Sympatheetomy for Raynaud's Phenomenon -...
10
Sympatheetomy for Raynaud's Phenomenon Follow-Up Study of 70 Women with Raynaud's Disease and 54 Women with Secondary Raynaud's Phenomenon By RAY W. GIFFORD, JR., M.D., EDGAR A. HINES, JR., M.D., AND WINCHELI McK. CRAIG, M.D. Follow-up information has been obtained from 70 women with Raynaud's disease and 54 women with secondary Raynaud's phenomenon who hsere subjected to surgical sympathetic denervation of one extremity or more. The results of sympathectomy in the upper and lower extremities are described. The effect of operation on the subsequent course, the complications and sequelae are presented and compared with the reports of others. GIFFORD and Hines' reviewed the clinical data from the records of 474 female pa- tients who had been seen at the Mayo Clinic from 1920 through 1945 and for whom a diag- nosis of Raynaud's disease had been confirmed by use of the criteria of Allen and Brown.2' Three hundred ninety-seven of these patients were treated by nonsurgical methods and the results presented. Seventy-seven women were subjected to surgical sympathetic denervation of one or more extremity. In this report the results of surgical sympathectomy are evalu- ated in the 70 women with Raynaud's disease in whom we have adequate follow-up informa- tion and in 54 women with secondary Raynaud's phenomenon. RAYNAUD'S DISEASE Method of Study. The diagnosis of Raynaud's disease was established either preoperatively or postoperatively in all cases by reference to the criteria of Allen and Brown.2, Stated briefly, these criteria are (1) episodes of Ray- naud's phenomenon excited by cold or emotion; (2) bilaterality of Raynaud's phenomenon; (:3) absence of gangrene, or, if present, its limitation to minimal grades of cutaneous gangrene; (4) absence of any other primary disease that might be causal, such as occlusive arterial disease, acrosclerosis, cervical rib, or organic disease of the nervous system, and (5) symptoms for at least 2 years. Cases of secondary Raynaud's phenomenon were carefully excluded. From the Mayo Clinic and the Mayo Foundation, Rochester, Minn. The Mayo Foundation, Rochester, Minn., is a part of the Graduate School of the Uni- versity of Minnesota. 5 Follow-up data were obtained by question- naire, by re-examination at the clinic, or both. Age at Onset and Duration of Symptoms Prior to Sympathectomy. The ages at onset of Ray- naud's disease as well as at time of sympathe(- tomy of the 70 patients are given in table 1. Ninety-three per cent of the patients were less than 40 years old and 70 per cent were less than 30 years old when symptoms of Raynaud's disease were first, noted. Seventy-three per cent were less than 40 years of age when sympa- thectomy was undertaken. The shortest dura- tion of Rlaynaud's phenomenon at time of sympathectomy was 1 year for 3 patients, and the longest duration of symptoms before opera- tion was 23 years for 1 patient. The mean durn- tion of symptoms before operation was 7 years. Eighty-one per cent had had symptoms for 10 years or less. Six patients were operated on less than 2 years after onset of symptoms, but for all, follow-up data were more than adequate to satisfy the fifth criterion of Allen and Brown. Location of Raynaud's Phenomenon. Ray- naud's phenomenon occurred in the fingers of both hands of all 70 patients. Fifty-one pa- tients noted vasomotor phenomena in the toes also, and the nose of one was similarly affected. Precipitating Factors. Exposure to cold was the only precipitating factor for Raynaud's phenomenon cited by 46 women. The remain- ing 24 stated that emotional reactions as Adell as exposure to cold were responsible. Phases of Color Change. Detailed descrip- tions of the phases of color change were avail- able for only 22 patients. Seventeen had the typical 3-phase color changes (pallor to cyano- sis to rubor), 4 had only 2 phases of color change, and 1 described pallor only. Circulation, Volume XVII, January 1958 by guest on May 25, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript of Sympatheetomy for Raynaud's Phenomenon -...

Sympatheetomy for Raynaud's PhenomenonFollow-Up Study of 70 Women with Raynaud's Disease and 54
Women with Secondary Raynaud's Phenomenon
By RAY W. GIFFORD, JR., M.D., EDGAR A. HINES, JR., M.D., AND WINCHELI McK. CRAIG, M.D.
Follow-up information has been obtained from 70 women with Raynaud's disease and 54 women
with secondary Raynaud's phenomenon who hsere subjected to surgical sympathetic denervationof one extremity or more. The results of sympathectomy in the upper and lower extremities are
described. The effect of operation on the subsequent course, the complications and sequelae are
presented and compared with the reports of others.
GIFFORD and Hines' reviewed the clinicaldata from the records of 474 female pa-
tients who had been seen at the Mayo Clinicfrom 1920 through 1945 and for whom a diag-nosis of Raynaud's disease had been confirmedby use of the criteria of Allen and Brown.2'Three hundred ninety-seven of these patientswere treated by nonsurgical methods and theresults presented. Seventy-seven women weresubjected to surgical sympathetic denervationof one or more extremity. In this report theresults of surgical sympathectomy are evalu-ated in the 70 women with Raynaud's diseasein whom we have adequate follow-up informa-tion and in 54 women with secondary Raynaud'sphenomenon.
