and science in sports and exercise 2004,36:533-553.
34. SorensenLE,PekkonenMM,MannikkoKH,LouhevaaraVA,SmolanderJ,AlenMJ:Asso-ciationsbetweenworkability,health-relatedqualityof life,physicalactivityandfitnessamongmiddle-agedmen.Applied ergonomics 2008,39:786-791.
35. SmeetsRJ,WittinkH,HiddingA,KnottnerusJA:Dopatientswithchroniclowbackpainhave a lower level of aerobic fitness than healthy controls?: are pain, disability, fear ofinjury,workingstatus,or levelof leisure timeactivityassociatedwith thedifference inaerobicfitnesslevel?Spine 2006,31:90-97.

122 Chapter7
36. SchuringM,BurdorfA,VoorhamAJ,derWeduweK,MackenbachJP:Effectivenessofahealthpromotionprogrammeforlong-termunemployedsubjectswithhealthproblems:arandomizedcontrolledtrial.Journal of epidemiology and community health 2009,63:893-899.
37. LakkaTA,KauhanenJ,SalonenJT:Conditioningleisuretimephysicalactivityandcardiore-spiratoryfitnessinsociodemographicgroupsofmiddle-agesmenineasternFinland.Int J Epidemiol 1996,25(1):86-93.

8General discussion


Ch
apte
r8
Generaldiscussion 125
8. GeneRaL Discussion
Therelationshipbetweenunemploymentandpoorhealthhasbeenwellestablished,
as demonstrated by a higher prevalence of illness and disability[1-2] and a higher
mortalityamongunemployedpersons.[3]Selectionandcausationmaycontributeto
theseinequalitiesinhealthamongemployedandunemployedpersons.Accordingto
theselectionhypothesisworkerswithapoorhealthmaybemorelikelytoleavethe
labourforce.Inaddition,unemployedpersonswithapoorhealthmaybelesslikely
toentertheworkforce.Thecausationhypothesissuggeststhatleavingtheworkforce
mayhaveanegativeinfluenceonhealthandthatgainingpaidemploymentmayhave
apositiveinfluenceonhealth.
Theobjectivesofthisthesisarethreefold:
1. To study the influence of poor health on entering (b) and maintaining (a) paid employment.
2. To study the influence of entering paid employment on different dimensions of perceived
health.
3. To evaluate the effectiveness of a health promotion programme among unemployed subjects
with health complaints on physical and mental health and re-employment.
8.1 main FinDinGs
In a descriptive study among unemployed inhabitants of the city of Rotterdam the
largesthealthinequalitiesbetweenemployedandunemployedpersonswereobserved
for native Dutch persons, whereas among persons with a non-Dutch origin, health
inequalities between employed and unemployed persons were less pronounced.
(Chapter2)
8.1.1HealthandWork
Objective 1a: To describe the influence of poor health on maintaining paid employment.
Inthisthesisapoorhealthwasdefinedaslessthangoodhealth.Alongitudinalstudy
with 2-year follow-up in the population aged over 50 years in 11 European Union
countries (SHARE) showed that the health status of older European workers had a
majorinfluenceonthelikelihoodofleavingtheworkforce.Apoorhealthwasarisk
factorforthetransitiontounemployment,retirementordisabilitypensionwithodd
ratiosvaryingfrom1.5to5.0.(Chapter3)

126 Chapter8
Secondary data-analysis on five waves (1994-1998) of the European Community
HouseholdPanel(ECHP)surveyontheworking-agepopulationin11Europeancoun-
tries also showed that transitions from paid employment to various forms of non-
employmentwereinfluencedbyhealth.Theeffectofpoorhealthontheprobabilityof
leavingtheworkforcewaslesspronouncedinmoredistantyearsandwasinfluenced
bysocio-economicvariables.Apoorhealthwasariskfactorforbecomingunemployed
orretiring,especiallyamonghighlyeducatedworkers.(Chapter4)
Objective 1b: To describe the influence of poor health on entering paid employment.
AprospectivestudyamongunemployedcitizensofthecityofRotterdamshowedthat
apoorperceivedhealthreducedtheprobabilityofenteringpaidemployment.Almost
alldimensionsofhealthatbaselinehadaninfluenceonthelikelihoodofenteringpaid
employment. The strongest association was found between physical functioning at
baselineandre-employment.(Chapter5)
TheaforementionedanalysisoffivewavesoftheECHPstudysupportedthefind-
ing that a poor health had a negative influence on the likelihood of entering paid
employment.Theeffectofpoorhealthonthelikelihoodofbecomingemployedwas
influencedbysocio-economiccharacteristics.Apoorhealthwasariskfactorfornot
enteringpaidemploymentamongmen,buthadlesseffectamongwomen.Theeffect
ofpoorhealthonenteringpaidemploymentwasconsistentlypresentuptofouryears
beforetheactualtransitiontookplace.Thehealthstatusamongunemployedsubjects
withpoorhealthremainedratherstableovertimeand,hence,hadalong-termeffect
ontheprobabilityofenteringpaidemployment.(Chapter4)
InmostEuropeancountries,apoorhealthwasariskfactorforleavingtheworkforce
andstayingunemployed,but largedifferencesamongcountrieswereobserved that
could partly be explained by the unemployment rate at national level. In countries
with a low national unemployment rate health competed with other labour market
factorsintheprocessofenteringorretainingpaidemployment,whereasincountries
withahighnationalunemploymentratetheeffectofhealthselectionoutofthework-
forcewasrelativesmallcomparedtootherfactorsthatdeterminelabouropportunities
forpersons.(Chapter4)
Inconclusion,apoorhealthofEuropeanworkersincreasedthelikelihoodofleaving
theworkforceduetounemployment,retirement,disabilitypension,ortakingcareof
ahousehold.Theeffectofpoorhealthontheprobabilityofleavingpaidemployment
waslesspronouncedinmoredistantyears.Unemployedsubjectswithapoorhealth
atbaselinewerealsolesslikelytoreturntopaidemployment.Almostalldimensions
ofhealth,butespeciallyphysical functioning,hadan influenceon the likelihoodof
entering paid employment. The effect of poor health on entering paid employment
Ch
apte
r8
Generaldiscussion 127
wasconsistentlypresentup to fouryearsbefore theactual transition tookplace. In
mostEuropeancountries,poorhealthwasariskfactorforleavingpaidemployment
andstayingunemployed,butlargedifferencesamongcountrieswereobserved.
8.1.2WorkandHealth
Objective 2: To determine the influence of entering paid employment on different dimensions
of perceived health.
A prospective study among unemployed subjects receiving social security benefits,
who were capable of full time employment and were referred to a re-employment
centre in theCityofRotterdam, showed that5%of theparticipants (47/965) found
paidemploymentduringthefollow-upperiodofsixmonths.Amongthere-employed
participants all self-reported dimensions of health increased, with estimated effect
sizes varying from 0.1 to 0.7. The largest relative improvements were observed for
mental health, social functioning, and role-limitations due to emotional or physical
problems, whereas physical functioning showed the smallest relative improvement.
Allparticipantswerereferredtoatrainingcentreforare-employmenttraining.How-
ever,only30%oftheparticipantsactuallystartedwithare-employmenttraining.This
re-employmenttrainingdidnothaveapositiveeffectonthechanceofre-employment
oronthehealthstatusofparticipants.(Chapter5)
Inconclusion,amongre-employedpersonsalldimensionsofhealthimproved,with
thelargestimprovementformentalhealth,withinashortperiodofsixmonths.
8.1.3Healthpromotionoftheunemployed
Objective 3: To evaluate the effectiveness of a health promotion programme among unemployed
subjects with health complaints on physical and mental health and re-employment.
In a randomised controlled trial (RCT) the effectiveness of a health promotion pro-
grammeamongunemployedsubjects(n=921)withhealthcomplaintsreceivingsocial
security benefits from the city of Rotterdam was evaluated. The RCT showed that
thehealthpromotionprogrammehadnobeneficialeffectonself-reportedmentaland
physical health, self esteem, mastery, and pain-related fear of movement of unem-
ployedpersonswithhealthcomplaints.Inaddition,valuesandattitudestowardspaid
employment, job search activities, and employment status at six months follow up
werenotaffectedbythehealthprogrammeeither.(Chapter6)
The study among participants who received the intervention showed that cardio
respiratoryfitnessincreasedonaverageby7%.However,thisimprovementwasnot

