Ryan Chuang Gillian Lieberman, MD July...
35
Intussusception Intussusception Ryan Chuang, Harvard Medical School, MS IV Ryan Chuang, Harvard Medical School, MS IV Gillian Lieberman, MD Gillian Lieberman, MD Ryan Chuang Gillian Lieberman, MD July 2002
-
Upload
truonghuong -
Category
Documents
-
view
227 -
download
0
Transcript of Ryan Chuang Gillian Lieberman, MD July...

IntussusceptionIntussusceptionRyan Chuang, Harvard Medical School, MS IVRyan Chuang, Harvard Medical School, MS IV
Gillian Lieberman, MDGillian Lieberman, MD
Ryan ChuangGillian Lieberman, MD July 2002

2
IntussusceptionIntussusception: Definition: Definition
Ryan ChuangGillian Lieberman, MD
• slipping of a length of intestine into an adjacent portion producing obstruction.
www.intellihealth.com
www.mayoclinic.com
IntussusceptumIntussuscipiens

3
Types of Types of IntussusceptionIntussusception
Ryan ChuangGillian Lieberman, MD
Anatomic Classification– Ileocolic– Ileoileal– Colocolic– Ileoileocolic
The CIBA Collection of Medical Illustrations; Vol. 3 Digestive System, Part II, Lower Digestive Tract. Netter, Frank, MD.

4
IntussusceptionIntussusception
Ryan ChuangGillian Lieberman, MD
Etiologic Classification1) Classical “idiopathic” presentation
- Mostly between ages 3 months – 3 years- Occurs more often in males than females- Theory of Hypertrophied Lymph Tissue Predisposition
2) Defined “lead point” cause- Occurs in all ages- < 10% of all cases- Generally requires surgical intervention

5
Possible Lead PointsPossible Lead Points
Ryan ChuangGillian Lieberman, MD
• Meckel’s diverticulum• Intestinal polyp• Intramural hematoma• Enteric duplication• LipomaCan occur in pts w/ lymphomas, Henoch-Schönlein purpura, Peutz-Jeghers Syndrome, etc.

6
Patient #1Patient #1
Ryan ChuangGillian Lieberman, MD
• 48 yo male w/ hx of tuberous sclerosis, mental retardation, and a seizure disorder
• Chief complaint on presentation:increased seizures, fever
• Incidental finding: “rigid abdomen”• Therefore, an abdominal CT was performed

7
Patient #1: CT ImagesPatient #1: CT Images
Ryan ChuangGillian Lieberman, MD
Small bowel-small bowel intussusceptionTarget Sign
Courtesy of the BIDMC Radiology Department

8
Patient #1: CT ReconstructionPatient #1: CT Reconstruction
Ryan ChuangGillian Lieberman, MD
Courtesy of the BIDMC Radiology Department
Intussusception,
Coronal View

9
Patient #2Patient #2
Ryan ChuangGillian Lieberman, MD
• 38 yo female w/ severe abdominal cramping and several episodes of bloody diarrhea presented at the Lahey ER
• Given IV fluids; Tolerated BRAT diet but 24 hours later, presented to PCP w/ RUQ & peri-umbilical pain, relieved by eating, radiating to back.
• No further diarrhea, no BRBPR, no melena

10
Patient #2Patient #2
Ryan ChuangGillian Lieberman, MD
• On PE, pt had mild RUQ tenderness• No guarding, no rebound, no masses felt• Bowel sounds are NL• On U/S, liver, spleen, and gallbladder all
appeared NL• Stool Cultures Pending• Family Hx negative for IBD or Colitis

11
Patient #2Patient #2
Ryan ChuangGillian Lieberman, MD
• Pt referred to the BIDMC• More history elicited…• No fevers or chills• No nausea or vomiting• Positive flatus and bowel movements• Had 2x similar episodes within past month;
Both resolved spontaneously. Most recent one associated with 3X of bloody stools

12
Patient #2Patient #2
Ryan ChuangGillian Lieberman, MD
• Pt takes no medications• Pt had no significant PMH• Pt had no history of surgeries• Colonoscopy done 2 yrs earlier was NL• Vital signs stable; Labs unremarkable
TIME TO IMAGE!!! TIME TO IMAGE!!! ☺☺Abdominal CT and BE were performedAbdominal CT and BE were performed

