THE SYNDROMES OF THE ARTERIES OF THE BRAIN AND, SPINAL …
10
I19 - N/ THE SYNDROMES OF THE ARTERIES OF THE BRAIN AND, SPINAL CORD Part II By LESLIE G. KILOH, M.D., M.R.C.P., D.P.M. First Assistant in the Joint Department of Psychological Medicine, Royal Victoria Infirmary and University of Durham The Vertebral Artery Each vertebral artery enters the foramen magnum in front of the roots of the hypoglossal nerve, inclines forwards and medially to the anterior aspect of the medulla oblongata and unites with its fellow at the lower border of the pons to form the basilar artery. The posterior inferior cerebellar and the anterior spinal arteries are its principal branches and it sometimes gives off the posterior spinal artery. A few small branches are supplied directly to the medulla oblongata. These are in line below with similar branches of the anterior spinal artery and above with the paramedian branches of the basilar artery. In some cases of apparently typical throm- bosis of the posterior inferior cerebellar artery, post-mortem examination has demonstrated oc- clusion of the entire vertebral artery (e.g., Diggle and Stcpford, 1935). In some of these the thrombus has extended from the posterior inferior cerebellar artery just before death but in others there is no doubt that it was the primary condition. In these it is usual to find that the basilar artery has commenced early in the region of the inferior olive and supplies the median area of the medulla oblongata normally irrigated by the vertebral and ,anterior spinal arteries. The usual result of vertebral artery thrombosis is simply a combination of those features which result from occlusion of the posterior inferior cerebellar artery and of the medullary portion of the anterior spinal artery with all their variations (q.v.). Several eponyrns have been attached to the syndrome of the vertebral artery. The common picture is sometimes known as the Babinski- Nageotte syndrome. The syndrome of Cestan- Chenais is similar but weakness of the tongue and involvement of the descending root of the fifth nerve and of the spinothalamic tract are absent. (See also Cabot, I937; Pines and Gilensky, 1930.) The Posterior Inferior Cerebellar Artery The posterior inferior cerebellar artery arises from the vertebral artery at the level of the lower border of the inferior olive and winds round the medulla oblongata between the roots of the hypo- glossal nerve. It passes rostrally behind the root- lets of the vagus and glossopharyngeal nerves to the lower border of the pons, bends backwards and caudally along the inferolateral boundary of the fourth ventricle and finally turns laterally into the vallecula. Branches: From the trunk of the artery, twigs enter the lateral aspect of the medulla oblongata and supply the region bounded ventrally by the inferior olive and medially by the hypo- glossal nucleus-including the nucleus ambiguus, the spinothalamic tract and the restiform body. A branch passes to the chorioid plexus of the fourth ventricle, and in the majority of individuals it also gives off the posterior spinal artery. A twig to the dentate nucleus is present in many individuals (Shellshear, I922). The medial terminal branch ramifies over the vermis; the lateral terminal branch supplies the lower surface of the cerebellar hemisphere. Occlusion of the posterior inferior cerebellar artery gives rise to the lateral medullary or Wallenberg's syndrome. Although credit for the earliest descriptions is usually given to Senator (I883) and Wallenberg (i895), a remarkably de- tailed and personal account by Gaspard Vieusseux, the Swiss physician, was published by Marcet in I8I7. The clinical picture of posterior inferior cere- bellar artery thrombosis shows much variation, though the main features are reasonably constant and diagnostic. copyright. on April 27, 2022 by guest. Protected by http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.29.329.119 on 1 March 1953. Downloaded from
Transcript of THE SYNDROMES OF THE ARTERIES OF THE BRAIN AND, SPINAL …

I19
- N/
THE SYNDROMES OF THE ARTERIESOF THE BRAIN AND, SPINAL CORD
Part II
By LESLIE G. KILOH, M.D., M.R.C.P., D.P.M.First Assistant in the Joint Department of Psychological Medicine, Royal Victoria Infirmary and University of Durham
The Vertebral ArteryEach vertebral artery enters the foramen
magnum in front of the roots of the hypoglossalnerve, inclines forwards and medially to theanterior aspect of the medulla oblongata and uniteswith its fellow at the lower border of the pons toform the basilar artery.The posterior inferior cerebellar and the
anterior spinal arteries are its principal branchesand it sometimes gives off the posterior spinalartery. A few small branches are supplied directlyto the medulla oblongata. These are in line belowwith similar branches of the anterior spinal arteryand above with the paramedian branches of thebasilar artery.
In some cases of apparently typical throm-bosis of the posterior inferior cerebellar artery,post-mortem examination has demonstrated oc-clusion of the entire vertebral artery (e.g., Diggleand Stcpford, 1935). In some of these thethrombus has extended from the posterior inferiorcerebellar artery just before death but in othersthere is no doubt that it was the primary condition.In these it is usual to find that the basilar arteryhas commenced early in the region of the inferiorolive and supplies the median area of the medullaoblongata normally irrigated by the vertebral and,anterior spinal arteries.The usual result of vertebral artery thrombosis
is simply a combination of those features whichresult from occlusion of the posterior inferiorcerebellar artery and of the medullary portion ofthe anterior spinal artery with all their variations(q.v.).
Several eponyrns have been attached to thesyndrome of the vertebral artery. The commonpicture is sometimes known as the Babinski-Nageotte syndrome. The syndrome of Cestan-Chenais is similar but weakness of the tongue andinvolvement of the descending root of the fifthnerve and of the spinothalamic tract are absent.
(See also Cabot, I937; Pines and Gilensky,1930.)
The Posterior Inferior Cerebellar ArteryThe posterior inferior cerebellar artery arises
from the vertebral artery at the level of the lowerborder of the inferior olive and winds round themedulla oblongata between the roots of the hypo-glossal nerve. It passes rostrally behind the root-lets of the vagus and glossopharyngeal nerves tothe lower border of the pons, bends backwards andcaudally along the inferolateral boundary of thefourth ventricle and finally turns laterally into thevallecula.
Branches: From the trunk of the artery,twigs enter the lateral aspect of the medullaoblongata and supply the region bounded ventrallyby the inferior olive and medially by the hypo-glossal nucleus-including the nucleus ambiguus,the spinothalamic tract and the restiform body. Abranch passes to the chorioid plexus of the fourthventricle, and in the majority of individuals it alsogives off the posterior spinal artery. A twig to thedentate nucleus is present in many individuals(Shellshear, I922).The medial terminal branch ramifies over the
vermis; the lateral terminal branch supplies thelower surface of the cerebellar hemisphere.
