Tapered, Fluted Femoral Fixation · 18% of cases or fracture of the femur in as many as 30% of...
9
CHAPTER 36 Tapered, Fluted Femoral Fixation Todd Swanson C H A P T E R P R E V I E W CHAPTER SYNOPSIS: The tapered, fluted revision hip stem has solved a serious problem in revision arthroplasty. By using the remaining intact diaphyseal bone stock for fixation, these stems offer a treatment option for proximally deficient femora and provide a reliable result in most cases. IMPORTANT POINTS: 1. Tapered, fluted revision stems are most useful for proximally deficient femora (Paprosky types IIIA, IIIB, and IV). 2. Such stems also are useful for periprosthetic fractures associated with nonsupportive proximal femoral bone (Vancouver types B2 and B3). 3. Most modular stems require proximal bony support to protect the modular junction. CLINICAL/SURGICAL PEARLS: 1. Determining the highest level of supportive femoral bone is important to place the taper into this bone. An extended trochanteric osteotomy is useful for removal of the old stem and facilitates placement of a relatively straight, tapered, fluted stem down a bowed femur, thus preventing anterior perforation of the stem through the anterior cortex. The intact diaphysis often will benefit from a cable around the highest level of intact bone to prevent fracture and provide a better end point during stem insertion. The proximal, nonsupportive metaphyseal bone should be reconstructed around the upper stem for support. CLINICAL/SURGICAL PITFALLS: 1. Axial stability is difficult to achieve when the bone is osteoporotic or when the length of intact diaphysis is less than 4 cm. A cable around the uppermost part of the intact diaphysis, with or without strut grafts, will help provide axial stability and discourage subsidence. Reconstruction of proximal bone stock provides support to the upper stem and averts stem fracture at the modular junction. VIDEO AVAILABLE: A video demonstrating insertion of a tapered, fluted revision stem after extended trochanteric osteotomy is available. INTRODUCTION The number of revision total hip replacements is predicted to more than double over the next 25 years from an esti- mated 40,800 in 2005 to approximately 96,700 in 2030. 1 Total hips are now being implanted in much younger patients, and the risk of multiple revisions demands better means of reconstruction. Although revision arthroplasty is amenable to many options when bone stock is good, poor bone stock often jeopardizes reconstruction with more cus- tomary implants. Before the use of cementless implants, cemented compo- nents served as the workhorse for revision arthroplasties. However, cemented revision components present several problems, including difficulty obtaining adequate interdigita- tion and fixation of cement into the smooth, sclerotic, endos- teal bone of the femur; extrusion of cement through femoral defects; and the need for a large volume of cement that impedes subsequent revisions and can threaten the patient’s cardiopulmonary system during introduction. 2 Cementless fixation provides solutions to many of these problems. However, proximal femoral bone loss continues to challenge adequate fixation and osseointegration with proxi- mally fixed components. Long, extensively porous coated femoral components allow more distal fixation. However, with severe proximal bone loss or large, ectatic canals, even these stems can fail. 3,4 In addition, fitting the stem to the canal often proves difficult, resulting in undersizing of the femoral component and failure of bony ingrowth in up to 18% of cases or fracture of the femur in as many as 30% of cases in some studies. 5–7 Wagner 8 first described the use of a distally tapered, fluted, revision femoral component in 1987 (Fig. 36–1). Axial 354
Transcript of Tapered, Fluted Femoral Fixation · 18% of cases or fracture of the femur in as many as 30% of...

C H A P T E R 3 6
Tapered, Fluted Femoral Fixation
Todd Swanson
C H A P T E R P R E V I E W
CHAPTER SYNOPSIS: The tapered, fluted revision hip stem has solved a serious problem in revision arthroplasty. By using the remaining intactdiaphyseal bone stock for fixation, these stems offer a treatment option for proximally deficient femora and provide a reliable result inmost cases.
IMPORTANT POINTS:
1. Tapered, fluted revision stems are most useful for proximally deficient femora (Paprosky types IIIA, IIIB, and IV).2. Such stems also are useful for periprosthetic fractures associated with nonsupportive proximal femoral bone (Vancouver types B2 and B3).3. Most modular stems require proximal bony support to protect the modular junction.
CLINICAL/SURGICAL PEARLS:
1. Determining the highest level of supportive femoral bone is important to place the taper into this bone. An extended trochanteric osteotomy isuseful for removal of the old stem and facilitates placement of a relatively straight, tapered, fluted stem down a bowed femur, thuspreventing anterior perforation of the stem through the anterior cortex. The intact diaphysis often will benefit from a cable around the highestlevel of intact bone to prevent fracture and provide a better end point during stem insertion. The proximal, nonsupportive metaphysealbone should be reconstructed around the upper stem for support.
