Simvastatin in Acute Respiratory Distress Syndrome · Simvastatin in Acute Respiratory Distress...
24
Confidential: For Review Please review the Supplemental Files folder to review documents not compiled in the PDF. Simvastatin in Acute Respiratory Distress Syndrome Journal: New England Journal of Medicine Manuscript ID: 14-03285.R2 Article Type: Rapid Review Date Submitted by the Author: n/a Complete List of Authors: McAuley, Daniel; The Queen's University of Belfast, Centre for Infection and Immunity Laffey, John; National University of Ireland, Galway, School of Medicine O'Kane, Cecilia; Queen's University of Belfast, Centre of Infection and Immunity Perkins, Gavin; Heart of England NHS Foundation Trust, Academic Dept of Critical Care Mullan, Brian; Royal Victoria Hospital, Regional Intensive Care Dept Trinder, John; The Ulster Hospital, Intensive Care Dept Johnston, Paul; Antrim Area Hospital, Intensive Care Unit Hopkins, Philip; Kings College Hospital, Surgical Critical Care Unit Johnston, Andrew; Addenbrooke's Hospital, John Farman Intensive Care Unit McDowell, Cliona; Northern Ireland Clinical Trials Unit, McNally, Christine; Northern Ireland Clinical Trials Unit, Abstract: Background: There are in vitro, animal and phase 2 studies suggesting that statins may be beneficial in the acute respiratory distress syndrome (ARDS). This study tested the hypothesis that treatment with simvastatin would improve clinical outcomes in patients with ARDS. Methods: In this multicentre, allocation concealed, double-blind clinical trial, patients with an onset of ARDS within the previous 48 hours were randomized in a 1:1 ratio to receive enteral simvastatin 80mg or placebo once daily for a maximum of 28 days. The primary outcome was the number of ventilator-free days to day 28. Secondary outcomes included number of non-pulmonary organ failure free days to day 28, mortality at 28 days and safety. Results: The study recruited 540 patients with 259 patients allocated to simvastatin and 281 patients to placebo. The groups were well matched with respect to demographic and baseline physiological variables. There was no significant difference between study groups in mean (± SD) ventilator-free days (12.6±9.9 with simvastatin and 11.5±10.4 with placebo, P = 0.21), non-pulmonary organ failure free days (19.4±11.1 with simvastatin and 17.8±11.7 with placebo, P = 0.11) or in 28-day mortality (22.0% with simvastatin and 26.8% with placebo, P = 0.23). There was no difference in the incidence of severe adverse events between the groups. Conclusions: Simvastatin therapy, while safe and with minimal adverse effects, did not improve clinical outcomes in patients with ARDS. (Funded by the UK National Institute for Health Research Efficacy and Confidential: Destroy when review is complete. Submitted to the New England Journal of Medicine
Transcript of Simvastatin in Acute Respiratory Distress Syndrome · Simvastatin in Acute Respiratory Distress...

Confidential: For Review
Please review the Supplemental Files folder to review documents not compiled in the PDF.
Simvastatin in Acute Respiratory Distress Syndrome
Journal: New England Journal of Medicine
Manuscript ID: 14-03285.R2
Article Type: Rapid Review
Date Submitted by the Author: n/a
Complete List of Authors: McAuley, Daniel; The Queen's University of Belfast, Centre for Infection and Immunity Laffey, John; National University of Ireland, Galway, School of Medicine O'Kane, Cecilia; Queen's University of Belfast, Centre of Infection and Immunity Perkins, Gavin; Heart of England NHS Foundation Trust, Academic Dept of Critical Care Mullan, Brian; Royal Victoria Hospital, Regional Intensive Care Dept Trinder, John; The Ulster Hospital, Intensive Care Dept Johnston, Paul; Antrim Area Hospital, Intensive Care Unit
Hopkins, Philip; Kings College Hospital, Surgical Critical Care Unit Johnston, Andrew; Addenbrooke's Hospital, John Farman Intensive Care Unit McDowell, Cliona; Northern Ireland Clinical Trials Unit, McNally, Christine; Northern Ireland Clinical Trials Unit,
Abstract:
Background: There are in vitro, animal and phase 2 studies suggesting that statins may be beneficial in the acute respiratory distress syndrome (ARDS). This study tested the hypothesis that treatment with simvastatin would improve clinical outcomes in patients with ARDS. Methods: In this multicentre, allocation concealed, double-blind clinical trial, patients with an onset of ARDS within the previous 48 hours were randomized in a 1:1 ratio to receive enteral simvastatin 80mg or placebo
once daily for a maximum of 28 days. The primary outcome was the number of ventilator-free days to day 28. Secondary outcomes included number of non-pulmonary organ failure free days to day 28, mortality at 28 days and safety. Results: The study recruited 540 patients with 259 patients allocated to simvastatin and 281 patients to placebo. The groups were well matched with respect to demographic and baseline physiological variables. There was no significant difference between study groups in mean (± SD) ventilator-free days (12.6±9.9 with simvastatin and 11.5±10.4 with placebo, P = 0.21), non-pulmonary organ failure free days (19.4±11.1 with simvastatin and 17.8±11.7 with placebo, P = 0.11) or in 28-day mortality
(22.0% with simvastatin and 26.8% with placebo, P = 0.23). There was no difference in the incidence of severe adverse events between the groups. Conclusions: Simvastatin therapy, while safe and with minimal adverse effects, did not improve clinical outcomes in patients with ARDS. (Funded by the UK National Institute for Health Research Efficacy and
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine

Confidential: For Review
Mechanism Evaluation Programme and others; Current Controlled Trials number, ISRCTN88244364.)
