
Setting up an early warning system for epidemic-prone diseases in Darfur: a participative approach
13
Setting up an early warning system for epidemic-prone diseases in Darfur: a participative approach Augusto Pinto, Mubarak Saeed, Hammam El Sakka, Adrienne Rashford, Alessandro Colombo, Marta Valenciano, Guido Sabatinelli 1 In April–May 2004, the World Health Organization (WHO) implemented, with local authorities, United Nations (UN) agencies and non-governmental organisations (NGOs), an early warning system (EWS) in Darfur,West Sudan, for internally displaced persons (IDPs).The number of consultations and deaths per week for 12 health events is recorded for two age groups (less than five years and five years and above).Thresholds are used to detect potential outbreaks.Ten weeks after the introduction of the system, NGOs were covering 54 camps, and 924,281 people (IDPs and the host population). Of these 54 camps, 41 (76%) were reporting regularly under the EWS. Between 22 May and 30 July, 179,795 consultations were reported: 18.7% for acute respiratory infections; 15% for malaria; 8.4% for bloody diarrhoea; and 1% for severe acute malnutrition. The EWS is useful for detecting outbreaks and monitoring the number of consultations required to trigger actions, but not for estimating mortality. Keywords: alert, displaced population, emergency, humanitarian crisis, infectious diseases, surveillance. Background: Darfur humanitarian crisis The first rumours of attacks in Darfur by armed members of the Sudan Liberation Army/ Movement (SLA/M), the Sudan Justice and Equality Movement and the government of Sudan and their supporters were heard in February 2003. From February 2004, the security situation of the local population in the greater Darfur region (the states of North, South and West Darfur) deteriorated due to the intensification of attacks on the local populations by militias and rebels (WHO, 2004; UN, 2004). Consequently, the Darfur population, seeking more security, abandoned its villages and concentrated around the region’s main urban centres (Al Geneina, El Fasher and Nyala) or near villages (such as Mornay). Darfur had an estimated population of six million in 2004. Some 1.3 million people were affected by the civil war (UN HC/RC, 2004), including one million internally displaced persons (IDPs), 100,000 residents and 200,000 refugees who had crossed the Chad border (UNHCR, 2004) (Table 1). Although a ceasefire between the SLA/M, the Sudan Justice and Equality Move- ment and the government of Sudan was agreed in April 2004 (African Union, 2004), the United Nations (UN) and other humanitarian agencies still had only limited access to IDPs in May–June 2004 (Moszynski, 2004). Disasters, 2005, 29(4): 310 − 322. © Overseas Development Institute, 2005 Published by Blackwell Publishing, 9600 Garsington Road, Oxford, OX4 2DQ, UK and 350 Main Street, Malden, MA 02148, USA
-
Upload
augusto-pinto -
Category
Documents
-
view
215 -
download
2
Transcript of Setting up an early warning system for epidemic-prone diseases in Darfur: a participative approach

Setting up an early warning system for epidemic-prone diseases in Darfur 311
Setting up an early warning system for epidemic-prone diseases in Darfur: a participative approach
Augusto Pinto, Mubarak Saeed, Hammam El Sakka, Adrienne Rashford, Alessandro Colombo, Marta Valenciano, Guido Sabatinelli1
In April–May 2004, the World Health Organization (WHO) implemented, with local authorities, United Nations (UN) agencies and non-governmental organisations (NGOs), an early warning system (EWS) in Darfur, West Sudan, for internally displaced persons (IDPs). The number of consultations and deaths per week for 12 health events is recorded for two age groups (less than five years and five years and above). Thresholds are used to detect potential outbreaks. Ten weeks after the introduction of the system, NGOs were covering 54 camps, and 924,281 people (IDPs and the host population). Of these 54 camps, 41 (76%) were reporting regularly under the EWS. Between 22 May and 30 July, 179,795 consultations were reported: 18.7% for acute respiratory infections; 15% for malaria; 8.4% for bloody diarrhoea; and 1% for severe acute malnutrition. The EWS is useful for detecting outbreaks and monitoring the number of consultations required to trigger actions, but not for estimating mortality.