CLINICAL/SURGICAL PITFALLS:
1. Axial stability is difficult to achieve when the bone is osteoporotic or when the length of intact diaphysis is less than 4 cm. A cable aroundthe uppermost part of the intact diaphysis, with or without strut grafts, will help provide axial stability and discourage subsidence. Reconstructionof proximal bone stock provides support to the upper stem and averts stem fracture at the modular junction.
VIDEO AVAILABLE:
A video demonstrating insertion of a tapered, fluted revision stem after extended trochanteric osteotomy is available.
INTRODUCTION
The number of revision total hip replacements is predictedto more than double over the next 25 years from an esti-mated 40,800 in 2005 to approximately 96,700 in 2030.1
Total hips are now being implanted in much youngerpatients, and the risk of multiple revisions demands bettermeans of reconstruction. Although revision arthroplasty isamenable to many options when bone stock is good, poorbone stock often jeopardizes reconstruction with more cus-tomary implants.
Before the use of cementless implants, cemented compo-nents served as the workhorse for revision arthroplasties.However, cemented revision components present severalproblems, including difficulty obtaining adequate interdigita-tion and fixation of cement into the smooth, sclerotic, endos-teal bone of the femur; extrusion of cement through femoral
defects; and the need for a large volume of cement thatimpedes subsequent revisions and can threaten the patient’scardiopulmonary system during introduction.2
Cementless fixation provides solutions to many of theseproblems. However, proximal femoral bone loss continues tochallenge adequate fixation and osseointegration with proxi-mally fixed components. Long, extensively porous coatedfemoral components allow more distal fixation. However,with severe proximal bone loss or large, ectatic canals, eventhese stems can fail.3,4 In addition, fitting the stem to thecanal often proves difficult, resulting in undersizing of thefemoral component and failure of bony ingrowth in up to18% of cases or fracture of the femur in as many as 30% ofcases in some studies.5–7
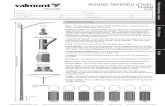
Wagner8 first described the use of a distally tapered,fluted, revision femoral component in 1987 (Fig. 36–1). Axial
354

stability was achieved by driving the tapered stem into theintact femoral diaphysis, which had been milled into a coni-cal shape to accept the distally tapered femoral component.Longitudinal flutes provided rotational control of the pros-thesis. However, subsidence of the stem, particularly in casesof weak or osteoporotic bone, continued to be an obstacle tocomplete success.9–13
Because the final height of the stem at which axial stabil-ity was attained was somewhat unpredictable, a modularproximal body was introduced in subsequent design modifi-cations. Modularity in total hip components initially raisedconcern about corrosion and breakage at the modular junc-tions. However, although some modular designs have seen
fatigue failures, the ability to adjust the height and antever-sion of the proximal stem after achieving solid primaryfixation of the distal stem proved extremely valuable in cor-recting leg length and achieving hip stability. At least onemanufacturer has redesigned the modular junction in itsstems of 17 mm or larger to improve the strength in thishigh-stress area.14 Modular, tapered, fluted stems have nowbecome one of the mainstays for reconstructing femurs withsignificant proximal bone loss.
CLASSIFICATION SYSTEMS
Revision Femoral Components
Femoral reconstruction can be accomplished in numerousways. No standard classification system has been adopted,but the most commonly used methods for femoral fixationand reconstruction are shown in Table 36–1. Revision femoralcomponents can be cemented or cementless, although cemen-ted revision components have largely fallen out of favor.
Cementless fixation method includes proximal fixation,distal fixation, or a combination of the two. Extensivelyporous coated stems are designed to achieve both, althoughin practice the fixation more commonly is distal.3,15 Cement-less stems can be modular or nonmodular; straight or bowed;porous coated, grit blasted, or hydroxyapatite coated; andfluted or nonfluted.
A third option for femoral fixation is the requisite use ofbone graft to obtain primary stability. Bone grafting may beeither structural or morselized. Although structural allo-graft-prosthesis composites can successfully rebuild bonestock—particularly important in younger patients—theypresent the potential complications of nonunion, graftresorption, component loosening, infection, and fracture.4,16
Morselized impaction grafting has met with reasonably goodsuccess in the hands of experienced surgeons. It providesprimary structural support of the femoral component, evenin extremely deficient femurs.17
A
B
FIGURE 36–1. Wagner’s tapered, fluted revision stem. (Reprinted fromKo PS, Lam JJ, Tio MK, et al: Distal fixation with Wagner revision stem in treatingVancouver type B2 periprosthetic femur fractures in geriatric patients, J Arthroplasty18(4):446-452, 2003.)
TABLE 36–1 Classification of Femoral Reconstruction Options
ReconstructionTechnique Cement Modularity Fixation Location
Mandatory BoneGraft Example
Cementedcomponent
Yes No Proximal andDistal
No Any long-stem cemented component
Cementless proximalfixation
No Yes or no Proximal(metaphyseal)
No S-Rom (DePuy, Warsaw, Ind.); Mallory/Head (Biomet Inc., Warsaw, Ind.)