128 Chapter8
sufficient to raise cardio respiratory fitnessofparticipants to levelsobserved in the
generalpopulation.(Chapter7)
Inconclusion,a randomisedcontrolled trial showed thatahealthpromotionpro-
grammeamongunemployedpersonswithhealthproblemsdidnot showbeneficial
effectsonself-reportedphysicalandmentalhealthandre-employment.
8.2 meTHoDoLoGicaL LimiTaTions
8.2.1HealthandWork
The SHARE study showed that the health status of older workers at baseline was
associatedwithemploymentstatustwoyearslater.(Chapter3)However,thisstudy
givesnoinsightintothetimewindowoftheinfluenceofapoorhealthontheprob-
ability to leave the workforce. The study includes only two measurements and the
exact moment of the employment transition within these two measurements is
unknown.Therefore,apoorhealthmayhaveanimmediateordelayedinfluenceon
theemploymenttransitionfromemploymenttonon-employment.Interruptedtime-
series with repeated measurements over longer periods can give more insight into
the time-dynamics of the influence of health on the transition from employment to
non-employment.TheECHPstudywasbasedonfivemeasurementsandshowedthat
the proportion of persons with a good health decreased among those who left the
workforce in theyearsbefore theemployment transition. (Chapter4)Therefore, the
ECHP study corroborates the findings of the SHARE study that a poor health is a
determinantoflabourforceexit.
TheECHPstudyshowedthattherewerelargevariationsbetweenEuropeancoun-
triesintheassociationbetweenillhealthandvariousformsofexitfrompaidemploy-
ment.[4]Duetosmallnumbers,thecountry-specificanalysesmaybelessreliablethan
theanalysisbasedon11Europeancountries.Thesevariationsmayreflectdifferences
between countries in institutional arrangements, e.g. the availability of disability
benefitschemesforthosewithhealthproblems.TheECHPstudyshowedthatalower
unemploymentrateatnationallevelwasassociatedwithlargereffectsofpoorhealth
onnotenteringpaidemploymentorbecomingunemployed.Thesestructuralfactors
atnationallevelmayalsoinfluenceresultswithinonecountry,suchasthestudiesthat
wereconductedintheCityofRotterdam,witharelativelyhighunemploymentrate
comparedtootherregionsoftheNetherlands.(Chapter2,5)

Ch
apte
r8
Generaldiscussion 129
8.2.2WorkandHealth
AprospectivestudyamongunemployedcitizensoftheCityofRotterdamshowedan
increaseofhealthamongthosewhostartedwithpaidemploymentwithintheshort
follow-upperiod.(Chapter5)Duetotheobservationaldesignofthestudytheresults
mayhavebeeninfluencedbyselectionbias.Subjectswhofoundemploymentdiffered
fromthosewhostayedunemployedwithrespect tohealthatbaselineandpersonal
characteristics.Thesevariableswereadjustedforintheanalysis,buttheremayhave
beenothervariablesthatinfluencedbothhealthchangeandre-employmentthatwere
notincludedintheanalysis.
Theprospectivestudyconsistedoftwomeasurementsinbetweenwhichtheevent
ofenteringpaidemploymenttookplace.Basedonthesefinding,itseemsmostlikely
thatstartingwithpaidemploymentresultsinhealthimprovement.However,dueto
thedesignofthestudyitcannotberuledoutthatitistheotherwayaround;achange
inhealth statusmay increase the likelihoodof findingpaidemployment.However,
areviewshowedthatanincreaseinhealthstatusoflong-termunemployedisrather
unlikely.[2]Interruptedtime-serieswithrepeatedmeasurementscangivemoreinsight
intothetime-dependenttrendofhealthstatusbeforeenteringpaidemploymentand
theinfluenceofenteringpaidemploymentonthistrendofhealthstatus.
8.2.3Healthpromotionoftheunemployed
Arandomisedcontrolledtrialshowedthatahealthpromotionprogrammeaimedat
promotion of self-reported physical and mental health and re-employment among
unemployedpersonswithhealthproblemsdidnotshowbeneficialeffects.(Chapter6)
Thehealthprogrammemayhavehadnoeffectonself-reportedphysicalandmental
healthbecauseofalackofsustainabilityoftheintervention.Inthedesignofthestudy
avocationaltrainingdirectlyaftertheendofthehealthprogrammewasthoughttobe
abletosustainpositiveeffectsoftheintervention.However,inpracticethevocational
training was often delayed or did not start at all. This lack of follow-up activities
canbe consideredasan implementation failure.Theactivitiesof thehealthpromo-
tionprogrammewerenotproperlyintegratedwiththeactivitiesoftheemployment
services.
The study did not show any effect of the health promotion programme on re-
employment.Oneexplanationisthatthestudywasunderpowered.Theprospective
studyofunemployedpersonsreceivingsocialsecuritybenefitsinthecityofRotterdam
showedthatlessthan5%foundpaidemploymentwithinaperiodofsixmonths.The
probabilityof findingpaidemploymentwasevenworsefor theRCTstudypopula-
tion,becauseallparticipantswerefacedwithmentalorphysicalhealthproblems.The

130 Chapter8
follow-up period of six months (including three months participating in the health
promotionprogramme)mayhavebeentooshort tobeable to findanyeffectof the
interventionontheprobabilityofre-employmentof long-termunemployedpersons
withhealthproblems.
8.3 neW insiGHTs
8.3.1HealthandWork
1. Health selection out of the workforce is influenced by socioeconomic position of workers.
Healthselectionoutofthelabourforceiswelldocumented.Considerablylessatten-
tionhasbeendirectedtothewaysinwhichhealthselectionoutofthelabourforceis
moderatedbythesocioeconomicpositionofworkers.[5]
In this thesis it was found that the effect of poor health on labour force exit was
morepronouncedamonghigh-andintermediate-educatedworkersthanamonglow-
educatedworkers.Theeffectofpoorhealthamonghigh-andintermediate-educated
workersbecamelessstronginmoredistantyearsbeforeleavingtheworkforce.Low-
educated workers had a higher probability of becoming unemployed compared to
high-educated workers. Among low-educated workers, the influence of health on
theprobabilityofbecomingunemployedwasrelativelysmall,buttheprevalenceof
becoming unemployed was much higher than among high-educated workers. The
populationattributablefractionsofhealthinexitfrompaidemploymentwere4.3%,
4.0%,and3.1%for low, intermediate,andhigheducatedworkers.Therefore,apoor
healthhasan important influenceon labour forceexit amonghigh-aswell as low-
educatedworkers.
Itwasalsoshowninthisthesisthatamongethnicminoritygroupshealthinequali-
tiesbetweenemployedandunemployedpersonswerelessprofoundcomparedtothe
native-Dutch population. However, unemployment rates were higher among ethnic
minoritygroupscomparedtotheDutchpopulation.Whentheunemploymentrateis
high,theeffectofhealthselectionoutoftheworkforceisrelativelysmallcomparedto
otherfactorsthatdeterminelabouropportunities.[6]Theproportionofpersonswith
poorhealth that theoretically couldbeattributed tounemploymentvariedbetween
14%and26%amongdifferentethnicminoritygroups,comparedto13%fortheDutch
population.Thisindicatesthatemploymentstatusisanimportantfactorinsocioeco-
nomichealthinequalitiesinallethnicgroups.