Occlusion of the posterior inferior cerebellarartery gives rise to the lateral medullary orWallenberg's syndrome. Although credit for theearliest descriptions is usually given to Senator(I883) and Wallenberg (i895), a remarkably de-tailed and personal account by Gaspard Vieusseux,the Swiss physician, was published by Marcet inI8I7.The clinical picture of posterior inferior cere-
bellar artery thrombosis shows much variation,though the main features are reasonably constantand diagnostic.
copyright. on A
pril 27, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.329.119 on 1 M
arch 1953. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL March 1953
The onset in a typical case is with intensevertigo, the patient's head and eyes turning to theside of the lesion. He may stagger to the same sideand may fall. Nausea and vomiting are almost in-variable and the latter may be intractable. Loss ofconsciousness though not to be expected has beenrecorded occasionally, as in two of Merritt andFinland's cases (I93o). Dysphagia is constant andmay even preclude the swallowing of saliva so thata hawking cough develops. Regurgitation offluids through the nose sometimes occurs althoughthe palatal palsy is strictly unilateral. Speech iscommonly affected and in different patients alldegrees from hoarseness to aphonia may occur.Less frequently, complaint is made of ipsilateraltinnitus or deafness and diplopia is sometimestroublesome. Hiccough is not infrequent and maypersist for days.
Generalized headache or suboccipital pain at thetime of onset of the ictus is frequent, but moreinteresting is the occurrence of facial pain on thesame side as the lesion. Rarely is pain in thethroat in the distribution of the glossopharyngealnerve experienced. Complaint is often made ofnumbness, coldness or of pins and needles over theipsilateral face and the contralateral body half.An ipsilateral Horner's syndrome is present in
at least 8o per cent. of cases but is frequentlyincomplete, anhidrosis occurring less commonlythan ptosis and miosis. It is due to interruption ofthe sympathetic connector fibres running from thehypothalamus to the cells of the lateral horn of thegrey matter of the cord.Some weakness of the ipsilateral masticatory and
facial muscles may be seen. There may also beloss of taste on the same side over the anterior two-thirds of the tongue. Involvement of the ipsi-lateral sixth nerve is fairly common giving rise todiplopia, but is often so slight that it is difficult todemonstrate clinically. Severe degrees of in-volvement of the sixth and seventh cranial nervesprobably indicate either that the posterior inferiorcerebellar artery supplies an unusually wideterritory or that short circumferential branches ofthe basilar artery have been affected coincidentally.
Infarction of the ipsilateral nucleus ambiguusand of its emerging nerve fibres is responsible forthe dysphagia, dysarthia and palatal weaknesswhich have already been mentioned. The ipsi-lateral pharyngeal weakness betrays itself by a' curtaining' effect of the posterior pharyngealwall on attempted swallowing and like the ipsi-lateral palatal weakness is usually severe. Theparalysis of the ipsilateral vocal cord may be lessmarked. The tongue is never affected.
Ipsilateral cerebellar ataxia is present- in thegreat majority of patients. It results mainly fromdamage to the inferior cerebellar peduncle. Less
commonly-because of its rich collateral circula-tion-the cerebellum is infarcted and this con-tributes to the dyssynergia. Nystagmus is usuallygross and there may be skew deviation of the eyes;these features are largely attributable to thevestibular disturbance.The typical sensory changes found are impair-
ment of pain and temperature sensations in thedistribution of the ipsilateral fifth nerve and similarimpairment over the contralateral body half fromthe second cervical segment downwards. Touch,the sense of passive movement and vibration senseare unaffected. The facial changes are due toischaemia of the descending tract of the fifth nervewhich, together with the spinal nucleus of thefifth nerve, underlies the tuberculum cinereum.(The upper part of the spinal nucleus of the fifthnerve is also affected but in the average case thelesion of the tract takes precedence.) The contra-lateral loss of pain and temperature sensations inthe trunk and limbs is due to interruption of thespinothalamic tract which at this level lies internalto the descending tract and nucleus of the fifthnerve. The opposite side of the face is rarelyaffected because the quintothalamic tract whicharises from the spinal nucleus of the fifth nervepursues a separate path in the medulla oblongataclose to the medial lemniscus and does not join thespinothalamic tract until it reaches the pons(Smyth, 1939). Trophic changes, including gan-grene of the side of the nose and adjoining cheekhave been reported, usually associated with the useof a nasal catheter (Savitsky and Elpern, 1948).Many interesting variants have been noted with
regard to the nature and area of the sensory loss.Sometimes the ipsilateral face is not involved andin others only the territory of the first or first andsecond divisions of the fifth nerve is affected. Inthe latter the upper parts of the descending tractand spinal nucleus of the fifth nerve escapedamage; this provides supporting evidence for the'upside down' arrangement of this nucleus.Rarely does ipsilateral impairment of tactilesensation accompany the loss of pain and tempera-ture sensations.
Occasionally the loss of facial sensation isbilateral, the crossed quintothalamic tract beingaffected as well as the ipsilateral descending root ofthe fifth nerve. Cases have been noted (Sheehanand Smyth, I937) in which such contralateral im-pairment of facial sensation has been restricted tothe area supplied by the ophthalamic division ofthe fifth nerve. This finding suggests that thequintothalamic tract is laminated, the fibres de-rived from the upper face (i.e., from the lowestpart of the spinal nucleus) lying on the outside.
Sometimes, owing to the similar lamination ofthe spinothalamic tract, the contralateral sensory
copyright. on A
pril 27, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.329.119 on 1 M
arch 1953. Dow
nloaded from

lAfarch 1953 KILOH: The Syndromes of the Arteries of the Brain'and Spinal Cord 121
loss spares the areas supplied by the cervical andeven the thoracic segments. The sacral, lumbar,thoracic and cervical fibres lie in this order fromwithout inwards and if the area of infarction doesnot extend sufficiently far medially, the cervical-and perhaps the thoracic-fibres will escapedamage.The prognosis following occlusion of the pos-
terior inferior cerebellar artery is surprisingly good.The dysphagia, dysarthria and vestibular symp-toms commonly disappear and the ataxia shows amarked improvement. The Horner's syndromeand the sensory loss usually persist but occasionlittle disability.
(See also Anderson et al., I93i; Goodhart andDavison, 1936; Spillane, I937).The Anterior Spinal Artery
Each anterior spinal artery arises near the ter-mination of the vertebral artery and runs obliquelydownwards and medially to the anterior aspect ofthe medulla oblongata, uniting with its fellowopposite the decussation of the pyramids. Thecombined artery runs downwards in the antero-median fissure reinforced at-intervals by twigs fromthe vertebral, posterior intercostal and lumbararteries. Sometimes the two vessels join at oncebut in other cases they remain independent forseveral centimetres. Occasionally one is absent.Twigs from each artery enter the bulb in line
with the paramedian branches of the basilar arteryand supply the anterior and medial portions of themedulla oblongata, including the pyramidal tractand the medial lemniscus. Stopford (I916, 1917)showed that these vessels also supply the hypo-glossal triangle.
