Jay W. Patti Harvard Medical School Gillian...
26
Jay Patti Gillian Lieberman, MD Radiofrequency Ablation Jay W. Patti Harvard Medical School Gillian Lieberman, M.D. September 2001
Transcript of Jay W. Patti Harvard Medical School Gillian...
Jay PattiGillian Lieberman, MD
Radiofrequency AblationJay W. Patti Harvard Medical School
Gillian Lieberman, M.D.
September 2001
Jay PattiGillian Lieberman, MD
But first, 2 unknown quiz cases
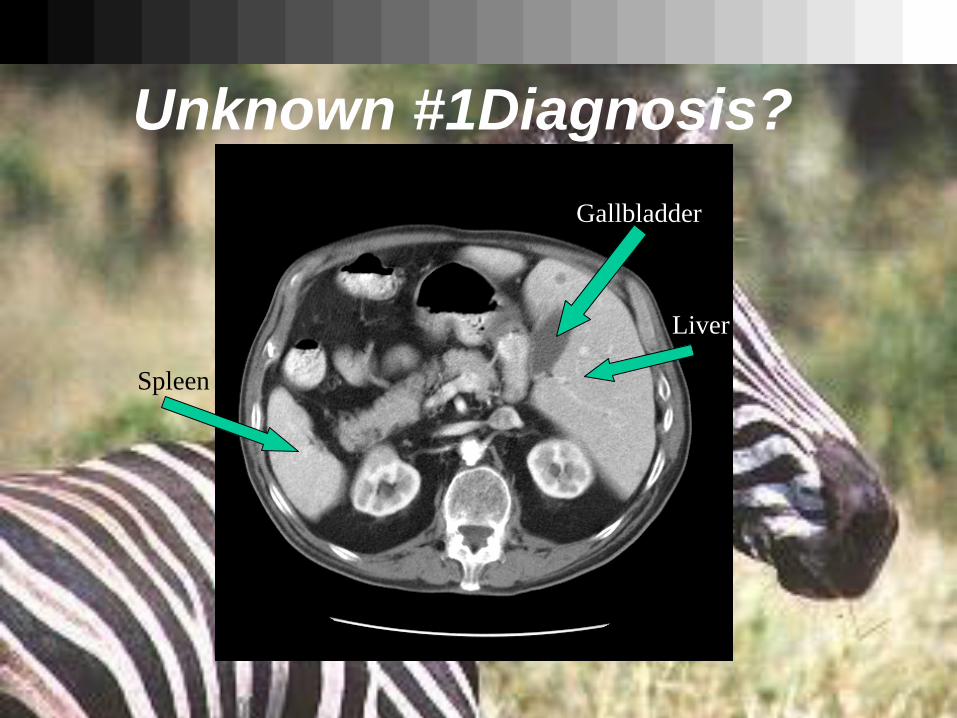
Jay PattiGillian Lieberman, MDUnknown #1Diagnosis?
Spleen
Gallbladder
Liver
Jay PattiGillian Lieberman, MD
Situs inversus viscerum• 1 in 10,000 to 15,000 adults in the United States• levocardia in the presence of situs inversus. • Can be associated with a single ventricle, pulmonary stenosis,
arterial transposition, VSDs, ASDs, atrioventricular septal defect, anomalous pulmonary venous return, tricuspid atresia, and pulmonary arterial hypoplasia or atresia.
• 50% of people with Primary Ciliary Dyskinesia (PCD) have Kartegener's syndrome: situs inversus, chronic sinusitis and otitis, and airways disease leading to bronchiectasis
• 25% of people with situs inversus have PCD• If none of the above associated abnormalities are present then it
is usually asymtomatic

Jay PattiGillian Lieberman, MD Unknown #2 Diagnosis?

Jay PattiGillian Lieberman, MD Unknown #2
Jay PattiGillian Lieberman, MD Diagnosis:
THE PATIENT TOOK A BREATHwhich moved the kidneys superior and created an artifact that appears as though there is a mass above the left kidney. It is very important to keep a wide angle when looking at an area of suspected pathology. (It is tempting to narrow ones field to the area of interest.)