Keywords: alert, displaced population, emergency, humanitarian crisis, infectious diseases, surveillance.
Background: Darfur humanitarian crisisThe first rumours of attacks in Darfur by armed members of the Sudan Liberation Army/ Movement (SLA/M), the Sudan Justice and Equality Movement and the government of Sudan and their supporters were heard in February 2003. From February 2004, the security situation of the local population in the greater Darfur region (the states of North, South and West Darfur) deteriorated due to the intensification of attacks on the local populations by militias and rebels (WHO, 2004; UN, 2004). Consequently, the Darfur population, seeking more security, abandoned its villages and concentrated around the region’s main urban centres (Al Geneina, El Fasher and Nyala) or near villages (such as Mornay). Darfur had an estimated population of six million in 2004. Some 1.3 million people were affected by the civil war (UN HC/RC, 2004), including one million internally displaced persons (IDPs), 100,000 residents and 200,000 refugees who had crossed the Chad border (UNHCR, 2004) (Table 1). Although a ceasefire between the SLA/M, the Sudan Justice and Equality Move-ment and the government of Sudan was agreed in April 2004 (African Union, 2004), the United Nations (UN) and other humanitarian agencies still had only limited access to IDPs in May–June 2004 (Moszynski, 2004).
Disasters, 2005, 29(4): 310−322. © Overseas Development Institute, 2005Published by Blackwell Publishing, 9600 Garsington Road, Oxford, OX4 2DQ, UK and 350 Main Street, Malden, MA 02148, USA
Setting up an early warning system for epidemic-prone diseases in Darfur 311
According to the UN Resident and Humanitarian Coordinator (UN HC/RC) for the Sudan Office, at the end of May 2004, only 39% of the conflict-affected popula-tion in the greater Darfur region had access to food assistance, 15% to clean water, 4% to sanitation, 5% to shelter material and 15% to primary healthcare facilities (UN HC/RC, 2004). In the context of this humanitarian crisis, prompt detection of outbreaks of epidemic-prone diseases was a top priority. In May 2004, the World Health Organization (WHO) collaborated with the national health authorities, UN agencies and non-governmental organisations (NGOs) to set up an early warning system (EWS).
Population figures, distribution and accessibilityThe IDPs were not only concentrated in organised camps but also in areas close to villages or towns, or they were hosted by the local population. By June 2004, the UN World Food Programme (WFP) had registered 129 camps or settlement areas across the three states of the region, spanning a total surface area of 510,000 square kilometres (Figure 1). Communication in the region was difficult. Roads were not covered in asphalt, and they were poorly maintained. Furthermore, their condition deteriorated during the rainy season, starting in June. Telephones were only available in state capitals. Commu-nication with the camps was only possible using international humanitarian agencies’ satellite telephones and radios. Due to the lack of security, humanitarian access to IDPs was restricted and the presence of international workers in the field was limited (WHO-Sudan, 2004).
