The Georgia Perinatal Quality Collaborative: Applying QI Strategies to Improve Perinatal Outcomes...
28
The Georgia Perinatal Quality Collaborative: Applying QI Strategies to Improve Perinatal Outcomes Georgia Hospital Association October 22, 2014
-
Upload
shana-thompson -
Category
Documents
-
view
221 -
download
0
Transcript of The Georgia Perinatal Quality Collaborative: Applying QI Strategies to Improve Perinatal Outcomes...

The Georgia Perinatal Quality Collaborative: Applying QI Strategies to Improve Perinatal Outcomes
Georgia Hospital Association
October 22, 2014

3 BABIESWILL DIE
TODAYIN GEORGIA

Perinatal Health in GeorgiaIn 2012, Georgia ranked 49th nationally for maternal mortality – with 35.5 deaths per 100,000 births.From 1993 – 2006, Black, Hispanic and Asian women accounted for 41% of all births nationwide , and for 62% of pregnancy-related deaths.
Preconception health such as diabetes, hypertension, cardiac issues and obesity increase risk of maternal death and LBW babies.In 2010, 19.9% of women smoked within the 3 months prior to pregnancy, and 8.3% of moms smoked in the final 3 months of pregnancy in 2010.
Tobacco exposure duringpregnancy and secondhand
smoke after delivery is a risk factorfor preterm birth, sleep-related death
and poor lung development
Georgia ranked 37th nationally for infant mortality – with 6.8 deaths
per 1000 live births in 2012.
Black, non-Hispanic infants were2.5 times more likely to die
than White, non-Hispanic infants.
The rate of SIDS in Georgiaremained stagnant
between 2007-2011.
Birth defects are the2nd most common
cause of infant death in GA,
but the no. 1 most common cause in the
US.
In 2010, only 55.2% of Georgia mothers started breastfeeding after delivery.*
Maternal Health Infant Health

2006 2007 2008 2009 2010 20114
5
6
7
8
9
10
11
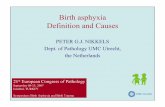
Infant Mortality in the Southeastern United States, 2006-2011
FloridaGeorgiaMississippiNorth CarolinaSouth CarolinaTennessee
Year
Infa
nt
Death
s p
er
1,0
00
Bir
ths

Infant Mortality Clusters within Georgia, 2002-2006

Maternal Risk Factors for Infant Mortality by Cluster
A B C D E FLess likely to have more than a high school degree
Less likely to be White non-Hispanic Less likely to have had adequate prenatal care
Less likely to be married More likely to have had a previous adverse pregnancy outcome
More likely to have had a c-section More likely to be a smoker More likely to be 19 years old or younger
More likely to have a chronic health condition

Looking at trends from across the state
Approx. 1 in 5 births
spaced < 2 years apart
in 2012
>17% of infant deaths in 2011 were
due to prematurity
or LBW
11 % of births were preterm in
2012
9.4 % of births were
LBW in 2012

Mission
VisionAll perinatal stakeholders in Georgia coming together to improve health and birth outcomes for all Georgia mothers and babies
To establish and maintain a robust statewide perinatal data and quality improvement system that engages stakeholders in evidence-based practices to improve health outcomes for mothers and babies throughout Georgia.
Georgia Perinatal Quality Collaborative

Summer 2011
The GAPQC Journey
Vision began to germinat
e for creation
of PQC
Stakeholder
engagement began, review of
other state PQCs
Formal creation
of GAPQC
2011- 2012Oct. 2012
Steering committee formed, Mission &
Vision created, projects selected
May 2013Review lessons
learned, identify
new projects,
begin recruiting
for Phase II of PQC.
Summer 2014
Pilot Launch.
July 2013

The GAPQC Steering CommitteeCo-Chairs: Catherine Bonk, MD, MPH, (OB/Gyn) and David Levine, MD, (Neo)
DPH Support: Seema Csukas, MD, PhD, MCH Director, Theresa Chapple-McGruder, PhD, Director of MCH Epidemiology, Maria Fernandez, Infant
Mortality DirectorPhysicians Community Partners and
Professional Organizations- Mike Armand, MD, Dekalb (NEO)
- David Carlton, MD, Emory & Grady (NEO)
- Armando Castillo, MD, NE GA Health System (NEO)
- Jane Ellis, MD, Grady (OB/GYN)- Jameela Harper, MD, NE GA
Health System (OB/GYN)- Demetrice Hill, MD, Columbus
Regional (OB/GYN)- Lucky Jain, MD, Emory & Grady
(NEO)- Ravi Patel, MD, Emory & Grady
(NEO)- Mitch Rodriguez, MD, Medical
Ctr of Central GA, (NEO)- Champa Woodham, MD,
Medical Ctr of Central GA, (OB/GYN)
- Pat Cota, Exec. Dir, Georgia OBGyn Society
- Fozia Eskew, Early Intervention Coordinator, GA AAP
- Lynne Hall, QI Consultant, GHA- Sarah Owens, Immediate Past
President, American College of Nurse Midwives (GA)
- Sheila Ryan, State Director, March of Dimes
- Kim Sumpter, Community Outreach, The United Way of Greater Atlanta
- Rick Ward, Exec. Dir., GA AAP- Sarah Dyer, Director, Maternal
Services, NE Georgia Health System

Maternal Health

Chronic Disease is a High Risk Factor for Maternal and Infant Outcomes
2008 2009 20100.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
0.8
0.7 0.7
1.4
1.3
1.4
Chronic conditions during pregnancy, GA birth certificate, 2008-2010
Chronic Diabetes
Chronic Hyper-tension
Perc
ent
of
live b
irth
s
Source: GA data repository, 2008-2010 final birth file

