Ruptured ectopic pregnancy in non-communicating right rudimentary horn: A case report
6
Ruptured ectopic pregnancy in non-communicating right rudimentary horn: A case report
-
Upload
apollo-hospitals -
Category
Health & Medicine
-
view
1.052 -
download
0
Transcript of Ruptured ectopic pregnancy in non-communicating right rudimentary horn: A case report

Ruptured ectopic pregnancy in non-communicating right rudimentary
horn: A case report

Case Report
Ruptured ectopic pregnancy innon-communicating right rudimentaryhorn: A case report
Ahmed S. Elagwany*, Hisham H. Elgamal, Tamer M. Abdeldayem
Department of Obstetrics and Gynecology, Alexandria University, Egypt
a r t i c l e i n f o
Article history:
Received 19 August 2013
Accepted 4 October 2013
Available online xxx
Keywords:
Acute abdomen
Hemoperitoneum
Rudimentary horn
Rupture
Ultrasound
a b s t r a c t
Rudimentary horn is a developmental anomaly of the uterus, and pregnancy in a non-
communicating rudimentary horn is very difficult to diagnose before it ruptures. As the
fetus enlarges in the rudimentary horn, the chances of rupture in the first or second
trimester are increased. Catastrophic hemorrhage results in increased maternal and
perinatal mortality and morbidity. To date, management of such cases remains a challenge
due to diagnostic dilemma. Expertise in ultrasonography and early resort to surgical
management are lifesaving in such cases. A case of undiagnosed rudimentary horn preg-
nancy presented to our department in shock with features of acute abdomen, and the
diagnosis was confirmed at laparotomy that revealed ruptured rudimentary horn preg-
nancy. And excision of the accessory horn was done.
Copyright ª 2013, Indraprastha Medical Corporation Ltd. All rights reserved.
1. Introduction
Congenital uterine malformations are the result of abnormal
Mullerian duct development, fusion, canalization and septal
resorption. The prevalence of congenital uterine anomalies
among fertilewomen is reported as 1:200e1:600.Where there is
atresia of one of the Mullerian duct, there is a unicornuate
uterus with a single tube. Its true incidence is unknown and is
approximately estimatedat a rate of about 1 in250.Unicornuate
uterusmay also have a rudimentary horn. Rudimentary horn is
one of the rarest congenital uterine anomalies. The prevalence
of unicornuate uterus with rudimentary horn is even rarer i.e.
1:100,000.1 The rudimentary horn may consist of a functional
cavity, or itmaybe a small solid lumpof theuterinemusclewith
no functional endometrium. In a series of 366 cases with rudi-
mentary horn, non-communicating horn accounted for 92% of
cases, and renal anomaly was found in 36% cases. Unilateral
renal agenesis was found in 38% cases in another series.2
Provided there is no obstruction to menstrual flow, these
uterine anomalies present few problems in the absence of
pregnancy. Pregnancy in a rudimentary horn is rare. The
incidence of rudimentary horn pregnancy is difficult to
calculate. Frequently quoted figures are between 1 per 76,000
and 1 per 140,000 pregnancies.3
A case of pregnancy occurring in a rudimentary horn with
consequent rupture is reported.
2. Case report
An unusual case of a 25-year-old woman, G1P0, with a preg-
nancy of 18 weeks, presented to the emergency unit of our
* Corresponding author. El-Shatby Maternity Hospital, Alexandria University, Alexandria, Egypt. Tel.: þ20 1228254247.E-mail address: [email protected] (A.S. Elagwany).
Available online at www.sciencedirect.com
journal homepage: www.elsevier .com/locate/apme
a p o l l o m e d i c i n e x x x ( 2 0 1 3 ) 1e4
Please cite this article in press as: Elagwany AS, et al., Ruptured ectopic pregnancy in non-communicating right rudimentaryhorn: A case report, Apollo Medicine (2013), http://dx.doi.org/10.1016/j.apme.2013.10.002
0976-0016/$ e see front matter Copyright ª 2013, Indraprastha Medical Corporation Ltd. All rights reserved.http://dx.doi.org/10.1016/j.apme.2013.10.002

department with acute abdominal pain and hypovolemic
shock. The patient did not seek antenatal care before admis-
sion. Pregnancy was diagnosed by urine pregnancy test after a
missed period for one week. Ultrasound was not done till
admission .The patient was illiterate and living in a rural area
far away from any health facility. She was not complaining
so she did not seek medical advice. No other significant his-
tory was noted.