Jay PattiGillian Lieberman, MD
Radiofrequency AblationIs the process by which discrete quantities of energy in the form of radiofrequency are deposited in specific tissues in an attempt to cause coagulative necrosis in a predetermined area.
(Cooking tumors in vivo)
Jay PattiGillian Lieberman, MD Patient History
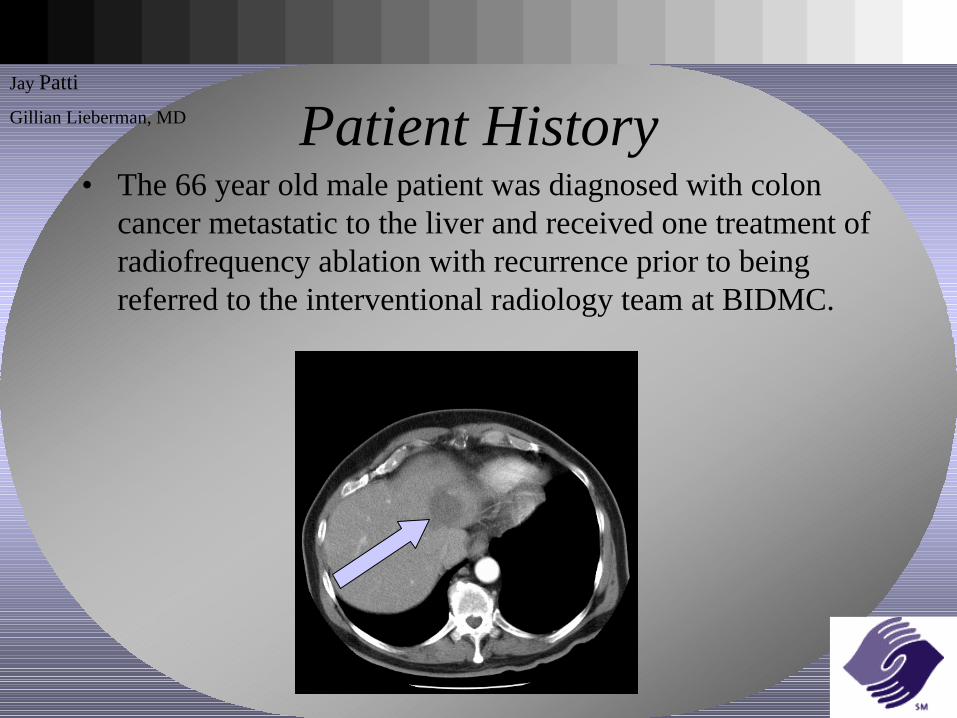
• The 66 year old male patient was diagnosed with colon cancer metastatic to the liver and received one treatment of radiofrequency ablation with recurrence prior to being referred to the interventional radiology team at BIDMC.
Jay PattiGillian Lieberman, MD Indication
• Radiofrequency ablation was first used in the treatment of unresectable hepatocellular carcinoma. This patient population provided a means to show that radiofrequency is safe, useful, technically straightforward and inexpensive.
• Currently radiofrequency ablation is used to treat hepatocellular carcinoma, colon metastases to the liver, renal cell carcinoma, chordomas, osteoid osteomas, fibroids, cutaneous metastases, and other tumors are under investigation. It is currently FDA cleared for the “treatment of soft tissue masses”
• Size and proximity to adjacent organs limits the use of radiofrequency ablation.
Jay PattiGillian Lieberman, MD The Procedure
• Radiofrequency ablation can be preformed either percutaneously or intraoperatively.
• The procedure is preformed under ultrasound or CT guidance. The skin over the area of interest is cleaned with iodine and draped. It is important to maintain sterile conditions as the resultant necrotic tissue in the burned lesion is a nutrient rich broth for bacterial growth.
• The patient is provided with conscious sedation (benzodiazipine and narcotic). Some patients experience severe pain during the procedure which subsides after the treatment. Post-procedure patients may experience a dull ache or may be pain free.
