Spinal Cord Syndromes-An Overveiw
34
Spinal Cord Syndromes Dr.W.A.P.R.S. Weerarathna Registrar-Ward 10/02 THJ
-
Upload
suneth-weerarathna -
Category
Health & Medicine
-
view
305 -
download
6
Transcript of Spinal Cord Syndromes-An Overveiw
Spinal Cord Syndromes
Dr.W.A.P.R.S. Weerarathna
Registrar-Ward 10/02
THJ
Objectives…
• Basic spinal cord Anatomy
• Types of spinal cord lesions
• Main spinal cord syndromes-Eight!
• Common clinical presentation
• Basic Neuroimaging-MRI/CT appearances
• Other spinal cord lesions
• Summary
Spinal cord Anatomy31 pairs of spinal cord segments,45 cm
Ventral-motor & Dorsal-sensory functions
Combined –mixed spinal nerves neuroforamina
Foramen magnum lower margin of L1
Vert. & SC segments –not nessasarily the same( SC is shorter than the vert.)
Blood supp-1 ant.spinal artery& 2 post.spinalarteries (vertebral)
Ant.2/3 & dorsal columns respectively.


Spinal cord lesions• Intra medullary vs extramedullary lesions
• Complete vs incomplete lesions
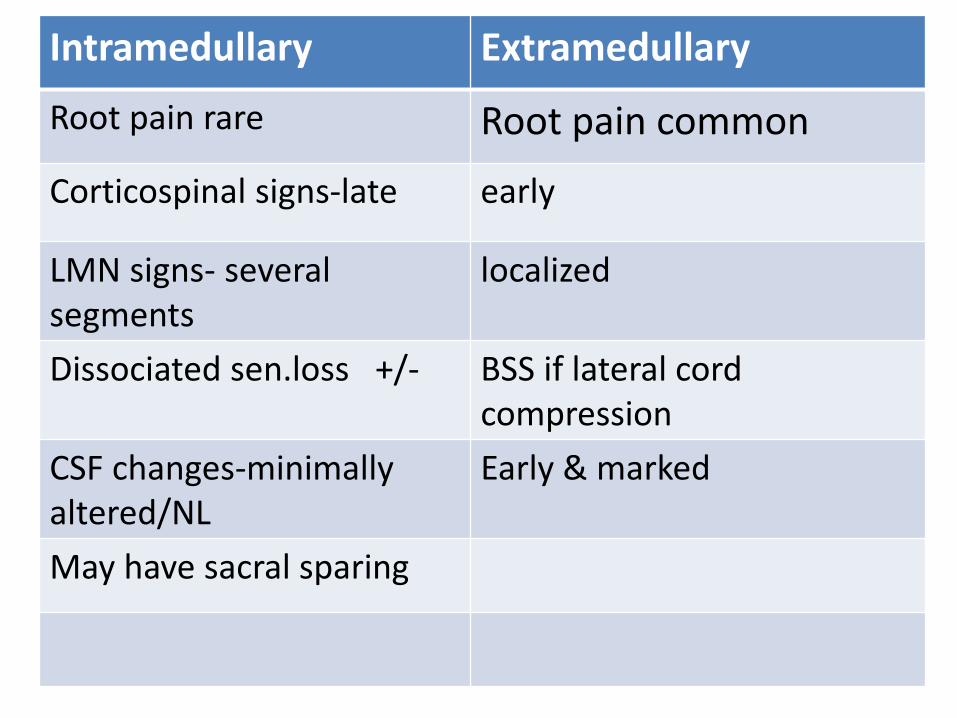
Intramedullary Extramedullary
Root pain rare Root pain common
Corticospinal signs-late early
LMN signs- several segments
localized
Dissociated sen.loss +/- BSS if lateral cord compression
CSF changes-minimally altered/NL
Early & marked
May have sacral sparing
• Incomplete:– Sensory, motor or both functions are partially
present below the neurologic level of injury
– Some degree of recovery
• Complete:
– Absence of sensory and motor function below the level of injury
– Loss of function to lowest sacral segment
– Minimal chance of functional motor recovery
Important SC syndromes (8)
1) Complete cord transection syndrome
2) Brown-Sequard syndrome
3) Central cord syndrome (syringomyelia)
4) Posterior column syndrome (tabes dorsalis)
5) Posterolateral cord syndrome (SACDC)
6) Combined AHC-pyramidal tract syndrome (ALS)
7) AHC syndrome
8) Anterior spinal artery artery occlusion
Others important condisions
• Conus medullaris syndrome(L2)
• Cauda equina syndrome is not a SC syndrome!(represent spinal roots, rather than SC.)-usually lesions below L2 level.