On examination, the patient was drowsy, in agony and in a
nearly shock state with pale, cold, clammy extremities, a
thready pulse of 120 beats/minute and arterial blood pressure
of 70/40 mmHg.
Abdominal examination revealed distention and tenderness
all over. On vaginal examination, mild vaginal bleeding was
noted. A speculum examination did not reveal any cervical or
vaginalpathology.Thecervicaloswas tightlyclosed.Thepatient
was resuscitatedwith intravenous fluids and blood transfusion.
Further assessment with transabdominal ultrasound
showed a free floating nonviable fetus of 18weeks gestation in
abdominal cavity with anhydramnios and moderate abdom-
inal collection surrounding. Absent visual continuity of myo-
metrial tissue surrounding the fetus was noted. The placenta
was intrauterine, lying posterior with no retroplacental clots
seen. Abdominal tapping with spinal needle revealed non
clotted dark bloody collection.
In view of the previous data, a provisional diagnosis of a
ruptured uterus with a differential diagnosis of an abdominal
pregnancy was made.
An emergency laparotomy was performed immediately
after resuscitation. Intraoperative findings revealed a uni-
cornuate uterus with a ruptured pregnancy in a right rudi-
mentaryhorn.Also, adead fetusfloating in theperitoneal cavity
with blood clots surrounding was noted. The placenta was still
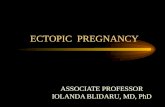
attached to the cavity of the rudimentary horn (Figs. 1 and 2).
It was, however, difficult to visualize the uterine septum.
No communication from the horn to the contralateral uterine
cavity was seen. The uterus, lying separate in the pelvis, was
soft in consistency, globular and enlarged to a size consistent
with tenweeks. The right fallopian tube and ovary were found
healthy and were attached normally to the unicornuate
uterus.
Excision of the rudimentary horn and the right fallopian
tube with conservation of the right ovary was done together
with the nonviable fetus and the placenta. All the pedicles
were secured with good hemostasis. A total volume of nearly
2 L of hemoperitoneum blood was also removed. Both the
ureters and kidneys were normal. Due to the significant blood
loss throughout the operation, the patient was given a
massive blood transfusion of four units and two units of
plasma transfusion.
The excised specimen was sent for histopathological ex-
amination, which was reported as (sections from the uterine
horn show areas of hemorrhage and necrosis. Section from
the fallopian tube was morphologically normal. Sections of
the placenta showfibrosed chorionic villi with syncytial knots.
No villitis was seen). Histopathology confirmed the diagnoses
(ruptured pregnant uterine rudimentary horn).
Post-operatively, hemoglobin level was 9.8 g/dl. Patient had
a smooth postoperative recovery. The patient was counseled
for contraception with oral pills for one year. The patient was
discharged healthy two days after admission.
Follow-up appointment was planned for intravenous uro-
gram to rule out any associated renal anomalies. No associ-
ated renal anomaly was diagnosed. The patient was
Fig. 1 e A nonviable fetus with placenta attached to ruptured right rudimentary horn.
a p o l l o m e d i c i n e x x x ( 2 0 1 3 ) 1e42
Please cite this article in press as: Elagwany AS, et al., Ruptured ectopic pregnancy in non-communicating right rudimentaryhorn: A case report, Apollo Medicine (2013), http://dx.doi.org/10.1016/j.apme.2013.10.002

scheduled for a hysterosalpingogram 6 weeks post-
operatively before any further decisions on future pregnancy.