RAYNAUD'S DISEASE
Method of Study. The diagnosis of Raynaud'sdisease was established either preoperativelyor postoperatively in all cases by reference tothe criteria of Allen and Brown.2, Statedbriefly, these criteria are (1) episodes of Ray-naud's phenomenon excited by cold or emotion;(2) bilaterality of Raynaud's phenomenon; (:3)absence of gangrene, or, if present, its limitationto minimal grades of cutaneous gangrene; (4)absence of any other primary disease that mightbe causal, such as occlusive arterial disease,acrosclerosis, cervical rib, or organic disease ofthe nervous system, and (5) symptoms for atleast 2 years. Cases of secondary Raynaud'sphenomenon were carefully excluded.
From the Mayo Clinic and the Mayo Foundation,Rochester, Minn. The Mayo Foundation, Rochester,Minn., is a part of the Graduate School of the Uni-versity of Minnesota.
5
Follow-up data were obtained by question-naire, by re-examination at the clinic, or both.Age at Onset and Duration of Symptoms Prior
to Sympathectomy. The ages at onset of Ray-naud's disease as well as at time of sympathe(-tomy of the 70 patients are given in table 1.Ninety-three per cent of the patients were lessthan 40 years old and 70 per cent were less than30 years old when symptoms of Raynaud'sdisease were first, noted. Seventy-three per centwere less than 40 years of age when sympa-thectomy was undertaken. The shortest dura-tion of Rlaynaud's phenomenon at time ofsympathectomy was 1 year for 3 patients, andthe longest duration of symptoms before opera-tion was 23 years for 1 patient. The mean durn-tion of symptoms before operation was 7 years.Eighty-one per cent had had symptoms for 10years or less. Six patients were operated on lessthan 2 years after onset of symptoms, but forall, follow-up data were more than adequateto satisfy the fifth criterion of Allen and Brown.
Location of Raynaud's Phenomenon. Ray-naud's phenomenon occurred in the fingers ofboth hands of all 70 patients. Fifty-one pa-tients noted vasomotor phenomena in the toesalso, and the nose of one was similarly affected.
Precipitating Factors. Exposure to cold wasthe only precipitating factor for Raynaud'sphenomenon cited by 46 women. The remain-ing 24 stated that emotional reactions as Adell asexposure to cold were responsible.
Phases of Color Change. Detailed descrip-tions of the phases of color change were avail-able for only 22 patients. Seventeen had thetypical 3-phase color changes (pallor to cyano-sis to rubor), 4 had only 2 phases of colorchange, and 1 described pallor only.
Circulation, Volume XVII, January 1958
by guest on May 25, 2018
http://circ.ahajournals.org/D
ownloaded from

GIFFORD, HINES, AND CRAIG
TABLE 1.-Ages of 70 Women with Surgical Treatment
Age (years)
Less than 10......10-19.............20-29...........30-39.............40-49.............50-55............Total ...........
Patients
At onset ofRaynaud's disease
22027165070
At time ofsympathectomy*
0
52818172
70
Youngest ......... 4 16Oldest ............ 42 55Mean ............. 25 32
* In cases in which more than one sympathectomywas done, age at time of first operation was recorded.
Family History. Only 2 patients gave a familyhistory of Raynaud's disease.
Associated Diagnoses. Thirteen of the 70patients were sufficiently troubled by variousfunctional and neurotic symptoms (exclusiveof migraine headache) to warrant their inclu-sion among the final diagnoses. Ten patientshad migraine headaches, and 2 had arterialhypertension (greater than 150 mm. Hgsystolic and 90 mm. Hg diastolic).
Incidence of Complications Before Operation.Only 24 (34 per cent) of the 70 women were
free of the complications of Raynaud's diseasebefore the diagnosis was first made at theclinic. Twenty-one (30 per cent) had or gave a
history of trophic changes* in the fingers. Onepatient had trophic changes in the toes. Tenwomen (14 per cent) had evidence of sclerodac-tyliat in the fingers when sympathectomy was
performed. Thirteen (19 per cent) had bothtrophic changes and sclerodactylia in the fingerspreoperatively and 1 had trophic changes andsClerodactylia in the fingers and toes. Onewoman had calcinosis in the finger tips in addi-
* By trophic changes we mean ulceration, necrosis,chronic or recurrent paronychia, scarring, andfissuring
t For the purposes of this paper sclerodacty liawill be defined as sclerodermatous changes confinedto the skin of the digits. As a complication of Ray-naud's disease it remains localized in the acral partsin contradistinction to the progressive selerodermathat is characteristic of acrosclerosis and diffusescleroderma.
tion to trophic lesions and sclerodactylia. Anonhealing and painful ulcer had led to ampu-tation of the terminal phalanx of the left thirdfinger of 1 patient before she was first seen atthe clinic.
