NHS Lewisham CCG Annual Report 2017/18€¦ · NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18...
175
Page 1 NHS Lewisham CCG Annual Report 2017/18
Transcript of NHS Lewisham CCG Annual Report 2017/18€¦ · NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18...
Page 1
NHS Lewisham CCG
Annual Report 2017/18

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 2
Contents
PERFORMANCE REPORT ............................................................................................... 3
Performance Overview ............................................................................................... 4
Performance analysis ............................................................................................... 17
ACCOUNTABILITY REPORT .................................................................................. 76
Corporate Governance Report ................................................................................. 77
Members Report ................................................................................................. 77
Statement of Accountable Officer’s Responsibilities ........................................... 82
Governance Statement ....................................................................................... 85
Remuneration and Staff Report .............................................................................. 129
Remuneration Report ....................................................................................... 129
Staff Report ...................................................................................................... 137
Parliamentary Accountability and Audit Report ..................................................... .143
ANNUAL ACCOUNTS ........................................................................................... 144

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 3
PERFORMANCE REPORT
Andrew Bland
Accountable Officer
25th May 2018

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 4
Performance Overview Welcome
I am pleased to present our annual report and accounts for 2017/18. In this report, we describe
how we have fulfilled our duties as laid down in the National Health Service Act 2006 and the
work we are doing to improve the health and care of people who live in Lewisham.
One of the biggest challenges that we - in conjunction with Lewisham and Greenwich Trust -
have faced over a number of years has been to improve and sustain access, within national
standards, to high performing local urgent and emergency care services, in particular
performance against the 95% Accident & Emergency 4 hour standard. In order to support the
CCG in bringing about speedy and stretching improved performance, NHS England used their
formal powers of direction. From 1st September 2017 some of our responsibilities for acute
commissioning and contracting have been temporarily transferred to Southwark Clinical
Commissioning Group (CCG). This has helped to galvanise the urgent and emergency care
system to keep a sharp focus on improving clinical safety and quality, improve year on year
performance and be relatively well prepared for one of the most challenging winters for
emergency care.
During 2017/18 we have also been working jointly within the Lewisham Health and Care
Partners programme on the integration of local services to support our vision for community
based care, and have presented our plans and progress to the Lewisham Health and
Wellbeing Board.
Along with the other CCGs in south east London, we carried out a comprehensive review of
our collaborative working arrangements. This has resulted in the establishment of new
executive leadership arrangements that will take effect from 1st April 2018. They include a
single Accountable Officer and single Chief Finance Officer for Lewisham, Bexley, Bromley,
Greenwich and Southwark CCGs who will both be members of our Governing Body along with
the new post of Lewisham CCG Managing Director. Other shared executive posts include two
directors of finance (one appointed jointly between Lewisham CCG and Greenwich CCG), and
further posts working across all of the south east London CCGs for financial strategy, contract
delivery, commissioning operations, contract delivery, and for the Sustainability and
Transformation Partnership (STP) programme.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 5
We have carried out public consultations on proposed changes to services: on prescribing
guidelines for over the counter medicines and on prescribing of anti-malarial medicines, and on
primary care access and the closure the New Cross Walk-in Centre. We are grateful for the
high levels of participation in these consultations from our local population and service users,
elected representatives, and community and voluntary groups, where we received over 2,000
survey responses as well as attendance at more than 70 events and activities. We have
responded to the concerns that were raised during these consultations by raising awareness
about self-care and malarial prevention as a result of the prescribing changes, and following
the consultation on primary care access and the closure the New Cross Walk-in Centre we
have promoted the GP extended access service and are piloting alternative provision of
primary care services for homeless people.
Throughout the year we have tracked our performance against the NHS Constitutional
Standards and the areas covered in the Improvement and Assessment Framework (IAF) for
CCGs and where necessary put in place actions for improvement. The IAF ratings have shown
that our diabetes care and dementia care are outstanding, while mental health has been rated
as good. Despite some improvement we have continued to experience particular challenges to
meet the Accident and Emergency 4 hour target, and we will continue our efforts so that with
the recovery plans that have been put in place since the application of legal directions we will
achieve further improvement during 2018/19. We are also working with our partners in south
east London to implement an improvement plan for cancer services, where we are not yet
meeting the 62 day standard for referral to treatment. Our efforts in the year have led to the
opening of the GP extended access service, and in mental health provision continuing
improvement in Improving Access to Psychological Therapies (IAPT), Early Intervention in
Psychosis (EIP) and mental health for children.
From April 2017 under delegated commissioning arrangements we assumed full responsibility
for contractual GP performance management, budget management and the design and
implementation of local incentive schemes.
We have met all of our statutory financial duties, as well as delivering a 2.4% cumulative
surplus and ensured compliance with prompt invoice payment requirements against the Better
Practice Payments Code (BPPC).
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 6
I would like to thank our member practices and all of Lewisham’s NHS and care staff, for the
work they do to treat, care for and support local people. I continue to value comments from
local people to help shape and improve local services as we take steps to ensure that services
are proactive and preventative, accessible and co-ordinated. We will continue to strive to
engage with and meet the needs of Lewisham’s diverse population and communities.
This Performance Overview and the sections of the Annual Report and Accounts that follow
provide more details on all of these areas and on the effective governance of NHS Lewisham
CCG. We have in place robust governance and management structures, and the plans to meet
the challenges for the future.
Andrew Bland
Accountable Officer 25th May 2018

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 7
1. IntroductionNHS Lewisham Clinical Commissioning Group (CCG) is a membership organisation made up
of all the GP practices in Lewisham. Our aim is to secure the best possible health and care
services for everybody in Lewisham, to reduce health inequalities and improve health
outcomes in a cost effective way that provides good value for money.
We use what we know about the health needs of our residents to plan how and where to
provide care which we commission from hospitals, community services, GPs and other
providers of care. This information comes from insight and feedback from our public
engagement activities, from our colleagues in the Lewisham Public Health team and from
national sources such as Public Health England and the Health and Care Information Centre
and is summarised in Lewisham’s Joint Strategic Needs Assessment. You can find out more
about the Joint Strategic Needs Assessment at http://www.lewishamjsna.org.uk/
We plan, buy and monitor most of the health services our residents use including:
• Community health services (such as district nursing)
• General practice
• Hospital care
• Rehabilitation services (such as physiotherapy)
• Urgent and emergency care
• Mental health care (both hospital and community based services)
• Services to support the most dependent people in the community.
We aim to improve care by:
• Ensuring services in Lewisham are of a high quality, safe and easily accessible and
appropriate for the range of diverse communities living in Lewisham
• Working closely with our local community to plan and improve services
• Having a good working relationship with the staff and organisations who deliver care
and other organisations responsible for local services.
• Making the most effective use of the money we have been allocated to commission
services.
Other health services such as pharmacies, opticians, dentists and some specialist health
services are commissioned by NHS England. Visit www.england.nhs.uk for more information.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 8
Decisions about what we do are made by our Governing Body, which is accountable to our
member practices and which meets in public on a regular basis. You can find out who is on our
Governing Body and the dates of forthcoming meetings on our website
2. Health in Lewisham
Demographics
Lewisham is part of London, the
largest, most culturally diverse city in
Europe. Lewisham covers an area of
13.4 square miles stretching from the
Thames at its most northerly point to
Bromley in the south of London.
Lewisham has a growing population,
projected to increase from 306,000 in
2017 to 323,000 by 2021, and is the
15th most ethnically diverse local
authority in England, 46% of the
population are from black, asian and ethnic minority groups and around 65% between the ages
of 0 to 19. Around 28,800 residents are above 65 years of age and approximately 4,000 are
aged over 85 years. This latter group often has the most complex health needs and therefore
bears a very high proportion of care costs.
The Index of Multiple Deprivation 2015 ranks Lewisham 48th of 326 districts in England and
10th out of 33 London boroughs. People living in the most deprived areas have poorer health
outcomes and lower life expectancy compared to the England average: life expectancy for men
is five years longer in Crofton Park, than in New Cross. For women the life expectancy gap is
even bigger at 8.5 years, between the Perry Vale and Crofton Park wards where life
expectancy is longest, and New Cross where it is lowest.
Lewisham has over 800 active voluntary and community sector organisations and more than
200 individual faith groups. All these groups and many others help to strengthen our
communities by galvanising our citizens, addressing local concerns and advocating on behalf
of some of the most vulnerable in society.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 9
There have been some improvements in
people’s health and care in Lewisham. The
life expectancy at birth was 78.8 years for
women and 72.3 years for men in 1992-94
while in 2014-16 it had increased to 83.3
years and 79.1 years respectively; people in
Lewisham are living longer because of the
success in managing particular conditions
such as stroke, heart disease and
respiratory disease. More people in contact
with mental health services in Lewisham are
living independently with or without support
in comparison to the national average.
Local Challenges
Every year demand on our services continues to grow while the money allocated to us is
increasing more slowly than demand is. We describe in more detail the challenges we are
facing in our section below on the NHS Constitutional Standards, particularly for Cancer and
Accident and Emergency (A&E) national targets. The current system is not sustainable and our
population is not achieving the health and care outcomes they should, as demonstrated below:
• While life expectancy has been improving, for men at 79.1 years life expectancy at birth
remains lower than the England average which is 79.5 years
• Many of these deaths are avoidable, around two thirds of deaths among the under 75s.
These deaths could be avoided through public health interventions such as getting
people to take more exercise or to stop smoking, by tackling the wider social
determinants of health (what is termed preventable mortality), or through health care
interventions such as early diagnosis of diseases or conditions and through effective
treatment (amenable mortality). (from ‘Living Well for Longer: a call to action to reduce avoidable
premature mortality’, Department of Health 2013)
• Cancer is now the main cause of death (28%), followed by circulatory disease (21%)
and respiratory disease (16%) in Lewisham

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 10
• Screening for bowel, breast and cervical cancer is significantly lower than the average
for England
Demand for care is increasing, both in numbers and complexity:
• 14% of people in Lewisham identify themselves as having limitations in carrying out
day-to-day activities. That is equivalent to around 38,000 people.
• Lewisham’s over 60s population is projected to have risen from 39,000 in 2016 to
44,000 in 2021 which will increase demand for the health and care services
More information is available about Lewisham’s population at www.lewishamjsna.org.uk
We need to change how we do things to meet these challenges. We want to work with our
residents to do this; however, there will be difficult decisions to be made.
3. Performance Overview
Our aim is to meet the health needs of the people living in Lewisham in the best possible way
with the money available, while addressing significant challenges of the population. Our
performance is discussed in more detail in the next section.
The NHS Constitutional standards provide performance measures over a range of key areas.
Some of the improvements we have achieved include ambulance response times, cancer two
week waits, diagnostics within six weeks, recovery rates for Improving Access to Psychological
Therapies (IAPT), waiting times for Early Intervention in Psychosis and for urgent eating
disorders for children, and the accident and emergency four hour waiting time, though it is still
less than the 95% standard. We continue to face challenges to meet the standards for the GP
referral to treatment for cancer within 62 days, 18 weeks for referral to treatment.
Against the NHS England Improvement and Assessment Framework (IAF) In 2017/18 we have
been assessed for the following Clinical Priorities:
• Diabetes Care: Outstanding
• Dementia Care: Outstanding
• Mental Health: Good

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 11
We are awaiting other clinical priorities scores for three other Clinical Priorities including
Cancer Care.
All CCG Improvement and Assurance Framework indicators can be found at My NHS on NHS
Choices. The following link takes you direct to the My NHS page for NHS Lewisham CCG here
Some of our other achievements for primary care in particular include:
• Co-ordinated care for 300 frequently admitted patients resulted in fewer admissions -
50% reduction
• Co-ordinated care for 300 frequent A&E attenders resulted in A&E attendance
reduced by 69%
• Improved immunisation of vulnerable adults and children in particular
• Lewisham CCG now has the highest vaccination rate in London for pneumococcal
vaccination of over 65s.
• Hypertension control has been improved across the borough by 4% (overall
improvement and reduced variation)
• 25% of newly diagnosed people with COPD stopped smoking (target was 15%)
twice the expected number of people were diagnosed with COPD (+268) and
hypertension (+1179)
• 593 new diabetes diagnoses equalled the predicted number, this means improved early
detection, treatment and improvement for people with these long term conditions.
• Online patient access, Lewisham is highest in London for registering patients online,
with benefits of access and flexibility for patients for not just appointments but for
prescriptions and queries
• Our rate for e-referrals (an electronic booking service for clinic and hospital
appointments) is 50%, the best in London, improving efficiency of referrals
• The Care Quality Commission ratings of our general practices were an indication of the
quality of primary care. Only three practices were rated overall as “Requires
Improvement,” one was rated “Outstanding” and all the rest were “Good.”
4. Financial Targets & Performance
Sound financial management and robust management of financial risks have ensured that we
have achieved all of our statutory financial duties for 2017/18, as planned. In accordance with

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 12
NHS England planning guidance, we are required to deliver a cumulative surplus of at least 1%
of available resources. CCGs must contain net expenditure within resource allocation limits set
by NHS England for the year. There are separate resource allocation limits for capital and
revenue expenditure, with revenue expenditure limits further split between programme spend
and running costs.
The CCG is required to comply with the statutory duties set out under a direction issued by the
NHS Commissioning Board (NHS England) under the National Health Service Act 2006 (as
amended). Also, the CCG is required to prepare Annual Accounts in accordance with the
Government Financial Reporting Manual taking account of the application guidance contained
in the Department of Health and Social Care Group Accounting Manual.
Our annual accounts for 2017/18 have been prepared on a going concern basis. Public sector
bodies are assumed to be going concerns where the continuation of the provision of a service
in the future is anticipated, as evidenced by inclusion of financial provision for that service in
published documents. Where a clinical commissioning group ceases to exist, it considers
whether or not its services will continue to be provided (using the same assets, by another
public sector entity) in determining whether to use the concept of going concern. If services will
continue to be provided the financial statements are prepared on the going concern basis.
The CCG has been notified of its resource allocation for 2018/19 and has agreed contracts in
place with its main providers. During the year the Governing Body has considered and
approved a number of documents that assume that services will be provided on an on-going
basis; including an operational plan with two year financial plan for 2017/18 to 2018/19 and
signed two year contracts with NHS providers for 217/18 to 2018/19. From April 2017 NHS
Lewisham CCG assumed full responsibility for contractual GP performance management,
budget management and the design and implementation of local incentive schemes under
delegated commissioning arrangements approved by NHS England.
5. Collaborative Working
We have been working with our local partners in
Lewisham’s Health and Care Partners (LHCP) to
plan and deliver care in a more accessible, co-
ordinated and sustainable way. The partners are

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 13
Lewisham CCG, London Borough of Lewisham, Lewisham & Greenwich NHS Trust, South
London and Maudsley NHS Foundation Trust (SLaM), and One Health Lewisham (GP
Federation).
The LHCP is committed to develop and deliver community based care which is:
• Population based
• Expands and strengthens primary and community care
• Promotes health and wellbeing
• Provides a co-ordinated response to the specific needs of the individual
• Works in partnership with patients, service users, carers and wider communities
• Takes a whole system approach
• Evidence based and outcome focused
The partnership work to take forward the strategic commissioning work has included
developing an outcomes framework, joint governance arrangements, a commissioners’
workforce strategy, joint plans for public engagement and commissioning intentions for ‘frailty’
and transition between children’s and adults’ services. These will be areas that are further
developed during 2018/19.
We also work in partnership with other CCGs and NHS provider organisations as well local
authorities, patients and the public in south east London’s Sustainability and Transformation
Partnership (STP), Our Healthier South East London (OHSEL). The next section of the report
covers further detail on the programme and its priorities, as well as highlights covering public
engagement, access to GPs, GP recruitment, cancer diagnosis, mental health services,
digitalisation of GP records, and the NHS 111 service.
We have also continued to work within the Healthy London Partnership (HLP), along with all
London CCGs, NHS England, London councils, the Greater London Authority, the Mayor of
London, Public Health England, and Health Education England. One of the particular highlights
of this partnership working was signing of the London Health and Care Devolution
Memorandum of Understanding in November 2017 by the Mayor of London, Secretary of State
for Health and Social Care Jeremy Hunt, London Councils and NHS, Public Health and wider
health and care leaders which will enable faster improvements to the way health and care
services are delivered. Other areas of work have covered urgent and emergency care

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 14
improvement, mental health and wellbeing, childhood obesity, access to healthcare for people
who are homeless, and HIV infection. Again, more detail on this work can be found in the next
section.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 15
Glossary
A&E Accident and Emergency BAF Board Assurance Framework BCF Better Care Fund BME Black and Minority Ethnic BAME Black, Asian and Minority Ethnic BPPC Better practice payments Code CAMHS Child and Adolescent Mental Health Services CBC Community Based Care CCG Clinical Commissioning Group CCNT Community Childrens Nursing Team COPD Chronic Obstructive Pulmonary Disease CQC Care Quality Commission CQUINS Commissioning for Quality and Innovation Schemes CQRG Clinical Quality Review Group CSU Commissioning Support Unit DNA Did Not Attend D2A Discharge to Assess ED Emergency Department EDS Equality Delivery System EIA Equality Impact Assessment EIP Early Intervention in Psychosis ENT Ear, Nose and Throat EPRR Emergency Preparedness Resilience and Response FCEA Financial Control Environment Assessment H@H Hospital at Home HIV Human Immunodeficiency Virus HLP Healthy London Partnership HRG Health Resource Group IAF Improvement and Assessment Framework IAPT Improving Access to Psychological Therapies (Programme) IGC Integrated Governance Committee JHOSC Joint Health Overview and Scrutiny JSNA Joint Strategic Needs Assessment KPI Key Performance Indicator LGT Lewisham and Greenwich NHS Trust LHCP Lewisham Health & Care Partners LIMOS Lewisham Integrated Medicines Optimisation Service LNPCIS Lewisham Neighbourhood Primary Care Improvement Scheme LSMS Local Security Management Specialist MESCH Maternal Early Childhood Sustained Home Visiting NCT Neighbourhood Community Teams NELCSU North East London Commissioning Support Unit NHSE NHS England NCN Neighbourhood Care Networks NICE National Institute for Health and Care Excellence NPSA National Patient Safety Agency OHSEL Our Healthier SE London

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 16
PCT Primary Care Trust PEEF Public Engagement and Equalities Forum PHSO Public Health Service Ombudsman PI Performance Indicator PMS Personal Medical Services PPG Patient Participation Group PRG Public Reference Group PSED Public Sector Equality Duty QA Quality Assurance QIPP Quality Innovation Productivity and Prevention RSS Referral Support Service SCAIT Social Care Advice & Information team SDMP Sustainable Development Management Plan SELDOC South East London Doctors on Call SIRO Senior Information Responsible Officer SLaM South London and Maudsley NHS Foundation Trust SNNT Special Needs Nursing Team STP Sustainability and Transformation Plan/Partnership UCC Urgent Care Centre UHL University Hospital Lewisham VSM Very Senior Managers VTS Vocational Training Scheme WRES NHS Workforce Race Equality Standard YTD Year to Date

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 17
Performance analysis 1. Introduction
This section describes how we measure our performance and fulfil our duties to improve the quality of services that we commission.
In 2017, the Governing Body agreed the CCG’s corporate objectives for 2017/18, which
identify specific commissioning areas of focus to deliver the CCG’s operational plan. This
approach enables the CCG to gain the greatest impact in improving the three strategic
domains of Better Health, Best Care and Best Value for Lewisham people, whilst delivering a
Quality, Innovation, Productivity and Prevention (QIPP) Programme of over £14million over the
financial year. The QIPP framework is about making health services more cost-effective while
improving the quality of services through innovation.
The corporate objectives for 2017/18 focused on the following three commissioning areas:
• Planned care (including prevention and early action)
• Urgent and emergency care
• Contract management
2. Improving Quality: Planned Care
The planned care objective covers our work to support people with long term conditions better
with proactive, holistic care which improves the quality of their lives, is provided ‘out of hospital’
and reduces the requirement for hospital based outpatient attendances and inpatient
admissions. There are a number of actions which we have taken to meet the planned care
objective.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 18
Improving the quality of care for patients with long term conditions including COPD, asthma and diabetes
In 2017/18 we started aligning contractual and financial incentives for improving quality of life
and quality of care on long term conditions across secondary, primary and community care.
For diabetes the aims were:
• Proactive and community based care
• Accessible services
• Coordinated and personalised care
We are part of the National Treatment and Care Programme to improve the three treatment
targets of blood sugar and cholesterol levels and blood pressure by increasing access to
structured education.
We commissioned both Lewisham & Greenwich NHS Trust (LGT) and the GP Federation (One
Health Lewisham) to work together on developing criteria and protocols to enable more
patients to be cared for in the community supported by a multi-disciplinary team (MDT)
working, virtual clinics, and specialist training for the workforce underpinned by self-
management from Cambridge Diabetes Education Programme.
To date this work across primary care is showing significant improvement in attainment of the
three treatment targets, from 35.8% to 41.6% of the diabetes population. We received a rating
of Outstanding nationally on the Improvement Assessment Framework (IAF) for diabetes care,
an improvement on our previous rating that was Requires Improvement.
We also commissioned specialists to support patients with Chronic Obstructive Pulmonary
Disease (COPD) and other breathing problems. These roles comprise of Community
Respiratory Nurse Consultant and Spirometry Technician. The Community Respiratory Nurse
Consultant is available to support and provide education sessions to practices and the
management of patients who regularly struggle with managing their COPD and attend
A&E. The Spirometry Technician provides education sessions to Practice Nurses and
undertakes spirometry testing in order to ensure a correct diagnosis.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 19
Enhancing the range of self-care information, advice and care to support people with long term conditions
We commissioned two structured education programmes from LGT for those living with
diabetes: the Dose Adjustment For Normal Eating programme known as ‘DAFNE’ for Type 1,
and the Diabetes Education and Self-Management for Ongoing and Newly Diagnosed
programme known as ‘DESMOND’ for Type 2 diabetes.
Case Study – Diabetes Support
Anne McBride, Diabetes peer support group facilitator
Anne McBride is one of four Diabetes peer support facilitators in Lewisham, she covers the Blackheath, Lee Green, Lewisham Central, Ladywell, Rushey Green area.
Anne was appointed in September 2017, she said: “I’ve always been interested in health as my mum has Type 2 Diabetes as well as a number of health problems. After becoming a mum myself, my own health became a concern and I wanted to take control, this is when my health journey began. I found ways to manage my condition through exercise and eating well. I’ve become really passionate about healthy living and this role allows me to share this enthusiasm with others. I’m really enjoying being a diabetes peer facilitator; I love being out and about and meeting new people. It’s early days, and I have already recruited four participants, we’ve had a couple of meetings and a group walk and I’m developing some great networks across the borough which are proving to be wonderful opportunities for my participants. We’ve got cooking classes, yoga classes and shopping tours in the pipeline as well as guest speakers talking about mental health, who knows what we’ll do next?”
Rosemary Squires, Diabetes peer support group participant
Rosemary lives in Lewisham and is one of the diabetes peer support group participants, she said: “My sister saw the group advertised and recommended I sign up as I have been living with diabetes for the last five years. I’m so pleased I found them! I really enjoyed the walk, it’s been such fun, I’ve found new friends and I’m learning about new ways to keep healthy and eat well. Anne and the others are really friendly and supportive; I’m really looking forward to the eating healthy workshop.”
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 20
We also commissioned GPs and practice nurses to refer newly diagnosed Chronic Obstructive
Pulmonary Disease (COPD) patients and patients with other breathing problems onto the Lung
Exercise Education Programme (LEEP). This is a 6 week programme of exercises, based at
three sites across Lewisham. This programme is tailored to meet individual needs and
provides education on how patients can manage their own condition.
We commissioned Healthwatch Lewisham and Bromley / Community Waves to deliver a
programme of Diabetes Peer Support Groups across Lewisham. Community Waves
implemented a programme of recruitment and training to support the engagement and
involvement of adults, their families and carers from a range underrepresented communities
living with Type 2 diabetes. There are four Diabetes Peer Support Groups, based in each
neighbourhood. The Diabetes Peer Support work launched during Diabetes Awareness Week
(Sunday 11th to Saturday 17th June). A number of training sessions have taken place
involving community participation and engagement. In addition, a further training session
focused on healthy eating and tools for making healthier and informed choices.
Improving outcomes for people with cancer by improving early diagnosis and urgent referrals for specialist advice
Our quality assurance work with local hospitals has shown that some patients with suspected
cancers have not been started on treatments within the expected timeframes. Whilst we have
been assured that delays to starting treatment have not caused additional harm to patients we
have been concerned about the poor patient experience and the distress that delays can
cause. In 2017 we developed plans to achieve sustained delivery of the cancer standards and
the recommendations of the national cancer strategy. We have closely monitored the
performance at our local hospitals in meeting the various waiting time standards, including two
week urgent referrals to a specialist, 31 days from diagnosis, and 62 days from referral to first
treatment. The latest data for the 62 days for referral standard shows that we are meeting the
target for the most recent period but the year to date figures are below the 85% required and
are worse compared to 2016/17. More on our performance against these standards is covered
in section 5 below.
One of the agreed priority areas was to improve earlier diagnosis. This has been approached
in three ways. Firstly, by improving public awareness though work with Cancer Research UK
(CRUK) and the Be Clear on Cancer Campaign. Secondly, by improving uptake of the three

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 21
screening programmes, and thirdly by education of primary care teams about the main causes
of cancer mortality locally and about ways to improve screening uptake.
We are working towards increasing cancer awareness. This year we were supported by CRUK
who held Cancer Awareness Events in local community groups. It is hoped that this will
improve the poorer outcomes that some residents currently experience through prevention,
and earlier diagnosis for instance by participating in screening programmes.
Education has also been addressed in several ways. Our local CRUK facilitators have
visited more than half the practices in Lewisham to deliver Screening Awareness Training to
reception staff and there have been two Cancer Educational Events for primary care and social
care staff in the past 12 months. We have also developed a Cancer Newsletter that has been
sent out on a quarterly basis to primary care teams highlighting local pathways and cancer
resources.
As Lewisham has a high 2 Week Wait (2WW) referral rate, work has been done on improving
the use of the pathway through work with LGT. There has been the introduction of an
electronic referral system and alternative ways of getting information and advice have been
highlighted to practice teams.
There has been effective joint working with local partners including Public Health Lewisham,
Macmillan Cancer Support and Cancer Research UK. We are working with our neighbouring
CCGs through Our Healthier South East London and the South East London Cancer
Alliance which brings together primary care, commissioners, hospital trusts, cancer charities,
patients and carers from south east London to improve cancer treatment. Funding was
secured to appoint a Macmillan Cancer GP Cancer Lead in each borough.
Improving patient safety and the patient experience by more joined-up multi-disciplinary working for people with long term conditions
This involves improving GPs’ care for people with long terms conditions through consistent
systematic identification of patients at risk (‘risk stratification’), better multidisciplinary working
at a neighbourhood level, enhanced mental health support from South London and Maudsley
NHS Foundation Trust (SLaM), peer review of elective referrals and easier access to specialist
advice and guidance.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 22
In Lewisham, as a part the Personal Medical Services (PMS) contract, GPs have been
commissioned to undertake risk stratification under locally agreed risk profiling protocols (using
a combination of emergency activity data, QAdmissions (a risk prediction tool) and clinical
opinion) with a specific focus on diabetes and respiratory patients. Practices identify patients
that would benefit from a multi-disciplinary input and co-ordinate Multi-Disciplinary Meetings
(MDMs) to support, review and manage the care for these patients in collaboration with health
and social care professionals in the Neighbourhood Community Teams and within the wider
health and care system. In addition to this, as required by the national GP contract, GP
Practices have identified moderate and severe frailty in patients aged 65 years and over and
are undertaking reviews for those identified as severely frail.
Three pilots were undertaken to test ways to improve the quality of care through multi-
disciplinary working in GP practices between May and October 2017. The pilots involved more
frequent multi-disciplinary meetings that included a wider range of professionals, including
mental health and home care providers. The evaluation demonstrates a wide range of positive
impacts that enabled more co-ordinated, person centred care and support:
• Stronger relationships were developed enabling a culture focussed on delivering co-
ordinated, compassionate care
• The flow of information across different professional teams and the speed of referrals
both improved
• Members of the team developed new skills and knowledge enabling them to case
manage more effectively, reducing delays to care
• The greater involvement of mental health professionals enabled more effective and
timely referrals to mental health services
An interim report in October 2017 identified key opportunities to improve multi-disciplinary
working and the following activity has been undertaken:
• The learning from the pilots was used to inform the development of a Standard
Operating Procedure for MDMs to establish greater consistency across Lewisham
• Safer and more person centred care is being facilitated for patients with mental health
conditions. Mental Health services have agreed to engage with all MDMs in north
Lewisham in the first instance with a wider roll out to all neighbourhoods planned during

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 23
2018. A regular mental health MDM is being tested at one practice in the south east
Lewisham neighbourhood
• The Neighbourhood Co-ordinators have strengthened links with key services including
housing
• A pilot to test how district nurses and home care workers can work better together has
also been developed. This 16 week pilot started in February 2018 and is bringing
together district nurses and care workers to work as one team to provide more person
centred care and support. Members of the team will work more flexibly to co-ordinate
care and support and reduce duplication across the different organisations
• Funding has been secured to strengthen Neighbourhood Care Networks. This will
involve training and the development of new approaches to multi-disciplinary working at
a neighbourhood level.
Improving the quality of care for some of our most vulnerable patients by providing enhanced primary care services in residential and nursing care homes We commissioned our local GP federation, One Health Lewisham Ltd, to provide an enhanced
primary care services to patients in local non-specialist residential and nursing homes, as well
as extra care housing. The care delivered is holistic and includes caring for those with complex
or multiple long term conditions. Care includes holistic clinical assessments (including
Case Study – Multi-Disciplinary Working
The GP referred a 63 year old woman with history of schizophrenia to the pilot MDM. She lived on her own, with limited networks and had been making daily phone calls to the practice requesting home visits as well as to the London Ambulance Service. The GP suggested different housing might reduce her social isolation. The mental health professional within the MDM confirmed that the patient was also known to mental health services and had an allocated community psychiatric nurse (CPN). The CPN provided an update to the next MDM and confirmed that work to rehouse the patient was in train.
This example demonstrates the value of the MDM in providing a mechanism for improving the flow of information across providers. The information that the GP requested was available much more quickly than would have ordinarily been the case. The GP would have struggled to know how to obtain this information and would most likely have referred to the Social Care Advice & Information team (SCAIT) or asked the Co-ordinator to investigate. The MDM therefore prevented an unnecessary initial assessment by SCAIT and also prevented additional work for the Neighbourhood Co-ordinator, all supporting a better outcome for the patient.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 24
medication reviews), proactive care planning, appropriate end of life care, regular clinical visits,
delivery of vaccinations as well as other provision. A key aspect of the service is to facilitate
multidisciplinary team working and close working with other related services. This will ensure
that patients, with long term conditions, are proactively managed to a high standard to avoid
unnecessary emergency admissions and A&E attendances.
By commissioning this service through our local GP federation, this will support a consistent
approach to the care provided and therefore improve patient outcomes.
Stroke Prevention in Atrial Fibrillation Project in Lewisham
Atrial fibrillation (AF) is a heart condition that causes an irregular and often abnormally fast rate
and is one of the leading and most preventable causes of stroke. Treatment may involve
medication to prevent a stroke of which anticoagulation (medicines that help prevent blood
clots) is the current gold standard. National Institute for Health and Care Excellence (NICE)
guidance states that all citizens with AF who are at risk of stroke should be offered
anticoagulation.
Working with a specialist pharmacist from the Health Innovation Network (HIN) the medicines
team worked with GP practices in Lewisham to identify patients on AF practice registers that
had not had anticoagulation issued recently and review patients in a virtual clinic.
Over 1000 patients were reviewed and of these 800 were not anti-coagulated and over almost
600 were at risk of stroke around one third of these patients have been referred to specialists
for anticoagulation. This could save 2 to 39 strokes a year with an associated saving of up to
£500,000.
3. Improving Quality: Urgent and Emergency Care
The Urgent and Emergency care objective is to commission services which align the adult and
children's physical and mental health services and addresses urgent care as early as possible
‘upstream’ – ‘right care, right time, right place’ .
Review of NHS Walk-in Centre, New Cross and improving provision and access to primary care
The CCG works closely with Healthwatch Lewisham to monitor and triangulate the experience
of patients as they seek health care advice. The regular Intelligence Reports from Healthwatch
Lewisham identified that some patients found it difficult to access primary care and were
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 25
confused by the apparent mixed messages on where to go for help. This information
triangulated well with our other assurance sources and we conducted a review of access to
primary and urgent care services in light of recently commissioned services and the need to
provide clarity for our population on the most appropriate way to access primary and urgent
care; cognisant of the multiple ‘front doors’ to services.
Urgent care in Lewisham was being accessed through a number of services; the Urgent Care
Centre located at the University Hospital Lewisham, the Primary Care Assessment Service
also located at the same site, GP Extended Access Service also located at the same site,
through their GP practice, the New Cross Walk-in Centre, via Integrated Urgent Care (formerly
NHS 111) or high street pharmacies. This provided confused messages and consequently
patients were not always seen in the right care setting and not always seen at the right time.
In July 2017, based on the findings the Governing Body agreed that a review and formal public
and stakeholder consultation should be undertaken to inform the future commissioning
intentions for the NHS Walk-in Centre in the context of the delivery of the CCG’s approved
strategy for primary and urgent care services.
Lewisham CCG conducted a formal 12 week public and stakeholder consultation from August
2017 to October 2017 into the future of the NHS Walk-in Centre and improving provision and
access to primary care. Over this 12 week period we engaged with patients, the general public,
public bodies, key stakeholders including health care partners and the third sector. In
November 2017 the Governing Body deferred their decision about the future of the NHS Walk-
in Centre in New Cross to give more time to review the feedback and consider alternative
proposals.
In January 2018 based on a comprehensive review and evaluation of the consultation
responses and proposed alternatives and a review of the capacity, access and public
awareness of the GP Extended Access Service, the Governing Body was assured that the
needs of patients using the Walk-in Centre could be met by mainstream primary care services.
The Governing Body agreed the closure of NHS Walk-in Centre at New Cross on 31st March
2018.
Improving patients’ experience through the clinical streaming & redirection service
In March 2017 NHS England issued new guidance around urgent primary care streaming. NHS
England recommended that urgent primary care streaming models should provide GPs in the

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 26
Urgent Care Centres (UCC) as well as a ‘front door’ streamer who assesses all patients and
then streams them to the appropriate care pathway, some of which might be away from the
hospital Emergency Department or UCC.
We commissioned LGT to deliver a streaming model in November 2017, We are currently
reviewing the service, which will assess all adults that arrive at the front door of the hospital
where they will be clinically assessed and then redirected to the correct pathway.
Improving patient safety and the patient experience with the GP Extended Access Service
The GP Extended Access Service (GPEA) in Lewisham commenced in April 2017 to increase
access to core general practice as a part of the GP Forward View (GPFV). The service is
delivered by One Health Lewisham, the federation of local GP practices in Lewisham. The
service provides bookable appointments, 7 days per week, 8-8pm, 365 days per year and has
access to patients full medical records (read and write access). The service provides face to
face access to GPs and Nurses and video consultations.
In 2017 we commissioned 25,426 bookable appointments, which increased to 29,914 later in
the year. The service relocated in November 2017 to a purpose built suite within Lewisham
Hospital, which enabled the service to provide appointments for children. This also meant that
the service was able to increase the number of available nurse appointments. In 2017 we
commissioned 5,021 nurse appointments and in 2018 there will be 8,926 more nurse
appointments made available.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 27
Improving patient safety and the quality of care to avoid unnecessary hospital admissions
There has also been quality improvement work undertaken to redesign the Emergency
Discharge Team to identify and support elderly frail patients as soon possible following
presentation in the Emergency Department to avoid any acute admissions. This service is now
a 7 day a week dedicated service therapy team who can then link the patients back into either
support at home or Brymore House, a nursing home that provides 25 community beds which
are both ‘step up’ and ‘step down’. Step up beds support patients who do not need admission
to an acute bed, but are not able to remain in their own homes either through illness or needing
some other short term support to help them to remain in the community. Step down beds
support the earlier discharge of patients from an acute bed once they are medically fit,
facilitating (where appropriate) a short spell of rehabilitation at Brymore House for up to 6
weeks.
Case Study – GP Extended Access Service The Extended Access service proved a lifeline for many people offering additional appointments to people who were unable to see their own GP, including 23 year old Nathan Young.
“I hadn’t had a great experience of GPs before using the service and had to either wait a long time for an appointment or was seen when it didn’t suit me.”
Nathan was treated at the hospital for an abscess but found on release his local GP surgery could only offer evening appointments for his daily change of dressings.
“I didn’t want to be hobbling around in the dark so the practice offered me an appointment at the extended access service, and they were able to see me that morning.
“It’s a good service and flexible to patients’ needs which is how it should be. I know doctors are under a lot of pressure but they have to be realistic about appointment times because we all have commitments.”
Steve Brown*, 50, also praised the service after it removed stiches from his heel after he had been in hospital. He was given an appointment the day after at a GP hub and was seen and treated within ten minutes.
He said the service was quick, professional and that the nurse who treated him was polite, helpful and professional.
*Name changed at request of patient

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 28
Our quality assurance processes have identified that too many older people experience painful
and harmful falls in the community. Accidental falls are one of the biggest avoidable hospital
admissions among the elderly and the Community Falls team established in July 2017 helps to
reduce incidence among over 65s. It is a multi-disciplinary team of occupational therapists,
physiotherapists, therapy assistants and postural stability instructors who help both reduce the
number of falls as well as harm suffered by people who have fallen. The team triage patients
via a designated falls helpline so receive appropriate support. The Falls helpline offers a single
point of access offering advice and information as well as making referrals to the team for
further assessment. The team also provides outreach and education to other organisations
delivering specialist prevention education and advice sessions. Its newest venture is offering
outreach and support in high risk care environments.
Case Study – Community Falls Team A typical example of the 340 referrals made to the service is Mrs Brenda Maloney* who came to the falls team’s attention via her daughter. She had fallen several times, wasn’t confident to go upstairs in her own home and had been repeatedly admitted to hospital.
A physiotherapist provided balance and strengthening exercise, while the Occupational therapist completed a bathing assessment so Mrs Maloney was able to use the shower again after an absence of two years.
She was encouraged to buy a four wheeled walker and then completed outdoor mobility and stairs re-education. Minor safety adaptations such as stair rails were installed.
A bed lever was installed as the patient had previously fallen out of bed and Mrs Maloney was referred for a 25 week strength and balance re-education programme as well as getting advice on transport and a referral to community connections for improved social access. *Name changed at request of patient
Case study – Brymore House
John Smith* is 79 years old and lives in Lewisham. He was admitted to Lewisham Hospital with a bowel obstruction as a medical emergency. He was referred to the Brymore Intermediate Care Unit as he had traits of Parkinsonism and reduced mobility following his stay in hospital. When he arrived he needed lots of support with his mobility and personal care such as taking his medication, kitchen tasks, cleaning, shopping and laundry as well as drinking from a cup and eating his meals.
He stayed at the unit for five weeks where he received rehabilitation treatment from a range of professionals including occupational therapists, physiotherapists, rehabilitation assistants, social worker, medicines optimisation team and nursing care staff. Following his treatment, MB restored his independence and mobility with the aid of a four wheeled walker, shower stool, electric bed, blister pack for his medication and he was able to go home and live independently.
*Name changed at request of patient