Spiller (I908) was the first to describe occlusionof the anterior spinal artery above the level of thedecussation of the pyramids. The changes whichresult constitute the syndrome of the anteriorspinal artery of the medulla (paramedian inferiorbulbar syndrome).Double incontinence is frequent at the onset but
loss of consciousness is unusual. Contralateralparaesthesiae may be experienced. The mostobvious feature is a contralateral hemiplegiaaffecting the limbs equally but sparing the face.Some contralateral impairment of the sense ofpassive movement and of vibration sense withastereognosis is usual and is occasionally associatedwith hyperpathia. Nystagmus is often seen. Anipsilateral 12th nerve paralysis when present ishighly characteristic. In its absence, confusionwith a lesion of the internal capsule is likely butthe escape of the face and the presence of nystag-mus will aid distinction.
Ifthe two anterior spinal arteries form a commontrunk at a higher level than usual or if one of the
.contributory arteries is absent, then thrombosisgives rise to a quadriplegia with sensory loss(Louis-Bar, I947). The resulting picture re-sembles that of basilar artery occlusion but will bedistinguished by the absence of ' pseudobulbar'signs.
(See also Davison, I937, I944; O'Brien andBender, I945).Thrombosis of the inframedullary portion of the
anterior spinal artery was first described byPreobrajensky (1907).Thrombosis may occur anywhere in the course
of the vessel but is most frequent in the cervicalregion. As it runs downwards the anterior spinalartery gives off paired anterior sulcal brancheswhich penetrate the substance of the cord andsupply the entire grey matter-with the exceptionof the tips of the posterior horns-and the greaterpart of the lateral and anterior funiculi. Thesupply of these from the posterior spinal arteries isfrugal. The latter vessels supply mainly theposterior columns and the tips of the posteriorhorns of the grey matter. The anterior sulcalarteries are strictly unilateral in their distribution(Herren and Alexander, 1939).
Pain is common at the onset and is experiencedeither in girdle distribution at the level of thelesion or radiating down the legs. Incontinence-or less commonly retention-of urine and faecesoccurs and is sometimes accompanied by priapism.If the artery is occluded in the cervical regionthere is weakness of all four limbs, initially withflaccidity. In the upper limbs the weakness islargely 'lower motor neurone' in character andis due to segmental destruction of anterior horncells. Flaccidity will therefore persist and in timewasting will appear. In the lower limbs the weak-ness is. 'upper motor neurone' in type andspasticity usually supervenes. The weakness iscommonly asymmetrical. Absence of some or allof the deep reflexes in the upper limbs is associatedwith the lower motor neurone lesion. The deepreflexes in the lower limbs are often absent in theflaccid stage but become exaggerated if the patientsurvives. Occlusion in the lumbar region of thecord results in a flaccid weakness of the lowerlimbs with wasting and loss of deep reflexes.
Sensory loss of a dissociated type is present butis variable in extent. Commonly it affects allsegments below the level of the lesion but is oftennot absolute and may be less marked on one side.Sometimes it is possible to define a zone of absoluteloss of pain and temperature sensations in the lowercervical and upper thoracic regions due to destruc-tion of the crossing fibres in the neighbourhood ofthe central canal, while below this level the sensoryloss is incomplete as the spinothalamic tracts re-
copyright. on A
pril 27, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.329.119 on 1 M
arch 1953. Dow
nloaded from

122 POSTGRADUATE MEDICAL JOURNAL March 1953·; ·- .-c.* ·. '.·
,..;.. ,.,1. 3.i
..
B
d;.--·u;
::
·I;·u*.. ;9
i·:
;1 f
'' h·· .e.ll..T· .-I·'·IYLU.I / /Y ·.III':
'· · .·1.· '.;.3.1UT.:· r·I'...I.Y .I;· \..Y'Pli.
r'i
II i·:i·-
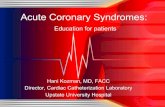
FIG. 4.-The arterial supply of the brain stem andcerebellum (semi-diagramatic).a Posterior cerebral artery.b Superior cerebellar artery.c Basilar artery.d Short circumferential branches of pons.e Anterior spinal artery.f Vertebral artery.g Middle cerebellar artery.
h Posterior inferior cerebellar artery.i Posterior communicating artery.j Internal carotid artery.k Trigeminal nerve.1 Oculomotor nerve.m Pons.n Lateral artery of medulla oblongata.(Foix and Hillemand, 1925b.)
ceive some blood from the posterior spinalarteries.The occurrence of a bilateral Horner's syn-
drome might be anticipated whenever the lesion isabove the level of the first thoracic segment.Curiously enough this appears to have been re-corded onc:e only--by Pariser and Lasagna (1949).It may well be more common than this, for itspresence nmay be difficult to establish, especially inill and perhaps dying patients.The asymmetry of the condition is sometimes
so marked as to merit the title of a Brown-Sequardsyndrome (lacking, of course, evidence of ipsi-lateral posterior column involvement). This mayoccur duriing the stage of recovery and whenpresent, suggests that the thrombosis has affectedmainly one. of the anterior sulcal branches.
In some cases a considerable degree of im-provement may take place. More commonly theparalysis remains severe, bed sores andc urinaryinfection develop and the patient suffers the usualfate of any severe chronic spinal affection.
(See also Adams and Merrit, '944; Steegman,1952; Sherman, 1948; Zeitlein and Lichtenstein,1936).
