South East London Sector A meeting of NHS Bromley CCG Governing Body 11 … guide... · A meeting...
27
Clinical Chair: Dr Andrew Parson 1 Chief Officer: Dr Angela Bhan South East London Sector A meeting of NHS Bromley CCG Governing Body 11 July 2013 ENCLOSURE 3 End of Life Business Case SUMMARY: As part of the ProMISE Programme, Bromley CCG is proposing the commissioning of an End of Life Care Model which facilitates and supports people in their last year of life and affords them the opportunity to die with dignity in their “normal place of residence”, rather than in an acute setting. In Bromley approximately 2,600 deaths are recorded each year, with circa 80% of those coded as expected deaths from chronic conditions; predominantly cancer, respiratory or cardiovascular disease. Bromley also has a higher than average number of deaths from dementia. Of those total deaths, 56% die in hospital. Comparatively however, those referred via St Christopher’s Hospice tend to die at home, with only 20% dying in hospital. Whilst the quality and cost issue exists in 2013, these will be further compounded as the over 65 years population grows by 14% by 2021. Activity data currently indicates that people in their last year of life tend to be admitted twice, preceding the point of admission when they die, with admission via A&E. Both unplanned admission costs and A&E admission will be charged under PbR, costing the CCG approximately £15,636,400 per annum. Bromley CCG therefore proposes a model of an End of Life Care Coordination Centre to include out of hours advice centre, focussing on a single point of entry, as set up with Bromley Healthcare and coordination of care for the last year of life. Patients will be case found and the centre will receive referrals leading to an anticipated improvement in home death rates for the benefit of patients and their families and reducing hospital admission in the final year of life . KEY ISSUES: A key issue for the Governing Body’s consideration is the recommendation that this service be offered to St Christopher’s Group without recourse to procurement. Presently End of Life services are provided routinely by various agencies; notably domiciliary carers via London Borough of Bromley Social Services, St Christopher’s Hospice and Harris Hospiscare providing in-patient care, home care and a range of outpatient and day care services, Community services provided by Bromley Healthcare.
Transcript of South East London Sector A meeting of NHS Bromley CCG Governing Body 11 … guide... · A meeting...
Clinical Chair: Dr Andrew Parson 1 Chief Officer: Dr Angela Bhan
South East London Sector
A meeting of NHS Bromley CCG Governing Body 11 July 2013
ENCLOSURE 3
End of Life Business Case
SUMMARY:
As part of the ProMISE Programme, Bromley CCG is proposing the commissioning of an End of Life Care Model which facilitates and supports people in their last year of life and affords them the opportunity to die with dignity in their “normal place of residence”, rather than in an acute setting. In Bromley approximately 2,600 deaths are recorded each year, with circa 80% of those coded as expected deaths from chronic conditions; predominantly cancer, respiratory or cardiovascular disease. Bromley also has a higher than average number of deaths from dementia. Of those total deaths, 56% die in hospital. Comparatively however, those referred via St Christopher’s Hospice tend to die at home, with only 20% dying in hospital. Whilst the quality and cost issue exists in 2013, these will be further compounded as the over 65 years population grows by 14% by 2021. Activity data currently indicates that people in their last year of life tend to be admitted twice, preceding the point of admission when they die, with admission via A&E. Both unplanned admission costs and A&E admission will be charged under PbR, costing the CCG approximately £15,636,400 per annum. Bromley CCG therefore proposes a model of an End of Life Care Coordination Centre to include out of hours advice centre, focussing on a single point of entry, as set up with Bromley Healthcare and coordination of care for the last year of life. Patients will be case found and the centre will receive referrals leading to an anticipated improvement in home death rates for the benefit of patients and their families and reducing hospital admission in the final year of life . KEY ISSUES:
A key issue for the Governing Body’s consideration is the recommendation that this service be offered to St Christopher’s Group without recourse to procurement. Presently End of Life services are provided routinely by various agencies; notably domiciliary carers via London Borough of Bromley Social Services, St Christopher’s Hospice and Harris Hospiscare providing in-patient care, home care and a range of outpatient and day care services, Community services provided by Bromley Healthcare.

Clinical Chair: Dr Andrew Parson 2 Chief Officer: Dr Angela Bhan
The current annual Bromley CCG investment in specialist end of life services is detailed below:
St Christopher’s Hospice o Contract £1,198,684 o CQUINS £17,496
Harris Hospiscare with St Christopher’s o Contract £714,097 o CQUINS £10,711
Care Home project – funded by a separate Service Level agreement o Contract £59,388
It should be noted that the payment from the CCG covers between one-third to one-half of the actual annual cost of the services provided to Bromley residents by the St Christopher’s Group. The remaining cost of the service is currently covered by the London Borough of Bromley within the Social Care budget.
Rationale for the waiver
The St Christopher’s Group already provides an excellent range of local End of Life Care services in Bromley
The service design is a reconfiguration of existing services, not a material change to the way in which services are presented to the “user” via pathway redesign or resource change, as supported by the waiver against completion of section 242 (NHS Act of 2006). Only the introduction of an out of hours coordination centre would be an addition to the service provision.
The costings for the care coordination centre demonstrates value for money, comparable with that of the Croydon service and charges the CCG for only the cost of the day service provision (including staff costs, IT training and marketing) with the out of hours service subsumed by St Christopher’s and Partners.
Significant patient and carer participation has contributed to the development of this model, as identified in Section 6 of the Full Business Case)
End of Life Care would be more fragmented if another specialist palliative care provider entered the market
There is currently no alternative local, specialist provider with significant experience already established in the area that could provide immediate service provision with limited infrastructure and startup costs.
St Christopher’s Hospice, LBB Carers and community staff have demonstrable capacity and experience that can be quickly adapted to develop this integrated service approach.
St Christopher’s is already well networked with local providers and agencies to support the integrated approach, with pace and scale
The organisation has both an intellectual capital and unparalleled experience with specialist end of life care in the Bromley area
80% of bereaved carers (VOICES-hospices survey respondents) consistently say that the care

