Abdominal manifestations of disease in AIDS...
43
Imaging of gastro-intestinal disease in patients with AIDS Cat Livingston, Harvard Medical School Year IV Gillian Lieberman, MD Cat Livingston, HMS IV Gillian Lieberman, MD November 2004
Transcript of Abdominal manifestations of disease in AIDS...

Imaging of gastro-intestinal disease in patients with AIDS
Cat Livingston, Harvard Medical School Year IVGillian Lieberman, MD
Cat Livingston, HMS IV Gillian Lieberman, MD
November 2004

2
Cat Livingston, HMS IV Gillian Lieberman, MD
Patient DR• DR is a 43 yo man with HIV and HCV who presents
with abdominal pain, one episode of minimal hematemesis, chronic weight loss, and diarrhea.
• Most recent viral load 15,500, CD4 91, on HAART• PMH
HIV/AIDSChronic Hepatitis CKaposi’s sarcomaCandida esophagitisRefractory ascitesEsophageal varices sp/ bandingHIV-associated dementia

3
Cat Livingston, HMS IV Gillian Lieberman, MD
DR’s Physical Exam (positive findings only)
General: Severely cachectic man
HEENT: Tongue beefy red, dried blood in mouth, dry mucous membranes
Abdomen: Distended, with shifting dullness. Guiaic +
Neuro: Alert and oriented x2. Perseverates. Motor 4/5 in all extremities.

4
Cat Livingston, HMS IV Gillian Lieberman, MD
DR’s Abdominal CT
Ascites
Cirrhotic liver Spleno-
megaly
PACS, BIDMC

5
Cat Livingston, HMS IV Gillian Lieberman, MD
MRI: cirrhosis and its consequences
Courtesy of Dr. Rofsky
Surface nodularity of the liver
Ascites
Varices
Splenomegaly

6
Cat Livingston, HMS IV Gillian Lieberman, MD
AIDS overview• 38 million people are living with HIV/AIDS • 20 million people have died since the beginning of
the epidemic• HAART markedly reduced mortality, AIDS,
AIDS-defining diagnoses and hospitalizations
• ¼ of HIV+ patients are co-infected with Hepatitis C virus
• Tuberculosis co-infection up to 40% - 60% in US inner cities.
UNAIDS. 2004 Report on the global HIV/AIDS epidemic. Geneva: Joint United Nationals Program on HIV/AIDS, July 2004.

7
Cat Livingston, HMS IV Gillian Lieberman, MD
DDx GI bleed and abdominal discomfort in DR
• Bleeding esophageal varices +/- coagulopathy• Bleeding ulcers (esophageal, gastric, duodenal)• Kaposi’s sarcoma• GI lymphoma• Cytomegalovirus colitis• Typhilitis• Cryptosporidiosis• Salmonellosis• Histoplasmosis• Spontaneous bacterial peritonitis

8
Cat Livingston, HMS IV Gillian Lieberman, MD
AIDS-defining illnesses (CDC)• Pneumocystis carinii pneumonia (42.6%)• Candidiasis of the esophagus or airway (15.0%)• Wasting (10.7%)• Kaposi’s sarcoma (10.7%)• Disseminated Mycobacterium avium complex (4.8%)• Tuberculosis (4.5%)• Cytomegalovirus disease (3.7%)• HIV-associated dementia (3.6%)• Recurrent bacterial pneumonia (3.0%)• Toxoplasmosis (2.6%)• Lymphoma (1.9%)• Cryptosporidiosis, persistent (1.5%)• Herpes simplex, chronic infection (0.5%)
Common
Less common

9
Cat Livingston, HMS IV Gillian Lieberman, MD
CD4 Count and Pathogens
CD4 >200 CD4 200-100 CD4 <100cells/uLTuberculosisCandidiasisHerpes simplexHerpes zosterHairy leukoplakiaKaposi’s sarcoma
CryptosporidiosisCoccidiodomycosis sCryptococcisToxoplasmosisPneumocystosis
Mycobacterium avium complexHistoplasmosisCytomegalovirusLymphoma