Cementless distalfixation
No Yes or no Distal (diaphyseal) No Wagner SL (Protek AG); Link MP(Exactech)
Cementless proximaland distal fixation
No Yes or no Metaphyseal anddiaphyseal
No Solution (DePuy); Echelon, extensivelyporous coated (Smith & Nephew,Memphis, Tenn.)
Proximal structuralallograft prosthesiscomposite
Yes (to allograft); alsomay cement to hostbone
Yes or no Proximal–toallograft; distal–tohost bone
Yes (structural) Any long-stem component
Morselized(impaction) grafting
Yes No Proximal anddistal
Yes (morselized) Exeter (Exeter, UK)
355C H A P T E R 36 Tapered, Fluted Femoral Fixation

Femoral Bone Deficiencies
Numerous classification systems for femoral bone loss havebeen described.18 Although these systems have many simila-rities, the author believes a classification system that helpsguide the type of fixation and predicts the results of interven-tion is most useful. For those reasons, this author prefers thePaprosky system (Table 36–2).19
The Paprosky system breaks femoral bone loss into types I,II, III, and IV.Type I femurs have onlyminimal loss ofmetaphy-seal cancellous bone and an intact diaphyseal isthmus. Type IIfemurs have more extensive loss of proximal metaphyseal bonebut an intact femoral diaphysis. Types I and II femoral meta-physes are supportive. Type III femurs are subdivided into IIIAand IIIB.Type IIIA femurs have extensive, nonsupportivemeta-physeal damage but more than 4 cm of intact diaphyseal isth-mus, whereas type IIIB femurs have similar extensivemetaphyseal loss with some intact diaphyseal femur of less than4 cm in length. Type IV femurs have global bone loss withoutsupportive bone in either the metaphysis or diaphysis.
Periprosthetic Femoral Fractures
Themost accepted classification system for periprosthetic fem-oral fractures is the Vancouver classification system describedby Duncan and Masri (Table 36–3).20 The Vancouver systemdivides periprosthetic femoral fractures into types A, B, and C.Type A fractures involve the trochanteric region only and sparethe femoral shaft. Type B fractures occur about the femoralcomponent. Type B fractures are further subdivided into typesB1, B2, and B3. In B1 fractures the femoral component remainsstable within the proximal femur. In B2 fractures the femoralcomponent is loose, but the bone stock surrounding the implantis supportive. B3 fractures occur about the femoral component,and the surrounding bone is deficient and nonsupportive. TypeC fractures occur well distal to the femoral component.
INDICATIONS AND CONTRAINDICATIONS
Wagner’s revision stem is a straight stem tapered 2 degreesalong its entire length. It uses 8 longitudinal flutes for rota-tional control, is grit blasted on its surface, and ranges from
190 to 305 mm in length.21 Cementless diaphyseal fixationallows treatment of proximally deficient femora without theuse of structural allograft or cement. Although Wagner metwith reasonable success, the prosthesis of his design is notwithout complications, most notably axial subsidence, legshortening, and hip instability (Fig. 36–2).9–11,13,22–24
Some of the early problems with subsidencemay have beenattributable to inexperience with this new mode of fixation,resulting in undersizing of the stem. Other causes were likelythe relatively shallow taper angle of 2 degrees and difficulty seat-ing the prosthesis at a level that was both axially stable andprovided the desired leg length and hip joint stability. Becauseof these problems, design modifications soon followed, includ-ing steeper taper angles andmodularity. Although advantageousfor attaining correct leg length and soft tissue tension, proximalmodularity was soon found to be a weakness, with several mod-ular stems designs fracturing at this high-stress location, partic-ularly when unsupported by proximal bone (Fig. 36–3).25,26
In hips with good proximal metaphyseal bone (Paproskytypes I or II), many fixation choices are available, includingthose that use the metaphysis for primary stability and sec-ondary fixation. Because some femora remodel into retrover-sion over time, the surgeon using a metaphyseal-filling stemmust take care to place the component in the correct antever-sion because the canal often dictates the version of thestem.27 Straight, distally tapered stems will work in thesecases as well, with care taken to avoid perforation of the tipof the stem through the anterior femoral cortex because ofthe natural anterior bow of the femur.