• It is also important to prevent collateral damage of adjacent organs. Appropriate planning and intraprocedural monitoring of adjacent structures is necessary.
• Ablation of the needle tract is believed to reduce seeding the tract.
Jay PattiGillian Lieberman, MD The Equipment
• THE BASICS:A RF probe is a metal needle that is covered by a plastic material on all but the tip of the probe. The tip makes direct contact with the tissue in the treatment area.
• There are many different types of RF probes in use but the two most common types are:
RITA probe - Has three, four or six umbrella shaped prongs which can be deployed from with in the tumor.
Cool-tip - Single or multiple parallel probes that are internally cooled during the procedure by a closed circuit cold water pump.
• Multiple grounding pads are used to complete the circuit.
Jay PattiGillian Lieberman, MD The Equipment
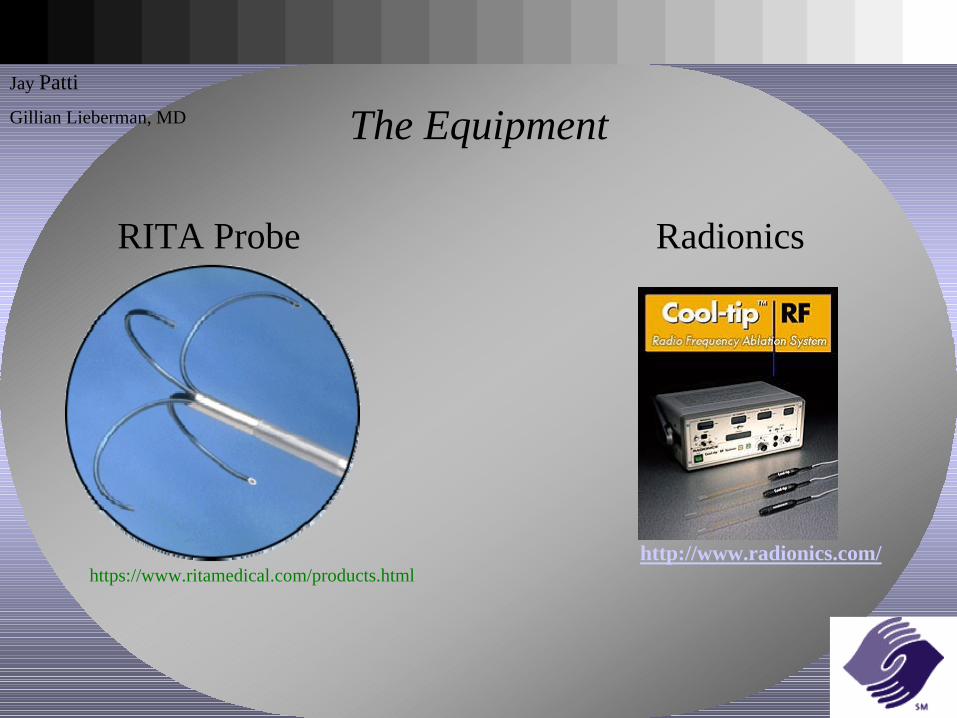
RITA Probe Radionics
http://www.radionics.com/https://www.ritamedical.com/products.html
Jay PattiGillian Lieberman, MD
Pathophysiology of Tissue Damage• The exposed tip of the probe emits radiofrequency in the range of 500
kHz. This energy excites the ions in the surrounding tissue which through friction raises the temperature of the tissue.
• At temperatures above 50 degrees centigrade the tissue literally cooks in vivo.
• The temperature is measured throughout the procedure by thermometers on the exposed tips of the probe.
• Current methods of RFA have increased the area of tissue necrosis from 1.6 cm diameter to 4-5 cm diameter.
• Temperature of 105 degrees centigrade for 10 minutes creates the ideal sphere. Time to return to body temperature indicates quality of treatment sphere.
• Treatment area should include a rim (margin) of healthy tissue to reduce recurrence.