10
Cat Livingston, HMS IV Gillian Lieberman, MD
Abdominal disease in AIDS
Two major categories:1) Infection
2) Neoplasma. Kaposi’s sarcomab. Non-Hodgkin’s lymphomas

11
Cat Livingston, HMS IV Gillian Lieberman, MD
Abdominal symptoms in AIDSVery common (up to 90%)
Intolerance to medicationsThrushDiarrhea – chronic, associated with weight
loss and malnutritionCommon
Odynophagia and dysphagiaAbdominal pain (RUQ especially)FeversAnorectal disease
12
Cat Livingston, HMS IV Gillian Lieberman, MD
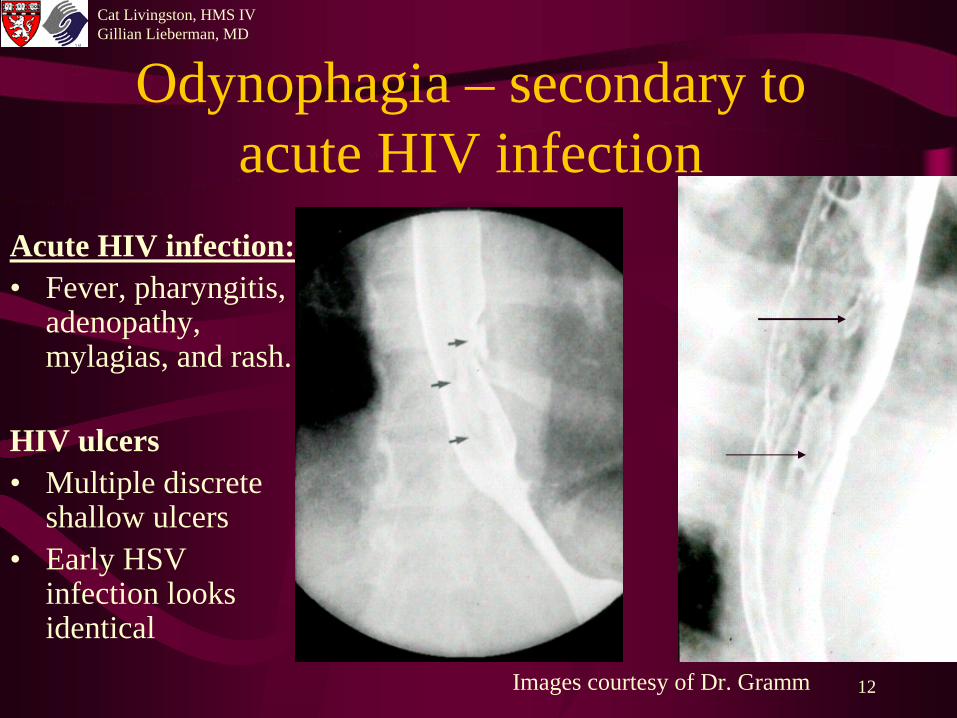
Odynophagia – secondary to acute HIV infection
Acute HIV infection:• Fever, pharyngitis,
adenopathy, mylagias, and rash.
HIV ulcers• Multiple discrete
shallow ulcers• Early HSV
infection looks identical
Images courtesy of Dr. Gramm

13
Cat Livingston, HMS IV Gillian Lieberman, MD
Candida esophagitis
Images Courtesy of Dr. Gramm
Second most common AIDS- defining illness
Present with odynophagia, dysphagia, or chest pain.
CD4 count <200cells/uL
Diffuse, confluent plaques present, with a “cobblestone” appearance.
Mild
Advanced

14
Cat Livingston, HMS IV Gillian Lieberman, MD
Candida esophagitis
Courtesy of Dr. Gramm
Creamy plaques present along the long axis of the esophagus in this less severe case.
Advanced case:
Confluent plaque creating a pseudo- membrane is present.
Wall SD, Yee J, Reeders J. Imaging of the lumenal gastrointestinal tract in AIDS. Saunders: London. 1998, pp. 168-187.