Ch
apte
r8
Generaldiscussion 131
2. The effect of ill health on labour force exit is influenced by labour market circumstances at
national level.
A comparative study of the relationship between unemployment and self-reported
healthin23Europeancountriesshowedthatthenegativerelationshipbetweenunem-
ploymentandhealth isconsistentacrossEuropebutvariesbywelfarestateregime,
suggestingthatlevelsofsocialprotectionmayhaveamoderatinginfluence.[7]Inthis
thesisitwasfoundthattheeffectofhealthonemploymentstatuswasinfluencedby
labourmarketcircumstances. Incountrieswithahighnationalunemploymentrate,
theeffectofhealthon labour forceexitwas lesspronouncedcompared tocountries
withalowunemploymentrate.Incountrieswithahighnationalunemploymentrate,
theeffectofhealth selectionoutof theworkforcewas relatively small compared to
otherfactorsthatdeterminedlabouropportunitiesforworkers.However,duetothe
highprevalenceoflabourforceexit,theamountofworkerswholefttheworkforcedue
tohealthproblemswasofcomparable importance incountrieswithahighnational
unemploymentrateaswellasincountrieswithalownationalunemploymentrate.It
wouldbeinterestingto investigatewhetherthelevelofprotectionforworkerswith
health problems against workforce exclusion and rehabilitation policies of different
Europeancountriescontributetotheinclusionofpersonswithhealthproblemsinthe
workforce.
3. Almost all dimensions of health, but especially physical functioning, had an influence on
the likelihood of becoming employed.
There is ample evidence to suggest that mental health influences the probability of
re-employment.[8] However, there is limited evidence about the influence of other
dimensionsofhealthontheprobabilityofre-employment.
Inthisthesisitwasfoundthatgeneralhealth,physicalfunctioning,bodilypain,so-
cialfunctioning,vitalityandrole-functioningduetoemotionalorphysicalproblems
allinfluencedthelikelihoodofre-employment.Thestrongestassociationwasfound
betweenphysicalfunctioningandre-employment.(Chapter5)
Health complaints may originate from a health condition, but the development
of chronic health problems often also depends on psychosocial factors. Perceptions
about the health problem and work may form a barrier to enter paid employment,
e.g.beliefsthatworkisharmful,andthatreturntoworkwilldofurtherdamageorbe
unsafe.[9]Inaddition,unemployedpersonswithhealthproblemsperformedlessjob
searchactivitiesandreceivedlessguidancetopaidemploymentfromtheemployment
services.[10-11](thisthesis,unpublishedresults)

132 Chapter8
To increase theprobabilityof re-employmentofunemployedpersonswithhealth
problems all barriers for entering paid employment should be addressed.[9] More
research is needed to develop evidence based practices to get unemployed persons
withhealthcomplaintsbackintotheworkforce.[12]
8.3.2Workandhealth
4. Among re-employed subjects mental as well as physical health improved within a short
time-period of six months.
In a review Waddel and Burton[13] concluded that re-employment leads to clear
benefitsinpsychologicalhealthandsomemeasuresofwell-being,althoughthereisa
dearthofinformationonphysicalhealth.Ameta-analyticstudyofthepsychological
and physical well-being during unemployment also demonstrated that the bulk of
researchisfocusedonmentalhealthoutcomes,suggestingthatotheraspectsofhealth
needmoreattention.[14]
Inthis thesis itwasfoundthatamongre-employedpersons,self-reportedgeneral
health, physical functioning, social functioning, vitality, mental health, bodily pain,
and role-limitations due to emotional or physical problems improved within six
monthsafterenteringpaidemployment,whereasthehealthstatusofthosewhocon-
tinuedtobeunemployedremainedunchanged.(Chapter5)
Workprovidesavarietyof features, including theopportunity for control,useof
skills, interpersonal contact, and provision of economic resources, that may be re-
sponsible for the increase of well-being among the re-employed persons.[15] In the
so-calledBlackreport(2008)itisstatedthatwork,matchedtoone’sknowledgeand
skillsandundertakeninasafe,healthyenvironment,canreversetheharmfuleffects
ofprolongedsicknessabsenceorlongtermunemployment,andpromotehealth,well-
beingandprosperity”.[16]Thisthesisprovidesevidencethatworkisindeedgoodfor
healthand,thus,workshouldbeconsideredasanimportantpartofhealthpromotion
programmesamongunemployedpersons.
8.3.3Healthpromotionoftheunemployed
5. It is of crucial importance among unemployed persons with health problems to integrate
activities to promote health with vocational training that promote re-employment.
Effortsoftheemploymentservicestoenhancere-employmentappearedtobenotef-
fectiveforunemployedpersonswithhealthproblems.(Chapter5)Thehealthproblems
haveanegativeinfluenceontheprobabilityofbecomingunemployed.Inaddition,the

Ch
apte
r8
Generaldiscussion 133
unemployment situation has a negative influence on the health problems, through
inactivity,socialisolationandalackofdailyroutine.Tobreakthroughthisnegative
spiral, effortsneed tobe focusedonhealthpromotionaswellas re-employment.[9]
This thesis showed that it isof crucial importance to integrateactivities topromote
healthwithvocationaltrainingtopromotehealthandre-employmentofunemployed
personswithhealthproblems.
Arandomizedtrialontheeffectivenessandimplementationofsupportedemploy-
ment showed that high levels of integration of psychiatric and vocational services
increased theprobabilityof successfulworkoutcomesofunemployedpersonswith
severementalillness.[17]Supportedemploymentemphasisesrapidjobsearchonthe
basisofaperson’spreferenceandcontinuingsupporttoemployeeandemployerfrom
anemploymentspecialistworkingasanintegralmemberofthementalhealthservice.
Different studies have shown that supported employment is effective in helping
unemployed persons with severe mental illness to obtain competitive employment.
[18-19]
8.4 RecommenDaTions
8.4.1Recommendationsforpractice
1. Measures to keep workers with health complaints in the workforce should focus on high as
well as low educated workers.
A poor health status of European workers had a major influence on the likelihood
ofleavingtheworkforce.Theinfluenceofhealthontheprobabilityofbecomingun-
employed was more pronounced among high- and intermediate-educated workers,
buttheprevalenceofbecomingunemployedwasmuchhigheramonglow-educated
workers. (Chapter3)Therefore,apoorhealthhasan important influenceon labour
forceexitamonghigh-aswellas low-educatedworkers.Measures tokeepworkers
withhealthcomplaintsintheworkforceshouldfocusonhigh-aswellasloweducated
workers.
2. Measures to include unemployed persons in the workforce are recommended to reduce
socioeconomic inequalities in health.
In Europe, differences in healthy life expectancy between socioeconomic groups
typically amount to 10 years or more, counted from birth [20] According to many,
such differences in health are unacceptable, and represent one of Europe’s greatest

134 Chapter8
challenges for public health. Unemployed persons are a specific socioeconomically
disadvantagedgroup.Among re-employedpersonshealth improvedwithina short
period of six months.(Chapter 5) Therefore, in the ambition to narrow the existing
healthgapmeasurestoincludepersonsintheworkforcearerecommended.
3. It is recommended to integrate health promotion activities with labour market interven-
tions.
Apoorhealthreducestheprobabilityofenteringpaidemployment.Inarandomized
controlledtrialitwasshownthatahealthpromotionprogrammedidnothaveaneffect
onself-reportedphysicalandmentalhealthandre-employment(Chapter6).Thislack
ofeffectofthehealthpromotionprogrammemaybecausedbyalackofintegration
ofthehealthpromotionactivitieswiththeactivitiesoftheemploymentservices.Itis
recommendedtointegratedactivitiestopromotehealthwithactivitiesthatpromote
re-employment.ArecentpilotinRotterdamshowedthatsuchintegratedapproachis
possible and most likely also effective.[22-23] Work as therapeutic intervention has
beenshowntobeeffective insupportedemploymentprojects, that integratemental
healthcarewithlabourmarketsupport.[18-19]
8.4.2Recommendationsforresearch
1. It is of interest to study the influence of socio-demographic and psychosocial characteristics
on the effect of poor health on labour force exit.
Thelongitudinalstudywith5-yearfollow-up(ECHP)showedthattheeffectofpoor
healthontheprobabilityofleavingtheworkforcewasinfluencedbysex,educational
levelandmaritalstatusofworkers.(Chapter4)Itwouldbeinterestingtoinvestigate
whetherothersocio-demographic(e.g.age,ethnicbackground)orpsychosocialchar-
acteristics(e.g.selfesteem,socialsupport)influencetheassociationbetweenillhealth
andlabourforceexit.Itwouldbeinterestingtostudywhysomeworkerswithahealth
conditionleavetheworkforceandothersdonot.
2. It is of interest to investigate whether national regulations concerning workforce exclusion
and rehabilitation of persons with health problems contribute to the inclusion of persons
with health problems in the workforce.
The aforementioned longitudinal study with 5-year follow-up on the working-age
populationin11Europeancountries(ECHP)showedthattherewerelargevariations
betweenEuropeancountriesintheassociationbetweenillhealthandlabourforceexit,