Health conditions of IDPs in May 2004Sudan has poor health indicators, such as a life expectancy at birth level of 59 years and a child mortality rate of 93 per 1,000 live births in 2003. In addition, there was a loss of 16% in total life expectancy due to poor health in 2002 (WHO, 2005). Therefore, the public health situation in Darfur, as in the rest of the country, was already severe before the crisis, with hospitals and primary healthcare units in bad condition, a limited supply of drugs and a shortage of health personnel. In May 2004, the food security situation in Darfur became precarious in spite of the efforts of WFP and its implementing partners (UN HC/RC, 2004). In Mukjar, West
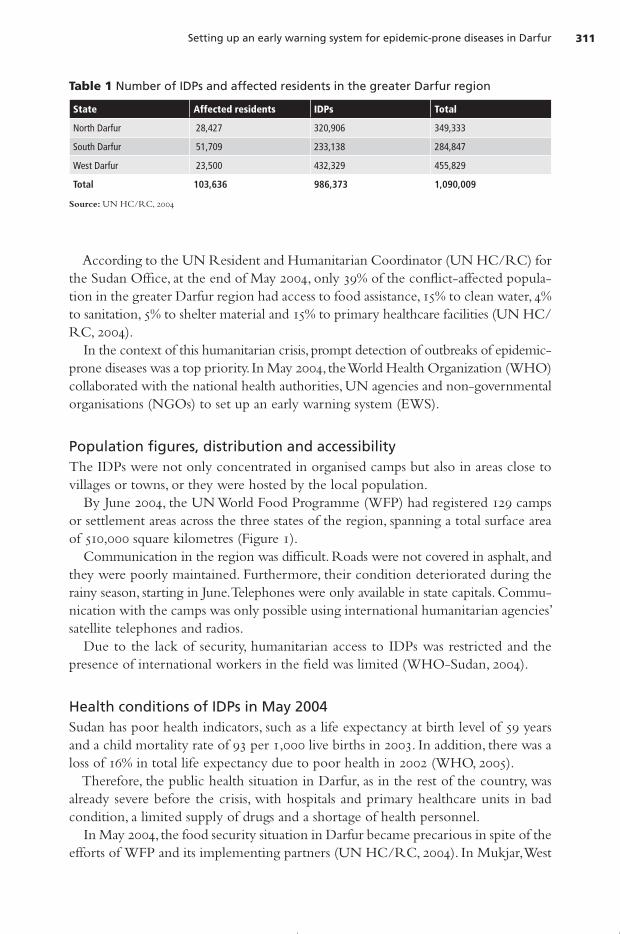
Table 1 Number of IDPs and affected residents in the greater Darfur region
State Affected residents IDPs Total
North Darfur 28,427 320,906 349,333
South Darfur 51,709 233,138 284,847
West Darfur 23,500 432,329 455,829
Total 103,636 986,373 1,090,009
Source: UN HC/RC, 2004

Augusto Pinto et al.312 Setting up an early warning system for epidemic-prone diseases in Darfur 313
Darfur, the results of a nutritional survey carried out by Médecins Sans Frontières showed that among 900 children included in the study, 20% were malnourished and 3% were suffering from severe acute malnutrition. The most common reported health events in the region were acute respiratory infec-tions, diarrhoea, malaria, measles and war injuries (Brown, 2004). The crude mortality rate (CMR) in West Darfur was greater than the internationally accepted benchmark of one death per 10,000 per day, indicating an emergency: 2.3 (Confidence Interval (CI) 1.4–3.7) in Zalingei, 3.4 (CI 2.6–4.6) in Murnei, 1.5 (CI 1.2–1.9) in Niertiti and 5.6 (CI 4.1–7.6) in El Geneina (Depoortere et al., 2004). In 12 camps in or around the town of El Geneina in June 2004, the major causes of deaths reported in children under five were acute diarrhoea, fever and cough. Violence accounted for 9.6% of all deaths among IDPs (Checchi, 2004).
Surveillance of communicable diseases in SudanThe national communicable disease surveillance system was reorganised in 2003. It includes 22 health events that should be reported for two age groups (less than five years and five years and above) by sentinel sites. According to the Federal Ministry of Health (FMOH)’s plan of action, Darfur was not included in the first phase of imple-mentation of the new system (due to the limited implementation capacities of the FMOH), but should be included later. National guidelines with case definitions have been published in Arabic and distri-buted to the sentinel sites.
Figure 1 Distribution of IDP camps in the greater Darfur region, June 2004
Source: WHO, Khartoum Office, 2004

Augusto Pinto et al.312 Setting up an early warning system for epidemic-prone diseases in Darfur 313
The laboratory network is based on the National Public Health Laboratory (NPHL) in Khartoum, which is the reference laboratory for the whole country.