The Basilar ArteryThe basilar artery is formed at the lower border
of the pons by the junction of the vertebralarteries. It occupies the basilar groove and endsby dividing into the two posterior cerebralarteries. Its other branches are classified by Foixand Hillemand (1926) into:
(a) Paramedian group (q.v.).(b) Short circumferential branches (q.v.).(c) Long circumferential branches: (i) Anterior
inferior cerebellar artery (q.v.). (ii) Superiorcerebellar artery (q.v.).The clinical picture resulting from occlusion of
the basilar artery varies widely, as might be ex-pected, according to the precise site and extent ofthe thrombus. It depends too on the size of theposterior communicating arteries. If these areunobstructed and of such a size as to provide anadequate collateral circulation, only the territoryof those branches blocked by the thrombus willbe affected.At the onset headache may occur and is usually
occipital in distribution. ' Dizziness' and, lesscommonly, true vertigo are frequent complaints.Impairment of consciousness varying from slight
copyright. on A
pril 27, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.329.119 on 1 M
arch 1953. Dow
nloaded from

March 195 3 KILOH: The Syndromes of the Arteries of the Brain and Spinal Cod [23
II
.e
FIG. 5.--The arterial supply of the brain stem andcerebellum-lateral aspect (semi-diagramatic). Keyas for Fig. 4. (Foix and Hillemand, I925b.)
clouding to deep coma is usual. Estimation of thedegree of impairment of consciousness may bedifficult if the double hemiplegia is so profound asto render impossible any response on the part ofthe patient. One of Biemond's cases (I95I) witha complete anarthria and quadriplegia could moveonly his eyes to indicate his awareness of the ex-ternal world. The explanation of the loss of con-sciousness which occurs so commonly is notaltogether clear, for in most of these cases post-mortem studies have failed to demonstrate anylesion outside the midbrain and pons. Bremer(x935), from animal experiments, concluded thatconsciousness ceases when the cerebrum is de-prived of afferent stimuli, as would occur in severemidbrain or upper pontine lesions. This view wasrecently reiterated by Purdon Martin (i949). Onthe other hand the work of Magoun's school(Lindsley, et al., 1950) suggests that damage to theascending reticular activating substance is primarilyresponsible for the alteration in the state of con-sciousness and Jefferson (1952) has emphasizedthis possibility in regard to brain stem lesions inman.
Urinary and faecal incontinence is almost in-variable even though consciousness be retained.Numbness or tingling down one or other side ofthe body is common and is most marked in thelips, hands and feet.
Dysarthria, amounting at times to anarthria,occurs in most cases and is due to bilateral in-terruption of the corticobulbar tracts. Other'pseudobulbar ' phenomena are equally prominentwhen consciousness is retained sufficiently to allowtheir demonstration; dysphagia, a spastic tonguewhich the patient is unable to protrude, bilateralloss of voluntary facial movements and patho-logical laughing and crying are evident. A doublehemiplegia is present in every case but variesgreatly in severity. It is frequently asymmetricaland on one side may be indicated by little morethan an extensor plantar response. The deep re-flexes are usually exaggerated but may bediminished or absent in the acute stage. It mightbe expected that decerebrate rigidity would becommon but this is not so, though it was aprominent feature in Scott and Lennon's case(I940). In Kubik and Adams' (I946) series of 25cases one only had tonic fits (which may be re-garded as transient decerebrate states). Theseauthors suggest that the rarity of the conditionmight be due to the existence of a state of' shock'equivalent to ' spinal shock.'The supranuclear connections of the eye muscle
nuclei are occasionally involved giving rise todefects of lateral or superior conjugate move-ments. Internuclear ophthalmoplegias occurrarely.
copyright. on A
pril 27, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.329.119 on 1 M
arch 1953. Dow
nloaded from

124 - POSTGRADUATE MEDICAL JOURNAL March I953
Theoretically a cerebellar dyssynergia should bepresent in every case and indeed can sometimes bedemonstrated though usually on one side only;commonly it is masked by the paralysis or byimpairment of consciousness. Nystagmus iscommon. Occasional cases show involvement ofthe third, fifth, sixth or seventh nerves but suchsigns are seen less often than might be expected.The pupils show some abnormality in nearly
every case. As a rule they are small and fixed tolight but occasionally one or both may be dilatedand unresponsive. The pupillary changes dependon involvement of the sympathetic pathways in thebrain stem, of the pupillary fibres in the thirdnerves and possibly of the pretecto-nuclear tracts.
Sometimes the thrombus extends into one orboth of. the posterior cerebral arteries leading toinfarction of the thalamus and the midbrain. Ifthe thrombus reaches beyond the junctions of theposterior communicating arteries--or if these arevery small-the area of infarction will include theoccipital cortex giving rise to a unilateral orbilateral homonymous hemianopia. It is possiblethat the rarity of such findings is due to the factthat infarction of this severity is almost alwaysfatal.
Tachypnoea, tachycardia and hyperpyrexia arecommon accompaniments of basilar artery oc-clusion, though they are usually terminal events.
It is not unlikely that some of the less severeexamples of basilar artery occlusion are regardedas cases of pseudobulbar palsy due to bilateralcapsular lesions.The prognosis in basilar artery occlusion is
generally considered to be grave, but the fact thatof Kubik and Adams' 25 cases seven were stillalive after periods varying from two to 14 months,suggests that the outlook is not quite so desperateas was once thought (see also Moniz, i933; Pinesand Gilensky, I932).The Paramedian and Short CircumferentialBranches of the Basilar Artery
In general the following description is based onthe work of Foix and Hillemand (1926) whichappears to be the most accurate assessment ofthis difficult region.(A) Paramedian BranchesThere are four to six of these entering the pons
a few millimetres on either side of the mid-line.Each divides into numerous branches (sometimescalled the median arteries of Diiret) runningperpendicularly into the substance of the pons.In the uppermost part only do they penetrate intothe tegmentum. Sometimes these vessels arisefrom the short or long circumferential branches
instead of directly from the basilar artery itself.The structures supplied include the corticobulbarand corticospinal tracts, the pontine nuclei, somefibres of the middle cerebellar peduncles andsometimes the medial part of the medial lemniscus.The usual result of occlusion of one of these
vessels is a simple crossed hemiplegia, the severityof which varies widely in different patients. As arule both limbs are affected equally. The hemi-plegia is very difficult to distinguish from one ofcapsular origin. In the latter a history of weaknesscommencing in one limb and later extending to theother may be obtained, whilst if the dominant bodyhalf is affected, yet aphasia is absent, the lesion islikely to be in the brain stem. Contralateral im-
'IJ-i;;F'·' i· E L
;i i 2i!Lrj b ;1 t
It } ·7 A,'i¢
'I*
l..|i. :F wif"r.'- .
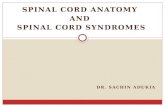
FIG. 6.-Distribution of branches of basilar artery tothe brain stem. The basilar artery has been re-moved. (Diagramatic.)a Posterior perforated substance.b Pons.c Trigeminal nerve.d. Pyramid.e Olive.f Oculomotor nerve.g Posterior cerebral artery.h Superior cerebellar artery.i Basilar artery.j Paramedian branches.k Lateral artery of medulla oblongata.I Short circumferential branches.m Accessory lateral artery' of the medulla
oblongata.n Middle cerebellar artery.(Foix and Hillemand, I9g5b.)
copyright. on A
pril 27, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.329.119 on 1 M
arch 1953. Dow
nloaded from

March 1953 KILOH: The Syndromes of the Arteries of the Brain and Spinal Cord I25
pairment of postural sensibility and of vibrationsense is stressed by some authors but is only anoccasional finding and is rarely severe. Cerebellarsigns, which might be anticipated in view of theinvolvement of the middle cerebellar peduncle,can rarely be demonstrated.