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 29
Improving patient safety and the appropriateness of care by redesigning discharge pathways
Our routine monitoring of the quality of care has identified that too many patients stay in
hospital longer than they need to. Nobody wants to be in hospital if they don’t need to be there
and we are working to help patients return home when it is safe to do so.
Discharge to Assess (D2A) is a mandate from NHS England supported by Associate Directors
of Adult Social Services (ADASS), it aims to facilitate timely discharge from an acute bed once
an individual is as well as they can be, where they are assessed as no longer needing medical,
nursing or therapy staff in hospital ensuring that any assessment for long term needs is
undertaken in the patient’s own home or ordinary residence.
D2A was jointly implemented by the CCG, LGT and the London Borough of Lewisham as a
pilot project on 20th March 2016. Patients are referred for D2A with a Discharge Passport;
these passports are screened to ensure that the right D2A pathway is implemented for the
individual concerned.
Through 2016 we have continued to develop this pathway; an integrated team of health and
social care staff visit people at home within two hours of discharge to ensure safety, and
initiate an initial period of assessment.
Outcomes include:
Safe at home with no further action required
Safe at home with up to six weeks of enablement (may include care, therapy input or a
combination of both)
Safe at home with a longer term package of care
In October 2017, the model incorporated the use of community beds at Brymore House to
facilitate a period of intensive rehabilitation where an individual may have the potential to return
to an acceptable level of independence before having their longer term needs assessed, or
where 24 hour care for a short period of time may also facilitate a return to the patients home
following a period of time in hospital. We are also piloting the use of a pop in night service, in
order to support a cohort of patients for a short period as part of the D2A process.
In January 2018, our Continuing Healthcare Team implemented a new process to facilitate the
completion of NHS Continuing Care Funding Assessments in an individual’s own environment

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 31
investment supports a greater focus on early interventions and greater collaboration with
generic community health services that will lead more effective local care pathways and
improved outcomes for women and their families.
We launched a new Primary Care Mental Health service in Lewisham to provide more
comprehensive mental health interventions and support for those individuals that have on-
going mental health needs but do not need to be supported by secondary care mental health
services. The service is providing on-going support and care for up to 500 patients during its
initial 12 month ‘pilot phase’ and is comprised of mental health trust and voluntary sector staff
whom will work with GP surgeries to ensure that services are supported to be and stay in the
community.
Integrating children’s urgent and crisis care service
The Children and Young People’s Joint Commissioning Team is responsible for designing,
commissioning and the contract managing children and young people’s services on behalf of
Lewisham Local Authority and NHS Lewisham CCG, key programmes of work include: Early
Intervention, Child and Adolescent Mental Health Services (CAMHS), Community Health,
Special Educational Needs and Disabilities (SEND) and Looked After Children.
The Five Year Forward View highlighted the opportunities to run health services more
efficiently and models of care that were expected to secure high-quality, more efficient and
effective healthcare for the population. Since 2016 we have been working on the remodelling
of the Children Community Nursing Team (CCNT) service (an overarching term for
CCNT/Special Needs Nursing Team/Hospital at Home) with an admission avoidance/early
discharge service in Lewisham. The first phase of work completed in Spring 2018 which
included a remodelling of emergency department attendances, inpatient admissions and
finances. The next phase of design has now begun. The aim of this work is to improve care
and outcomes for children and young people with acute and long term conditions by
remodelling and bringing together an ambulatory care response team to provide rapid
response in/outreach into acute, admission avoidance with on-going care provided at home
and community settings by the CCNT.
Improving the quality of care for people with learning disabilities We know that people with learning disabilities experience inequalities in healthcare provision
and that this contributes to significantly shorter life expectancies compared to the general

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 32
population. To help us improve the quality of health and social care for people with Learning
Disabilities the CCG and the London Borough of Lewisham joined the Learning Disabilities
Mortality Review (LeDeR) Programme in the summer of 2017. The aim of the programme is to
review the deaths of all those people in Lewisham that have a Learning Disability, to identify
learning from those deaths and use that learning to improve services. The programme is in its
infancy and facing challenges related to stretched resources but we completed our first reviews
in December 2017 and are implementing plans to improve the scale and pace of the
programme in the coming year.
Our routine quality assurance processes have identified that too few people with Learning
Disabilities are recorded on GP registers or receive an annual health check. Our benchmarking
reports show that performance in this area is better in Lewisham than at other CCGs but there
is significant room for improvement. Working in parallel with the LeDeR Programme we have
recently developed a local project to increase the number of people with Learning Disabilites
on GP registers and the proportion of these that receive an annual health check and this will
lead to improved quality of care for these patients.
4. Working with the Care Quality Commission to improve the quality ofservices
We work closely with the Care Quality Commission (CQC) to identify and resolve quality issues
as part of our routine quality assurance processes. The CQC published its Quality Report for
LGT in August 2017. The outcome of the report was that the Trust “Requires Improvement” for
all domains of quality for its hospital services and “Outstanding” for the community services it
provides to Lewisham residents. The CCG took part in a Quality Summit with the Trust, the
CQC and other key agencies in September 2017 to discuss how the whole health and care
system can work together to improve the quality of services in Lewisham and other local
boroughs. Out of the summit and work in the Trust an action plan for quality improvement was
developed and is now being implemented. The CCG monitors the implementation of the action
plan at its monthly Clinical Quality Review Group with the Trust and as a member of the Trust’s
internal quality improvement group. By the end of March 2018 most of the actions had been
implemented and will drive quality improvement across much of the work of the Trust but
further work is required to complete the action plan.
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 33
Similarly we have worked closely with the CQC following the inspection of community based
mental health services for adults provided by SLaM which was published in July 2017. The
CQC identified issues related to the quality of risk assessments and care plans carried out by
the community teams and in response the Trust has been carrying out audits of all the current
risk assessments and care plans in place with a view to improving these where necessary. We
have been monitoring the audits and associated actions at its regular quality meetings with the
Trust and expect to see significant quality improvement as a result.
Quality Assurance visits to service providers We carry out routine and occasional visits to our commissioned services to see quality for
ourselves and in the year we visited the emergency departments at our main hospital and all
the Care Homes with Nursing in the borough. Our visit to the emergency and urgent care
departments in January 2018 at Lewisham Hospital took place towards the end of the severe
pressures period after the Christmas and New Year holidays. No immediate risks were
identified during the visit and we were particularly impressed by the dedication of staff and with
the new Ambulatory Care Unit and the GP Extended Access facility. Some long standing
issues were seen such as problems with recruiting and retaining staff and with IT systems that
were not fully integrated.
Our visits to nursing care homes are designed to provide advice and support particularly with
safeguarding matters. During the visits our Safeguarding Nurse Advisor carries out clinical
audits on topics such as medicines management and care planning and is able to provide
expert advice to improve the quality of care and the patient experience.
5. Improving Quality: learning from when things go wrong
Complaints We received 59 complaints during the year. Learning from the complaints and resultant quality
improvement was widespread and varied:
• In response to a complaint about staff at the New Cross Walk-in Centre, the New Cross
Walk-in Centre reviewed their website to ensure the types of clinicians providing
services was clear and the services they can offer patients more detailed;

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 34
• In response to a complaint about BCG vaccinations in Lewisham, arrangements for the
provision of the vaccinations were reviewed with service managers and the complaint
was passed to Lewisham Immunisations Strategy group to explore implications and
ensure the problems were resolved in future;
• In response to complaints about Continuing Healthcare letters, an electronic pathway
and patient records system was implemented to ensure timely responses and up-to-
date contact information;
• In response to complaints about the Interpreting Service, the Standard Operating
Procedure was reviewed by the CCG to ensure that Interpreters are able to attend all of
their appointments;
• In response to a complaint about the processing of a Mental Health Act assessment, the
CCG worked in conjunction with North East London Commissioning Support Unit
(NELCSU) to review the Collaborative Claims team set up and training requirements to
ensure measures were put in place to prevent the incident happening again;
• In response to a complaint regarding the Interpreting Service, the provider re-iterated to
its interpreters the importance of notifying them should they be running late due to
unforeseen circumstances.
Serious Incidents reported to the CCG by providers There have been no “Never Events” affecting Lewisham residents during the year. There have
been 24 Serious Incidents reported to the CCG by our main acute hospital provider and 21 by
our main mental health provider, much the same as in previous years. These are often the
most serious of quality failures in the health system and are very rare events requiring
providers to report the incidents locally and nationally to ensure that wherever possible lessons
are learned.
Most of the Serious Incidents reported by our mental health provider relate to attempts,
successful or not, to self-harm including suicide. Suicides in patients known to mental health
services are particularly distressing and we work closely with our provider to ensure that a
thorough investigation is carried out so that any lapses in care are identified. Often we find that
care was of a high standard and a suicide or incident of self-harm cannot be directly attributed
to care failures but there are often incidental findings that can lead to improvements. One
theme to emerge from investigations has been a need to improve the quality of risk
assessments and associated care plans. This finding triangulates well with findings from a

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 35
recent Care Quality Commission inspection at the Trust and we have been supporting work to
improve this area of care. The Trust has been systematically auditing risk assessments and
care plans and providing staff with additional supervision and support where indicated.
A rare but recurring theme from a small number of Serious Incidents reported by our general
hospital has been a failure to recognise when a patient’s condition is getting worse and to
escalate this appropriately for further medical care. Sometimes a failure to record vital
observations and to act on them appropriately can lead to unnecessary harm to patients. We
are working with our providers to improve the recording and appropriate escalation of
observations including the implementation of a computerised system which will ensure
accuracy of recording and consistency in response.
6. Contract Management
Our objective in effective contract management is to manage the CCG’s contract portfolio
effectively to ensure that the CCG’s operating plan commitments are met in 2017/18. This
includes ensuring our financial targets are met and value for money is delivered.
NHS England used their formal powers of direction so that from 1st September 2017 our
responsibility for acute commissioning and contracting has been temporarily transferred to
Southwark CCG. This was in response to long-standing issues around emergency
performance at LGT and in the light of the Care Quality Commission (CQC) visit to the Trust in
March 2017. We have contributed to the Urgent & Emergency Care Improvement Plans,
working closely with the Trust, Bexley and Greenwich CCGs as well as the contracting team
hosted by Southwark CCG. The plans have encompassed measures to improve the accident
and emergency 4 hour standard, bed occupancy, discharge processes, and staffing. Our
Governing Body and Integrated Governance Committee have continued to monitor
performance and quality of acute services.
Community contracts
Our main provider of community services is LGT and for these services we have a block
contract arrangement, where the value of the contract is independent of the number of patients
treated or the amount of activity undertaken.
The standards required of NHS commissioned providers are set out in Schedule 4 of the NHS
Standard Contract. The Standard Contract specifies targets and thresholds for operational
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 36
standards, National Quality Requirements, Local Quality Requirements, Never Events and
Commissioning for Quality and Innovations schemes (CQUINs). Penalties for breaches of the
standards are also specified.
CQUINs are a contractual lever to incentivise providers to improve quality or develop
innovative services. Lewisham CCG’s approach to CQUINs in 2017/18 was to transform
Community Services to deliver improved quality and outcomes via community-based care.
Locally developed CQUINs focus on improvements in:
• Diabetes
• Respiratory
• Integrated Community Services
• End of Life Care
These CQUIN goals aided by the national Advice & Guidance CQUIN support the shift in
resources and care ‘out of hospital’ (within existing budgets) to be community based and better
interfaced with General Practice.
GP contract
Lewisham CCG was formally approved on 14th February 2017 as a Level 3 commissioner of
primary care (General Practice) by NHS England and from the 1st April 2017 we became
accountable for the following primary care contracts: 4 General Medical Services (GMS), 35
Personal Medical Services (PMS), and 1 Alternative Provider Medical Services (APMS).
Level 3 delegated commissioning for primary care (General practice) offers CCGs the
opportunity to assume full responsibility for commissioning general practice services, whilst
NHS England legally retain liability for the performance of primary medical care
commissioning.
Management of level 3 delegated commissioning is through the Primary Care Commissioning
Committee which reviews performance and quality of GP contracts as well as considering
practice business cases for change (i.e. mergers, relocations, partnership changes).
In 2017/18, Lewisham performed well in regard to CQC inspections with all practices rated as
Good and one as Outstanding.
A new PMS contract went live on the 1st January 2018 which all Lewisham PMS practices have
signed up to. As part of this contract, there is a PMS premium element of £11.14 per weighted

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 37
patient for 2017/18. Commissioning Intentions against this Premium, which support delivery of
the CCGs primary care strategy, Lewisham Health & Wellbeing Strategy and wider STP, were
agreed and allocated across a range of KPIs and service specifications.
The commissioning intentions included within the new PMS contract as part of the ‘PMS
premium element’ are:
• Referral management
• Patient Voice
• Childhood Obesity
• Alcohol
• Pre-diabetes
• Bowel Cancer screening
• Cervical Cancer screening
• Vaccinations
• End of Life
• Home Visiting
• Risk Profiling & Multidisciplinary Working
• Wound care
• Drug monitoring
The four GMS practices in Lewisham were made an equivalent offer against these
commissioning intentions which was accepted by all four practices. We therefore have total
population coverage against the commissioning intentions.
The one APMS.contract in Lewisham ceased on the 31st January 2018.
GP Federation contracts
We commissioned One Health Lewisham Limited, the federation of local GPs, to deliver the
following three key contracts in 2017/18:
• GP Extended Access Service
• Enhanced Primary Care Service to for Care Homes
• Coordinated Care Service

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 38
Through the Coordinated Care Service, the following outcomes have been delivered:
• 81% of Diabetics patients had a Blood Pressure 140/80 mmHg or less
• 79% of Diabetic patients had a Cholesterol of 5.0 or less
• 71% of Diabetic patients had a HbA1c of 59 or less
• 92% of COPD patients had an annual review
• 82% of Hypertension patients had a Blood Pressure of 150/90 or less
• 74% of over 65 year olds were vaccinated against pneumococcal
• 30% of newly diagnosed people with COPD stopped smoking
• Lewisham fully utilised its allocated capacity against the national Diabetes Prevention
Programme
Mental health contracts
Our efforts focused on delivering the agreed trajectories for Improving Access to Psychological
Therapies (IAPT), First Episode Psychosis (FEP) and dementia diagnosis rates and improving
the quality of care by reducing delays in transfers of care and the patient experience on
inpatient wards.
We continue to be on schedule to meet our agreed performance targets for IAPT, First Episode
Psychosis and the Dementia Diagnosis rate by the end of March 2018. Over the last 12
months our core provider, SLaM, has reduced the number of delayed discharges from our
inpatient wards, although there is further work to complete to ensure that patients with high
levels of need that require intensive support once they leave hospital are identified at the
earliest possible stage. This early identification increases the likelihood that our patients will
receive all aspects of their care in a timely way and should result in a more effective transfer
from hospital to community based care when required.
7. Constitutional Standards and Other Key Performance Measures
We have been reporting against Standards that are included in the NHS Constitution provided
to patients and other key measures that the CCG has planned to improve during the year. The
Scorecards set out over the next few pages outline the key standards, the expected
performance, the date to which the information is available to and whether the performance
has improved so far against the previous year.
Full year performance for 2017/18 for all measures will be available at the end of June 2018.
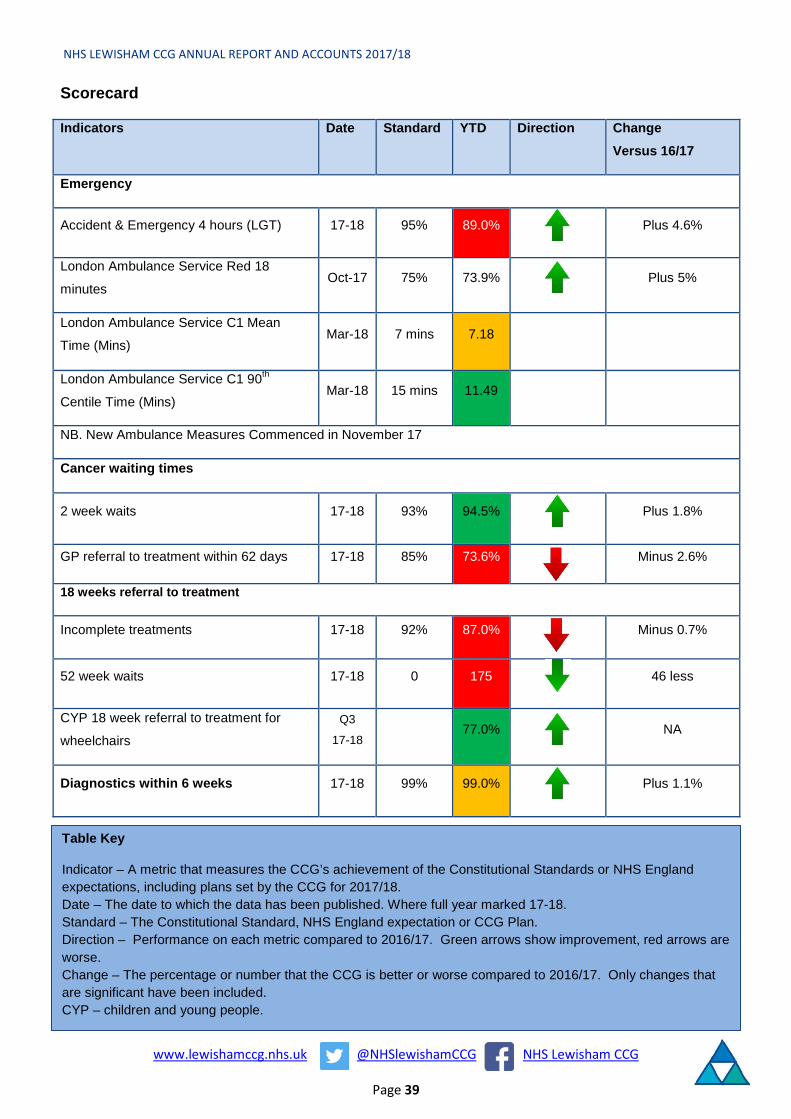
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 39
Scorecard
Indicators Date Standard YTD Direction Change Versus 16/17
Emergency
Accident & Emergency 4 hours (LGT) 17-18 95% 89.0% Plus 4.6%
London Ambulance Service Red 18
minutes Oct-17 75% 73.9% Plus 5%
London Ambulance Service C1 Mean
Time (Mins) Mar-18 7 mins 7.18
London Ambulance Service C1 90th
Centile Time (Mins) Mar-18 15 mins 11.49
NB. New Ambulance Measures Commenced in November 17
Cancer waiting times
2 week waits 17-18 93% 94.5% Plus 1.8%
GP referral to treatment within 62 days 17-18 85% 73.6% Minus 2.6%
18 weeks referral to treatment
Incomplete treatments 17-18 92% 87.0% Minus 0.7%
52 week waits 17-18 0 175 46 less
CYP 18 week referral to treatment for
wheelchairs Q3
17-1877.0% NA
Diagnostics within 6 weeks 17-18 99% 99.0% Plus 1.1%
Table Key
Indicator – A metric that measures the CCG’s achievement of the Constitutional Standards or NHS England expectations, including plans set by the CCG for 2017/18. Date – The date to which the data has been published. Where full year marked 17-18. Standard – The Constitutional Standard, NHS England expectation or CCG Plan. Direction – Performance on each metric compared to 2016/17. Green arrows show improvement, red arrows are worse. Change – The percentage or number that the CCG is better or worse compared to 2016/17. Only changes that are significant have been included. CYP – children and young people.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 40
While the performance for Lewisham and Greenwich NHS Trust on the Accident and
Emergency 4 hour measure is still short of the 95% standard, like many other parts of the
country, it has improved by almost 5% year on year. In 2017/18 the Ambulatory Care Unit at
the Lewisham site has been more embedded in practice and the CCG has invested in a GP
helping to direct patients to the right service as people register at the front of A&E.
The London Ambulance Service (in common with other services) has changed its
measurement to be in line with a new clinically led streaming service nationally in November
2017. For the highest category, London Ambulance Service has marginally missed the 7
minute median time (but is just under a minute faster than the national position) and meets the
90th centile time by over 3 minutes.
Within Cancer Services, Lewisham people are beginning their diagnosis process faster than
the previous year within the standard, but once diagnosed the percentage of people having
their treatment begin with 62 days of a GP referral has worsened during the year. The
Governing Body reviewed the plan to improve services to be closer to the standard across
South East London by the end of 2017/18. In particular, the focus is on joint working between
Lewisham and Greenwich NHS Trust and Guys and St Thomas Foundation Trust, so that
people are referred in a timely way so that their treatment can begin at Guys and St Thomas.
Improved access to diagnostics is also part of the plan.
18 weeks Referral to Treatment times are measured by the percentage of people within 18
weeks on the incomplete – or waiting list. This measure is close to the plan set, which is linked
to issues with providers, especially Kings College NHS Foundation Trust. There are plans for
2018/19 that will reduce the number of people waiting, and significantly reduce those people
waiting over 52 weeks.
Overall diagnostic waits within 6 weeks has been almost met in 17/18 year to date this year,
whereas it was not met in 2016-17.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 41
Indicators Date Standard YTD Direction Change
Mental Health Adults
Improving Access to Psychological
Therapies Recovery Rate Feb-18 50.0% 52.5% Plus 5.9%
Improving Access to Psychological
Therapies Access Rate Feb-18 4.2% 4.2% Plus 0.3%
Early Intervention in Psychosis 2 weeks 17-18 50.0% 67.1% Plus 9.5%
Dementia Diagnosis Rate 17-18 66.7% 71.3%
Mental Health Children
Eating Disorders Urgent in 1 week 17-18 100.0% 100.0%
Eating Disorders Routine in 4 weeks 17-18 75.0% 77.4% Plus 38%
Others
E Referral Rate out of Referrals Feb-18 80% 54.0% Plus 17%
Personal Health Budgets per 100000
Registered Population
Q4
17-1818.6 15.5 Plus 2.1
Infection Control
MRSA 17-18 0 7 Plus 3
Cdifficile 17-18 53 38
All existing mental health standards have been met year to date with particular improvements
in the psychological therapies recovery rate and the percentage of people with psychosis being
seen in two weeks improving by nearly 10%. However, the percentage of people accessing
psychological therapies within 6 weeks is below the standard required in the middle of the
year, but this should recover to the standard early in 18/19 as people entering treatment are
meeting the standard.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 42
For 2017/18 there is a new measure for access to Children and Young People to Eating
Disorder Services. For urgent referrals all Children and Young People access the service
within 1 week. For routine referrals within 4 weeks, the percentage achieved has doubled year
on year and has met the plan or 75%.
The NHS e-Referral Service (e-RS) combines electronic booking with a choice of place,
date and time for first hospital or clinic appointments. Patients can choose their initial
hospital or clinic appointment, book it in the GP surgery at the point of referral, or later at
home on the phone or online. E Referrals from primary care to outpatients, including two
week cancer referrals, has improved year on year by 17%, so that half of Lewisham people
have that electronic booking. The February 2018 level is 76% which is nearly at the planned
level of 4 out of 5 people being referred in this way. This is higher than the England and
London rates.
For infection control there has been a rise year on year in MRSA (Methicillin-resistant
Staphylococcus aureus) infections, while Cdificile infections are well within the plan set for the
CCG.
8. Improvement and Assurance Framework
NHS Lewisham CCG is assessed against the NHS England CCG Improvement and Assurance
Framework providing a common set of metrics covering Better Health, Better Care,
Governance and Sustainability. Within this there are a set of Clinical Priorities for which CCGs
are assessed as Outstanding, Good, Requires Improvement and Inadequate.
In 2017/18 the CCG has been assessed for the following Clinical Priorities:
• Diabetes Care: Outstanding
This included an assessment for people with diabetes for their control of blood sugar,
blood pressure and cholesterol, which is aimed to provide them with better outcomes.
Working with GPs and staff in practices and in the community people with diabetes have
improved their level of control by 5% year on year.
• Dementia Care: Outstanding
Practices have identified a high number of people with dementia compared to the likely
prevalence rate for Lewisham. A high number of those (80%) have had their care plan
reviewed over the last year.
• Mental Health: Good

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 43
Psychological Therapies Services have supported 54% of service users in achieving
recovery so far in 2017-18. This is against a 50% standard and is the first time this has
been met for Lewisham service users.
The CCG is awaiting scores for three other Clinical Priorities including Cancer Care.
During the year the CCG received confirmation that the survey for those Lewisham people
diagnosed with cancer indicated significant improvements in their views of both cancer care
and the number who confirmed that they had a care plan compared to previous surveys and
nationally.
All CCG Improvement and Assurance Framework indicators can be found at My NHS on NHS
Choices. The following link takes you directly to the My NHS page for NHS Lewisham CCG
here.
9. Financial Performance
In 2017/18 we achieved all of our statutory financial duties which are:
• Total CCG gross expenditure should not exceed CCG income.
• Total CCG net expenditure should not exceed revenue resource allocation.
• Capital expenditure should not exceed the amount allocated by NHSE.
• Expenditure on administration should not exceed the allocated running cost allowance.
We also exceeded the Better Practice Payments Code requirement to pay at least 95% of
invoices within 30 days.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 44
The table below sets summarises the delivery of these duties. These are also shown in our
financial accounts statements. Duty Duty
Achieved Target Performance
Yes/No £000 £000
Expenditure not to exceed income Yes 477,140 476,160
Capital resource use does not exceed the amount specified in
Directions Yes 50 50
Revenue resource use does not exceed the amount specified in
Directions Yes 471,333 470,353
Capital resource use on specified matter(s) does not exceed the
amount specified in Directions Yes 0 0
Revenue resource use on specified matter(s) does not exceed the
amount specified in Directions Yes 0 0
Revenue administration resource use does not exceed the amount
specified in Directions Yes 6,651 6,260
A planned cumulative surplus of £9,380k was agreed with NHS England at the start of the year
with a planned nil in-year movement. A financial risk share agreement is in place across the six
CCGs in South East London. It was agreed through the governance of each CCG that the risk
share agreement be enacted in 2017/18. The final revenue resource limit values included in
the 2017/18 annual accounts of each CCG reflect the outcome of the risk share agreement.
As set out in the 2017/18 NHS Planning Guidance, CCGs were required to hold a 0.5 per cent
reserve uncommitted from the start of the year, created by setting aside the monies that CCGs
were otherwise required to spend non-recurrently. In the event, the national position across the
whole of the NHS has been such that NHS England has been unable to allow CCGs to spend
the 0.5% non-recurrent budgets. Therefore, to comply with this requirement, NHS Lewisham
CCG has released its 0.5% reserve to the bottom line at year end, resulting in an additional
surplus above plan for the year of £2.08m. Similarly NHS England asked CCGs to release the
in year benefit of reductions in the prices of some primary care prescribed drugs. For
Lewisham this was £336k. These benefits are offset by an over spend of £1.45m caused by
the cost pressure of “No Cheaper Stock Obtainable” (NCSO) drugs (also known as “Short
Supply” drugs (SSD).

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 45
The adjustments to the CCG’s control total target are summarised in the table below: Cumulative
£000 In-Year
£000
Initial target 9,380 nil
Less allowable short supply drugs unavoidable cost pressure (1,452k) (1,452k)
Add release of 0.5% System Risk Reserve 2,077 2,077
Add benefit of release of rebate for Cat M drugs 336 336
Revised target year end surplus 10,341 961
Actual year end surplus 10,360 980
Better/(worse) than target 19 19
The actual cumulative surplus at the year end was £10,360k. This is £19k better than target.
The £10,360k surplus will be carried forward and for drawdown in future years.
Our expenditure on commissioned services in 2017/18
We commission the majority of NHS services for Lewisham people. We spend the money
available to us on healthcare for Lewisham patients and we aim to spend it in the best way that
will improve the health of and the care for Lewisham people, which delivers value for money to
the taxpayer and is sustainable in the long term.
In 2017/18 our net annual expenditure was £470.4m. Approximately 80% of our expenditure is
on a combination of hospital services, mental health services and community services.
The following chart shows the breakdown of our expenditure by service type in 2017/18.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 46
Mental Health Services, £72.77m,
15.47% Community Services, £31.30m, 6.66%
Continuing Care Services, £17.36m,
3.69%
Primary Care Prescribing and Other Services , £39.41m, 8.38%
Primary Care Co-Commissioning, £41.95m, 8.92%Better Care Fund,
£20.52m, 4.36% Other Services, £9.99m, 2.12%
Hospital Services, £237.04m, 50.40%
Commissioning Expenditure 2017-18 (£m)

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 47
2016/17 expenditure excluded primary care co-commissioning as this was a CCG delegated responsibility from 1st April 2017. The charts below
therefore exclude primary care co-commissioning in order to enable a comparison of expenditure on commissioned services between 2016/17 and
2017/18.
Mental Health Services,
£71.84m, 17.22%
Community Services,
£29.71m, 7.12%
Continuing Care Services,
£16.52m, 3.96%
Primary Care Services ,
£39.09m, 9.37%
Better Care Fund, £20.17m, 4.83%
Other Services, £13.12m, 3.15%
Hospital Services, £226.69m,
54.34%
Commissioning Expenditure 2016-17 (£m)
Mental Health Services, £72.77m, 16.99%
Community Services, £31.30m,
7.31%
Continuing Care Services,
£17.36m, 4.05%
Primary Care Prescribing and Other Services , £39.41m,
9.20% Better Care
Fund, £20.52m,
4.79%
Other Services, £9.99m, 2.33%
Hospital Services,
£237.04m, 55.33%
Commissioning Expenditure 2017-18 (excluding Primary Care Co-Commissioning) (£m)

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 48
The table below shows the 2017/18 expenditure on hospital services (services from other NHS
Trusts in Note 5 to the Annual Accounts). It includes non-recurrent expenditure of £1.75m that
was paid by the CCG to Lewisham and Greenwich Trust as part of an NHS system-wide
contractual commitment, totalling £10.5m, which was agreed by NHS England in 2013 when
the Trust was formed. This commitment is applicable to 2016/17 and 2017/18 only.
2017/18 Expenditure on Local Hospital Providers by Service Type
Provider Lewisham and
Greenwich NHS Trust
Guys and St. Thomas’ NHSFT
Kings College
Hospitals NHSFT
Service Type £m £m £m
A&E 12.52 1.22 2.21
Emergency/Non Elective
53.15 7.02 9.84 Outpatients
21.42 9.15 8.25 Inpatients
15.43 10.11 6.69 Maternity
7.93 3.82 4.10 Others
29.03 8.24 4.54 Total
139.47 39.56 35.63
10. Sustainable DevelopmentAs an NHS organisation, and as a spender of public funds, we have an obligation to work in a
way that has a positive effect on the communities for which we commission and procure
healthcare services. Sustainability means spending public money well, the smart and efficient
use of natural resources and building healthy, resilient communities. By making the most of
social, environmental and economic assets we can improve health both in the immediate and
long term even in the context of rising cost of natural resources. Spending money well and
considering the social and environmental impacts is enshrined in the Public Services (Social
Value) Act (2012). We acknowledge this responsibility to our patients, local communities and
the environment by working hard to minimise our footprint.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 49
In order to fulfil our responsibilities, NHS Lewisham CCG has a Sustainability Policy to
"improve both the sustainability of an organisation and the way that it provides services and
interacts with people in the community"
Modelled Carbon Footprint
Resulting in an estimated total carbon footprint of 114,450 tonnes of carbon dioxide equivalent
emissions (tCO₂e). The majority of this impact is from the services we commission.
Category tCO2e % CO2e
Core 34 0% Commissioning 103,868 91% Supply chain 10,528 9% Community 20 0%
Climate Change Act target
Lewisham CCG has refreshed its sustainability policy, which will be reflected in a Sustainable
Development Management Plan (SDMP). During 2016/17 the CCG implemented a meeting
management system, Modern.Gov. This system produces electronic committee papers,
thereby reducing the impact on the environment through the printing and collation of papers.
Since June 2017, the system has been fully embedded in the CCG ways of working, being
uses across all committees.
0%
91%
9%
0%
Proportions of Carbon Footprint
Core
Commissioning
Supply chain
Community
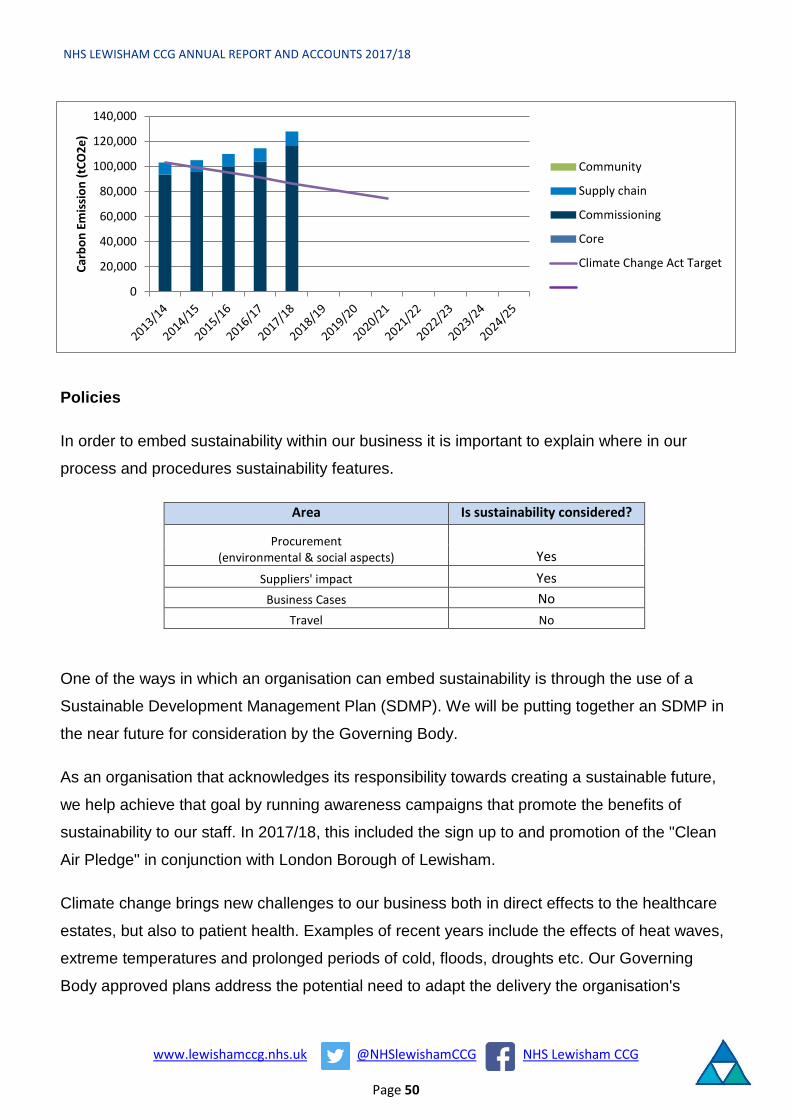
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 50
Policies
In order to embed sustainability within our business it is important to explain where in our
process and procedures sustainability features.
Area Is sustainability considered?
Procurement (environmental & social aspects) Yes
Suppliers' impact Yes Business Cases No
Travel No
One of the ways in which an organisation can embed sustainability is through the use of a
Sustainable Development Management Plan (SDMP). We will be putting together an SDMP in
the near future for consideration by the Governing Body.
As an organisation that acknowledges its responsibility towards creating a sustainable future,
we help achieve that goal by running awareness campaigns that promote the benefits of
sustainability to our staff. In 2017/18, this included the sign up to and promotion of the "Clean
Air Pledge" in conjunction with London Borough of Lewisham.
Climate change brings new challenges to our business both in direct effects to the healthcare
estates, but also to patient health. Examples of recent years include the effects of heat waves,
extreme temperatures and prolonged periods of cold, floods, droughts etc. Our Governing
Body approved plans address the potential need to adapt the delivery the organisation's
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
Carb
on E
mis
sion
(tCO
2e)
Community
Supply chain
Commissioning
Core
Climate Change Act Target

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 51
activities and infrastructure to climate change and adverse weather events. We have not
assessed the social and environmental impacts for the trust.
NHS Lewisham CCG fully supports the Government’s objectives to eradicate modern slavery
and human trafficking but does not meet the requirements for producing an annual Slavery and
Human Trafficking Statement as set out in the Modern Slavery Act 2015.
Our organisation evaluates the environmental and socio-economic opportunities during our
procurement process, as stated in our Procurement Policy which was approved by the
Governing Body in November 2016.
Adaptation
Events such as heatwaves, cold snaps and flooding are expected to increase as a result of
climate change. To ensure that the CCG would continue to meet the needs of our local
population during such events we have developed and implemented a number of policies and
protocols in partnership with other local agencies these include:
o Lewisham CCG Business Continuity Plans
Green space & Biodiversity
Currently the organisation does not have a formal approach to unlock the opportunity and
benefits of natural capital within a healthcare environment in supporting the health and
wellbeing of patient, staff and the community and to protect biodiversity.
Partnerships
As a commissioning and contracting organisation, we will need effective contract mechanisms
to deliver our ambitions for sustainable healthcare delivery. The NHS policy framework already
sets the scene for commissioners and providers to operate in a sustainable manner. Crucially
for us as a CCG, evidence of this commitment will need to be provided in part through
contracting mechanisms. We have not currently established any strategic partnerships. For
commissioned services here is the sustainability comparator for our providers:

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 52
Organisation Name SDMP On track for
34% reduction
GCC Healthy travel plan
Adaptation SD
Reporting score
LEWISHAM AND GREENWICH NHS TRUST
No
4. NoSustainableDevelopmentManagementPlan
No No No Poor
SOUTH LONDON AND MAUDSLEY NHS FOUNDATION TRUST
Yes 1. On trackto meettarget
No Yes Yes Minimum
KING'S COLLEGE HOSPITAL NHS FOUNDATION TRUST
Yes 1. On trackto meettarget
No Yes No Good
GUY'S AND ST THOMAS' NHS FOUNDATION TRUST
Yes 1. On trackto meettarget
No No Yes Good
More information on these measures is available here: www.sduhealth.org.uk/policy-
strategy/reporting/organisational-summaries.aspx
Performance
Organisation
As a part of the NHS, public health and social care system, it is our duty to contribute towards
the level of ambition set in 2014 of reducing the carbon footprint of the NHS, public health and
social care system by 34% (from a 1990 baseline) equivalent to a 28% reduction from a 2013
baseline by 2020. It is our aim to meet this target by reducing our carbon emissions 10% by
2015 using 2007 as the baseline year. Here's how we have done:

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 53
Commissioned activity
Organisation Name Building energy
use
Building energy use per
FTE Water
Water use per FTE
Percent high cost
waste
Waste cost
increase
LEWISHAM AND GREENWICH NHS TRUST
0-10%decrease 3.8 >20%
increase 54.0 >89%highcost
>20%increase
SOUTH LONDON AND MAUDSLEY NHS FOUNDATION TRUST
Data not available 4.5 0-20%
increase 32.1 >75%highcost
Data not available
KING'S COLLEGE HOSPITAL NHS FOUNDATION TRUST
>10%decrease 3.5 >20%
increase 29.3 >75%high cost
>20%increase
GUY'S AND ST THOMAS' NHS FOUNDATION TRUST
0-10%decrease 5.1 >20%
increase 45.0 >75%highcost
0-20%increase
More information on these measures is available here: www.sduhealth.org.uk/policy-strategy/reporting/organisational-
summaries.aspx
Travel
We can improve local air quality and improve the health of our community by promoting active
travel – to our staff, through our providers and to the patients and public that use the services
we commission. Every action counts and we are a lean organisation trying to realise
efficiencies across the board for cost and carbon (CO2e) reductions. We support a culture for
active travel to improve staff wellbeing and reduce sickness.
Category Mode 2014/15 2015/16 2016/17 2017/18
Staff commute miles 58,598 66,283 54,777 61,480 tCO2e 21.53 23.97 19.80 21.91
Business Travel miles 7,712 6,477 2,946 2,551 tCO2e 2.83 2.34 1.06 0.91
Active and public transport miles 3,304 3,511 4,202 2,616 tCO2e 0.30 0.30 0.39 0.24
Owned Electric and plug-in hybrid electric vehicle mileage
miles 0 0 0 0 tCO2e 0.00 0.00 0.00 0.00
The Staff Commute has increased for Lewisham CCG as the number of WTE staff has
increased from 57 in 2016/17 to 64 in 2017/18. Despite this increase in staff business travel
has reduced across the same comparable timescale.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 54
Energy
NHS Lewisham CCG has spent £9,578 on energy in 2017/18, which is a 48.9% increase on
energy spend from last year.
Resource 2014/15 2015/16 2016/17 2017/18
Gas Use (kWh) 148,695 161,326 41,443 118,815 tCO2e 31 34 9 25
Oil Use (kWh) 0 0 0 0 tCO2e 0 0 0 0
Coal Use (kWh) 0 0 0 0 tCO2e 0 0 0 0
Electricity Use (kWh) 133,675 120,518 46,010 52,555 tCO2e 83 69 24 23
Green Electricity Use (kWh) 0 0 0 0 tCO2e 0 0 0 0
Total Energy CO2e 114 103 32 49 Total Energy Spend £ 20,464 £ 16,198 £ 6,434 £ 9,578
0% of our electricity use comes from renewable sources.
0
50
100
150
2014/15 2015/16 2016/17 2017/18
Carb
on (t
CO2e
)
Carbon Emissions - Energy Use
Gas Oil Coal Electricity Green Electricity

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 55
Waste
Waste 2014/15 2015/16 2016/17 2017/18
Recycling/ reuse (tonnes) 0 0 0 0 tCO2e 0.00 0.00 0.00 0.00
Other (tonnes) 0 0 0 0 tCO2e 0.00 0.00 0.00 0.00
Landfill (tonnes) 0 0 0 0 tCO2e 0.00 0.00 0.00 0.00
Total Waste (tonnes) 0 0 0 0 % Recycled or Re-used
Total Waste tCO2e 0.00 0.00 0.00 0.00
Waste Data for Lewisham CCG is not known.
The introduction of Modern.Gov for the production of committee papers has reduced waste of
paper and chemicals associated with printing. The system streamline processes for the
electronic production of committee papers thereby reducing the impact on the environment and
cost of printing and collation of papers for which printing alone costs 1.99p a colour and 0.199
for a black/white page. The cost of the production of an average set of papers for the
Governing Body was approximately £4.50.
Re-use
The re-use of goods and community equipment in the NHS has several key co-benefits,
reducing cost to the NHS, it also reduces emissions from procuring and delivery of new goods
and can provide social value when items are re-used in the community
Category 2014/15 2015/16 2016/17 2017/18 Internal reuse of durable goods £ 0 0 0 0
External reuse of durable goods £ 0 0 0 0

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 56
Paper
The movement to a Paperless NHS can be supported by staff reducing the use of paper at all
levels, this reduces the environmental impact of paper, reducing cost of paper to the NHS and
can help improve data security;
Paper 2014/15 2015/16 2016/17 2017/18
Volume used Tonnes 0 0 0 0
Carbon emissions tCO2e 0 0 0 0 Modern.Gov has been fully integrated across all Lewisham CCG Committees since June 2017.
This has significantly reduced the cost and environmental impact for the use of paper, and
promoted a 'paperless' way of working.
Finite resource use – Water
Water 2014/15 2015/16 2016/17 2017/18
Mains m3 636 826 291 452 tCO2e 0.58 0.75 0.26 0.41
Water & Sewage Spend £ - £ - £ - £ 1,275
Benchmarking
050
100150200250300350400450
Carb
on E
miss
ions
(kgC
O2e
)
Organisation Carbon Footprint by population
Community
Supply chain
Commissioning
Core
Benchmark (CCG)

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 57
11. Patient and Public Involvement
Our vision for engagement
We believe engagement goes further than communication or consultation, and involves
commissioners in providing opportunities for patients, carers and the public to work alongside
them as equal partners in transparent decision-making.
Engagement is a ‘two-way process, involving interaction and listening, with the goal of making
better decisions and commissioning better services that deliver our strategic vision for all –
‘better health, best care and best value.’
Our public engagement charter
We have many ways in which we carry out local involvement. These are outlined in our Public
Engagement Charter:
We will:
1. listen to people and ensure in every way possible that public views are heard and acted
upon
2. involve the public early in developing our strategic plans and how we plan to deliver
improvements in local services
3. involve the public early in our decision-making about how we commission new services,
and redesign them.
4. demonstrate what impact the public has had on the decisions we make
5. always feed back to people who have worked with us
6. use the information provided to ensure that we improve the quality of our services,
support equality and identify inequalities in access to healthcare
7. be honest about when we are engaging, when we are consulting and when we are
providing information
8. support the Involvement of patients in decisions about their care
9. make sure that everyone who works with us will recognise and promote the value of
involving the public.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 58
Lewisham has a diverse population and, in particular, a
wide range of Black and Minority Ethnic communities.
We seek to ensure that we are engaging with all of our
communities, especially ‘seldom heard’ groups. In
2017/18 we engaged with a wide range of charity, faith
and community groups including those working with
people who are homeless, those working with refugees
and migrants, those working with people with a
disability, young people and people at risk of social
isolation.
During 2017/2018 we carried out well over 100
engagement activities, reaching more than 2,000
people, including at the Phoenix Festival in May 2017,
the Our Healthier Lewisham event in June, Lewisham’s People’s Day in July 2017, our Annual
General Meeting in September 2017 and in many meetings with local voluntary and community
groups throughout the year.
Following the Governing Body’s decision in July
2017 to formally consult on the future of the NHS
Walk-in Centre and improving provision and access
to primary care we commenced formal consultation
with the public and local stakeholders. Over a 12
week period from August to October 2017, we
consulted extensively with the public and
stakeholders on the future of the NHS Walk-in
Centre at the Waldron Health Centre, New Cross
and proposals to improve primary care in Lewisham.
During the consultation we conducted 40 face to face
outreach activities. These included drop-in sessions at the Waldron Health Centre and
meetings with homeless charities, community development groups, community hubs, children’s
centres, parents’ forums, patient participation groups, faith groups, local ward assemblies and
students. The consultation also included a survey that was completed by 1,768 people.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 59
During the consultation concerns were expressed
by politicians, residents, homeless charities, GP
practices, and faith groups about the impact of
the proposed closure on vulnerable and
homeless people. To discuss this issue we held a
multi-agency homeless summit with Lewisham
Council in October 2017, which resulted in us
working with the homeless charities, faith groups,
Lewisham Council, the Healthy London
Partnership and two local practices to develop a
pilot Rough Sleepers service which will be launched in April 2018. Feedback from the
consultation indicated that many people were unaware of the alternatives, such as the GP
Extended Access Service. In response we ran a wide-reaching public campaign to promote
awareness of the GP Extended Access Service.
We also ran a dedicated campaign in the north of the borough to encourage people to ‘Use
The Right Service’ in response to our review of the presenting conditions, which demonstrated
that most people who attended the Walk-in Centre did not need to see a GP. Since the
decision was taken we have continued to re-engage with the same homeless charities,
community development groups, community hubs, children’s centres, parents’ forums, patient
participation groups, faith groups, local ward assemblies and students about the changes.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 60

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 61
In 2017/18 we engaged extensively with local
people about proposed changes to prescribing
in Lewisham. The proposals included to no
longer support the routine prescribing of a
range of self-care medicines which are
available over the counter in pharmacies and
to no longer prescribe malaria prevention
medicines on an NHS prescription. Prior to
consulting on these proposals we discussed
them with our Public Reference Group and
tested the materials at Lewisham People’s
Day. During the public consultation, which ran
from August to October 2017, we shared
information widely across the borough
including in GP practices, pharmacies, faith
groups, voluntary and community
organisations. 361 people completed the survey. We invested in paid for advertising on
Facebook which targeted people most likely to travel to countries where malaria prevention
medicine is recommended. To discuss the proposals with people from our West African
communities we held a focus group, inviting a number of community and faith groups. We
strengthened our links with organisations including Lewisham Islamic Centre and Africa
Advocacy Foundation which will be helpful for our future engagement. Following our Governing
Body’s decision to go ahead with the proposals we used the feedback from the consultation to
develop campaigns to inform people about self-care, our Pharmacy First scheme, and we
worked with the West African community to develop information about malaria prevention.
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 62
Our AGM in September 2017 was the best
attended since the CCG formed in April 2013
with 153 participants (a 70% increase on
2016). The event was themed ‘How can we
look after ourselves and our families better?’
and included a Forum Theatre performance
developed by Cardboard Citizens which
explored real issues experienced by
Lewisham people. The play was followed by
a discussion with audience members who were invited on to the stage to put themselves in the
shoes of the resident or staff member being played by the actor and solve the problems being
portrayed. This proved to be a creative way of engaging with residents and staff about our
priority areas of self-care and
prevention which received positive
feedback from virtually everyone
who attended. We also included a
patient who spoke about how, on
advice from doctors and
physiotherapists, has taken
positive steps to improve her
health and wellbeing. There were a
number of key findings from the
event including: recommendations
to improve communication
between clinicians and patients;
the importance of education to improve prevention; and the need to change attitudes for staff
to ensure they consider patients as a whole and for the public to be more pro-active when
taking care of their own and other’s health. These findings have helped to shape our
communications and engagement plans for 2018/19 and a learning event with GPs in February
2018. They have also been shared with Public Health, Lewisham Community Provider
Education Network, One Health Lewisham GP Federation and the Lewisham Local Medical
Committee.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 63
Some comments from people who attended our AGM
“A really interesting and informative event… appreciated the willingness of the staff to engage during the breaks and to discuss difficult topics openly”
“Excellent use of theatre to make it interactive”
“Theatre session very good … needed more time to address the extensive range of
issues raised”
“Presentation of complex financial info was clear and accessible”
“Everybody needs the opportunity to have an input - everybody has something to say. “

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 64
As part of our public engagement around the Our Healthier South East London (OHSEL)
Sustainability and Transformation Partnership (STP) we hosted a lively public event in June
2017. The Our Healthier
Lewisham event was attended
by 107 local people, more than
any of the similar events in
neighbouring boroughs. Local
commissioners and service
providers discussed with people
what the south east London
plans mean for services in
Lewisham, there was a panel
discussion where senior staff
answered questions from the
audience and feedback was
collected from participants which has been collated and published on the OHSEL website.
There is more about this event and the engagement work which the OHSEL and Healthy
London Partnership teams carry out on our behalf later in this report.
Our public engagement team’s work plan is overseen by the CCG’s Public Engagement and
Equalities Forum (PEEF) and supported by the Public Reference Group, a group of local
people which is reflective of the borough’s diversity. The PRG’s role includes:
• Ensuring that public engagement is integrated into the commissioning cycle.
• Acting as a ‘mediating voice’ between the public and the CCG across all commissioning
services in respect of patient and public engagement.
• Supporting the CGG in engaging and communicating more widely with the public to
gather their views, and to inform the public of the challenges facing the NHS and any
proposed changes to services.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 65
In 2017/18 the PRG were strengthened by recruiting
4 new members. The group carried out valuable work
in a range of areas including proposed changes to
prescribing; carers’ information, advice and support;
our Use The Right Service campaign; mental health;
rehabilitation services and the consultation around
the future of the Walk-in Centre. They have also been
actively involved in our EDS2 (Equality Delivery
System) assessment which helps us to review and
improve our performance for people with
characteristics protected by the Equality Act 2010.
PRG members helped decide which services were
reviewed and participated in a grading event which
graded case studies from the Ambulatory Care
Service, Mindcare Dementia Service, and Hospital at
Home Service.
We commissioned Community Waves to set up Diabetes Peer Support Groups covering the
whole of the borough. The four facilitators who were recruited in September 2018 have been
trained and are now running groups in each of the four neighbourhoods. The groups support
local people to manage their diagnosis, increase their awareness of living with diabetes and
share support mechanisms with other people. The peer support groups also provide the CCG
with a valuable insight into local need to inform our commissioning decisions.
We are committed to being open and transparent in our decision-making and providing
opportunities for the entire population in Lewisham to engage with us. Some areas in which we
do this are: public sessions at each of our Governing Body and Primary Care Commissioning
Committee meetings where people can ask questions and at our Annual General Meeting. We
also produce a video following each Governing Body meeting in which our Chair summarises
the meeting.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 66
12. Promoting Equality and Reducing InequalitiesOur strategic priorities are based on an analysis of Lewisham’s Joint Strategic Needs
Assessment’s (JSNA) which identifies health needs of the local population. This includes
disease prevalence amongst different ethnic groups, the health needs of different age groups,
and the impact of deprivation and other factors which affect health equality and inequalities.
Working in partnership with Lewisham Council we identified commissioning intentions for
2017/18 and 2018/19 that have been reviewed and agreed by the Health and Wellbeing Board.
Within these commissioning intentions we define Lewisham Commissioners’ expectations of all
its providers is to deliver advice, support and care that includes:
• Population based – which is a way of looking at patients/service users not just as
individuals but as a part of a wider population
• Promoting health and wellbeing - helping people to get the right advice, support and
care in the right place, first time with a shift towards proactive and preventative services
and supporting community development
• Evidence based and outcome focused - meeting the needs of whole population,
addressing inequality and equalities issues
Case Study - Raising awareness of autism
The CCG has set aside money to raise awareness of autism in the borough as part of a Government call to action.
It was initially alerted to the lack of understanding about the condition by a patient who said the autistic community’s needs weren’t being met in Lewisham
In response, we are working in partnership with the local authority to identify and reach out to this group whose numbers remain unclear.
Its three-pronged approach includes:
• Identifying individuals and providing them with additional advice and supportthrough a partnership with the National Autism Society
• Ensuring the needs of the autistic community are recognised in the borough’s JointStrategic Needs Assessment so potential partnership opportunities can beidentified
• Awareness training ensuring staff and work contracts are autism friendly.
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 67
• Co-produced with patients, service users, carers and wider communities - in partnership
with the people and communities. As Commissioners we believe it is only by the
engagement of the current and potential service users to help reshape services that we
can achieve better outcomes
To support implementation of these commissioning intentions, we commissioned the South
East Commissioning Support Unit (now North East London Commissioning Support Unit) to
carry out an equalities impact assessment (EIA) on them. The analysis concluded that the
commissioning intentions are largely positive, but identified where attention should be given to
specific groups with protected characteristics, carers and social deprivation. Recommendations
are made for the implementation of plans for community based care, neighbourhood care
networks, prevention and early action, planned care, and urgent and emergency care. The
summary of the EIA report is published on the CCG website here
We published our annual equalities report in January 2018 (here). It describes in detail and
provides case studies that show how we are meeting our general and specific duties of the
Equality Act 2010, through our commissioning intentions, equalities analyses, public
engagement and our equalities objectives. It includes case studies that describe in more detail
how we have met the needs of groups from our local population who have shared protected
characteristics and/or experience health inequality. Some of the examples are:
• Ambulatory Care Service was commissioned from Lewisham & Greenwich Trust to
provide assessment and same day discharges for adult patients. The service is reducing
the number of medical admissions, reducing the number of GP referrals to the
emergency department, and reducing the length of stay for some patients. In terms of
service uses and their protected characteristics – the age is quite broad and centred on
those under 64 years. With regard to ethnicity the data for the first 4 months of the
service is reflective of the local population. However, with regard to patients who
completed the Friends & Family Test – more than half described that their day to day
activities were limited because of a health problems or disability.
• Lewisham MindCare – Dementia and Information Service
Lewisham MindCare is a dementia information and support service for anyone in the
borough / with a GP in the borough living with dementia. The service supports people
living with dementia and their carers to ‘live well’ with the condition regardless of the
level of need, severity of the disorder.
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 68
• Hospital at Home for Children ambulatory care or rapid response in the form of
in/outreach into acute adding to the capacity of the Children’s Community Nursing Team
(CCNT) responsible for the provision of on-going care at home.
As part of our assessment for the NHS Equality Delivery System (EDS2) in September 2017
we asked local stakeholders and service users for their views on how well we had delivered
our commissioning responsibilities in these services. Their conclusions were that all three
services reviewed are delivering good quality services, but only one of them was able to
demonstrate (with data) that more than three or four of the nine protected characteristics is
being collected and being analysed to provide assurance that there is not a group of patients
with a particular characteristic who are not accessing the service, are able to access the
services or what has been the experience of patients who have particular these protected
characteristics. Therefore two of the services were graded as ‘developing’.
For the four goals of the EDS2 the CCG achieved the following gradings:
EDS2 Goals Grading achieved In 2017
1 – Better Health Outcomes DEVELOPING
2 – Improved patient access and experience DEVELOPING
3 – A representative and supported workforce DEVELOPING 4 – Inclusive leadership DEVELOPING
The grade for EDS2 Goal 3 took into account the results of the Staff Survey which
demonstrated that from the data available overall most staff members from most protected
groups fare as well as the overall workforce but with some areas for improvement, such as
access to training and development opportunities.
The CCG grade for Goal 4 was assessed independently. The independent assessor noted that
performance has improved, highlighting, for example, strong examples from Governing Body
members of promoting equalities, and examples from Governing Body reports with good
explanations of how services were being amended to reduce inequalities.
The NHS Workforce Race Equality Standard (WRES) is a benchmarking tool introduced by
NHS England to assess the progress of race equality within NHS organisations annually.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 69
The percentage of BAME people in the Lewisham population is 46.5 %. Our aim is to reflect
this diversity in our workforce however, analysis of the CCG workforce shows that CCG
representation of BAME employees in the CCG’s workforce is 39% and the percentage of
BAME staff in bands 8-9 and VSM is 28%, which is 8% less than in 2016. The percentage of
BAME Governing Body members is 20%, which is 5% less than last year. A WRES action plan
is being delivered to improve the representation of BAME staff at senior levels and Board
membership.
The CCG’s Equality & Diversity Steering Group has also assessed the performance against
the WRES of the CCG’s main provider organisations, in particular to confirm that they have
been meeting the reporting requirements and milestones of the WRES and that they have
action plans in place. For example, the group has received a report outlining SLaM’s plans to
improve the diversity of its board’s membership, changing the purpose, requirements and
advertising of board level roles, and participating in a national programme to develop greater
diversity in trust boards. Through the contractual arrangement, the CCG will receive reports at
the Clinical Quality Review Groups (CQRGs) from local providers, who are expected to take
steps underway to address key shortcomings in data, or significant gaps between the
treatment and experience of white and BAME staff, and to publish WRES data on their web
sites and share with Board and staff.
The outcomes of the EDS assessment process and the review of the WRES have informed the
development of our organisational equalities objectives, helping to ensure that we can build on
areas of strength, such as the better health outcomes EDS goal 1, and continue to improve
further in the other areas. The objectives cover access and experience for BAME patients with
long-term conditions, the use of digital technologies in health care, and the representativeness
of our workforce.
13. Our Healthier South East LondonOur Healthier South East London (OHSEL) is south east London’s Sustainability and
Transformation Partnership (STP), and is a coming together of our health and social care
partners in south east London to make sure we are doing all we can to work in partnership to
get the best health outcomes for our population. It has evolved from a commissioner-led
strategy, established in 2013, into a partnership between local commissioners and providers,
working with local authorities, patients and the public.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 70
The STP is not a blueprint for the next five years, it is a series of plans for different clinical
areas and enablers, such as workforce and estates, which are at different stages of
development.
The STP (full version and summary) was published on 4 November 2016 and was one of the
first in the country to be made public.
Our STP has set the following five priorities:
1. Developing consistent and high quality community based care (CBC), primary care
development and prevention
This includes promoting self-care, prevention and better co-operation between different
organisations
2. Improve quality and reducing variation across both physical and mental health
This includes better integration of mental health, and reducing the pressure on and
simplifying urgent and emergency care
3. Reducing cost through provider collaboration
This includes consolidation of some non-clinical support services, including pathology
and finance back office
4. Developing sustainable specialised services
This includes mental health collaboration, renal and cardiac work
5. Changing how we work together to deliver transformation
This includes the development of integrated care. It also focused on how we can make
sure that we are able to provide care for the population of south east London as it grows
and ages in a way that is affordable and meets the needs of a 21st century population.
Engagement
In the summer of 2017, the STP held a
series of six public events, one in each
of the boroughs. The aim was to
engage further with our communities
about how they would like health
services to develop in South East

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 71
London, and to get feedback on our existing plans. The overall message was that we need to
focus more on prevention, partnership working and better co-ordination of services. There was
also a strongly held view that we need to do more to explain and engage on the STP. We
published an independent feedback report from these events and also our response to how we
will adapt to this feedback.
In addition:
• We have patient and public voices and Healthwatch representatives on each of our
clinical and decision making workstreams influencing all our key programmes of work
and feeding into our Patient and Public Advisory Group
• We are working with Maternity Voice Partnerships from each borough to co-produce our
Better Births Implementation Plan, setting our maternity transformation priorities for the
whole of south east London
We also continue to hold south east London wide Equalities Steering and Stakeholder
Reference Group meetings to ensure our plans are assured around patient and public
engagement and equalities issues.
Our approach has been informed and endorsed by The Consultation Institute, who advise on
best practice engagement at national level. The engagement programme was also shortlisted
for a national award by the Association of Healthcare Communications and Marketing (AHCM).
Some highlights from 2017
We have made significant progress in a range of areas through the contribution of our
colleagues across primary care, acute and mental health services, and commissioning.
• Better access to GPs
An extra £7.5 million has gone into primary care in south east London so that patients
can book a GP at a time that suits them – including more evening and weekend slots.
SEL has now delivered extended GP access at 100 per cent compliance.
• GP workforce
SE London STP secured national funding to recruit 45 international GPs to the
boroughs of Bexley, Bromley, Greenwich and Lewisham. The first 25 recruits are
anticipated to arrive in the SE London in autumn 2018. Lambeth and Southwark have

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 72
since indicated that they too wish to participate in this programme and a further bid has
been made to the national programme.
• Faster cancer diagnosis
A Rapid Access Diagnostic Clinic based at Guy’s and St Thomas’ Hospital was
launched to provide swift access to a range of diagnostic tests for patients presenting
with vague symptoms. They have received over 400 referrals, with 31 of those resulting
in a cancer diagnosis. Following a successful pilot in Lambeth and Southwark, the
service is being extended to Bromley, Bexley, Lewisham and Greenwich from April
2018.
• Mental health services:
We are improving the link between physical and mental health and mental health
support and liaison team in A&Es 24/7 and working towards no out-of-area placements
for non-specialist care by 2021. We introduced an initiative to improve the mental health
of people with diabetes through the ‘three dimensions for diabetes’ pilot. The overall aim
is to integrate medical, psychological and social care for people with persistent and
poorly controlled diabetes
• Digitalisation of GP patient records
OHSEL secured funding to help 22 GP practices across south east London to digitalise
their paper records. This will mean space can be made available for further clinical care
and end reliance on paper records.
• NHS 111
The online service was launched at www.111.nhs.uk, enabling patients to self-assess,
receive self-care advice, be signposted to an appropriate service or receive a call back
from an NHS 111 clinician, the pan London Dental Nurse Triage Service or one of the
out of hours GP services.
6. Healthy London PartnershipNHS Lewisham CCG, along with all London CCGs and NHS England (London), funded
Healthy London Partnership (HLP) in 2017/18 to bring together the NHS in London and our
partners to deliver London’s 10 ambitions to transform health and care for all Londoners.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 73
Our partners include the Mayor of London, Greater London Authority, Public Health England,
London Councils and Health Education England. We believe that collectively we can make
London the healthiest global city in the world by uniting all of London to deliver the ambitions
set out in Better Health for London: Next Steps and the national NHS Five Year Forward View.
During 2017, HLP set up the Urgent and Emergency Care Improvement Collaborative on
behalf of NHS England (London), NHS Improvement (London) and The Association of
Directors of Adult Social Services to transform the way that Londoners receive unplanned
urgent care and support. This includes preventing the need to go to hospital, supporting them
to become medically fit and well in hospital and then helping them to go home as soon as
possible. The aim of the collaborative is to bring together leaders from health and social care
working to define what improvement work needs to happen in London, drawing on the best
practice around sustainable improvement and working with the leaders in this field. Key to this
has been providing data to drive change, and as part of this work HLP ran three days of
surveys of hospital bed occupants across 17 London hospital sites to understand where our
improvement efforts need to be targeted.
Other highlights for the partnership during 2017/18 have included working with partners to
launch Thrive LDN, a joint new citywide movement with the Mayor of London to improve
mental health and wellbeing. Community workshops and problem solving booths were held
across London as part of Thrive’s ‘Are we okay London?’ campaign which has reached
15.5 million people so far.
The findings from HLP’s year-long engagement with Londoners on childhood obesity, the
Great Weight Debate, were published in 2018. Nine out of 10 Londoners who responded to the
Great Weight Debate survey said tackling London’s childhood obesity epidemic should be
either the top or a high priority for the capital. The findings are being used to inform every
London borough’s childhood obesity strategy and have informed the Mayor’s London Plan
which includes a policy to prevent new hot food takeaways from opening within 400 metres of
a school. Following on from this, HLP is now working with fast food shops, businesses and
communities in three London boroughs (Southwark, Lambeth and Haringey) to pilot their ideas
for making high streets healthier for children and young people through the Healthy High
Streets Challenge.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 74
HLP also worked on behalf of London CCGs with NHS England (London region) to raise
awareness of GP online services and GP extended access services across London. Nearly
two million Londoners are now registered for GP online services and every London borough
offers evening and weekend appointments to people in their local area.
Through HLP’s partnership working, the Mayor of London, Secretary of State for Health &
Social Care Jeremy Hunt, London Councils and NHS, Public Health and wider health and care
leaders signed the London Health and Care Devolution Memorandum of Understanding in
November 2017. This deal paves the way for improving the health and wellbeing of all
nine million Londoners. Devolution provides the foundations to enable us to improve the way
health and care services are delivered in the capital at a faster pace. Through the work of the
pilots over the past year we have learned much more can be done to prevent ill-health, support
people to make healthier choices and to join up health and care particularly when we work
closely together. HLP is now leading engagement with system leaders to co-design the future
of health and care across London which began with an event in December 2017. The London
Health and Care Strategic Partnership Board (SPB) has been established to provide strategic
and operational leadership for London-level health and care activities. HLP will continue to
support the Board and the wider system to implement devolution and wider health and care
transformation goals and is committed to ensuring health and care leaders are updated on
progress and are also involved in shaping the next steps for London.
In 2017 HLP developed and published online training for GP receptionists to help people who
are homeless access GP practices and produced 60,000 ‘my right to access healthcare’ cards
for people who are homeless to make sure they can get equal access to healthcare given that
they are much more likely to use A&E services than other Londoners.
Finally at the beginning of 2018 HLP began working with partners including the Mayor of
London, London Councils, Public Health England and the NHS, on a joint plan to cut rates of
new HIV infection and eliminate associated discrimination and stigma. This followed the
signing of the 'Paris Declaration on Fast-Track Cities Ending the AIDS Epidemic' in January
2018.
During 2018 Healthy London Partnership will evolve to formally support all of the health and
care partners to work together and strengthen their governance and delivery arrangements, so

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 75
as a city we can implement the devolution agreement and our wider health and care
transformation goals, to make sure we deliver on our commitments to make London the world's
healthiest city.
7. Health and wellbeing strategy
The CCG’s positive relationship with the Health & Wellbeing Board and other local partners,
and contribution to the delivery of local strategies and priorities is integral to this report, for
instance the work of the Lewisham Health & Care Partners and adult integration programme in
the development of the whole system model of care. This has been reflected in reports that the
Board has received at its April, July and November 2017 meetings, as well as the partnership
commissioning intentions that the Board has agreed. Health and Wellbeing Board members
have been consulted on this review, at its meeting on 1st March 2018, noting the CCG
contribution to the delivery of local strategies and priorities such as the work of the Lewisham
Health & Care Partners and adult integration programme in the development of the whole
system model of care.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 76
ACCOUNTABILITY REPORT
Andrew Bland
Accountable Officer
25th May 2018

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 77
Corporate Governance Report
Members Report
Member practices NHS Lewisham CCG was made up of the following member practices during
2017/18:
Practice Name Neighbourhood Address
Mornington Surgery North 433 New Cross Road, SE14 6TJ
Queens Road Practice North 387 Queens Road, New Cross, London,
SE14 5HD
Kingfisher North Kingfisher Medical Centre, Staunton Street,
Deptford, SE8 5DA
Clifton Rise North Clifton Rise Family Practice, Waldron Health
Centre, Stanley Street, London, SE8 4BG
New Cross Health Centre North New Cross Health Centre, 40 Goodwood
Road, New Cross, SE14 6BL Grove Medical Centre North Windlass Place, London, SE8 3QH Vesta Road Surgery North 58 Vesta Road, London, SE4 2NH Amersham Vale Training Practice
North Waldron Health Centre, Stanley Street, London, SE8 6TJ
Deptford Surgery North 502-504 New Cross Road, London, Se14
6TJWaldron Family Group Practice
North Waldron Health Centre, Stanley Street, London, SE8 4BG
Deptford Medical Centre North 2 Pearsons Avenue, SE14 6TG
Belmont Hill Central The Surgery, 36 Belmont Hill, Lewisham,
SE13 5AY
Lee High Road Central Lewisham Medical Centre, 308 Lee High
Road, Lee, SE13 5PJ
Lee Health Centre Central Lee Health Centre, 2 Handen Road, Se12
8NP
Morden Hill Central The Surgery, 21 Morden Hill, London, SE13
7NN St Johns Medical Centre Central 56-60 Loampit Hill, Lewisham, SE13 7SX
The Surgery, 20 Lee Road Central The Surgery, 20 Lee Road, Blackheath, SE3
9RT Brockley Road Central 465-467 Brockley Road, Brockley, SE4 2PJHilly Fields Medical Centre Central 172 Adelaide Avenue, Brockley, SE4 1JN
Honor Oak Group Practice Central Honor Oak Health Centre, 20 Turnham
Road, SE4 2LA
Triangle Group Central The Triangle Group Practice, 2 Morley Road,
London, SE13 6DQ

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2018/19
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 78
Practice Name Neighbourhood Address
Rushey Green Central The Primary Care Centre, Hawstead Road,
London, SE6 4JH
Woodlands Health Centre Central 4 Edwin Hall Place, Hither Green Lane,
London, SE13 6RN Nightingale Central 2 Handen Road, SE12 8NP
Hurley Group ** Central Waldron Health Centre, Amersham Vale,
London, SE14 6LD
South Lewisham South East 50 Conisborough Crescent, Catford, London, SE6 2SP
The Surgery, Torridon Road South East The Surgery, 80 Torridon Road, Catford, SE6
1RB
Downham Family Practice South East Downham Health and Leisure Centre, 7-9 Moorside Road, Downham, BR1 5EP
The Surgery, Downham Way South East The Surgery, 481-483 Downham Way,
Downham, Kent, BR1 5HU The Surgery, Winlaton * South East 139 Winlaton Road, Bromley, Kent, BR1 5QA ICO Group - The Surgery, Chinbrook
South East 32 Chinbrook Road, Grove Park, London, SE12 9TH
Parkview Surgery South East 186 Brownhill Road, Catford, London, SE6
1AT ICO Group - Marvels Lane Health Centre
South East 37 Marvels Lane, Grove Park, SE12 9PN
ICO Group - Moorside South East Downham Health and Leisure Centre, 7-9 Moorside Road, Downham, BR1 5EP
ICO Group - The Surgery Boundfield Road
South East The Surgery, 103 Bounfield Road, Catford, SE6 1PG
Oakview Family Practice South East 190 Shroffold Road, Downham, Kent, BR1
5NJ
Baring Road Medical Centre South East Baring Road Medical Centre, 282 Baring
Road, London, SE12 0DS
Jenner Practice South West 201 Stanstead Road, Forest Hill, London, SE23 1HU
Sydenham Green Group Practice
South West 26 Holmshaw Close, Sydenham, London, SE26 4TH
Woolstone Medical Centre South West Woolstone Road, London, SE23 2TR Sydenham Surgery South West 2 Sydenham Road, Sydenham, SE26 5QW
Wells Park Practice South West The Wells Park Practice, 1 Wells Park Road,
Sydenham, London, SE26 6JQ
Bellingham Green Surgery South West Bellingham Green Surgery, 24 Bellingham
Green, Catford, London, SE6 3JB
Vale Medical Centre South West The Vale Medical Practice, 195-197 Perry
Vale, Forest Hill, London, SE23 2JF
* Closed with effect from 01 August 2017
** Closed with effect from 01 February 2018

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2018/19
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 79
Composition of Governing Body The Chair of the CCG Governing Body continues to be Dr Marc Rowland. Mr Martin
Wilkinson has been the Accountable Officer.
The Membership Body, which at NHS Lewisham CCG has been known locally as the
Clinical Directors Committee (supported by wider membership structures as set out
in our constitution), has comprised the seven elected GP members of the CCG’s
Governing Body plus the Accountable Officer (or his deputy).
During 2017/18 this included:
• Dr Marc Rowland (Chair)
• Dr David Abraham (Senior Clinical Director)
• Dr Faruk Majid (Senior Clinical Director until 31st August then as Clinical
Director)
• Dr Jacky McLeod (Clinical Director until 31st August then as Senior Clinical
Director)
• Dr Angelika Razzaque (Clinical Director)
• Dr Sebastian Kalwij (Clinical Director)
• Dr Charles Gostling (Clinical Director)
• Dr Esther Appleby (Clinical Director from 1st March)
• Mr Martin Wilkinson (Accountable Officer)
The Governing Body during 2017/18 has included the members of the Clinical
Directors Committee shown above, the Chief Financial Officer, lay members,
registered nurse member, and secondary care doctor:
• Mr Tony Read (Chief Financial Officer)
• Mr Ray Warburton (Lay member, deputy chair)
• Ms Shelagh Kirkland (Lay member)
• Ms Anne Hooper (Lay member from 8th May)
• Ms Alison Browne (Registered nurse member)
• Dr Mark Hamilton (Secondary Care Doctor until 18th April)
• Prof Simon MacKenzie (Secondary Care Doctor from 1st August)

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2018/19
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 80
Committee(s), including Audit Committee The CCG’s Audit Committee comprised the following members during the year
ending 31st March 2018:
• Mr Ray Warburton (Chair)
• Dr Faruk Majid (until October 2017)
• Dr Jacky McLeod (from January 2018)
• Ms Shelagh Kirkland (Lay member)
• Ms Anne Hooper (Lay member from 8th May)
• Prof Simon MacKenzie (Secondary Care Doctor from 1st August)
Details of the members of other committees can be found in Annual Governance
Statement and further details of the Governing Body and Clinical Director’s
Committee can be found in the Remuneration and Staff Report.
Register of Interests
Lewisham CCG is committed to the principles of good governance, leading to open
and transparent decision making. We have therefore established a policy to manage
Conflict of Interests to ensure that decisions made by the CCG will be taken and
seen to be taken without any possibility of the influence of external or private
interests. Our updated policy that takes account of the latest statutory guidance and
was updated in June 2017.
A conflict of interest is defined as:
• A conflict between the private interests and the official responsibilities of a
person in a position of trust
• A set of conditions in which professional judgement concerning a primary
interest (such as patients' welfare or the validity of research) tends to be
unduly influenced by a secondary interest (such as financial gain)
• The creation of a set of circumstances where one party is favoured over
another by an inadvertent preferential interest
In line with our conflicts of interest policy, arrangements to seek and receive
declarations of interest and maintain appropriate Registers of Declared Interests and
Gifts and Hospitality have been put in place. We publish our register of interests on