Types II and IIIA femoral deficiencies can be handledquite effectively with extensively porous coated stems.Type IIIB and IV femoral bone loss presents a challengefor most cementless stems. Although type IIIB femoraldeficiencies with canal diameters less than 19 mm do reason-ably well with extensively porous coated stems, type IIIBfemurs larger than 19 mm in diameter and type IVfemurs—with minimal or no supportive bone in either themetaphysis or diaphysis—often require the use of cement,structural allograft, impaction allografting, or a tapereddiaphyseal fixation stem.4
TABLE 36–2 Paprosky Classification of Femoral Bone Lossfor Revision Total Hip Arthroplasty
Classification Description
I Minimal loss of metaphyseal cancellous bone and anintact diaphysis
II Extensive loss of metaphyseal cancellous bone but anintact diaphysis
IIIA Severe nonsupportive metaphyseal damage with>4 cm intact diaphyseal bone at isthmus
IIIB Severe nonsupportive metaphyseal damage with<4 cm intact diaphyseal bone at isthmus
IV Severe bone metaphyseal and diaphyseal bone losswith no supportive bone in diaphysis
TABLE 36–3 Vancouver Classification System forPeriprosthetic Femoral Fractures
Classification Subclassification Description
A Trochanteric regionAG Greater trochanterAL Lesser trochanter
B Around the femoral componentB1 Prosthesis stableB2 Prosthesis unstable but
surrounding bone supportiveB3 Prosthesis unstable and
surrounding bone deficient andnonsupportive
C Distal to prosthesis
356 REVISION THA: THE FEMUR

Periprosthetic femoral shaft fractures, particularlyVancouver types B2 and B3, lend themselves well to fixationwith a distally tapered, fluted femoral stem. Because the prox-imally fractured femur usually is nonsupportive, distal fixationinto the intact diaphysis provides axial and rotation stability,allowing reconstruction of the fracture fragments around theupper part of the stem. Several authors have reported excellentresults treating periprosthetic fractures in this manner.28–31
SURGICAL TECHNIQUE
Any hip reconstruction must achieve rotational and axial stabil-ity, restoration of leg length, and hip stability. Extensive boneloss makes these goals challenging. Tapered diaphyseal fixationachieves both rotational and axial stability by secure contact withthe remaining diaphyseal isthmus. If the isthmus is deficient, itcan sometimes be reconstructed with cortical struts and cablesto provide secure fixation of the stem within the canal.
Good preoperative planning is essential. The length of thestem chosen must position the taper at the level of the intactdiaphyseal isthmus of the femur (Fig. 36–4). If the taper is toofar proximal or distal, axial stability of the stem in the canal can-not be achieved. Preoperative planning also will determine thevertical position of the stem needed to restore leg length, theoffset needed to restore hip stability, and whether an osteotomywill be necessary to correct femoral deformity.
Many difficult reconstructions of this type will benefitfrom an extended trochanteric femoral osteotomy, firstdescribed by Wagner8 in 1987 as a “transfemoral approach.”
Since then many surgeons have popularized the technique,with minor modifications (Fig. 36–5).32,33 Proximal femoralosteotomy helps to visualize the diaphyseal femur andremove the old implant and cement and insert a straight stemdown a bowed or deformed femur, thus averting perforationof the stem tip through the femoral cortex. The standard, lat-eral, extended trochanteric osteotomy mobilizes the greatertrochanter with abductors, vastus lateralis, and at least 8 cmof lateral femoral cortex attached, hinging the osteotomyanteriorly on its muscular attachments.
Whether or not an osteotomy is used, the key to suc-cessful femoral fixation is reaming a taper into the healthydiaphyseal femur such that the stem taper wedges snuglyinto the femur canal. Once the reamer makes initial corticalcontact, the surgeon may need to ream an additional 2 to3 mm in diameter to create a diaphyseal taper sufficient toprovide good axial support for the tapered stem. A minimumof 2 cm of good cortical contact is necessary to obtain axialstability of a tapered stem; a distance of 4 to 8 cm is optimal.With a stem tapered 3 degrees, each millimeter of reamingprovides 19 mm additional longitudinal bony contact withthe taper (Fig. 36–6). For a 2-degree taper, each millimeterof reaming provides 29 mm additional longitudinal contact.However, the smaller the taper angle, the closer to parallelthe surfaces of the stem and bone become. The geometryeventually approaches a cylinder in a tube, which can resistsubsidence only by frictional forces and not by the geometricattributes of the taper. Placement of a cable at the mostproximal aspect of the intact diaphysis often can prevent
A B C
FIGURE 36–2. Subsidence of a modular, tapered, fluted distal fixation revision stem. A custom modular body wasmanufactured to correct the 15-mm shortening resulting from stem subsidence. A, Original implantation. B, Subsidence of15 mm 3 months postoperatively. C, Restoration of leg length with a custom modular body.
357C H A P T E R 36 Tapered, Fluted Femoral Fixation

a longitudinal crack in the cortex and provide better fixationin this area, even more important if the bone is thin or oste-oporotic. For more extensive thinning or osteoporosis, thesurgeon may place struts and cables around the diaphysealfemur, with the option to extend them proximally into thedeficient, ectatic metaphyseal area.