Page 1 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 1 -
Simvastatin in Acute Respiratory Distress Syndrome
Prof Daniel F McAuley MD1,2,3*
, Prof John G Laffey MD4,5
, Dr Cecilia M O’Kane PhD1,
Prof Gavin D Perkins MD6,7
, Dr Brian Mullan MB2, Dr T John Trinder MB
8, Dr Paul
Johnston MB9, Dr Philip A Hopkins PhD
10, Dr Andrew J Johnston MD
11, Cliona
McDowell MSc3, Christine McNally BA
3, and the HARP-2 investigators* on behalf of the
Irish Critical Care Trials Group.
1 Centre for Infection and Immunity, Queen's University of Belfast, Belfast BT9 7AE,
UK
2 Regional Intensive Care Unit, Royal Victoria Hospital, Belfast BT12 6BA, UK
3 Northern Ireland Clinical Trials Unit, Royal Victoria Hospital, Belfast BT12 6BA, UK
4 Anaesthesia, School of Medicine, HRB Galway Clinical Research Facility, Clinical
Sciences Institute, National University of Ireland, Galway, Ireland
5 Department of Anesthesia, Centre for Critical Care Research, Keenan Research Centre
for Biomedical Science, St. Michael's Hospital, University of Toronto, Canada.
6 Heart of England NHS Foundation Trust, Bordesley Green East, Birmingham B9 5SS,
UK
7. Warwick Medical School Clinical Trials Unit, University of Warwick, Warwick CV4
7AL, UK
8. Intensive Care Unit, The Ulster Hospital, Upper Newtownards Road, Belfast BT16
1RH, UK
9 Intensive Care Unit, Antrim Area Hospital, Antrim BT41 2RL, UK
10 Critical Care Units, King's Health Partners (King's College Hospital), London SE5
9RS, UK
Page 2 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 2 -
11 John Farman Intensive Care Unit, Cambridge University Hospitals NHS Foundation
Trust, Cambridge CB2 0QQ, UK
* HARP-2 investigators are listed in the Supplementary Appendix, available at NEJM.org.
*Corresponding author
Professor Danny McAuley
Centre for Infection and Immunity, Queen's University of Belfast
Health Sciences Building, 97 Lisburn Road
Belfast, BT9 7AE
UK
Telephone: 02890 972144
Fax: 02890 972671
Email: [email protected]
Source of funding: This study was funded by the UK National Institute for Health
Research, Efficacy and Mechanism Evaluation (EME) programme (08/99/08). This study
was also funded in Ireland by the Health Research Board (HRA_POR-2010-131). The HSC
R&D Division, Public Health Agency in Northern Ireland, the Intensive Care Society of
Ireland and REVIVE provided additional funding.
Word count (excluding abstract, references and legends): 2325
Page 3 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 3 -
Abstract
Background: There are in vitro, animal and phase 2 studies suggesting that statins may be
beneficial in the acute respiratory distress syndrome (ARDS). This study tested the
hypothesis that treatment with simvastatin would improve clinical outcomes in patients
with ARDS.
Methods: In this multicentre, allocation concealed, double-blind clinical trial, patients with
an onset of ARDS within the previous 48 hours were randomized in a 1:1 ratio to receive
enteral simvastatin 80mg or placebo once daily for a maximum of 28 days. The primary
outcome was the number of ventilator-free days to day 28. Secondary outcomes included
number of non-pulmonary organ failure free days to day 28, mortality at 28 days and
safety.