15
Cat Livingston, HMS IV Gillian Lieberman, MD
CMV esophagitis
Redvanly RD, Silverstein JE. Intra-abdominal manifestations of AIDS. In Radiologic Clinics of North America: Imaging of the patient with AIDS. 1997 35(5): Figure 8.
There are multiple large (>2cm), discrete ulcers in the distal esophagus. Note the intervening mucosa is normal.
Vasculitis ischemia ulcer formation

16
Cat Livingston, HMS IV Gillian Lieberman, MD
Diarrhea in an patient with AIDS Symptoms Likely Pathogens
Epigastric cramps, bloating, nausea MAC, Cryptosporidium, Isospora
Severe watery diarrhea, weight loss Cryptosporidiosis
Hematochezia and lower abdominal CMV, C. diff, Shigella, cramping Campylobacter
Anorectal tenesmus, dyschezia Herpes simplex virus, N. gonorrhea, Chlamydia
An aggressive approach to diagnosis is recommended.

17
Cat Livingston, HMS IV Gillian Lieberman, MD
Cryptosporidiosis
• Occurs with CD4 count <200cells/uL• Intracellular parasites that infect GI tract epithelial cells• Causes a hypersecretory diarrhea
– Similar to Isospora belli and Microsporidia infection
Non-specific radiographic findings:• Small bowel fold enlargement• Gastropathy (rigidity)• Gallbladder wall thickening

18
Cat Livingston, HMS IV Gillian Lieberman, MD
CryptosporidiosisGastropathy with retained food
Jejunal fold enlargement
Courtesy of Dr. Gramm

19
Cat Livingston, HMS IV Gillian Lieberman, MD
Mycobacterium avium complex
• Occurs with CD4 count<100cells/uL• Typically present with clinical enteritis:
abdominal pain, fevers, malabsorption, night sweats, weight loss, severe anemia,
• Bulky mesenteric adenopathy and small bowel involvement
• Disseminated MAC infection hepatosplenomegaly with microabscesses

20
Cat Livingston, HMS IV Gillian Lieberman, MD
Mycobacterium avium complex
Wilcox, CM. Overview of gastrointestinalmanifestations of AIDS. UpToDate. 2004.
Duodenal and jejunal irregular fold thickening
Courtesy of Dr. Gramm
Lamina propria macrophages containing MAC

21
Cat Livingston, HMS IV Gillian Lieberman, MD
MAC enteritis
Redvanly RD, Silverstein JE. Intra-abdominal manifestations of AIDS. In Radiologic Clinics of North America: Imaging of the patient with AIDS. 1997 35(5): 1083-1125.
Jejunal bowel wall thickening

22
Cat Livingston, HMS IV Gillian Lieberman, MD
Mycobacterium avium complexBulky mesenteric lymphadenopathy present.
CD4 < 50cells/uL
It is important to distinguish from tuberculosis lymphadenitis.
Courtesy of Dr. Gramm

23
Cat Livingston, HMS IV Gillian Lieberman, MD
Nodal enlargement DDx• Mycobacterium tuberculosis• Mycobacterium avium complex• Cytomegalovirus• Varicella zoster virus• Pneumocystis carinii• Histoplasmosis• Cryptococcosis• Lymphoma• Kaposi’s sarcoma

24
Cat Livingston, HMS IV Gillian Lieberman, MD
Mycobacterium tuberculosis
PACS, BIDMC
“The Great Imitator”
Most common – low attenuation mesenteric lymphadenopathy, nodules in the omentum and peritoneum, and high attenuation ascites.
Minimal retro- peritoneal adenopath y, low attenuation

25
Cat Livingston, HMS IV Gillian Lieberman, MD Cytomegalovirus colitis
PACS, BIDMC
CMV is most common life threatening opportunistic infection in the AIDS patient. CD4 count <100cells/uL. Pneumatosis and bowel perforation can result.
Markedly thickened folds of the transverse and descending colon, consistent with pseudo- membrane formation