With the use of modular tapered stems, the stem is drivendistally to its final, stable level at the outset. The leg lengthand hip stability are then adjusted with a proximal body of thecorrect height and offset. Most manufacturers now recommendtrying to achieve some additional support proximally becausemost of these stems bear high stresses at the subtrochantericlevel of the modular connection. Proximal bodies with porousingrowth surfaces can be used, with cables and strut graftsproviding additional proximal support for the stem.
If an extended trochanteric osteotomy has been per-formed, it can be closed down on the upper stem with cablesand strut grafts if needed. Conversely, if no osteotomy hasbeen performed, episiotomy of the ectatic metaphyseal femuroften is useful to reduce it around the upper prosthesis, thusgiving support and encouraging bony ingrowth to the modu-lar body. Cables or wires can augment support with or with-out the addition of strut grafts.
POSTOPERATIVE RESTRICTIONSAND REHABILITATION
Most distally tapered, fluted, revision femoral stems have acorundum-blasted titanium surface. Multiple studies showreliable osseointegration to this type of surface finish over
the course of several weeks.34,35 In most cases weight bearingshould be restricted to toe touch until secondary osseointe-gration has been achieved, usually for a minimum of 6 weeks.Depending on the quality of the bone stock, partial weightbearing often can be instituted at 6 weeks if the stem remainsstable and the femur appears to be healing. Any evidence ofsubsidence in the early postoperative period should be trea-ted with an extended period of toe-touch weight bearing.Weight-bearing restrictions past 3 months are not likelybeneficial.
The condition of the metaphyseal femur and greater tro-chanter may require avoidance of active abduction and activehip flexion for a period to minimize muscular pull on the tro-chanter during healing. If the trochanteric fixation seemsdurable, these exercises can be instituted early.
OUTCOMES AND RESULTS
Multiple factors influence short- and long-term results offemoral reconstruction with fluted, distally tapered, cement-less stems. The earliest results reported were with theWagner nonmodular prosthesis, for which the incidence ofsignificant early subsidence was as high as 20%.12 Causesincluded probable undersizing of the stem during the initiallearning curve, a relatively small taper angle of 2 degrees,and a tendency to seat the prosthesis at the level appropriateto correct leg length and provide hip joint stability ratherthan the point at which the stem achieved axial stabilitywithin the femoral canal.
A B
FIGURE 36–3. Breakage of a modular distal fixation stem. This prosthesis was implantedwithout any proximal bony support. A, Immediate postoperative radiograph. B, One year aftersurgery the stem had fractured at the modular junction.
358 REVISION THA: THE FEMUR

Several early studies reported unacceptable subsidencerates. Ponziani et al12 reported unsatisfactory results fromsubsidence in four of 20 revision Wagner stems. Isacsonet al24 reported five of 27 Wagner revisions with subsidencegreater than 2 cm. Kolstad et al36 reported five early revi-sions in 31 hips for dislocation or subsidence. Bircheret al37 reported six of 99 stems that subsided enough torequire repeat revision arthroplasty.
Other complications included dislocation and leg-lengthdiscrepancies. Boisgard et al38 studied 52 revisions with theWagner prosthesis at 44 months and found a high rate of dis-location (8%), leg-length discrepancy (15%), and limp.Gutierrez del Alamo et al39 recently reported 79 revisionWagner femoral components followed up for a minimum of5 years. Eleven dislocations (13.9%) required five repeat revi-sions in the early postoperative period, and stem subsidencewas associated with poor canal fill. Isacson et al24 reportednine of 27 hips that dislocated subsequent to revision.
As surgeons became more familiar with the use of thisfixation method, results gradually improved. Bohm andBischel40 reviewed 129 consecutive revision femoral arthro-plasties with the Wagner SL revision stem (Protek AG, Bern,Switzerland) with a mean follow-up of 8.1 years. Six stemsrequired repeat revision between 0.13 and 4.6 years postop-eratively, with a cumulative survival of 95.2% at 14.1 years.Only one of these stems was revised for subsidence.
With the advent of modular bi-body stems, some ofthese problems were solved but others surfaced. Modularityallowed seating of the distal stem to a level where axial sta-bility was achieved, whereas leg length and offset wereadjusted through the proximal modular body. However,introduction of a modular interface at the subtrochantericlevel, where the highest stresses occur, produced severalreports of stem fractures, some within the first year. Sincethen most manufacturers have recommended that surgeonssupplement distal fixation with some type of proximal sup-port—by using ingrowth bodies and collapsing the ectaticmetaphysis around them to attain bony contact, with orwithout placement of cortical strut grafts, or by usingproximal structural allograft.
Kwong et al41 reviewed 143 patients from three centersreceiving the Link MP modular tapered distal fixation stem(Exactech Inc., Gainesville, Fla.) who were followed for amean of 40 months. Satisfactory results included a 97.2%survival rate and average subsidence of only 2.1 mm. Oneundersized stem subsided 11.3 mm. Murphy and Rodri-guez42 reported minimal subsidence and stable osseointegra-tion in 34 of 35 revision arthroplasties with the same stemfollowed for a minimum of 2 years, although six reoperationswere necessary for recurrent dislocations.
