The Adult with Transposition - Home - NCUSncus.org/files/spring2015/loehr2.pdf · 3/5/2015 3 L-TGV:...
11
3/5/2015 1 The Adult with Transposition Do two wrongs make a right? Forms of Transposition • L-Transposition of the Great Vessels • D-Transposition without pulmonary stenosis − Atrial Repair − Anatomic repair (arterial switch) • D-Transposition, VSD, pulmonary stenosis − Rastelli repair Figure 3. Relative survival of patients and patient groups. Nieminen H et al. Circulation 2001;104:570-575 Copyright © American Heart Association L-transposition of the Great Vessels • Rare: Less than 1 % of congenital heart disease • Atrioventricular discordance and ventriculoarterial discordance • If no major associated anomalies, survival to adulthood without intervention is common • High frequency of major anomalies that can dominate early history L-TGV: Two wrongs Normal vs. L-TGV
Transcript of The Adult with Transposition - Home - NCUSncus.org/files/spring2015/loehr2.pdf · 3/5/2015 3 L-TGV:...

3/5/2015
1
The Adult with
Transposition Do two wrongs make a right?
Forms of Transposition
• L-Transposition of the Great Vessels
• D-Transposition without pulmonary stenosis
− Atrial Repair
− Anatomic repair (arterial switch)
• D-Transposition, VSD, pulmonary stenosis
− Rastelli repair
Figure 3. Relative survival of patients and patient groups.
Nieminen H et al. Circulation 2001;104:570-575
Copyright © American Heart Association
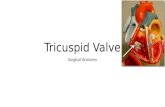
L-transposition of the Great
Vessels
• Rare: Less than 1 % of congenital heart disease
• Atrioventricular discordance and ventriculoarterial
discordance
• If no major associated anomalies, survival to
adulthood without intervention is common
• High frequency of major anomalies that can
dominate early history
L-TGV: Two wrongs Normal vs. L-TGV

3/5/2015
2
L-transposition: tricuspid valve closer to apex L-transposition: mitral-pulmonary valve continuity
L-transposition
• Associated anomalies
− VSD in 70%
− PS 40%
− Systemic AV valve abnormalities
Ebstein’s Anomaly
Progressive Tricuspid Regurgitation
− Progressive dysfunction of systemic right ventricle
L-transposition
• Conduction system abnormalities
− Dual AV node anatomy and abnormal His
bundle
− Progression to AV Block estimated at 2% per
year

3/5/2015
3
L-TGV: ECG L-TGV: Echocardiography
• Tricuspid valve closer to cardiac apex
− Importance of tricuspid regurgitation
• Mitral-pulmonary valve continuity
• Aorta usually anterior and to the left of pulmonary
artery
L-transposition: tricuspid regurgitation L-transposition: right ventricular function
RV failure
• In those without associated lesions, some degree
on CHF in about 1/3 by fifth decade
− Role of tricuspid regurgitation
• Frequency greater in patients with previous heart
surgery
D-TGV
• Ventriculoarterial discordance
− D-loop, RV on right side of heart
− Ao tends to be on right and
anterior
• Cyanosis
• Associated lesions
• Role of PS

3/5/2015
4
Atrial Repair
• Senning 1958, Mustard later
− Baffle atrial blood to contralateral AV valve
Atrial repair
Atrial repair
• Good early results
• Late complications
− Sinus node dysfunction;
sinus rhythm in 77% at 5
years, 40% in 20 years
− Atrial flutter may be
marker of sudden death
Atrial repair
• Late ventricular dysfunction and tricuspid regurgitation
• Actuarial survival 80% at 20 years
• Evaluation of RV function difficult due to different
architecture of RV
• Baffle leaks and obstruction (SVC>IVC>pulmonary
venous)
• Pulmonary hypertension more frequent in those
operated at > 2 years of age
Atrial repair
• Actuarial survival
• Mortality 1-5 %
• Late sudden death
• High frequency of good functional class (80% symptom
free with NYHA Class I)
• Progressive increase in RV dysfunction, TR, arrhythmias
− 2.5% early mortality, 2.5% late mortality
Atrial repair
• Loss of sinus rhythm
• Increase in atrial
arrhythmias
• Late sudden death

3/5/2015
5
Atrial Repair: Echo
• Evaluate right (systemic) ventricular function
− RV size and contractility (often subjective)
− Tricuspid regurgitation
• Evaluate for baffle obstruction
− Systemic venous (more common)
− Pulmonary venous
Atrial repair of D-TGV
Atrial repair: Pulmonary venous baffle Atrial repair: Pulmonary venous baffle
Atrial repair: Tricuspid regurgitation
Arterial switch
• Introduced by Jatene in 1976
• Transect great arteries,
transpose them and move
coronaries
• Distortion of branch
pulmonary arteries, aortic
insufficiency, coronary
occlusion early
postoperatively