13
Patient #2: CT ScanPatient #2: CT Scan
Ryan ChuangGillian Lieberman, MD
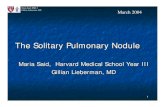
Mid-Transverse Colon Intussusception w/ associated mesentary stranding.
Lead point: 3.5x4.7 cm fatty mass representing an intraluminal lipoma.
Lipoma
Courtesy of the BIDMC Radiology Department

14
Patient #2: Barium EnemaPatient #2: Barium Enema
Ryan ChuangGillian Lieberman, MD
Barium enema performed next day showed contrast freely through the sigmoid and descending colon to the level of the mid-transverse colon and a large, rounded, intraluminal filling defect w/in the mid-transverse colon.
Courtesy of the BIDMC Radiology Department

15
Patient #2: Barium EnemaPatient #2: Barium Enema
Ryan ChuangGillian Lieberman, MD
Courtesy of the BIDMC Radiology Department
Colocolic Intussusception

16
Patient #2: Barium EnemaPatient #2: Barium Enema
Ryan ChuangGillian Lieberman, MD
• Barium enema has often been used to diagnosis and treat intussusception
• Standard method of reduction: rule of 3s- barium placed 3 feet above pt- let hang for 3 minutes- 3 tries before going to surgery
• If suspect bowel perforation, use H2 0- soluble contrast

17
Patient #2Patient #2
Ryan ChuangGillian Lieberman, MD
• For this pt, surgery treatment necessary• A right hemicolectomy w/ the lipoma
removed was performed a day after the barium enema
• Pt tolerated surgery well• Pt went home POD #3 in stable condition
with Percocet for pain

18
Patient #3Patient #3
Ryan ChuangGillian Lieberman, MD
• 14 yo boy w/ a 6 month hx of intermittent abdominal pain.
• Most recent episode of pain started one wk before presentation and associated w/ nausea and 2x emesis
• No fever, diarrhea, hematemesis, hematochezia nor melena

19
Patient #3Patient #3
Ryan ChuangGillian Lieberman, MD
• On PE, abdomen was diffusely tender• No masses palpable• No blood in stool• Prior CT at outside facility reportedly NL• Initial plain films of the abdomen taken…

20
Patient #3: Plain FilmPatient #3: Plain Film
Ryan ChuangGillian Lieberman, MD
Courtesy of the Children’s Hospital, Boston
Plain film: Some small bowel distention w/ multiple air-fluid levels in the small bowel and paucity of gas in the large bowel

21
Patient #3: Abdominal CTPatient #3: Abdominal CT
Ryan ChuangGillian Lieberman, MD
• Pt failed to improve, so a repeat abdominal CT was performed
Ileoileal Intussusception
Courtesy of the Children’s Hospital, Boston

22
Patient #3Patient #3
Ryan ChuangGillian Lieberman, MD
• CT scan revealed an ileoileal intussusception• Pt went to the operating room• Findings in the OR: Straw-colored ascites fluid,
an ileoileal intussusception, and an inverted Meckel’s diverticulum
• The intussusception was manually reduced• Meckel’s was resected, incidental appy performed,
and pt did well post-op.

23
Patient #4Patient #4
Ryan ChuangGillian Lieberman, MD
• 5 yo child presents with one week history of severe, intermittent, cramping abdominal pain, nausea and vomiting and 1x episode of blood in stool.
• Pt thought to have constipation – given 1x Fleet Enema for Children
• Pain felt worse, pt came to the Boston Children’s Hospital ER

24
Patient #4Patient #4
Ryan ChuangGillian Lieberman, MD
• Except for age, this is a more classical presentation of intussusception
• Common symptoms include intermittent, severe, crampy abdominal pain, vomiting and bloody stools
• Classic triad of abdominal pain, currant- jelly stools, and a sausage-shaped abdominal mass in R side of abdomen

25
Patient #4: UltrasoundPatient #4: Ultrasound
Ryan ChuangGillian Lieberman, MD
Pt had U/S exam in ER:
Courtesy of the Children’s Hospital, Boston
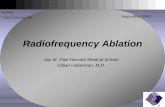
RUQ Transverse View
“Bull’s eye” / “Coiled spring” sign of Intussusception