Clinical Chair: Dr Andrew Parson 3 Chief Officer: Dr Angela Bhan
St Christopher’s Group home care patients receive is ‘exceptional’ or excellent’
The 5 CCG Cluster contract with St Christopher’s Hospice expired on 31st March 2013 and is being rebased in year, with the provision of a new 3 year contract to be discussed in September 2013.
OVERALL RISK ASSESSMENT
See Section 10 of business case attached
COMMITTEE INVOLVEMENT:
ProMISE Programme Board
Strategy Planning Group
Clinical Executive
Clinical Advisory Group
PUBLIC AND USER INVOLVEMENT:
See section 6 of Business Case attached
IMPACT ASSESSMENT:
See Appendix 5 of Business Case attached RECOMMENDATIONS:
The Governing Body is asked to:-
Approve the business case and agree to the recommendation that the waiver of the single tender requirement and the award of the contract for this service to St Christopher’s Group
ACRONYMS
CCG – Clinical Commissioning Group CQUIN – Commissioning for quality and innovation LBB – London Borough of Bromley QIPP – Quality Innovation Productivity and Prevention
DIRECTORS CONTACT:
Name: Meredith Collins E-Mail: [email protected] Telephone: ext. 2723
AUTHOR CONTACT: Name: Kate Dawes E-Mail: [email protected] Telephone: 07841 707684, ext. 2675

1
For the Attention Of Bromley CCG
ProMISE Board
Agenda Heading End of Life Care - Service Enhancement
Date 17th June 2013
Consideration of Project Principles Insert
cross (x)
Scale and pace √
Patient engagement x
Joint working (JSNA, Wellness agenda etc.) √
Using best practice √
Developing appropriate commissioning to imbed the business case √
Date for Post Implementation Review July 2014
Report Author Kate Dawes, Programme Manager
Date 17th June 2013
Contact Details [email protected]
Senior Sponsor Meredith Collins, Director of Healthcare System Reform
Signed off by Name Signature Date
Programme Board Paul White
Finance Lucy Cole
Informatics Sarah Osborn
Project Management
Chris Evennett
Pathway Redesign TBC
IT N/A
HR N/A

2
1 Business Case History
1.1 Document Location This document is only valid on the day it was printed.
The source of the document will be found at this location: Strategic Programmes\Promise integrated
care\end of life.
1.2 Revision History Date of this revision: 08.05.2013
Date of next revision:
Date of further revision: 12.4.13 following discussions at SPG
Revision
date
Previous
revision date
Summary of Changes Changes
marked
08.05.2013 08.05.2013 First cut of the CCG business case
1.3 Approvals This document requires the following approvals.
Signed approval forms should be filed appropriately in the project filing system.
Name Signature Title Date of
Issue
Version
Meredith Collins
1.4 Distribution This document has been distributed to:
Name Title Date of Issue Version
ProMISE Programme Board
Clinical Advisory Group
Strategic Planning Group
3
2 Table of contents
Item Page
3 Executive summary 4
4 The case for change 5
5 Current service provision for specialist end of life care 6
6 Consultation with residents, users & stakeholder groups 7
7 Proposed solution 8
8 Financial modelling 10
9 Options for the way forward 13
10 Risk 13
11 Performance monitoring 13
Appendix 1 Description of services provided by the St Christopher’s Group 15
Appendix 2 A visual outline of the Bromley End-of-Life Care Partnership 16
Appendix 3 Financial model costings 17
Appendix 4 Market Management, Redesign and Procurement Assessment Tool
18
Appendix 5 Equality Impact Assessment 22

4
3 Executive Summary
As part of the ProMISE Programme, Bromley CCG is proposing the commissioning of an End of Life
Care Model which facilitates and supports people in their last year of life and affords them the
opportunity to die with dignity in their “normal place of residence”, rather than in an acute setting.
The proposed model integrates well within the wider strategic paradigm for Coordinate My Care and
NHS 111.
In Bromley approximately 2,600 deaths are recorded each year, with circa 80% of those coded as
expected deaths from chronic conditions; predominantly cancer, respiratory or cardiovascular disease.
Bromley also has a higher than average number of deaths from dementia. Of those total deaths, 56%
die in hospital. Comparatively however, those referred via St Christopher’s hospice tend to die at
home, with only 20% dying in hospital. Whilst the quality and cost issue exists in 2013, these will be
further compounded as the over 65 years population grows by 14% by 2021.
Activity data currently indicates that people in their last year of life tend to be admitted twice,
preceding the point of admission when they die, with admission via A&E. Both unplanned admission
costs and A&E admission will be charged under PbR, costing the CCG approximately £15,636,400 per
annum.
Bromley CCG therefore proposes a model of an End of Life Care Coordination Centre to include out of
hours advice centre, focussing on a single point of entry, as set up with Bromley Healthcare and
coordination of care for the last year of life. Patients will be case found and the centre will receive
referrals. Key components of the service will be provision of:
Nurse specialist assessment, including
advance care planning conversations
Key workers
Coordinate my care registers
Three monthly reassessment
Organising Marie Curie nursing
Coordinate Medical equipment
Support links in to community services
for integrated approach
Rapid response to patient’s who’s
conditions have changed
Provide personal care services for up
to 6 weeks for PRU discharges
Cost for the provision of this service is estimated at £243,000, with additional community costs for
alternative community care stay costs (to acute provision) at £188 per day. The St Christopher’s Group
has fully disclosed the costs of this service, which passes on only the resource costs for the day staff,
with out of hours staff costs and margins excluded. (Appendix 3).
Scenario modelling has ascertained the savings and costs below dependent on the number of hospital
deaths to be avoided. It is anticipated that the most likely scenario (scenario 3) will achieve net savings
of £321,000.
Scenario Reduction in emergency admissions @£3,987 LOS 8 days
Reduction in prior admissions @£1716 LOS 2 days
Reduction in A & E attendances @£311
Cost of alternative community care for both stays @£188 per day (LOS 10 days)
Cost of new Centre
Net Savings
Best case 305 305 610 3050 days
£1,216K £523K 189K £573K £243K £1,112K

5
Worst case 52 52 104 520 days
£207K £89K £32K £98K £243K £9K
Most likely *
179 179 357 1790 days
£714K £307K £111K £337K £243K £552K *Please note that changes to figures as presented to the Clinical Executive have not been checked by finance,
but relate to a midpoint of best and worst cases, which have been ratified by Finance.
4 The case for change
The demographic challenge
The London Borough of Bromley has an estimated population of 312,580 people1, with a higher than
average older population and approximately 2,600 deaths each year. Of these 20 – 25% will die
suddenly, leaving 80% dying predominantly of cancer, respiratory or cardiovascular disease. Bromley
also has a higher than average number of death from dementia, 21% as opposed to a national average
of 17.3%. This is statistically significant as end of life care has been shown to be more challenging for
dementia patients and they experience a lower rate of home deaths and, in general, poor end of life
care.
The palliative care needs of Bromley residents are likely to increase in time as it is estimated that the
population will grow by 14% by 2021; this is faster than the UK average growth of 9% for the same
time period. This population growth is coinciding with demographic changes occurring across the UK
as a result of the ageing baby boom population which will mean that the number of people residing in
Bromley that will require end of life services is set to increase rapidly over the coming years.
Opportunities to improve the quality of the service
Bromley also faces a unique challenge for the palliative care needs of its ageing population and there
is some evidence that residents are currently not satisfied with the level of care that they are receiving
1. NHS England’s outcomes benchmark and support packs show that Bromley is one of the worst
performing areas in England in terms of patients rating of the out-of-hours GP provision.
Identification of end of life care patients is important in ensuring they receive the right co-ordinated
care from all different service and that their care preferences are recorded and communicated to the
variety of care providers that they may encounter. For this reason many areas have begun to keep End
1 End of life care intelligence network, Bromley Local Authority profile, 2012