MethodsHealth status assessments indicated that the IDPs in Darfur were living in an environ-ment with poor sanitation and a restricted supply of water. Moreover, food insecurity, overcrowding, prevalent malnutrition and limited access to healthcare were factors that could facilitate outbreaks. Thus, in such an emergency, one of the top priorities was to strengthen the early warning function of the national surveillance system to detect immediately outbreaks and to trigger a prompt response to preserve the health of the displaced and local population. Other priorities were food distribution, sanitation, water supply, shelter and security for the IDPs. In order to strengthen surveillance in the region without creating a parallel system, the EWS had to be coherent, corresponding with the principles of the national surveill-ance system. It had to be an adaptation of the latter, in terms of objectives, reporting sites, timeliness and sensitivity. Because the IDPs were scattered, integrated into the local population, with poor accessibility, the system had to be decentralised to allow detection and action to be taken. This meant strengthening the peripheral level and making tools available to national health staff and humanitarian agencies working directly with the IDPs. Data had to be standardised and activities coordinated, and all actors had to accept and participate in the system. To ensure acceptability of the EWS, a working group was set up to develop a proto-col, involving all national (FMOH) and international agencies. The protocol had to be a reference document for all partners aiming to homogenise procedures. It included practical guidelines on training of all personnel involved in the EWS. The working group agreed that the attributes that had to guide the design of the EWS were ability to detect all potential outbreaks, timeliness, to permit a prompt response, and flexibility to adapt to any new threat that could appear in this unstable environment. Moreover, the system had to be simple, given the dearth of trained health personnel and the difficulty of ensuring proper supervision due to poor accessibility. To guarantee the support of all stakeholders, the protocol was discussed in each of the three states of Darfur with the local health authorities and NGOs working in the field. Several donors supporting the WHO response to the humanitarian crisis funded the EWS.
Description of the EWS protocolThe objectives of the EWS were:
• to ensure early detection of outbreaks among the affected population in the greater Darfur region, a timely response and control of outbreaks;

Augusto Pinto et al.314 Setting up an early warning system for epidemic-prone diseases in Darfur 315
• to monitor communicable disease trends in order to take appropriate public health action; and
• to estimate the workload of health units attending to the affected population, to improve resource allocation.
The population under surveillance was defined as all IDPs settled in established or informal camps or IDPs hosted by the resident population. In the areas where IDPs were integrated into the resident population, residents were using the same health services and were included in the EWS target population. The population figures used were the estimates of the United Nations Office for the Coordination of Humanitarian Affairs (OCHA). For feasibility reasons, only camps with an NGO presence (n=54)—among the 129 registered camps—were included in the first phase of the EWS. Of the 22 health events reported by the national surveillance system, 12 were selected for inclusion in the EWS because of their potential risk to the IDPs (Table 2). Simple syndromic case definitions were established for the selected health events. Each case definition was compared to the corresponding one in the national surveil-lance system to ensure coherence and to facilitate its use by medical staff on the front line. Data were reported for the same age groups employed in the national surveillance system: under five and five years and above. The reporting units were all health centres in the camps or in the areas with IDPs included in the EWS. These units had to report, on a weekly basis, and using a standard surveillance form, all new cases and deaths to the state epidemiology unit. Staff involved in data collection, reporting and analysis at the state level were trained in how to use the EWS protocol. Data were transmitted using satellite e-mail systems, which were available in most of the camps, or, in some instances, by hand. As for the national surveillance system, the state epidemiology unit had to transmit the data to the federal level using a satellite e-mail connection, with the support of the local WHO Office (Figure 2). To increase the sensitivity and the timeliness of the EWS, a rumour verification process was set up, with community leaders in the camps acting as key informants. If an unusual health event occurred or an outbreak was suspected, community leaders
Table 2 Health events included in the EWS
Acute flaccid paralysis Malaria
Acute jaundice syndrome Neonatal tetanus
Acute respiratory infection Severe malnutrition
Acute watery diarrhoea Suspected measles
Bloody diarrhoea Suspected meningitis
Injuries Unexplained fever

Augusto Pinto et al.314 Setting up an early warning system for epidemic-prone diseases in Darfur 315
Figure 2 Data and specimen flow in the EWS
had to inform immediately the medical assistant in the area who would verify the information and take action when needed. To detect alerts at the peripheral and central level, simple thresholds based on the total number of cases per camp and per week were defined (such as one case of sus-pected measles and one case of acute flaccid paralysis). Incidence and mortality rates were computed. A simple computer application based on free-share software, EPIINFO 6.04 and EpiData 3.2, was developed for data entry, data analysis and automatic production of standard reports at the state and federal level. A user manual was distributed to all personnel using the computer application. The application generated the following indicators every week:
• number of new cases and deaths for each health event per week;• total number of consultations;

Augusto Pinto et al.316 Setting up an early warning system for epidemic-prone diseases in Darfur 317
• incidence of health events per week and by geographical level;• under five mortality rate per 10,000 members of the population per week;• CMR per 10,000 members of the population per week;• case fatality ratio;• proportional morbidity by age group; • number of new cases by age and geographical level;• number of deaths by age and geographical level; • number of health facilities reporting/number of health facilities expected to report;• timeliness of data transmission from camps to the state; and• timeliness of data transmission from the state to the federal level.