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2018/19
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 81
our website which can be found at here, with the Gifts and Hospitality register found
on our website here.
Personal data related incidents Information relating to the disclosure of incidents involving data loss and
confidentiality breaches can be found in the Annual Governance Statement.
Statement of Disclosure to Auditors
Each individual who is a member of the CCG at the time the Members’ Report is
approved confirms:
• so far as the member is aware, there is no relevant audit information of
which the CCG’s auditor is unaware that would be relevant for the
purposes of their audit report
• the member has taken all the steps that they ought to have taken in order
to make him or herself aware of any relevant audit information and to
establish that the CCG’s auditor is aware of it.
Modern Slavery Act
NHS Lewisham CCG fully supports the Government’s objectives to eradicate
modern slavery and human trafficking but does not meet the requirements for
producing an annual Slavery and Human Trafficking Statement as set out in the
Modern Slavery Act 2015.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2018/19
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 82
Statement of Accountable Officer’s Responsibilities The National Health Service Act 2006 (as amended) states that each Clinical
Commissioning Group shall have an Accountable Officer and that Officer shall be
appointed by the NHS Commissioning Board (NHS England). NHS England has
appointed Martin Wilkinson to be the Accountable Officer of NHS Lewisham CCG
who held the position throughout 2017/18. Andrew Bland was appointed as
Accountable Officer with effect from 1st April 2018.
The responsibilities of an Accountable Officer are set out under the National Health
Service Act 2006 (as amended), Managing Public Money and in the Clinical
Commissioning Group Accountable Officer Appointment Letter. They include
responsibilities for:
• The propriety and regularity of the public finances for which the Accountable
Officer is answerable,
• For keeping proper accounting records (which disclose with reasonable
accuracy at any time the financial position of the Clinical Commissioning
Group and enable them to ensure that the accounts comply with the
requirements of the Accounts Direction),
• Such internal control as they determine is necessary to enable the preparation
of financial statements that are free from material misstatement, whether due
to fraud or error
• For safeguarding the Clinical Commissioning Group’s assets (and hence for
taking reasonable steps for the prevention and detection of fraud and other
irregularities).
• The relevant responsibilities of accounting officers under Managing Public
Money,
• Ensuring the CCG exercises its functions effectively, efficiently and
economically (in accordance with Section 14Q of the National Health Service
Act 2006 (as amended)) and with a view to securing continuous improvement
in the quality of services (in accordance with Section14R of the National
Health Service Act 2006 (as amended)),
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2018/19
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 83
• Ensuring that the CCG complies with its financial duties under Sections 223H
to 223J of the National Health Service Act 2006 (as amended).
Under the National Health Service Act 2006 (as amended), NHS England has
directed each Clinical Commissioning Group to prepare for each financial year
financial statements in the form and on the basis set out in the Accounts Direction.
The financial statements are prepared on an accruals basis and must give a true and
fair view of the state of affairs of the Clinical Commissioning Group and of its net
expenditure, changes in taxpayers’ equity and cash flows for the financial year.
In preparing the financial statements, the Accountable Officer is required to comply
with the requirements of the Group Accounting Manual issued by the Department of
Health and in particular to:
• Observe the Accounts Direction issued by NHS England, including the
relevant accounting and disclosure requirements, and apply suitable
accounting policies on a consistent basis;
• Make judgements and estimates on a reasonable basis;
• State whether applicable accounting standards as set out in the Group
Accounting Manual issued by the Department of Health have been
followed, and disclose and explain any material departures in the financial
statements; and,
• Assess the CCG’s ability to continue as a going concern, disclosing, as
applicable, matters related to going concern; and
• Use the going concern basis of accounting unless they have been informed by
the relevant national body of the intention to dissolve the CCG without the
transfer of its services to another public sector entity.
To the best of my knowledge and belief, and subject to the disclosures set out below,
I have properly discharged the responsibilities set out under the National Health
Service Act 2006 (as amended), Managing Public Money and in my Clinical
Commissioning Group Accountable Officer Appointment Letter.
Disclosures:
NHS England issued legal directions to help address long standing performance
problems with local urgent and emergency care services. Under these directions
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2018/19
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 84
from 1st September 2017 our responsibility for acute commissioning and contracting
has been temporarily transferred to Southwark CCG This also supported our
ambitions as a CCG and help us address areas found to require improvement in
2016/17. High quality healthcare and patient experience is the most important thing
to Lewisham CCG and we have worked closely with local NHS partners to ensure
that patients receive the very best standards from the NHS. The Integrated Contracts
Delivery Team (ICDT) hosted by Southwark CCG has provided regular performance
monitoring reports to our Integrated Governance Committee.
I also confirm that:
• as far as I am aware, there is no relevant audit information of which the
CCG’s auditors are unaware, and that as Accountable Officer, I have
taken all the steps that I ought to have taken to make myself aware of any
relevant audit information and to establish that the CCG’s auditors are
aware of that information.
• that the annual report and accounts as a whole is fair, balanced and
understandable and that I take personal responsibility for the annual
report and accounts and the judgments required for determining that it is
fair, balanced and understandable
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2018/19
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 85
Governance Statement
Introduction and context NHS Lewisham CCG is a body corporate established by NHS England on 1 April
2013 under the National Health Service Act 2006 (as amended).
The clinical commissioning group’s statutory functions are set out under the National
Health Service Act 2006 (as amended). The CCG’s general function is arranging the
provision of services for persons for the purposes of the health service in England.
The CCG is, in particular, required to arrange for the provision of certain health
services to such extent as it considers necessary to meet the reasonable
requirements of its local population.
As at 1 September 2017, the clinical commissioning group is subject to directions
from NHS England issued under Section 14Z21 of the National Health Service Act
2006 / as follows:
• NHS England issued legal directions to help address long standing
performance problems with local urgent and emergency care services.
Under these directions from 1st September 2017 our responsibility for
acute commissioning and contracting has been temporarily transferred to
Southwark CCG This also supported our ambitions as a CCG and help us
address areas found to require improvement in 2016/17. High quality
healthcare and patient experience is the most important thing to
Lewisham CCG and we have worked closely with local NHS partners to
ensure that patients receive the very best standards from the NHS
• https://www.england.nhs.uk/wp-content/uploads/2017/09/lewisham-ccg-
directions.pdf
Scope of responsibility
As Accountable Officer, I have responsibility for maintaining a sound system of
internal control that supports the achievement of the clinical commissioning group’s
policies, aims and objectives, whilst safeguarding the public funds and assets for
which I am personally responsible, in accordance with the responsibilities assigned

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2018/19
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 86
to me in Managing Public Money. I also acknowledge my responsibilities as set out
under the National Health Service Act 2006 (as amended) and in my Clinical
Commissioning Group Accountable Officer Appointment Letter.
I am responsible for ensuring that the clinical commissioning group is administered
prudently and economically and that resources are applied efficiently and effectively,
safeguarding financial propriety and regularity. I also have responsibility for
reviewing the effectiveness of the system of internal control within the clinical
commissioning group as set out in this governance statement.
Governance arrangements and effectiveness The main function of the governing body is to ensure that the group has made
appropriate arrangements for ensuring that it exercises its functions effectively,
efficiently and economically and complies with such generally accepted principles of
good governance as are relevant to it.
The Clinical Commissioning Group Governance Framework
Governing Body
The National Health Service Act 2006 (as amended), at paragraph 14L(2)(b) states:
“The main function of the governing body is to ensure that the group has made
appropriate arrangements for ensuring that it complies with such generally accepted
principles of good governance as are relevant to it.”
The CCG is governed by its constitution, signed by all the CCG’s members.
The constitution sets out the CCG’s governance structures and processes
including the role of the Governing Body and its individual members. During
2017/18 changes to the constitution were agreed by the CCG membership
that allowed for a change of managerial structure across South East London
and the provision of an additional Clinical Director.
Each member of the Governing Body shares responsibility as part of a team
to ensure that the group exercises its functions effectively, efficiently and
economically, with good governance and in accordance with the terms of its

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2018/19
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 87
constitution. Each Governing Body member brings their unique perspective,
informed by their skills, knowledge and experience.
During the year, the Governing Body:
• has approved the CCG’s operating plan and corporate objectives for
2017/18
• agreed the CCG’s budgets for the year
• approved the annual equalities report
• approved the sign-off of the Financial Control Environment
Assessment
• approved the refreshed Policy on Policies
• received and endorsed the plan for collaborative working across
South East London
• made arrangements to meet with the public before its formal
meetings
• received an integrated performance report, with additional exception
reports, through which the Governing Body has been advised of the
quality and safety of commissioned services and other performance
and financial issues. Where necessary the Governing Body has
taken appropriate action, for instance in critical areas of performance
such as cancer waits and A&E waits
• received and taken assurance that strategic risks were effectively
mitigated
• agreed to allow the extended contract for the NHS Walk-in Centre,
New Cross to expire on the 31st March 2018 and improve access
and provision to urgent and non-urgent primary care services
• received confirmation of ‘substantial’ assurance against the NHS
England Core Standards for Emergency Preparedness, Resilience
and Response (EPRR) from IGC.
• ensured that all conflicts of interest or potential conflicts of interest were
effectively managed.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2018/19
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 88
There were six meetings of the Governing Body held in public during the year. All of
the meetings were well attended and were quorate. The table below shows the
Governing Body members and attendance record. The Governing Body and all
other committees discussed below were supported by the CCG management team,
with appropriate attendance, as required.
*Ms Gwenda Scott on behalf of Danny Ruta
Absences are normally agreed with the Chair as members are frequently required to
attend other meetings.
The CCG is a membership organisation with a federated structure. The
organisational chart below shows the governance structures in place during the
financial year ending 31 March 2018.
Members Role May
July
Sept
Nov
Jan
Mar
Dr Marc Rowland CCG Chair Y Y Y Y Y Y
Mr Ray Warburton Lay Member, deputy chair Y Y Y Y Y Y Mr Martin Wilkinson Chief Officer Y Y Y Y Y Y
Mr Tony Read Chief Financial Officer Y X Y Y Y Y
Dr David Abraham Senior Clinical Director Y Y Y Y Y X Dr Faruk Majid Senior Clinical Director/Clinical Director X Y Y Y Y Y
Dr Jacqueline McLeod Clinical Director/Senior Clinical Director Y Y Y Y X Y
Dr Angelika Razzaque
Clinical Director Y X Y Y X Y
Dr Charles Gostling Clinical Director Y Y Y Y Y Y Dr Sebastian Kalwij Clinical Director Y Y Y Y Y Y
Dr Esther Appleby Clinical Director In post from 1/3/18 Y Ms Alison Browne Registered Nurse Y Y Y X Y X
Prof Simon Mackenzie Secondary Care Doctor In post from
1/8/17 X Y Y Y
Ms Anne Hooper Lay Member Y Y X Y Y Y
Ms Shelagh Kirkland Lay Member Y Y Y Y Y Y
Dr Magna Aidoo Representative, Healthwatch Lewisham Y Y X Y Y X Ms Aileen Buckton Executive Director Community Services,
London Borough of Lewisham Y Y Y Y Y X
Dr Simon Parton Lewisham LMC Chair Y Y X X Y X
Danny Ruta Public Health Director, London Borough of Lewisham
Y* Y Y Y X Y

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2018/19
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 89
The chart indicates the inter-relationship between membership bodies on the left (the Clinical
Directors’ Committee, Membership Forum and Neighbourhood Meetings) and the key governance
committees, headed by the Governing Body in the centre of the chart. The chart also shows the
important links with our partner organisations including the Lewisham Health and Well Being-
Board.
Clinical Directors Committee
The Clinical Directors Committee is a standing Committee of Lewisham CCG, made up of the GPs
elected to the Governing Body by the CCG members and including the members of the senior
management team. It has been the high level membership body to provide a formal connection,
transacted through the Membership Forum, between the on-going business of the Governing Body
and CCG member practices. It provides a vehicle in which the Clinical Directors seek and
consider ideas, views and concerns from members and galvanised their support and participation
to deliver the CCG’s objectives. During the year the work of the Clinical Directors Committee
included:
• influenced the development of the CCG’s strategic plans and priorities ensuring that the
membership’s views were incorporated

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2018/19
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 90
• promoted the CCG’s strategic plans with the membership ensuring engagement, support
and participation
• reviewed the progress against the Corporate Objectives
• assessed and reviewed QIPP and new ideas to achieve the QIPP target
• reviewed potential models for developing the local healthcare system
There were 22 meetings of the Clinical Directors Committee during the year. All of the meetings
were well attended. The table below shows the members and attendance record. The Clinical
Directors Committee was supported by the CCG management team, with appropriate attendance,
as required.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2018/19
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 91
Members Role Apr 6
th
Apr
20th
May
4th
May
25th
Jun 1st
Jun 15
th
Jul 6
th
Jul 20th
Aug 3
rd
Aug
17th
Sept
7th
Sept
21st
Oct 5
th
Oct 19
Nov
2N
D
Nov
16th
Dec
7th
Jan 4th
Jan
18th
Feb 1st
Feb
15th
Mar
1st
Dr Angelika Razzaque
Clinical Director
Y Y Y Y Y Y Y X Y Y Y X Y Y Y Y Y Y Y X Y Y
Dr David Abraham
Senior Clinical Director
Y Y Y Y Y Y Y Y Y Y X Y Y X Y Y Y Y Y Y Y Y
Dr Faruk Majid
Senior Clinical Director
Y Y Y Y Y Y X Y Y Y Y Y Y X Y Y Y Y X Y Y Y
Dr Jacky McLeod
Clinical Director
Y Y Y Y Y Y Y Y Y X Y Y Y X Y Y Y X Y Y Y Y
Dr Marc Rowland
Chair X Y Y Y Y X Y Y Y X Y Y Y Y Y Y Y Y X Y X Y
Dr Charles Gostling
Clinical Director
Y Y Y Y Y Y Y Y X Y Y Y Y Y Y Y Y Y Y X Y X
Dr Sebastian Kalwij
Clinical Director
Y Y Y Y Y X Y Y X X Y Y X Y Y Y Y Y Y Y Y Y
Mr Martin Wilkinson
Chief Officer
Y Y Y Y X X Y Y Y Y Y X Y Y Y Y Y X Y Y X Y
Dr Esther Appleby
Clinical Director
In post from 01/03/2018 Y
Absences are normally agreed with the Chair as members are frequently required to attend other meetings.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 92
Audit Committee
The committee was established to take an independent and objective view of the CCG’s financial
systems, compliance with laws and compliance with best practice in its arrangements for corporate
governance.
The committee has reflected on its work and had agreed that it goes about its business in an
organised, inclusive and accountable way. In 2017/18:
• its work programme followed a plan agreed at the start of the year
• it makes it clear to CCG management and staff what is required from them in the
preparation and running of meetings
• it meets in a private session with the CCG’s independent assurance providers at the end of
each meeting
• it reported the headlines of each meeting to the Governing Body, and minutes have also
been provided when they have been confirmed
During the year, the work of the Audit Committee included:
• approved the 2016/17 CCG Annual Report and Annual Accounts on behalf of the Governing
Body
• received the Head of Internal Audit Opinion for 2016/17
• agreed key performance indicators for External Audit and Internal Audit
• approved the Internal Audit plan for 2017/18 and commented on the reports of the reviews
• reviewed Service Auditor Reports
• approved the Counter Fraud Work Plan for 2017/2018 and commented on progress
• scrutinised and advised on the format and content of the Board Assurance Framework,
including deeper dives into specific areas.
• considered the CCG’s Financial Control Environment Self Assessment (FCEA) .
• Reviewed the CCG’s self-assessment against the Counter Fraud NHS Standards for
Commissioners and was updated on work undertaken since the assessment
• Reviewed the local security management workplan for 2017/18 and commented on
progress
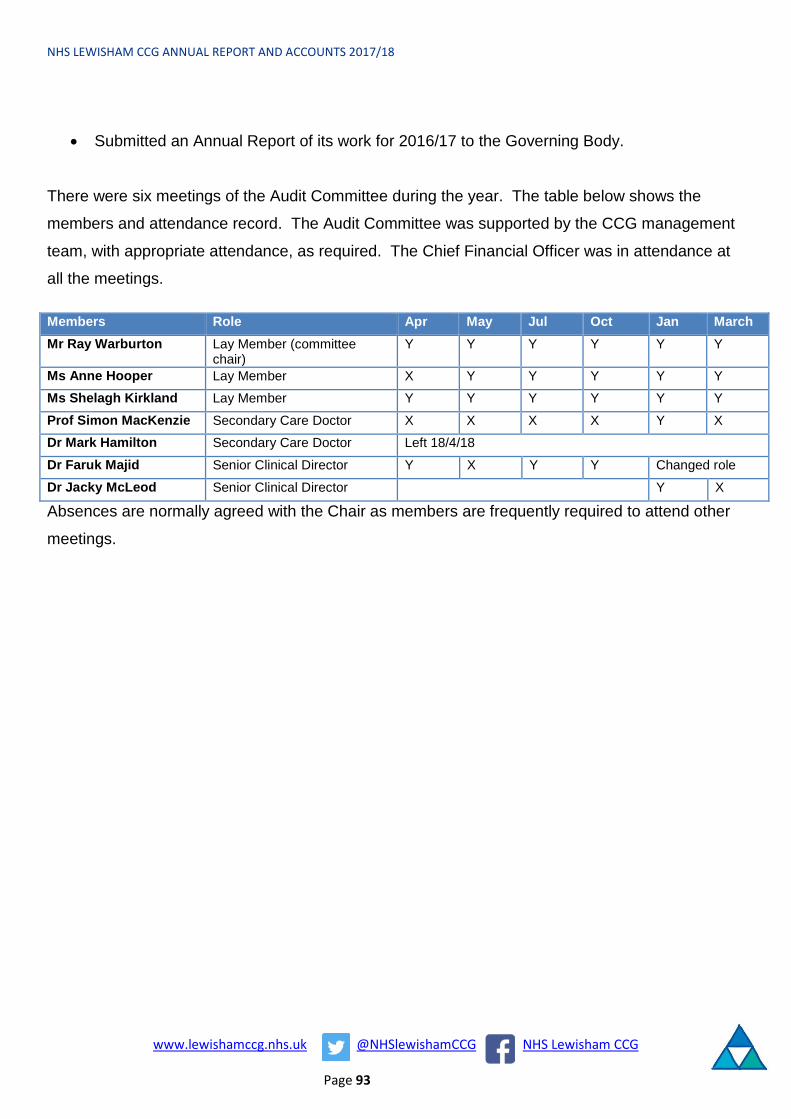
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 93
• Submitted an Annual Report of its work for 2016/17 to the Governing Body.
There were six meetings of the Audit Committee during the year. The table below shows the
members and attendance record. The Audit Committee was supported by the CCG management
team, with appropriate attendance, as required. The Chief Financial Officer was in attendance at
all the meetings.
Members Role Apr May Jul Oct Jan March Mr Ray Warburton Lay Member (committee
chair) Y Y Y Y Y Y
Ms Anne Hooper Lay Member X Y Y Y Y Y Ms Shelagh Kirkland Lay Member Y Y Y Y Y Y
Prof Simon MacKenzie Secondary Care Doctor X X X X Y X Dr Mark Hamilton Secondary Care Doctor Left 18/4/18
Dr Faruk Majid Senior Clinical Director Y X Y Y Changed role
Dr Jacky McLeod Senior Clinical Director Y X
Absences are normally agreed with the Chair as members are frequently required to attend other
meetings.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 94
Remuneration Committee
The Remuneration Committee is responsible for approving the terms and conditions, remuneration
and travelling or other allowances for Governing Body members, including pensions and gratuities
in addition to the terms and conditions of employment for all employees on Very Senior Manager
(VSM) grades.
During the year, the Remuneration Committee agreed levels of remuneration for Governing Body
members. During 2017/18 the Remuneration Committee also considered the structure and the
associated Job Descriptions for the collaborative working arrangements across South East
London, and approved the terms of conditions for the executive leadership roles.
There were four meetings of the Remuneration Committee during the year. The table below
shows the members and attendance record. The Remuneration Committee was supported by the
CCG management team, with appropriate attendance, as required. Due process was followed
when conflicts of interest occurred during meetings.
Members Role June October November December
Mr Ray Warburton Lay Member (committee chair)
Y Y Y Y
Ms Anne Hooper Lay Member X Y Y Y
Ms Shelagh Kirkland Lay Member Y Y Y Y
Prof Simon MacKenzie Secondary Care Doctor
Started 1/8/17 Y Y Y
Absences are normally agreed with the Chair as members are frequently required to attend other meetings.
Strategy and Development Workshop
The Strategy and Development Workshop was established to set and maintain the CCG’s strategic
direction for commissioning and to develop formal strategic and operational plans for approval by
the Governing Body.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 95
There were six meetings of the Strategy and Development Committee during the year. The table
below shows the members and attendance record. The Strategy and Development Committee
was supported by the CCG management team, with appropriate attendance, as required.
Members Role Apr Jun Aug Oct Dec Feb Dr David Abraham Senior Clinical Director
(committee chair) Y Y Y Y Y Y
Dr Marc Rowland CCG Chair X X X X Y Y
Mr Ray Warburton Lay Member Y Y Y Y Y Y
Mr Martin Wilkinson Chief Officer Y X Y Y Y Y Mr Tony Read Chief Financial Officer Y Y X Y X X
Dr Faruk Majid Senior Clinical Director/Clinical Director
Y Y Y Y X X
Dr Jacky McLeod Clinical Director/Senior Clinical Director
Y Y Y Y Y Y
Dr Angelika Razzaque Clinical Director Y Y Y Y Y Y Dr Sebastian Kalwij Clinical Director X Y X X Y Y
Dr Charles Gostling Clinical Director Y Y X Y Y X Ms Anne Hooper Lay Member Started
8/5/17 Y Y Y Y Y
Ms Shelagh Kirkland Lay Member Y Y Y Y Y Y
Ms Alison Browne Registered Nurse/Director of Nursing & Quality
Y Y Y Y X Y
Dr Mark Hamilton Secondary Care Doctor X Left 18/4/17
Prof Simon Mackenzie Secondary Care Doctor Started 1/8/17 X Y X Y Ms Susanna Masters Corporate Director Y X Y Y X X
Mr Charles Malcolm-Smith
Deputy Director (Strategy & Organisation Development)
Y Y Y Y Y Y
Absences are normally agreed with the Chair as members are frequently required to attend other
meetings.
During the year, the work of the Strategy and Development Workshop included:
• reviewing the CCG’s objectives and priorities for the coming year
• reviewing the investment case for population health information management system
• reviewing developments for health and care integration and development of community
based care in Lewisham
• reviewing the CCG’s progress against the Equality Delivery System (EDS2) goals and the
public sector equalities duties

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 96
• receiving the outcomes of the CCG stakeholder and staff surveys and organisational
development plans
Integrated Governance Committee
The Integrated Governance Committee was established to monitor the performance of
commissioned health services in all aspects and to monitor delivery of our operational plans in
year. The committee reviewed our position against key performance, quality and financial metrics,
and identified mitigating steps where delivery was off-track.
The Integrated Governance Committee received reports from a number of subgroups to monitor
performance against plans in detail and these included groups to monitor quality and information
governance.
There were 10 meetings of the Integrated Governance Committee during the year. The table
below shows the members and attendance record. The Integrated Governance Committee was
supported by the CCG management team with appropriate attendance as required.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 97
Absences are normally agreed with the Chair as members are frequently required to attend other
meetings.
During the year the work of the Integrated Governance Committee included:
• receiving the Corporate Objectives priorities for action for 2017/18
• monitoring the Board Assurance Framework against the achievement of the Corporate
Objectives
• receiving performance and exception reports against the NHS Constitutional Standards,
and in particular ensuring actions are undertaken on A&E performance, cancer waiting
times, and referral to treatment times
• monitoring financial performance
• monitoring performance of QIPP projects
• received confirmation of ‘substantial’ assurance against the NHS England Core Standards
for Emergency Preparedness, Resilience and Response (EPRR)
Finance and Investment Committee
The purpose of the Finance and Investment Committee is to maintain a detailed overview of the
CCG’s assets and resources in relation to the achievement of financial targets and business
objectives and the financial stability of the CCG. This includes:
• overseeing the development and maintenance of the CCG’s financial strategy
• reviewing and monitoring financial plans and their link to operational performance and
quality
• overseeing financial risk evaluation, measurement and management
• scrutiny and approval of business cases and oversight of the capital programme
• maintaining oversight of the key financial policies and other financial issues that may arise
There were 8 meetings of the Finance and Investment Committee during the year. The table
below shows the members and attendance record.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 98
Members Role May Jul Aug Sep Oct Dec Jan Feb Prof Simon MacKenzie
Secondary Care Doctor (committee chair)
Started 1/8/17 Y Y Y Y Y Y
Mr Ray Warburton
Lay Member Y Y Y Y Y Y Y Y
Mr Martin Wilkinson
Chief Officer Y Y Y Y X Y Y Y
Mr Tony Read Chief Financial Officer
Y X Y X Y Y Y Y
Dr David Abraham
Senior Clinical Director
Y X Y X X X Y X
Dr Faruk Majid Senior Clinical Director
Y Y Y Y X Change of roles
Dr Jacky McLeod
Senior Clinical Director
Y Y Y
Shelagh Kirkland
Lay Member Y∞ Y∞ Y∞ Y Y Y Y Y
Alison Browne Registered Nurse Y Y Y Y Y Y Y X
∞ Committee Chair
Absences are normally agreed with the Chair as members are frequently required to attend other
meetings.
During the year the committee:
• considered the business case and the KPIs for the Integrated Urgent Care programme
across South East London
• Assessed and discussed the QIPP Pipeline
• Considered the Planning Guidance for 2018

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 99
Public Engagement and Equalities Forum The Public Engagement and Equalities Forum was established in 2016/17 in order to strengthen
engagement in the CCG, support assurance for the Governing Body, and to monitor its impact on
the work of the organisation. Equalities aspects in public engagement are also a major
consideration for the group.
There were 6 meetings of the Public Engagement & Equalities Forum during the year. The table
below shows the members and attendance record.
Members Role May June Sept Oct Dec Feb
Ms Anne Hooper Lay Member (committee chair) Y X Y Y Y Y
Dr Angelika Razzaque Clinical Director Y X Y Y Y X
Mr Charles Malcolm-Smith Deputy Director (Strategy & OD) x Y Y Y Y Y
Dr Faruk Majid Clinical Director Y Y Y Y Y X
Folake Segun Healthwatch Representative Y Y Y Y Y Y
Russell Cartwright Head of Communications & Engagement Y Y Y Y Y Y
Susanna Masters Corporate Director Y Y Y X X Y
During the year the Forum:
• reviewed the public engagement priorities for 2017/18.
• Reviewed the public consultation on the Walk in Centre
• Reviewed the public consultation on the proposed changes to prescribing;
• Reviewed the plans for the CCG Annual General Meeting

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 100
Primary Care Commissioning Committee
The Primary Care Commissioning Committee was established in accordance with statutory
provisions from NHS England to enable the membership of the committee to make collective
decisions on the review, planning and procurement of primary care services in Lewisham, under
delegated authority from NHS England.
There were 5 meetings of the Primary Care Commissioning Committee during the year. The table
below shows the ‘voting’ members and attendance record.
Members Role Apr June Aug Oct Feb Ms Shelagh Kirkland Lay Member (committee chair) Y Y Y Y Y
Dr Marc Rowland CCG Chair Y Y X Y Y Mr Ray Warburton Lay Member Y Y Y Y Y
Mr Martin Wilkinson Chief Officer Y X Y Y Y
Mr Tony Read Chief Financial Officer Y Y Y Y X Dr Faruk Majid Clinical Director X Y Y Y Y
Dr Jacky McLeod Clinical Director Y Y X Y Y Ms Anne Hooper Lay Member Started
8/5/17 Y Y Y Y
Ms Alison Browne Registered Nurse Y X X X X
Ms Diana Braithwaite Commissioning Director Y Y Y X Y
The Primary Care Commissioning Care Committee met for the first time in April 2017 and agreed
its governance arrangements and terms of reference in line with NHS England guidelines for level
3 delegated commissioners.. The key decision areas addressed by the committee during the year
included:
• Personal Medical Service (PMS) Commissioning Intentions: The committee approved the
commissioning intentions for the PMS premium for GP practices.
• Primary Care Equalities Objectives: Received an update on delivery of the 3 year Primary
Care Equalities Objectives Programme.
• GP Five Year Forward View: A review of progress on delivering the GP Five Year Forward
View.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 101
• Care Quality Commission (CQC): The committee considered contractual actions following
CQC inspections of GP practices.
• Incentive Schemes: The committee approved the Engagement in Clinical Commissioning
Improvement and the Primary Care Incentive & Qaulity Incentive Schemes.
• Practice Mergers: The committee approved the following mergers for Winlaton Surgery and
South Lewisham Group Practice; and Baring Road Medical Centre and the Rushey Green
Group Practice.
• Estates Developments: The committee approved the relocation of the New Cross Health
Centre to the Waldron Health Centre and expansion of the Amersham Vale Training
Practice estate at the Waldron Health Centre.
• Primary Care Operational Group: The Committee received updates from the chair of the
operational group.
Full meeting papers for 17/18 can be found on our website
UK Corporate Governance Code We are not required to comply with the UK Corporate Governance Code. However, we have
reported on our Corporate Governance arrangements by drawing upon best practice available,
including those aspects of the UK Corporate Governance Code we consider to be relevant to the
CCG and best practice.
Discharge of Statutory Functions In light of recommendations of the 1983 Harris Review, the clinical commissioning group has
reviewed all of the statutory duties and powers conferred on it by the National Health Service Act
2006 (as amended) and other associated legislative and regulations. As a result, I can confirm
that the clinical commissioning group is clear about the legislative requirements associated with
each of the statutory functions for which it is responsible, including any restrictions on delegation of
those functions.
Responsibility for each duty and power has been clearly allocated to a lead Director. Directorates
have confirmed that their structures provide the necessary capability and capacity to undertake all
of the clinical commissioning group’s statutory duties.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 102
Risk management arrangements and effectiveness In line with good practice, we adopted a risk management process which has been designed to
provide continuous identification, assessment, control, communication and monitoring of risk with
clear escalation processes. When faced by risks, we take a positive and controlled approach to
risk management, acceptable to the Governing Body, as described below.
Risks to achieving our objectives and business plans were identified at project or programme
board meetings, at assurance committees when inadequate or no assurances were given or at
routine business meetings. Wherever a risk was identified the escalation route was the same.
Project and programme risks were assessed and managed at the project or programme
management level. Where risks were considered to have an impact on our corporate objectives,
these were escalated to the Risk Management Group. The role of the Risk Management Group
has been to:
• review and evaluate new and amended risks and instruct that the Risk Register is updated
accordingly
• review the Board Assurance Framework (BAF) by scrutinising the existing controls and
assurances ensuring that the register is an accurate summary of the risks to the
organisation.
“Risk owners” at Director or senior manager level were assigned to all risks and risk owners have
been responsible for identifying controls and actions to mitigate risks to target levels. Controls
have included the development of policies, for example for the management of conflicts of interest,
mandatory training programmes, or actions to mitigate risks to achieving our corporate objectives.
All this information has been collated over the year in the Board Assurance Framework which is
discussed at each meeting of the Governing Body.
The management of risk is the duty of all staff, inclusive of the reporting of incidents and near-
misses in accordance with the policies and procedures in place. All managers are accountable for
the day-to-day management of risks within their areas of responsibility, ensuring assessments are
undertaken and risk registers updated as appropriate. Directors are responsible for providing risk
management leadership and sponsorship across the CCG.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 103
The risk controls in place, enable us to determine whether the risks are being managed effectively
through:
• policies, procedures and guidelines
• training and staff development
• equipment and facilities
• staff competency
• induction programme
• any other measures deemed necessary
The Board Assurance Framework has been improved and developed during the year following
discussions with the Audit Committee, the Integrated Governance Committee and Governing Body
members. Improvements have included work to identify mitigating actions which are SMART with
action owners and timelines for expected delivery.
Equality Impact Assessments (EIA) are a core part of policy, strategy and project development
within Lewisham CCG. The NHS Lewisham CCG Policy on Policies ensures that there is a
regulated approach to the development of policies and procedural documents. It is a policy
requirement for that all policy and procedural documents developed by the CCG describe how they
meet the Public Sector Equality Duty.
As a key partner, Healthwatch Lewisham provided a representative voice of patients from the
many diverse communities in Lewisham into our risk management processes. Their involvement
in the CCG structure included membership of our Public Engagement and Equalities Forum, and
our Integrated Governance Committee, which reviewed ‘quality’ in respect of patient safety, clinical
effectiveness and patient experience of the services we commissioned for our population.
Risk Assessment Our Risk Management Framework sets out our risk assessment process and is based on the
National Patient Safety Advice (NPSA) guidance and aligned to the adopted internationally
recognised AS/NZS 4360:1999 guideline which provides a model for identifying, assessing and
controlling risks. Further information on how the CCG manages the principles of Risk
Management, can be found under the Risk Management Framework section above.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 104
Risks in relation to governance, risk management and internal control were identified and
evaluated by the Risk Management Group early in the year. These risks have been incorporated
into the Governing Body Board Assurance Framework (BAF) and the CCG’s Risk Register for
scrutiny.
The BAF broadly provides assurance of the controls in place that mitigate the risks that may
prevent Lewisham CCG meeting its annual Strategic Objectives. The ‘heat map’ below is used to
show the distribution of all the 39 risks on the CCG Risk Register. Throughout 2017/18 the
Governing Body has received detailed reports of the controls in place, assurances given and
further actions being taken to manage or mitigate those risks that have a residual score of 12 or
above (score of Likelihood multiplied by Impact). These reports are contained within the papers
for our Governing Body meetings (found on our website here)
During the 2017/18, four risks were assessed at the end of the year to have a ‘very high’ rating in
March 2018).
These were:
• Cancer waiting times; Cancer 62 days (Risk of not achieving the access
performance standards for timely access to cancer treatment (as measured by the
62 day standard for 62 days from GP referral to treatment))

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 105
Heat Map - June 2017 Current Ratings
Almost Certain5
Likely4
No. of Risks = 5Risk ID: 8, 78, 80,
81, 83
Possible3
No. of Risks = 1Risk ID: 21
No. of Risks = 4Risk ID: 30, 38,
84, 87No. of Risks = 3
Risk ID: 53, 77, 86
Unlikely2
No. of Risks = 2Risk ID: 59, 88
No. of Risks = 6Risk ID: 22, 25, 39, 41, 63, 74
No. of Risks = 1Risk ID: 90,
Rare1
Risk MatrixNegligible
1Minor
2Moderate
3Major
4Catastrophic
5
Total Number of Risks = 22
Likelihood
Impact
• A&E: System wide delivery (The improvement programme across Lewisham,
Greenwich and Bexley local system does not deliver the anticipated outcomes for
our patients and local populations at the pace required)
• Improved community upstream and Supported Discharge Initiatives (Failure to
manage the flow of patients through the hospital who are fit for discharge)
• QIPP - Planning for 2018/19 and 2019/20 (If the CCG does not deliver a credible
QIPP programme this will jeopardise delivery of the financial control total for future
years).
In response to this risk rating the Governing Body received detailed action plans for how the CCG
would work in conjunction with partners to reduce these.
The ‘heatmap’ tables below show the distribution of all risks identified through the Corporate Risk
Register, using “current risk score”, comparing the initial assessment of risk made in Quarter 1
(April-June 2017) to that made at the end of the year in Quarter 4 (January-March 2018).
2017/18 Q1 Risk Assessment

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 106
2017/18 Q4 Risk Assessment
This demonstrates that during the year, the CCG assessed that the number of risks to the
achievement of its corporate objectives increased. A number of these risks did decrease during
the year, but the environment that the CCG was working in relation to the performance of our main
acute providers and the financial position, resulted in four risks remaining at a very high level.
Other sources of assurance
Internal Control Framework
A system of internal control is the set of processes and procedures in place in the clinical
commissioning group to ensure it delivers its policies, aims and objectives. It is designed to
identify and prioritise the risks, to evaluate the likelihood of those risks being realised and the
impact should they be realised, and to manage them efficiently, effectively and economically.
The system of internal control allows risk to be managed to a reasonable level rather than
eliminating all risk; it can therefore only provide reasonable and not absolute assurance of
effectiveness.
A system of internal control is the set of processes and procedures in place in the CCG to ensure
that it delivers its policies, aims and objectives. It is designed to identify and prioritise the risks, to
evaluate the likelihood of those risks being realised, the impact should they be realised, and to
manage them efficiently, effectively and economically.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 107
The system of internal control allows risk to be managed to a reasonable level rather than
eliminating all risk; it can therefore only provide reasonable and not absolute assurance of
effectiveness.
The chart below illustrates how risks have been identified and escalated through the organisation
to the Governing Body. The bottom of the chart includes a table which shows the type of risk,
shown here as the “risk category,” the committee or work group where detailed review of the risk
and controls took place and the main assurance committee that held oversight of the risk. The
main body of the chart shows how risks are escalated to the Governing Body.
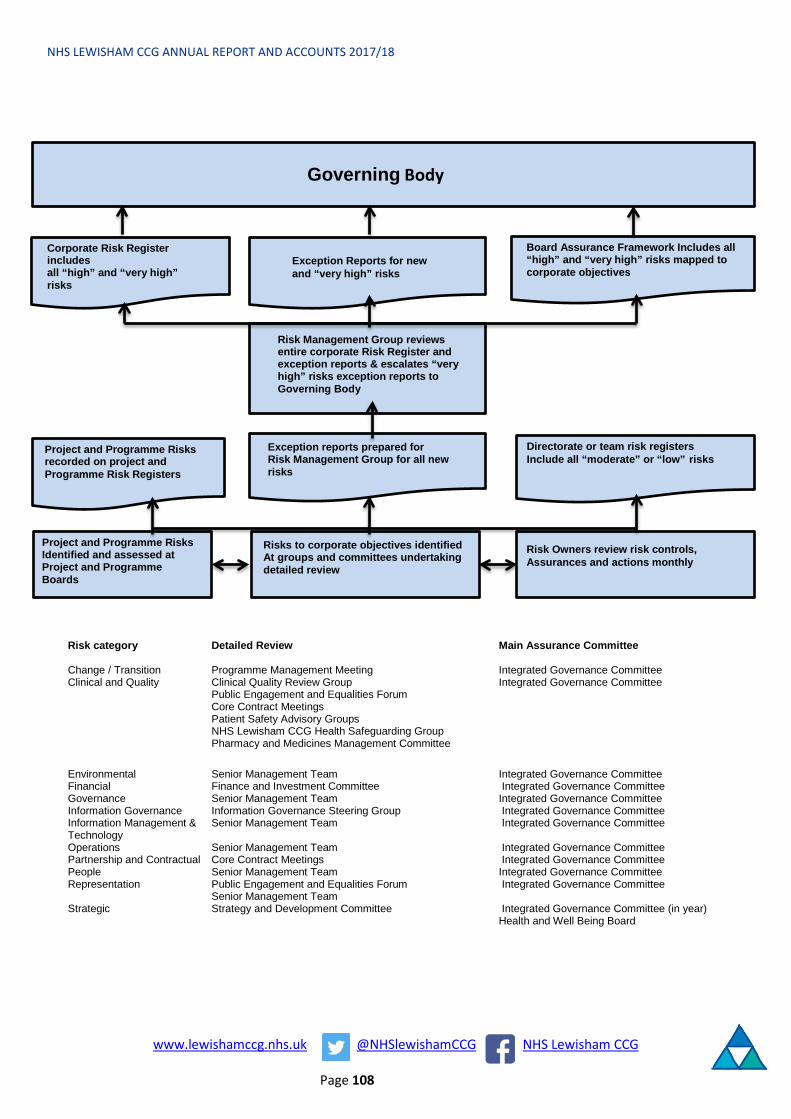
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 108
Governing Body
Corporate Risk Register includesall “high” and “very high” risks
Exception Reports for new and “very high” risks
Board Assurance Framework Includes all “high” and “very high” risks mapped to corporate objectives
Risk Management Group reviews entire corporate Risk Register and exception reports & escalates “very high” risks exception reports to Governing Body
Project and Programme Risks recorded on project and Programme Risk Registers
Exception reports prepared forRisk Management Group for all new risks
Directorate or team risk registersInclude all “moderate” or “low” risks
Project and Programme RisksIdentified and assessed at Project and Programme Boards
Risks to corporate objectives identifiedAt groups and committees undertakingdetailed review
Risk Owners review risk controls, Assurances and actions monthly
Risk category Detailed Review Main Assurance Committee Change / Transition Programme Management Meeting Integrated Governance CommitteeClinical and Quality Clinical Quality Review Group Integrated Governance Committee
Public Engagement and Equalities Forum Core Contract Meetings Patient Safety Advisory Groups NHS Lewisham CCG Health Safeguarding GroupPharmacy and Medicines Management Committee
Environmental Senior Management Team Integrated Governance CommitteeFinancial Finance and Investment Committee Integrated Governance CommitteeGovernance Senior Management Team Integrated Governance CommitteeInformation Governance Information Governance Steering Group Integrated Governance CommitteeInformation Management & Senior Management Team Integrated Governance CommitteeTechnology Operations Senior Management Team Integrated Governance CommitteePartnership and Contractual Core Contract Meetings Integrated Governance CommitteePeople Senior Management Team Integrated Governance CommitteeRepresentation Public Engagement and Equalities Forum Integrated Governance Committee
Senior Management TeamStrategic Strategy and Development Committee Integrated Governance Committee (in year)
Health and Well Being Board