6
of Life Care registers of patients who are nearing the end of their life. There is evidence to show that
Bromley may not be recording their palliative care patients effectively. This is supported by the data
shown below:
Source: Marie Curie End of Life Atlas
The chart shows that Bromley has much lower percentages of deaths recorded on a palliative care
register than the other boroughs in South East London. This includes both deaths with and without
palliative care needs. Of the 56% of people in Bromley who die in hospital, there is an imbalance in
terms of diagnosis. Over a five year period, people with cancer were much less likely to die in hospital
than people with other conditions. (43% cancer and 65% other conditions), suggesting more needs to
be done.
The Results of the first national VOICES survey of bereaved people showed that SE London had
comparatively low results for the majority of the end of life measures. Research shows us that if given
the choice, most people would prefer to die at home and the least preferred place of death is in
hospital. Rates of hospital deaths in Bromley remain round 56% with only 36% dying in their own
home (incl. care homes) 1. The major limitation of the current end of life provision is not being able to
exploit the benefits (both financial and human) which derive from early referral and the potential for
more integrated and coordinated health and social care. Amongst these are:
Avoidance of hospital admissions
A smooth and speedy transition from hospital to home
Increasing further patient and carer satisfaction
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
Bexley
PCT
Bromley
PCT
Greenwich
Teaching
PCT
Lambeth
PCT
Lewisham
PCT
South
East
London
Total
Southwark
PCT
UK Total
% of deaths with PC need on a PC register % of ALL deaths on palliative care register

7
A link to a wider population which offers the added value of community engagement and of a bespoke volunteer programme
The benefits of getting ‘all care in one go in one place’ – a ‘one stop shop’ approach. We know that working with multiple agencies saps people’s care giving capacity and energy. Also the benefits of one key person knowing someone’s ‘story’ – patients and carers not having to repeat themselves
5 Current service provision for specialist end of life care
End of life care is of course provided routinely by local health and social care providers, but specialist
palliative care services are provided by the St Christopher’s Group from two sites – one in Sydenham
and the other in Orpington. These services include in-patient care, home care and a range of
outpatient and day care services. These are detailed in appendix 1.
In 2011 the St Christopher’s Group had 472 referrals in Bromley North and 490 referrals in Bromley
South. Patients receive 24 hour advice and visiting service and have access to an extensive specialist
multi-disciplinary team. The St Christopher’s Group reverse the trend of where Bromley residents die
with only 20% of their caseload dying in hospital and 54% of their caseload dying at home/care home.
Using a validated outcome measure, St Christopher’s Index of Patient Priorities (SKIPP), levels of
satisfaction with the care provided have remained consistently at over 80%.
The annual Bromley CCG investment in specialist end of life services is detailed below:
St Christopher’s Hospice
Contract £1,198,684
CQUINS £17,496
Harris Hospiscare with St Christopher’s
Contract £714,097
CQUINS £10,711
Care Home project – funded by a separate Service Level agreement
Contract £59,388 per year
It should be noted that the payment from the CCG covers between one third to one half of the actual
annual cost of the services provided to Bromley residents by the St Christopher’s Group.
6 Consultation with residents, users and stakeholder groups

8
St Christopher’s has worked in partnership with Bromley Health Care, London Borough of Bromley and
Marie Curie to develop this proposal. Other key partners are still in negotiation and include GPs,
PRUH, Carers Bromley, Age UK, Oxleas and residential and nursing homes.
Specific consultation is documented below:
Report commissioned by BHC relating to feedback from recently bereaved carers of people
who had died of a non-malignancy and had not been under the care of St Christopher’s. 2011
QUALYCARE gathered bereaved relatives views of care in three London boroughs. The Public
Health department in Bromley were part of a research study being carried out by the Cicely
Saunders Institute at King’s Hospital.
User Forums’ at St Christopher’s and HarrisHospice held regularly and frequently.
SKIPP (St Christopher’s Index of Patient Priorities) which demonstrates the impact of the
difference it makes patients when their care is co-ordinated by St Christopher’s.
Bromley End of Life Strategy Group- Nursing Director of St Christopher’s has membership and
is Vice Chair.
Feedback questionnaire to service users of various parts of the service, specifically Patients
receiving the Community Support Volunteer service and those receiving social care and night
sitting service, looking at
o Perceived reliability and helpfulness of worker
o Dignity and respect
o Responsiveness to individuals’ needs
o Communication (and coordination of care)
7 Proposed solution
This is a proposal to radically redesign the end of life pathway in Bromley offering a new commitment
to end of life care in the local community.
What will the service look like?
The Bromley End-of-Life Care Partnership:
1. A new End of Life Care Co-ordination to include an out of hours
advice service:
This will be hosted and managed by the St Christopher’s Group and will focus on referral into a
single point of entry (SPE) already set up with Bromley Health. The details of anyone who is on or
eligible to be on the GSF/CMC registers will be forwarded to the co-ordination centre (details
below). The centre will ensure that health and social care services do not work in silos and that the
9
patient and family experiences timely and co-ordinated care.
How will it work in practice?
Case-finding the extra 800 patients - this will be achieved in the following ways:
From those referred into the St Christopher’s reablement hospital discharge pilot
From the St Christopher’s Group Clinical Nurse Specialists who currently attend Primary
Care/GSF/Nursing Home meetings. These meetings are fundamental to achieving ‘joined-
up’ care. The CNS’s will case-find the non-specialist population via these meetings
The St Christopher’s Group will shortly be launching a palliative heart failure service across
Bromley. This is a research study/service evaluation and will be working with Bromley
Health, the CCG and the PRUH. Academic support is being provided by the Cicely Saunders
Institute, Kings College London University. This new service will be able to identify another
group of people in the last year of life
The St Christopher’s Group works closely with Bromley Health and will be re-configuring
services in line with the newly developing Integrated Teams. Within this they will also
have contact with the specialist nurses in COPD and Heart Failure who will be another
source of case identification
More specifically the new centre will:
Each referral to the co-ordination centre will have an assessment by a nurse experienced in
end of life care. This will be agreed as a joint visit with a district nurse or community matron,
for example, if they are already involved with the referred patient. The assessment will
include a medical/nursing assessment, medication review, advance care planning and
conversations concerning preferred place of care/death and whether to attempt
cardiopulmonary resuscitation. A carers assessment will also be completed.
Following the assessment a decision will be jointly made to the appropriate key worker. This
decision will be made in consultation with the nurse attending the joint assessment
The co-ordination centre will therefore ensure that all patients referred will receive the
appropriate care package and professional support at the right time
Patients’ details will be entered, with their consent, onto the CMC register and the register
will be kept up to date
The centre will ensure feedback to primary care GSF meetings of the clinical picture of their
patients by centre staff or via one of the partners
Once on the ‘hub’ (co-ordination centre) register the hub nurses will reassess the patient 3
monthly either together with the named key worker or by telephone