The results were presented to all partners during the weekly health coordination meeting organised by the FMOH and WHO in Khartoum. A weekly epidemiological bulletin was distributed at the central and peripheral level via e-mail and discussed every week in the health coordination meeting at the state level. Laboratory specimens collected in the greater Darfur region, within the framework of EWS activities, were transported to Khartoum. Standard operating procedures were included in the EWS protocol to ensure quality, prompt diagnosis and an immediate response. Media for specimen collection were positioned at the state level and in camps with poor accessibility. A private carrier ensured the transport of the media from the Darfur region to Khartoum in 24 hours. The NPHL in Khartoum was supplied with reagents and tests for antibiotic sensi-tivity. A plan of action was developed to improve the diagnostic capacities of the field laboratories in the state capitals in the medium and long term. Resources were identified in each state to ensure prompt investigation if outbreaks were detected. Outbreak control teams, including epidemiologists from the Ministry of Health (MOH) at the state level and WHO personnel, were created. Officers with the polio eradication programme participated in the EWS and supported the system via the polio logistic network, especially with regard to outbreak control.
ResultsThe EWS officially started on week 21 (22 May 2004). Among the 54 reporting units included in the first phase of the EWS, the participation rate increased steadily from week 21 to week 30 (Figure 3). Between 22 May and 30 July, the reporting units participating in the EWS reported 179,795 consultations: 18.7% for acute respiratory infections; 15% for malaria; 8.4% for bloody diarrhoea; and 1% for severe malnutrition (Table 3). More than 1,000 cases of acute watery diarrhoea were reported; cholera was excluded after field visits to the reporting camps. With respect to the 868 deaths reported, the three main causes were severe malnu-trition, measles and bloody diarrhoea, accounting for 101 (11.6%), 34 (4%) and 26 (3%) fatalities, respectively.

Augusto Pinto et al.316 Setting up an early warning system for epidemic-prone diseases in Darfur 317
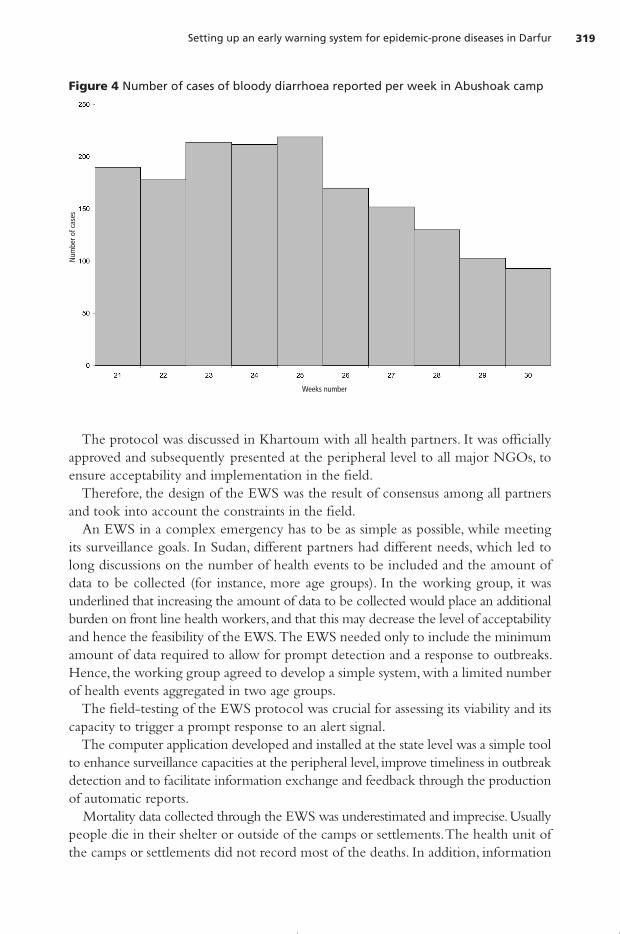
These figures only reflect the deaths reported by the heath centres in the partici-pating camps. Deaths at the community or hospital level are not included in the EWS. Due to the rise in the number of reported cases of acute bloody diarrhoea, two outbreaks of Shigella dysenteriae were detected in West and North Darfur. These were confirmed in weeks 24 and 26, respectively. Figure 4 shows the number of cases of acute bloody diarrhoea reported by the only health centre functioning in the camp of Abushok in North Darfur, on the periphery of the town of El Fasher. Seven specimens were sent for confirmation to the NPHL in Khartoum on 30 June; three tested positive for Shigella dysenteriae 1. No specimens were sent abroad to ensure quality control. The increase in the