Park et al33 reviewed 62 revision THAs with a fluted,modular, distally tapered stem (Lima-Lto, Udine, Italy).Fifty-two percent of the revisions were performed with anextended trochanteric osteotomy. Mean subsidence was only1.1 mm, and complications included 6% diaphyseal split, 6%cortical perforations, and 5% dislocations. Overall, the ratesof cortical perforation and more than 5 mm stem subsidencewere significantly less in the group treated with an extendedtrochanteric osteotomy.33
Sporer and Paprosky4 reported satisfactory results in 15of 16 patients revised with the Link or ZMR (Zimmer,Warsaw, Ind.) modular fluted, tapered stems in types IIIB andIV femurs at 2.0 years with only one repeat revision.27 Schuhet al43 reported satisfactory results in 77 of 79 revision arthro-plasties with the modular MRP-Titan revision stem (PeterBrehm GmbH,Weisendorf, Germany) at 4-year follow-up.
However, some modular, distally tapered revision stemshave not fared as well. McInnis et al13 reviewed 70 PFMstems (Zimmer) followed for a mean of 47 months. Althoughonly two stems required repeat revision during this period,six (8.6%) were judged to be loose radiographically and84% of the stems subsided a mean 9.9 mm, with one stemsubsiding 52 mm. In addition, seven hips (10%) dislocated,with a mean subsidence of 23 mm.
Several authors have suggested that the use of distallytapered, fluted stems may allow reconstitution of the proxi-mal bone stock. Gutierrez del Alamo et al39 found proximalnew bone regeneration in 50 of 79 hips revised with theWagner stem and an increase in the thickness of the femoralcortex and outer femoral diameter compared with immedi-ate postoperative radiographs. McInnis et al13 noted resto-ration of proximal bone stock in 56% of 70 patients after47 months of follow-up. Bohm and Bischel40 found good,
BA
FIGURE 36–4. Correct axial positioning of taper. A, With less proximalbone loss, the taper should engage higher in the femoral canal, atthe upper level of retained isthmic bone. B, With more extensivefemoral bone loss, a longer stem is needed to position the taper toengage the highest level of intact femoral isthmus.
359C H A P T E R 36 Tapered, Fluted Femoral Fixation

A B
C D
FIGURE 36–5. Extended trochanteric osteotomy. A, The osteotomy is made along the proximal shaft of the femur from posterior to anterior,hinging it on the attached anterior soft tissues. B, Reaming of the intact femoral canal after removal of the loose prosthesis and placing aprophylactic cable around the upper end of the intact femoral cortical tube, just distal to the osteotomy. C, Distally tapered, fluted stem beinginserted into the intact femoral isthmus. D, Proximal modular body attached to distal stem and extended osteotomy being cabled backaround proximal prosthesis.
19 mm 19 mm 38 mm
14 mm 13 mm 12 mm 3.0° 10 mm
FIGURE 36–6. The magnitude of the distal taper angle affects the resistance to subsidence and the amountof taper in contact with bone. Most newer designs use an included taper angle of approximately3 degrees. With a 3-degree taper angle, each millimeter of increased diameter reamed increases thelongitudinal contact area by 19 mm.
360 REVISION THA: THE FEMUR

or excellent restoration of proximal femoral bone stock in88% of 129 Wagner stems followed up for 8.1 years. Othershave noted similar reconstitution of proximal bone stockafter revision with distally fixed, tapered revisionstems.24,31,36,44,45
SUMMARY
Tapered, fluted, distal fixation femoral stems have provided analternative for dealing with the complex revision femur.Although a unique set of complications may occur when usingdistal fixation of this type, the philosophy of fixation intoremaining good bone is practical. Modularity has providedgreater flexibility and predictability of results, although it alsohas created new problems inherent to the modular junction.
Although the revision hip surgeon has several alterna-tives available, the tapered, fluted, distal fixation stem is thetreatment of choice for femora with a nonsupportive meta-physis and some remaining intact diaphysis. It also providesan excellent option for periprosthetic femur fractures thatrender the proximal femur nonsupportive.
FUTURE CONSIDERATIONS
The concept of distal femoral fixation with a taper and fluteshas created another option for revision of the proximallydeficient femur, but present modular designs still have pro-blems. Modular junctions must be strengthened or elimi-nated to control the risk of stem fracture. Axial stabilityremains somewhat unpredictable, particularly in soft, osteo-porotic bone. Other methods of achieving axial stabilitylikely will be developed in the future to ensure that stemsdo not subside. In addition, better means of rebuilding prox-imal bone stock in these deficient femora will be imperativebecause younger and younger patients are requiring revisionarthroplasties. As with any technology, innovative designmodifications will likely improve current results.