10
The centre will ensure the delivery of a personal care service up to six weeks for discharges
from the PRUH and continued personal care for CC1 patients (One year pilot project funded
by the Reablement Board)
For patients who are receiving social care from a domiciliary agency, the ‘hub’ will have
regular contact to optimise joined up delivery of care and to encourage social carers to
feedback any concerns or changes they have observed in the patients. Training will be
offered by the ‘hub’.
The centre will organise Marie Curie night nursing
The centre will have a direct link with MEDIQUIP equipment services and will administrate
the ordering of equipment for patients referred to ensure people can access the right
equipment as quickly as possible
The centre will have strong links to Bromley Health services, including community nursing
and therapists to ensure the delivery of care is integrated
The centre will have a strong link to the Local Authority and Social Services and OXLEAS
(regarding the management of end stage dementia) to ensure all the appropriate services
are involved
The centre will work directly with the St Christopher’s Group specialist community services
and ensure that patients are referred into these services at the appropriate time
St Christopher’s is developing extensive support in the community via a bespoke volunteer
support service. The centre will have access to this
The centre will be able to respond rapidly to patients whose condition has changed and a
reassessment needed
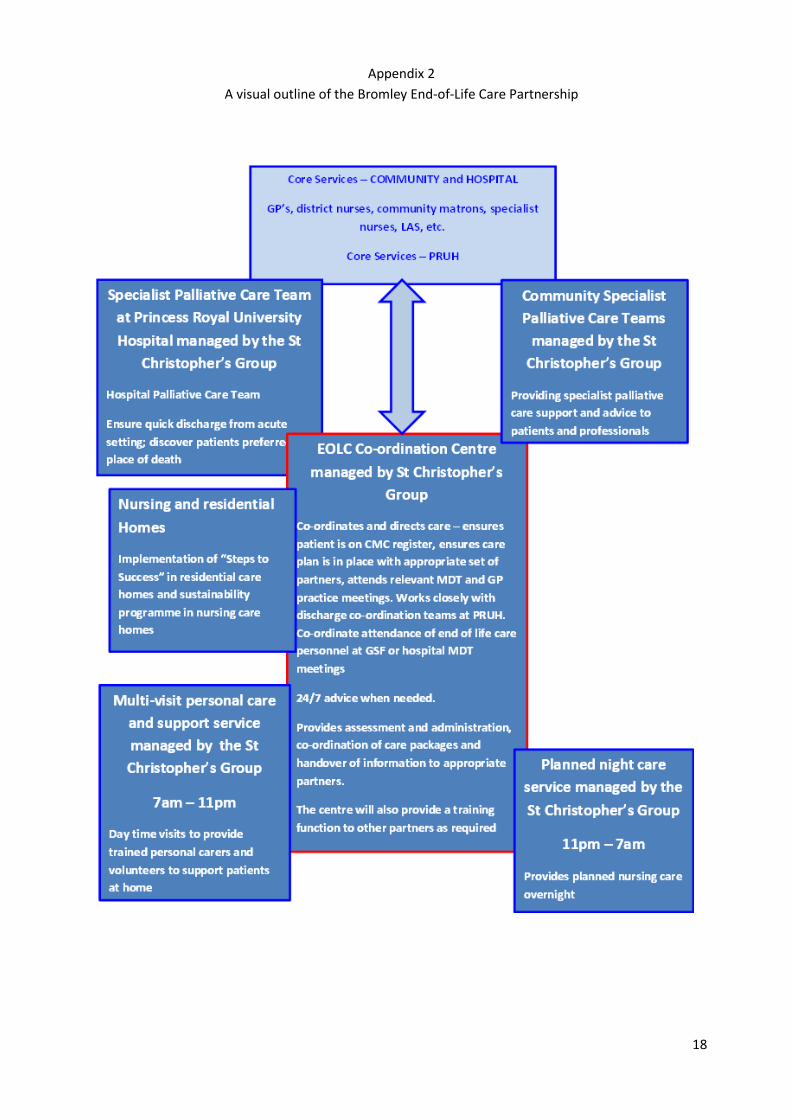
A diagrammatical representation of the new model is shown in Appendix 2
What are the expected outcomes of the new service?
The outcomes of the new service:
1. In the first year of operation the new service is expected to achieve a home death rate of
50% for those who are referred to the co-ordination centre.
2. National data has demonstrated that most people in their last year of life have an average of
3 hospital admissions. This would be monitored with the expectation that in Bromley the