• Friedreich’s ataxia-spino cerebellardegeneration.

• 1-complete cord transection•
• Causes- trauma, h’age,epiduralabscess,metastasis,MS ,post vaccinial syn.ect
• Results in
1. Spinal shock
2. Spastic paralysis(hypertonic,hyperfeflexic)
3. Loss of all sensory modalities bilaterally
4. Autonomic disturbances
• Spinal shock-
1. Complete loss of voluntary movements, sensations below the level of lesion
2. Loss of all reflexes in isolated cord segments
3.Duratin varies-1-6 weeks commonly
• Spastic paralysis
1. Follows the period of spinal shock
2. Initially positive Babinski sign ,later-increased tone & deep tendon reflexes
3. Disuse muscle atrophy
• Loss of superficial reflexes(abdominal, cremasteric) below the level
• Loss of all sensations bilaterally below the lesion
1. Loss of propioception, vibration,tactilediscrimination, pain,temp, light touch, viseralsensibility
2. Complete lesion-no recovery
• Autonomic disturbances
1. Bowel/bladder dysfunction-urinary retention/constipation
2. Initial retention due to loss of vol.control
3. Flaccid neuropathic bladder with overflow incontinence with recovery……
• Spastic neuropathic bladder with autonomic bladder
5.few-’’ mass reflex’’ bowel/bladder empty on a segmental autonomic basis reflexly.
6. Vasomotor instability-Cutaneous BV below do not respond to cold/hot stimuli
7.Anhydrosis-Honer’s syndrome may occur in some.
8.Sexual dysfunction
• Transection of SC above C5- not survive due to involvement of phrenic nerve nuclei-res.paralysis
• Below C5-quadriplagic/between Cx & L-S segments-paraplagic.

• 2. BSS
• Motor changes-
1. UMN signs below the hemisection on I/L side
2. LMN signs at the level on I/L side
• Sensory changes-
1. Pain/temp loss on C/L side –upper level of sen. Loss is few segments below the leasion.(?)
2. Vib. & propi, loss on I/L side
3. There may be band of sensory loss on the I/L side at level of the leasion.
• Causes-
1. MS
2. Angioma
3. Glioma
4. Trauma
5. Myelitis
6. Post radiation myelopathy
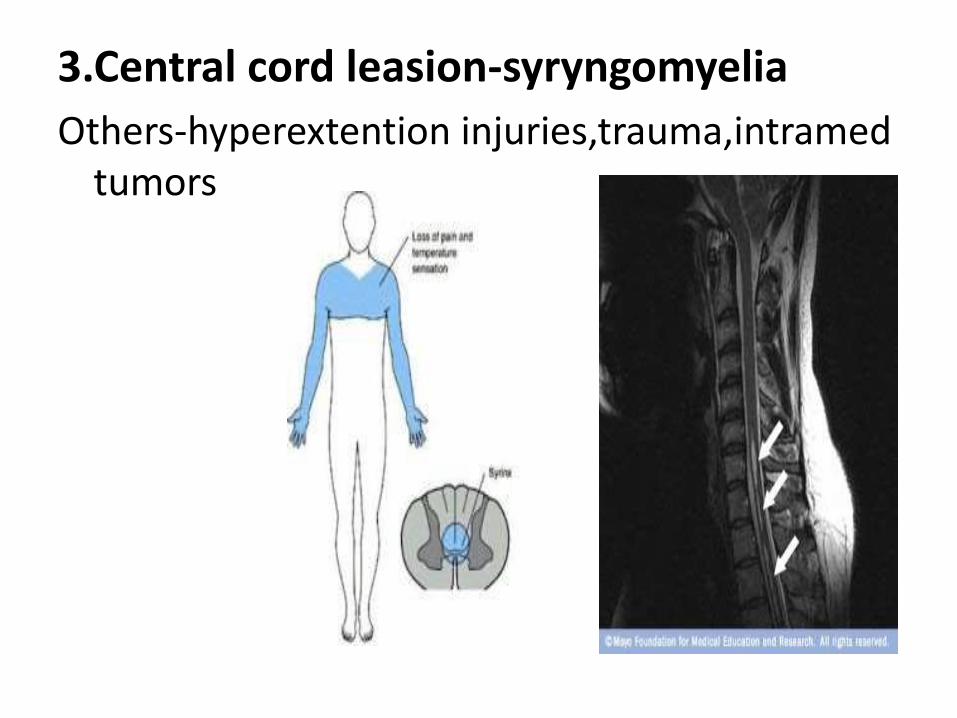
3.Central cord leasion-syryngomyelia
Others-hyperextention injuries,trauma,intramedtumors
• Expanding central canal in the SC –more in Cervical cord,symetrical leasions
• STTsalways affected- fibers cross through syrinx
• CSTs spares until syrinx very large
• DCs always spared
• nerve roots at sequential levels affected
• Clinical triod-
1. Loss of pain/temp. over neck, shoulders & arms-’’cape distribution’’
2. Amyotrophy-weakness,atrophy ,areflexia of hands/arms
• 3.UMNL in lower limbs
• Other features horner’s syndrome(syrinxaffecting sym. Nerves & C8/T1
• Charcot’s joints-long standing ,loss of pain sensation
• Associated kypphoscoliosis.