3/5/2015
6
Arterial switch
• Advantage: Left ventricle is the systemic
ventricle
• Substantial morbidity and mortality in early
experience
• Recent results much improved, but long term
results are still evolving
Surgical mortality
• Only studies are
retrospective
• High early mortality
with arterial switch,
probably better long
term mortality
• Increased mortality
with single or
intramural coronaries
Figure 1. Top, Actuarial survival in 1200 patients who had ASO. Numbers indicate number of patients
observed at beginning of interval.
Losay J et al. Circulation 2001;104:I-121-I-126
Copyright © American Heart Association
ASO: Late complications
• Late death relatively rare
• Branch pulmonary stenosis
• Progressive aortic insufficiency
• Evaluate for coronary occlusion
Aortic insufficiency

3/5/2015
7
Figure 3. Actuarial survival free from grade II or more AI (Ao insufficiency) for 1095 survivors.
Losay J et al. Circulation 2001;104:I-121-I-126
Copyright © American Heart Association
• 19 year-old S/P arterial switch
• Asymptomatic but with increasing left ventricular size
Arterial Switch: Aortic Insufficiency Arterial Switch: Aortic Insufficiency
Arterial switch
• Probably lower risk of late death, but population is
growing older
• Often asymptomatic in presence of progressive
disease
• Increased risk of coronary findings later in life
which are difficult to visualize echocardigraphically
“Complex” D-TGA
• Most frequent complex
lesion is with ventricular
septal defect and
pulmonary (valvar and
sublalvar) stenosis
• Most common mode of
repair is the Rastelli
procedure

3/5/2015
8
Rastelli repair
• Mean age (initially) age 4 years
• Current survival 93% at 20
years, but early was 52% at 20
years
− Late sudden death
• Reoperation due to progressive
stenosis of RV-PA conduit
Rastelli
• Surgical issues—recurrent
LVOTO, conduit
obstruction, arrhythmias,
late mortality
− Perioperative heart block
− Straddling tricuspid valve
Rastelli: reintervention
Rastelli: Echo
• Evaluate for both LV and RV outflow obstruction
• Evaluate for ventricular dysfunction
• Investigate for residual VSD
“Complex” D-TGA: Rastelli “Complex” D-TGA: Rastelli

3/5/2015
9
“Complex” D-TGA: Rastelli “Complex” D-TGA: Rastelli
“Complex” D-TGA: Rastelli, residual VSD
Transcatheter valve
replacement
Transcatheter valve
replacement
“Complex” D-TGA: Rastelli

3/5/2015
10
“Complex” D-TGA: Rastelli
Suprasternal notch view for branch pulmonary arteries
“Complex” D-TGA: Rastelli
Prognosis in Adults Good Intermediate Uncertain/Poor
Atrial Septal
Defect Aortic Stenosis
D-Transposition
(arterial switch)
Patent Ductus
Arteriosus Tetralogy of Fallot L-Transposition
Pulmonary
Stenosis
D-Transposition
(Senning/Mustard
)
Ebstein’s
Anomaly
Ventricular Septal
Defect Single Ventricle
Coarctation
Mortality-->Insurance Lesion
Late Mortality
(%)
Mortality
Ratio Underwriting
ASD/PDA/PS 5-12 70-200 100
VSD 20 667 100-200
CoA 16 320 100-300
Aortic Sten. 15 375 225-400+
ToF 14 350 200-400
Senning 24 480 Declined
Single Vent. 85 >2800 Declined
Cognitive issues
• Cognitive function probably diminished
• Lower than average scores on
neuropsychological testing as adolescents
• Many receive remedial academic or behavioral
services during school years

3/5/2015
11
Pregnancy in TGA
• Prognosis dictated by ventricular function and
arrhythmias
• Thorough evaluation of rhythm particularly in
atrial switch and L-TGV patients
• Complications of valve anticoagulation
• Increased risk of congenital heart disease in
offspring
Pregnancy
Lesion Success
rate Complications Reference
L-TGV 83%
CHF with valve
replacement after
delivery
JACC 33:1692 (1999)
Atrial
Switch 82%
Arrhythmias 22%,
other 80% Eur Ht J 26:2588 (2005)
Arterial
Switch
13/17
(76%)
VT, valve
thrombosis AJC 106:417 (2010)
Rastelli 50% Increased sub-
aortic stenosis
Aust NZ Obstet Gyn 45:243
(2005)
There are more adults than children
with congenital heart disease in the
U.S…
…boldly going where no group
of patients has gone before.