11
average would fall to around 2 admissions or less
3. Validated outcome tools (i.e. SKIPP and VOICES) to monitor satisfaction and impact of the new centre.
There are three areas of impact for SKIPP - a) Quality of Life b) Organisational impact c) Presence or absence of symptoms
VOICES is an assessment of impact of the service as opposed to a specific QOL.
It is anticipated that 75% of patients referred to the centre would rate the difference the
services provided by the centre to have made a positive impact.
4. After accounting for the necessary investment in additional community services, significant
net savings will be made on the hospital commissioning budget. See section 8 below.
** All outcomes will be measured by St Christopher’s Hospice, as part of the monthly contract
management and performance monitoring with Bromley CCG. In addition the outcomes will be
monitored for the next 3 years by the ProMISE Programme team and included within the balanced
scorecard.
8 Financial modelling
Key assumptions
There are four key assumptions that underpin the financial modelling for the business case. These are
as follow;
1. The proposed service aims to reduce the number of people who die in hospital. This is expected
to impact primarily on the number of deaths following a medical emergency admission.
Each year there are approximately 2600 deaths in Bromley, of which 1455 people die in hospital
(56%). This is slightly higher than the national average of 54.5%. (Source “End of Life Intelligence
Network 2012”). However, where care is coordinated by St Christopher’s Hospice, only 20% of their
patients die in hospital. Whilst it is appreciated that the services offered by St Christopher’s Hospice
will not be suitable for all patients, the opportunity exists to enable more people to die in the
surroundings of their choice, which is usually at home or in a community setting.
To assess the potential to reduce the number of people dying in hospital, the business case focuses on
those people whose death only followed an emergency medical admission, to remove trauma and
surgically related admissions that are unlikely to be affected by the proposed service model. Of the
1455 hospital deaths, 1044 of these were medical emergency admissions. St Christopher’s currently
receives around 800 referrals a year for Specialist Palliative Care in Bromley, and only 20% (160) of
“their” patients die in hospital. If we assume all the 160 St Christopher’s Hospice patients are part of
the 1044 deaths following a medical emergency admission, there is a pool of 884 remaining patients
who could benefit from the expanded service.

12
Because of the innovative nature of this proposal, there is no direct evidence on which to assess how
many more people could be cared for outside of hospital if this service was commissioned, although a
roughly similar approach has been developed in Somerset which has achieved a hospital death rate of
only 7%, albeit for a much smaller cohort of patients.
In order to calculate the savings associated with a person’s last hospital admission, the 50th percentile
tariff value has been used. (Appendix 3)
2. It is common for people in their last year of life to make several trips to hospital. It is assumed
that one additional hospital admission will be saved prior to the patient’s last admission.
For each admission when the patient dies, there are typically two previous hospital stays within the
last year of life. An examination the same 1044 cohort of medical patients shows there were a further
2025 inpatient episodes. For the purposes of the model, one additional admission is presumed saved
by the new service. Once again, in order to assess the most likely tariff savings, the 50th percentile
tariff has been used. (Appendix 3)
3. The A & E costs associated with the both admissions will also be avoided.
The model assumes a reduction of two inpatient episodes per patient, described in 1 and 2 above.
Associated with both admissions will be an A & E attendance. Once again the 50th percentile tariff has
been chosen as the most appropriate to calculate the potential savings. (Appendix3)
4. Additional service provision in the community for both social care and nursing
The cost of providing alternative packages of community care for both admissions detailed above will
be funded using some of the savings generated from the acute commission budget. Again, using the
same 50th percentile corresponding to the admissions, the two associated lengths of stays of have
been used to build the community care costs. (Appendix 3)
These patient-specific costs, along with the fixed cost of running the 24hr co-ordination centre
(£243,000) are set against the hospital tariff savings to highlight the affordability of the service model
and scale of financial savings.
The scenarios
As discussed above, given the innovative nature of the project there is little robust information to
quantify the expected reduction in the number of people dying in hospital. Therefore three different
scenarios have been calculated to show the potential range of savings.
Best case
In this scenario it is assumed that Bromley CCG matches the best overall hospital death rate in England
of 42.2% which would require a reduction of 305 admissions, reducing the medical emergencies that
resulted in death from 1044 down to 739.
Worst case
In this scenario, it is assumed that the service has marginal impact, reducing the number of people
dying in hospital by only 52 per year, and reducing the medical emergency admission death rate from
1044 to 992.

13
Most likely
In this scenario the mid-point point between the above two scenarios and assumes a reduction of 179
people dying in hospital and therefore a medical emergency admissions death rate of 865. (1044-179)
The table below calculate the potential savings for each scenario.
Scenario Reduction in emergency admissions @£3,987 LOS 8 days
Reduction in prior admissions @£1716 LOS 2 days
Reduction in A & E attendances @£311
Cost of alternative community care for both stays @£188 per day (LOS 10 days)
Cost of new Centre
Net Savings
Best case 305 305 610 3050 days
£1,216K £523K £189K £573K £243K £1,112K
Worst case 52 52 104 520 days
£207K £89K £32K £98K £243K £9K
Most likely *
179 179 357 1790 days
£714K £307K £111K £337K £243K £552K
*Please note that changes to figures as presented to the Clinical Executive have not been checked by finance,
but relate to a midpoint of best and worst cases, which have been ratified by Finance.
Additional service “in kind” benefits
St Christopher’s is also committed to adding a number of costs ‘in kind’ to the project. The project will
have management support from a Lead Senior Nurse for the first year based at the St Christopher’s
Group, who will provide operational and clinical leadership to the Bromley Care Partnership and will
act as a liaison point between individual organisations on operational issues Services in-kind will also
include a bespoke trained volunteer service to support the Social Care aspect of the project, and
access to the dynamic Social Programme at the Anniversary Centre/Caritas Centre. It is assumed that
this role will no longer be required in following years, as the post will support initial set up in the first
12 months.
St Christopher’s also intends to cover premises and back-office costs for the first year of the project.
Any future costs for these aspects of the service will be renegotiated with the St Christopher’s Group
as part of future planning. However, it is expected that this cost will continued to be funded by St
Christopher’s Hospice.