• Syringobulbia syrinx in brain stem/extention-facial dissociated sensory loss,bulbar palsy,nystagmus & cebellar ataxia
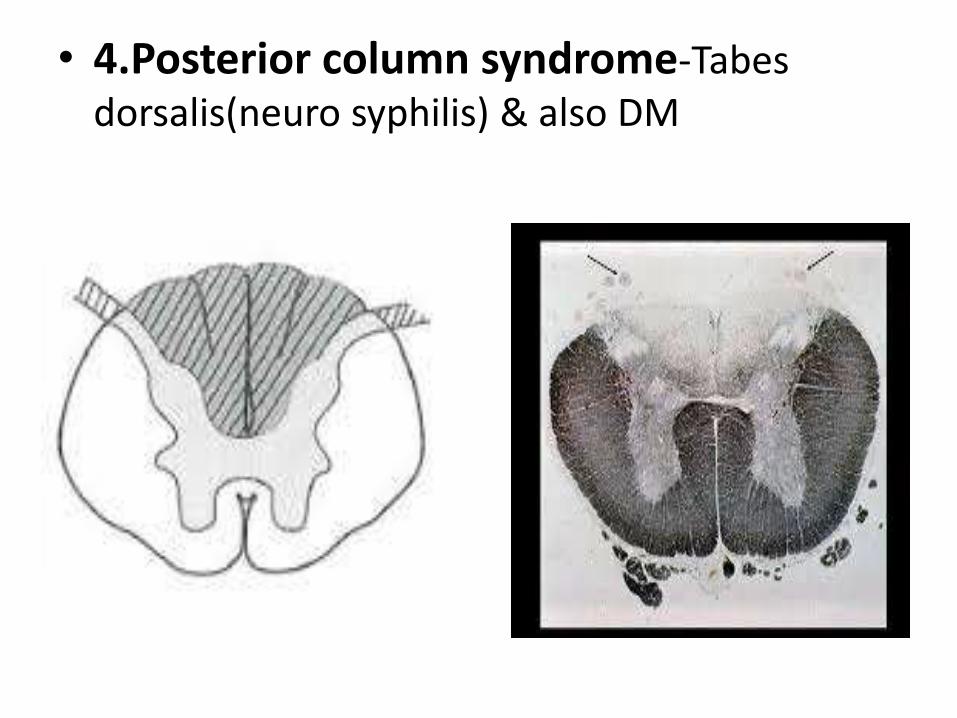
• 4.Posterior column syndrome-Tabesdorsalis(neuro syphilis) & also DM
• CNS infection of syphilis after 3-18 years
• DCs & dorsal roots degenerate
• DCs loss of vibration & propioception ,+veRomberg’s sign(&+ve Hermitte’s sign)
• CSTs not affected. if involved =‘’TABUPARESIS’’
• STTs spared.
• Others neuropathic joint destruction <10% (charcot’s joints) trophic ulcers,
• Argyll Robertson pupils 90% (ARP),optic atrophy(rare),opthalmolagia.