Jay PattiGillian Lieberman, MD Limitations
Char-Broil:• The impedance of the tissue rises as the cellular framework becomes disrupted and the
tissues begin to char.• The increased impedance acts as an insulation and hence isolates the energy producing
tip from more distant tissues. Heat Sink:• Tissue is continuously cooled by the relatively cool blood supply passing the cooking
tissue. This too prevents the heating of tissues distant from the site of treatmentVariable Heat Conduction: • Some tumors conduct heat better than others, presumably due to vascularity and ionic
density although never specifically shown. Neighboring Structures:• Structures such as blood vessels use the heat sink effect as an internal protection.
Structures such as the gallbladder and loops of bowel do not have such internal defenses and are particularly vulnerable to the increased temperatures.
Jay PattiGillian Lieberman, MD Working Around Limitations
Char-Broil:• Most probes currently in use have internal safety mechanisms to limit both the increase
in impedance and temperature. The turn off or pulse (much like a microwave oven in defrost mode) when they reach a defined level.
Heat Sink:• The pringle maneuver is often used to reduce the heat sink effect while ablating a tumor
in the liver. Variable Heat Conduction: • Some tumors are better conductors of heat. This phenomenon can be beneficial in that
the tumor acts as vector for transferring heat to more tumor. Healthy tissue is hence protected from the increased heat transferred to other malignant tissue. A cirrhotic liver can also act as an insulator for the treatment area which aids in ablation (oven effect).
Neighboring Structures:• Extra thermometers are often placed between the treatment area and the threatened
organ the local temperature can be monitored and treatment can be pulsed accordingly.
Jay PattiGillian Lieberman, MD Lost to Follow-up
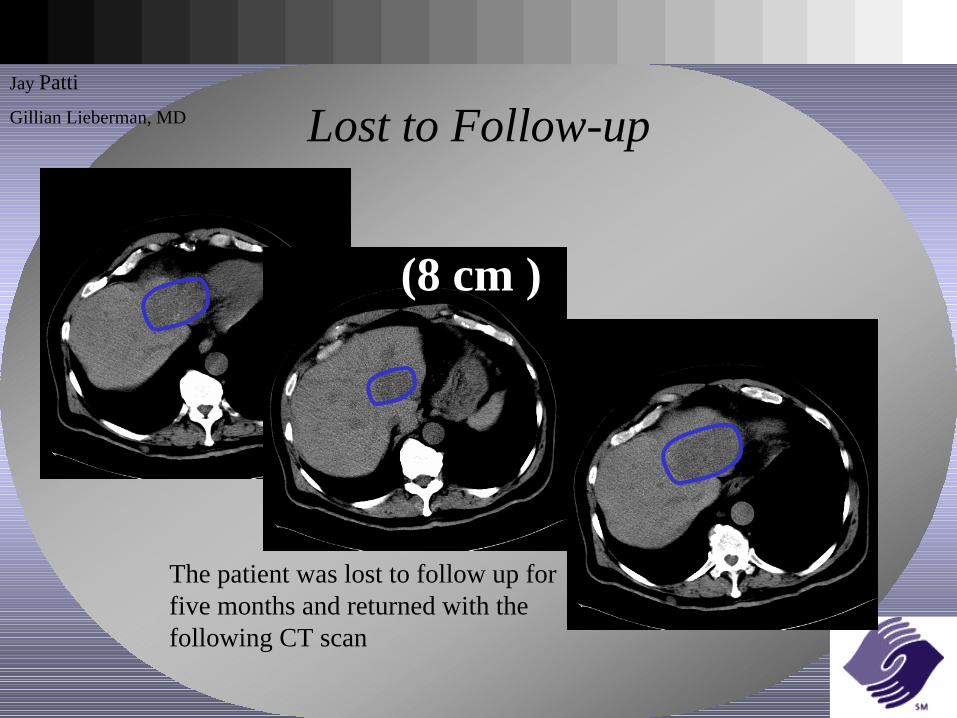
The patient was lost to follow up for five months and returned with the following CT scan
(8 cm )

Jay PattiGillian Lieberman, MD The Sphere of Ablation
• Around every burn area is an area of tissue that has been heated but not killed. This area is where most malignant cells evade ablation.