number of cases of acute jaundice reported in Morni camp, West Darfur, led to an outbreak of Hepatitis E being detected in week 29 (Figure 5). Specimens were sent to the Naval Medical Research Unit 3 (NAMRU 3) laboratory in Cairo, Egypt. Confirmation was obtained using Polymerase Chain Reaction (PCR). In response to these outbreaks, humanitarian agencies, NGOs and the MOH re-inforced water and sanitation programmes by enhancing the quantity and quality of water supplied and by building more latrines. Given the type of pathogens implied in the two outbreaks, Shigella dysenteriae and Hepatitis E, children and pregnant women were most at risk of mortality. Therefore, programmes to reduce morbidity and mor-tality among these groups were launched. Health promotion programmes included training in the use of latrines, personal hygiene and soap distribution.
DiscussionIn May 2004, a major intervention was required to limit the human catastrophe facing IDPs in the greater Darfur region. In such a complex emergency setting, the occurrence
Figure 3 Number of reporting units per week (weeks 21–30)
Weeks number
Num
ber o
f rep
ortin
g un
its

Augusto Pinto et al.318 Setting up an early warning system for epidemic-prone diseases in Darfur 319
of an outbreak could have a devastating impact on the already vulnerable population. To improve early detection and the response to outbreaks, therefore, the establishment of an EWS becomes one of the 10 key priorities (Médecins Sans Frontières, 1997) to be settled in the first phase of an emergency. The EWS in Darfur allowed for standardisation of data collection, information dis-semination and identification of intervention priorities. Partners had information on all accessible camps covered by the system in the whole region, not only in the geogra-phical area where a particular organisation was carrying out its activities. In such a complex emergency, with various national and international partners not always sharing the same priorities, building a system that could be accepted, supported and adopted by all actors and stakeholders was a challenge. The objectives of the system had to satisfy the needs of all partners and had to be based on consensus. The EWS is an adaptation of the national surveillance system, responding to the plight of the IDPs, and not a parallel system. This may have contributed to the participation of the FMOH, the Darfur states and national health staff. The designation of the NPHL in Khartoum as the reference laboratory, to confirm suspected outbreaks, helped to make the EWS acceptable to the national health authori-ties. Moreover, the direct involvement of the NPHL in the EWS offered an opportunity to strengthen its technical and diagnostic capacities. The participation of humanitarian agencies and NGOs in the preparatory phase was essential in defining a system that responded to the needs of each partner. The develop-ment of the protocol required a phase of open discussion and mediation in order to reach agreement on, and a common understanding of, the aims of the system.