In summary, 51 per cent of the patients withRaynaud's disease had or gave a history oftrophic lesions of the digits and 34 per cent hadsclerodactylia. These figures include the 20 percent who had both.That patients with the more severe lesions
were chosen for sympathectomy is amply dem-onstrated by comparing these figures with theincidence of initial complications among thepreviously reported group' treated conserva-tively. Among 307 such patients only 3 per centhad trophic changes in the digits, 7 per cent hadsclerodactylia, and 2 per cent had both whenthe diagnosis of Raynaud's disease was firstmade or suspected at the clinic. Amputationof terminal phalanges of 2 toes had been neces-sary for 1 woman.The mean age at onset of Raynaud's disease
was lower for the surgical group (25 years) ascompared to the nonsurgical group (33 years).Emotional reactions were factors in precipi-tating Raynaud's phenomenon in a greaterpercentage of the surgically treated group.
Types of Sympathectomy. Eighty-nine opera-tions to interrupt sympathetic nervous path-ways were performed on the 70 women withRaynaud's disease, and the types of proceduresemployed are listed in table 2. Sympathectomywas performed on 52 women for the upperextremities only, for the lower extremities onlyfor 2 women, and for both the upper and thelower extremities for 16 women. More extensiveganglionectomy was performed on 2 womenwho had obtained no relief from earlier ganglion-ectomy. Each is included as only 1 operationin table 2. Three women underwent cervicotho-racic ganglionectomy after resection of thethoracic trunk had failed to give relief. Only thefinal result for each patient will be included insubsequent tables. Bilateral procedures wereconsidered and evaluated as 1 operation be-cause in most cases the responses betweenpaired denervated extremities did not vary ap-preciably.The cervicothoracic ganglionectomy of Ad-
6
by guest on May 25, 2018
http://circ.ahajournals.org/D
ownloaded from

SYMPATHECTOMY FOR RAVNAUD'S PHENOMENON
son4 consists of the extirpation of the stellateganglion and, usually but not always, of thesecond thoracic sympathetic ganglion througha posterior approach. It is a postganglionicsympathectomy. Resection of the thoracictrunk, proposed independently by Smithwick5and Telford,6 consists of dividing the sympa-thetic chain between the third and fourththoracic ganglia and dividing the rami to thesecond and third ganglia. The second and thirdthoracic nerves are divided proximal to thesensory root ganglia. No ganglia are removedand hence this is a preganglionic sympathec-tomy. The anterior rhizotomy performed for 1patient was a variation of the preganglionicsympathectomy.
Duration of Follow-up after Sympathectomy.The period of postoperative follow-up for these70 women varied from 1 to 28 years and themean was 12 years. The mean period of fol-low-up after cervicothoracic sympathectomywas 11 years, and after lumbar sympathectomy14 years.
Effect of Sympathectomy on Raynaud'sPhenomenon. Forty-three (63 per cent) of the68 patients with Raynaud's disease who under-
TABLE 2. Types of Sympathectomy Performedon 70 Women
Type of operation
Cervicothoracic ganglionec-tomy (Adson)
unilateral ...................bilateral ....................
Resection of thoracic trunk(Smithwick; Telford)
bilateral ....................Undetermined type (per-
formed elsewhere)unilateral ...................bilateral ....................
Bilateral rhizotomy(T2 3. 4 , 5) .. .. .. .. .. .. ..
Bilateral lumbar sympathec-tomy.........
Total ...
Operations
153
9
16
1
1889*
* More than one operation was performed on 19women as follows: thoracic trunk resection followedlater by cervicothoracic ganglionectomy on 3;bilateral lumbar sympathectomy in addition tosympathectomy for upper extremities on 16. Tenoperations were performed elsewhere.
TABLE 3.--Effect of Sympathectomy on Raynaud'sPhenomenon
Raynaud's phenomenonafter operation
Disappeared ......Improved....Same or worse....Total ...........
Patients having extremities denervated
Upper
9342568
Lower
1521
18
vent sympathectomy for the upper extremitiesnoted definite lessening in the severity and fre-quency of Raynaud's phenomenon after opera-tion (table 3). For 9 of these patients Raynaud'sphenomenon disappeared entirely. Complica-tions of Raynaud's disease in the form oftrophic lesions of the digits or sclerodactylia orboth were present preoperatively for 45 percent of the women who obtained complete re-lief from Raynaud's phenomenon; complica-tions were present preoperatively for almost 70per cent of those who obtained only partial orno relief. There were no striking differences inthe results produced by preganglionic and post-ganglionic procedures.