Results: The study recruited 540 patients with 259 patients allocated to simvastatin and 281
patients to placebo. The groups were well matched with respect to demographic and
baseline physiological variables. There was no significant difference between study groups
in mean (± SD) ventilator-free days (12.6±9.9 with simvastatin and 11.5±10.4 with placebo,
P = 0.21), non-pulmonary organ failure free days (19.4±11.1 with simvastatin and
17.8±11.7 with placebo, P = 0.11) or in 28-day mortality (22.0% with simvastatin and
26.8% with placebo, P = 0.23). There was no difference in the incidence of severe adverse
events between the groups.
Conclusions: Simvastatin therapy, while safe and with minimal adverse effects, did not
improve clinical outcomes in patients with ARDS.
(Funded by the UK National Institute for Health Research Efficacy and Mechanism
Evaluation Programme and others; Current Controlled Trials number, ISRCTN88244364.)
(Abstract 249 words)
Key Words: simvastatin, acute respiratory distress syndrome
Page 4 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 4 -
Background
The acute respiratory distress syndrome (ARDS) is a common devastating clinical
syndrome characterized by life-threatening respiratory failure requiring mechanical
ventilation and multiple organ failure. ARDS is characterized by an uncontrolled
inflammatory response which results in alveolar damage with exudation of protein rich
pulmonary oedema fluid in the alveolar space1. Hydroxyl-methylglutaryl coenzyme A
reductase inhibition with statins has been shown to modify a number of the underlying
mechanisms implicated in the development of ARDS2. Statins decrease inflammation and
histological evidence of lung injury in murine models of ARDS3. Simvastatin reduced
pulmonary and systemic inflammatory responses in a human model of ARDS induced by
LPS inhalation4. In addition in a small single centre, randomized, placebo-controlled study
simvastatin improved non-pulmonary organ dysfunction and was safe5. That phase 2 study
was not designed or powered to show an effect of simvastatin on clinical outcomes. The
aim of this trial was to test the hypothesis that treatment with enteral simvastatin 80mg
would improve clinical outcomes in patients with ARDS irrespective of etiology.
Study design
Patients were recruited from adult general intensive care units (ICUs) in 40 hospitals in the
United Kingdom and Ireland (see the Supplementary Appendix, available with the full text
of this article at NEJM.org). The study was approved by a research ethics committee
(10/NIR02/36) and research governance departments at each site in the UK and by the
institutional Research Ethics Committee at each site in Ireland. The Northern Ireland
Clinical Trials Unit coordinated the overall trial, with support from the HRB Galway
Clinical Research Facility for centres in Ireland. Patients or their representatives provided
written informed consent. Simvastatin was purchased for use in the study.
Page 5 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 5 -
The study design has been published in detail previously6 and the study protocol and
statistical analysis plan are available at NEJM.org.
Patients
Patients were eligible if they were intubated and mechanically ventilated and had a partial
pressure of arterial oxygen to fractional inspired oxygen concentration (PaO2/FIO2) ratio of
300 mmHg or less, if bilateral pulmonary infiltrates consistent with pulmonary edema were
present on chest radiograph, and if there was no evidence of left atrial hypertension7.
Exclusion criteria are listed in Fig. 1 and in full in the protocol at NEJM.org. The study was
amended to permit enrolment of patients receiving macrolides and for the level of alanine
aminotransferase and/or aspartate aminotransferase for eligibility to be increased from more
than 5 times to 8 times the upper limit of the normal range.
Study medication
Patients were randomized in a 1:1 ratio using an automated centralised 24-hour
randomization service. Randomization was by permuted block stratified by site and by
vasopressor requirement.
Patients received once daily simvastatin 80mg or identical placebo tablets enterally for up
to 28 days. The first dose of study drug was administered as soon as possible, ideally within
4 hours of randomization, and subsequent doses were given each morning starting on the
following calendar day.
Study drug was continued until day 28, discharge from critical care, death or
discontinuation of active medical treatment, development of a clinical condition requiring
immediate treatment with a statin or withdrawal of the patient from the study. The study
drug was stopped on safety grounds if the attending clinician determined that this was
Page 6 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 6 -
required, if the levels of creatine kinase were more than 10 times the upper limit of the
normal range or if the levels of alanine aminotransferase and/or aspartate aminotransferase
were more than 8 times the upper limit of the normal range.
Data collection and procedures
At enrolment, the patients’ demographic characteristics, ventilatory and physiological
variables and admission acute physiology and chronic health evaluation II (APACHE II)
scores were recorded. The cause of ARDS was identified by the treating clinician. For each
day in the ICU, ventilatory and physiological variables as well as data on organ support
based on the United Kingdom’s critical care minimum data set8 were recorded. Vital status
at 28 days was collected but cause of death was not recorded.