It has been claimed that ipsilateral paralysis ofthe fifth, sixth and seventh nerves may result fromocclusion of the paramedian vessels but this isdenied by Foix and Hillemand who say that suchfeatures indicate involvement of the short circum-ferential branches. On anatomical grounds itappears likely that they are correct.
(B) The Short Circumferential Branches(i) The lateral artery of the medulla oblongata.
This is the lowest lateral branch of the basilarartery. When present it supplies a wedge-shapedarea of the lateral aspect of the upper medullaoblongata immediately rostral to that supplied bythe posterior inferior cerebellar artery though notincluding the restiform body (Alexander and Suh,1937). Foix, Hillemand and Schalit (i925) main-tain that occlusion of this vessel gives rise to a syn-drome indistinguishable from that followingthrombosis of the posterior inferior cerebellarartery and that most of the cases diagnosed as thelatter are, in fact, examples of occlusion of thelateral medullary artery. In view of the very largenumber of cases in which involvement of theposterior inferior cerebellar artery has been provedby post-mortem examination, this view wouldappear to be exaggerated.
(ii) To the Pons. There are four or five of theseand they pass laterally for about one centimetrebefore entering the pons. A branch of one ofthem which penetrates the pons with the fifthnerve is sometimes known as the trigeminal arteryof Duret. These vessels supply the lateral three-fifths of the pons including the lateral portion ofthe corticospinal tract, the main mass of the mediallemniscus, the trigeminal, abducens and facialnuclei and the middle cerebellar peduncle. Withthe exception of its uppermost part, these vesselssupply the entire tegmentum.When one or more of these vessels is occluded
the result depends very much on whether or notthe area of infarction includes the tegmentum.
(a) When it does not, the usual finding is anisolated ipsilateral cerebellar dyssynergia. Insome cases this is associated with contralateralsensory loss either affecting all modalities or'lesscommonly pain and temperature sensations alone.A contralateral hemiplegia-slight in degree-mayalso be present.
(b) When the tegmentum is affected, variouscranial nerves, their nuclei and certain adjacentstructures may be involved. Although the result-
ing syndromes are discussed as clear-cut entities,they also occur in varying combinations:
(i) Millard-Giibler's syndrome. In addition tothe long tract involvement of which a contra-lateral hemiplegia is constant, there is an ipsilateralsixth and seventh nerve paralysis. The latter maybe incomplete.
(2) Raymond's syndrome. This is similar tothe syndrome of Millard-Giibler but the seventhnerve is not affected.
(3) Foville's syndrome. The essential featureis the presence of paralysis of lateral conjugateocular movements to the side of the lesion. Thisis sometimes stated to be due to damage to theparabducens nucleus, but the existence of thisbody has never been confirmed and it is morelikely to result from a lesion of the corticonuclearfibres entering the sixth nerve nuclei. Evidence oflong tract involvement is present and there mayalso be an ipsilateral facial palsy. Foix andHillemand remark that when due to thrombosis,the hemiplegia seen in these syndromes is neversevere. When it is marked it suggests that thecausal lesion is a haemorrhage or a neoplasm.
(4) Posterior internuclear ophthalmoplegia. Thisis associated with damage to the medial longi-tudinal bundle in the neighbourhood of the sixthnerve nuclei. On looking to the side of the lesion,the ipsilateral eye either fails to deviate outwardsor having done so, slowly wanders back towardsthe neutral position. On looking to the oppositeside, the diverging eye may show a similar defectthough in lesser degree. In addition, whenlooking to either side the converging eye may de-,velop coarse lateral jerking movements (ataxicnystagmus). Superficially there is a resemblanceto a unilateral or bilateral sixth nerve paralysis butthere is no convergent strabismus and the in-tegrity of the sixth nerves can be demonstrated byinducing a vestibular nystagmus.
(5) Bulbopontine syndrome of Duret's tri-geminal artery. This syndrome was described byGereb (I949) and his case appears to be the onlyone recorded. There was ipsilateral sensory lossrestricted to the lower two divisions of the fifthnerve, most evident in the tongue, with loss oftaste on the same side and considerable vestibulardisturbance.
(6) Palato - pharyngo - laryngeal myoclonus.Rhythmic myoclonic movements of the palate,pharynx and larynx at a rate of 50 to I8o per min.sometimes result from lesions of the pontinetegmentum. The lingual, facial and ocular musclesmay also participate in the disturbance. Rarelythe diaphragm too is affected. When due tounilateral vascular disease the myoclonus is alsostrictly unilateral but is on the opposite side. Itresults from destruction of the central tegmental
copyright. on A
pril 27, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.329.119 on 1 M
arch 1953. Dow
nloaded from

I26 POSTGRADUATE MEDICAL JOURNAL March I953
tract (thalamo-olivary bundle) (Foix and Hille-mand, I926). The ipsilateral inferior olive showsa trans-synaptic degeneration and pseudohyper-trophy which is in part due to gliosis (Davison,Riley and Brock, I936). A lesion of the dentatenucleus is also said to give rise to the same syn-drome but in this case the myoclonus is ipsilateral(Guillain, et al., I933).
Palato - pharyngo - laryngeal myoclonus mayoccur in isolation but is more commonly accom-panied by symptoms of vestibular disturbance andis sometimes combined with a Millard-Gubler orFoville syndrome.
(7) The occurrence of an isolated hemiplegia orof a cerebellar syndrome has already been noted.An isolated spinothalamic lesion giving rise to adissociated anaesthesia of the entire body half mayalso occur.The existence of such discrete features raises the
interesting question as to whether or not isolatedsixth and seventh nerve palsies (and third nerveparalyses from equivalent lesions of the midbrain)might not have a similar origin. The third andsixth nerve palsies of sudden onset so common inlate adult life are usually attributed to smallaneurysms or, if none can be demonstrated, topressure on the nerve by an atheromatous oranomolous vessel. It seems reasonable to suggestthat some of these cases are, in fact, the result ofbrain stem thromboses although no pathologicalproof of this can be offered.
(See also Alajouanine et al., I935).(C) Long Circumferential Branches
(i) The anterior inferior cerebellar artery (middlecerebellar artery). The anterior inferior cerebellarartery arises from the basilar artery at the junctionof its middle and lower thirds and passes laterallyand downwards crossing the acoustic nerve.