In striking contrast to the results of sympa-thectomy for the upper extremities are theresults obtained by lumbar sympathectomy forthe lower extremities. Complete and permanentrelief from Raynaud's phenomenon in the feetwas obtained for 83 per cent of these patients
TABLE 4. Effect of Sympathectomy on Trophic Lesionsand Sclerodactylia
Effect on lesion
Present before operationDisappeared ...........Improved ..............Same or worse.........
Not present beforeoperation
None after operation.Appeared after opera-
tion...............Total ................
Trophic lesionsof patientshaving
extremitiesdenervated
Upper Lower
13 18 014 0
29
468
16
Sclerodactyliaof patientshaving
extremitiesdenervated
Upper Lower
588
34
1 618 61*
000
18
018
* Follow-up data insufficient for evaluation in 7cases.
7
by guest on May 25, 2018
http://circ.ahajournals.org/D
ownloaded from

GIFFORD, HINES, ANI) CRAIG
with Raynaud's disease and only 1 patient (6per cent) failed to obtain any relief. Only 1patient had complications of Raynaud's diseasein the feet before operation, and she obtainedan excellent result.
Effect of Sympathectomy on Trophic Lesions.Trophic lesions were present on the fingers of35 patients with Raynaud's disease beforecervicothoracic sympathectomy. Thirty-sevenper cent of these women had no further diffi-culty with trophic lesions after operation.Sympathectomy reduced the severity and fre-quency of trophic lesions of 23 per cent butfailed to give permanent improvement of thetrophic lesions of 40 per cent (table 4).
Trophic lesions of the fingers appeared forthe first time after cervicothoracic sympathec-tomy in 4 (12 per cent) of 33 women withRaynaud's disease. With regard to trophiclesions of the upper extremities, the results ob-tained by preganglionic procedures were notsignificantly different from those obtained bypostganglionic procedures. Lumbar sympa-thectomy was followed by complete disappear-ance of trophic lesions of the toes in the onlycase of Raynaud's disease in which they werepresent preoperatively. Trophic lesions of thetoes developed postoperatively in 1 of 17women who had no such lesions preoperatively.
Effect of Sympathectomy on Sclerodactylia.Twenty-four patients with Raynaud's diseasehad sclerodactylia of the fingers before cervi-cothoracic sympathectomy was performed, butfollow-up data with regard to sclerodactyliawere adequate for cnly 21. Five (24 pet cent)noted complete regression of sclerodactylia aftersympathectomy, and 8 (38 per cent) noteddefinite improvement (table 4). Sclerodactyliawas not present preoperatively on the fingersof 44 women. Postoperative follow-up datawere adequate with regard to sclerodactylia foronly 40 women of whom 6 (15 per cent) firstnoted sclerodactylia postoperatively. Therewas no appreciable difference between pre-ganglionic and postganglionic procedures withregard to their effect on sclerodactylia of theupper extremities.
Sclerodactylia was not present in the toes ofany patient undergoing lumbar sympathectomyeither before or after operation.
Incidence of Calcinosis after Sympathectomy.Calcinosis developed postoperatively in thefingers of 5 (7 per cent) of the 68 women withRaynaud's disease who had undergone sympa-thectomy for the upper extremities. All 5 hadtrophic lesions or sclerodactylia or both preop-eratively and these complications persisted invarying degrees of severity after operation. Allhad undergone bilateral stellate ganglionee-tomy, and for 4 of the 5 women the secondthoracic ganglia were extirpated also. Ray-naud's phenomenon failed to improve afteroperation for 4 of the 5 women who subse-quently developed calcinosis.The one woman who had calcinosis before
sympathectomy was subj ected to cervicotho-racic sympathectomy (type unknown) else-where. The result was unsatisfactory in allrespects, in that Raynaud's phenomenon,trophic lesions, sclerodactylia, and calcinosispersisted with undiminished severity.
Incidence of Amputation after Sympathec-tomy. Two women (3 per cent) of the 68 whounderwent sympathectomy for Raynaud'sdisease of the upper extremities lost parts offingers at a later time. No patient requiredamputation of toes after lumbar sympathec-tomy.A woman, aged 27 years, had had Raynaud's
phenomenon for 2 years when she was first seenat the clinic in 1944. A sweating test showedthat sympathectomy performed elsewhere forthe upper extremities was incomplete. Becauseof recurrent ulcerations of the tips of the fingers,bilateral stellate and second thoracic ganglion-ectomy was performed in 1944. For 2 yearsafter operation considerable improvement inthe Raynaud's phenomenon and in the recur-rent ulcerations of the fingers occurred. There-after symptoms recurred and the patient finallylost the distal phalanx of the right secondfinger due to painful, infected ulcerations.Whether this phalanx was amputated orsloughed spontaneously is not clear from fol-low-up data.A woman, aged 48 years, had had Raynaud's
disease for 23 years before bilateral stellateganglionectomy was performed in 1942. For5 years after operation she was free of allsymptoms including trophic lesions and scle-
8
by guest on May 25, 2018
http://circ.ahajournals.org/D
ownloaded from

SYMPATHECTOMY FOR RAYNAUD 'S PHENOMENON
rodactylia that were present initially. In1948, infected ulcers developed at the tips ofthe thumb and second, third, and fourth fingersof the right hand, and sclerodactylia was againevident. A sweating test indicated completesympathetic denervation of the upper extremi-ties. The distal 2 phalanges of the right ringfinger had to be amputated.As mentioned previously, 1 woman, aged 21
years who. had had Raynaud's disease for 3years, had required amputation of the distalphalanx of the left third finger before comingto the clinic the first time in 1944. Bilateralstellate ganglionectomy was performed at theclinic. In the ensuing 7 years she had no furthertrouble with trophic lesions of the fingers andRaynaud's phenomenon was much less trouble-some. Scierodactylia was not present at anytime.