26
Cat Livingston, HMS IV Gillian Lieberman, MD
Cytomegalovirus colitis
http://www.hopkins- aids.edu/educational/caserounds/images/jhas_ case_abpelvic2.jpeg
Wall SD, Yee J, Reeders J. Imaging of the lumenal gastrointestinal tract in AIDS. In Reeders J, Mathieson JR (Eds.) AIDS Imaging: A practical clinical approach. Saunders: London. 1998, figure 16.20..
Circumferential ulcerated stricture
Vasculitis in submucosathrombosis and ischemia

27
Cat Livingston, HMS IV Gillian Lieberman, MD
Liver and Biliary Tree• Hepatomegaly very common
(50% clinically, vast majority at autopsy)• Chronic HBV or HCV infection widespread• Liver tests are non-specific in HIV-infected
patients and liver biopsies abnormal in 95%.• AIDS cholangiopathy

28
Cat Livingston, HMS IV Gillian Lieberman, MD
AIDS cholangiopathy
• Cryptosporidium or Cytomegalovirus• Present with right upper quadrant pain,
nausea, vomiting, fever, and elevated white count and serum alkaline phosphatase
• Acalculous cholecystitis• AIDS cholangitis – features:
– Papillary stenosis– Biliary duct strictures and thickening

29
Cat Livingston, HMS IV Gillian Lieberman, MD
Acalculous Cholecystitis
Images courtesy of Dr. Gramm
Gallbladder wall thickening in both CT and ultrasound. Minimal pericholecystic fluid is present on ultrasound.

30
Cat Livingston, HMS IV Gillian Lieberman, MD
AIDS cholangiopathy
Courtesy of Dr. Gramm
strictures
large abscess
Mathieson JR, Smith FR. Hepatobiliary and pancreatic ultrasound in AIDS. Saunders: London. 1998, Figure 17.19.
ductal dilatation

31
Cat Livingston, HMS IV Gillian Lieberman, MD
Anorectal Disease• Most common in patients who engage in anal intercourse
Symptoms:Dyschezia, BRBPR, tenesmus
Findings:Perirectal abscessesAnal fistulasUlcerations ProctitisAnorectal carcinoma

32
Cat Livingston, HMS IV Gillian Lieberman, MD
HSV Proctitis
PACS, BIDMC
Peri-rectal wall thickening secondary to inflammation, with possible fistula formation.

Neoplasms of the GI tract

34
Cat Livingston, HMS IV Gillian Lieberman, MD
Kaposi’s sarcoma
Courtesy of Dr. Gramm
• More likely to occur in homo- or bi-sexual patients with CD4 count <200cells/uL
• Associated with human herpes virus 8
• Preceded by cutaneous manifestations
Bulky polypoid lesions

35
Cat Livingston, HMS IV Gillian Lieberman, MD
Kaposi’s sarcoma of the colonComplications: Diarrhea, bleeding, obstruction, perforation, and protein-losing enteropathy
Hepatosplenomegaly is also common
DDx: lymphoma, infection, hematogenous metastases, polyps, Crohn’s, and bacillary angiomatosis
Large, annular, submucosal red-purple masses – circumferential infiltration and obstruction in the colon
Dezube BJ, Groopman JE. AIDS-related Kaposi’s sarcoma: Clinical features and treatment. UpToDate 1December 2003. Picture 4.

36
Cat Livingston, HMS IV Gillian Lieberman, MD
Non-Hodgkins lymphoma
• 60-fold greater risk of developing lymphoma than in the general population
• Almost all have extranodal disease
• Bulky adenopathy common• (DDx includes KS and mycobacterium)

37
Cat Livingston, HMS IV Gillian Lieberman, MD
Non-Hodgkins lymphoma
*
*
Hepatomegaly with two low attenuation lesions present in the liver.
*
*
Koh DM. Langroudi B, Padley SPG. Abdominal CT in patients with AIDS. Imaging 2002: 24-34. Figure 12a.
Ultrasound of liver with multiple hypoechoic lesions.
Redvanly RD, Silverstein JE. Intra-abdominal manifestations of AIDS. In Radiologic Clinics of North America: Imaging of the patient with AIDS. 1997 35(5).