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 109
Annual audit of conflicts of interest management The revised statutory guidance on managing conflicts of interest for CCGs (published June 2016
and updated in 2017) requires CCGs to undertake an annual internal audit of conflicts of interest
management. To support CCGs to undertake this task, NHS England has published a template
audit framework.
An audit of Conflicts of Interest at Lewisham CCG was undertaken as part of the approved Internal
Audit periodic plan for 2017/18.
A conflict of interests (CoI) is "a set of circumstances by which a reasonable person would
consider that an individual's ability to apply judgement or act, in the context of delivering,
commissioning, or assuring taxpayer funded health and care services is, or could be, impaired or
influenced by another interest they hold". It is therefore important the CCG acts proactively to
manage interests, both potential and actual, to give the public confidence that any decisions made
by the CCG are fair and transparent.
Lewisham CCG updated its Conflicts of Interest Policy in August 2017 in accordance with the
NHSE Managing CoI: Revised Statutory Guidance for CCGs which was published in June 2017.
The policy applies to all CCG staff, Governing Body (GB) members and GP partners, and outlines
the roles and responsibilities, and processes and arrangements in place for managing conflicts of
interests.
A Conflicts of Interest Guardian is in place at the CCG who also holds the position of Chair of the
Audit Committee (Ray Warburton, Lay Member). There are three lay members on the CCG GB
whose roles are to provide an independent voice in the decision-making process.
It is a requirement of all CCG staff, GB members and GP Partners to declare any conflicts of
interests at the beginning of their appointment and regularly (annually or where circumstances
change); a Register of Interest (ROI) is maintained to capture these centrally. Furthermore,
declarations of interest are a standing agenda item at the beginning of the GB and all Committee
meetings. The CCG further maintains a Register of Gifts and Hospitality and a Procurement
Opportunities Awards Register.
To make staff across the CCGs more aware of their duty to make true declarations, NHS England
has developed an online training module that was launched in January 2018 and is mandatory for
all our staff to complete by the end of May 2018.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 110
Taking account of the issues identified, the Governing Body took partial assurance that the
controls to manage this risk are suitably designed and consistently applied. Action is needed to
strengthen the control framework to manage the identified risk(s). The Auditors identified one high
and four medium priority issues in relation to the design and application of the control framework
with three low priority issues and included:
• Completeness: Not all staff were found within the registers. Additionally, Declaration forms
were not all completed consistently.
• An inconsistency was found out of a sample of ten individuals tested, where a live
directorship was shown on the tracker for an individual but this detail was not held by the
CCG
• The CCG’s Procurement Opportunities Awards Register did not include individuals involved
in the decision-making process, and the governance group where the decision was made
(and the date).
• The Procurement Opportunities Awards Register was not being reviewed by any
governance group
All of the recommendations made by the Auditors were reviewed and completed within the
financial year.
Data Quality
In line with the need to know principles set out in the Caldicott 2 Information Governance Review
Report, the CCG ensures that information presented to the Governing Body and other governance
forums does not identify individuals and is fully anonymised.
Senior management diligently reviews information to be set out in governance and decision
making information prior to consideration and presentation to the relevant governance forums.
The quality of information that the Governing Body and other governance forums receive to
consider and direct decision making is also assured through the service level specification
arrangements with the South East Commissioning Support Unit and the use of contractual
arrangements with the commissioned providers.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 111
Information Governance The NHS Information Governance Framework sets the processes and procedures by which the
NHS handles information about patients and employees, in particular personal identifiable
information. The NHS Information Governance Framework is supported by an information
governance toolkit and the annual submission process provides assurances to the clinical
commissioning group, other organisations and to individuals that personal information is dealt with
legally, securely, efficiently and effectively
We place high importance on ensuring there are robust information governance systems and
processes in place to help protect patient and corporate information. We have established an
information governance management framework and are developing / have developed information
governance processes and procedures in line with the information governance toolkit. We have
ensured all staff undertake annual information governance training and have implemented a staff
information governance handbook to ensure staff are aware of their information governance roles
and responsibilities.
There are processes in place for incident reporting and investigation of serious incidents. We are
developing information risk assessment and management procedures and a programme will be
established to fully embed an information risk culture throughout the organisation against identified
risks.
A Senior Information Risk Owner (SIRO) is accountable for leading the information risk culture and
approach of the CCG has been put in place in line with NHS requirements. The Chief Financial
Officer of the CCG fulfils the SIRO role.
The Senior Information Risk Officer (SIRO) is responsible for:
• Understanding how the strategic business goals of the CCG may be impacted by
information risks: acting as an advocate for information risks on the Governing Body and in
internal discussions
• Ensuring the Governing Body is adequately briefed on information risk issues
• Overseeing the development of an Information Risk Policy, and a strategy for implementing
the policy within the CCG’s Information Governance Framework
• Reviewing the annual information risk assessment to support and inform the Annual
Governance Statement
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 112
• Taking ownership of risk assessment processes for information risks, supported by the
Information Governance Manager, Information Security Lead, Records Manager and the
Caldicott Guardian
• Reviewing and agreeing action in respect of identified information risks.
• Providing a focal point for the resolution and/or discussion of information risk issues
A separate Caldicott Guardian role also acts as the conscience of the organisation regarding
confidentiality and privacy matters affecting individual persons and to avoid a potential conflict of
interest with the organisational responsibilities of the SIRO. The Director of Nursing & Quality fulfils
the Caldicott Guardian role.
For the year 2017/18 the CCG has satisfied the requirements of the Information Governance
Toolkit and achieved an overall score of 100%, compare to the 87% score in 2016/17.
Business Critical Models
NHS England recognises the importance of quality assurance across the full range of its analytical
work. In partnership with analysts in the Department of Health we have developed an approach
that is fully consistent with the recommendations in Sir Nicholas Macpherson's review of quality
assurance of government models. The framework includes a programme of mandatory workshops
for NHS England analysts, which highlights the importance of quality assurance across the full
range of analytical work.
The Macpherson Report on the review of quality assurance (QA) of Government Analytical Models
set out the components of best practice in QA making eight key recommendations. We recognise
the importance of this and have been working with partners to ensure appropriate quality
assurance processes are in place across its analytical work.
For 2017/18 Lewisham CCG has continued to work with other CCGs and NHS providers in south
east London, through the Sustainability and Transformation Partnership (STP), to develop the
business and financial modelling for the five year strategic plan. The modelling is led through
South East London Project Management Organisation (PMO) and reports back to the South East
London Finance Leads Group. The group includes Directors of Finance and Chief Financial
Officers from all organisations within the STP. The group is chaired by the Chief Financial Officer

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 113
of Southwark CCG, who acts as the Senior Responsible Officer for the development of the model.
The output of the financial modelling is reviewed by a varied number of stakeholders from different
disciplines, both internal and external, and underpins the modelling of the impacts of service
changes over the next five years.
Locally, Lewisham CCG has developed a number of business and financial models which underpin
areas such as local financial planning, QIPP delivery and service transformation. The identified
senior responsible officer is the Chief Financial Officer, who ensures that there are effective
processes underpinning the modelling, including appropriate guidance, documentation and
training, as well as sharing best practice. This includes ensuring that appropriate assurance
processes are in place to govern the robustness of any modelling.
Control Issues No significant internal control issues have been identified
Review of economy, efficiency & effectiveness of the use of resources
In year monitoring of performance against our plans, in terms of quality, finance and other
performance standards (e.g. NHS constitutional standards) has been carried out by our Integrated
Governance Committee. This includes assuring that projects and programmes are delivering
economic, effective and high quality services.
The Governing Body’s scrutiny over finance, investment and procurement was strengthened
through the introduction of the Finance and Investment Committee. The Committee oversees the
CCG’s capital expenditure, investment decisions and associated procurements and management
of financial risk.
Under the CCG Improvement and Assessment Framework indicators leadership ratings are
reviewed on a quarterly basis, the latest available results (to the end of December 2017) show that
the CCG has improved from red to amber for the Quality of Leadership. Year end results for the
Improvement and Assessment Framework are published by NHS England.
Counter fraud arrangements We contract an Accredited Counter Fraud Specialist to provide the full range of anti-crime work
that is proportionate to the risks identified and fully compliant with the NHS Standards for

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 114
Commissioners. The annual work-plan is developed from risks identified through the counter fraud
risk assessment and discussions with key staff within the CCG. The annual work-plan is agreed
with the Chief Financial Officer and ratified by the Audit Committee. Progress is regularly reported
to the Chief Financial Officer and the Audit Committee. The Audit Committee reviews the results
of the CCG annual self-assessment against the NHS Counter Fraud Standards for
Commissioners. The Audit Committee monitors progress on remedial actions against areas of
non-compliance or following an NHS Protect Quality Inspection.
The Accredited Counter Fraud specialists also delivered training to staff, which complies with the
CCG Mandatory Training requirements.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 115
Head of Internal Audit Opinion Following completion of the planned audit work for the financial year for the clinical commissioning
group, the Head of Internal Audit issued an independent and objective opinion on the adequacy
and effectiveness of the clinical commissioning group’s system of risk management, governance
and internal control. The Head of Internal Audit concluded that:
This document provides our annual internal audit opinion for 2017/18. Our list of opinions is provided in Appendix A.
1.1 The opinion For the 12 months ended 31 March 2018, the head of internal audit opinion for Lewisham Clinical Commissioning Group is as follows:
Head of internal audit opinion 2017/18
The enhancements referred to are primarily due to our findings from our Conflicts of Interest, Continuing Healthcare and Cyber Security reviews. For Conflicts of Interest, the Register of Interest and/or Declaration of Interest forms were not always fully accurate and complete, and there were improvements required in relation to the Procurement Awards Opportunities Register.
For Continuing Healthcare, the main improvements were required in relation to completion of checklists, provider contracts, approval of providers selected and compliance to decision timelines. There were also further enhancements in relation to reviewing the Continuing Healthcare QIPP Recovery Plan.
For our Cyber Security review we were unable to validate a number of core controls as operating effectively to meet best practice standards. We conducted our review in conjunction with the NEL Commissioning Support Unit which have been agreed with Management to strengthen the control environment. We are assured that by the time of issuing this opinion many of these control
In accordance with Public Sector Internal Audit Standards, the Head of Internal Audit is required to provide an annual opinion, based upon and limited to the work performed, on the overall adequacy and effectiveness of the organisation’s risk management, control and governance processes. The opinion should contribute to the organisation's annual governance statement.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 116
improvements have already been put in place and will continue to follow up on the implementation of the remaining actions and report back to the Audit Committee.
Please see appendix A for the full range of annual opinions available to us in preparing this report and opinion.
1.2 Scope and limitations of our work The formation of our opinion is achieved through a risk-based plan of work, agreed with management and approved by the audit committee. Our opinion is subject to inherent limitations, as detailed below:
• the opinion does not imply that internal audit has reviewed all risks and assurances relatingto the organisation;
• the opinion is substantially derived from the conduct of risk-based plans generated from arobust and organisation-led assurance framework. As such, the assurance framework isone component that the board takes into account in making its annual governancestatement (AGS);
• the opinion is based on the findings and conclusions from the work undertaken, the scopeof which has been agreed with management;
• the opinion is based on the testing we have undertaken, which was limited to the area beingaudited, as detailed in the agreed audit scope;
• where strong levels of control have been identified, there are still instances where thesemay not always be effective. This may be due to human error, incorrect managementjudgement, management override, controls being by-passed or a reduction in compliance;
• due to the limited scope of our audits, there may be weaknesses in the control systemwhich we are not aware of, or which were not brought to attention; and
• it remains management’s responsibility to develop and maintain a sound system of riskmanagement, internal control and governance, and for the prevention and detection ofmaterial errors, loss or fraud. The work of internal audit should not be seen as a substitutefor management’s responsibilities around the design and effective operation of thesesystems.
1.3 Factors and findings which have informed our opinion We have issued assurance opinions in relation to the following reviews:
• Financial Planning and QIPP Delivery (Substantial Assurance)• Risk Management and Board Assurance Framework (Substantial Assurance)• Primary Care Delegated Commissioning (Reasonable Assurance)• Procurement (Reasonable Assurance)
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 117
• Information Governance Toolkit (Advisory)
We raised Partial Assurance for the following reviews during 2017/18:
Conflicts of Interest
We identified that there were individuals not included in the Register of Interest, and instances where Declaration of Interest forms were either not fully complete, not signed by the individual / counter signed, and the interest and period it related to were not accurately reflected on the Register of Interests. In addition, we also found the Procurement Awards Opportunities Register did not document those individuals and governance groups involved in the procurement decision, and the Register was not reviewed by an allocated governance group on a periodic basis. Those management actions agreed for implementation prior to 31 March were all confirmed as implemented.
Continuing Healthcare
Our review highlighted that there were instances where checklists, and provider contracts were not in place, and fast track decisions and non-fast track decisions took longer than the target time for both (target: two days and 28 working days respectively). We also found that where providers were not selected from the approved list, there was not always evidence of approval. Furthermore, there was a QIPP Continuing Healthcare Recovery Plan in place, however this had not been discussed at the Executive Board meeting at the time of the review. We confirmed that all of the medium and high priority issues raised had been satisfactorily implemented by 31 March.
Joint working across South East London - Cyber Assurance
An advisory audit of Cyber Security was undertaken as part of the 2017/18 approved internal audit periodic plans for Lambeth, Southwark, Lewisham and Greenwich CCGs.
As a part of this review testing was conducted on the NHSLOCAL domain (used by Lambeth, Southwark, and Lewisham CCGs). Work was conducted at NEL Commissioning Support Unit.
Based upon the evidence available at the time of our fieldwork, we were able to agree that 21 of the 34 requirements for the five Cyber Essentials control themes had evidence to support the self-assessment that controls are established. Of the remaining 13 requirements there was one where we ‘Agree not fully implemented’, six where ‘Evidence does not fully support the self-assessment score’, one ‘Not applicable’, and five where work has ‘Not Started’; the 13 weaknesses are across the various control themes, including; boundary firewalls and internet gateways, secure configuration, access control, patch management.
The validated self-assessment scores generate an overall status of “Working Towards Implementation for the CSU’s implementation of Cyber Essentials” for this domain.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 118
As a part of this review, 11 ‘Medium’ management actions have been raised specific to the applicable NHSLOCAL domain. Management have agreed actions to resolve issues identified and we will continue to follow-up management actions as they become due and communicate the results of our work at the Audit Committee meetings.
We have an agreed set of actions for all finalised reports, and we are currently undertaking follow up for these agreed actions to confirm implementation. The results of this exercise will be included in the final Head of Internal Audit opinion.
1.4 Working with other assurance providers We have reviewed the Service Auditor Report for National Shared Business Services, who provide financial transactional support to the CCG, via its contract with NHS England. No notable exceptions were reported.
The Service Auditor Report for NHS Digital did not raise any exceptions. NHS Digital (the trading name of the “Health and Social Care Information Centre”) provides IT services as part of the end to end service alongside other organisations to support processing of NHS payments and deductions to providers of general practice (“GP”) services in England. The service auditor report was for the year ending 31 March.
We reviewed the Service Auditor Reports for Capita, who process payments to providers of general practice via a contract with NHS England, from whom the CCG has delegated primary care commissioning responsibilities. Whilst there has been some improvement in the number of control exceptions, there remained seven out of sixteen key controls assessed as suitably designed but not appropriately complied with over the period October 2017 to March 2018. Management action plans are in place to remedy the issues identified.
We have reviewed the Service Auditor Report for NEL Commissioning Support Unit, who provide some financial and payroll services to the CCG. We reviewed reports covering the eleven months to 28 February 2018 and the accompanying bridging letter to take the period covered up to 31 March 2018. Whilst we noted a number of exceptions were identified, we do not consider amongst these there are any which represent a significant risk to the CCG’s control environment.
We have liaised with External Audit and the Local Counter Fraud Specialist as appropriate.
1.5 Topics judged relevant for consideration as part of the annual governance statement Based on the work we have undertaken on the CCG’s system on internal control, we do not consider that within these areas there are any issues that need to be flagged as significant control issues within the Annual Governance Statement (AGS). However, we would expect the CCG to consider in the formulation of the AGS the internal control weaknesses identified within our partial assurance opinions and cyber security report summarised above, along with the actions being taken to address the issues identified.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 119
Appendix A: Annual opinions The following shows the full range of opinions available to us within our internal audit methodology to provide you with context regarding your draft internal audit opinion.
Annual opinions Factors influencing our opinion
The factors which are considered when influencing our opinion are:
• inherent risk in thearea being audited;
• Limitations in theindividual auditassignments
• The adequacy andeffectiveness of therisk managementand / or governancecontrol framework
• The impact ofweakness identified
• The level of riskexposure
• The response tomanagementactions raised andtimeliness of actionstaken
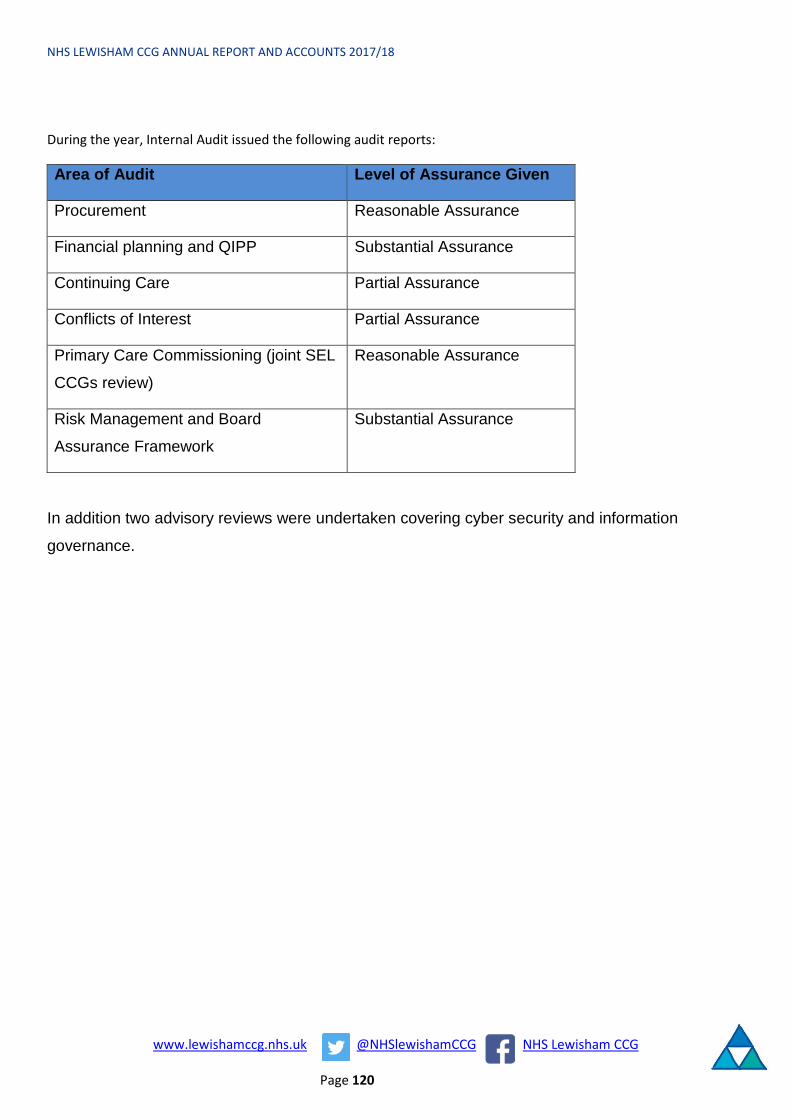
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 120
During the year, Internal Audit issued the following audit reports:
Area of Audit Level of Assurance Given
Procurement Reasonable Assurance
Financial planning and QIPP Substantial Assurance
Continuing Care Partial Assurance
Conflicts of Interest Partial Assurance
Primary Care Commissioning (joint SEL
CCGs review)
Reasonable Assurance
Risk Management and Board
Assurance Framework
Substantial Assurance
In addition two advisory reviews were undertaken covering cyber security and information
governance.
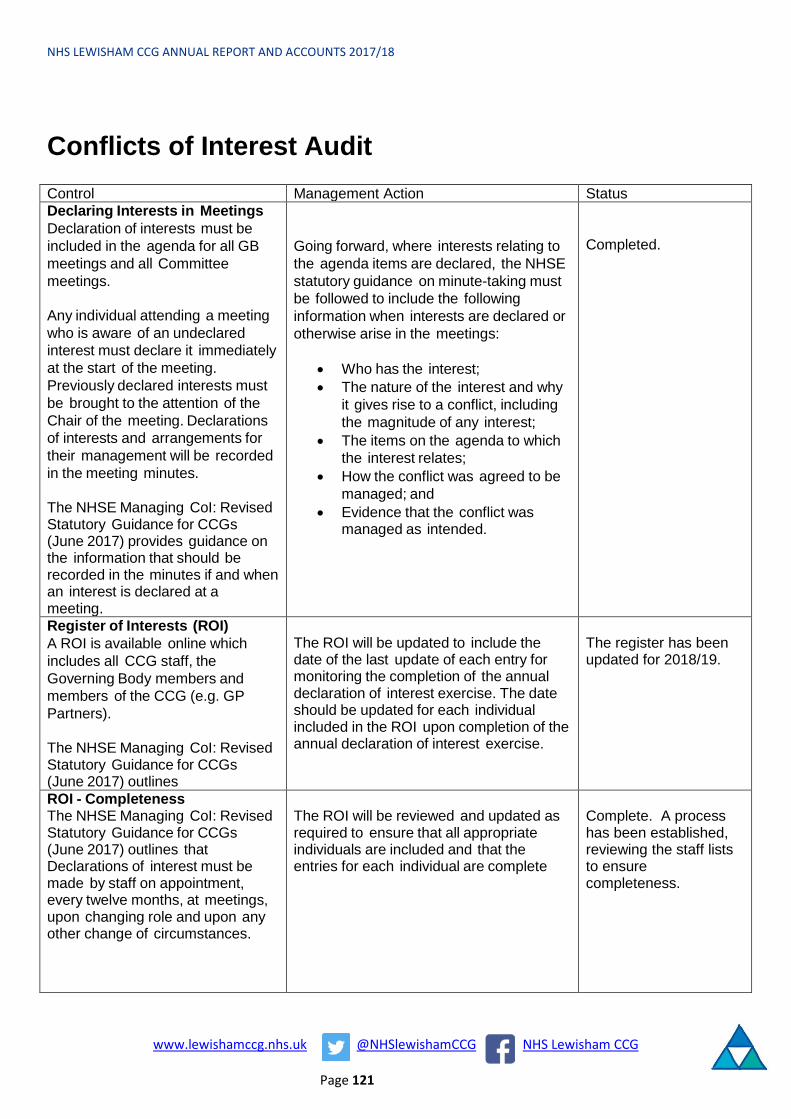
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 121
Conflicts of Interest Audit Control Management Action Status Declaring Interests in Meetings Declaration of interests must be included in the agenda for all GB meetings and all Committee meetings.
Any individual attending a meeting who is aware of an undeclared interest must declare it immediately at the start of the meeting. Previously declared interests must be brought to the attention of the Chair of the meeting. Declarations of interests and arrangements for their management will be recorded in the meeting minutes.
The NHSE Managing CoI: Revised Statutory Guidance for CCGs (June 2017) provides guidance on the information that should be recorded in the minutes if and when an interest is declared at a meeting.
Going forward, where interests relating to the agenda items are declared, the NHSE statutory guidance on minute-taking must be followed to include the following information when interests are declared or otherwise arise in the meetings:
• Who has the interest;• The nature of the interest and why
it gives rise to a conflict, includingthe magnitude of any interest;
• The items on the agenda to whichthe interest relates;
• How the conflict was agreed to bemanaged; and
• Evidence that the conflict wasmanaged as intended.
Completed.
Register of Interests (ROI) A ROI is available online which includes all CCG staff, the Governing Body members and members of the CCG (e.g. GP Partners).
The NHSE Managing CoI: Revised Statutory Guidance for CCGs (June 2017) outlines
The ROI will be updated to include the date of the last update of each entry for monitoring the completion of the annual declaration of interest exercise. The date should be updated for each individual included in the ROI upon completion of the annual declaration of interest exercise.
The register has been updated for 2018/19.
ROI - Completeness The NHSE Managing CoI: Revised Statutory Guidance for CCGs (June 2017) outlines that Declarations of interest must be made by staff on appointment, every twelve months, at meetings, upon changing role and upon any other change of circumstances.
The ROI will be reviewed and updated as required to ensure that all appropriate individuals are included and that the entries for each individual are complete
Complete. A process has been established, reviewing the staff lists to ensure completeness.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 122
Declaration of Interests (DOI) Forms The NHSE Managing CoI: Revised Statutory Guidance for CCGs (June 2017) outlines that Conflicts should be declared as soon as the individual becomes aware of the potential conflict and a declaration of interest form must be completed and sent to the Board Secretary
As part of the annual DOI refresh, the CCGs will ensure that the DoI forms are appropriately completed by all GB members, CCG staff and members of the CCG e.g. clinical leads in localities.
The RoIs will be subsequently reviewed to ensure that all declarations made via the DoI forms are appropriately and correctly captured.
Completed. For 17/18 all anomalies were addressed. For 18/19 any forms provided that are incomplete are not being accepted and returned to individuals.
Completeness and Accuracy of Interest Declared – RSM Tracker Searches were conducted on the RSM Tracker to identify any undeclared directorships from the sample at the CCG. Included in the sample were members of the Governing Body, clinical leads and members of staff. RSM Tracker is a tool that provides public information on live and resigned directorships for public and private companies (trading or otherwise). This information was compared to the register of interests maintained and where sufficient information is available on the tracker.
CCG will discuss the discrepancy with the relevant individual to determine if these could be considered conflicts of interest and if these should be declared going forward.
Complete. A revised form was completed.
Register of Procurement Decisions The NHSE Managing CoI: Revised Statutory Guidance for CCGs (June 2017) outlines that each CCG must maintain a Register of Procurement Decisions including details of decisions made, who was involved in the decision-making process, a summary of any conflicts of interests and how they were managed and the award decision taken.
The register will be updated whenever a procurement decision is made and the register will form part of the CCG's annual accounts.
The Register of Procurement Opportunities Awards will be reviewed and updated to ensure that this meets the minimum requirements of information inclusion as outlined in the NHSE statutory guidance on CoI and that this is complete. The Register should indicate: • The governance group where thedecision was made and the date of themeeting;• The individuals involved in thedecision-making process; and• Any conflicts of interest declaredand their management.
It is recommended that the guidance template provided by the NHSE is used.
To be completed in Q1 2018/19.
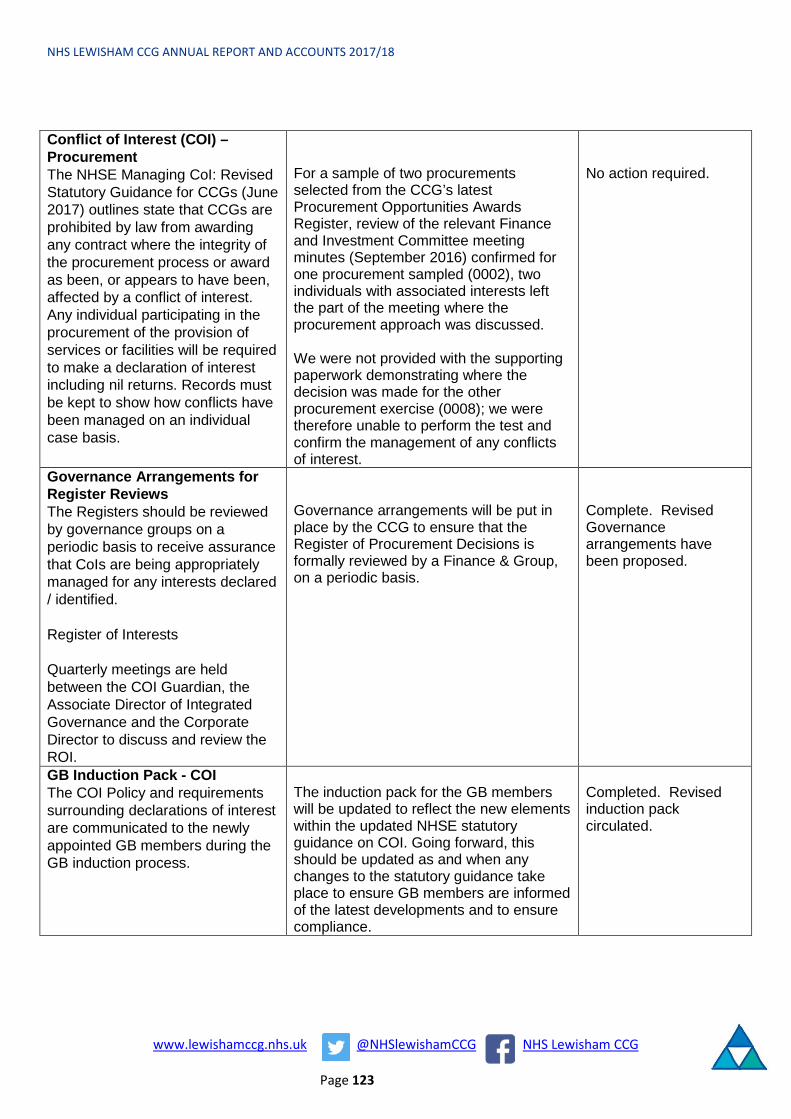
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 123
Conflict of Interest (COI) – Procurement The NHSE Managing CoI: Revised Statutory Guidance for CCGs (June 2017) outlines state that CCGs are prohibited by law from awarding any contract where the integrity of the procurement process or award as been, or appears to have been, affected by a conflict of interest. Any individual participating in the procurement of the provision of services or facilities will be required to make a declaration of interest including nil returns. Records must be kept to show how conflicts have been managed on an individual case basis.
For a sample of two procurements selected from the CCG’s latest Procurement Opportunities Awards Register, review of the relevant Finance and Investment Committee meeting minutes (September 2016) confirmed for one procurement sampled (0002), two individuals with associated interests left the part of the meeting where the procurement approach was discussed.
We were not provided with the supporting paperwork demonstrating where the decision was made for the other procurement exercise (0008); we were therefore unable to perform the test and confirm the management of any conflicts of interest.
No action required.
Governance Arrangements for Register Reviews The Registers should be reviewed by governance groups on a periodic basis to receive assurance that CoIs are being appropriately managed for any interests declared / identified.
Register of Interests
Quarterly meetings are held between the COI Guardian, the Associate Director of Integrated Governance and the Corporate Director to discuss and review the ROI.
Governance arrangements will be put in place by the CCG to ensure that the Register of Procurement Decisions is formally reviewed by a Finance & Group, on a periodic basis.
Complete. Revised Governance arrangements have been proposed.
GB Induction Pack - COI The COI Policy and requirements surrounding declarations of interest are communicated to the newly appointed GB members during the GB induction process.
The induction pack for the GB members will be updated to reflect the new elements within the updated NHSE statutory guidance on COI. Going forward, this should be updated as and when any changes to the statutory guidance take place to ensure GB members are informed of the latest developments and to ensure compliance.
Completed. Revised induction pack circulated.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 124
CHC Audit
Control Action for management Status Checklist: The checklist is used to assess the patient’s eligibility for continuing healthcare and to help practitioners identify people who need a full assessment for NHSE continuing healthcare; the checklist is based on the Decision Support Tool (DST).
All Funded Nursing Care (FNC) reviews, community reviews and hospital referrals are required to have a completed checklist for all new admissions, uploaded to LAS and submitted to the duty nurse and panel.
Some specialist hospitals do not provide a checklist when assessing users. All completed checklists are uploaded onto the LAS system. Prior to October 17, these were uploaded onto the CCG's shared drive to access as the team structure has recently undergone a change.
Management will remind the hospitals to submit a completed checklist when referring a CHC service user to ensure they have been appropriately assessed and to pass on the details to the next of kin, or it will be noted clearly why one has not been completed.
Checklists are now completed on the electronic patient record system LAS. Received checklists are uploaded onto LAS. The Enhanced Checklist were introduced 15/01/2018 as part of Discharge to assess process therefore all CHC referrals have an Enhanced Checklist.
Review of Continuing Healthcare Support: Care reviews are undertaken for individual service users initially within three months following the eligibility decision from the DST and again on an annual basis after the three-month review has occurred.
The CHC team will ensure all 3 month and annual reviews are clearly recorded on LAS going forward in order to ensure users are being reviewed at the correct time.
The patient record system (LAS) has a drop down menu called CHC/FNC 3 Month Review and CHC/FNC Annual Review
Continuing Care Contracts/ Service User Placement Agreements: Care plans are developed for each service user and care packages are commissioned from care homes, domiciliary care providers and from Nursing Agencies. There are four main providers for Dom-care where standard contracts are already in place.
IPAs should be included within the service user's online profile in order to confirm the agreement of the contract has been authorised; these should be signed by both the commissioner and the service provider.
IPAs are now sent for each Service User entering into a CHC Funded Nursing Bed.
LAS (Social Care Database) is used to note that the IPA has been issued, and also to note when it is returned.
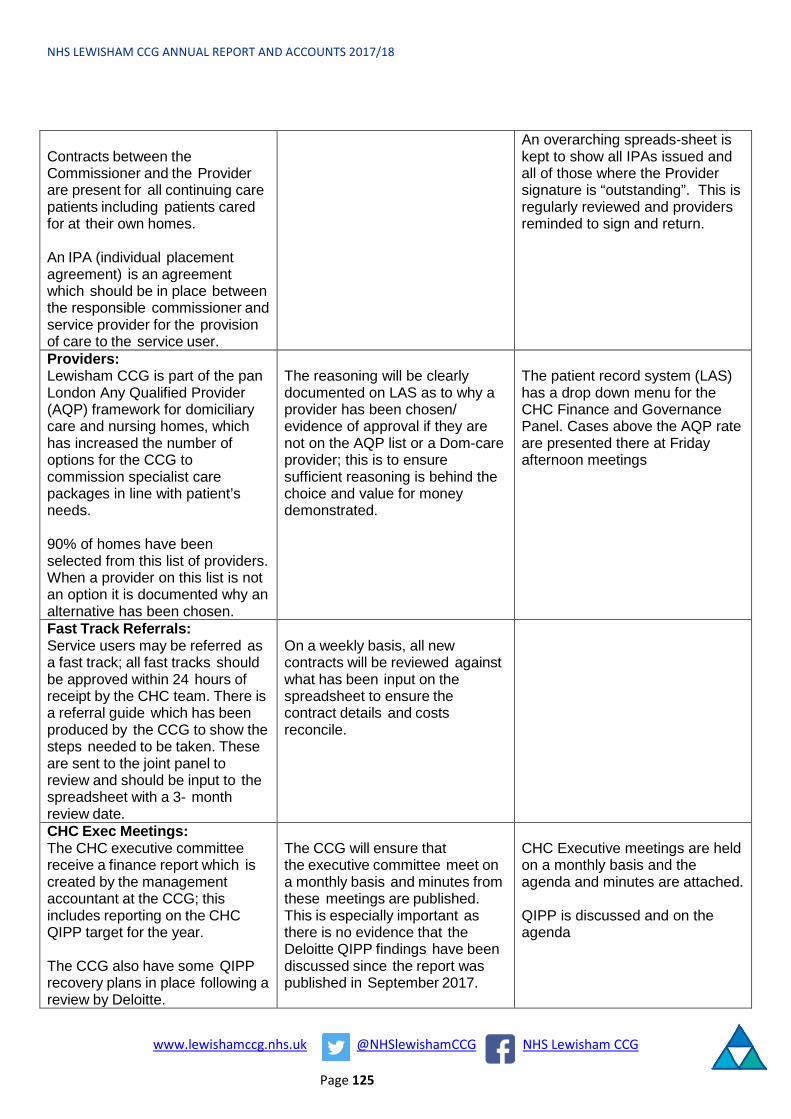
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 125
Contracts between the Commissioner and the Provider are present for all continuing care patients including patients cared for at their own homes.
An IPA (individual placement agreement) is an agreement which should be in place between the responsible commissioner and service provider for the provision of care to the service user.
An overarching spreads-sheet is kept to show all IPAs issued and all of those where the Provider signature is “outstanding”. This is regularly reviewed and providers reminded to sign and return.
Providers: Lewisham CCG is part of the pan London Any Qualified Provider (AQP) framework for domiciliary care and nursing homes, which has increased the number of options for the CCG to commission specialist care packages in line with patient’s needs.
90% of homes have been selected from this list of providers. When a provider on this list is not an option it is documented why an alternative has been chosen.
The reasoning will be clearly documented on LAS as to why a provider has been chosen/ evidence of approval if they are not on the AQP list or a Dom-care provider; this is to ensure sufficient reasoning is behind the choice and value for money demonstrated.
The patient record system (LAS) has a drop down menu for the CHC Finance and Governance Panel. Cases above the AQP rate are presented there at Friday afternoon meetings
Fast Track Referrals: Service users may be referred as a fast track; all fast tracks should be approved within 24 hours of receipt by the CHC team. There is a referral guide which has been produced by the CCG to show the steps needed to be taken. These are sent to the joint panel to review and should be input to the spreadsheet with a 3- month review date.
On a weekly basis, all new contracts will be reviewed against what has been input on the spreadsheet to ensure the contract details and costs reconcile.
CHC Exec Meetings: The CHC executive committee receive a finance report which is created by the management accountant at the CCG; this includes reporting on the CHC QIPP target for the year.
The CCG also have some QIPP recovery plans in place following a review by Deloitte.
The CCG will ensure that the executive committee meet on a monthly basis and minutes from these meetings are published. This is especially important as there is no evidence that the Deloitte QIPP findings have been discussed since the report was published in September 2017.
CHC Executive meetings are held on a monthly basis and the agenda and minutes are attached.
QIPP is discussed and on the agenda

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 126
Decision Support Tool (DST): The DST is used by health professionals to assess people for a full consideration for NHS continuing healthcare.
The DST should be used to establish patient eligibility, unless the Fast Track Pathway Tool is used. Within the DST the multi-disciplinary assessment is carried out to assess the severity of the patient's needs so that the most appropriate care package is compiled.
The assessments are carried out by qualified members of staff such as nurses or GPs and are signed and dated at the time of assessment.
Decisions will be made at panel for service users within 28 working days of the CCG receiving the completed DST. It will also be reminded that DSTs will be uploaded to LAS going forward.
28 day compliance is at 56% for February 2018
All DST’s are completed electronically on LAS and saved as an assessment completed on LAS.
CHC Policy: A CHC policy is in place for Lewisham CCG based on the National Services Framework for Continuing Health Care and is available for the public to view.
Management will review the CHC policy and ensure the updated version is available on the CCG website; this policy will reflect the new systems which are in place to monitor CHC and clearly state the roles and responsibilities.
Delayed pending SEL STP CHC review of choice policy