R E F E R E N C E S
1. Kurtz S, Ong K, Lau E, et al: Projections of primary and revisionhip and knee arthroplasty in the United States from 2005 to 2030,J Bone Joint Surg (Am) 89A(4):780–785, 2007.
2. Franzen H, Mjoberg B, Onnerfalt R: Early loosening of femoralcomponents after cemented revision. A roentgen stereophotogram-metric study, J Bone Joint Surg (Br) 74B:721–724, 1992; erratum75B:169, 1993.
3. Busch CA, Charles MN, Haydon CM, et al: Fractures of distally-fixed femoral stems after revision arthroplasty, J Bone Joint Surg(Br) 87(10):1333–1336, 2005.
4. Sporer SM, Paprosky WG: Revision total hip arthroplasty: the limitsof fully coated stems, Clin Orthop Relat Res Dec(417):203–209, 2003.
5. Weeden SH, Paprosky WG: Minimal 11-year follow-up of exten-sively porous-coated stems in femoral revision total hip arthroplasty,J Arthroplasty 17(4 suppl 1):134–137, 2002.
6. Moreland JR, Moreno MA: Cementless femoral revision arthro-plasty of the hip: minimum 5 years followup, Clin Orthop Relat ResDec(393):194–201, 2001.
7. Meek RM, Garbuz DS, Masri BA, et al: Intraoperative fracture ofthe femur in revision total hip arthroplasty with a diaphyseal fittingstem, J Bone Joint Surg (Am) 86A(3):480–485, 2004.
8. Wagner H: Revision prosthesis for the hip joint in severe bone loss[in German], Orthopade 16(4):295–300, 1987.
9. Lyu SR: Use of Wagner cementless self-locking stems for massivebone loss in hip arthroplasty, J Orthop Surg (Hong Kong) 11(1):43–47, 2003.
10. Isacson J, Stark A, Wallensten R: The Wagner revision prosthesisconsistently restores femoral bone structure, Int Orthop 24(3):139–142, 2000.
11. Kolstad K, Adalberth G, Mallmin H, et al: The Wagner revisionstem for severe osteolysis. 31 hips followed for 1.5-5 years, ActaOrthop Scand 67(6):541–544, 1996.
12. Ponziani L, Rollo G, Bungaro P, et al: Revision of the femoral pros-thetic component according to the Wagner technique, Chir OrganiMov 80(4):385–389, 1995.
13. McInnis DP, Horne G, Devane PA: Femoral revision with a fluted,tapered, modular stem seventy patients followed for a mean of 3.9years, J Arthroplasty 21(3):372–380, 2006.
14. ZMR hip system: surgeon manual, Warsaw, IN, 2003, Zimmer.15. Nadaud MC, Griffin WL, Fehring TK, et al: Cementless revision
total hip arthroplasty without allograft in severe proximal femoraldefects, J Arthroplasty 20(6):738–744, 2005.
16. Blackley HR, Davis AM, Hutchison CR, et al: Proximal femoralallografts for reconstruction of bone stock in revision arthroplastyof the hip: a nine to fifteen-year follow-up, J Bone Joint Surg (Am)83A:346–354, 2001.
17. Oakes DA, Cabanela ME: Impaction bone grafting for revision hiparthroplasty: biology and clinical applications, J Am Acad OrthopSurg 14(11):620–628, 2006.
18. Haddad FS, Masri BA, Garbuz DS, et al: Femoral bone loss in totalhip arthroplasty: classification and preoperative planning, InstructCourse Lect 49:83–96, 2000.
19. Della Valle CJ, Paprosky WG: Classification and an algorithmicapproach to the reconstruction of femoral deficiency in revisiontotal hip arthroplasty, J Bone Joint Surg (Am) 85A:1–6, 2003.
20. Duncan CP, Masri BA: Fractures of the femur after hip replacement,Instr Course Lect 44:293–304, 1995.
21. Wagner H: Revision of femoral stem with important loss of bonestock. In Gallinaro P, ed: Postgraduate lectures of the first EuropeanFederation of National Associations of Orthopaedics and Traumatology(EFORT), Paris, 1993, Masson, p 74.
22. Boisgard S, Moreau PE, Tixier H, et al: Bone reconstruction, leglength discrepancy, and dislocation rate in 52 Wagner revision totalhip arthroplasties at 44-month follow-up [in French], Rev ChirOrthop Reparatrice Appar Mot 87(2):147–154, 2001.
23. Weber M, Hempfing A, Orler R, et al: Femoral revision using theWagner stem: results at 2–9 years, Int Orthop 26(1):36–39, 2002.
24. Isacson J, Stark A,Wallensten R: TheWagner revision prosthesis con-sistently restores femoral bone structure, Int Orthop 25(1):63–64, 2001.