Table 3 Number of cases of 12 reported health events, weeks 21–30
21 22 23 24 25 26 27 28 29 30 Total
Diarrhoea 0 0 0 66 73 211 217 453 165 50 1,235
Bloody diarrhoea 757 783 1,025 1,284 1,762 1,519 1,232 1,618 1,968 3,126 15,074
Measles 42 22 114 146 111 111 67 24 12 30 679
Meningitis 3 1 2 3 0 2 2 0 1 1 15
Malaria 1,167 1,872 1,302 1,600 1,585 2,251 2,942 3,534 4,141 6,528 26,922
Acute Flaccid Paralysis 0 0 0 0 0 0 0 0 3 0 3
Acute jaundice 5 2 2 7 15 63 33 76 222 330 755
Acute Respiratory Infections
1,701 1,572 3,169 3,472 2,603 3,109 3,741 4,358 4,890 5,008 33,623
Neonatal Tetanus 0 0 0 0 0 0 0 0 1 4 5
Unexplained fever 5 0 407 657 596 641 232 212 503 440 3,693
Malnutrition 54 62 78 145 131 235 186 404 355 240 1,890
Injuries 70 54 140 246 205 507 431 586 743 1,242 4,224
Other 4,222 2,927 7,472 7,392 8,287 1,0821 9,546 10,692 13,051 17,267 91,677
Augusto Pinto et al.318 Setting up an early warning system for epidemic-prone diseases in Darfur 319
The protocol was discussed in Khartoum with all health partners. It was officially approved and subsequently presented at the peripheral level to all major NGOs, to ensure acceptability and implementation in the field. Therefore, the design of the EWS was the result of consensus among all partners and took into account the constraints in the field. An EWS in a complex emergency has to be as simple as possible, while meeting its surveillance goals. In Sudan, different partners had different needs, which led to long discussions on the number of health events to be included and the amount of data to be collected (for instance, more age groups). In the working group, it was underlined that increasing the amount of data to be collected would place an additional burden on front line health workers, and that this may decrease the level of acceptability and hence the feasibility of the EWS. The EWS needed only to include the minimum amount of data required to allow for prompt detection and a response to outbreaks. Hence, the working group agreed to develop a simple system, with a limited number of health events aggregated in two age groups. The field-testing of the EWS protocol was crucial for assessing its viability and its capacity to trigger a prompt response to an alert signal. The computer application developed and installed at the state level was a simple tool to enhance surveillance capacities at the peripheral level, improve timeliness in outbreak detection and to facilitate information exchange and feedback through the production of automatic reports. Mortality data collected through the EWS was underestimated and imprecise. Usually people die in their shelter or outside of the camps or settlements. The health unit of the camps or settlements did not record most of the deaths. In addition, information
Figure 4 Number of cases of bloody diarrhoea reported per week in Abushoak camp
Weeks number
Num
ber o
f cas
es

Augusto Pinto et al.320 Setting up an early warning system for epidemic-prone diseases in Darfur 321
on the population of the camps was not accurate, affecting computation of mortality rates at the camp and state level. An active mortality surveillance system should be developed to record deaths. However, this can present some problems, due to costs and the difficulty in estimating reliable mor-tality rates when the population of the camps is not stable, as in many camps in Darfur. The representativeness of the system was limited because of lack of accessibility to some areas. Improving accessibility should be a priority in order to provide primary healthcare services to IDPs and to include data from all camps in the EWS.
ConclusionAs stressed in relation to previous complex emergencies, such as those in Albania and Iraq (Valenciano et al., 1999; Valenciano et al., 2003), close collaboration between inter-national humanitarian agencies and national staff and authorities is critical for setting up and implementing an acceptable and efficient early warning system to monitor, detect and respond to eventual outbreaks. Three principles have to be taken into account:
• national health authorities should be involved from the start of the process;• all international partners engaged as healthcare providers should participate; and• the EWS has to be integrated to as great a degree as possible into national public
health programmes.
In Darfur, the EWS detected outbreaks and monitored the number of consultations required to trigger action. The completeness of the system improved progressively with the weekly enrolment of new IDPs camps.