Over-all Resuits of Sympathectomy. Heretoforethe effects of sympathectomy on Raynaud'sphenomenon, trophic lesions, and sclerodactyliahave been considered separately. Such evalua-tion does not take into consideration the factthat in a single patient sympathectomy mayhave dissimilar effects on Raynaud's phenome-non and the pre-existing complications ofRaynaud's disease. Striking improvement inonly 1 (ategory was often responsible for agreater degree of rehabilitation than moderateimprovement in 2 or 3 categories. Conversely,striking improvement in nondisabling symp-toms was occasionally nullified by lack ofimprovement in the most disabling symptomor complication. An attempt has been made,therefore, to evaluate the total result of sym-pathectomy for each patient individually,taking into consideration preoperative andpostoperative disability according to the fol-lowing criteria:
1. An excellent result indicates absolutely nodisability from Raynaud's disease. To be in-cluded in this group a patient must have ob-tained complete and permanent relief not onlyfrom Raynaud's phenomenon but also fromany preoperative complications that may haveexisted.
2. A good result indicates definite and oftenstriking reduction in disability from Raynaud'sdisease. Many patients included in this group
Over-all results
Excellent .........
Good .............
Fair ...........Poor ..............
Total ..........
Patients having extremities denervated
Upper Lower
7 1530 26 0
25* 168t 18
* Incomplete denervation in 4 patients indicatedby sweating test.
t Two women (3 per cent) required amputation ofphalanges in follow-up period.
might well have been included in the group ofexcellent results had minor symptoms not per-sisted.
3. A fair result indicates only modest im-provement with continuation or recurrence ofdisability after operation, although less markedthan preoperatively. Usually the most disablingsymptom was least improved.
4. A poor result indicates that disability con-
tinued or recurred postoperatively with un-
abated severity. In some cases new complica-tions of Raynaud's disease appeared, so thatdisability was actually greater after operation.The results of sympathectomy for Raynaud's
disease according to these criteria are given intable 5. In the upper extremities sympathec-tomy yielded good or excellent results for 54per cent of cases. In 4 women persistence ofsweating in the hands indicated that denerva-tion of the upper extremities was incompleteafter sympathectomy and they failed to obtainrelief. If these cases are excluded from theseries, the proportion of patients obtaininggood or excellent results is increased to 58 per
cent. Good or excellent results were apparentimmediately after sympathectomy, and im-provement was maintained throughout theperiod of follow-up. However, of the 31 women
for whom sympathectomy yielded a fair or poor
result, the failure was apparent immediatelyafter operation for only 8 (26 per cent). Theremainder had relapses after showing consider-able improvement for periods that varied from2 months to 6 years after operation.Only 1 patient from the group with good or
excellent results was followed for less than 2years postoperatively, and only 5 from this
TABLE 5. Over-All Results of Sympathectoiny_-
9
by guest on May 25, 2018
http://circ.ahajournals.org/D
ownloaded from

GIFFORD, HINES, AND CRAIG
group were followed for less than 5 years. Themean period of postoperative follow-up forthis group was 12 years.Good or excellent results were obtained ill 65
per cent of the women without complicationsof Raynaud's disease before operation, whereasonly 49 per cent of women with complicationsbefore operation obtained good or excellent re-sults. Otherwise there was no correlation be-tween preoperative data and the result obtainedby synipathectomy. Specifically, the resultobtained by sympathectomy in the upperextremities did not seem to be influenced byage (either at onset of the disease or at time ofoperation), duration of symptoms beforeoperation, the incidence of emotional reactionsas precipitating factors for the vasospasticphenomena, or the use of tobacco. Likewise,the type of sympathectomy performed seemedto have no influence on the final results.Good or excellent results were obtained for
94 per cent of women who had lumbar sympa-thectomies for Raynaud's disease of the feet.Eighty-three per cent got excellent (completeand permanent) relief. Only 1 patient who hadlumbar sympathectomy had complications ofRlaynaud's disease in the feet later.
Sixteen women had sympathectomy in bothupper and lower extremities and none obtaineda better result in the upper extremities than inthe lower. In 11, the results in the lowerextremities were better than in the upperextremities and in 5 the results in the upperand lower extremities were the same.