Branches from the main stem: Internal auditoryartery (in the majority of individuals). Smallpontine branches supplying the lateral portion ofthe lower two-thirds of the pons (including thefifth and seventh nerve nuclei and the cochlearnucleus), the middle cerebellar peduncle andsometimes the uppermost part of the medullaoblongata.
Terminal branches: (a) A branch runninglaterally and downwards along the medial andanterior border of the cerebellar hemisphere. (b)A branch running directly laterally round theupper edge of the flocculus over the surface of themiddle cerebellar peduncle and on to the cere-bellar hemisphere.There is considerable variation in the size and
therefore of the importance of the anterior inferiorcerebellar artery. As a rule its size is inversely
proportional to that of the posterior inferiorcerebellar artery.
Dizziness, tinnitus, nausea and vomiting arecommon at the onset of occlusion of this vesselbut consciousness is usually retained. On thesame side as the lesion are found a cerebellardyssynergia with nystagmus, a Homer's syndrome,a lower motor neurone facial weakness and nervedeafness. Impairment of all forms of sensationover the ipsilateral face is usually present thoughtactile sensibility may be less affected than pain andtemperature sensations. The sensory loss is dueto involvement of the incoming fifth nerve or ofits main sensory nucleus. The only contralateralabnormal finding is impairment of pain and tem-perature sensations in the trunk and limbs.Typically this is incomplete because the area ofinfarction is sufficiently posterolateral as not toinvolve the entire spinothalamic tract.A number of cases of occlusion of the anterior
inferior cerebellar artery following attempted re-moval of acoustic neuromata have been reported byAtkinson (I949) who believes that the consequentinfarction of the tegmental area is responsible fora transient rise of blood pressure and for thedevelopment of cerebral oedema which so com-monly leads to death in these patients.
All the features just described as typical ofocclusion of the anterior inferior cerebellar arterymay occas:ionally follow thrombosis of the posteriorinferior c:erebellar artery. Involvement of thenucleus a nbiguus never results from disease of theformer v ssel and the presence or absence ofdysarthria and dysphagia will enable a distinctionto be made.
(See also Goodhart and Davison, 1936).(ii) Thi superior cerebellar artery. The superior
cerebellar arteries are the most constant of thecerebellar vessels. Each arises near the terminationof the bai.lar trunk and runs laterally, parallel tothe poster ior cerebral artery but separated from itby the third nerve. It turns dorsally round thelateral aspect of the cerebral peduncle to reach thecerebellum.
Branches: Twigs sometimes arise from themain vessel and supply the dorsal aspect of thepons and midbrain. The medial and lateralterminal branches ramify over the superior aspectof the vermis and lateral lobe of the cerebellum andform the main supply of the cerebellar white matterand nuclei, including the dentate nucleus. Twigsalso supply the middle and superior cerebellarpeduncles, the upper lateral part of the pontinetegmentum, the lateral aspect of the midbrain andthe quadrigeminal plate. -As with occlusion of the other cerebellar
arteries, dizziness, vertigo, nausea and vomitingare common at the onset. A cerebellar dyssynergia
copyright. on A
pril 27, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.329.119 on 1 M
arch 1953. Dow
nloaded from

March 1953 KILOH: The Syndromes of the Arteries of the Brain and Spinal Cord I27
is usually present on the same side as the lesion butmay be absent--probably because of the richnessof the anastomoses which this artery makes withthe other cerebellar vessels. An ipsilateralHorner's syndrome may be seen. The moststriking feature is the presence of ipsilateral in-voluntary movements which may be associatedwith diminished or absent deep reflexes. Thenature of the movements varies from patient topatient and has been described as a coarse tremorby Schuster and Critchley (1933), sinuous move-ments accentuated by emotion or attempts atvoluntary movement by Worster-Drought andAllen (1929), a rapid athetosis by Guillain, Bertrandand Peron (1928) and as chorea by Adams (I943).The movements have been ascribed to involve-ment of the superior cerebellar peduncle or of thedentate nucleus. Considerable degeneration ofthe opposite red nucleus with demyelinization ofits entering fibres is present in these cases.
Contralateral loss of pain and temperaturesensation affects the entire body half including theface but is absent if only the medial branch of theartery is occluded. Sometimes it is confined tothe lower part of the body due to the lamination ofthe spinothalamic tract.
Involvement of cranial nerves or their nuclei isnot a feature of superior cerebellar artery occlusionand the partial lesions of the ipsilateral sixth andseventh nerves which have occasionally beendescribed, usually indicate coincidental involve-ment of the pontine arteries. An ipsilateral fourthnerve paralysis has been described by Girard, etal (1950).An occasional featUre, notably in the cases
described by Mills (90o8) and Russel (I93 ), isloss of emotional movements with preservation ofvoluntary movements over the contralateral face.This is to be explained as the result of a lesion ofthe mimic tracts subserving emotional movementswhich run independently of the pyramidal tracts.
(See also Davison et al., 1935; Freeman andJaffe, I94I; Sandler, 1935.)
AcknowledgmentsWe acknowledge with thanks permission to
publish illustrations 4, 5 and 6 from the RevueNeurolgique and permission to publish illustrationsI and z from Williams and Wilkins Co., Baltimore.
BIBLIOGRAPHY
ABBIE, A. A. (I933), ' Clinical significance of the anterior chorioidalartery,' Brain, 56, 233.
ADAMS, R. D. (I943), 'Occlusion of the anterior inferior cere-bellar artery,' Arch. Neurol. & Psychiat., 49, 765.
ADAMS, R. D and MERRIT, H. H. (x944), 'Meningeal andvascular syphilis of the spinal cord,' Medicine, 23, i8I.
AKELAITIS, A. J., RISTEEN, W. A., HERREN, R. Y., andWAGENEN, W. P. (I942), 'Studies on the corpus callosum,'Arch. Neurol. & Psychiat., 47, 97I.
ALAJOUANINE, T., THUREL, R., and HORNET, T. (I935),'An anatomoclinical case of palatal and ocular myoclonia,'Rev. Neurol., 64, 853.
ALEXANDER, L., and SUH, T. H. (I937), ' Arterial supply of thelateral parolivary area of the medulla oblongata in man,' Arch.Neurol. & Psychiat., 38, 1243.
ANDERSON, A. G., LOCKHART, R. D., and SOUTER, W. C.(1931), 'Lateral syndrome of the medulla oblongate,' Brain,54, 6o0.
ATKINSON, W. J. (1949), ' The anterior inferior cerebellar artery,'J. Neurol. Neurosurg. & Psychiat., 12, 137.
BACALOGLU, NICOLESCO, J., RAILEANU, C., andHORNET, T. (x934), 'A propos de la pathologie vasculairethalamo-mesencdphalique,' Rev. Neurol., 2, 896.