Ch
apte
r8
Generaldiscussion 135
thatcouldpartlybeexplainedby theunemployment rateatnational level.(Chapter
4)Thesevariationsmayreflectdifferencesbetweencountriesininstitutionalarrange-
ments,e.g.theavailabilityofdisabilitybenefitschemesforthosewithhealthproblems.
Itwouldbeinterestingtoinvestigatewhetherthelevelofprotectionforworkerswith
health problems against workforce exclusion and rehabilitation policies of different
Europeancountriescontributetotheinclusionofpersonswithhealthproblemsinthe
workforce.
3. The influence of entering paid employment on different dimensions of perceived health
should be corroborated
TheprospectivestudyamongunemployedcitizensoftheCityofRotterdamwithtwo
measurements inbetweenwhich theeventofenteringpaidemployment tookplace
showedanincreaseofhealthamongthosewhostartedwithpaidemploymentwithin
ashortfollow-upperiodofsixmonths.(Chapter5)Itisrecommendedtocorroborate
these findings with an interrupted time-series design with repeated measurements
overlongerperiods.Thisstudydesignwithmultiplemeasurementsofhealthbefore
andafterenteringpaidemploymentcangivemore insight into the time-dependent
trendofhealthstatusbeforeenteringpaidemploymentandtheinfluenceofentering
paidemploymentonthistrendofhealthstatus.Alongerfollow-upperiodisrecom-
mendedtoinvestigatewhetherthehealthimprovementissustainedintheyearsafter
re-employment.
4. It is recommended to evaluate the effectiveness of a highly integrated programme on health
and re-employment among unemployed persons with health problems in a randomised
controlled trial with a follow-up period of at least two years.
Arandomisedcontrolledtrialshowedthatahealthpromotionprogrammeaimedat
promotion of self-reported physical and mental health and re-employment among
unemployedpersonswithhealthproblemsdidnotshowbeneficialeffects.(Chapter6)
Itisadvisedtointegrateactivitiestopromotehealthwithactivitiesthatpromotere-
employment.Healthpromotionwithastrongfocusonincreasingsocial-andlabour
force participation may be a promising integrated approach to increase health and
re-employment of unemployed persons with health problems. Work as therapeutic
interventiontopromotehealthmayalsobeapromisingintegratedapproachtopro-
motehealthandre-employmentofunemployedpersonswithhealthproblems. It is
recommendedtoevaluatetheeffectivenessoftheseintegratedapproachesonhealth
andre-employmentamongunemployedpersonsinarandomisedcontrolledtrialwith
afollow-upofatleasttwoyears.

136 Chapter8
ReFeRences
1. BartleyM,SackerA,ClarkeP:Employmentstatus,employmentconditions,andlimitingillness:prospectiveevidencefromtheBritishhouseholdpanelsurvey1991-2001.Journal of epidemiology and community health 2004,58:501-506.
2. JanlertU:Unemploymentasadiseaseanddiseasesoftheunemployed.Scand J Work Environ Health 1997,23Suppl3:79-83.
3. MorrisJK,CookDG,ShaperAG:Lossofemploymentandmortality.BMJ (Clinical research ed 1994,308:1135-1139.
4. AlaviniaSM,BurdorfA:Unemploymentandretirementandill-health:across-sectionalanalysisacrossEuropeancountries.International archives of occupational and environmental health 2008,82:39-45.
5. McDonoughP,AmickBC,3rd:Thesocialcontextofhealthselection:alongitudinalstudyofhealthandemployment.Soc Sci Med 2001,53:135-145.
6. FayersPM,SprangersMA:Understandingself-ratedhealth.Lancet 2002,359:187-188. 7. BambraC,EikemoTA:Welfarestateregimes,unemploymentandhealth:acomparative
studyoftherelationshipbetweenunemploymentandself-reportedhealthin23Europeancountries.Journal of epidemiology and community health 2009,63:92-98.
8. ClaussenB,BjorndalA,HjortPF:Healthandre-employmentinatwoyearfollowupoflongtermunemployed.Journal of epidemiology and community health 1993,47:14-18.
9. WaddellG,Burton,A.K.:Conceptsofrehabilitationforthemanagementofcommonhealthproblems.London: The Stationery Office 2004(www.tsoshop.co.uk):ISBN0117033944.
10. IWI:Kansenenbelemmeringen.Deondersteuningvanwerklozenmeteenuitkering.Inspec-tieWerkenInkomenMinisterievanSocialeZakenenWerkgelegenheid2008:oktober2008.
11. UWV:Kwartaalverkenning2009-I.2009. 12. BambraC,WhiteheadM,HamiltonV:Does‘welfare-to-work’work?Asystematicreviewof
theeffectivenessoftheUK’swelfare-to-workprogrammesforpeoplewithadisabilityorchronicillness.Soc Sci Med 2005,60:1905-1918.
13. WaddellG,Burton,A.K.:Isworkgoodforyourhealthandwell-being?London:TheStatio-neryOffice2006(www.tsoshop.co.uk):ISBN:9780117036949.
14. McKee-RyanF,SongZ,WanbergCR,KinickiAJ:Psychologicalandphysicalwell-beingdur-ingunemployment:ameta-analyticstudy.J Appl Psychol 2005,90:53-76.
15. WarrP,JacksonP:Adaptingtotheunemployedrole:alongitudinalinvestigation.Soc Sci Med 1987,25:1219-1224.
16. BlackC:Workingforahealthiertomorrow.London: The Stationery Office 2008(http://www.workingforhealth.gov.uk/Carol-Blacks-Review/):ISBN:9780117025134
17. CookJA,LehmanAF,DrakeR,McFarlaneWR,GoldPB,LeffHS,BlylerC,TopracMG,Razzano LA, Burke-Miller JK et al: Integration of psychiatric and vocational services: amultisite randomized, controlled trial of supported employment. Am J Psychiatry 2005,162:1948-1956.
18. CrowtherRE,MarshallM,BondGR,HuxleyP:Helpingpeoplewithseverementalillnesstoobtainwork:systematicreview.BMJ (Clinical research ed 2001,322:204-208.
19. BurnsT,CattyJ,BeckerT,DrakeRE,FiorittiA,KnappM,LauberC,RosslerW,TomovT,vanBusschbachJ et al:Theeffectivenessofsupportedemploymentforpeoplewithseverementalillness:arandomisedcontrolledtrial.Lancet 2007,370:1146-1152.

Ch
apte
r8
Generaldiscussion 137
20. MackenbachJP:HealthInequalities:EuropeinProfile.Anindependent,expertreportcom-missionedby,andpublishedundertheauspicesof,theUKPresidencyoftheEU2005.
21. Lundin A, Lundberg I, Hallsten L, Ottosson J, Hemmingsson T: Unemployment andmortality--alongitudinalprospectivestudyonselectionandcausationin49321Swedishmiddle-agedmen.Journal of epidemiology and community health 2010,64:22-28.
22. JagmohansinghS:EvaluatieExITFeijenoord.RapportvandeSociaalWetenschappelijkeafdelingvandedienstSocialeZakenenWerkgelegenheid,Rotterdam2008.
23. OldenhofH,ColijnD:ExIT-ExtraIntensieveTrajectbegeleiding-Hetmultidisciplinairere-integratie instrumentvooreennaarvermogenparticiperendeengezondestad.RapportvandeDienstSocialeZakenenWerkgelenheidvandeGemeenteRotterdam2009.