14
9 Options for the way forward
Option 1 Do nothing
This option is easily discounted as the main quality and financial benefits of this service proposal would not be met
Option 2
Tender for the enhanced specialist services.
Option 3
Negotiate a contract variation with the existing provider/s
Preferred option
A market management and procurement assessment has been completed (appendix 4) suggesting option three is the right approach on the basis that:
The St Christopher’s Group already provides an excellent range of local End of life services in Bromley
The integrated service design has an estimated value of £242,603, approximately 13% of the existing £1.923m contract with St Christopher’s Hospice, Harris Hospiscare and the Care Home Project, including both contracts and CQUINS.
The service design is a reconfiguration of existing services, not a material change to the way in which services are presented to the “user” via pathway redesign or resource change, as supported by the waiver against completion of section 242 (NHS Act of 2006). Only the introduction of an out of hours coordination centre would be an addition to the service provision. (13% of the total contract value).
End of Life care would be more fragmented if another speciality palliative care provider entered the market
There is currently no alternative local, specialist provider with significant experience already established in the area that could provide immediate service provision. St Christopher’s Hospice, LBB Carers and community staff have demonstrable capacity and experience that can be quickly adapted to develop this integrated service approach.
St Christopher’s is already well networked with local providers and agencies to support the integrated approach, with pace and scale
The organisation has a both an intellectual capital and unparalleled experience with specialist end of life care in the Bromley area
80% of bereaved carers (VOICES-hospices survey respondents) consistently say that the care St Christopher’s Group home care patients receive is ‘exceptional’ or excellent’
The 5 CCG Cluster contract with St Christopher’s Hospice expired on 31st March 2013 and is being rebased in year, with the provision of a new 3 year contract to be discussed in September 2013. Bromley is looking to extricate itself from this arrangement with this service enhancement, which further endorses our recommendation for single tender waiver.
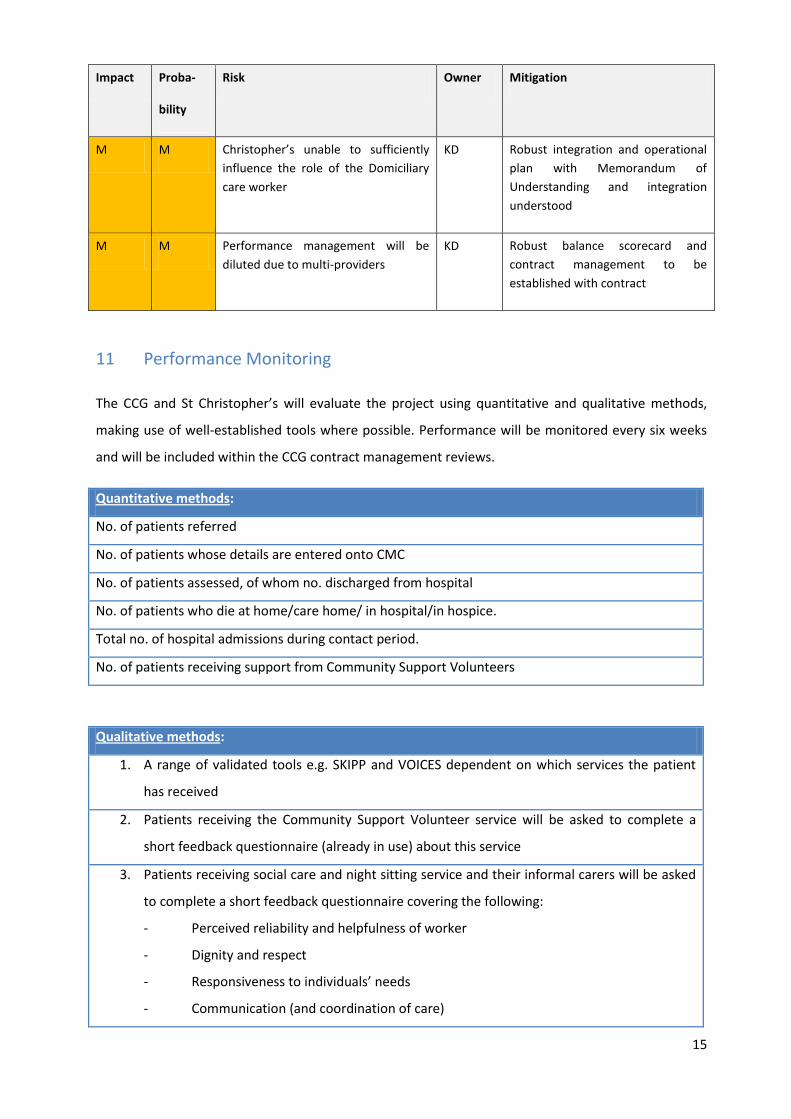
10 Risks
15
Impact Proba-
bility
Risk Owner Mitigation
M M Christopher’s unable to sufficiently
influence the role of the Domiciliary
care worker
KD Robust integration and operational
plan with Memorandum of
Understanding and integration
understood
M M Performance management will be
diluted due to multi-providers
KD Robust balance scorecard and
contract management to be
established with contract
11 Performance Monitoring
The CCG and St Christopher’s will evaluate the project using quantitative and qualitative methods,
making use of well-established tools where possible. Performance will be monitored every six weeks
and will be included within the CCG contract management reviews.
Quantitative methods:
No. of patients referred
No. of patients whose details are entered onto CMC
No. of patients assessed, of whom no. discharged from hospital
No. of patients who die at home/care home/ in hospital/in hospice.
Total no. of hospital admissions during contact period.
No. of patients receiving support from Community Support Volunteers
Qualitative methods:
1. A range of validated tools e.g. SKIPP and VOICES dependent on which services the patient
has received
2. Patients receiving the Community Support Volunteer service will be asked to complete a
short feedback questionnaire (already in use) about this service
3. Patients receiving social care and night sitting service and their informal carers will be asked
to complete a short feedback questionnaire covering the following:
- Perceived reliability and helpfulness of worker
- Dignity and respect
- Responsiveness to individuals’ needs
- Communication (and coordination of care)

