Sepsis - Continuous Learning, Education &...
46
Sepsis ! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015
Transcript of Sepsis - Continuous Learning, Education &...

Sepsis !
Dr Eric Van Den Bergh
Consultant in Emergency Medicine
2015



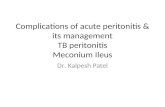
0 10000 20000 30000 40000
Lung cancer
COPD
Heart attack
Stroke
Sepsis
Lung cancer
COPD
Heart attack
Stroke
Sepsis
Annual UK Mortality

Severe Sepsis/Septic Shock
Audit
E. Van Den Bergh
C.Smith
01/2015 -7/2015
Sepsis 6
1. Give high-flow oxygen via non-rebreather bag
2. Take blood cultures and consider source control
3. Give IV antibiotics according to local protocol
4. Start IV fluid resuscitation Hartmann’s or equivalent
5. Check lactate
6. Monitor hourly urine output consider catheterisation
within one hour
…plus Critical Care support to complete EGDT

Inclusion criteria (Severe Sepsis)
Suspicion of Severe Infection AND Any TWO of the following:
Temperature > 38o
or < 36oC
Respiratory Rate > 20/min
Heart Rate > 90/min
WCC < 4000 or > 12000
AND ONE of the following:
Systolic Blood Pressure < 90mm Hg
Serum lactate > 4mmols/l
Severe Sepsis & Septic Shock Pathway
Ref Sepsis Six =
PATIENT NAME:
DATE OF BIRTH: AFFIX LABEL
CC NUMBER:
1. Take Blood Cultures
2. Give IV antibiotics
3. Start IV fluid resuscitation
4. Give high flow oxygen
5. Check haemoglobin and lactate
6. Monitor accurate hourly urine output
FIRST 60 MINUTES Pathway Commenced on _/ / (Date) at :
Investigate:
INSTITUTE THE ‘SEPSIS SIX’ * Tick Time
Blood culture, FBC, U&Es, Coag. Screen, LFTs, Lactate, ABGs/ VBG Urinanalysis and micro/C&S Chest x-ray
Give:
IV antibiotics - refer to Hospital Guidelines
20-30ml/Kg Crystalloid or Colloid over 30minutes (Caution: Monitor for fluid overload)
Oxygen and consider need for IPPV
Monitor :
Urine output hourly [ consider urine catheter ]
Oxygen saturation and non-invasive blood pressure every 15 minutes
ECG continously
MEWS Scores
Discuss with Senior Doctor on Duty Refer Critical care outreach (VOIP 2314) and Refer to the appropriate Speciality Team
:
:
:
:
:
:
:
__-------:-------
:
:
:
Initial assessment completed by (PRINT) (Signed) at : _(Time)
Severe Sepsis Pathway V2 April 2015
(Page Over)
Risk factors, Signs or symptoms of infection
Red-Flags in ambulance handover
Immunocompromised
Indwelling medical devices
Recent surgery/invasive procedure
Recent Rigors/fever
Chest: Cough/SOB
Urine: dysuria, frequency, odour
Skin: cellulitis
Abdomen: pain, peritonitis
Neuro: Headache, Meningism, confusion

Desired Outcomes
• Promote early recognition of community acquired sepsis.
• Ensure sepsis is graded and the sickest patients are identified early.
• Ensure a basic set of treatments are performed in a timely manner
• Get antibiotic stewardship right.
• Improve coding of sepsis, severe sepsis and septic shock

Method
• 30 consecutive patient records coded as having severe sepsis, commencing 01/01/15
• Paper notes, PDOC, nursing notes and lab results examined for evidence of meeting audit criteria

29
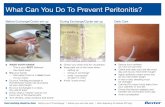
24
27
23
17
6
29 29
27
24
15
1
3
5
8
0
5
10
15
20
25
30
35
High flow O2initiated
Serum lactatemeasurement
Blood cultures First intravenouscrystalloid fluid
bolus
Antibiotics Urine outputmeasured
2015 Time from arrival or triage to:
<1 hour <2 hours >2 hours
Results

Results
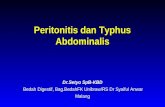
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
Within 1Hour
Within 2Hours
> 2 hours NotRecorded
Within 1Hour
Within 2Hours
> 2 hours NotRecorded
2015 2014
IV antibiotics given

Results
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
Within 1Hour
Within 2Hours
> 2 hours NotRecorded
Within 1Hour
Within 2Hours
> 2 hours NotRecorded
2015 2014
IV crystalloid given

What is sepsis?

Burns
Burns
Infection Sepsis Severe Sepsis
Septic shock
SIRS Organ dysfunction Hypoperfusion

Burns
Burns
Infection Sepsis Severe Sepsis
Septic shock
SIRS Organ dysfunction Hypoperfusion
<1% 10% 35% 50%
50% 50%

Where did we start ?

“Early goal-directed therapy in the treatment of severe sepsis and septic
shock”
Rivers et al.
New England Journal of Medicine [N Engl J Med 2001;345:1368-77]

Getting the basics right






We need Red Flags!


UK Sepsis Trust Clinical Toolkits 2014- Produced in association with NHS England
Modified from Surviving Sepsis Campaign’s
‘Evaluation for Severe Sepsis Screening Tool’ 2005





Simple Strategy
• Concentrate on the front end
• Concentrate on getting the simple stuff right
• More recent papers tell us this was probably the right approach
Suspect
Screen
Sepsis Six

Is any red flag present?
Systolic B.P < 90 mmHg or MAP < 65 mmHg Lactate > 2 mmol/l Heart rate > 130 per minute Respiratory rate > 25 per minute Oxygen saturations < 91% Responds only to voice or pain/ unresponsive Purpuric rash

Time for Action

Achieving reliable sepsis care


Successes
• Established motivated core team
• Simple message that is accessible to everyone
• Linking to other work


Challenges
• The enormity of the problem
– patients to treat
– people to train
• Keeping everyone involved and enthused

Antibiotics
Although a global restriction of antibiotics is an important strategy to reduce the development of antimicrobial resistance and to reduce cost, it is not an appropriate strategy in the initial therapy for this patient population”

Definitions change – SIRS is dead!
• Definitions to change from sepsis/severe sepsis and septic shock to sepsis/septic shock
• SIRS no longer to be utilised as access point to screening tool.
• Likely to be NEWS score of 5 or more, or individual parameter scoring 3.
• To be used in Red Flag assessment – Syst <100mmHG, RR>25, GCS <14.
• Changes to occur Feb 2016

Summary
• Everyone has the potential to get sepsis
• Patients by definition have a high risk of sepsis
• Easy to identify – we know what we’re looking for
• Tools – EWS, Clinical Acumen and Experience
• Sepsis Screening Tool

Take home messages
• Sepsis presentation maybe non-specific, hugely
variable and multi-system
• When source unclear – review presenting symptoms
and signs and use appropriate imaging
• Procalcitonin is a useful biomarker in sepsis
• PCR techniques such as Septifast can aid with the
rapid detection of known bacterial genome

Any questions ?