• Autonomic degeneration-neuropathic bladder(incontinance),constipation
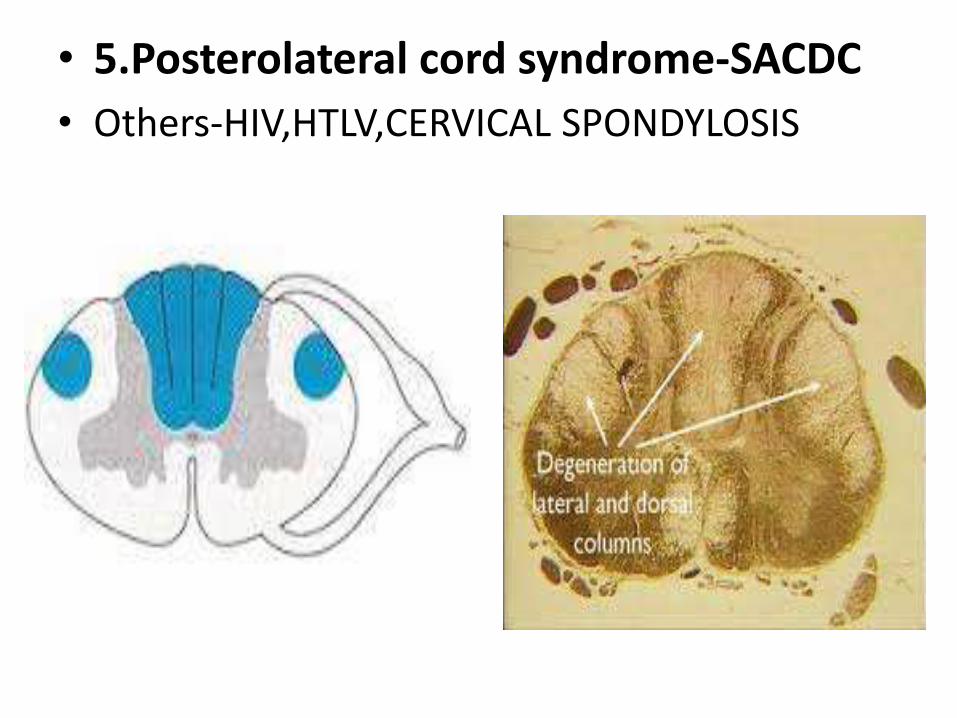
• 5.Posterolateral cord syndrome-SACDC
• Others-HIV,HTLV,CERVICAL SPONDYLOSIS
• Due to Vit.B12 deficiency
• DCs symmetrically degenarate,loss of vibration & propioception over feet,+veRhomberg’s sign, Ataxic gait
• CSTs symetrical UMN signs in LLs(spastic paraparesis),extensor planters, absent AJ, possible brisk KJ
• STTs spared or involved as part of PN(less common & mild)
• Others optic atrophy with centrocecalscotomata,dementia,autoimmunedisease(pernicious anemia)

• Causes of extesor planters &absent KJ
• D- DM(uncommon)
• M-MND,metachromatic leucodystrophy
• A- Adrenoleucodystrophy
• S- SACDC,SYPHILIS
• T-Tabuparesis
• Cauda equina syndrome
• 6.Combined AHC –pyramida tract syndrome-(ALS)
• typical form of MND, AD inheritance, mutation in SOD1
• Mixed UMN & LMN degeneration with cerebral motor pathways & brain stem nuclei
• Muscle wasting or weakness with preserved or brisk reflexes, sphincter involvement is very late if at all.