3. Discussion
The incidence of uterine anomalies ranges between 0.5% and
2%. Unicornuate uterus (Type II) can further be classified as
those having an endometrial cavity and those with no endo-
metrial cavity, and 90% of the cases are those with an endo-
metrial cavity. A further division can be between the
communicating and non-communicating types. Identification
of unicornuate uterus is almost always accidental, as it is
usually asymptomatic until reproductive age. Initial presen-
tation often takes place with a recurrent first trimester
miscarriage (5e10%), a second trimester loss (25%), or during
an infertility work-out.4
Mariceau and Vassal published the first description of a
rudimentary horn pregnancy in 1669, and 600 cases have since
been described.5 Pregnancies occur in both communicating
and non-communicating horns in proportion to their relative
incidence and are equally likely to rupture. Neonatalmortality
is very high as most cases are emergency laparotomies after
uterine rupture at premature gestational age. Maternal mor-
tality is low (0.5%) but morbidity is very high in view of
massive blood loss and morbidly adherent placentation.2,6
In cases with successful pregnancy, the risks of recurrent
early trimester loss andmid-trimester loss are increased, with
preterm delivery and abnormal fetal lie contributing factors.
Pregnancy in a rudimentary horn is a form of ectopic
pregnancy and it can cause mortality or severe morbidity. It
can occur in both communicating and non-communicating
types. In the case of a non-communicating rudimentary
horn like our patient had, it is postulated that the fertilization
was possibly due to transperitoneal migration of the sperm.7
The outcomes of pregnancy in rudimentary horns are
ectopic pregnancy (2.7%), first trimester loss 24.3%, second
trimester abortion 9.7%, preterm delivery 20.1%, intrauterine
demise (10.5%) and 49.9% live birth up to 28e30 weeks of
gestation. Uterine rupture in the second trimester is usually a
life-threatening condition resulting from a much thinner myo-
metrial part of the rudimentary horn, with the non-functional
endometrium leading to placenta adherence anomalies.8
The prerupture diagnosis of pregnancy in rudimentary
horn has drastically reduced maternal mortality.7 But the
sensitivity of ultrasound to detect prerupture rudimentary
horn pregnancy is very poor (30%),8 probably because of rarity
of the diagnosis and non-familiarity of the radiologists about
this potentially lethal condition. Early diagnosis before
rupture can be managed laparoscopically.9
Prerupture diagnosis of rudimentary horn pregnancy is
challenging. A careful ultrasound in the first trimester with a
high index suspicion, one should be able to make a diagnosis
of pregnancy in the rudimentary horn and sensitivity de-
creases as the pregnancy advances.10 In such cases magnetic
resonance imaging (MRI) is very useful not only in confirming
the diagnosis, it also helps to plan the surgery.11 Tubal preg-
nancy, cornual pregnancy, and abdominal pregnancy are
common sonographic and clinical misdiagnosis. It is very
difficult to establish diagnosis in second trimester due to lack
of definitive clinical criteria.
Tsafrir et al. proposed the following criteria for ultrasono-
graphic diagnosis: 1. a pseudo pattern of an asymmetrical
bicornuate uterus, 2. absent visual continuity tissue sur-
rounding the gestation sac and the uterine cervix, and 3. the
presence of myometrial tissue surrounding the gestation sac.8
Three-dimensional ultrasound imaging and MRI are useful
tools in the improvement of diagnostic accuracy, guiding both
counseling and surgical planning.12
The traditional and established treatment for rudimentary
horn pregnancy is surgical removal of the pregnant horn even
in unruptured case to prevent rupture and recurrent rudi-
mentary horn pregnancy.13,14
Laparoscopic excision of the rudimentary horn pregnancy
prior to rupture has been done successfully since last two de-
cades.10,11 Renal anomalies are found in 36% of cases; hence it is
mandatory to assess these women prior to surgery and if
required better to doureterolysis before the excision of thehorn.
Medical management with methotrexate during early preg-
nancy in the rudimentary horn has also been used
successfully.14
In our patient, the diagnosis of ectopic pregnancy was only
established when she went into hypovolemic shock at 18
weeks. The non-communicating rudimentary horn rupture
was only confirmed intraoperatively and removal of the
rudimentary horn and ipsilateral fallopian tube was done.
This was to reduce the risk of the patient having another
ectopic pregnancy in the future.
This case further raises the question of whether routine
excision of rudimentary horn be undertaken in women with
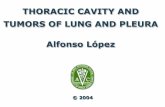
Fig. 2 e Site of perforation in right rudimentary horn.
a p o l l o m e d i c i n e x x x ( 2 0 1 3 ) 1e4 3
Please cite this article in press as: Elagwany AS, et al., Ruptured ectopic pregnancy in non-communicating right rudimentaryhorn: A case report, Apollo Medicine (2013), http://dx.doi.org/10.1016/j.apme.2013.10.002

unicornuate uterus as a prophylaxis to prevent such catas-
trophes. In our opinion, routine laparoscopic excision of
rudimentary horn with ipsilateral fallopian tube should be
offered to these women and those refusing should be
adequately counseled regarding the potential complications
and if pregnancy occurs in rudimentary horn first trimester
laparoscopic excision should be done.