Fifty-two women had undergone sympathec-tomy for the upper extremities only. Thirty-three of these women also had Raynaud's dis-ease of the lower extremities but not severeenough to warrant lumbar sympathectomy.After cervicothoracic sympathectomy, Ray-naud's disease became more marked in thelower extremities of 7 of these 33 women, re-mained unchanged in 1, and improved or dis-appeared in 14. There was inadequate follow-upinformation concerning Raynaud's disease inthe lower extremities in the remaining 11.
Causes of Death in Follow-up Period. Sixwomen who had undergone sympathectomy forRaynaud's disease died during the period offollow-up. There was no operative mortality,
and all deaths occurred at least 1 year aftersympathectomy. One pat ent died of pneu-monia, 1 of pulmonary tuberculosis, and 1 diedsuddenly after injection of a local anestheticagent. Causes of death in the remaining 3women were unknown. Ages at time of deathvaried from 30 to 52 years and averaged 39years. All had had Raynaud's disease for atleast 10 years prior to death. The sympathec-tomy had given good or excellent results for allexcept 1 of the patients who died.
DLscuTssoNWhen results of this study are compared with
results of previous similar investigations (table6), it should be remembered that all of onalpatients were women and all had Raynatid'sdisease. All cases of secondary Raynaud'sphenomenon were carefully separated. Previousauthors have not confined their folow-upstudies to women, a though by the nature ofthe disease, the majority would be women, andsome have included patients with secondaryRaynaud's phenomenon and other arteriospas-tic diseases such as livedo reticularis and acro-cyainosis. We have no reason to believe that theresults of sympathectomy for Raynaud'sdisease would be different in male patients, butno large series is available for comparisonM.Apparent y Raynaud's disease is not severe inlmen, since Hines and Christensenll4 reportedthat only 2 of 69 male patients with Raynaud'sdisease were subjected to sympathectomy. Bothobtained satisfactory results.We are in agreement with all previous
authors that the results of sympathectomy forRaynaud's disease are vastly better and morepredictable in the lower extremities than inthe upper.
Like others, we have found a high incidenceof relapse in the first few years after sympathee-tomy in the upper extremities. Blain and col-leagues"' observed relapse as late as 13 yearsafter cervicothoracic sympathectomy wheieasBarcroft and Hamilton,9 and Kinmonth andHadfield'3 stated that most failures are evidentwithin the first year after operation. Our dataindicate that most relapses occur within thefirst 2 years after operation, as shown by 1ielderand colleagues,10 although in our study 1 re-
10
by guest on May 25, 2018
http://circ.ahajournals.org/D
ownloaded from
SYMIPATHEC(TOMY FOR RAYNAUI)'S PHENOMENON
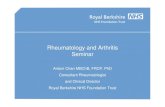
TABLE 6.-Review of the Literature on Sympathec-tomiy for Raynaud's Disease and Allied Conditions*
Author and date
Telford, 19447..
Haxton, 19478..Barcroft andHamilton ,91948..... ...
Felder and co-
workers,'0 1949Blain, Coller,and Carver,1951" ........
Robertson andSmithwick,'21951..........
Kinmonth andHadfield,'31952.........
Gifford, Hines,and Craig, 195'
Results in per cent of casesor extremities
Follow- Upper extremities Lower extremitiesUP
(years) Good Good
oro
ex- Fair Poor excel Fair Poorcel- lentlent
More 43 22 35 100 - _than
1-14 35 20 45 57 29 14
1-6 89
'2-20 64
4-15 58
5-15 45
1-13 69
71-28 54
42
13
9
11
36
42
13
18
37
70
100
100
94
* Some authors included a few cases
13
.-1 6
of livedoreticularis, acrocyanosis, and secondary Raynaud'sphenomenon.