Sum
mar
y
139Summary
summary
Therelationshipbetweenunemploymentandpoorhealthhasbeenwellestablished,
asdemonstratedbyahigherprevalenceofillnessanddisabilityandahighermortality
amongunemployedpersons.Selectionandcausationmaycontributetotheinequali-
tiesinhealthamongemployedandunemployedpersons.Selectionmayactthrough
twodifferentpathways.Workerswithapoorhealthmaybemorelikelytoleavethe
labourforce.Unemployedpersonswithapoorhealthmaybelesslikelytoenterthe
workforce.Causationmayalsoactintwodifferentways.Leavingtheworkforcemay
haveanegativeinfluenceonhealthoftheex-workers.Theotherwayaround,gaining
paidemploymentmayhaveapositiveinfluenceonhealth.
Theprimaryobjectivesofthisthesiswere(1)tostudytheinfluenceofpoorhealthon
enteringandmaintainingpaidemployment,(2)toinvestigatetheinfluenceofenter-
ingpaidemploymentondifferentdimensionsofperceivedhealth,and(3)toevaluate
theeffectivenessofahealthpromotionprogrammeamongunemployedpersonswith
healthcomplaintsonphysicalandmentalhealthandre-employment.Thefirstobjec-
tivewasaddressedinChapter3and4,thesecondobjectivewasaddressedinChapter
5,andthethirdobjectivewasaddressedinChapter6and7.
The associations between health and employment may not be similar across all
socio-economicgroups.chapter 2presentsacross-sectionalstudyamonginhabitants
oftheCityofRotterdamintheNetherlands,whichaimedtoevaluatewhetherhealth
inequalitiesassociatedwithunemploymentwerecomparableacrossdifferentethnic
groups. Differences in ill health between employed and unemployed persons were
lessprofoundinethnicminoritygroupscomparedwiththenativeDutchpopulation,
buttheprevalenceofunemploymentwasmuchhigherinethnicminoritygroups.The
proportions of persons with poor health that could be attributed to unemployment
variedbetween13%and28%acrossethnicgroups.
HeaLTH anD WoRk
Inmanyindustrializedcountries thepopulation isageing,dueto increasing lifeex-
pectancyandfallingbirthrates.Aratherparadoxicaldevelopmentisthat,despitein-
creasesinlifeexpectancy,theaveragetimepersonsspendinpaidworkhasdecreased
orbeenstable inmostEuropeancountries.Thisparadox isexplainedbyprolonged
educationamongyoungercohortsandamoreimportantcontributoristhehighrate
ofexitfromthelabourmarketatolderages.
In chapter 3, a longitudinal study with 2-year follow-up in the working popula-
tion aged between 50 and 63 years in 11 European Union countries (SHARE) was

Summary140
presented.Thislongitudinalstudyaimedtodeterminetheimpactofillhealthonexit
frompaidemploymentinEuropeamongolderworkers.Duringthetwo-yearfollow-
upperiod,17%ofemployedworkersquittedpaidemployment,primarilyduetoearly
retirement. Poor self-perceived health was strongly associated with exit from paid
employmentduetoretirement,unemployment,ordisability(ORsfrom1.32to4.37).
Consequencesofillhealthforthelikelihoodofbecomingorstayingunemployment
may also depend on socioeconomic position of workers and labour market circum-
stancesatnationallevel.Inchapter 4,alongitudinalstudywithfiveannualwavesof
theEuropeanCommunityHouseholdPanel(ECHP)surveyispresented,whichaimed
toexaminetheeffectofillhealthonenteringandmaintainingpaidemployment.The
effectofillhealthonlabourforceexitstronglydependedoneducation,sex,andfam-
ilysituation.InmostEuropeancountries,apoorhealthorachronichealthproblem
predicted staying or becoming unemployed and the effects of health were stronger
withalowernationalunemploymentlevel.
WoRk anD HeaLTH
Thereisampleevidencetosuggestthatre-employmentleadstoclearbenefitsinpsy-
chologicalhealth.However,itislessclearwhetherre-employmentalsohasbeneficial
effects on other measures of health, e.g. physical health. chapter 5 presents a pro-
spectivestudywith6monthsfollow-upamongunemployedsubjectsreceivingsocial
securitybenefitsfromtheCityofRotterdam,theNetherlands.Theaimofthisprospec-
tivestudywastoinvestigatetheeffectofre-employmentondifferentdimensionsof
healthwithinashortperiodafterenteringpaidemployment.Amongthere-employed
participantsallself-reporteddimensionsofhealthincreasedwithinsixmonths,with
estimatedeffectsizesvaryingfrom0.1to0.7.Thelargestrelativeimprovementswere
observedformentalhealth,socialfunctioning,androle-limitationsduetoemotional
or physical problems, whereas physical functioning showed the smallest relative
improvement.
HeaLTH PRomoTion amonG THe unemPLoyeD
Apoorhealthwillactasabarriertoreturntopaidemployment.Inordertoincrease
the possibilities for re-employment, improvement in health of unemployed persons
may,therefore,beanimportantstep.Inchapter 6,arandomisedcontrolledtrial(RCT)
with six months follow-up among unemployed persons with health complaints is
presented.TheaimofthisRCTwastoevaluatetheeffectivenessofahealthpromotion

Sum
mar
y
141Summary
programmeamongunemployedpersonswithphysicalandmentalhealthcomplaints
andre-employment.TheRCTshowedthatthehealthpromotionprogrammehadno
beneficial effect on self-reported mental and physical health, self esteem, mastery,
and pain-related fear of movement. In addition, values and attitudes towards paid
employment, job search activities, and employment status at six months follow up
were not influenced by the health programme either. The lack of integration of the
intervention intoregularvocationalrehabilitationactivitiesmayhavenegativelyaf-
fectedtheresultsofthehealthprogrammeamongunemployedpeople.
chapter 7 presentsa longitudinal studyamongparticipantswho received the in-
tervention.Theaimofthisstudywastoevaluatechangesinphysicalhealthamong
participants.Thestudyshowedthatcardiorespiratoryfitnessincreasedonaverageby
7%.However,thisimprovementwasnotsufficienttoraisecardiorepiratoryfitnessof
participantstolevelsobservedinthegeneralpopulation.
chapter 8,theGeneralDiscussion,startswithasummaryofthemainresultsofthis
thesis,followedbystudylimitationsthatshouldbeacknowledgedwheninterpreting
the results. Five specific new insights from the studies described above were dis-
cussed.Basedontheresearchpresentedinthisthesisthefollowingrecommendations
arepresented:
RecommenDaTions FoR PRacTice
1) Measurestokeepworkerswithhealthcomplaints intheworkforceshouldfocus
onhighaswellasloweducatedworkers.
2) Measures to includeunemployedpersons in theworkforceare recommended to
reducesocioeconomicinequalitiesinhealth.
3) It is recommended to integrate health promotion activities with labour market
interventions.
RecommenDaTions FoR ReseaRcH
1) Itisofinteresttostudytheinfluenceofsocio-demographicandpsychosocialchar-
acteristicsontheeffectofpoorhealthonlabourforceexit.
2) It isof interest to investigatewhethernationalregulationsconcerningworkforce
exclusion and rehabilitation of persons with health problems contribute to the
inclusionofpersonswithhealthproblemsintheworkforce.
3) Theinfluenceofenteringpaidemploymentondifferentdimensionsofperceived
healthshouldbecorroborated.

Summary142
4) Itisrecommendedtoevaluatetheeffectivenessofahighlyintegratedprogramme
onhealthandre-employmentamongunemployedpersonswithhealthproblems
inarandomisedcontrolledtrialwithafollow-upperiodofatleasttwoyears.