Figure 5 Number of cases of acute jaundice reported per week in Morni, weeks 21–30
Weeks number
Num
ber o
f cas
es

Augusto Pinto et al.320 Setting up an early warning system for epidemic-prone diseases in Darfur 321
However, mortality data collected through the EWS was unreliable. The CMR is a key indicator of an emergency in a humanitarian crisis setting, but other mortality pointers should be considered, such as periodical retrospective mortality surveys, grave counting and daily interviews with families through community health workers (as conducted by some NGOs in Darfur). Denominators need to be defined as early as possible in each camp or settlement to produce reliable incidence rates. Security is the crucial aspect in the Darfur humanitarian crisis: ensuring the security of the IDP population, the resident population affected by the crisis and the humani-tarian agencies is essential if one is to gain access to the whole population. Furthermore, this is fundamental for developing an effective early warning and response system that contributes to better health in Darfur. The EWS should be evaluated after the first phase of implementation, usually six to 12 months later, in order to identify its weaknesses and the changes that need to be made to improve the system. Moreover, this evaluation would help with documenting the process and highlighting the lessons learned in Darfur, which can be used to im-prove communicable disease surveillance in other complex emergency contexts.
CorrespondenceAugusto Pinto, World Health Organization, 58 Avenue debourg, 69007, Lyon, France. Telephone: +33 472 72 64 73; fax: +33 472 64 71; e-mail: [email protected].
Endnotes1 Augusto Pinto and Marta Valenciano represent the World Health Organization (WHO), Communicable
Diseases Surveillance and Response Department, Epidemiological Surveillance Strengthening Team, Lyon, France; Mubarak Saeed represents the National Public Health Laboratory, Khartoum, Sudan; Hammam El Sakka, Adrienne Rashford and Guido Sabatinelli represent the WHO, Khartoum Office, Sudan; and Alessandro Colombo represents the WHO, Health Action in Crises, Geneva, Switzerland.
ReferencesAfrican Union (2004). Press Release. 51/2004. http://www.africaunion.org/News_Events/Press_Releases/
51%2004Sudanese%20parties%20sign%20agreement.pdf. Brown, V. (2004) Epidemiological surveillance, MSF-F emergency, West Darfur, Sudan. Draft report. Epicentre,
Paris. Checchi, F. (2004) A survey of internally displaced persons in El Geneina, Western Darfur. Epicentre/Médecins
Sans Frontières, Paris.Depoortere, E. et al. (2004) ‘Violence and mortality in West Darfur, Sudan (2003–04): epidemiological
evidence from four surveys’. Lancet. 364. pp. 1315–1320.Médecins Sans Frontières (1997) Refugee Health, an approach to emergency situations. Médecins Sans Fron-
tières, MacMillan Education LTD.P, Paris.

Augusto Pinto et al.322
Moszynski, P. (2004) ‘Officials warn of looming humanitarian crisis in Sudan’. British Medical Journal. 328. p. 424.
UN (2004) ‘High level Mission to Darfur, the Sudan, 27 April–2 May 2004’. Mission Report. http://www. unsudanig.org/emergencies/darfur/reports/data/missions/HighLevelMissionReport.pdf.
UNHCR (United Nations High Commissioner for Refugees) (2004) ‘Chad: new arrivals reported from Sudan; the burden on Chad’. UNHCR Briefing Notes. Press Briefing, 17 April 2004, Palais des Nations, Geneva.
UN HC/RC (UN Resident and Humanitarian Coordinator for the Sudan) (2004) Darfur Humanitarian Profile. 2. UN, Khartoum.
Valenciano, M. et al. (1999) ‘Surveillance of communicable diseases among the Kosovar refugees in Abania, April–June 1999’. Eursurveillance. 4(4). pp. 92–95.
Valenciano, M. et al. ( 2003) ‘Challenges for communicable disease surveillance and control in Southern Iraq, April–May 2003’. The Journal of the American Medical Association (JAMA). 290. pp. 654–658.
WHO (World Health Organization) (2004). ‘UN Situation Reports’. 18 and 20. April. http://www.unsudanig. org/emergencies/darfur/sitreps/index.jsp.
WHO (2005) ‘Statistical Information System. Country: Sudan’. http://www3.who.int/whosis/country/indicators.cfm?country=sdn.
WHO-Sudan (2004) ‘Darfur Crisis’. Progress Report. 8.


