Participating ICUs were encouraged to use low tidal volume ventilation at 6 to 8 ml per
kilogram of predicted body weight and to maintain plateau pressure less than 30 cmH2O9,
but no specific ventilator management scheme was promulgated. All other treatment was
determined by the patients’ physicians.
Outcome measures
The primary outcome measure was ventilator-free days (VFDs) to day 28 defined as the
number of days from the time of initiating unassisted breathing, to day 28 after
randomization6. A detailed definition of VFDs is provided in the study protocol available at
NEJM.org. Secondary outcomes included change in oxygenation index (OI) and sequential
organ failure assessment (SOFA) score10 up to day 28, number of non-pulmonary organ
failure free days (OFFDs) to day 28, all cause mortality 28 days post randomization,
mortality at discharge from critical care and from hospital, and safety.
Page 7 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 7 -
Additional secondary outcomes are listed in the protocol. Plasma C-reactive protein (CRP)
was measured by immunoturbidimetric assay (Randox Testing Services, UK) in blood
obtained at baseline, day 3 and 7.
Statistical analysis
Sample size assumptions were based on previously published data5,9
. Assuming a mean
(SD) for VFDs of 12.7 (10.6) days, a sample size of 524 subjects would need to be enrolled
to have 80% power at a two-tailed significance level of 0.05 to detect a mean difference of
2.6 VFDs. Data from the PAC-Man trial were used to estimate a dropout rate of 3%11 and
therefore the study required a total of 540 patients.
Analyses were on an intention-to-treat basis. As VFDs and non-pulmonary OFFDs are
known to have a bimodal distribution, the groups were initially analysed by t-test with
difference in means and 95% confidence intervals (CI) presented. A secondary analysis of
these outcome measures involving a bootstrapped t-test was also conducted to support the
findings of the t-tests as detailed in the statistical analysis plan available at NEJM.org. For
binary outcome measures, risk ratios and associated 95% CI were calculated. Time-to-event
data are presented using Kaplan-Meier plots. The hazard ratios (HR) were calculated and
the log rank chi-square test used to compare the survival function of treatment arms. All
HRs are presented with a 2-sided 95% CI. All P values are 2-sided. To assess whether
treatment was more or less effective in pre-defined subgroups, analyses were undertaken to
analyse whether the treatment effect was modified by age, vasopressor requirement,
presence of sepsis and baseline CRP. Subgroup analyses used a statistical test for
interaction and are reported using 99% CI.
Page 8 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 8 -
Results
Participants
Patients were recruited from 21st December 2010 until 13th March 2014. Of the 5926
patients who were assessed for eligibility, 540 (9%) underwent randomization. Four
patients who did not fulfil the eligibility criteria were randomized in each group and are
included in the analysis. Five patients allocated to simvastatin and 3 patients in the placebo
group did not receive study drug. One patient in the simvastatin group was lost to follow-
up. No data on the primary outcome was available in 1 patient in the simvastatin group and
2 patients in the placebo group (Fig. 1).
The baseline characteristics of the patients at randomization were similar in the two study
groups except for a small but statistically significant lower PaO2/FIO2 ratio in the
simvastatin group (Table 1). The main causes of ARDS were pneumonia and sepsis. There
was no significant difference in tidal volume at day 3; mean difference (95% CI) was 0.1 (-
0.6 to 0.7) ml/kg predicted body weight (P = 0.89).
Patients received study drug for a mean (±SD) of 10.2 ± 7.1 days in the simvastatin group
and 11 ± 7.9 days in the placebo group (P = 0.23). The commonest reasons for
discontinuation of study drug were discharge from critical care, death and a study drug
related adverse event. Five patients allocated to simvastatin and 3 patients allocated to
placebo received treatment with non-trial statins (Table S1 in the Supplementary
Appendix).
Outcomes
The number of ventilator-free days was not significantly different between the study groups
(12.6±9.9 with simvastatin and 11.5±10.4 with placebo, mean difference (95% CI) of 1.1 (-
0.6 to 2.8); P = 0.21). There was no significant difference in the number of ventilator-free
Page 9 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 9 -
days after adjusting for the baseline PaO2/FIO2 ratio (mean difference (95% CI) of 1.4 (-0.3
to 3.2); P = 0.10).