Sam
env
atti
ng
143Samenvatting
samenvatting
Derelatietussenwerkloosheideneenslechtegezondheidisveelvuldigaangetoond,
zoalsblijktuiteenhogereprevalentievanziekteenbeperkingeneneenhogeresterfte
onder werklozen. Twee verschillende mechanismen, selectie en causatie, dragen bij
aandegezondheidsverschillentussenwerkendeenwerklozemensen.Selectiewerkt
optweeverschillendemanieren.Teneerstehebbenwerknemersmeteenslechtege-
zondheideengroterekansomdearbeidsmarktteverlaten.Tentweedehebbenwerk-
lozen met een slechte gezondheid minder kansen om een betaalde baan te vinden.
Causatie werkt mogelijk ook op twee verschillende manieren. Stoppen met werken
heefteennegatieveinvloedopdegezondheidvanex-werknemers.Daarnaastkanhet
verkrijgenvaneenbetaaldebaandegezondheidpositiefbeïnvloeden.
Debelangrijkstedoelstellingenvanditproefschriftzijn(1)hetonderzoekenvande
invloedvaneenslechtegezondheidophetverkrijgenenbehoudenvaneenbetaalde
baan, (2)hetonderzoekenvande invloedvanhetverkrijgenvaneenbetaaldebaan
op verschillende aspecten van de ervaren gezondheid, en (3) het evalueren van de
effectiviteit van een gezondheidsbevorderingsprogramma op de fysieke en mentale
gezondheid en werkhervatting van werklozen met gezondheidsklachten. De eerste
doelstelling wordt behandeld in Hoofdstuk 3 en 4, de tweede doelstelling wordt
behandeldinHoofdstuk5endederdedoelstellingwordtbehandeldinHoofdstuk6
en7.
De samenhang tussen gezondheid en werkstatus is mogelijk niet gelijk voor ver-
schillende sociaaleconomische groepen. Hoofdstuk 2 beschrijft een cross-sectionele
studienaardesamenhangtussengezondheidenwerkstatusbijRotterdammersmet
verschillende etnische achtergronden. Gezondheidsverschillen tussen werkenden
enwerklozenwarenmindergrootbij etnischeminderheden invergelijkingmetau-
tochtoneNederlanders,maarhetwerkloosheidspercentagewashogeronderetnische
minderheden.Deproportiepersonenmeteenslechtegezondheiddoorwerkloosheid
varieerdeperetnischegroepvan13%tot23%.
GezonDHeiD en WeRk
Inveelgeïndustrialiseerdelandenveroudertdepopulatie,dooreentoenamevande
levensverwachtingeneenafnamevanhetgeboortecijfer.Eenparadoxaleontwikke-
ling is dat, ondanks de toenemende levensverwachting, het gemiddeld aantal jaren
datiemandbesteedtaanbetaaldwerkindeafgelopendecenniaisgedaaldofgelijkis
gebleven indemeesteEuropese landen.Dezeparadoxwordtgedeeltelijkverklaard

Samenvatting144
doordatjongeremensenlangeronderwijsvolgen,maareenbelangrijkereverklaringis
dehogeuitvaluitdearbeidsmarktonderouderemedewerkers.
In Hoofdstuk 3 wordt een longitudinale studie onder oudere werknemers in 11
Europeselanden.Doelvandezelongitudinalestudiewashetbepalenvandeinvloed
vaneenslechtegezondheidopuitstroomuitdearbeidsmarktinEuropaonderoudere
werknemers(leeftijd50-63jaar).Gedurendedefollow-upperiodevantweejaarverliet
17%vandeouderewerknemersdearbeidsmarkt,voornamelijkvanwegevervroegde
pensionering.Erwaseensterkesamenhangtusseneenslechteervarengezondheiden
uitvaluitdearbeidsmarktdoorpensionering,werkloosheidofarbeidsongeschiktheid
(oddsratio’svariërendvan1.32tot4.37).
Consequentiesvaneenslechtegezondheidopdekansomwerkloostewordenente
blijvenismogelijkookafhankelijkvandesociaaleconomischepositievanwerknemers
endearbeidsmarktomstandighedenopnationaalniveau.InHoofdstuk 4wordteen
longitudinalestudiemetvijf jaarlijksemeetmomentenvaneenvragenlijstonderzoek
onder Europese huishoudens (ECHP) beschreven, naar het effect van een slechte
gezondheidoneenbetaaldebaanteverkrijgenentebehouden.De invloedvaneen
slechtegezondheidopuitstroomuitdearbeidsmarktisafhankelijkvanopleidingsni-
veau,geslachtengezinssituatie.IndemeesteEuropeselandeniseenslechtegezond-
heidvaninvloedopdekansomwerkloostewordenenteblijven,waarbijdeinvloed
vangezondheidgroterisinlandenmeteenlaagwerkloosheidspercentage.
WeRk en GezonDHeiD
Er is veelvuldig aangetoond dat werkhervatting een positieve invloed heeft op de
mentalegezondheid.Echter,het isminderduidelijkofwerkhervattingook leidt tot
verbetering van de fysieke gezondheid. In Hoofdstuk 5 wordt een prospectief on-
derzoekonderwerklozeRotterdammersmeteenbijstandsuitkeringbeschrevenmet
eenfollow-upperiodevanzesmaanden.Hetdoelvandezeprospectievestudiewas
hetonderzoekenvande invloedvanhetstartenmeteenbetaaldebaanopverschil-
lendeaspectenvandegezondheidbinnenkortetijdnahetstartenmeteenbetaalde
baan.Alleaspectenvandeervarengezondheidvanmensendiegestartwarenmeteen
betaalde baan verbeterden binnen zes maanden. Het starten met een betaalde baan
hadrelatiefdegrootste invloedopdementalegezondheid,hetsociale functioneren
enrolbeperkingendooreenemotioneeloffysiekprobleem,terwijlfysiekfunctioneren
deminsteverbeteringlietzien.

Sam
env
atti
ng
145Samenvatting
GezonDHeiDsbevoRDeRinG bij WeRkLozen
Een slechte gezondheid vormt een belemmering voor het starten met een betaalde
baan. Het verbeteren van de gezondheid van werklozen is mogelijk een belangrijk
stapomdekansophetvindenvaneenbetaaldebaantevergroten. InHoofdstuk 6
wordteengerandomiseerdexperimentbeschrevenmeteenfollow-upperiodevanzes
maanden onder werklozen met gezondheidsklachten. Het doel van dit experiment
was het evalueren van de invloed van een gezondheidsbevoderingsprogramma op
defysiekeenmentalegezondheidenkansophetstartenmeteenbetaaldebaanvan
werklozenmetgezondheidsproblemen.Uithetonderzoekbleekdathetgezondheids-
bevorderingsprogrammageeninvloedhadopervarenmentaleenfysiekegezondheid,
zelfwaardering,hetomgaanmetproblemenenpijngerelateerdeangstomtebewegen.
Daarnaasthadhetgezondheidsprogrammaookgeeninvloedoppersoonlijkewaarden
enattitudestenaanzienvanbetaaldwerk,hetzoekennaareenbetaaldebaan,enhet
daadwerkelijkstartenmeteenbetaaldebaan.Hetontbrekenvaneengoedeintegratie
vanhetgezondheidsprogrammainderegulierere-integratieactiviteitenheeftmoge-
lijkeennegatiefeffectgehadopdeeffectiviteitvanhetgezondheidsprogrammavoor
werklozen.
Hoofdstuk 7 beschrijft een longitudinaal onderzoek naar verandering van de fy-
sieke gezondheid van deelnemers van het gezondheidsprogramma. Het onderzoek
laatziendathetfysiekeuithoudingsvermogenvandeelnemersvanhetgezondheids-
programmagemiddeld7%verbeterde.Echter,dezeverbeteringwasnietvoldoende
omdefysiekeconditieophetniveauvandealgemenebevolkingtekrijgen.
Hoofdstuk 8,dealgemenediscussie,begintmeteensamenvattingvandebelangrijk-
steresultatenvanditproefschrift,vervolgenswordenbeperkingenvanhetonderzoek
beschrevendieinhetachterhoofdgehoudenmoetenwordenbijhetinterpreterenvan
deresultaten.Vijfnieuweinzichtenvoortkomenduitbovenstaandeonderzoekenwor-
denbeschreven.Opbasisvanhetonderzoekinditproefschriftwordendevolgende
aanbevelingengegeven:
aanbeveLinGen vooR De PRakTijk
1. Maatregelen om werknemers met gezondheidsklachten aan het werk te houden
moetenzichrichtenopzowelhogeralsoplageropgeleidewerknemers.
2. Maatregelengerichtophetaanhetwerkgaanvanwerklozenmetgezondheids-
klachten kunnen bijdragen aan het verkleinen van sociaaleconomische gezond-
heidsverschillen.