Damaged
Killed
Jay PattiGillian Lieberman, MD Expanding the Sphere
Current research is concentrating on creating larger yet predictable spheres of ablation.
Injection of hypertonic fluids Chemoembolization
Multiple Probes Heat Activated Liposomes
Aimed at increasing tonicity of tissues and decreasing impedance within tumor
Two strike concept making the RF area more succeptable to chemo or vise versa.
Multiple treatment areas within the same treatment session. This is commonly used.
Liposomes that carry chemotherapy across membranes can be activated by heat.
Jay PattiGillian Lieberman, MD
Pretreatment with Doxorubicin
• This particular patient was chosen for a new protocol which involved pretreatment with systemic doxorubicin.
• Patient was in the “48 hour Pre-treatment” group. Optimal timing of treatments is currently under investigation.
• Recent studies by Goldberg et. al. (2001) in mice have showed the ability to increase treatment area by possibly increasing the tumor cell sensitivity to RFA.
• Diameter of treatment area has been shown to double with combined treatment.
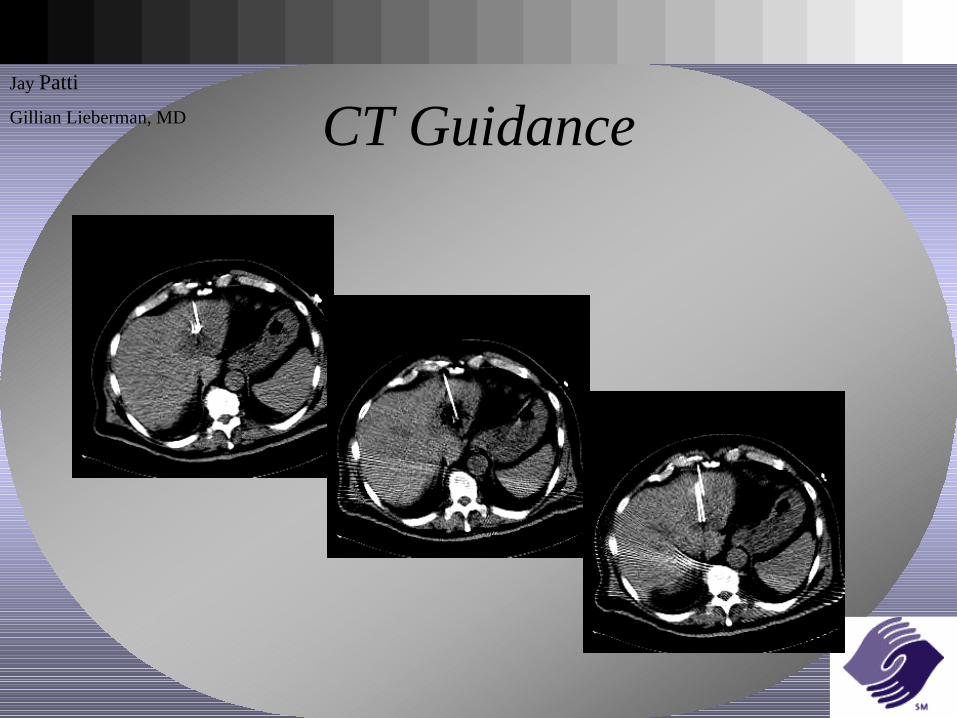
Jay PattiGillian Lieberman, MD CT Guidance
Jay PattiGillian Lieberman, MD Post Ablation Imaging
• Immediate post ablation imaging has been shown to have limited ability to correctly differentiate kill area and residual tumor.
• The kill area will appear hypodense and non enhancing
• The “Damaged Area” enhances as there is vascular permeability and inflammatory response.
• CT imaging is recommended after 2 weeks and is usually done at 6 weeks post ablation.