There were no significant differences in the change in oxygenation index (Tables S2 and S3
in the Supplementary Appendix) or SOFA score from baseline between the groups (Table
S2 in the Supplementary Appendix). There was no significant difference in the number of
non-pulmonary organ failure free days or 28-day mortality. Mortality at critical care
discharge or hospital discharge was also not significantly different (Table 2). For survivors
only, the duration of ICU stay was 13.9±14.4 days in the simvastatin group and 14.4±13.3
days in the placebo group (mean difference (95% CI) of -0.5 (-3.2 to 2.2); P = 0.71); the
duration of hospital stay was 37.7±64.5 days and 35.4±31.1 days, respectively (mean
difference (95% CI) of 2.3 (-8.0 to 12.6); P = 0.66). There was no significant difference in
the probability of breathing without assistance to day 28 or survival (Fig. 2).
Subgroup analyses did not suggest that the effects of simvastatin were modified by any of
the variables investigated. There was no statistically significant interaction between
treatment and age (P = 0.62), vasopressor requirement (P = 0.17), presence of sepsis (P =
0.50) and baseline C-reactive protein (CRP) (P = 0.77) (Table S4 in the Supplementary
Appendix).
There were no differences in plasma CRP between the simvastatin and placebo groups at
baseline, at day 3 or day 7 or in the change in the CRP from baseline (Tables S5 and S6 in
the Supplementary Appendix).
Overall adverse events related to study drug were significantly more common in the
simvastatin group. The majority were related to elevated creatine kinase and hepatic
transaminases. Serious adverse events (SAEs) (other than those reported as trial outcomes
e.g. death) were similar in both groups (Table S7 in the Supplementary Appendix). There
was no difference in the proportion of patients with non-pulmonary organ dysfunction as
Page 10 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 10 -
measured by a SOFA score less than 2, by organ, between the groups (Table S8 in the
Supplementary Appendix).
Discussion
In this large, multicentre, double-blind, randomized, placebo-controlled clinical trial in
patients with ARDS, simvastatin did not improve clinical outcomes. Simvastatin was
associated with an increase in adverse events; however there was no increase in serious
adverse events. The recent SAILS study in patients with sepsis-induced ARDS found
rosuvastatin did not improve clinical outcomes and was associated with fewer days free of
renal and hepatic failure12 The patient population in this study was not limited to sepsis-
induced ARDS, and therefore taken together these data do not support the routine use of
statins in ARDS, regardless of aetiology.
We used simvastatin 80mg based on our previous human data4,5
where simvastatin
improved surrogate outcomes and biological mechanisms implicated in ARDS. The data
from this study and SAILS demonstrate that neither lipophilic (simvastatin) nor hydrophilic
(rosuvatatin) statins are effective in ARDS. The high dose (80mg) used in this trial was
selected based on our pilot data5 as well as pre-clinical data
3 and observational studies
13,14
which supported using a higher dose. While we did not measure simvastatin concentrations,
it is likely that an adequate simvastatin concentration was achieved for several reasons.
Prior studies in the critically ill indicate that simvastatin 80mg daily produces systemic
drug concentrations that are in the high therapeutic range15. Furthermore patients received
simvastatin for a mean of 10 days. Finally the increased incidence of expected statin related
adverse events suggest that sufficient simvastatin concentrations were achieved. The lack of
an effect on plasma CRP suggests that statins are unable to modulate inflammation
sufficiently to translate into a beneficial clinical effect in ARDS. It is possible that
Page 11 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 11 -
HMGCo-A reductase is already significantly inhibited as reflected by the low cholesterol
levels seen in the critically ill16.
Although there was a higher incidence of adverse events related to simvastatin, the number
of serious adverse events were similar in both groups. The finding that the proportion of
patients with no organ dysfunction as measured by SOFA score over the course of the study
was similar in both groups is reassuring. The absence of serious harm with simvastatin in
this population provides reassurance in regard to the safety of statins in patients with ARDS
used for other proven indications.
We recruited a heterogeneous cohort of patients with ARDS due to any etiology to ensure
that our findings would be generalisable. Recent data have suggested that it may be
possible to identify specific phenotypes within ARDS17. Future studies may identify an
ARDS subpopulation which might be more responsive to simvastatin.
Although we recommended best practice for ARDS including lung protective ventilation,
we did not measure details of clinical management. At randomization, the tidal volume was
8.1ml/kg predicted body weight and it is possible that this level of tidal volume may have
confounded the potential effects of simvastatin. However this is unlikely given the similar
absence of benefit for rosuvastatin in the SAILS study where the mean tidal volume was
6.6-6.8ml/kg predicted body weight. Our data for tidal volume and plateau pressure are
consistent with those seen in other clinical trials in critical care where ventilation is not
strictly protocolized18.
Despite promising findings for statins in ARDS in early phase clinical trials, these have not
been translated into improvements in patient centred outcomes in large clinical trials.