• Progressive bulbar involvement(20%) sialorrhoea, dysarthria,dysphagia
• Cognition generally spared, 15% FTD
• Sensory-NOT affected, superficial reflexes-preserved
• ANS-intact
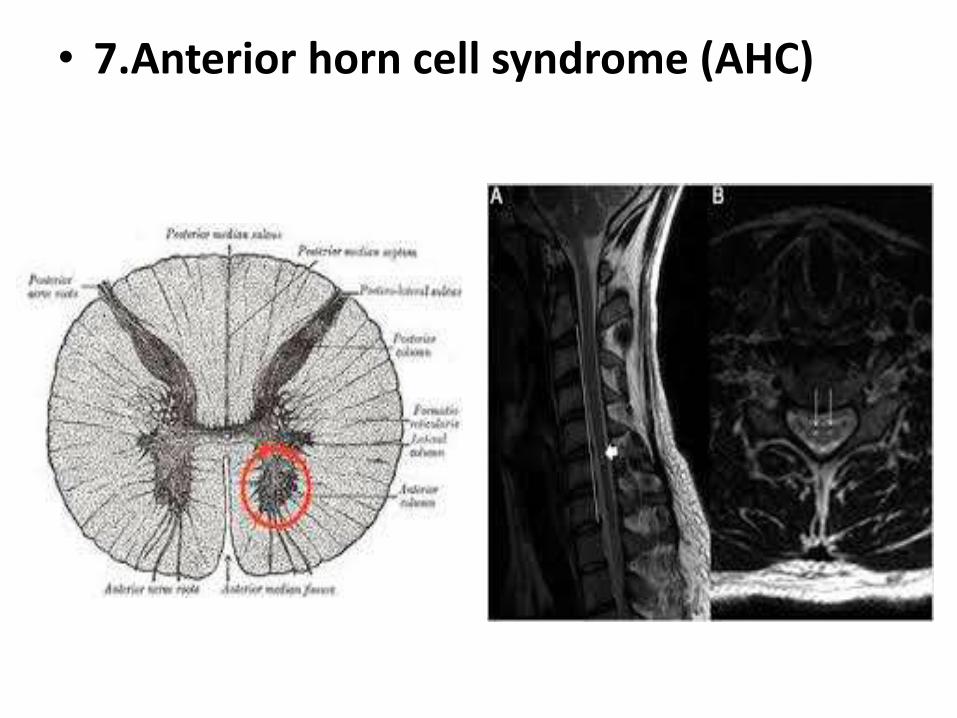
• 7.Anterior horn cell syndrome (AHC)
• CAUSED BY SPINAL MUSCULAR ATROPHY.
• MOTOR
• weakness ,atrophy and fasciculations.
• Hypotonia, depressed reflexes.
• Muscles of trunk and extremities are affected.
• Sensory system is not affected.
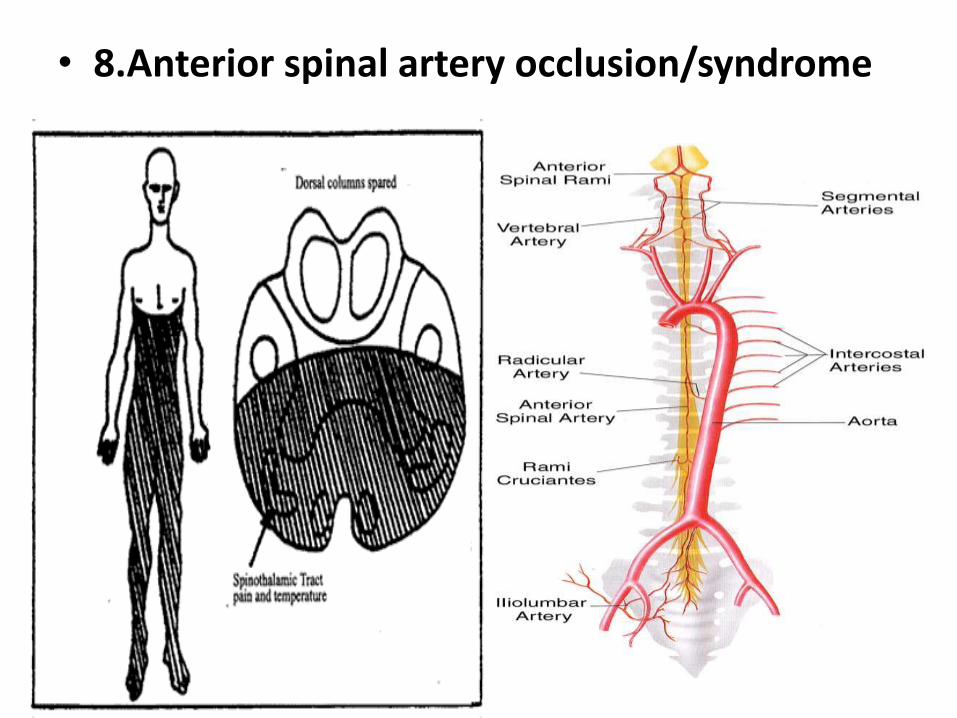
• 8.Anterior spinal artery occlusion/syndrome

• MOTOR-Flaccid and areflexic paraplegia• SENSORY-• Loss of pain and temperature.• Preservation of position and vibration.• AUTONOMIC-• urinary incontinence.• Spinal cord infarction usually occurs in T1 to
T4 segment. and L1 • Occurs due to syphilitic arteritis ,aortic
dissection, atherosclerosis of aorta, SLE & AIDS,AVM
• Posterior spinal artery occlusion/syndrome-
• Uncommon.
• Loss of proprioception and vibratory sense.
• Pain and temperature is preserved.
• Absence of motor deficit.