Samenvatting146
3. Activiteitengerichtophetverbeterenvandegezondheidvanwerklozenzouden
geïntegreerdmoetenwordenmetwerkgerelateerdeinterventies.
aanbeveLinGen vooR onDeRzoek
1. Hetwordtaanbevolenomdeinvloedvansociaaldemografischeenpsychosociale
kenmerken op de relatie tussen een slechte gezondheid en uitstroom uit de ar-
beidsmarktteonderzoeken.
2. Het wordt aanbevolen om de invloed van nationale regelingen op het op de
arbeidsmarkt krijgen en behouden van mensen met gezondheidsklachten te on-
derzoeken.
3. Deinvloedvanhetstartenmeteenbetaaldebaanopverschillendeaspectenvande
ervarengezondheiddientdoorandereonderzoekenbevestigdteworden.
4. Hetwordtaanbevolenomdeeffectiviteitvaneen integraleaanpakvangezond-
heidsproblemenenre-integratienaarwerkvoorwerklozenmetgezondheidspro-
blemen te onderzoeken in een gerandomiseerd experiment met een follow-up
periodevanminstenstweejaar.

Dan
kw
oo
rd
147Dankwoord
Dankwoord
Alleenmijnnaamprijktopdevoorkant,maarvelenhebbenbijgedragenaandetot-
standkomingvanditproefschrift.Graagwilikeenaantalmensenbedankenvoorhun
bijdrage.
Allereerst wil ik mijn promotoren, Lex Burdorf en Johan Mackenbach, bedanken.
Lex,jouwambitieomhoogleraartewordenisrecentverwezenlijkt.Mijnpromoveren
markeertdaarmeetevensvoorjoueenspeciaalmoment,waarinjevoorheteerstals
promotorzaloptreden.Dankzijjouwsteunenvertrouwenishetvoormijmogelijkom
mijn ambities te verwezenlijken, als promovendus en inmiddels als postdoc onder-
zoeker.Ikwiljebedankenvoordeprettigeenleerzamesamenwerking.
Ikbeschouwhetalseenvoorrechtdatnietéén,maartweehooglerarenvandeafdel-
ingMaatschappelijkeGezondheidszorgalspromotoroptreden.Johan,het ismijeen
eer en genoegen dat jij van meet af aan betrokken bent geweest bij het onderzoek.
Bedanktvoorjeinhoudelijkebijdrageaanditproefschrift.GraagwilikookInezJoung
bedankenvoorhaarinzetalsbegeleiderbijdestartvanhetproject“Gezondaande
Slag”.
HetprojectGezondaandeSlag isontstaanuiteenunieksamenwerkingsverband
tussen de GGD Rotterdam-Rijnmond, de dienst Sociale Zaken en Werkgelegenheid
(SoZaWe) van de gemeente Rotterdam en het Erasmus MC. Dit project is de basis
geweest voor een belangrijk deel van dit proefschrift. Vanuit de GGD waren Toon
Voorham, Sven Graumans en Kees der Weduwe intensief betrokken bij het project.
VanuitdeSoZaWespeeldenAatBrandenPaulvandenBergeenbelangrijkerol.Ikwil
alle ledenvanhetprojectteamhartelijkbedankenvoorhunbijdrageaanhetproject
GezondaandeSlag.
VanuitErgocontrolhebbenmetnameJanPlat,AnnekeZwartenallebetrokkendo-
centeneenbelangrijkerolgespeeldbijhetprojectGezondaandeSlag.Hetuitvoeren
vandeinterventiehebbenjulliemetheelveeltoewijdinggedaan.Dankdaarvoor.
Graagwil ikookHalukArslanenalle interviewersbedankenvoordeuitdagende
taakominterviewsaftenemenbijeenbijzondermoeilijktebereikendoelgroep.Jul-
lie zijn in staat geweest om gewapend met de vragenlijst kwalitatief goede data te
verzamelen.Veeldankdaarvoor.
Ondermijncollega’svanhetMGZzijnernogeenaantalmensendieikgraagwil
bedanken voor hun bijdrage aan dit proefschrift. Heren van de helpdesk en dames
van het secretariaat, bedankt voor de goede ondersteuning. Marieke Hartman en
Christine Schutgens, graag wil ik jullie bedanken voor jullie inzet bij het uitvoeren
van het onderzoek voor jullie Master thesis. Halime, als onderzoeksassistent heb jij
veel werk voor het project Gezond aan de Slag verricht. Ik kon daarbij blindelings

Dankwoord148
opjevertrouwen.Daarnaastkondenwehetookpersoonlijkgoedmetelkaarvinden.
Dankvoordefijnesamenwerking.
Het zijn mijn directe collega’s die ervoor zorgen dat ik met plezier op het MGZ
werk.Graagwil ikmijnkamergenoten,Frank,Freek,Karien,Mohammed,Goedele,
Carlijn,EefjeenHester,bedankenvooralleleukeeninteressantegesprekken.Delunch-
wandelingiseengoedegewoontevanveleMGZ-ers.GraagwilikmijnMGZcollega’s
bedanken voor die gezellige wandelingen en de vele gesprekjes ‘onderweg naar de
koffieautomaat’.Fijnookdatikaltijdeveneenkamerkanbinnenlopenmeteenvraag
ofzomaar.Elin,Tilja,Suzan,Karien,Bart,Hilde,Klazine,Birgitte,Katrina,Willemieke,
Marianne en Loes, bedankt voor de gezelligheid door de jaren heen. Karien, jij zal
ééndagvóórmij jeproefschriftverdedigenen...westaanerallebeiopdiedagniet
alleenvoor!Carlijn,hetisfijnomjoualsvriendinéncollegatehebben.Bedanktvoor
jebetrokkenheidensteun.Hetiseengeruststellendideedatjijalsparanimfaanmijn
zijdezalstaanbijdeverdedigingvanmijnproefschrift.
Alhoewelfamilieenvriendengeendirectebijdragehebbengeleverdaanhetproef-
schrift,zijnzeindirectwelvanbelanggeweest.Andrea,Marie-JoséeenAnnemieke,
bedanktvoorjullievriendschapengezelligheidtijdenshetdrinkenvaneenkopjethee,
etentjeofwandeling.Annemieke,alsparanimfhebjeeenbelangrijkesymbolischerol
opdepromotiedag.Ikvindhetfijndatjijopmijnpromotiedagerbijzalzijn.
Lieve familieleden, bedankt voor de oprechte interesse door de jaren heen. Oma
Annie,nuisereindelijk,naastaldieingenieurs,ookeendoctorindefamilie!Mamma
enDick,bedanktvoorjulliebetrokkenheidensteun.Hetisfijnomtewetendatjullie
trotszijnopmij. Julliewetenalsgeenanderdathetsomsnietmeevaltomwerken
gezin tecombineren. Ikkomnogaltijdgraagbij jullie langsomeven ‘uit tepuffen’
vanonsdrukkebestaan.Roos,alsgrotezusheb jealtijdeenbelangrijke rol inmijn
leven gespeeld. Fijn dat we met onze gezinnen zo’n fijne familie vormen. Thea, ik
hebhet erggetroffenmetzo’n lieve schoonmoeder.Bedanktvoor jegastvrijheiden
behulpzaamheid.
Lieve Bastiaan, bedankt voor het leven dat wij samen leven. Inmiddels met drie
kleineboevenerbij endevierdeopkomst.Hetafrondenvanditproefschrift is een
mijlpaal, maar geen eindpunt. Er liggen nog vele uitdagingen op onze weg. Samen
metjoudurfikdezeaantegaan.