Another recent randomized controlled trial in patients with ventilator associated pneumonia
found simvastatin did not improve clinical outcomes19. Data on efficacy based on surrogate
outcomes must be considered with caution given lack of clear correlation between surrogate
Page 12 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 12 -
and patient centred outcomes. More work is required to identify surrogates outcomes which
more closely track patient outcomes.
In conclusion, our study showed that simvastatin, while safe and generally well tolerated,
did not increase the number of ventilator free days or improve other clinical outcomes in
patients with ARDS. These results do not support the use of simvastatin in the management
of ARDS.
Author contributions
DM conceived the study. DM, JGL and CMO designed and obtained the funding for the
study. DM, JGL, CMD and CMN managed the undertaking of the trial with the clinical
trials unit. All authors made a substantial contribution to the protocol development. DFM,
JGL, GDP, BM, JT, PJ, PAH and AJJ contributed substantially to patient recruitment and
data collection. CMD was the study statistician and DM, JGL and CMO interpreted the
data. DM wrote the first draft of the manuscript and all authors have reviewed and have
approved this final version of the manuscript.
Acknowledgements
This project was supported by the Efficacy and Mechanism Evaluation (EME) Programme,
an MRC and NIHR partnership (08/99/08). The EME Programme is funded by the MRC
and NIHR, with contributions from the CSO in Scotland and NISCHR in Wales and the
HSC R&D Division, Public Health Agency in Northern Ireland. The views expressed in
this publication are those of the authors and not necessarily those of the MRC, NHS, NIHR
or the Department of Health. This study was also funded in Ireland by a Health Research
Award from the Health Research Board, Dublin, Ireland (HRA_POR-2010-131). The HSC
R&D Division, Public Health Agency in Northern Ireland and the Intensive Care Society of
Page 13 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 13 -
Ireland and REVIVE provided additional funding. DFM and GDP are Directors of
Research for the Intensive Care Foundation and the support of the UK Intensive Care
Foundation is gratefully acknowledged. We thank all patients and their legal representatives
who participated in the trial, all the research nurses and the pharmacists in all participating
centres for their help, and medical and nursing staff in participating centres who cared for
patients and collected data. We thank Regina Verghis, Evie Gardner and all the staff of the
Northern Ireland Clinical Trials Unit for their support in delivering this trial. We thank
Michael Faherty, Emma Deenihan, Veronica McInerney and Lisa Daly from the HRB
Galway Clinical Research Facility, Galway, Ireland, for their help in conducting the study
in Ireland. We are grateful for the support of Margaret McFarland and staff at Victoria
Pharmaceuticals (Belfast, UK) for management of the study drug. We are grateful for the
support of the Intensive Care National Audit and Research Centre (ICNARC) for providing
APACHE II data for sites that participate in ICNARC’s Case Mix Programme. The authors
acknowledge the support of the Northern Ireland Clinical Research Network and the
National Institute for Health Research Clinical Research Network.
References
1. Ware LB, Matthay MA. The Acute Respiratory Distress Syndrome. N Engl J Med
2000;342:1334-49.
2. Terblanche M, Almog Y, Rosenson RS, Smith TS, Hackam DG. Statins: panacea
for sepsis? Lancet Infect Dis 2006;6:242-8.
3. Jacobson JR, Barnard JW, Grigoryev DN, Ma S-F, Tuder RM, Garcia JGN.
Simvastatin attenuates vascular leak and inflammation in murine inflammatory lung injury.
Am J Physiol Lung Cell Mol Physiol 2005;288:L1026-32.
Page 14 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 14 -
4. Shyamsundar M, McKeown S, O’Kane C, et al. Simvastatin decreases
lipopolysaccharide-induced pulmonary inflammation in healthy volunteers. Am J Respir
Crit Care Med 2009;179:1107-14.
5. Craig TR, Duffy MJ, Shyamsundar M, et al. A randomized clinical trial of
hydroxymethylglutaryl- coenzyme a reductase inhibition for acute lung injury (The HARP
Study). Am J Respir Crit Care Med 2011;183:620-6.
6. McAuley DF, Laffey JG, O'Kane CM, et al. Hydroxymethylglutaryl-CoA reductase
inhibition with simvastatin in Acute lung injury to Reduce Pulmonary dysfunction (HARP-
2) trial: study protocol for a randomized controlled trial. Trials 2012;13:170.
7. Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus
Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial
coordination. Am J Respir Crit Care Med 1994;149:818-24.
8. Felton TW, Sander R, Al-Aloul M, Dark P, Bentley AM. Can a score derived from
the Critical Care Minimum Data Set be used as a marker of organ dysfunction? - a pilot
study. BMC Res Notes 2009;2:77.