25. Department of Health and Ageing, Therapeutic Goods and Admin-istration: Femoral stem fractures in Zimmer Modular Revision (ZMR)hip systems. Available at: http://www.tga.gov.au/docs/html/tganews/news40/iris.htm#femoral.
26. Pierson JL, Crowninshield RD, Earles DR: Fatigue fracture of a mod-ular revision femoral component: a report of forty cases, AAOS AnnualMeeting, Washington, DC, February 25, 2005.
27. Sporer SM, Paprosky WG: Femoral Fixation in the face of consider-able bone loss. The use of modular stems, Clin Orthop Relat Res Dec(429):227–231, 2004.
28. Mulay S, Hassan T, Birtwistle S, et al: Management of types B2 andB3 femoral periprosthetic fractures by a tapered, fluted, and distallyfixed stem, J Arthroplasty 20(6):751–756, 2005.
29. Ko PS, Lam JJ, Tio MK, et al: Distal fixation with Wagner revisionstem in treating Vancouver type B2 periprosthetic femur fractures ingeriatric patients, J Arthroplasty 18(4):446–452, 2003.
30. Eingartner C, Volkmann R, Ochs U, et al: Intramedullary stabiliza-tion of periprosthetic fractures of the femur taking special accountof bone defects, Oper Orthop Traumatol 18(4):341–363, 2006.
31. Berry DJ: Treatment of Vancouver B3 periprosthetic femur fractureswith a fluted tapered stem,ClinOrthopRelat ResDec(417):224–231, 2003.
32. Peters PC, Head WC, Emerson RH: An extended trochantericosteotomy for revision total hip replacement, J Bone Joint Surg(Br) 75B:158–159, 1993.
33. Park YS, Moon YW, Lim SJ: Revision total hip arthroplasty using afluted and tapered modular distal fixation stem with and withoutextended trochanteric osteotomy, J Arthroplasty 22(7):993–999, 2007.
361C H A P T E R 36 Tapered, Fluted Femoral Fixation

34. Hacking SA, Bobyn JD, Tanzer M, et al: The osseous response tocorundum blasted implant surfaces in a canine hip model, ClinOrthop Relat Res Jul(364):240–253, 1999.
35. Min B, Longjohn DB, Dorr LD, et al: Radiographic comparison ofdiaphyseal grit blasted with smooth surface stems by matched pairanalysis, Clin Orthop Relat Res Dec(381):156–167, 2000.
36. Kolstad K, Adalberth G, Mallmin H, et al: The Wagner revisionstem for severe osteolysis. 31 hips followed for 1.5-5 years, ActaOrthop Scand 67(6):541–544, 1996.
37. Bircher HP, Riede U, Luem M, et al: The value of the Wagner SLrevision prosthesis for bridging large femoral defects [in German],Orthopade 30(5):294–303, 2001; erratum 30(7):443, 2001.
38. Boisgard S, Moreau PE, Tixier H, et al: Bone reconstruction, leglength discrepancy, and dislocation rate in 52 Wagner revision totalhip arthroplasties at 44-month follow-up [in French], Rev ChirOrthop Reparatrice Appar Mot 87(2):147–154, 2001.
39. Gutierrez del Alamo J, Garcia-Cimbrelo E, Castellanos V, et al:Radiographic bone regeneration and clinical outcome with theWagner SL revision stem: a 5-year to 12-year follow-up study,J Arthroplasty 22(4):515–524, 2007.
40. Bohm P, Bischel O: The use of tapered stems for femoral revisionsurgery, Clin Orthop Relat Res Mar(420):148–159, 2004.
41. Kwong LM, Miller AJ, Lubinus P: A modular distal fixation optionfor proximal bone loss in revision total hip arthroplasty: a 2- to6-year follow-up study, J Arthroplasty 18(3 suppl 1):94–97, 2003.
42. Murphy SB, Rodriguez J: Revision total hip arthroplasty with prox-imal bone loss, J Arthroplasty 19(4 suppl 1):115–119, 2004.
43. Schuh A, Werber S, Holzwarth U, et al: Cementless modular hiprevision arthroplasty using the MRP Titan Revision Stem: outcomeof 79 hips after an average of 4 years’ follow-up, Arch Orthop TraumaSurg 124(5):306–309, 2004.
44. Volkmann R, Bretschneider C, Eingartner C, et al: Revision arthro-plasty—femoral aspect: the concept to solve high grade defects, IntOrthop 27(suppl 1):S24–S28, 2003.
45. Voigt C, Zimmer-Amrheim S, Enes-Gaiao F, et al: Using of aWagner stem in revision-arthroplasty following loosening of a totalhip endoprosthesis [in Slovak], Acta Chir Orthop Traumatol Cech61(2):77–80, 1994.
362 REVISION THA: THE FEMUR