Cu
rric
ulu
mV
itae
149CurriculumVitae
curriculum vitae
Merel Schuring werd geboren op 24 maart 1977 teAlphen aan den Rijn. Zij genoot
haarbasisonderwijsopdeAlphenseMontessorischoolinAlphenaandenRijn.In1995
behaaldezijhaarVWO-diplomaaanhetScalaCollegeinAlphenaandenRijn.Daarna
startte zij met de studie Biologie aan de Universiteit Utrecht. In 2001 behaalde zij
haardoctoraalBiologie.Vanafapril2001werktezijalswetenschappelijkonderzoeker
bij het Coronel Instituut voorArbeid en Gezondheid van hetAMC inAmsterdam.
Vanaf november 2003 tot augustus 2008 was zij als wetenschappelijk onderzoeker
verbondenaandeafdelingMaatschappelijkeGezondheidszorgvanhetErasmusMC
inRotterdamenvoerdehetpromotieonderzoekuitdatresulteerdeinditproefschrift.
GelijktijdigvolgdezedeMasteropleidingPublicHealthaanhetNIHES(Netherlands
Institute for Health Sciences) en behaalde in augustus 2008 haar Master of Public
Health.Vanaugustus2008totmei2009waszijwerkzaamalsstatistischonderzoeker
bijhetCentraalBureauvoordeStatistiekinVoorburg.Sinds1mei2009iszeopnieuw
verbondenaandeafdelingMaatschappelijkeGezondheidszorgvanhetErasmusMC
inRotterdamals(postdoctoraal)onderzoeker.
Merel isgetrouwdmetBastiaandeBruinensamenhebbenzijdriezonen:Tobias
(2005),Storm(2007)enQuinten(2009).
Merel Schuring was born on March 24, 1977, in Alphen aan den Rijn, the Nether-
lands.Shereceivedherprimaryschooleducationat theAlphenseMontessorischool
in Alphen aan den Rijn. She obtained her secondary school education at the Scala
CollegeinAlphenaandenRijnin1995.Thereafter,shestartedstudyingattheFaculty
ofBiologyattheUniversityofUtrecht.In2001shegraduatedherMasterofScience
inBiology.Shewasthenemployedasascientificresearcherat theCoronelInstitute
ofOccupationalHealthattheAcademicMedicalCentreinAmsterdam.From2003to
2008,sheworkedasascientificresearcherattheDepartmentofPublicHealthatthe
ErasmusMedicalCentreinRotterdam,whereshecarriedouttheresearchpresented
inthisthesis.Duringthistime,shealsoenrolledintheMasterofScienceprogramme
at the Netherlands Institute for Health Sciences, and obtained her Master of Public
Health inAugust2008.FromAugust2008toMay2009,shewasemployedasasta-
tisticalresearcheratStatisticsNetherlandsinVoorburg.Sheiscurrentlyemployedas
postdoctoral researcherat theDepartmentofPublicHealthat theErasmusMedical
CentreinRotterdam.
MerelismarriedtoBastiaandeBruinandtheyhavethreesons:Tobias(2005),Storm
(2007)andQuinten(2009).


151Publicationsinthisthesis
Pu
bli
cati
on
s
Publications in this thesis
SchuringM,BurdorfA,KunstA,VoorhamT,MackenbachJ.(2009).Ethnicdifferences
inunemploymentandillhealth.International Archives of Occupational and Environmen-
tal Health,82:1023-30.
Schuring M, BurdorfA, VoorhamAJ, der Weduwe K, Mackenbach JP (2009). Effec-
tivenessofahealthpromotionprogrammefor long-termunemployedsubjectswith
healthproblems:arandomizedcontrolledtrial.Journal of Epidemiology and Community
Health,63:893-899.
Schutgens CAE, Schuring M, Voorham AJ, Burdorf A (2009). Changes in physical
health among participants in a multidisciplinary health programme for long-term
unemployedpersons.BMC Public Health,9:197.
SchuringM,BurdorfA,KunstAE,Mackenbach JP (2007).Theeffectof illhealthon
enteringandmaintainingpaidemployment:evidenceinEuropeancountries.Journal
of Epidemiology and Community Health, 61:597-604.
SchuringM,MackenbachJ,VoorhamAJ,BurdorfA.Theeffectofre-employmenton
perceivedhealth.Journal of Epidemiology and Community Health,inpress.
vandenBergT,SchuringM,AvendanoM,MackenbachJ,BurdorfA.Theimpactof
ill health on exit from the labour market in Europe. Occupational and Environmental
Medicine,inpress.
oTHeR PubLicaTions
derWeduweK,SchuringM,BurdorfL,VoorhamT(2006).GezondaandeSlag-ge-
zondheidbevorderenvanlangduriguitkeringsgerechtigden.TijdschriftvoorGezond-
heidswetenschappen,6:354-357
HaafkensJ,MoermanC,SchuringM,vanDijkF(2006)Searchingbibliographicdata-
basesfor literatureonchronicdiseaseandworkparticipation.Occupational Medicine
(London),56:39-45.

Publicationsinthisthesis152
Schuring M, Sluiter JK, Frings-Dresen MHW (2004) Evaluation of top-down imple-
mentationofhealthregulationsinthetransportsectorina5-yearperiod.International
Archives of Occupational and Environmental Health,77:53-9.
Schuring M, Sluiter JK, Frings-Dresen MHW (2003) Onregelmatige werktijden: het
ontstaanenherstelvanvermoeidheid.Tijdschrift voor Ergonomie,28:4-10.

Ph
DP
ort
foli
o
153PhDPortfolio
PhD Portfolio
summary of PhD training and teaching activities
NamePhDstudent:MerelSchuring PhDperiod:November2003–August2008ErasmusMCDepartment:Publichealth Promotors:J.P.Mackenbach,MD,PhD
A.Burdorf,PhDResearchSchool:Netherlandsinstituteforhealthsciences(Nihes)
year Workload(ecTs)
1. PhD training
General academic skills & Research skillsMasterofScienceinPublicHealth,NetherlandsInstituteforHealthSciences(Nihes),Rotterdam,TheNetherlands
2004-2008 70
Presentations SchuringM,MackenbachJP,VoorhamAJ,BurdorfA.“Theeffectofre-employmentonperceivedhealth”.PaperpresentedattheDepartmentofPublicHealth,ErasmusMC,Rotterdam,TheNetherlands
SchuringM,BurdorfA.“EvaluatieGezondaandeSlag”.ErgoControlCongres,Woudenberg,TheNetherlands
SchuringM,BurdorfA.“EvaluatieGezondaandeSlag-deinterventie”.ExpertmeetingGezondaandeSlag,Rotterdam,TheNetherlands
SchuringM,GraumansS.“GezondaandeSlag!Gezondheidbevorderenvanlangduriguitkeringsgerechtigden”.KenniscentrumGroteSteden;expertatelierSEGV,TheNetherlands.
VoorhamAJ,SchuringM,BoschR.Workshop:“GezondaandeSlag!Gezondheidbevorderenvanuitkeringsgerechtigden”.NederlandsCongresVolksgezondheid,Rotterdam,TheNetherlands.
2010
2008
2007
2006
2006
1
1
1
1
1
2. Teaching activities
SupervisingMaster’sthesis
Lecture(oninvitation)mastercourseWorkandOrganisationalPsychology,RadboudUniversityNijmegen,TheNetherlands
2006-2007
2010
6
1


