26
Patient #4: UltrasoundPatient #4: Ultrasound
Ryan ChuangGillian Lieberman, MD
• U/S sensitivity and specificity for intussusception approaches 100%
• Classic U/S image: “bull’s eye” or “coiled spring” lesions representing layers of intestine within intestine.
• Lack of perfusion in intussusceptum detected w/ color duplex imaging may indicate development of ischemia

27
Patient #4: Air EnemaPatient #4: Air Enema
Ryan ChuangGillian Lieberman, MD
• With positive dx of Intussusception on U/S, the pt proceeded to an air enema
• Technique introduced in N. America by Chinese physicians in 1970s
• Perforation rate of <1%• Maximum P from air enema – 120 mmHg• 75-90% success rate

28
Patient #4: Air EnemaPatient #4: Air Enema
Ryan ChuangGillian Lieberman, MD
Courtesy of the Children’s Hospital, Boston
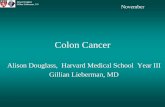
Pt in prone position on exam table
L R
Crescent Sign

29
Patient #4: Air EnemaEnema
Ryan ChuangGillian Lieberman, MD
• Crescent Sign – leading edge of the intussusceptum in the intussuscepiens
• Place child in prone position for air enema, hold down tightly, can feel a characteristic “pop” upon reduction
• If not working in prone position, can flip child over to supine and try again…

30
Patient #4: Air EnemaPatient #4: Air Enema
Ryan ChuangGillian Lieberman, MD
Courtesy of the Children’s Hospital, Boston
Pt in Supine Position on Exam Table
L LRR

31
Patient #4Patient #4
Ryan ChuangGillian Lieberman, MD
• Ileocecal intusussception successfully reduced in supine position!!! ☺
• Recurrence after successful nonoperative reduction is approximately 10%
• Recurrences should be handled as if it were an original episode
• Recurrences after surgery are <1%

32
IntussusceptionIntussusception: Overview: Overview
Ryan ChuangGillian Lieberman, MD
• Common cause of intestinal obstruction in young children (typically 3 mo – 3 yrs)
• Affects boy greater than girls• Most often seen in spring and fall• Symptoms include intense abdominal pain,
vomiting, fever, irritability, lethargy, and currant jelly stool.

33
IntussusceptionIntussusception: Overview: Overview
Ryan ChuangGillian Lieberman, MD
Role of Radiology: Diagnosis and CURE!• Abdominal X-ray – May show obstruction• Abdominal CT – Better at showing lesion• Ultrasound – Very sensitive AND specific• Barium Enema – Diagnostic and Curative!• Air Enema – Also Diagnostic and Curative!

34
ReferencesReferences
Ryan ChuangGillian Lieberman, MD
Lecture:Lecture:“Intussusception.” Children’s Department Radiology Rounds,Dr. Carlo Buonomo. July 18, 2002
Web Sites:Web Sites:www.uptodate.comwww.mayoclinic.comwww.intellihealth.com
Literature:Literature:The CIBA Collection of Medical Illustrations. Vol. 3 Digestive System, Part II Lower Digestive Tract. P. 134 “Intussusception.” Netter, Frank, MD.
The Radiologic Clinics of North America: Imaging the Acute Abdomen (Sept. ’94), Pediatric Gastrointestinal Radiology (July ’96), and the Imaging of the Acute Pediatric Abdomen (July ’97). W.B. Saunders Co.

35
AcknowledgementsAcknowledgementsSPECIAL THANKS TO:SPECIAL THANKS TO:The BIDMC Radiology DepartmentThe BIDMC Radiology Department
Gillian Lieberman, MD; Course Director Pamela Lepkowski, Course Assistant Larry Barbaras and Cara Lyn D’amour, WebmastersResidents Daniel Saurborn, MD; Michelle Swire, MDResidents Matthew Spencer, MD; Michael Goldfinger, MD
Children’s Hospital, Boston, Radiology Dept.Children’s Hospital, Boston, Radiology Dept.Dr. Carlo Buonomo, MDDr. Michael Callahan, MD
And Christian Dancz, HMS III
Ryan ChuangGillian Lieberman, MD
THE END!!! THE END!!! ☺☺