lapse developed 6 years after cervicothoracicsympathectomy. This tendency to relapseafter initial improvement must be taken intoconsideration in evaluating the results of sym-
pathectomy for Raynaud's disease in the upper
extremities.Our data do not reveal any way by which
the results of sympathectomry in the upper
extremities can be predicted in advance, exceptthat good or excellent results were obtainedmore often when complications of Raynaud'sdisease were not present before operation. Thiswas also true in the series of Kinmonth andHadfield.Y' Our conclusion that good or excel-lent results were obtained more often whencomplications of Raynaud's disease were notpresent before operation is of little practicalimportance, however, since our companionstudy' has shown that most patients with un-
complicated Raynaud's disease get along well
on conservative management and surgicaltreatment is not usually indicated.The data presented herein do not permit us
to take sides in the controversy between theproponents of preganglionic sympathectomy7' 12and the proponents of postganglionic sympa-thectomy.10' 11 Three women in this series whofailed to obtain relief from resection of thethoracic trunk (preganglionic sympathectomy)subsequently received great benefit from cervi-cothoracic ganglionectomy (postganglionic).If these 3 cases are counted as failures fortrunk resection and as successes for ganglion-ectomy, good or excellent results were obtainedafter 50 per cent of the latter operations andafter 67 per cent of the former. The smallnumber of trunk resections performed doesnot make this difference significant. Haxton'and Kinmonth and Hadfield'3 also foundthat the two types of sympathectomy givesimilar results. Stellate ganglionectomy aloneseemed to yield good or excellent results asoften as when the second thoracic ganglionwas also removed. Felder and associates"found that the results of sympathectomy werebetter when the stellate ganglion was extir-pated. Recently Ray"5 has suggested that amore complete sympathectomy for the upperextremity might be achieved by removing thesympathetic chain from the middle cervicalganglion to the third thoracic ganglion inclu-sive. There is no evidence as yet that this pro-cedure gives better results than those obtainedby the less extensive operations employed forthis series.The incidence of long-term good results of
the surgical treatment of Raynaud's diseasepresented in this paper is not much greater thanthe incidence of long-term good results of con-servative treatment presented in the previousstudy.' The 2 groups of patients are not strictlycomparable, however, since patients with themore severe disease were more likely to bechosen for, and to accept, sympathectomy.This is ably demonstrated by the higher inci-dence of complications among the surgicallytreated group.The early age at death of 6 patients with
Raynaud's disease in this series is disturbingand raises the question of mistaken diagnoses or
1 1
by guest on May 25, 2018
http://circ.ahajournals.org/D
ownloaded from

GIFFORD, HINES, AND CRAIG
untoward sequelae of cervicothoracic sympa-thectomy. Since the causes of death of 3patients are not known and 64 of the 70 womenwere still alive at the time of last follow-up, noconclusions can be drawn as yet.
Secondary Raynaud's Phenomenon
In addition to the 70 women with Raynaud'sdisease, 54 women with Raynaud's phenomenonsecondary to other diseases were also subjectedto sympathectomy of the upper or lower ex-tremities or both prior to 1946. The diagnosesincluded acrosclerosis (37 patients), rheumatoidarthritis (5 patients), livedo reticularis or acro-cyanosis (5 patients), chronic occlusive arterialdisease (2 patients) and chronic pernio, periar-teritis nodosa, scalenus anticus syndrome, inde-terminate hemorrhagic diathesis, and indeter-minate disease of the central nervous system(1 patient each). Sympathectomy, althoughgiving better results in the lower than in theupper extremities, was successful much less fre-quently than in primary Raynaud's disease(table 7). The majority of the good or excellentresults were obtained in the patients withacrocyanosis, livedo reticularis, scalenus anticussyndrome, and chronic pernio. Sympathectomywas followed by major or minor amputationsin 6 patients in this group. Nineteen (35 percent) of the women with secondary Raynaud'sphenomenon were dead at the time of follow-up.The average age at death was 39 years.
Errors in the diagnosis of Raynaud's diseasewill lead to disappointing results from sympa-thectomy since Raynaud's phenomenon second-
TABLE 7.-Over-All Results of Sympathectomyfor Sec ndary Raynaud's Phenomena
Over-all results*
Excellent ...........
Good ...............
Fair ................Poor ................
Total .............
Patients having extremities denervated
Upper
2
7
4
3:3
46*
Lower
7
2
0
9
* Four patients required amputations of one or
more phalanges after sympathectomy and one patientrequired amputation of an arm.
t One patient required amputation of both legsafter lumbar sympathectomy.
ary to other diseases (notably acrosclerosis)usually responds poorly to sympathectomy.
SUMMARY
Sympathectomy for Raynaud's disease affect-ing the upper extremities gave good or excellentresults in 37 (54 per cent) of 68-women in thisseries. Good or excellent results were obtainedmore frequently if complications of Raynaud'sdisease (trophic lesions or sclerodactylia orboth) were not present before operation. Therewas no significant difference between the resultsobtained by preganglionic and postganglionicsympathectomies. Two (3 per cent) of the 68patients lost portions of fingers after sympa-thectomy. Of the patients who had a fair orpoor long-term result, the majority initiallyobtained a good result and then had relapsesduring the first 2 years after sympathectomy.Sympathectomy for the lower extremities
gave good or excellent results for 17 (94 percent) of 18 women with Raynaud's disease.Sympathectomy for Raynaud's phenomenonsecondary to other diseases gave poor resultsin the upper extremities in 72 per cent of casesand only slightly better results in the lowerextremities.Sympathectomy should be reserved for pa-
tients with the more severe and progressiveRaynaud's disease, since the prognosis is goodwithout sympathectomy when the disease ismild or moderately severe, and not progressing.