9. The ARDS Network investigators. Ventilation with lower tidal volumes as
compared with traditional tidal volumes for acute lung injury and the acute respiratory
distress syndrome. The Acute Respiratory Distress Syndrome Network. New Engl J Med
2000;342:1301-8.
10. Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure
Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group
on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive
Care Med 1996;22:707-10.
Page 15 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 15 -
11. Harvey S, Harrison DA, Singer M, et al. Assessment of the clinical effectiveness of
pulmonary artery catheters in management of patients in intensive care (PAC-Man): a
randomised controlled trial. Lancet 2005;366:472-7.
12. The National Heart, Lung, and Blood Institute ARDS Clinical Trials Network,
Truwit JD, et al. Rosuvastatin for sepsis-associated Acute Respiratory Distress Syndrome.
N Engl J Med 2014;370:2191-200.
13. Al Harbi SA, Tamim HM, Arabi YM. Association between statin therapy and
outcomes in critically ill patients: a nested cohort study. BMC Clin Pharmacol 2011;11:12.
14. Shah AI, Sobnosky S, Shen AY, Jorgensen MB. High dose statins are associated
with a reduced all cause mortality in patients hospitalized with sepsis and severe sepsis.
Crit Care Med 2009;36:pA15.
15. Drage SM, Simpkin AL, Neuvonen PJ, Watkinson PJ, Barber VS, Young JD.
Plasma simvastatin concentrations in critically ill septic patients. J Intensive Care Soc
2009;10:61.
16. Chiarla C, Giovannini I, Giuliante F, et al. Severe hypocholesterolemia in surgical
patients, sepsis, and critical illness. J Crit Care 2010;25:361.e7-12.
17. Calfee CS, Delucchi K, Parsons PE, et al. Subphenotypes in acute respiratory
distress syndrome: latent class analysis of data from two randomised controlled trials.
Lancet Respir Med 2014;2:611-20.
18. Jaswal DS, Leung JM, Sun J, et al. Tidal volume and plateau pressure use for Acute
Lung Injury from 2000 to present: A systematic literature review. Crit Care Med 2014 (in
press).
19. Papazian L, Roch A, Charles PE, et al. Effect of statin therapy on mortality in
patients with ventilator-associated pneumonia: a randomized clinical trial. JAMA
2013;310:1692-700.
Page 16 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 16 -
Table 1. Baseline characteristics of the patients.*
Simvastatin
(N = 259)
Placebo
(N = 280)
Age - yr 53.2 ±16.1 54.4 ± 16.7
Male sex – no. (%) 137 (52.9) 170 (60.7)
Sepsis – no. (%) 189 (73.0) 218 (77.9)
Etiology of ARDS#
Smoke/toxin inhalation 1 (0.3) 2 (0.5)
Gastric content aspiration 21 (6.0) 29 (7.7)
Thoracic trauma 22 (6.3) 10 (2.7)
Pneumonia 161 (46.0) 154 (41.1)
Sepsis 106 (30.3) 118 (31.5)
Pancreatitis 5 (1.4) 17 (4.5)
Non-thoracic trauma 4 (1.1) 8 (2.1)
Other 30 (8.6) 37 (9.9)
APACHE II score† 19.4±6.9 18.3± 6.2
SOFA score‡ 8.5±3.2 8.8±2.9
Vasopressor dependent – no. (%) 169 (65.2) 187 (66.8)
Lowest mean arterial pressure -
mmHg
65.4±9.3 64.9± 8.4
Inspiratory plateau pressure – cm of
water
23.6± 6.07 23.6± 6.03
Tidal Volume - ml/kg of predicted 8.1± 2.8 8.1± 2.6
Page 17 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 17 -
body weight§
PaO2/FiO2 ratio¶ - mm Hg 123.0±54.8 132.4±55.4
Oxygenation index - cm of
water/mm Hg
15.0±11.6 14.9±11.9
Alanine aminotransferase - U/liter 45.5±47.1 45.8±43.2
Aspartate aminotransferase - U/liter 59.9±49.4 65.3±63.9
Creatine kinase - U/liter 327.2±499.3 298.3±487.7
* Plus–minus values are means ±SD. There was no significant difference between groups
except PaO2/FIO2.
ARDS denotes acute respiratory distress syndrome, FiO2 fraction of inspired oxygen, and
PaO2 partial pressure of arterial oxygen (mmHg).
# Patients can have more than one cause for ARDS identified.
† Scores on the Acute Physiology and Chronic Health Evaluation (APACHE) II scale range
from 0 to 71, with higher scores indicating more severe disease.