BALDY, R. (1927), ' Les syndromes de l'arthre cer6brale antdrierue,Paris, Jouve et Cie, cit., Critchley (1930), q.v.
BIEMOND, A. (I95s), 'Thrombosis of the basilar artery and thevascularization of the brain stem,' Brain, 74, 300.
BREMER, F. (I935), 'Cerveau isola et physiologie de sommeil,'C.R. Soc. Biol., Paris., 8,I235.
BROCK, S. J. (I937), 'Basis of Clinical Neurology,' Baltimore,William Wood & Co.
CABOT, Case 23371 (I937), 'Thrombosis of the right vertebralartery,' New England J. Med., 217, 487.
COGAN, D. G., KUBIK, C. C., SMITH, W. L. (I95O), ' Unilateralinternuclear ophthalmoplegia,' Arch. Ophth., 44, 783.
CRITCHLEY, M. (1930), 'The anterior cerebral artery and itssyndromes,' Brain, 53, 120.
DANDY, W. E. (I930), 'Artery of consciousness,' Am. _. Physiol.,93, 643.
DAVISON, C. (Iq37), ' The syndrome of the anterior spinal arteryof the medulla oblongata,' Arch. Neurol. & Psychiat., 37, 9I.
DAVISON, C. (I944), 'Syndrome of the anterior spinal artery ofthe medulla oblongata,' J. Neuropath. & Exper. Neurol., 3, 73.
DAVISON, C., GOODHART, S. P., and NEEDLES, W. (I933),' Cerebral localization in cerebrovascular disease,' Arch. Neurol.& Psychiat., 30, 749.
DAVISON, C., GOODHART, S. P., and SAVITSKY, N. (I935),'The syndrome of the superior cerebellar artery and itsbranches,' Ibid., 33, I I43.
DAVISON, C., RILEY, H. A., and BROCK, S. (1936),' Rhythmicmyoclonus of the muscles of palate, larynx and other regions,'Bull. Neurol. Inst., N. Y., 5, 94.
DIRJERINE, J., and EGGER, M. (1903), 'Contribution a l'dtudede la physiologie pathologique de l'incoordination motrice,'Rev. Neurol., II, 397.
DiJERINE, J., and ROUSSY, G. (I906), 'Le syndrome thala-mique,' Ibd., 14, 521.
DIGGLE, F. H., and STOPFORD, J. S. B. (I935), 'Posteriorinferior cerebellar and vertebral artery thrombosis,' Lancet,i,12I4.
DIMITRI, V., and VICTORIA, M. (1936), 'Syndrome of theanterior cerebral artery,' Revista Neurol., Buenos Ayres, x, 8I.
ELVIDGE, A. R., and WERNER, A. (s95i), 'Hemiplegia andthrombosis of the internal carotid system,' Arch. Neurol. &Psychiat., 66, 752.
ETHELBERG, S. (I95I), 'On changes in circulation through theanterior cerebral artery,' Acta. Psychiatra et Neurologica,$upplementum No. 75.
FISHER, M. (I95I), 'Occlusion of the internal carotid artery,Arch. Neurol. & Psychiat., 65, 346.
FOIX, CH., and HILLEMAND, P. (I925a), 'Les syndromes del'artere cer6brale anterieure,' Encdphale, 20, 209.
FOIX, CH., and HILLEMAND, P. (1925b), 'Les arteres de l'axeencephalique jusqu'au diencephale inclusivement,' Rev.Neurol., 2, 705.
FOIX, CH., and HILLEMAND, P. (1926), ' Contribution a l'etudedes ramollissements protuberantiels,' Rev. de Mddecine, 43, 287.
FOIX, CH., HILLEMAND, P., and SCHALIT (I925), 'Sur elsyndrome lateral du bulbe et l'irrigation du bulbe superieure,'Rev. Neurol., x, i6o.
FOIX, CH., and LeVY, M. (I927), ' Softening in the region of theSylvian artery,' bid., 2, x.
FREEMAN, W., and JAFFE, D. (I94I), 'Occlusion of the superiorcerebellar artery; report of a case with autopsy,' Arch. Neurol.& Psychiat., 46, x .
copyright. on A
pril 27, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.329.119 on 1 M
arch 1953. Dow
nloaded from

128 POSTGRADUATE MEDICAL JOURNAL March I953
GER1B, T. (1948),' Bulbopontile syndrome of Diiret's trigeminalartery,' Monatschr. f. Psychiat. u. Neurol., 115, 103.
GIRARD, P. F., BONAMOUR, GARDE, and ETIENNE (X950),'Les syndromes de l'obliteration de l'artere c6r&belleusesup6rieure,' Rev. Neurol., 83, 199.
GOODHART, S. P., and DAVISON, C. (1936), 'Syndromes ofthe posterior inferior and anterior inferior cerebellar arteriesand their branches,' Arch. Neurol. & Psychiat., 35, 501.
GUILLAIN, G., BERTRAND, I., and PtRON, N. (1928), 'Lesyndrome de l'artere cer6belleuse superieure,' Rev. Neurol.,2, 835.
GUILLAIN, G., THUREL, R., and BERTRAND, I. (1933)'Examen anatamopathologique d'un cas de myoclonies v6lo-pharyngo-oculo-diaphragmatiques,' Ibid., 2, 8oi.
HERREN, R. Y., and ALEXANDER, L. (I939), ' Sulcal and in-trinsic blood vessels of the human spinal cord,' Arch. Nefurol.& Psychiat., 4i, 678.
HYLAND, H. H. (I933), 'Thrombosis of intracranial arteries,Ibid., 30, 342.
JEFFERSON, M. (1952), 'Altered consciousness associated withbrain stem lesions,' Brain, 75, 55.
KUBIK, C. S., and ADAMS, R. D. (1946), Occlusion of the basilarartery,' Ibid., 69, 73.
LANGWORTHY, O. R., and FOX, H. NI. (x937), 'Thalamicsyndrome; syndrome of posterior cerebral artery,' Arch. Int.Med., 60, 203.
LINDSLEY, D. B., SCHREINER, L. H., KNOWLES, W. B.,and MAGOUN, H. W. (1950), ' Behavioural and EEG changesfollowing chronic brain stem lesions in the cat,' EEG Clin.Neurophysiol., 2, 483.
LOUIS-BAR, D. (1947), Syndrome of the anterior spinal arteryparamedian inferior bulbar syndrome),' Monatschr. f. Ps3,chiat.u. Neurol., 113, 40.
MARCET, A. (I817), ' History of a singular nervous or paralyticaffection attended with anomalous morbid sensations,' Medico-(Chirurgical Trans., 2, 217.