38
Cat Livingston, HMS IV Gillian Lieberman, MD
Disseminated disease
• Hematogenous dissemination is rare• Why? Neutrophil function is relatively intact
• Granulocytopenia secondary to– Medications– Infected indwelling catheters

39
Cat Livingston, HMS IV Gillian Lieberman, MD Disseminated candidiasis
Necrotizing entercolitis
Redvanly RD, Silverstein JE. Intra-abdominal manifestations of AIDS. In Radiologic Clinics of North America: Imaging of the patient with AIDS. 1997 35(5): Figure 6.
Pneumatosis intestinalis and mesenteric air are present.

40
Cat Livingston, HMS IV Gillian Lieberman, MD
DRDR is a patient with advanced AIDS• Bleeding esophageal varices secondary to portal
hypertension from cirrhosis and coagulopathyA therapeutic paracentesis was performed.During his hospital course he received treatment for
candidal esophagitis.Social work became involved because it was unclear
he had been taking his medications, a VNA was re-organized.
He was placed on a NJ feeding tube for his AIDS enteropathy (chronic diarrhea, weight loss, and malnourishment).

41
Cat Livingston, HMS IV Gillian Lieberman, MD
ReferencesCDC Surveillance for AIDS: Defining opportunistic illnesses 1992-1997. MMWR Morbidity
and Mortality Weekly Report 1999; 48:1.
Dezube BJ, Groopman JE. AIDS-related Kaposi’s sarcoma: Clinical features and treatment. UpToDate December 2003. Picture 4.
Erbelding, EJ. Case 2: A 30 yuear old woman with AIDS, abdominal pain, and fevers. http://www.hopkins-aids.edu/educational/caserounds/images/jhas_case_abpelvic2.jpeg
Koh DM. Langroudi B, Padley SPG. Abdominal CT in patients with AIDS. Imaging 2002: 24-34. Figures 12a and 12c.
Mathieson JR, Smith FR. Hepatobiliary and pancreatic ultrasound in AIDS. In Reeders J, Mathieson JR (Eds.) AIDS Imaging: A practical clinical approach. Saunders: London. 1998, 188-202.
Radin DR. Hepato-pancreato and biliary imaging in AIDS: Computed Tomography. In Radiologic Clinics of North America: Imaging of the patient with AIDS. 1997 35(5): 203-213.
Redvanly RD, Silverstein JE. Intra-abdominal manifestations of AIDS. In Radiologic Clinics of North America: Imaging of the patient with AIDS. 1997 35(5): 1083-1125.
Scully RE, Mark EJ, McNeely WF, Ebeling SH, Ellender SM. Case Records of the Massachusetts General Hospital. Case 5-2000. New England Journal of Medicine 2000, 342(7):493-500.

42
Cat Livingston, HMS IV Gillian Lieberman, MD
References continuedUNAIDS. 2004 Report on the global HIV/AIDS epidemic. Geneva: Joint United
Nationals Program on HIV/AIDS, July 2004.Wall SD, Yee J, Reeders J. Imaging of the lumenal gastrointestinal tract in AIDS.
In Reeders J, Mathieson JR (Eds.) AIDS Imaging: A practical clinical approach. Saunders: London. 1998, pp. 168-187.
Wilcox, CM. Overview of gastrointestinal manifestations of AIDS. UpToDate. 2004. Histology 1.

43
Cat Livingston, HMS IV Gillian Lieberman, MD
Acknowledgements
Herbert Gramm, MDNeil Rofsky, MDPamela LepkowskiGillian Lieberman, MDLarry Barbaras