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 127
Review of the effectiveness of governance, risk management and internal control My review of the effectiveness of the system of internal control is informed by the work of the
internal auditors, executive managers and clinical leads within the clinical commissioning group
who have responsibility for the development and maintenance of the internal control framework. I
have drawn on performance information available to me. My review is also informed by comments
made by the external auditors in their annual audit letter and other reports.
Our assurance framework provides me with evidence that the effectiveness of controls that
manage risks to the clinical commissioning group achieving its principles objectives have been
reviewed.
I have been advised on the implications of the result of my review of the effectiveness of the
system of internal control by the Governing Body, the Audit Committee and Risk Management
Group and a plan to address weaknesses and ensure continuous improvement of the system is in
place.
The Governing Body and Audit Committee have provided regular feedback on the completeness
and effectiveness of our systems of internal control via their comments and feedback on the
completeness of the Board Assurance Framework. Control and assurance gaps were identified,
resulting in existing controls and assurances being further reviewed and strengthened. In order to
provide additional assurance, the Audit Committee also carried out detailed reviews into the risks
associated with the CCG priorities.
The report into the Board Assurance Framework (BAF) process from our internal auditors stated
that effective risk management provides a structure and process that will enable the CCG to focus
on those risks that might compromise achieving its objectives. The report concluded that the CCG
has established a risk management framework, a Board Assurance Framework (‘BAF’) and a
Corporate Risk Register (‘CRR’). There is a clear process via which risk management is escalated
through the organisation from departments to the Risk Management Group and through to the
Integrated Governance Committee and Governing Body. The Audit Committee maintains an
independent oversight of the risk management process and the associated BAF.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 128
The risk management arrangements at Lewisham Clinical Commissioning Group were reviewed
and an overall assessment of substantial assurance was provided.
The structure of the current risk register (BAF) and its completeness was assessed by Internal
Auditors and found that the CCG has a robust risk identification process in place where risks are
identified both top-down, driven by the strategic objectives and also bottom-up.
It was found that these risks have been clearly articulated in the BAF and are reviewed regularly at
the monthly review at the Risk Management Group and that the risks registers contain an
appropriate level of detail, with clear risk ratings. Risks with a residual risk rating of 12 or higher
are captured in the BAF for Governing Body scrutiny.
Conclusion In conclusion I confirm that no significant internal control issues have been identified.
Mr Andrew Bland
Accountable Officer
25th May 2018
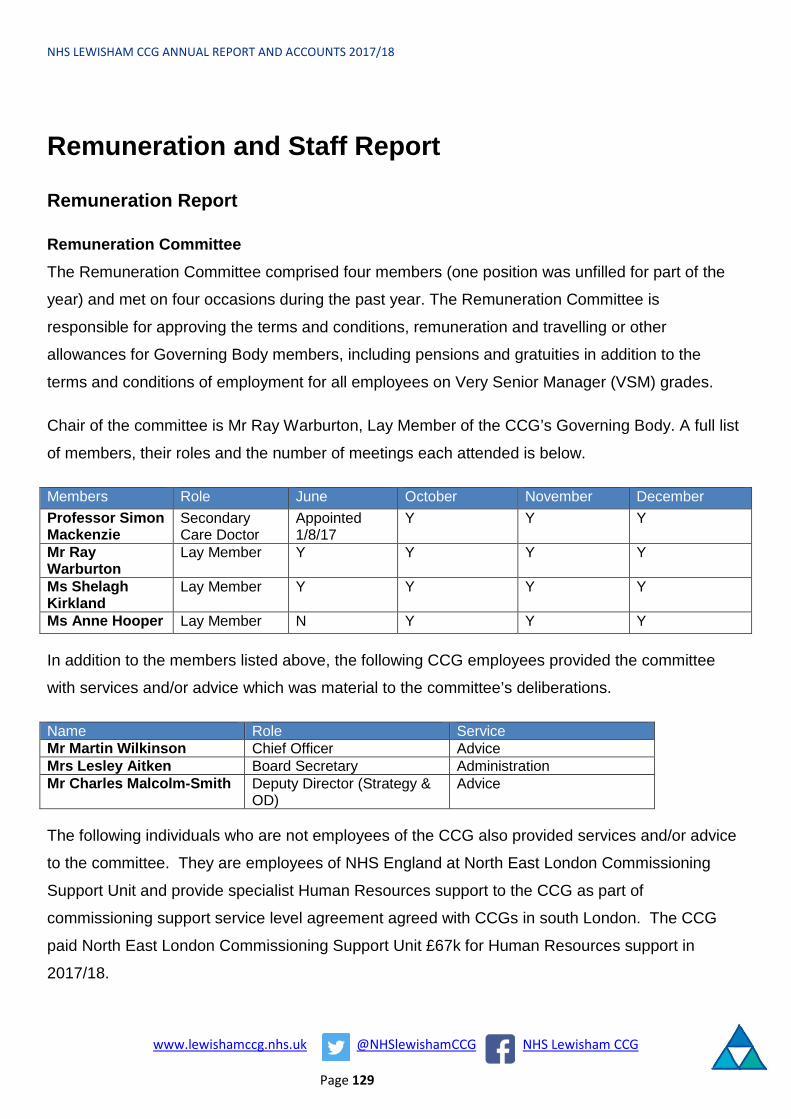
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 129
Remuneration and Staff Report
Remuneration Report
Remuneration Committee The Remuneration Committee comprised four members (one position was unfilled for part of the
year) and met on four occasions during the past year. The Remuneration Committee is
responsible for approving the terms and conditions, remuneration and travelling or other
allowances for Governing Body members, including pensions and gratuities in addition to the
terms and conditions of employment for all employees on Very Senior Manager (VSM) grades.
Chair of the committee is Mr Ray Warburton, Lay Member of the CCG’s Governing Body. A full list
of members, their roles and the number of meetings each attended is below.
Members Role June October November December Professor Simon Mackenzie
Secondary Care Doctor
Appointed 1/8/17
Y Y Y
Mr Ray Warburton
Lay Member Y Y Y Y
Ms Shelagh Kirkland
Lay Member Y Y Y Y
Ms Anne Hooper Lay Member N Y Y Y
In addition to the members listed above, the following CCG employees provided the committee
with services and/or advice which was material to the committee’s deliberations.
Name Role Service Mr Martin Wilkinson Chief Officer Advice Mrs Lesley Aitken Board Secretary Administration Mr Charles Malcolm-Smith Deputy Director (Strategy &
OD) Advice
The following individuals who are not employees of the CCG also provided services and/or advice
to the committee. They are employees of NHS England at North East London Commissioning
Support Unit and provide specialist Human Resources support to the CCG as part of
commissioning support service level agreement agreed with CCGs in south London. The CCG
paid North East London Commissioning Support Unit £67k for Human Resources support in
2017/18.
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 130
Name Role Service Ms Gail Tarburn Head of Human Resources Advice Mr Tim Widdowson Head of HR Business Partnering Advice
Policy on the remuneration of senior managers The Committee’s deliberations are carried out within the context of national pay and remuneration
guidelines, local comparability and taking account of independent advice regarding pay structures.
The CCG’s remuneration policy is consistent with nationally agreed pay awards for very senior
managers and Agenda for Change Terms and Conditions of Employment. The Remuneration
Committee assesses the performance of staff employed on Very Senior Manager (VSM) Pay in
line with the VSM Framework, comparable benchmarking and local pay arrangements and agrees
proposed performance assessment ratings. This policy is applicable for future years until any such
time as a new policy is agreed and implemented.
Senior managers’ performance related pay
The CCG does not have a policy of performance related pay for senior managers.
Senior managers’ service contracts
The CCG’s policy concerning senior managers’ contracts is that they are on-going (reviewed on an
annual basis), with a notice period of 6 months. Termination payments are calculated on the basis
of one month’s pay for every completed year of service.
The CCG may terminate the appointment at any time and with immediate effect by making a
payment in lieu of notice, in accordance with the contract of employment, as a lump sum payment
equal to that of the basic salary (as at the date of termination) which would have been payable
during the notice period, less income tax and national insurance contributions. Payments in lieu of
notice are at the sole and absolute discretion of the CCG and with the approval of the CCG’s
Remuneration Committee.
Payments in lieu of notice do not include: a) any additional payments that might otherwise have
been due during the period for which payment in lieu is made; b) any payment in respect of
benefits one would have been entitled to receive during the period; c) any payment in respect of

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 131
any holiday entitlement that would have accrued during the period for which the payment in lieu is
made.
Remuneration of Very Senior Managers
There are no senior managers of the CCG paid more than £150,000 per annum.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 132
Senior manager remuneration, including salary and pension entitlements (audited)
Note: *Taxable expenses and benefits in kind are expressed to the nearest £100. These include reimbursement of travel and course/training costs.
** Dr M Rowland held the position of Chair of the Governing Body for Lewisham CCG throughout the period. He also held the position of Chair of the London Clinical Commissioning Committtee. His
total salary for the 12 month period for these NHS roles was £95-100k.
Mr Andrew Bland became Accountable Officer for the CCG with effect from 1st April 2018. He did not receive any remuneration from Lewisham CCG for 2017/18.
(a)Salary & Fees
(bands of £5,000)
(b)Expense Payments
(taxable)to nearest £100*
(c)Performance pay and
bonuses (bands of £5,000)
(d)Long term
performance pay and bonuses (bands of
£5,000)
(e)All pension-related
benefits (bands of £2,500)
(f)TOTAL(a to e)
(bands of £5,000)
£000 £00 £000 £000 £000 £000
Mr Martin Wilkinson, Chief Officer 115 - 120 11 32.5 - 35 150 - 155
Mr Tony Read, Chief Financial Officer 105 - 110 0 25 - 27.5 135 - 140
Ms Diana Braithwaite, Commissioning Director 105 - 110 0 42.5 - 45 145 - 150
Ms Susanna Masters, Corporate Director 65 - 70 0 25 - 27.5 90 - 95
Ms Alison Browne, Director of Nursing and Quality / Registered Nurse Member
85 - 90 0 17.5 - 20 105 - 110
Dr Marc Rowland, Chair of the Governing Body** 60 - 65 0 60 - 65
Dr David Abraham, Senior Clinical Director 55 - 60 0 55 - 60
Dr Faruk Majid, Senior Clinical Director / Clinical Director 45 - 50 0 45 - 50
Dr Seb Kalwij, Clinical Director 40 - 45 0 40 - 45
Dr Charles Gostling, Clinical Director 40 - 45 0 40 - 45
Dr Angelika Razzaque, Clinical Director 40 - 45 0 40 - 45Dr Jacqueline McLeod, Clinical Director / Senior Clinical Director 50 - 55 0 50 - 55
Mr Ray Warburton, Lay Member 15 - 20 0 15 - 20
Dr Mark Hamilton, Secondary Care Doctor Member 0 - 5 0 0 - 5
Ms Anne Hooper, Lay Member 10 - 15 0 10 - 15
Dr Esther Appleby, Clinical Director 0 - 5 0 0 - 5
Ms Shelagh Kirkland, Lay Member 10 - 15 0 10 - 15
Prof Simon Mackenzie, Secondary Care Doctor Member 10 - 15 0 10 - 15
2017/18
Name and Title

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 133
*Note: Taxable expenses and benefits in kind are expressed to the nearest £100. These include reimbursement of travel and course/training costs.
(a)Salary & Fees
(bands of £5,000)
(b)Expense
Payments (taxable)
to nearest £100*
(c)Performance pay
and bonuses (bands of £5,000)
(d)Long term
performance pay and bonuses (bands of
£5,000)
(e)All pension-related
benefits (bands of £2,500)
(f)TOTAL(a to e)
(bands of £5,000)
£000 £00 £000 £000 £000 £000Mr Martin Wilkinson, Chief Officer 110 - 115 22 25 - 27.5 140 - 145Mr Tony Read, Chief Financial Officer 105 - 110 11 32.5 - 35 140 - 145Ms Diana Braithwaite, Commissioning Director 95 - 100 0 40 - 42.5 140 - 145Ms Susanna Masters, Corporate Director 65 - 70 1 17.5 - 20 80 - 85Ms Alison Browne, Director of Nursing and Quality 100 - 105 0 32.5 - 35 135 - 140Dr Marc Rowland, Chair od the Governing Body 60 - 65 0 60 - 65Dr David Abraham, Senior Clinical Director 55 - 60 0 55 - 60Dr Faruk Majid, Senior Clinical Director 55 - 60 0 55 - 60Dr Seb Kalwij, Clinical Director 40 - 45 0 40 - 45Dr Charles Gostling, Clinical Director 40 - 45 0 40 - 45Dr Angelika Razzaque, Clinical Director 40 - 45 0 40 - 45Dr Jacqueline McLeod, Clinical Director 40 - 45 0 40 - 45Mr Ray Warburton, Lay Member 15 - 20 0 15 - 20Dr Mark Hamilton, Secondary Care Doctor Member 20 - 25 0 20 - 25Ms Rosemarie Ramsay, Lay Member 5 - 10 0 5 - 10Ms Shelagh Kirkland, Audit Committee Member 0 - 5 0 0 - 5Professor Ami David, Registered Nurse Member 5 - 10 0 5 - 10
2016/17
Name and Title

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 134
Pension benefits as at 31 March 2018 (audited)
* The cash equivalent transfer value (CETV) at 31st March 2018 is not applicable to Alison Browne as she is over Normal Retirement Age in the existing scheme
(a)Real increase in
pension at pension age (bands of £2,500)
(b)Real increase in
pension lump sum at pension age
(bands of £2,500)
(c)Total accrued pension
at pension age at 31 March 2018 (bands of
£5,000)
(d)Lump sum at pension age related to accrued
pension at 31 March 2018
(bands of £5,000)
(e)Cash Equivalent Transfer Value at 1 April 2017
(f)Real increase in Cash Equivalent Transfer
Value
(g)Cash Equivalent
Transfer Value at 31 March 2018
(h)Employers
contribution to stakeholder pension
£000 £000 £000 £000 £000 £000 £000 £00Mr Martin Wilkinson, Chief Officer
0 - 2.5 0 - 2.5 35 - 40 90 - 95 573 507 61 0
Mr Tony Read, Chief Financial Officer
0 - 2.5 0 - 2.5 40 - 45 115 - 120 819 744 67 0
Ms Diana Braithwaite, Commissioning Director
2.5 - 5 0 - 2.5 20 - 25 45 - 50 331 276 52 0
Ms Susanna Masters, Corporate Director
0 - 2.5 0 - 2.5 35 - 40 115 - 120 903 836 58 0
Ms Alison Browne, Director of Nursing *and Quality
0 - 2.5 2.5 - 5 30 - 35 90 - 95 N/A N/A N/A 0
Name and title
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 135
Cash equivalent transfer values A cash equivalent transfer value (CETV) is the actuarially assessed capital value of the pension
scheme benefits accrued by a member at a particular point in time. The benefits valued are the
member’s accrued benefits and any contingent spouse’s (or other allowable beneficiary’s) pension
payable from the scheme.
A CETV is a payment made by a pension scheme or arrangement to secure pension benefits in
another pension scheme or arrangement when the member leaves a scheme and chooses to
transfer the benefits accrued in their former scheme. The pension figures shown relate to the
benefits that the individual has accrued as a consequence of their total membership of the pension
scheme, not just their service in a senior capacity to which disclosure applies.
The CETV figures and the other pension details include the value of any pension benefits in
another scheme or arrangement which the individual has transferred to the NHS pension scheme.
They also include any additional pension benefit accrued to the member as a result of their
purchasing additional years of pension service in the scheme at their own cost. CETVs are
calculated within the guidelines and framework prescribed by the Institute and Faculty of Actuaries.
Real increase in CETV This reflects the increase in CETV effectively funded by the employer. It takes account of the
increase in accrued pension due to inflation, contributions paid by the employee (including the
value of any benefits transferred from another scheme or arrangement) and uses common market
valuation factors for the start and end of the period.
Compensation on early retirement of for loss of office
No payment for compensation on early retirement or for loss of office were made during the
financial year 2017/18.
Payments to past members
No awards were made to past senior managers during the financial year 2017/18.
Pay multiples
Reporting bodies are required to disclose the relationship between the remuneration of the highest
paid member in their organisation and the median remuneration of the organisation’s workforce.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 136
The banded remuneration of the highest paid member in Lewisham CCG in the financial year
2017/18 was £114,300 (pro rata) (2016/17: £112,000). This was 2.69 times (2016/17: 2.33) the
median remuneration of the workforce, which was £42,535 (2016/17: £48,034).
In 2017/18, no employees received remuneration in excess of the highest-paid member.
Remuneration on a full time equivalent basis ranged from £17,000 to £200,100 (2016/2017:
£17,000 to £150,000)
Total remuneration includes salary, non-consolidated performance-related pay, benefits-in-kind,
but not severance payments. It does not include employer pension contributions and the cash
equivalent transfer value of pensions.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 137
Staff Report
Staff numbers, composition and costs (audited)
In 2017/18 NHS Lewisham CCG employed on average 81 staff; 52 female and 29 male.
The numbers of staff who were a VSM (Very Senior Manager) grade was 1 male.
The Governing Body was made up of 6 women and 9 men.
The Clinical Director’s Committee (Membership Body) was made up of 3 women and 5 men.
In relation to the 2016/17 Annual Report the number of other employees was not included in this
Table. This has been rectified for 2017/18 and the prior year numbers have now been stated.
Employee Benefits (audited)
The following tables show the values of employee benefits for 2017/18 and 2016/17.
Total Number
Permanently employed Number
Other Number
Total Number
Permanently employed Number
Other Number
Average number of CCG employed staff 81 64 17 79 54 25Female 52 42 10 50 35 15Male 29 22 7 29 19 10Of the above: Number of whole time equivalent people engaged on capital projects 0 0 0 0 0 0
2017-2018 2016-2017

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 138
2017/18
Total£000
Permanent Employees
£000Other£000
Total£000
Permanent Employees
£000Other£000
Total£000
Permanent Employees
£000Other£000
Salaries and Wages 5,038 3,628 1,411 3,056 2,559 497 1,983 1,069 914Social Security Costs 407 407 0 288 288 0 119 119 0Employer contributions to the NHS Pension Scheme
325 325 0 240 240 0 85 85 0
Other Pension Costs 0 0 0 0 0 0 0 0 0Apprenticeship Levy 5 5 0 5 5 0 0 0 0Other post-employment beneifts
0 0 0 0 0 0 0 0 0
Termination benefits 0 0 0 0 0 0 0 0 0Gross employee benefits expenditure
5,774 4,364 1,411 3,588 3,091 497 2,186 1,273 914
Less recoveries in respect of employee beneifts (note 4.1.2)
0 0 0 0 0 0 0 0 0
Total - Net admin employee benefits including capitalised costs
5,774 4,364 1,411 3,588 3,091 497 2,186 1,273 914
Less: Employee costs capitalised
0 0 0 0 0 0 0 0 0
Net employee benefits excluding capitalised costs
5,774 4,364 1,411 3,588 3,091 497 2,186 1,273 914
Total Admin Programme
2016/17
Total£000
Permanent Employees
£000Other£000
Total£000
Permanent Employees
£000Other£000
Total£000
Permanent Employees
£000Other£000
Salaries and Wages 5,420 2,956 2,464 3,363 2,328 1,035 2,056 628 1,428Social Security Costs 359 359 0 290 290 0 69 69 0Employer contributions to the NHS Pension Scheme
399 399 0 329 329 0 71 71 0
Other Pension Costs 0 0 0 0 0 0 0 0 0Other post-employment beneifts
0 0 0 0 0 0 0 0 0
Termination benefits 0 0 0 0 0 0 0 0 0Gross employee benefits expenditure
6,178 3,714 2,464 3,982 2,946 1,035 2,196 768 1,428
Less recoveries in respect of employee beneifts (note 4.1.2)
0 0 0 0 0 0 0 0 0
Total - Net admin employee benefits including capitalised costs
6,178 3,714 2,464 3,982 2,946 1,035 2,196 768 1,428
Less: Employee costs capitalised
0 0 0 0 0 0 0 0 0
Net employee benefits excluding capitalised costs
6,178 3,714 2,464 3,982 2,946 1,035 2,196 768 1,428
Total Admin Programme

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 139
Sickness absence data
Staff sickness absence and ill health retirements 2017-18 2016-17
Number Number
Total Days Lost 242 329
Total Staff Years 63 58
Average working Days Lost 3.8 5.7
The source of the table above is NHS Digital – Sickness Absence Publication.
Ill health retirement costs are met by the NHS Pension Scheme. The CCG did not have any ill
health retirements in 2017/18.
The CCG's Sickness Absence Policy confirms the importance of promoting and supporting the
health and welfare of its employees whilst at the same time being committed to achieving
excellence in terms of attendance at work. An employee assistance scheme is provided to support
staff. Our policies also confirm that the CCG will ensure that it abides by its duty of care to all staff,
and other such legislation in order to provide a supportive environment within which sickness
absence levels can be reduced. This can be achieved by the implementation of positive
procedures and guidelines. A consistent and pro-active approach to improving attendance is being
applied in the following areas:
• monitoring the attendance of staff on a regular basis
• positively reinforcing the good attendance of staff
• showing an understanding towards those who need to be absent from work on a long term
basis through sickness; and dealing fairly and consistently with staff whose attendance is of
concern
• ensuring that managers are supported, trained and encouraged to manage sickness
absence competently, fairly and consistently in line with good practice.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 140
Sickness absence rates are affected, among other things, by leadership and the working culture.
At the CCG, there is an inclusive and supportive leadership style and culture. Our average
monthly sickness absence rate was 1.53% (April 2017 – March 2018). The CCG national average
is 2.80%. Sickness absence is recorded, verified, monitored and reported as part of the monthly
HR Workforce Report to the CCG management team. Sickness absence data reported includes
sickness absence reason, days lost, full time equivalent days lost, and number of episodes. It also
categorises the absence by short and long term. The HR Business Partner works closely with
managers to ensure that sickness absence cases are managed in a timely way and in accordance
with the CCG's Sickness Absence Policy.
Staff policies Disabled Persons
Disabled employees are protected under the "protected characteristics" of the Equality Act 2010.
The CCG's Equality & Diversity Policy confirms that the CCG will make reasonable adjustments to
working conditions or to the physical working environment where that would help overcome the
practical effects of a disability. The policy also confirms that the CCG will provide support to enable
disabled members of staff to participate fully in meetings and training courses. Reasonable
adjustments will be taken into account and full use will be made of the advice and assistance
available via current government employment initiatives when consideration is being made of a
disabled applicant’s suitability for a vacant post. The CCG's Sickness Absence Policy confirms that
every effort will be made to facilitate an employee’s return to work including making reasonable
adjustments under the Disability Discrimination Act 1995 which may include applications for grants
where appropriate and taking advice from Disability Advisers in the Employment Service.
Expenditure on consultancy During 2017/18 the CCG expenditure on consultancy was £655k.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 141
Off-payroll engagements
Table 1: Off-payroll engagements longer than 6 months
For all off-payroll engagements as at 31 March 2018, for more than £245 per day and that last
longer than six months:
Table 2: New off-payroll engagements
For all new off-payroll engagements between 01 April 2017 and 31 March 2018, for more than
£245 per day and that last longer than six months:
Number
No. of existing engagements as of 31 March 2018 6
No. that have existed for less than one year at the time of reporting 0
No. that have existed for between one & two years at the time of reporting 6
No. that have existed for between two & three years at the time of reporting 0
No. that have existed for between three and four years at the time of reporting 0
No. that have existed for fout or more years at the time of reporting 0
Of which…
Number
Number of new engagements, or those that reached six months in duration, between 1 April 2017 and 31 March 2018
1
No. assessed as caught by IR35 0
No. assessed as not caught by IR35 1
No. engaged directly (via PSC contracted to department) and are on the departmental payroll
0
No. of engagements reassessed for consistency /assurance purposes during the year. 0
No. of engagements that saw a change to IR35 statusfollowing the consistency review 0
Of which:

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
www.lewishamccg.nhs.uk @NHSlewishamCCG NHS Lewisham CCG
Page 142
Table 3: Off-payroll engagements / senior official engagements
For any off-payroll engagements of Board members and / or senior officials with significant
financial responsibility, between 01 April 2017 and 31 March 2018.
Exit packages, including special (non-contractual) payments (audited) During 2017/18 NHS Lewisham CCG provided no exit packages or severance payments.
Mr Andrew Bland
Accountable Officer
25th May 2018
Number
Number of off-payroll engagements of board members, and/or senior officers with significant financial responsibility, during the financial year 0
Total no. of individuals on payroll and off-payroll that have been deemed “board members, and/or, senior officials with significant financial responsibility”, during the financial year. This figure should include both on payroll and off-payroll engagements.
17

Page 143
NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
Parliamentary Accountability and Audit Report
NHS Lewisham CCG is not required to produce a Parliamentary Accountability and Audit Report.
Disclosures on remote contingent liabilities, losses and special payments, gifts, and fees and
charges are included as notes in the following Financial Statements. An audit certificate and
report is also included at pages 147 to 149 of the Financial Statements.

NHS LEWISHAM CCG ANNUAL REPORT AND ACCOUNTS 2017/18
Page 144
ANNUAL ACCOUNTS
Andrew Bland
Accountable Officer
25th May 2018

Data entered below will be used throughout the workbook:
Entity name: NHS Lewisham CCGThis year 2017-18This year ended 31-March-2018This year commencing: 01-April-2017
145

NHS Lewisham CCG - Annual Accounts 2017-18
Page Number
The Primary Statements:
Statement of Comprehensive Net Expenditure for the year ended 31st March 2018 150Statement of Financial Position as at 31st March 2018 151Statement of Changes in Taxpayers' Equity for the year ended 31st March 2018 152Statement of Cash Flows for the year ended 31st March 2018 153
Notes to the AccountsAccounting policies 154Other operating revenue 159Revenue 159Employee benefits and staff numbers 160Operating expenses 163Better payment practice code 164Income generation activities 164Investment revenue 164Other gains and losses 164Finance costs 164Net gain/(loss) on transfer by absorption 165Operating leases 165Property, plant and equipment 166Intangible non-current assets 167Investment property 167Inventories 167Trade and other receivables 168Other financial assets 169Other current assets 169Cash and cash equivalents 169Non-current assets held for sale 169Analysis of impairments and reversals 169Trade and other payables 170Deferred revenue 170Other financial liabilities 170Borrowings 170Private finance initiative, LIFT and other service concession arrangements 170Finance lease obligations 170Finance lease receivables 170Provisions 171Contingencies 172Commitments 172Financial instruments 172Operating segments 174Pooled budgets 174NHS Lift investments 174Related party transactions 175Events after the end of the reporting period 176Third party assets 176Financial performance targets 176Impact of IFRS 176
CONTENTS
146

INDEPENDENT AUDITOR’S REPORT TO THE MEMBERS OF THE GOVERNING BODY OF NHS LEWISHAM CLINICAL COMMISSIONING GROUP REPORT ON THE AUDIT OF THE FINANCIAL STATEMENTS
opinion We have audited the financial statements of NHS Lewisham Clinical Commissioning Group (“the CCG”) for the year ended 31 March 2018 which comprise the Statement of Comprehensive Net Expenditure, Statement of Financial Position, Statement of Changes in Taxpayers Equity and Statement of Cash Flows, and the related notes, including the accounting policies in note one.
In our opinion the financial statements:
• give a true and fair view of the state of the CCG’s affairs as at 31 March 2018 and ofits income and expenditure for the year then ended; and
• have been properly prepared in accordance with the accounting policies directed bythe NHS Commissioning Board with the consent of the Secretary of State as beingrelevant to CCGs in England and included in the Department of Health GroupAccounting Manual 2017/18.
Basis for opinion
We conducted our audit in accordance with International Standards on Auditing (UK) (“ISAs (UK)”) and applicable law. Our responsibilities are described below. We have fulfilled our ethical responsibilities under, and are independent of the Trust in accordance with, UK ethical requirements including the FRC Ethical Standard. We believe that the audit evidence we have obtained is a sufficient and appropriate basis for our opinion.
Going concern
We are required to report to you if we have concluded that the use of the going concern basis of accounting is inappropriate or there is an undisclosed material uncertainty that may cast significant doubt over the use of that basis for a period of at least twelve months from the date of approval of the financial statements. We have nothing to report in these respects.
Other information in the Annual Report
The Accountable Officer is responsible for the other information presented in the Annual Report together with the financial statements. Our opinion on the financial statements does not cover the other information and, accordingly, we do not express an audit opinion or, except as explicitly stated below, any form of assurance conclusion thereon.
Our responsibility is to read the other information and, in doing so, consider whether, based on our financial statements audit work, the information therein is materially misstated or inconsistent with the financial statements or our audit knowledge. Based solely on that work we have not identified material misstatements in the other information. In our opinion the other information included in the Annual Report for the financial year is consistent with the financial statements.
Annual Governance Statement
We are required to report to you if the Annual Governance Statement does not comply with guidance issued by the NHS Commissioning Board. We have nothing to report in this respect.
Remuneration and Staff Report
In our opinion the parts of the Remuneration and Staff Report subject to audit have been properly prepared in accordance with the Department of Health Group Accounting Manual 2017/18.
Accountable Officer’s responsibilities
147

As explained more fully in the statement set out on page 82, the Accountable Officer is responsible for: the preparation of financial statements that give a true and fair view; such internal control as they determine is necessary to enable the preparation of financial statements that are free from material misstatement, whether due to fraud or error; assessing the CCGs ability to continue as a going concern, disclosing, as applicable, matters related to going concern; and using the going concern basis of accounting unless they have been informed by the relevant national body of the intention to dissolve the CCG without the transfer of its services to another public sector entity.
Auditor’s responsibilities
Our objectives are to obtain reasonable assurance about whether the financial statements as a whole are free from material misstatement, whether due to fraud or error, and to issue our opinion in an auditor’s report. Reasonable assurance is a high level of assurance, but does not guarantee that an audit conducted in accordance with ISAs (UK) will always detect a material misstatement when it exists. Misstatements can arise from fraud or error and are considered material if, individually or in aggregate, they could reasonably be expected to influence the economic decisions of users taken on the basis of the financial statements.
A fuller description of our responsibilities is provided on the FRC’s website at www.frc.org.uk/auditorsresponsibilities
REPORT ON OTHER LEGAL AND REGULATORY MATTERS
Opinion on regularity
We are required to report on the following matters under Section 25(1) of the Local Audit and Accountability Act 2014.
In our opinion, in all material respects, the expenditure and income recorded in the financial statements have been applied to the purposes intended by Parliament and the financial transactions conform to the authorities which govern them.
Report on the CCG’s arrangements for securing economy, efficiency and effectiveness in its use of resources
Under the Code of Audit Practice we are required to report to you if the CCG has not made proper arrangements for securing economy, efficiency and effectiveness in its use of resources.
Qualified conclusion
Except for the matters outlined in the basis for qualified conclusion paragraph below we are satisfied that in all significant respects NHS Lewisham CCG put in place proper arrangements for securing economy, efficiency and effectiveness in the use of resources for the year ended 31 March 2018.
Basis for qualified conclusion
The Clinical Commissioning Group was placed under legal directions from NHS England from 1 September 2017. The legal directions require the Clinical Commissioning Group to cease to exercise its acute commissioning functions including the contract with Lewisham and Greenwich NHS Trust. During the period of legal directions, acute commissioning functions are to be exercised by NHS Southwark Clinical Commissioning Group on behalf of NHS Lewisham Clinical Commissioning Group.
The legal directions also require the production and implementation of a Recovery Plan in respect of the contract between Lewisham and Greenwich NHS Trust and the Clinical Commissioning Group, specifically addressing urgent and emergency care services and ensuring that such services meet all applicable national standards.
Respective responsibilities in respect of our review of arrangements for securing economy, efficiency and effectiveness in the use of resources
148

As explained more fully in the statement set out on page 82, the Accountable Officer is responsible for ensuring that the CCG exercises its functions effectively, efficiently and economically. We are required under section 21(1)(c) of the Local Audit and Accountability Act 2014 to be satisfied that the CCG has made proper arrangements for securing economy, efficiency and effectiveness in its use of resources.
We are not required to consider, nor have we considered, whether all aspects of the CCGs arrangements for securing economy, efficiency and effectiveness in the use of resources are operating effectively.
We have undertaken our review in accordance with the Code of Audit Practice, having regard to the specified criterion issued by the Comptroller and Auditor General (C&AG) in November 2017, as to whether the CCG had proper arrangements to ensure it took properly informed decisions and deployed resources to achieve planned and sustainable outcomes for taxpayers and local people. We planned our work in accordance with the Code of Audit Practice and related guidance. Based on our risk assessment, we undertook such work as we considered necessary.
Statutory reporting matters
We are required by Schedule 2 to the Code of Audit Practice issued by the Comptroller and Auditor General (‘the Code of Audit Practice’) to report to you if:
• we refer a matter to the Secretary of State under section 30 of the Local Audit andAccountability Act 2014 because we have reason to believe that the CCG, or an officer ofthe CCG, is about to make, or has made, a decision which involves or would involve thebody incurring unlawful expenditure, or is about to take, or has begun to take a course ofaction which, if followed to its conclusion, would be unlawful and likely to cause a loss ordeficiency; or
• we issue a report in the public interest under section 24 of the Local Audit andAccountability Act 2014; or
• we make a written recommendation to the CCG under section 24 of the Local Audit andAccountability Act 2014.
We have nothing to report in these respects.
THE PURPOSE OF OUR AUDIT WORK AND TO WHOM WE OWE OUR RESPONSIBILITIES
This report is made solely to the Members of the Governing Body of NHS Lewisham CCG, as a body, in accordance with Part 5 of the Local Audit and Accountability Act 2014. Our audit work has been undertaken so that we might state to the Members of the Governing Body of the CCG, as a body, those matters we are required to state to them in an auditor’s report and for no other purpose. To the fullest extent permitted by law, we do not accept or assume responsibility to anyone other than the Members of the Governing Body, as a body, for our audit work, for this report or for the opinions we have formed.
CERTIFICATE OF COMPLETION OF THE AUDIT
We certify that we have completed the audit of the accounts of NHS Lewisham CCG in accordance with the requirements of the Local Audit and Accountability Act 2014 and the Code of Audit Practice.
Richard Hewes for and on behalf of KPMG LLP, Statutory Auditor Chartered Accountants 15 Canada Square London, E14 5GL
25 May 2017 149

NHS Lewisham CCG - Annual Accounts 2017-18
Statement of Comprehensive Net Expenditure for the year ended31 March 2018
2017-18 2016-17Note £'000 £'000
Income from sale of goods and services 2 (5,693) (3,247)Other operating income 2 (64) (872)Total operating income (5,757) (4,119)
Staff costs 4 5,774 6,178Purchase of goods and services 5 470,459 414,718Depreciation and impairment charges 5 0 0Provision expense 5 (250) 224Other Operating Expenditure 5 127 137Total operating expenditure 476,110 421,257
Net Operating Expenditure 470,353 417,138
Finance incomeFinance expense 10 0 0Net expenditure for the year 470,353 417,138Net Gain/(Loss) on Transfer by Absorption 0 0Total Net Expenditure for the year 470,353 417,138Other Comprehensive ExpenditureItems which will not be reclassified to net operating costsNet (gain)/loss on revaluation of PPE 0 0Net (gain)/loss on revaluation of Intangibles 0 0Net (gain)/loss on revaluation of Financial Assets 0 0Actuarial (gain)/loss in pension schemes 0 0Impairments and reversals taken to Revaluation Reserve 0 0Items that may be reclassified to Net Operating Costs 0 0Net gain/loss on revaluation of available for sale financial assets 0 0Reclassification adjustment on disposal of available for sale financial assets 0 0Sub total 0 0
Comprehensive Expenditure for the year ended 31 March 2018 470,353 417,138
150

2017-18 2016-17
Note £'000 £'000
13 50 014 0 015 0 017 0 018 0 0
50 0
16 0 017 5,678 4,45318 0 019 0 020 91 397
5,769 4,850
21 0 0
5,769 4,850
5,819 4,850
23 (31,997) (28,309)24 0 025 0 026 0 030 (46) (323)
(32,043) (28,632)
(26,224) (23,782)
23 0 024 0 025 0 026 0 030 0 0
0 0
(26,224) (23,782)
(26,224) (23,782)0 00 00 0
(26,224) (23,782)
NHS Lewisham CCG - Annual Accounts 2017-18
Statement of Financial Position as at31 March 2018
Non-current assets:Property, plant and equipmentIntangible assetsInvestment propertyTrade and other receivablesOther financial assetsTotal non-current assets
Current assets:InventoriesTrade and other receivablesOther financial assetsOther current assetsCash and cash equivalentsTotal current assets
Non-current assets held for sale
Total current assets
Total assets
Current liabilitiesTrade and other payablesOther financial liabilitiesOther liabilitiesBorrowingsProvisionsTotal current liabilities
Non-Current Assets plus/less Net Current Assets/Liabilities
Non-current liabilitiesTrade and other payablesOther financial liabilitiesOther liabilitiesBorrowingsProvisionsTotal non-current liabilities
Assets less Liabilities
Financed by Taxpayers’ EquityGeneral fundRevaluation reserveOther reservesCharitable ReservesTotal taxpayers' equity:
The notes on pages 154 to 176 form part of this statement
The financial statements on pages 150 to 176 were approved by the Audit Committee on 23 May 2018 under delegated authority from the Governing Body and signed on its behalf by:
151
Accountable OfficerAndrew Bland

General fundRevaluation
reserveOther
reservesTotal
reserves£'000 £'000 £'000 £'000
(23,782) 0 0 (23,782)
0 0 0 0(23,782) 0 0 (23,782)
(470,353) (470,353)
0 00 00 0
0 0 0 0
0 0 0 00 0 0 00 0 0 00 0 0 00 0 0 00 0 0 00 0 0 00 0 0 00 0 0 00 0 0 0
(470,353) 0 0 (470,353)
467,911 0 0 467,911
(26,224) 0 0 (26,224)
General fundRevaluation
reserveOther
reservesTotal
reserves£'000 £'000 £'000 £'000
(19,699) 0 0 (19,699)
0 0 0 0(19,699) 0 0 (19,699)
(417,138) (417,138)
0 00 00 0
0 0 0 0
0 0 0 00 0 0 00 0 0 00 0 0 00 0 0 00 0 0 00 0 0 00 0 0 00 0 0 00 0 0 0
(436,837) 0 0 (436,837)
413,055 0 0 413,055
(23,782) 0 0 (23,782)
NHS Lewisham CCG - Annual Accounts 2017-18
Statement of Changes In Taxpayers Equity for the year ended31 March 2018
Changes in taxpayers’ equity for 2017-18
Balance at 01 April 2017Transfer between reserves in respect of assets transferred from closed NHS bodiesAdjusted NHS Clinical Commissioning Group balance at 31 March 2018
Changes in NHS Clinical Commissioning Group taxpayers’ equity for 2017-18Net operating expenditure for the financial year
Net gain/(loss) on revaluation of property, plant and equipmentNet gain/(loss) on revaluation of intangible assetsNet gain/(loss) on revaluation of financial assetsTotal revaluations against revaluation reserve
Net gain (loss) on available for sale financial assetsNet gain (loss) on revaluation of assets held for saleImpairments and reversalsNet actuarial gain (loss) on pensionsMovements in other reservesTransfers between reservesRelease of reserves to the Statement of Comprehensive Net ExpenditureReclassification adjustment on disposal of available for sale financial assetsTransfers by absorption to (from) other bodiesReserves eliminated on dissolutionNet Recognised NHS Clinical Commissioning Group Expenditure for the Financial Yea
Net funding
Balance at 31 March 2018
Changes in taxpayers’ equity for 2016-17
Balance at 01 April 2016Transfer of assets and liabilities from closed NHS bodies as a result of the 1 April 2013 transitionAdjusted NHS Clinical Commissioning Group balance at 31 March 2017
Changes in NHS Clinical Commissioning Group taxpayers’ equity for 2016-17Net operating costs for the financial year
Net gain/(loss) on revaluation of property, plant and equipmentNet gain/(loss) on revaluation of intangible assetsNet gain/(loss) on revaluation of financial assetsTotal revaluations against revaluation reserve
Net gain (loss) on available for sale financial assetsNet gain (loss) on revaluation of assets held for saleImpairments and reversalsNet actuarial gain (loss) on pensionsMovements in other reservesTransfers between reservesRelease of reserves to the Statement of Comprehensive Net ExpenditureReclassification adjustment on disposal of available for sale financial assetsTransfers by absorption to (from) other bodiesReserves eliminated on dissolutionNet Recognised NHS Clinical Commissioning Group Expenditure for the Financial Yea
Net funding
Balance at 31 March 2017
The notes on pages 154 to 176 form part of this statement
152