• >50% of women are overweight or obese; 1/3 are obese*
• 48% of reproductive-aged women are overweight or obese;26% are obese†
• > 40% of pregnant women are overweight or obese*
*Retrieved from BRFSS (2011) †Retrieved from PRAMS (2010)
Obesity in Georgia

2008 2009 2010 2011 201220
21
22
23
24
25
26
All of GeorgiaRural Non-Rural
% o
f t
ota
l liv
e b
irth
s
Only 12% of women indicated a desire to have a child in the next year,* but more than 20% are having a baby in <2 years
* Based on recent Medicaid/CHIP Health Care Quality survey

States with highest rate of repeat teen pregnancy

*
* Based on recent Medicaid/CHIP Health Care Quality survey
While 6:10 women want to space their pregnancies, 6:10 women also are not using the most effective birth control to achieve their goals

AL FL MA NC NY TNEarly Elective Deliveries
Post-partum Hemorrhage (AWHONN)
ANCS Hypertension/Preeclampsia
Breastfeeding
Maternal Health: Opportunities
What about supporting high risk women (teens, preexisting chronic conditions) to better plan and space their pregnancies?

Maternal Health: QI Strategy
AimImprove maternal and infant health outcomes by increasing rate of immediate post-partum LARC insertion to help high risk women better control chronic conditions and achieve birth planning goals
Key Drivers
- Address policies and processes that impact women receiving preferred birth control option at discharge
- Increase training and awareness in the inpatient and outpatient setting for providers, clinicians and others
- Provide patient-focused and sensitive education and counseling
- Leverage changes in Medicaid reimbursement to expand LARC access to women who may not have received LARCS previously
Collaborative Opportunity
DCH and DPH Collaboration on QI project sponsored by CMS. Kick off begins in November for nine-month cycle.

Infant Health

10 Leading Causes of Infant DeathGeorgia, 2002-2006
Cause of Death #
% of total Rate
Rank
All Causes 5743
100 8.24 --
Disorders related to short gestation and low birth weight, not elsewhere classified
1117
19.5 1.62 1
Congenital malformations, deformations and chromosomal abnormalities
964 16.8 1.39 2
Sudden infant death syndrome & sleep-related deaths
621 10.8 0.90 3
Newborn affected by complications of pregnancy
321 5.6 0.46 4
Respiratory distress of newborn 245 4.3 0.35 5
Accidental/unintentional injuries 181 3.2 0.26 6
Bacterial sepsis of newborn 169 2.9 0.24 7
Newborn affected by complications of placenta, cord and membranes
164 2.9 0.24 7
Necrotizing enterocolitis of newborn 134 2.3 0.19 9
Disease of circulatory system 131 2.3 0.19 9

Georgia’s NBS program panel expansion
Congenital heart defects are the most common birth defect. By expanding the panel to include screening, we can have an impact on:• Infant, child and adolescent mortality rates• Healthcare utilization and costs for children with special healthcare needs

Three new screens added to the panel
1CCHD screen detects 12 conditions
3Hemoglobinopathi
es
20Inborn Metabolic
errors
4Other Metabolic errors (includes
SCID)
2Endocrine disorders
1Audiology screen
for hearing impairment

Infant Health: QI Strategy
AimImprove support hospitals in the implementation of CCHD as part of newborn screening to increase awareness, identification and treatment of children born with congenital heart defects.
Key Drivers
- Address policies, staffing models, supply chain considerations and procedures to support efficient implementation and reduce rejections of NBS cards.
- Identify and implement best practices for short-term and long-term training of physicians, clinicians and other staff
- Provide patient-focused and sensitive education and counseling to families
Collaborative Opportunity
Both Children’s National Medical Center and the University of Minnesota have issued toolkits to support CCHD screening implementation. Georgia is developing a toolkit that integrates best practices from both to support the implementation in Georgia, across a variety of hospital settings.

AL FL MA NC NY TNNeonatal Abstinence Syndrome
CLABSIs and other HAIs
NICU Human Milk The “Golden Hour”* Newborn Screening/CCHD
Neonatal High Risk Follow-Up Clinic*
Infant Health: Opportunities
* Based on toolkit from California toolkit

Why Join GAPQC?
Working together we accomplish more:
- Bringing together neonatologists and ob/gyns, we can address the spectrum of factors that impact perinatal outcomes.
- Larger numbers let us pool resources, see more changes and outcomes more quickly.
- We can attract other stakeholders and partners – combining the clinical interventions with patient/family education we can address the variety of issues that impact outcomes.
- The better our outcomes and the larger our reach, the more we are able to demonstrate our value to payors, funding sources and communities

GaPQC Timeline July 1, 2014 - June 30, 2015
Sept
July15
Oct. Nov. Jan.
Launch recruitment effort and Phase II QI Project planning begins Finalize
project planning
GA AAP Meeting
Full day Kickoff Session
Design PlanningImplementation &
Reporting
2 Education sessions
Education Session
Next Wave Recruited and Project Planning Launched
Ongoing Monthly Conference Calls to Review Data and Plan PDSA Cycles

Recruitment Goal: Statewide Collaborative with All Perinatal Stakeholders
Pilot 2015 2016 2017
No. of Hospitals:
5 12-18 25-40 41+
Kick-Off Educational Session: January 2015
Atlanta, GA
Application Deadline: November 25