‡ Scores on the Serial Organ Failure Assessment scale range from 0 to 24, with higher
scores indicating more severe disease.
§ Predicted body weight was calculated as 2.3 kg for each inch of height above 60 in. added
to 50 kg for men or 45.5 kg for women.
¶ P=0.049
Page 18 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 18 -
Table 2. Main Clinical Outcome variables.*
Simvastatin
Placebo
Difference or
Risk Ratio
(95% CI)
p-value
Ventilator-free days
to 28 days post
randomization¶
n 258 279
12.6±9.9
(11.3 to 13.8)
11.5±10.4
(10.2 to 12.7)
1.1 (-0.6 to 2.8)‡
1.1 (-0.7 to 2.8)‡
0.21
0.22†
Non pulmonary organ
failure-free days to 28
days post
randomization #
n 257 279
19.4±11.1
(18.0 to 20.8)
17.8±11.7
(16.4 to 19.2)
1.6 (-0.4 to 3.5)‡
1.6 (-0.3 to 3.5)‡
0.11
0.10†
All-cause mortality 28 days post
randomization – no./total no. (%)
and 95% CI
57/259 (22.0)
(17.0 to 27.1)
75/280 (26.8)
(21.6 to 32.0)
0.8 (0.6 to 1.1)§ 0.23
Death before discharge from
critical care – no./total no. (%)
and 95% CI
56/259 (21.6)
(16.6 to 26.6)
70/280 (25.0)
(19.9 to 30.1)
0.9 (0.6 to 1.2)§ 0.36
Death before discharge from
hospital – no./total no. (%)
and 95% CI
67/259 (25.9)
(20.5 to 31.2)
90/280 (32.1)
(26.7 to 37.6)
0.8 (0.6 to 1.1)§ 0.13
* Plus–minus values are means ±SD with 95% CI. CI denotes confidence interval.
‡ Difference and 95% CI.
Page 19 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 19 -
¶ Ventilator-free days are defined in the study protocol. Patients who died before day 28
were assigned zero ventilator free days.
† The results from the bootstrapped t-test also presented.
# Non pulmonary organ failure-free days are defined in the study protocol. Patients who
died before day 28 were assigned zero non pulmonary organ failure-free days. Organs were
considered failure-free after patients were discharged from the critical care unit.
§ Risk Ratio and 95% CI.
Page 20 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
- 20 -
Figure legends
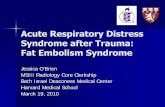
Figure 1. Screening, randomization, and follow-up of the study participants.
There may have been more than one reason for exclusion of a patient. ARDS denotes Acute
Respiratory Distress Syndrome and CK creatine kinase.
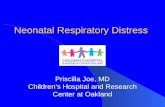
Figure 2. Probability of survival and breathing without assistance from randomization to
day 28 according to whether patients received simvastatin or placebo. Alive, Simvastatin
denoted in black, Alive, Placebo in red, Unassisted breathing, Simvastatin in blue and
Unassisted breathing, Placebo in green. The numbers of patients at risk in each group are
indicated in the corresponding colour.
Page 21 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
Figure 1.
5926 were assessed for eligibility
258 were included in the analysis of the primary outcome
1 patient was lost to follow-‐up
1 patient was lost to follow-‐up (day 9)
259 were allocated to simvastatin 254 received simvastatin 5 did not receive simvastatin
2 were on a statin 1 had elevated transaminases 2 unable to insert nasogastric tube
0 patients were lost to follow-‐up
281 were allocated to placebo 278 received placebo 3 did not receive placebo
1 had elevated CK 1 consent was withdrawn 1 other reason
279 were included in the analysis of the primary outcome
2 withdrawal of consent
540 were randomized
5386 were excluded
9 were <16 years of age 312 were not intubated/ventilated 719 were more than 48 hours from onset of ARDS 15 were known to be pregnant 194 had elevated CK 342 had elevated transaminases 340 had interaction with concomitant drug 235 had severe renal impairment and were not receiving renal replacement therapy 223 had severe liver disease (Child-‐Pugh score > 12) 1803 had received statins within the previous two weeks 75 required a statin for a proven indication 117 had a contraindication to enteral drug administration 103 were enrolled in another drug trial 309 treatment withdrawal imminent 197 declined to consent 836 had other reason
Page 22 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review
Number at risk
Survival
Simvastatin 259 238 217 208 202
Placebo 280 250 231 220 205
Unassisted breathing
Simvastatin 258 166 87 43 19
Placebo 279 178 102 60 33
Page 23 of 22
Confidential: Destroy when review is complete.
Submitted to the New England Journal of Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960