16
4. Summary of ad hoc feedback received (compliments/complaints/comments)
17
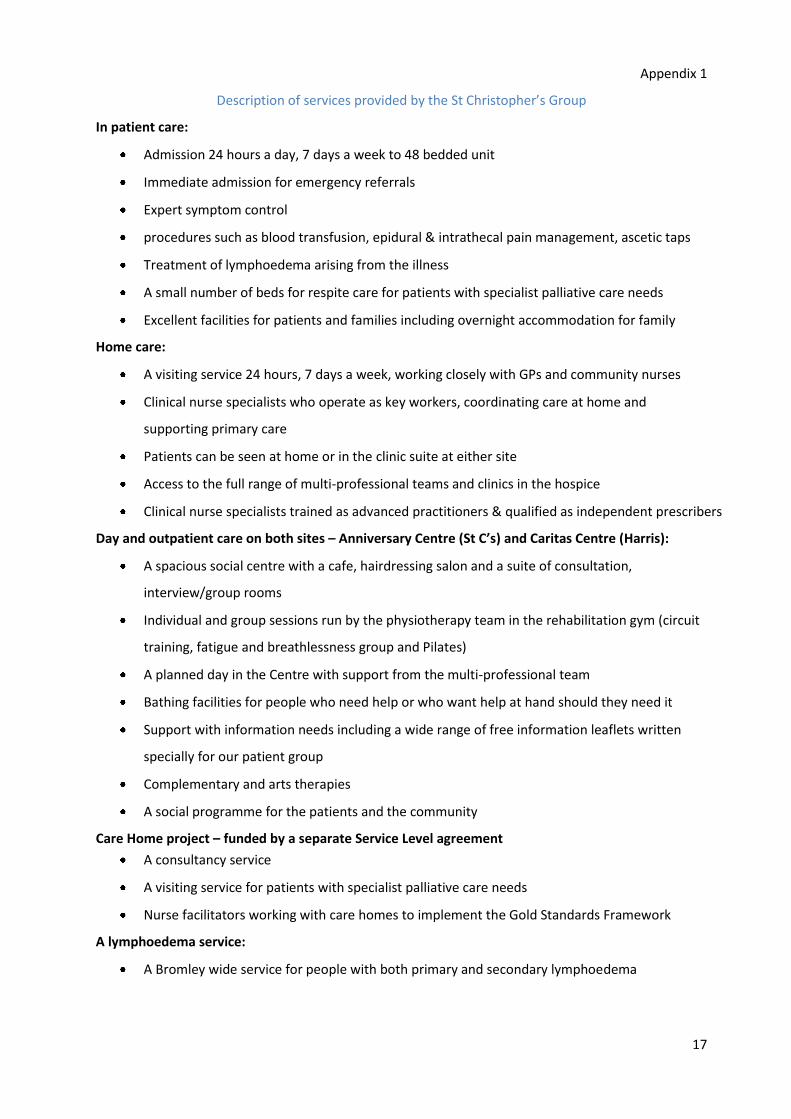
Appendix 1
Description of services provided by the St Christopher’s Group
In patient care:
Admission 24 hours a day, 7 days a week to 48 bedded unit
Immediate admission for emergency referrals
Expert symptom control
procedures such as blood transfusion, epidural & intrathecal pain management, ascetic taps
Treatment of lymphoedema arising from the illness
A small number of beds for respite care for patients with specialist palliative care needs
Excellent facilities for patients and families including overnight accommodation for family
Home care:
A visiting service 24 hours, 7 days a week, working closely with GPs and community nurses
Clinical nurse specialists who operate as key workers, coordinating care at home and
supporting primary care
Patients can be seen at home or in the clinic suite at either site
Access to the full range of multi-professional teams and clinics in the hospice
Clinical nurse specialists trained as advanced practitioners & qualified as independent prescribers
Day and outpatient care on both sites – Anniversary Centre (St C’s) and Caritas Centre (Harris):
A spacious social centre with a cafe, hairdressing salon and a suite of consultation,
interview/group rooms
Individual and group sessions run by the physiotherapy team in the rehabilitation gym (circuit
training, fatigue and breathlessness group and Pilates)
A planned day in the Centre with support from the multi-professional team
Bathing facilities for people who need help or who want help at hand should they need it
Support with information needs including a wide range of free information leaflets written
specially for our patient group
Complementary and arts therapies
A social programme for the patients and the community
Care Home project – funded by a separate Service Level agreement
A consultancy service
A visiting service for patients with specialist palliative care needs
Nurse facilitators working with care homes to implement the Gold Standards Framework
A lymphoedema service:
A Bromley wide service for people with both primary and secondary lymphoedema
18
Appendix 2
A visual outline of the Bromley End-of-Life Care Partnership

19
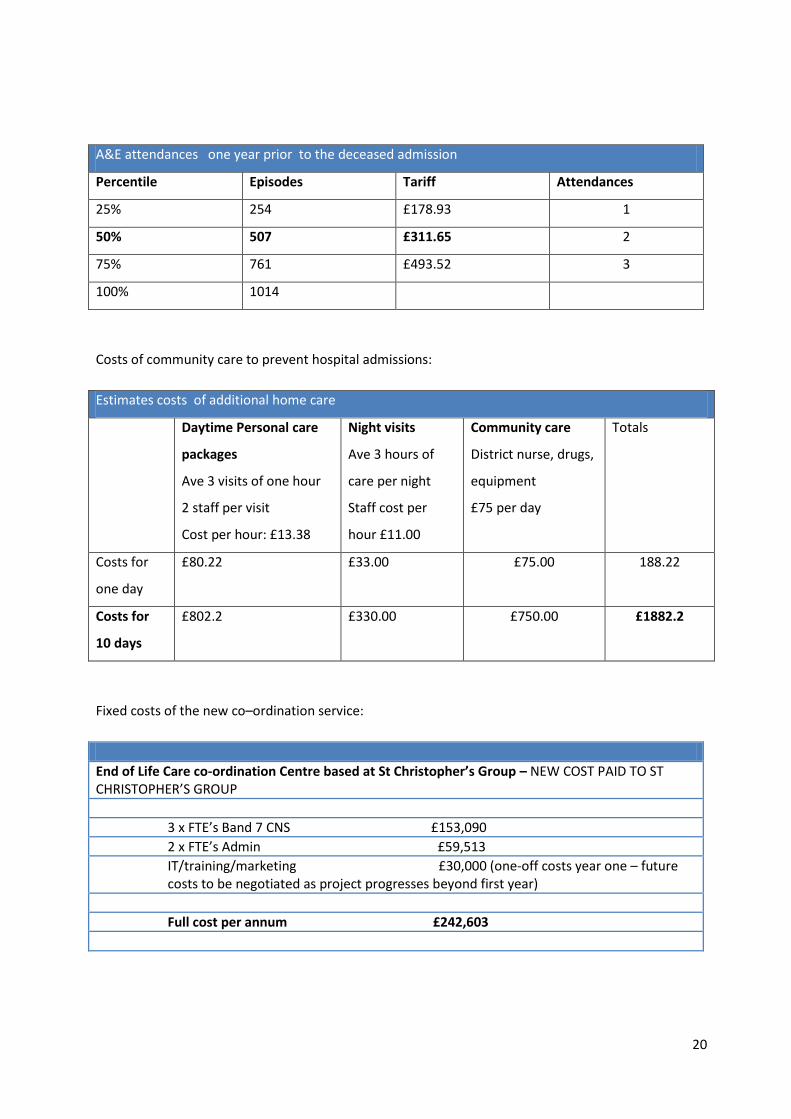
Appendix 3
Costings used in the financial model
Potential saving associated with reducing deaths in hospital
Procedure and Diagnosis driven - medical emergency admissions over 65s
Percentile Episodes Tariff Ave Length of Stay
25% 261 £2874 3
50% 522 £3,987 8
75% 783 £4,940 17
100% 1044 11.8
Procedure driven only - medical emergency admissions over 65s
Percentile Episodes Tariff Ave Length of Stay
25% 56 £2,180 4
50% 112 £5,655 12
75% 168 £7,882 30
100% 224 14.8
Diagnosis driven only - medical emergency admissions over 65s
Percentile Episodes Tariff Ave Length of Stay
25% 205 £3,042 3
50% 410 £3,987 9
75% 615 £4,615 26
100% 820 11
In patient episodes one year prior to the deceased admission
Percentile Episodes Tariff Ave Length of Stay
25% 205 £664 O
50% 410 £1,716 2
75% 615 £3,846 9
100% 2015
20
A&E attendances one year prior to the deceased admission
Percentile Episodes Tariff Attendances
25% 254 £178.93 1
50% 507 £311.65 2
75% 761 £493.52 3
100% 1014
Costs of community care to prevent hospital admissions:
Estimates costs of additional home care
Daytime Personal care
packages
Ave 3 visits of one hour
2 staff per visit
Cost per hour: £13.38
Night visits
Ave 3 hours of
care per night
Staff cost per
hour £11.00
Community care
District nurse, drugs,
equipment
£75 per day
Totals
Costs for
one day
£80.22 £33.00 £75.00 188.22
Costs for
10 days
£802.2 £330.00 £750.00 £1882.2
Fixed costs of the new co–ordination service:
End of Life Care co-ordination Centre based at St Christopher’s Group – NEW COST PAID TO ST CHRISTOPHER’S GROUP
3 x FTE’s Band 7 CNS £153,090
2 x FTE’s Admin £59,513
IT/training/marketing £30,000 (one-off costs year one – future costs to be negotiated as project progresses beyond first year)
Full cost per annum £242,603