SUMMARIO IN INTERLINGUA
Sympathectomia in le tractamento de morbode Raynaud afficiente le extremitates superiorproduceva bon o excellente resultatos in 37 exle 68 feminas del presente serie (54 pro cento).Bon o excellente resultatos esseva obteniteplus frequentemente quando complicationesde morbo de Raynaud lesiones trophic osclerodactylia o ambes-non esseva presenteante le operation. Nulle significative differentiaesseva notate inter le resultatos obtenite persympathectomia preganglionic e le resultatosobtenite per sympathectomia postganglionic.Duo del 68 patientes (3 pro cento) perdivapartes de digito post sympathectomia. Quantoal patientes in qui le resultatos a longe vistaesseva solmente acceptabile o clarmente mal,
12
by guest on May 25, 2018
http://circ.ahajournals.org/D
ownloaded from

SYMPATHECTOMY FORItRAYNAU) S PHENO()MENON 13
le majoritate de illes comenciava per monstrarbon resultatos sed habeva recidivas durante leprime 2 annos post le sympathectomia.Sympathectomia pro morbo de Raynaud
in le extreinitates inferior produceva bon oexcellente resultatos in 17 ex 18 feminas (94pro cento).Sympathectomia pro phenomeno de Ray-
naud secundari a altere morbos produceva malresultatos in 72 pro cento del casos in que leextremitates superior esseva afficite e resultatosnon multo melior in le casos in que le extremi-tates inferior esseva afficite.Sympathectomia debe esser reservate pro
patientes con morbo de Raiynaud in formasever e progressive, proque le prrognose es bonsin sympathectomia quando le m( rbo es leve omoderatemente sever e non progredente.
REFERENCES1 GIFFORD, R. W., JR., AND HINES, E. A. JR.:
Raynaud's disease among women and gi; ls.Circulation 16: 1012, 1957.
2 ALLEN, E. V., AND BROWN, G. E.: Raynaud'sdisease: A critical review of minimal requisitesfor diagnosis. Am. J. M. Sc. 183: 187, 1932.
3- AND : Raynaud's disease affecting men.Ann. Int. Med. 5: 1384, 1932.
4ADSON, A. W.: Changes in technique of cervico-thoracic ganglionectomy and trunk resection.Am. J. Surg. n.s. 23: 287, 1934.
5SMITHWICK, R. H.: Modified dorsal sympathec-tomy for vascular spasm (Raynaud's disease)
of the upper extremity: A preliminary ieport.Ann. Surg. 1Oi: 339, 1936.
6 TELFORD, E. D.: The technique of sympathec-to.-ny. Brit. J. SUrg. 23: 448, 1'335.7 Discussion on peripheral vascular lesions.
Proc. Roy. Soc. Med. 37: 621, 1944.8 HAXTON, H. A.: Regeneration after sympathec-
tomy and its effects on Raynaud's disease.Brit. J. Surg. 35: 69, 1947.
9 BARCROFT, H., AND HAMILTON, G. T. C.: Resultsof sympathectomy of the upper limb: XWithspecial reference to Raynaud's disease. Lancet1: 441, 1948.
10 FELDER, D. A., SIMEONE, F. A., LINTON, R. R.,AND WELCH, C. E.: Evaluation of sympatheticneurectomy in Raynaud's disease: Based on afollow-up study of forty patients. Surgery 25:1014, 1949.
11 BLAIN, A., III, COLLER, F. A., AND CARVER, G.B.: Raynaud's disease: A study of criteria forprognosis. Surgery 29: 387, 1951.
12 ROBERTSON, C. XW., AND SMITHWICK, R. H.:The recurrence of vasoconstrictor activity afterlimb sympathectomy in Raynaud's diseaseand allied vasomotor states. New England J.Med. 245: 317, 1951.
13 KINMONTH, J. B., AND HADFIELD, G. .J.: Sym-pathectomy for Raynaud's disease: Resultsof ganglionectomy and preganglionic sectioncompared. Brit. M. J. 1: 1377, 1952.
14 HINES, E. A., JR., AND CHRISTENSEN, N. A.:Raynaud's disease among men. ,J. A. M. A.129: 1, 1945.
15 RAY, B. S.: Sympathectomy of upper extremity;evaluation of surgical methods. ,J. Neurosurg.10: 624, 1953.
But these sufferinc,s are not at all necessary; they are the effects of our inexperience, and would insimilar circumstances, more or less attend the exhibition of almost every active and powerfulmedicine we use.-WILLIAM WITHERING. An Account of the Foxglove, and Somle of Its MedicalUses. Birmingham, 1785.
13
by guest on May 25, 2018
http://circ.ahajournals.org/D
ownloaded from

RAY W. GIFFORD, JR., EDGAR A. HINES, JR. and WINCHELL MCK. CRAIGPhenomenon
with Raynaud's Disease and 54 Women with Secondary Raynaud's Sympathectomy for Raynaud's Phenomenon: Follow-Up Study of 70 Women
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1958 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.17.1.51958;17:5-13Circulation.
http://circ.ahajournals.org/content/17/1/5located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on May 25, 2018
http://circ.ahajournals.org/D
ownloaded from