MARTIN, P. (1949), Consciousness and its disturbances,' Lancet,i, I.
MERRITT, H. H., and FINLAND, M. (1930), 'Vascular lesionsof the hind brain (lateral medullary syndrome),' Brain, 53, 290.
MEYERS, R., SWEENEY, D. B., and SCHWIDDE, J. T. (I950),Hemiballismus, aetiology and treatment,' J. Neurol. Neuro-
surg. & Psychiat., 13, 115.MILLS, C. K. (i908), 'Hemianaesthesia to pain and temperature
and loss of emotional expression of right side with ataxia ofupper limb on the left,' J7. Nerv. & Mental Dis., 35, 331.
MONIZ, E. (i03i), 'Hemibalismo, a proposito de tres casos,'Lisbon Medica, 8, 481.
MONIZ, E. (1933), 'The basilar trunk and arteries derived fromit,' Encdphale, 28, 705.
NIELSON, J. M. (1946), 'Agnosia, apraxia and asphaia,' NewYork, Paul B. Hoeber.
O'BRIEN, F. H., and BENDER, M. B. (1945), 'Localizing valueof vertical nystagmus (anterior spinal artery thrombosis),' Arch.Neurol. & Psychiat., 54, 378.
PARISER, S., and LASAGNA, L. (r949), 'Occlusion of theanterior spinal artery,' J7. Mt. Sinai Hosp., x6, 128.
PINES, L., and GILENSKY, E. (1930), Thrombosis of vertebralartery,' Arch. f. Ps3,chiat., 90o, I77.
PINES, L., and GILENSKY, E. (1932), 'Thrombosis of basilarartery and vascularization of pons varolii,' Ibid., 97, 380.
POPPEN, J. L. (x939), ' Ligation of the anterior cerebral artery,'Arch. Neurol. & Psychiat., 41, 495-
PREOBRAJENSKY (i907), ' Thrombosis of anterior spinal artery,'cit., Zeitlin and Lichtenstein (1936), q.v.
RUBINSTEIN, H. S. (x944), ' The anterior communicating arteryin man,' J. Veuropath. & Exp. Path., 3, x96.
RUSSEL, C. K. (1931), ' Syndrome of the brachium conjunctivumand tractus spinothalmicus,' Arch. Neurol. & Psychiat., 25,1003.
SANDLER, S. A. (1935), ' Syndrome of superior cerebellar artery,J. Nerv. & Mental Dis., 82, 263.
SAVITSKY, N., and ELPERN, S. P. (1948), 'Gangrene of facefollowing occlusion of posterior inferior cerebellar artery,Arch. Int. Med., 84, 43I.
SCHALLER, W. F., ROBERTS, A. M., and STADTHERR, E. F.(1932), 'Acute myelitis (syndrome of occlusion of anteriorspinal artery),' J.A.M.A., 99, 1572.
SCHUSTER, P., and CRITCHLEY, M. (1933), 'BeitrAge zurAnatomie und Pathologie der Arteria cerebelli superior,'Ztschr. f.d. ges Neurol. u. Psychiat., I44, 68I.
SCOTT, M., and LENNON, H. C. (1940), ' Decerebrate tonicextensor convulsions as a sign of occlusion of the basilar artery,'Arch. Neurol. & Psychiat., 44, IO02.
SENATOR, H. (1883), 'Zur diagnostik der Herderkrankungen inder BrUcke under der verlangerten Mark,' Arch. f. Psychiat.,14, 643.
SHEEHAN, C., and SMYTH, G. E. (1937), 'A study of theanatomy of vertebral thrombosis,' Lancet, ii, 614.
SHELLSHEAR, J. L. (I922), ' Blood supply of the dentate nucleusof the cerebellum, Ihid., i, 1046.
SHERMAN, I. C. (1948), 'Thrombosis of anterior spinal artery,Arch. Neurol. & Psychiat., 59, 844.
SMYTH, G. E. (I 939), The systematization and central connectionsof the spinal tract and nucleus of the trigeminal nerve,' Brain,62, 41.
SPILLANE, J. D. (x937), 'Posterior inferior cerebellar arterythrombosis,' Bull. Neutrol. Inst. New York, 6, 529.
SPILLER, W. G. (I9o8), ' The symptom complex of a lesion of theuppermost portion of the anterior spinal and adjoining portionof the vertebral arteries,' J. Nert. & Mental Dis., 35, 775.
STEEGMAN, A. T., and ROBERTS, D. J. (1935), ' Syndrome ofanterior chorioidal artery,' J.A.M.A., xo4, x695.
STOPFORD, J. S. B. (I916, I917), The arteries of the pons andmedulla oblongata. J. Anat. & Physiol., 5o, 131, 255; SI, 252.
'ICHY, F. (I949), ' Syndromes of cerebral arteries,' Arch. Path,48, 475.
WALLENBERG, A. (1895), 'Acute Bulbaraffection (Embolie derArt. Cerebellar post. inf. sinistr.?),' Arch. f. Psychiat., 27, 504.
WILLIAMS, D. J. (I936), ' Origin of the posterior cerebral artery,'Brain, 59, I75.
WORSTER-DROUGHT, C., and ALLEN, I. M. (I929),' Throm-bosis of superior cerebellar artery,' Lancet, ii, 137.
ZEITLEIN, H., and LICHENSTEIN, B. W. (I936), 'Occlusionof the anterior spinal artery,' Arch. Neurol. & Psychiat., 36,96.
H.K. LEWIS&Co. Ltd. Medical Lending LibraryMedical Pu blishers ANNUAL SUBSCRIPTION from TWENTY-FIVE SHILLINGS
For the CONVENIENCE of POST-GRADUATE STUDENTS SHORTand Booksellers PERIOD SUBSCRIPTIONS ARE ARRANGED - for 3 or 6 monthsCatalogues on request State interests Detailed Prospectus on application1 36 GOWER STREET The Library Catalogue revised to December, 1949, containing
classified index of authors and subjectsLONDON, W.C. 1 To subscribers 17/6 net; To non-subscribers 35/- net. Postage 1/3
(Adjoining University College and Hospital) Supplement 1950-1952 in preparationBi-Monthly List of New Books and New Editions
Telephone: EUSton 4282 (7 lines) sent post free on requestTelegrams: Publicavit, Westcent, LondonBusinesshours:a.m.to5p.m. Saturdays: p.m. NEW BOOKS ADDED IMMEDIATELY UPON PUBLICATIONBusiness hours: 9 a.m. to 5 p.m. Sarturdays: I p.m.
copyright. on A
pril 27, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.29.329.119 on 1 M
arch 1953. Dow
nloaded from