4. Conclusion
Rudimentary horn pregnancy is a rare complication which
carries grave risk to the mother. More than 90% of the cases
present in second trimester with intraperitoneal hemorrhage
due to rupture of the horn. Ideally, history of repeated abor-
tions must be investigated before conception to exclude
Mullerian duct malformation. In addition, an intravenous
pyelogram is indicated because of high incidence of associ-
ated urinary anomalies in the presence of genital anomalies.
Diagnosis prior to rupture should be the concern in early
pregnancy with either ultrasound or MRI to prevent life-
threatening complications. The recent trend is to do laparo-
scopic excision of the rudimentary horn; laparotomy is still an
option when the patient is in shock.
Conflicts of interest
All authors have none to declare.
r e f e r e n c e s
1. Grimbizis GF, Camus M, Tarlatzis BC. Clinical implications ofuterine malformations and hysteroscopic treatment results.Hum Reprod Update. 2001;7:161e174.
2. Jayasinghe Y, Rane A, Stalewski H. The presentation and earlydiagnosis of the rudimentary uterine horn. Obstet Gynecol.2005;105:1456e1467.
3. Acien P. Incidence of Mullerian defects in fertile and infertilewomen. Hum Reprod. 1997;12:1372e1376.
4. Fitzmaurice LE, Ehsanipoor RM, Porto M. Rudimentary hornpregnancy with herniation into the main uterine cavity. Am JObstet Gynecol. 2010;202(3).
5. Chopra S, Keepanasseril A, Rohilla M. Obstetric morbidityand the diagnostic dilemma in pregnancy in rudimentaryhorn: retrospective analysis. Arch Gynecol Obstet.2009;280:907e910.
6. Lawhon BP, Wax JR, Dufort RT. Rudimentary uterine hornpregnancy diagnosed with magnetic resonance imaging.Obstet Gynecol. 1998;91(5 Pt 2):869.
7. Nahum GG. Rudimentary uterine horn pregnancy. The 20th-century worldwide experience of 588 cases. J Reprod Med.2002;47:151e163.
8. Tsafrir N, Rojansky HY, Sela J. Rudimentary horn pregnancy:first-trimester prerupture sonographic diagnosis andconfirmation by magnetic resonance imaging. J UltrasoundMed. 2005;24:219e223.
9. Yan CM. Laparoscopic management of three rare types ofectopic pregnancy. Hong Kong Med J. 2010;16:132e136.
10. Sharma D, Usha MG, Gaikwad R. Laparoscopic resection ofunruptured rudimentary horn pregnancy. Int J ReprodContracept Obstet Gynecol. 2013;2:95e98.
11. Edelman AB, Jensen JT, Lee DM. Successful medical abortionof a pregnancy within a noncommunicating rudimentaryuterine horn. Am J Obstet Gynecol. 2003;189:886e887.
12. Nahum G, Stanislaw H, McMohan C. Preventing ectopicpregnancies: how often does transperitoneal transmigrationof sperm occur in effecting human pregnancy? Br J ObstetGynecol. 2004;111:706e714.
13. Reichman D, Laufer MR, Robinson BK. Pregnancy outcomes inunicornuate uteri: a review. Fertil Steril. 2009;91:1886e1894.
14. Sunilkumar KS, Yaliwal LV, Amarnath A. Rupturedrudimentary horn of the unicornuate uterus at 16 weeks ofpregnancy: a case report. Int J Reprod Contracept Obstet Gynecol.2013;2:248e250.
a p o l l o m e d i c i n e x x x ( 2 0 1 3 ) 1e44
Please cite this article in press as: Elagwany AS, et al., Ruptured ectopic pregnancy in non-communicating right rudimentaryhorn: A case report, Apollo Medicine (2013), http://dx.doi.org/10.1016/j.apme.2013.10.002

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/