21
Appendix 4
Market Management, Redesign and Procurement Assessment Tool
Disease Group End of Life Care
Disease Sub-group Cancer, COPD, Heart Failure etc
Prepared by Chris Evennett/Kate Dawes
Date 15th
May 2013
Assessment (see guidance notes for further explanation of the assessment questions)
Criteria Assessment question Answer Justification
Quality Is it a quality service
currently?
Yes. The service offered by St Christopher’s Hospice is well respected and performs well in patient surveys, particularly when
compared with the provision of end of life care provided by exiting providers.
Establishing another specialist end of life service would make it more complicated to integrate care between the various
agencies, particularly as the business model emphasis the need for better coordination of care
Availability Are there other
providers in the market?
No There are no other local providers of specialist end of life care. The service model dictates that the specialist provider must
be locally based to establish the seamless communication networks
Capacity Is additional capacity of
sufficient quality
required?
No Only a limited amount of additional community care capacity will be spot purchased to enable more people die in their
own homes.
Commerciality Is the contract
commercially sound?
The contract would benefit from more specific KPIs to ensure that more people died in the setting of their choice.
Next steps proposed:
It is proposed to negotiate a contract extension with St Christopher’s Hospice to deliver this enhanced service. (Scenario 6)
Scenario 1 Scenario 2 Scenario 3 Scenario 4 Scenario 5 Scenario 6 Assessment Criteria Scenario 7 Scenario 8 Scenario 9 Scenario 10
Yes Yes Yes Yes Yes Yes QUALITY No No No No
Yes Yes Yes No No No AVAILABILITY Yes Yes No No
Yes No No Yes No No CAPACITY Yes No Yes No
Yes No Yes No COMMERCIALITY
Tender Monitor
Engage /
Renegotiate
Stimulate /
Tender Monitor
Engage /
Renegotiate OUTCOME Tender Redesign
Redesign /
Stimulate Redesign
Outcomes Description
Tender Reprocure service
Monitor Ongoing contract monitoring
Engage/
Renegotiate
Engage with existing provider /
renegotiate contract
Stimulate
Stimulate existing provider and
market
Redesign
Redesign of clinical pathway /
service delivery
22
Appendix 5

End of Life Business Case Procurement Paper
Purpose of the Paper The purpose of this paper is set out the rationale for seeking a single tender waiver for procurement of an End of Life service within Bromley, contrary to NHS England Procurement route of open tender. Existing provision Presently End of Life services are provided routinely by various agencies; notably domiciliary carers via London Borough of Bromley Social Services, St Christopher’s Hospice and Harris Hospiscare providing in-patient care, home care and a range of outpatient and day care services, Community services provided by Bromley Healthcare. The current annual Bromley CCG investment in specialist end of life services is detailed below:
St Christopher’s Hospice Contract £1,198,684 CQUINS £17,496
Harris Hospiscare with St Christopher’s Contract £714,097 CQUINS £10,711
Care Home project – funded by a separate Service Level agreement Contract £59,388 per year
It should be noted that the payment from the CCG covers between one-third to one-half of the actual annual cost of the services provided to Bromley residents by the St Christopher’s Group. The remaining cost of the service is currently covered by the London Borough of Bromley within the Social Care budget. Rationale for the waiver
The St Christopher’s Group already provides an excellent range of local End of life services in Bromley
The integrated service design proposed has an estimated additional value of £242,603, equating to approximately 13% of the existing combined £1.923m contract with St Christopher’s Hospice, Harris Hospiscare and the Care Home Project, including both contracts and CQUINS.
The service design is a reconfiguration of existing services, not a material change to the way in which services are presented to the “user” via pathway redesign or resource change, as supported by the waiver against completion of section 242 (NHS Act of 2006).

The costings for the care coordination centre demonstrates value for money, comparable with that of the Croydon service and charges the CCG for only the cost of the day service provision (including staff costs, IT training and marketing) with the out of hours service subsumed by St Christopher’s and Partners.
Significant patient and carer participation has contributed to the development of this model, as identified in Section 6 of the Full Business Case)
End of Life Care would be more fragmented if another speciality palliative care provider entered the market
There is currently no alternative local, specialist provider with significant experience already established in the area that could provide immediate service provision. St Christopher’s Hospice, LBB Carers and community staff have demonstrable capacity and experience that can be quickly adapted to develop this integrated service approach.
St Christopher’s is already well networked with local providers and agencies to support the integrated approach, with pace and scale
The organisation has both an intellectual capital and unparalleled experience with specialist end of life care in the Bromley area
80% of bereaved carers (VOICES-hospices survey respondents) consistently say that the care St Christopher’s Group home care patients receive is ‘exceptional’ or excellent’
The 5 CCG Cluster contract with St Christopher’s Hospice expired on 31st March 2013 and is being rebased in year, with the provision of a new 3 year contract to be discussed in September 2013.
Recommendation It is recommended that there is sufficient mandate for single tender waiver, as identified by local procurement resources, in accordance with the Bromley Procurement Policy and that of NHS England (formerly NHS Commissioning Board) http://www.england.nhs.uk/wp-content/uploads/2012/09/procure-brief-5.pdf