Jay PattiGillian Lieberman, MD
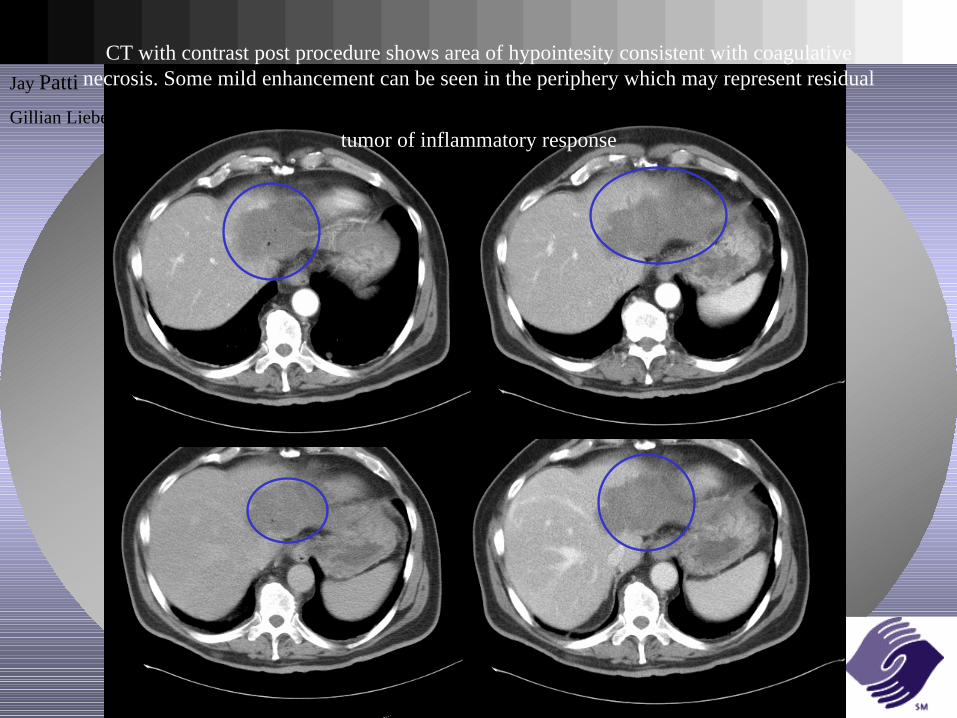
CT with contrast post procedure shows area of hypointesity consistent with coagulative necrosis. Some mild enhancement can be seen in the periphery which may represent residual
tumor of inflammatory response
Jay PattiGillian Lieberman, MD Summary
Indicationhepatocellular carcinoma, colon metastases to the liver, renal cell carcinoma, chordomas, osteoid osteomas, fibroids, cutaneous metastases, and other tumors are under investigation.
ProcedureUsing an insulated probe with the tip exposed, Radiofrequency is administered at a specific site guided by CT or US.
Pathophysiology of Tissue DamageIonic agitation to ideal temperature coagulative necrosis
Limitations and Working Around ThemChar Broil, Heat Sink, Tissue Conduction, Collateral Damage
Current RFA ResearchHypertonic Fluids, Chemoembolization, Multiple Probes, Liposomes
Jay PattiGillian Lieberman, MD
References
1. Goldberg SN, Saldinger PF, Gazelle GS, Huertas JC, Stuart KE, Jacobs T, Kruskal JB. Percutaneous Tumor Ablation Increases Necrosis with Combined Radiofrequency Ablation and Intratumoral Doxorubicin Injection in the Rat Breast Tumor Model. Radiology 2001;220(2)420-427
2. Gazelle GS, Goldberg SN, Solbiati L, Livraghi T. Tumor Ablation with Radiofrequency Energy. Radiology 2000;217:633-646
3. Livraghi T, Goldberg SN, Lazzaroni S, Meloni F, Solbiati L, Gazelle GS. Small Hepatocellular Carcinoma: Treatment with Radiofrequency Ablation versus Ethanol Ablation. Radiology 1999;210:655-661
4. MDConsult.com Surgery Text Book.…… and many more
Jay PattiGillian Lieberman, MD
Acknowledgements
•Special thanks to Larry Barbaras and Cara Lyn D’amour, our Webmasters
•Dr. Gillian Lieberman
•Pamela Lepkowski