2017-18 2016-17Note £'000 £'000
(470,353) (417,138)5 0 05 0 0
0 00 00 00 00 00 00 00 00 00 0
17 (1,225) (299)0 0
23 3,687 4,4500 0
30 (26) (11)30 (250) 224
(468,167) (412,774)
0 0(50) 0
0 00 00 00 00 00 00 00 00 00 00 00 0
(50) 0
(468,217) (412,774)
467,911 413,0550 00 00 00 00 0
467,911 413,055
20 (306) 281
397 116
0 0
91 397
NHS Lewisham CCG - Annual Accounts 2017-18
Statement of Cash Flows for the year ended31 March 2018
Cash Flows from Operating ActivitiesNet operating expenditure for the financial yearDepreciation and amortisationImpairments and reversalsMovement due to transfer by Modified AbsorptionOther gains (losses) on foreign exchangeDonated assets received credited to revenue but non-cashGovernment granted assets received credited to revenue but non-cashInterest paidRelease of PFI deferred creditOther Gains & LossesFinance CostsUnwinding of Discounts(Increase)/decrease in inventories(Increase)/decrease in trade & other receivables(Increase)/decrease in other current assetsIncrease/(decrease) in trade & other payablesIncrease/(decrease) in other current liabilitiesProvisions utilisedIncrease/(decrease) in provisionsNet Cash Inflow (Outflow) from Operating Activities
Cash Flows from Investing ActivitiesInterest received(Payments) for property, plant and equipment(Payments) for intangible assets(Payments) for investments with the Department of Health(Payments) for other financial assets(Payments) for financial assets (LIFT)Proceeds from disposal of assets held for sale: property, plant and equipmentProceeds from disposal of assets held for sale: intangible assetsProceeds from disposal of investments with the Department of HealthProceeds from disposal of other financial assetsProceeds from disposal of financial assets (LIFT)Loans made in respect of LIFTLoans repaid in respect of LIFTRental revenueNet Cash Inflow (Outflow) from Investing Activities
Net Cash Inflow (Outflow) before Financing
Cash Flows from Financing ActivitiesGrant in Aid Funding ReceivedOther loans receivedOther loans repaidCapital element of payments in respect of finance leases and on Statement of Financial Position PFI and LIFT Capital grants and other capital receiptsCapital receipts surrenderedNet Cash Inflow (Outflow) from Financing Activities
Net Increase (Decrease) in Cash & Cash Equivalents
Cash & Cash Equivalents at the Beginning of the Financial Year
Effect of exchange rate changes on the balance of cash and cash equivalents held in foreign currencies
Cash & Cash Equivalents (including bank overdrafts) at the End of the Financial Year
The notes on pages 154 to 176 form part of this statement
153

NHS Lewisham CCG - Annual Accounts 2017-18
Notes to the financial statements
1 Accounting PoliciesNHS England has directed that the financial statements of clinical commissioning groups shall meet the accounting requirements of the Group Accounting Manual issued by the Department of Health and Social Care. Consequently, the following financial statements have been prepared in accordance with the Group Accounting Manual 2017-18 issued by the Department of Health and Social Care. The accounting policies contained in the Group Accounting Manual follow International Financial Reporting Standards to the extent that they are meaningful and appropriate to clinical commissioning groups, as determined by HM Treasury, which is advised by the Financial Reporting Advisory Board. Where the Group Accounting Manual permits a choice of accounting policy, the accounting policy which is judged to be most appropriate to the particular circumstances of the clinical commissioning group for the purpose of giving a true and fair view has been selected. The particular policies adopted by the clinical commissioning group are described below. They have been applied consistently in dealing with items considered material in relation to the accounts.
1.1 Going ConcernThese accounts have been prepared on the going concern basis.Public sector bodies are assumed to be going concerns where the continuation of the provision of a service in the future is anticipated, as evidenced by inclusion of financial provision for that service in published documents.Where a clinical commissioning group ceases to exist, it considers whether or not its services will continue to be provided (using the same assets, by another public sector entity) in determining whether to use the concept of going concern for the final set of Financial Statements. If services will continue to be provided the financial statements are prepared on the going concern basis.During the year the Governing Body has considered and approved a number of documents that assume that services will be provided on an on-going basis:- South East London Sustainability and Transformation Plan (STP) updates- Population of the South East London Sustainability and Transformation Plan financial model- Long term CCG allocations and income plan- Operational plan with two year financial plan- Better Care Fund Plan approved by the Health and Well-Being Board- Acceptance of full delegation from NHS England for the co-commissioning of primary care services. NHS Lewisham CCG has assumed fullresponsibility for contractual GP performance management, budget management and the design and implementation of local incentive schemesfrom 1st April 2018- New governance arrangements for CCG and co-commissioning scrutiny and decision making- Changes to the CCG's Constitution- Approval of shared executive management and leadership arrangements across 5 CCGs and the SEL STP- The CCG has agreed main service contracts for 2018/19 and 2019/20 and has a cash plan for 2018/19 based on the CCG's notified MaximumCash Drawdown
1.2 Accounting ConventionThese accounts have been prepared under the historical cost convention modified to account for the revaluation of property, plant andequipment, intangible assets, inventories and certain financial assets and financial liabilities.
1.3 Acquisitions & Discontinued Operations
Activities are considered to be ‘acquired’ only if they are taken on from outside the public sector. Activities are considered to be ‘discontinued’ only if they cease entirely. They are not considered to be ‘discontinued’ if they transfer from one public sector body to another.
1.4 Pooled BudgetsWhere the clinical commissioning group has entered into a pooled budget arrangement under Section 75 of the National Health Service Act 2006 the clinical commissioning group accounts for its share of the assets, liabilities, income and expenditure arising from the activities of the pooled budget, identified in accordance with the pooled budget agreement.If the clinical commissioning group is in a “jointly controlled operation”, the clinical commissioning group recognises:· The assets the clinical commissioning group controls;· The liabilities the clinical commissioning group incurs;· The expenses the clinical commissioning group incurs; and,· The clinical commissioning group’s share of the income from the pooled budget activities.If the clinical commissioning group is involved in a “jointly controlled assets” arrangement, in addition to the above, the clinical commissioninggroup recognises:· The clinical commissioning group’s share of the jointly controlled assets (classified according to the nature of the assets);· The clinical commissioning group’s share of any liabilities incurred jointly; and,· The clinical commissioning group’s share of the expenses jointly incurred.
1.5 Critical Accounting Judgements & Key Sources of Estimation UncertaintyIn the application of the clinical commissioning group’s accounting policies, management is required to make judgements, estimates andassumptions about the carrying amounts of assets and liabilities that are not readily apparent from other sources. The estimates and associatedassumptions are based on historical experience and other factors that are considered to be relevant. Actual results may differ from thoseestimates and the estimates and underlying assumptions are continually reviewed. Revisions to accounting estimates are recognised in theperiod in which the estimate is revised if the revision affects only that period or in the period of the revision and future periods if the revisionaffects both current and future periods.
1.5.1 Critical Judgements in Applying Accounting PoliciesThe following are the critical judgements, apart from those involving estimations (see below) that management has made in the process ofapplying the clinical commissioning group’s accounting policies that have the most significant effect on the amounts recognised in the financialstatements:
- NHS Lewisham CCG exercised critical judgement in respect of prescribing accruals (see Note 23) and Continuing Healthcare provisions (seeNote 30).- Our judgement is that no provision is required in the accounts for any dilapidation costs that may potentially fall due on the CCG upondecanting Cantilever House
1.5.2 Key Sources of Estimation UncertaintyThe following are the key estimations that management has made in the process of applying the clinical commissioning group’s accountingpolicies that have the most significant effect on the amounts recognised in the financial statements:NHS Lewisham CCG had no materila key sources of estimation uncertainty
154

NHS Lewisham CCG - Annual Accounts 2017-18
Notes to the financial statements
1.6 RevenueRevenue in respect of services provided is recognised when, and to the extent that, performance occurs, and is measured at the fair value of the consideration receivable.Where income is received for a specific activity that is to be delivered in the following year, that income is deferred.The clinical commissioning group commissions services jointly with other CCGs and Trusts. Where the clinical commissioning group holds the contract and incurs expenditure on behalf of another party, a recharge is made to the joint commissioning partner and the expenditure is accounted for 'net' of revenue.
1.7 Employee Benefits1.7.1 Short-term Employee Benefits
Salaries, wages and employment-related payments are recognised in the period in which the service is received from employees, including bonuses earned but not yet taken.The cost of leave earned but not taken by employees at the end of the period is recognised in the financial statements to the extent that employees are permitted to carry forward leave into the following period.
1.7.2 Retirement Benefit Costs
Past and present employees are covered by the provisions of the NHS Pensions Scheme. The scheme is an unfunded, defined benefit scheme that covers NHS employers, General Practices and other bodies, allowed under the direction of the Secretary of State, in England and Wales. The scheme is not designed to be run in a way that would enable NHS bodies to identify their share of the underlying scheme assets and liabilities. Therefore, the scheme is accounted for as if it were a defined contribution scheme: the cost to the clinical commissioning group of participating in the scheme is taken as equal to the contributions payable to the scheme for the accounting period.For early retirements other than those due to ill health the additional pension liabilities are not funded by the scheme. The full amount of the liability for the additional costs is charged to expenditure at the time the clinical commissioning group commits itself to the retirement, regardless of the method of payment.Some employees are members of the Local Government Superannuation Scheme, which is a defined benefit pension scheme. The scheme assets and liabilities attributable to those employees can be identified and are recognised in the clinical commissioning group’s accounts. The assets are measured at fair value and the liabilities at the present value of the future obligations. The increase in the liability arising from pensionable service earned during the year is recognised within operating expenses. The expected gain during the year from scheme assets is recognised within finance income. The interest cost during the year arising from the unwinding of the discount on the scheme liabilities is recognised within finance costs. Actuarial gains and losses during the year are recognised in the General Reserve and reported as an item of other comprehensive net expenditure.
1.8 Other ExpensesOther operating expenses are recognised when, and to the extent that, the goods or services have been received. They are measured at the fair value of the consideration payable.Expenses and liabilities in respect of grants are recognised when the clinical commissioning group has a present legal or constructive obligation, which occurs when all of the conditions attached to the payment have been met.
1.9 Property, Plant & Equipment1.9.1 Recognition
Property, plant and equipment is capitalised if:· It is held for use in delivering services or for administrative purposes;· It is probable that future economic benefits will flow to, or service potential will be supplied to the clinical commissioning group;· It is expected to be used for more than one financial year;· The cost of the item can be measured reliably; and,· The item has a cost of at least £5,000; or,· Collectively, a number of items have a cost of at least £5,000 and individually have a cost of more than £250, where the assets arefunctionally interdependent, they had broadly simultaneous purchase dates, are anticipated to have simultaneous disposal dates and are undersingle managerial control; or,· Items form part of the initial equipping and setting-up cost of a new building, ward or unit, irrespective of their individual or collectivecost.Where a large asset, for example a building, includes a number of components with significantly different asset lives, the components are treatedas separate assets and depreciated over their own useful economic lives.
1.9.2 ValuationAll property, plant and equipment are measured initially at cost, representing the cost directly attributable to acquiring or constructing the assetand bringing it to the location and condition necessary for it to be capable of operating in the manner intended by management. All assets aremeasured subsequently at valuation.Land and buildings used for the clinical commissioning group’s services or for administrative purposes are stated in the statement of financialposition at their re-valued amounts, being the fair value at the date of revaluation less any impairment.Revaluations are performed with sufficient regularity to ensure that carrying amounts are not materially different from those that would bedetermined at the end of the reporting period. Fair values are determined as follows:· Land and non-specialised buildings – market value for existing use; and,· Specialised buildings – depreciated replacement cost.HM Treasury has adopted a standard approach to depreciated replacement cost valuations based on modern equivalent assets and, where itwould meet the location requirements of the service being provided, an alternative site can be valued.Properties in the course of construction for service or administration purposes are carried at cost, less any impairment loss. Cost includesprofessional fees but not borrowing costs, which are recognised as expenses immediately, as allowed by IAS 23 for assets held at fair value.Assets are re-valued and depreciation commences when they are brought into use.Fixtures and equipment are carried at depreciated historic cost as this is not considered to be materially different from current value in existinguse.An increase arising on revaluation is taken to the revaluation reserve except when it reverses an impairment for the same asset previouslyrecognised in expenditure, in which case it is credited to expenditure to the extent of the decrease previously charged there. A revaluationdecrease that does not result from a loss of economic value or service potential is recognised as an impairment charged to the revaluationreserve to the extent that there is a balance on the reserve for the asset and, thereafter, to expenditure. Impairment losses that arise from a clearconsumption of economic benefit are taken to expenditure. Gains and losses recognised in the revaluation reserve are reported as othercomprehensive income in the Statement of Comprehensive Net Expenditure.
155

NHS Lewisham CCG - Annual Accounts 2017-18
Notes to the financial statements
1.9.3 Subsequent ExpenditureWhere subsequent expenditure enhances an asset beyond its original specification, the directly attributable cost is capitalised. Where subsequent expenditure restores the asset to its original specification, the expenditure is capitalised and any existing carrying value of the item replaced is written-out and charged to operating expenses.
1.10 Intangible Assets1.10.1 Recognition
Intangible assets are non-monetary assets without physical substance, which are capable of sale separately from the rest of the clinical commissioning group’s business or which arise from contractual or other legal rights. They are recognised only:
· When it is probable that future economic benefits will flow to, or service potential be provided to, the clinical commissioning group;· Where the cost of the asset can be measured reliably; and,· Where the cost is at least £5,000.Intangible assets acquired separately are initially recognised at fair value. Software that is integral to the operating of hardware, for example anoperating system, is capitalised as part of the relevant item of property, plant and equipment. Software that is not integral to the operation ofhardware, for example application software, is capitalised as an intangible asset. Expenditure on research is not capitalised but is recognised asan operating expense in the period in which it is incurred. Internally-generated assets are recognised if, and only if, all of the following have beendemonstrated:· The technical feasibility of completing the intangible asset so that it will be available for use;· The intention to complete the intangible asset and use it;· The ability to sell or use the intangible asset;· How the intangible asset will generate probable future economic benefits or service potential;· The availability of adequate technical, financial and other resources to complete the intangible asset and sell or use it; and,· The ability to measure reliably the expenditure attributable to the intangible asset during its development.
1.10.2 MeasurementThe amount initially recognised for internally-generated intangible assets is the sum of the expenditure incurred from the date when the criteria above are initially met. Where no internally-generated intangible asset can be recognised, the expenditure is recognised in the period in which it is incurred.
Following initial recognition, intangible assets are carried at current value in existing use by reference to an active market, or, where no active market exists, at the lower of depreciated replacement cost or the value in use where the asset is income generating . Internally-developed software is held at historic cost to reflect the opposing effects of increases in development costs and technological advances.
1.11 Depreciation, Amortisation & ImpairmentsFreehold land, properties under construction, and assets held for sale are not depreciated.Otherwise, depreciation and amortisation are charged to write off the costs or valuation of property, plant and equipment and intangible non-current assets, less any residual value, over their estimated useful lives, in a manner that reflects the consumption of economic benefits or service potential of the assets. The estimated useful life of an asset is the period over which the clinical commissioning group expects to obtain economic benefits or service potential from the asset. This is specific to the clinical commissioning group and may be shorter than the physical life of the asset itself. Estimated useful lives and residual values are reviewed each year end, with the effect of any changes recognised on a prospective basis. Assets held under finance leases are depreciated over their estimated useful lives.
At each reporting period end, the clinical commissioning group checks whether there is any indication that any of its tangible or intangible non-current assets have suffered an impairment loss. If there is indication of an impairment loss, the recoverable amount of the asset is estimated to determine whether there has been a loss and, if so, its amount. Intangible assets not yet available for use are tested for impairment annually.A revaluation decrease that does not result from a loss of economic value or service potential is recognised as an impairment charged to the revaluation reserve to the extent that there is a balance on the reserve for the asset and, thereafter, to expenditure. Impairment losses that arise from a clear consumption of economic benefit are taken to expenditure. Where an impairment loss subsequently reverses, the carrying amount of the asset is increased to the revised estimate of the recoverable amount but capped at the amount that would have been determined had there been no initial impairment loss. The reversal of the impairment loss is credited to expenditure to the extent of the decrease previously charged there and thereafter to the revaluation reserve.
1.12 LeasesLeases are classified as finance leases when substantially all the risks and rewards of ownership are transferred to the lessee. All other leases are classified as operating leases.
1.12.1 The Clinical Commissioning Group as LesseeProperty, plant and equipment held under finance leases are initially recognised, at the inception of the lease, at fair value or, if lower, at the present value of the minimum lease payments, with a matching liability for the lease obligation to the lessor. Lease payments are apportioned between finance charges and reduction of the lease obligation so as to achieve a constant rate on interest on the remaining balance of the liability. Finance charges are recognised in calculating the clinical commissioning group’s surplus/deficit.Operating lease payments are recognised as an expense on a straight-line basis over the lease term. Lease incentives are recognised initially as a liability and subsequently as a reduction of rentals on a straight-line basis over the lease term.Contingent rentals are recognised as an expense in the period in which they are incurred.Where a lease is for land and buildings, the land and building components are separated and individually assessed as to whether they are operating or finance leases.
1.12.2 The Clinical Commissioning Group as LessorAmounts due from lessees under finance leases are recorded as receivables at the amount of the clinical commissioning group’s net investment in the leases. Finance lease income is allocated to accounting periods so as to reflect a constant periodic rate of return on the clinical commissioning group’s net investment outstanding in respect of the leases.Rental income from operating leases is recognised on a straight-line basis over the term of the lease. Initial direct costs incurred in negotiating and arranging an operating lease are added to the carrying amount of the leased asset and recognised on a straight-line basis over the lease term.
156
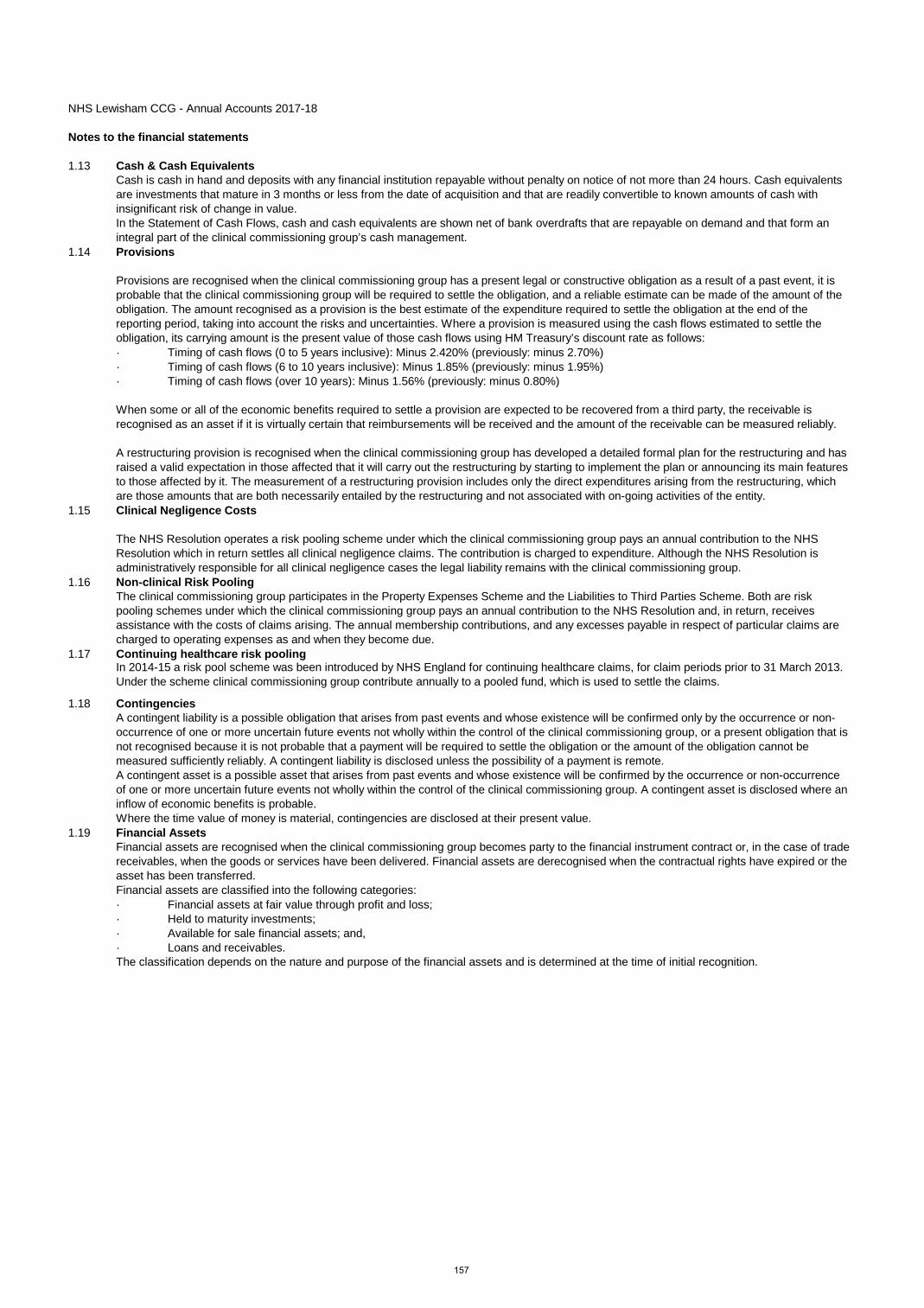
NHS Lewisham CCG - Annual Accounts 2017-18
Notes to the financial statements
1.13 Cash & Cash EquivalentsCash is cash in hand and deposits with any financial institution repayable without penalty on notice of not more than 24 hours. Cash equivalents are investments that mature in 3 months or less from the date of acquisition and that are readily convertible to known amounts of cash with insignificant risk of change in value.In the Statement of Cash Flows, cash and cash equivalents are shown net of bank overdrafts that are repayable on demand and that form an integral part of the clinical commissioning group’s cash management.
1.14 Provisions
Provisions are recognised when the clinical commissioning group has a present legal or constructive obligation as a result of a past event, it is probable that the clinical commissioning group will be required to settle the obligation, and a reliable estimate can be made of the amount of the obligation. The amount recognised as a provision is the best estimate of the expenditure required to settle the obligation at the end of the reporting period, taking into account the risks and uncertainties. Where a provision is measured using the cash flows estimated to settle the obligation, its carrying amount is the present value of those cash flows using HM Treasury’s discount rate as follows:· Timing of cash flows (0 to 5 years inclusive): Minus 2.420% (previously: minus 2.70%)· Timing of cash flows (6 to 10 years inclusive): Minus 1.85% (previously: minus 1.95%)· Timing of cash flows (over 10 years): Minus 1.56% (previously: minus 0.80%)
When some or all of the economic benefits required to settle a provision are expected to be recovered from a third party, the receivable is recognised as an asset if it is virtually certain that reimbursements will be received and the amount of the receivable can be measured reliably.
A restructuring provision is recognised when the clinical commissioning group has developed a detailed formal plan for the restructuring and has raised a valid expectation in those affected that it will carry out the restructuring by starting to implement the plan or announcing its main features to those affected by it. The measurement of a restructuring provision includes only the direct expenditures arising from the restructuring, which are those amounts that are both necessarily entailed by the restructuring and not associated with on-going activities of the entity.
1.15 Clinical Negligence Costs
The NHS Resolution operates a risk pooling scheme under which the clinical commissioning group pays an annual contribution to the NHS Resolution which in return settles all clinical negligence claims. The contribution is charged to expenditure. Although the NHS Resolution is administratively responsible for all clinical negligence cases the legal liability remains with the clinical commissioning group.
1.16 Non-clinical Risk PoolingThe clinical commissioning group participates in the Property Expenses Scheme and the Liabilities to Third Parties Scheme. Both are risk pooling schemes under which the clinical commissioning group pays an annual contribution to the NHS Resolution and, in return, receives assistance with the costs of claims arising. The annual membership contributions, and any excesses payable in respect of particular claims are charged to operating expenses as and when they become due.
1.17 Continuing healthcare risk poolingIn 2014-15 a risk pool scheme was been introduced by NHS England for continuing healthcare claims, for claim periods prior to 31 March 2013. Under the scheme clinical commissioning group contribute annually to a pooled fund, which is used to settle the claims.
1.18 ContingenciesA contingent liability is a possible obligation that arises from past events and whose existence will be confirmed only by the occurrence or non-occurrence of one or more uncertain future events not wholly within the control of the clinical commissioning group, or a present obligation that is not recognised because it is not probable that a payment will be required to settle the obligation or the amount of the obligation cannot be measured sufficiently reliably. A contingent liability is disclosed unless the possibility of a payment is remote.A contingent asset is a possible asset that arises from past events and whose existence will be confirmed by the occurrence or non-occurrence of one or more uncertain future events not wholly within the control of the clinical commissioning group. A contingent asset is disclosed where an inflow of economic benefits is probable.Where the time value of money is material, contingencies are disclosed at their present value.
1.19 Financial AssetsFinancial assets are recognised when the clinical commissioning group becomes party to the financial instrument contract or, in the case of trade receivables, when the goods or services have been delivered. Financial assets are derecognised when the contractual rights have expired or the asset has been transferred.Financial assets are classified into the following categories:· Financial assets at fair value through profit and loss;· Held to maturity investments;· Available for sale financial assets; and,· Loans and receivables.The classification depends on the nature and purpose of the financial assets and is determined at the time of initial recognition.
157
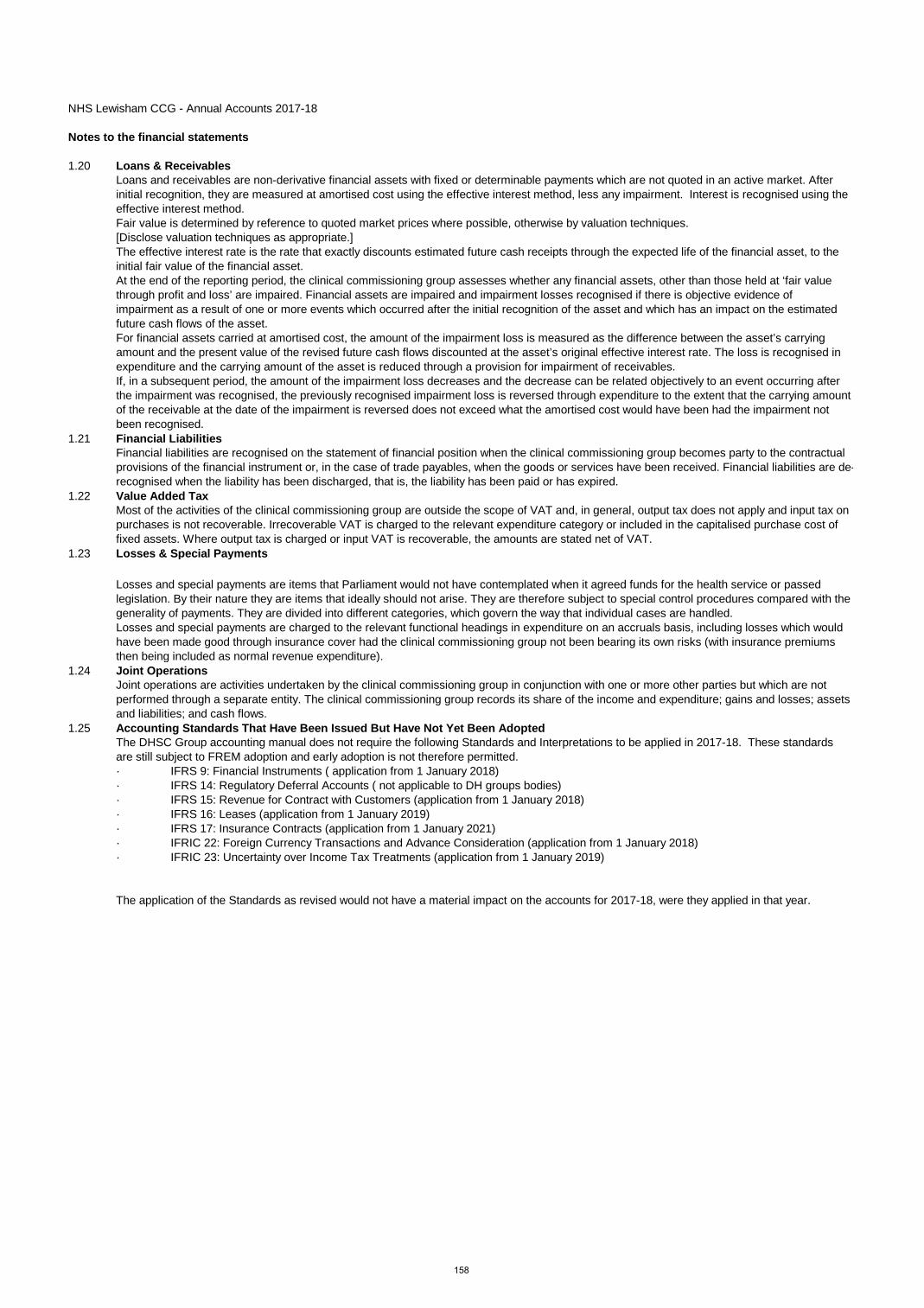
NHS Lewisham CCG - Annual Accounts 2017-18
Notes to the financial statements
1.20 Loans & ReceivablesLoans and receivables are non-derivative financial assets with fixed or determinable payments which are not quoted in an active market. After initial recognition, they are measured at amortised cost using the effective interest method, less any impairment. Interest is recognised using the effective interest method.Fair value is determined by reference to quoted market prices where possible, otherwise by valuation techniques.[Disclose valuation techniques as appropriate.]The effective interest rate is the rate that exactly discounts estimated future cash receipts through the expected life of the financial asset, to the initial fair value of the financial asset.At the end of the reporting period, the clinical commissioning group assesses whether any financial assets, other than those held at ‘fair value through profit and loss’ are impaired. Financial assets are impaired and impairment losses recognised if there is objective evidence of impairment as a result of one or more events which occurred after the initial recognition of the asset and which has an impact on the estimated future cash flows of the asset.For financial assets carried at amortised cost, the amount of the impairment loss is measured as the difference between the asset’s carrying amount and the present value of the revised future cash flows discounted at the asset’s original effective interest rate. The loss is recognised in expenditure and the carrying amount of the asset is reduced through a provision for impairment of receivables.If, in a subsequent period, the amount of the impairment loss decreases and the decrease can be related objectively to an event occurring after the impairment was recognised, the previously recognised impairment loss is reversed through expenditure to the extent that the carrying amount of the receivable at the date of the impairment is reversed does not exceed what the amortised cost would have been had the impairment not been recognised.
1.21 Financial LiabilitiesFinancial liabilities are recognised on the statement of financial position when the clinical commissioning group becomes party to the contractual provisions of the financial instrument or, in the case of trade payables, when the goods or services have been received. Financial liabilities are de-recognised when the liability has been discharged, that is, the liability has been paid or has expired.
1.22 Value Added TaxMost of the activities of the clinical commissioning group are outside the scope of VAT and, in general, output tax does not apply and input tax on purchases is not recoverable. Irrecoverable VAT is charged to the relevant expenditure category or included in the capitalised purchase cost of fixed assets. Where output tax is charged or input VAT is recoverable, the amounts are stated net of VAT.
1.23 Losses & Special Payments
Losses and special payments are items that Parliament would not have contemplated when it agreed funds for the health service or passed legislation. By their nature they are items that ideally should not arise. They are therefore subject to special control procedures compared with the generality of payments. They are divided into different categories, which govern the way that individual cases are handled.Losses and special payments are charged to the relevant functional headings in expenditure on an accruals basis, including losses which would have been made good through insurance cover had the clinical commissioning group not been bearing its own risks (with insurance premiums then being included as normal revenue expenditure).
1.24 Joint OperationsJoint operations are activities undertaken by the clinical commissioning group in conjunction with one or more other parties but which are not performed through a separate entity. The clinical commissioning group records its share of the income and expenditure; gains and losses; assets and liabilities; and cash flows.
1.25 Accounting Standards That Have Been Issued But Have Not Yet Been AdoptedThe DHSC Group accounting manual does not require the following Standards and Interpretations to be applied in 2017-18. These standards are still subject to FREM adoption and early adoption is not therefore permitted.· IFRS 9: Financial Instruments ( application from 1 January 2018)· IFRS 14: Regulatory Deferral Accounts ( not applicable to DH groups bodies)· IFRS 15: Revenue for Contract with Customers (application from 1 January 2018)· IFRS 16: Leases (application from 1 January 2019)· IFRS 17: Insurance Contracts (application from 1 January 2021)· IFRIC 22: Foreign Currency Transactions and Advance Consideration (application from 1 January 2018)· IFRIC 23: Uncertainty over Income Tax Treatments (application from 1 January 2019)
The application of the Standards as revised would not have a material impact on the accounts for 2017-18, were they applied in that year.
158

NHS Lewisham CCG - Annual Accounts 2017-18
2 Other Operating Revenue2017-18 2017-18 2017-18 2016-17
Total Admin Programme Total
£'000 £'000 £'000 £'000
Recoveries in respect of employee benefits 0 0 0 0Patient transport services 0 0 0 0Prescription fees and charges 0 0 0 0Dental fees and charges 0 0 0 0Education, training and research 41 21 20 68Charitable and other contributions to revenue expenditure: NHS 0 0 0 0Charitable and other contributions to revenue expenditure: non-NHS 64 1 63 119Receipt of donations for capital acquisitions: NHS Charity 0 0 0 0Receipt of Government grants for capital acquisitions 0 0 0 0Non-patient care services to other bodies 5,652 102 5,550 3,179Continuing Health Care risk pool contributions 0 0 0 0Income generation 0 0 0 0Rental revenue from finance leases 0 0 0 0Rental revenue from operating leases 0 0 0 0Non cash apprenticeship training grants revenue 0 0 0 0Other revenue 0 0 0 753Total other operating revenue 5,757 124 5,633 4,119
3 Revenue2017-18 2017-18 2017-18 2016-17
Total Admin Programme Total£'000 £'000 £'000 £'000
From rendering of services 5,757 124 5,633 4,119From sale of goods 0 0 0 0Total 5,757 124 5,633 4,119
159

NHS Lewisham CCG - Annual Accounts 2017-18
4. Employee benefits and staff numbers
4.1.1 Employee benefits 2017-18
TotalPermanent Employees Other
£'000 £'000 £'000Employee BenefitsSalaries and wages 5,039 3,628 1,411Social security costs 407 407 0Employer Contributions to NHS Pension scheme 325 325 0Other pension costs 0 0 0Apprenticeship Levy 5 5 0Other post-employment benefits 0 0 0Other employment benefits 0 0 0Termination benefits 0 0 0Gross employee benefits expenditure 5,775 4,364 1,411
Less recoveries in respect of employee benefits (note 4.1.2) 0 0 0Total - Net admin employee benefits including capitalised costs 5,775 4,364 1,411
Less: Employee costs capitalised 0 0 0Net employee benefits excluding capitalised costs 5,775 4,364 1,411
4.1.1 Employee benefits 2016-17
TotalPermanent Employees Other
£'000 £'000 £'000Employee BenefitsSalaries and wages 5,420 2,956 2,464Social security costs 359 359 0Employer Contributions to NHS Pension scheme 399 399 0Other pension costs 0 0 0Apprenticeship Levy 0 0 0Other post-employment benefits 0 0 0Other employment benefits 0 0 0Termination benefits 0 0 0Gross employee benefits expenditure 6,178 3,714 2,464
Less recoveries in respect of employee benefits (note 4.1.2) 0 0 0Total - Net admin employee benefits including capitalised costs 6,178 3,714 2,464
Less: Employee costs capitalised 0 0 0Net employee benefits excluding capitalised costs 6,178 3,714 2,464
4.1.2 Recoveries in respect of employee benefits
There were no recoveries in respect of employee benefits in 2017/18
Total
Total
160

NHS Lewisham CCG - Annual Accounts 2017-18
4.2 Average number of people employed2016-17
TotalPermanently
employed Other TotalNumber Number Number Number
Total 81 64 17 79
Of the above:Number of whole time equivalent people engaged on capital projects 0 0 0 0
4.3 Staff sickness absence and ill health retirements2017-18 2016-17Number Number
Total Days Lost 242 329Total Staff Years 63 58Average working Days Lost 4 6
2017-18 2016-17Number Number
Number of persons retired early on ill health grounds 0 1
£'000 £'000Total additional Pensions liabilities accrued in the year 0 0
Ill health retirement costs are met by the NHS Pension Scheme
4.4 Exit packages agreed in the financial year
2017-18 2017-18 2017-18
Number £ Number £ Number £Less than £10,000 0 0 0 0 0 0£10,001 to £25,000 0 0 0 0 0 0£25,001 to £50,000 0 0 0 0 0 0£50,001 to £100,000 0 0 0 0 0 0£100,001 to £150,000 0 0 0 0 0 0£150,001 to £200,000 0 0 0 0 0 0Over £200,001 0 0 0 0 0 0Total 0 0 0 0 0 0
Number £ Number £ Number £Less than £10,000 0 0 1 2,296 1 2,296£10,001 to £25,000 0 0 1 13,910 1 13,910£25,001 to £50,000 0 0 0 0 0 0£50,001 to £100,000 0 0 0 0 0 0£100,001 to £150,000 0 0 0 0 0 0£150,001 to £200,000 0 0 0 0 0 0Over £200,001 0 0 0 0 0 0Total 0 0 2 16,206 2 16,206
Number £ Number £Less than £10,000 0 0 0 0£10,001 to £25,000 0 0 0 0£25,001 to £50,000 0 0 0 0£50,001 to £100,000 0 0 0 0£100,001 to £150,000 0 0 0 0£150,001 to £200,000 0 0 0 0Over £200,001 0 0 0 0Total 0 0 0 0
Analysis of Other Agreed Departures
Number £ Number £Voluntary redundancies including early retirement contractual costs 0 0 0 0Mutually agreed resignations (MARS) contractual costs 0 0 0 0Early retirements in the efficiency of the service contractual costs 0 0 0 0Contractual payments in lieu of notice 0 0 2 16206Exit payments following Employment Tribunals or court orders 0 0 0 0Non-contractual payments requiring HMT approval* 0 0 0 0Total 0 0 2 16206
2016-17Compulsory redundancies
Nil non-contractual payments (£NIL) were made to individuals where the payment value was more than 12 months’ of their annual salary.
The Remuneration Report includes the disclosure of exit payments payable to individuals named in that Report.
2016-17
Where the clinical commissioning group has agreed early retirements, the additional costs are met by NHS Lewisham CCG and not by the NHS Pension Scheme, and are included in the tables. Ill-health retirement costs are met by the NHS Pension Scheme and are not included in the tables.
Exit costs are accounted for in accordance with relevant accounting standards and at the latest in full in the year of departure.
Other agreed departures
2017-18
Other agreed departures
There were no non-contractual severance payments made following judicial mediation and none relating to non-contractual payments in lieu of notice.
These tables report the number and value of exit packages agreed in the financial year. The expense associated with these departures may have been recognised in part or in full in a previous period.
Compulsory redundancies Other agreed departures Total
Departures where special payments have been made
2016-17 2016-17
Departures where special payments have been made
2017-18 2016-17
Other agreed departures Total
2017-18
161

NHS Lewisham CCG - Annual Accounts 2017-18
4.5 Pension costs
Past and present employees are covered by the provisions of the NHS Pension Scheme. Details of the benefits payable under these provisions can be found on the NHS Pensions website at www.nhsbsa.nhs.uk/.
The Scheme is an unfunded, defined benefit scheme that covers NHS employers, GP practices and other bodies, allowed under the direction of the Secretary of State, in England and Wales. The Scheme is not designed to be run in a way that would enable NHS bodies to identify their share of the underlying scheme assets and liabilities.
Therefore, the Scheme is accounted for as if it were a defined contribution scheme: the cost to the clinical commissioning group of participating in the Scheme is taken as equal to the contributions payable to the Scheme for
The Scheme is subject to a full actuarial valuation every four years (until 2004, every five years) and an accounting valuation every year. An outline of these follows:
4.5.1 Full actuarial (funding) valuation
The purpose of this valuation is to assess the level of liability in respect of the benefits due under the schemes (taking into account recent demographic experience), and to recommend contribution rates payable by employees and employers.
The last published actuarial valuation undertaken for the NHS Pension Scheme was completed for the year ending 31 March 2012. The Scheme Regulations allow for the level of contribution rates to be changed by the Secretary of State for Health, with the consent of HM Treasury, and consideration of the advice of the Scheme Actuary and employee and employer representatives as deemed appropriate.
The next actuarial valuation is to be carried out as at 31 March 2016 and is currently being prepared. The direction assumptions are published by HM Treasury which are used to complete the valuation calculations, from which the final valuation report can be signed off by the scheme actuary. This will set the employer contribution rate payable from April 2019 and will consider the cost of the Scheme relative to the employer cost cap. There are provisions in the Public Service Pension Act 2013 to adjust member benefits or contribution rates if the cost of the Scheme changes by more than 2% of pay. Subject to this ‘employer cost cap’ assessment, any required revisions to member benefits or contribution rates will be determined by the Secretary of State for Health after consultation with the
For 2017-18, employers’ contributions of £324,551 were payable to the NHS Pensions Scheme (2016-17: £399,443 ) were payable to the NHS Pension Scheme at the rate of 14.3% of pensionable pay. The scheme’s actuary reviewsemployer contributions, usually every four years and now based on HMT Valuation Directions, following a full schemevaluation. The latest review used data from 31 March 2012 and was published on the Government website on 9June 2012. These costs are included in the NHS pension line of note 4.1.
162

NHS Lewisham CCG - Annual Accounts 2017-18
5. Operating expenses5235.08561 2017-18 2017-18 2017-18 2016-17539.33181 Total Admin Programme Total
£'000 £'000 £'000 £'000Gross employee benefitsEmployee benefits excluding governing body members 5,235 3,049 2,186 5,554Executive governing body members 540 540 0 624Total gross employee benefits 5,775 3,588 2,186 6,178
Other costsServices from other CCGs and NHS England 3,310 1,574 1,735 3,503Services from foundation trusts 154,142 0 154,142 148,507Services from other NHS trusts 185,503 16 185,488 174,992Sustainability Transformation Fund 0 0 0 0Services from other WGA bodies 1 0 1 0Purchase of healthcare from non-NHS bodies 40,693 0 40,693 45,241Purchase of social care 1,210 0 1,210 0Chair and Non Executive Members 127 127 0 137Supplies and services – clinical 0 0 0 0Supplies and services – general 3,394 499 2,895 978Consultancy services 655 105 551 1,201Establishment 1,157 130 1,027 1,093Transport 3 3 0 1Premises 400 190 209 336Impairments and reversals of receivables 0 0 0 0Inventories written down and consumed 0 0 0 0Depreciation 0 0 0 0Amortisation 0 0 0 0Impairments and reversals of property, plant and equipment 0 0 0 0Impairments and reversals of intangible assets 0 0 0 0Impairments and reversals of financial assets· Assets carried at amortised cost 0 0 0 0· Assets carried at cost 0 0 0 0· Available for sale financial assets 0 0 0 0Impairments and reversals of non-current assets held for sale 0 0 0 0Impairments and reversals of investment properties 0 0 0 0Audit fees 52 52 0 76Other non statutory audit expenditure· Internal audit services 0 0 0 0· Other services 0 0 0 0General dental services and personal dental services 0 0 0 0Prescribing costs 36,968 0 36,968 37,976Pharmaceutical services 0 0 0 0General ophthalmic services 0 0 0 0GPMS/APMS and PCTMS * 42,489 0 42,489 118Other professional fees excl. audit 340 27 313 371Legal fees 32 31 1 0Grants to Other bodies 0 0 0 0Clinical negligence 0 0 0 0Research and development (excluding staff costs) 0 0 0 0Education and training 109 43 66 60Change in discount rate 0 0 0 0Provisions (250) 0 (250) 225Funding to group bodies 0 0 0 0CHC Risk Pool contributions 0 0 0 264Non cash apprenticeship training grants 0 0 0 0Other expenditure 0 0 0 0Total other costs 470,335 2,797 467,538 415,079
Total operating expenses 476,110 6,385 469,725 421,257
In accordance with SI 2008 no.489, The Companies (Disclosure of Auditor Remuneration and Liability Limitation Agreements) Regulations 2008 , the CCG is required to disclose the limit of its auditor's liability. The contract signed on 29 March 2017, states that the liability of KPMG, its members, partners and staff (whether in contract, negligence, or otherwise) shall in no circumstances exceed £2,000k, aside from where the liability cannot be limited by law. This is in aggregate in respect of all services. The audit fee disclosed above excluding irrecoverable VAT is £43,100.
163

NHS Lewisham CCG - Annual Accounts 2017-18
6.1 Better Payment Practice Code
Measure of compliance 2017-18 2017-18 2016-17 2016-17Number £'000 Number £'000
Non-NHS PayablesTotal Non-NHS Trade invoices paid in the Year 8,588 88,266 7,582 52,738Total Non-NHS Trade Invoices paid within target 8,380 85,596 7,303 51,244Percentage of Non-NHS Trade invoices paid within target 97.58% 96.98% 96.32% 97.17%
NHS PayablesTotal NHS Trade Invoices Paid in the Year 3,375 347,185 3,335 324,489Total NHS Trade Invoices Paid within target 3,276 345,661 3,283 324,249Percentage of NHS Trade Invoices paid within target 97.07% 99.56% 98.44% 99.93%
6.2 The Late Payment of Commercial Debts (Interest) Act 1998 2017-18 2016-17£'000 £'000
Amounts included in finance costs from claims made under this legislation 0 0Compensation paid to cover debt recovery costs under this legislation 0 0Total 0 0
7 Income Generation Activities
The clinical commissioning group did not undertake any income generation activities during 2017-18.
8. Investment revenue
The clinical commissioning group had no investment revenue as at 31 March 2018.
9. Other gains and losses
The clinical commissioning group had no other gains or losses as at 31 March 2018.
10. Finance costs
The clinical commissioning group had no finance costs as at 31 March 2018.
164

NHS Lewisham CCG - Annual Accounts 2017-18
11. Net gain/(loss) on transfer by absorption
2017-18 2016-17£'000 £'000
Transfer of property plant and equipment 0 0Transfer of intangibles 0 0Transfer of cash and cash equivalents 0 0Transfer of receivables 0 0Transfer of payables 0 0Transfer of provisions 0 0Net loss on transfers by absorption 0 0
12. Operating Leases
12.1 As lessee
12.1.1 Payments recognised as an Expense 2017-18Land Buildings Other Total Land Buildings£'000 £'000 £'000 £'000 £'000 £'000
Payments recognised as an expenseMinimum lease payments 0 125 18 143 0 152Contingent rents 0 0 0 0 0 0Sub-lease payments 0 0 0 0 0 0Total 0 125 18 143 0 152
12.1.2 Future minimum lease payments 2017-18Land Buildings Other Total Land Buildings£'000 £'000 £'000 £'000 £'000 £'000
Payable:No later than one year 0 125 18 143 0 - Between one and five years 0 0 0 0 0 - After five years 0 0 0 0 0 - Total 0 125 18 143 0 0
12.2 As lessor12.2.1 Rental revenue 2017-18 2016-17
£'000 £'000Recognised as incomeRent 0 0Contingent rents 0 0Total 0 0
12.2.2 Future minimum rental value 2017-18 2016-17£'000 £'000
Receivable:No later than one year 0 0Between one and five years 0 0After five years 0 0Total 0 0
Transfers as part of a reorganisation fall to be accounted for by use of absorption accounting in line with the Government Financial Reporting Manual, issued by HM Treasury. The Government Financial Reporting Manual does not require retrospective adoption, so prior year transactions (which have been accounted for under merger accounting) have not been restated. Absorption accounting requires that entities account for their transactions in the period in which they took place, with no restatement of performance required when functions transfer within the public sector. Where assets and liabilities transfer, the gain or loss resulting is recognised in the Statement of Comprehensive Net Expenditure, and is disclosed separately from operating costs.
Whilst our arrangements with NHS Property Services Limited, in relation to Cantilever House, fall within the definition of operating leases, the clinicais not party to any building related leases.The clinical commissioning group has two leases for two items of office equipment
Whilst our arrangements with NHS Property Services Limited, in relation to Cantilever House, fall within the definition of operating leases, rental chanot yet been agreed. Consequently this note does not include future minimum lease payments, for buildings, for the arrangements only.
165

NHS Lewisham CCG - Annual Accounts 2017-18
13 Property, plant and equipment
2017-18 Land
Buildings excluding dwellings Dwellings
Assets under construction
and payments on account
Plant & machinery
Transport equipment
Information technology
Furniture & fittings Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000Cost or valuation at 01 April 2017 0 0 0 0 0 0 0 0 0
Addition of assets under construction and payments on account 0 0Additions purchased 0 0 0 0 0 0 50 0 50Additions donated 0 0 0 0 0 0 0 0 0Additions government granted 0 0 0 0 0 0 0 0 0Additions leased 0 0 0 0 0 0 0 0 0Reclassifications 0 0 0 0 0 0 0 0 0Reclassified as held for sale and reversals 0 0 0 0 0 0 0 0 0Disposals other than by sale 0 0 0 0 0 0 0 0 0Upward revaluation gains 0 0 0 0 0 0 0 0 0Impairments charged 0 0 0 0 0 0 0 0 0Reversal of impairments 0 0 0 0 0 0 0 0 0Transfer (to)/from other public sector body 0 0 0 0 0 0 0 0 0Cumulative depreciation adjustment following revaluation 0 0 0 0 0 0 0 0 0Cost/Valuation at 31 March 2018 0 0 0 0 0 0 50 0 50
Depreciation 01 April 2017 0 0 0 0 0 0 0 0 0
Reclassifications 0 0 0 0 0 0 0 0 0Reclassified as held for sale and reversals 0 0 0 0 0 0 0 0 0Disposals other than by sale 0 0 0 0 0 0 0 0 0Upward revaluation gains 0 0 0 0 0 0 0 0 0Impairments charged 0 0 0 0 0 0 0 0 0Reversal of impairments 0 0 0 0 0 0 0 0 0Charged during the year 0 0 0 0 0 0 0 0 0Transfer (to)/from other public sector body 0 0 0 0 0 0 0 0 0Cumulative depreciation adjustment following revaluation 0 0 0 0 0 0 0 0 0Depreciation at 31 March 2018 0 0 0 0 0 0 0 0 0
Net Book Value at 31 March 2018 0 0 0 0 0 0 50 0 50
Purchased 0 0 0 0 0 0 50 0 50Donated 0 0 0 0 0 0 0 0 0Government Granted 0 0 0 0 0 0 0 0 0Total at 31 March 2018 0 0 0 0 0 0 50 0 50
Asset financing:
Owned 0 0 0 0 0 0 50 0 50Held on finance lease 0 0 0 0 0 0 0 0 0On-SOFP Lift contracts 0 0 0 0 0 0 0 0 0PFI residual: interests 0 0 0 0 0 0 0 0 0
Total at 31 March 2018 0 0 0 0 0 0 50 0 50
Revaluation Reserve Balance for Property, Plant & Equipment
Land Buildings Dwellings
Assets under construction & payments on account
Plant & machinery
Transport equipment
Information technology
Furniture & fittings Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000Balance at 01 April 2017 0 0 0 0 0 0 0 0 0
Revaluation gains 0 0 0 0 0 0 0 0 0Impairments 0 0 0 0 0 0 0 0 0Release to general fund 0 0 0 0 0 0 0 0 0Other movements 0 0 0 0 0 0 0 0 0Balance at 31 March 2018 0 0 0 0 0 0 0 0 0
166

NHS Lewisham CCG - Annual Accounts 2017-18
13 Property, plant and equipment cont'd
13.1 Cost or valuation of fully depreciated assets
The cost or valuation of fully depreciated assets still in use was as follows:2017-18 2016-17
£'000 £'000Land 0 0Buildings excluding dwellings 0 0Dwellings 0 0Plant & machinery 0 0Transport equipment 0 0Information technology 0 0Furniture & fittings 0 0Total 0 0
13.2 Economic lives
Buildings excluding dwellings 0 0Dwellings 0 0Plant & machinery 0 0Transport equipment 0 0Information technology 3 3Furniture & fittings 0 0
14 Intangible non-current assets
NHS Lewisham CCG had no intangible assets as at 31 March 2018 or during 2017-18.
15 Investment property
The clinical commissioning group had no investment property as at 31 March 2018.
16 Inventories
The clinical commissioning group had no inventories as at 31 March 2018.
Minimum Life (years)
Maximum Life (Years)
167

NHS Lewisham CCG - Annual Accounts 2017-18
17 Trade and other receivables Current Non-current Current Non-current2017-18 2017-18 2016-17 2016-17
£'000 £'000 £'000 £'000
NHS receivables: Revenue 1,257 0 1,514 0NHS receivables: Capital 0 0 0 0NHS prepayments 2,234 0 2,094 0NHS accrued income 1,623 0 161 0Non-NHS and Other WGA receivables: Revenue 313 0 397 0Non-NHS and Other WGA receivables: Capital 0 0 0 0Non-NHS and Other WGA prepayments 53 0 27 0Non-NHS and Other WGA accrued income 189 0 215 0Provision for the impairment of receivables 0 0 0 0VAT 10 0 45 0
Private finance initiative and other public private partnership arrangement prepayments and accrued income 0 0 0 0Interest receivables 0 0 0 0Finance lease receivables 0 0 0 0Operating lease receivables 0 0 0 0Other receivables and accruals 0 0 1 0Total Trade & other receivables 5,678 0 4,453 0
Total current and non current 5,678 4,453
Included above:Prepaid pensions contributions 0 0
17.1 Receivables past their due date but not impaired 2017-18 2017-18 2016-17£'000 £'000 £'000
DH Group Bodies
Group Bodies
All receivables prior years
By up to three months 34 68 53By three to six months 45 0 17By more than six months 5 49 2Total 84 117 72
£64k of the amount above has subsequently been recovered post the statement of financial position date.
The clinical commissioning group did not hold any collateral against receivables outstanding at 31 March 2018.
17.2 Provision for impairment of receivables 2017-18 2017-18 2016-17£'000 £'000 £'000
DH Group Bodies
Group Bodies
All receivables prior years
Balance at 01 April 2017 0 0 0
Amounts written off during the year 0 0 0Amounts recovered during the year 0 0 0(Increase) decrease in receivables impaired 0 0 0Transfer (to) from other public sector body 0 0 0Balance at 31 March 2018 0 0 0
The majority of trade is with NHS England. As NHS England is funded by Government to provide funding to clinical commissioning groups to commission services, no credit scoring of them is considered necessary.
168

NHS Lewisham CCG - Annual Accounts 2017-18
18 Other financial assets
The clinical commissioning group had no other financial assets as at 31 March 2018.
19 Other current assets
The clinical commissioning group had no other current assets as at 31 March 2018.
20 Cash and cash equivalents
2017-18 2016-17£'000 £'000
Balance at 01 April 2017 397 116Net change in year (306) 281Balance at 31 March 2018 91 397
Made up of:Cash with the Government Banking Service 91 397Cash with Commercial banks 0 0Cash in hand 0 0Current investments 0 0Cash and cash equivalents as in statement of financial position 91 397
Bank overdraft: Government Banking Service 0 0Bank overdraft: Commercial banks 0 0Total bank overdrafts 0 0
Balance at 31 March 2018 91 397
Patients’ money held by the clinical commissioning group, not included above 0 0
21 Non-current assets held for sale
22 Analysis of impairments and reversals
The clinical commissioning group had no non-current assets held for sale as at 31 March 2018.
The clinical commissioning group had no impairments or reversals of impairments recognised in expenditure during 2017-18.
169

NHS Lewisham CCG - Annual Accounts 2017-18
Current Non-current Current Non-current2017-18 2017-18 2016-17 2016-17
£'000 £'000 £'000 £'000
Interest payable 0 0 0 0NHS payables: revenue 4,634 0 5,052 0NHS payables: capital 0 0 0 0NHS accruals 5,436 0 7,369 0NHS deferred income 0 0 0 0Non-NHS and Other WGA payables: Revenue 2,785 0 705 0Non-NHS and Other WGA payables: Capital 0 0 0 0Non-NHS and Other WGA accruals 18,390 0 14,805 0Non-NHS and Other WGA deferred income 0 0 0 0Social security costs 26 0 52 0VAT 0 0 0 0Tax 68 0 54 0Payments received on account 0 0 0 0Other payables and accruals 657 0 272 0Total Trade & Other Payables 31,996 0 28,309 0
Total current and non-current 31,996 28,309
24 Other financial liabilitiesThe clinical commissioning group had no other financial liabilities as at 31 March 2018.
25 Other liabilitiesThe clinical commissioning group had no other liabilities as at 31 March 2018.
26 BorrowingsThe clinical commissioning group had no borrowings as at 31 March 2018.
27 Private finance initiative, LIFT and other service concession arrangementsThe clinical commissioning group had no private finance initiative, LIFT or other service concession as at 31 March 2018.
28 Finance lease obligationsThe clinical commissioning group had no finance lease obligations as at 31 March 2018.
29 Finance lease receivablesThe clinical commissioning group had no finance lease receivables as at 31 March 2018.
Other payables include £66k outstanding pension contributions at 31 March 2018
23 Trade and other payables
170

NHS Lewisham CCG - Annual Accounts 2017-18
30 ProvisionsCurrent Non-current Current Non-current2017-18 2017-18 2016-17 2016-17
£'000 £'000 £'000 £'000Pensions relating to former directors 0 0 0 0Pensions relating to other staff 0 0 0 0Restructuring 0 0 0 0Redundancy 0 0 0 0Agenda for change 0 0 0 0Equal pay 0 0 0 0Legal claims 0 0 0 0Continuing care 46 0 323 0Other 0 0 0 0Total 46 0 323 0
Total current and non-current 46 323
Pensions Relating to
Former Directors
Pensions Relating to Other Staff Restructuring Redundancy
Agenda for Change Equal Pay Legal Claims
Continuing Care Other Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Balance at 01 April 2017 0 0 0 0 0 0 0 323 0 323
Arising during the year 0 0 0 0 0 0 0 46 0 46Utilised during the year 0 0 0 0 0 0 0 (26) 0 (26)Reversed unused 0 0 0 0 0 0 0 (297) 0 (297)Unwinding of discount 0 0 0 0 0 0 0 0 0 0Change in discount rate 0 0 0 0 0 0 0 0 0 0Transfer (to) from other public sector body 0 0 0 0 0 0 0 0 0 0Transfer (to) from other public sector body under absorption 0 0 0 0 0 0 0 0 0 0Balance at 31 March 2018 0 0 0 0 0 0 0 46 0 46
Expected timing of cash flows:Within one year 0 0 0 0 0 0 0 46 0 46Between one and five years 0 0 0 0 0 0 0 0 0 0After five years 0 0 0 0 0 0 0 0 0 0Balance at 31 March 2018 0 0 0 0 0 0 0 46 0 46
Continuing Care provisions (£46k) relate to new continuing care claims arising in 2017-18There are no legal claims currently lodged with NHS Resolution.
171

NHS Lewisham CCG - Annual Accounts 2017-18
31 Contingencies
The clinical commissioning group had no contingent liabilities or contingent assets as at 31 March 2018.
32 Commitments
32.1 Capital commitments
The clinical commissioning group had no capital commitments as at 31 March 2018.
32.2 Other financial commitments
33 Financial instruments
33.1 Financial risk management
33.1.1 Currency risk
33.1.2 Interest rate risk
33.1.3 Credit risk
33.1.3 Liquidity risk
Because the majority of the NHS Clinical Commissioning Group and revenue comes parliamentary funding, NHS Clinical Commissioning Group has low exposure to credit risk. The maximum exposures as at the end of the financial year are in receivables from customers, as disclosed in the trade and other receivables note.
NHS Clinical Commissioning Group is required to operate within revenue and capital resource limits, which are financed from resources voted annually by Parliament. The NHS Clinical Commissioning Group draws down cash to cover expenditure, as the need arises. The NHS Clinical Commissioning Group is not, therefore, exposed to significant liquidity risks.
The NHS Clinical Commissioning Group has entered into no non-cancellable contracts (which are not leases, private finance initiative contracts or other service concession arrangements) during 2017-18.
Financial reporting standard IFRS 7 requires disclosure of the role that financial instruments have had during the period in creating or changing the risks a body faces in undertaking its activities.
Because NHS Clinical Commissioning Group is financed through parliamentary funding, it is not exposed to the degree of financial risk faced by business entities. Also, financial instruments play a much more limited role in creating or changing risk than would be typical of listed companies, to which the financial reporting standards mainly apply. The clinical commissioning group has limited powers to borrow or invest surplus funds and financial assets and liabilities are generated by day-to-day operational activities rather than being held to change the risks
Treasury management operations are carried out by the finance department, within parameters defined formally within the NHS Clinical Commissioning Group standing financial instructions and policies agreed by the Governing Body. Treasury activity is subject to review by the NHS Clinical Commissioning Group and internal auditors.
The NHS Clinical Commissioning Group is principally a domestic organisation with the great majority of transactions, assets and liabilities being in the UK and sterling based. The NHS Clinical Commissioning Group has no overseas operations. The NHS Clinical Commissioning Group and therefore has low exposure to currency rate fluctuations.
The Clinical Commissioning Group borrows from government for capital expenditure, subject to affordability as confirmed by NHS England. The borrowings are for 1 to 25 years, in line with the life of the associated assets, and interest is charged at the National Loans Fund rate, fixed for the life of the loan. The clinical commissioning group therefore has low exposure to interest rate fluctuations.
172

NHS Lewisham CCG - Annual Accounts 2017-18
33 Financial instruments cont'd
33.2 Financial assets
At ‘fair value through profit and
loss’Loans and
ReceivablesAvailable for
Sale Total2017-18 2017-18 2017-18 2017-18
£'000 £'000 £'000 £'000
Embedded derivatives 0 0 0 0Receivables:· NHS 0 2,879 0 2,879· Non-NHS 0 502 0 502Cash at bank and in hand 0 91 0 91Other financial assets 0 0 0 0Total at 31 March 2018 0 3,472 0 3,472
At ‘fair value through profit and
loss’Loans and
ReceivablesAvailable for
Sale Total2016-17 2016-17 2016-17 2016-17
£'000 £'000 £'000 £'000
Embedded derivatives 0 0 0 0Receivables:· NHS 0 1,674 0 1,674· Non-NHS 0 612 0 612Cash at bank and in hand 0 397 0 397Other financial assets 0 1 0 1Total at 31 March 2018 0 2,684 0 2,684
33.3 Financial liabilities
At ‘fair value through profit and
loss’ Other Total2017-18 2017-18 2017-18
£'000 £'000 £'000
Embedded derivatives 0 0 0Payables:· NHS 0 10,070 10,070· Non-NHS 0 21,832 21,832Private finance initiative, LIFT and finance lease obligations 0 0 0Other borrowings 0 0 0Other financial liabilities 0 0 0Total at 31 March 2018 0 31,902 31,902
At ‘fair value through profit and
loss’ Other Total2016-17 2016-17 2016-17
£'000 £'000 £'000
Embedded derivatives 0 0 0Payables:· NHS 0 12,422 12,422· Non-NHS 0 15,782 15,782Private finance initiative, LIFT and finance lease obligations 0 0 0Other borrowings 0 0 0Other financial liabilities 0 0 0Total at 31 March 2018 0 28,204 28,204
173
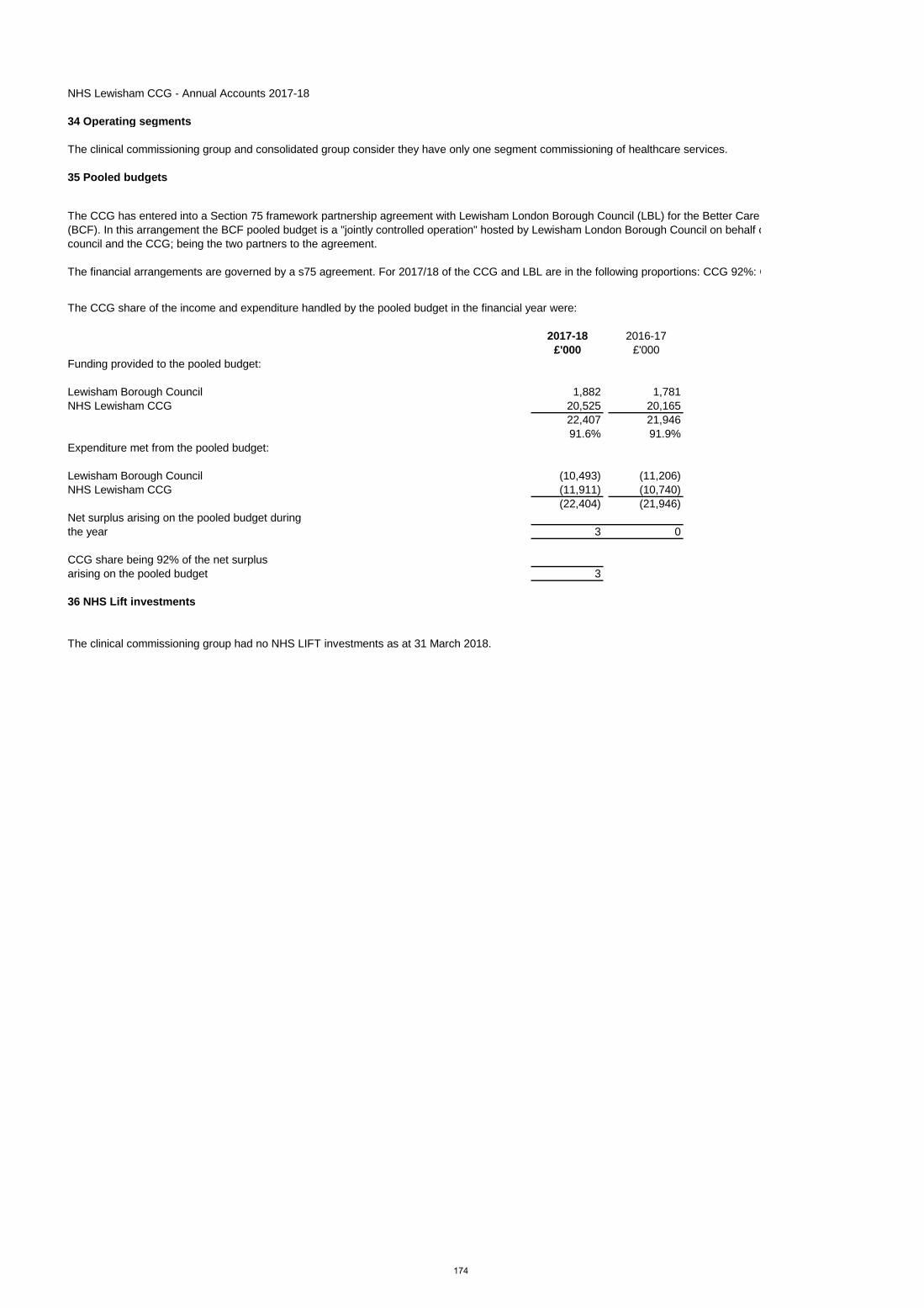
NHS Lewisham CCG - Annual Accounts 2017-18
34 Operating segments
The clinical commissioning group and consolidated group consider they have only one segment commissioning of healthcare services.
35 Pooled budgets
The financial arrangements are governed by a s75 agreement. For 2017/18 of the CCG and LBL are in the following proportions: CCG 92%: C
2017-18 2016-17£'000 £'000
Funding provided to the pooled budget:
Lewisham Borough Council 1,882 1,781NHS Lewisham CCG 20,525 20,165
22,407 21,94691.6% 91.9%
Expenditure met from the pooled budget:
Lewisham Borough Council (10,493) (11,206)NHS Lewisham CCG (11,911) (10,740)
(22,404) (21,946)Net surplus arising on the pooled budget during the year 3 0
CCG share being 92% of the net surplus arising on the pooled budget 3
36 NHS Lift investments
The CCG has entered into a Section 75 framework partnership agreement with Lewisham London Borough Council (LBL) for the Better Care (BCF). In this arrangement the BCF pooled budget is a "jointly controlled operation" hosted by Lewisham London Borough Council on behalf ocouncil and the CCG; being the two partners to the agreement.
The clinical commissioning group had no NHS LIFT investments as at 31 March 2018.
The CCG share of the income and expenditure handled by the pooled budget in the financial year were:
174

NHS Lewisham CCG - Annual Accounts 2017-18
37 Related party transactions
Payments to Related Party
Receipts from
Related Party
Amounts owed to Related Party
Amounts due from Related
Party
Payments to Related
Party
Receipts from
Related Party
Amounts owed to Related
Party
Amounts due from Related
Party£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
SELDOC LTD 1,130 0 201 0 774 0 120 0ONE HEALTH LEWISHAM LTD 3,377 0 1,016 0 589 0 0 0LONDONWIDE LMCs 145 0 0 0 0 0 0 0ST GEORGES UNIVERSITY HOSPITALS NHS FOUNDATION TRUST 851 0 185 0 663 0 0 88TOTAL 5,503 0 1,402 0 2,026 0 120 88
Payments to Related Party
Receipts from
Related Party
Amounts owed to Related Party
Amounts due from Related
Party
Payments to Related
Party
Receipts from
Related Party
Amounts owed to Related
Party
Amounts due from Related
Party£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
BELMONT HILL SURGERY 810 0 5 0 29 0 4 0JENNER PRACTICE 1,620 0 63 0 47 0 4 0SOUTH LEWISHAM GROUP PRACTICE 1,897 0 114 0 11 0 9 0MORNINGTON SURGERY 531 0 10 0 2 0 4 0QUEENS ROAD PARTNERSHIP 1,209 0 92 0 7 0 4 0DR JAINS PRACTICE 567 0 12 0 1 0 4 0LEWISHAM MEDICAL CENTRE 1,188 0 5 0 41 0 4 0SYDENHAM GREEN GROUP PRACTICE 1,533 0 179 0 39 0 4 0CLIFTON RISE PRACTICE 881 0 0 106 2 0 4 0PENROSE LEE SURGERY 761 0 20 0 28 0 4 0TORRIDON ROAD MEDICAL PRACTICE 1,336 0 8 0 7 0 4 0MORDEN HILL SURGERY 1,115 0 0 0 41 0 5 0BARING ROAD MEDICAL CENTRE 950 0 0 38 3 0 4 0ST JOHNS MEDICAL CENTRE 1,830 0 17 0 49 0 19 0LEES ROAD SURGERY 1,362 0 33 0 41 0 4 0BROCKLEY SURGERY 618 0 35 0 17 0 4 0HILLY FIELDS MEDICAL CENTRE 1,530 0 7 0 54 0 4 0DOWNHAM FAMILY MEDICAL PRACTICE 686 0 123 0 1 0 4 0WOOLSTONE MEDICAL CENTRE 1,024 0 13 0 24 0 4 0NEW CROSS HEALTH CENTRE 614 0 35 0 1 0 7 0SYDENHAM SURGERY 467 0 9 0 15 0 4 0GROVE MEDICAL CENTRE LONDON 1,146 0 35 0 27 0 4 0HONOR OAK GROUP PRACTICE 998 0 90 0 58 0 4 0CHINBROOK SURGERY 1,285 0 92 0 1 0 4 0VESTA ROAD SURGERY 733 0 0 66 8 0 4 0WELLS PARK PRACTICE 1,327 0 37 0 38 0 4 0DR BR JACOBS 807 0 15 0 25 0 4 0PARKVIEW SURGERY LONDON 562 0 19 0 13 0 4 0BELLINGHAM GREEN SURGERY 904 0 30 0 27 0 5 0RUSHEY GREEN GROUP PRACTICE 1,708 0 90 0 114 0 18 0VALE MEDICAL CENTRE 1,430 0 6 0 44 0 4 0AMERSHAM VALE TRAINING PRACTICE 983 0 260 0 1 0 4 0DEPTFORD SURGERY 510 0 7 0 8 0 4 0OAKVIEW FAMILY PRACTICE 567 0 16 0 1 0 4 0WALDRON HEALTH CENTRE 623 0 222 0 1 0 4 0WOODLANDS HEALTH CENTRE LONDON 1,007 0 34 0 43 0 4 0NIGHTINGALE SURGERY LONDON 687 0 9 0 23 0 4 0DEPTFORD MEDICAL CENTRE 387 0 13 0 3 0 4 0LEWISHAM GP LED HEALTH CENTRE 496 0 373 0 2 0 4 0TOTAL 38,689 0 2,129 210 897 0 195 0
Notes:-
Payments to Related Party
Receipts from
Related Party
Amounts owed to Related Party
Amounts due from Related
Party
Payments to Related
Party
Receipts from
Related Party
Amounts owed to Related
Party
Amounts due from Related
Party£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
GUYS & ST THOMAS HOSPITAL NHS FOUNDATION TRUST 43,627 460 115 0 43,293 503 886 0KING`S COLLEGE HOSPITAL NHS FOUNDATION TRUST 36,181 0 566 0 32,924 0 589 353LEWISHAM & GREENWICH NHS TRUST 168,201 0 3,002 0 158,069 154 5,594 1,799SOUTH LONDON AND MAUDSLEY NHS FOUNDATION TRUST 64,892 116 209 0 63,679 116 1,944 0NHS BEXLEY CCG 0 6 0 0 29 202 23 87NHS BROMLEY CCG 97 28 14 0 965 23 426 1NHS GREENWICH CCG 216 31 138 0 189 286 137 121NHS LAMBETH CCG 72 334 0 0 98 462 2 98NHS SOUTHWARK CCG 4 2,060 0 0 728 559 97 176NHS ENGLAND 39 1,592 0 0 396 980 0 1,979LONDON AMBULANCE SERVICE NHS TRUST 11,450 0 351 0 11,492 0 757 0TOTAL 324,780 4,627 4,395 0 311,862 3,285 10,455 4,614
LONDON BOROUGH OF LEWISHAM 25,526 934 5,549 0 29,344 1,069 4,071 331
Notes:-
The transactions in relation to interests declared by Governing Body members (excluding transactions with GP practices, Department of Health and Social Care bodies and other government departments)
2017-18 2016-17
The transactions with GP practices where GP practices are members of NHS Lewisham CCG, where GP Practices employed the Chair and/or Clinical Directors of the NHS Lewisham CCG Governing Body as partners or salaried GPs or where GP practices employed GPs or Non GP Partners that have contributed to the work of NHS Lewisham CCG
2017-18 2016-17
1 The payments above are not made to the individuals themselves but to their associated General Practice for clinical services commissioned by the CCG. These payments to the GP Practices exclude funding for prescribing.
2 The values of transactions in 2017/18 are significantly higher than 2016/17 due to the delegation to the CCG of primary care co-commissioning responsibility from 1st April 2017.
2 In 2017/18 the CCG also made payments to NHS Property Services Ltd, HM Revenue and Customs, NHS Business Services Authority and NHS Resolution.
1 A financial risk share agreement is in place across the six CCGs in south east London. It was agreed through the governance of each CCG that the risk share agreement be enacted in 2017/18. The final revenue resource limit values included in the 2017/18 annual accounts of each CCG reflect the outcome of the risk share agreement
Material transactions with Department of Health and Social Care group organisations2017-18 2016-17
175

NHS Lewisham CCG - Annual Accounts 2017-18
38 Events after the end of the reporting period
39 Third party assets
The clinical commissioning group held no third party assets as at 31 March 2018.
40 Financial performance targets
NHS Clinical Commissioning Group have a number of financial duties under the NHS Act 2006 (as amended).NHS Clinical Commissioning Group performance against those duties was as follows:
2017-18 2017-18 2016-17 2016-17Target Performance Target Performance
£'000 £'000 £'000 £'000Expenditure not to exceed income 477,140 476,160 431,287 421,257Capital resource use does not exceed the amount specified in Directions 50 50 0 0Revenue resource use does not exceed the amount specified in Directions 471,333 470,353 427,168 417,138Capital resource use on specified matter(s) does not exceed the amount specified in Directions 0 0 0 0Revenue resource use on specified matter(s) does not exceed the amount specified in Directions 0 0 0 0Revenue administration resource use does not exceed the amount specified in Directions 6,651 6,260 6,608 6,539
41 Impact of IFRSAccounting under IFRS had no impact on the results of the clinical commissioning group during the 2017-18 financial year.
With effect from 1st April 2018, the management structure across the south east London CCGs has moved to there being one Accountable Officer and one Chief Financial Officer across Bexley, Bromley, Greenwich, Lewisham and Southwark CCGs. There is a Director of Finance managing Lewisham and Greenwich CCGs and one Director of Finance managing Bexley, Bromley and Southwark CCGs. There is also a Strategic Finance Director who is responsible for overseeing the STP financial plan which includes both commissioners and providers. A separate Accountable Officer is responsible for Lambeth and Croydon CCGs (as is currently the case) and Lambeth CCG have a separate Chief Financial Officer. There has been a phased transition to this structure and there is not expected to be any impact from these changes for the organisations in question.
As a result of an amended calculation methodology from NHS England, the 2017/18 in year revenue allocation has been calculated on the basis of the total allocation, adjusted for the historic financial outturn of the CCG. In 2016/17 the figure was recorded as just the total in year allocation notified to the CCG
176