Rhinoscleroma in an Urban Non-endemic Setting€¦ · He was previously treated for allergic...
1
Poster Design & Printing by Genigraphics ® - 800.790.4001 Pavlina P. Suchanova, MD Bobby R. Alford Department of Otolaryngology-Head and Neck Surgery Email: [email protected] Phone: 713-798-7217 Website: www.bcm.edu/oto Objectives: To increase awareness and understanding of the clinical presentation, diagnosis and treatment options of respiratory rhinoscleroma among otolaryngologists in non- endemic areas. Review current literature, including our clinical experience, and propose a treatment algorithm for rhinoscleroma cases in a non-endemic setting. Study Design: Retrospective chart review of rhinoscleroma cases at Ben Taub General Hospital in Houston, Texas, from 1.1.2010 to 12.31.2010. Subjects and Methods: Report two cases of nasal and one case of laryngeal rhinoscleroma in an urban non-endemic setting in Ben Taub General Hospital in Houston, Texas. All patients presented in the spring of 2010 and were treated medically and /or surgically with an established follow up of more than 12 months. Results: Rhinoscleroma is a chronic, slowly progressive, infectious disease of the respiratory tract that is rare in non-endemic countries. Increased travel from endemic areas is increasing its incidence in a non-endemic setting and there is a need for an increased awareness of its clinical presentation and treatment options. The condition can easily mimic other pathology and, if untreated, lead to disfiguring nasal anatomy and laryngeal stenosis. No comprehensive review exists as many case reports are published in their respective native languages only. Conclusions: Treatment algorithm based on available literature review and our clinical experience is proposed with a full review of clinical presentation, diagnosis and the natural course of the disease, including its histopathology. Rhinoscleroma in an Urban Non Rhinoscleroma in an Urban Non - - endemic Setting endemic Setting Pavlina P. Suchanova, MD 1,3 ; Nadia G. Mohyuddin, MD 1,3 ; Susan A. Eicher, MD 1,3 ; Paul M. Rodriguez-Waitkus, MD/PhD 2,3 1 Bobby R. Alford Department of Otolaryngology-Head and Neck Surgery; 2 Department of Pathology and Immunology; 3 Ben Taub General Hospital, Houston, TX; Baylor College of Medicine Case 1 56-year-old female from Honduras, otherwise healthy, presented to our otolaryngology clinic in the spring of 2010 for an evaluation of a right sided thyroid nodule. A left fleshy nasal mass filling most of the inferior meatus was incidentally found on exam. Patient denied any nasal symptoms except for decreased nasal flow on the left. A biopsy taken in the clinic was consistent with rhinoscleroma on histopathology and patient was started on Sulfamethoxazole/ Trimethoprim (SMT/TMP) 500 mg twice daily for 6 months with a complete resolution of the lesion. She is currently scheduled for a right thyroid lobectomy with a possible total thyroidectomy for her multinodular goiter and will be followed closely . Case 2 35-year-old male from Mexico, otherwise healthy, presented to our otolaryngology clinic in the spring of 2010 with a 4 month history of right sided nasal obstruction with intermittent epistaxis. He was previously treated for allergic rhinitis by his primary care physician with nasal steroids and oral antihistamines but his symptoms did not improve with medical therapy. A large fleshy and friable nasal mass filling the right nasal cavity was seen on our head and neck exam. A biopsy taken in the clinic was consistent with rhinoscleroma on histopathology and CT sinus without contrast showed 4x2x3 cm right nasal soft tissue mass without bony erosion (Figure 1). Patient was started on Ciprofloxacin 500mg twice daily and had an interval improvement in size of the mass after 3 months of treatment both radiographically (Figure 2) and clinically (Figure 6). Limited surgical debridement followed by a total of 6 months of antibiotic therapy achieved a complete resolution of the lesion. Case 3 46-year-old female from El Salvador with a history of metastatic papillary thyroid carcinoma and laryngeal papillomas with several debridements in the past, presented with a history of worsening hoarseness for several years. Direct laryngoscopy in the operating room revealed multiple polypoid like lesions in the supraglottis and glottis (Figure 7) with biopsy results consistent with rhinoscleroma. Patient was treated with a total of 6 months of antibiotic therapy with Sulfamethoxazole/ Trimethoprim and then Ciprofloxacin (changed due to right arm dysesthesias) with a complete resolution of all lesions. Even though respiratory scleroma is a rare diagnosis in the US, with the increasing travel and influx of immigrant population from endemic areas, there is an increase in its incidence in the non-endemic areas. Lack of awareness when disease presents in developed countries often leads to delay in diagnosis and can cause nasal deformities, airway obstruction and symptoms mimicking allergic rhinitis and prolonged sinusitis. The disease process usually involves the nasal cavity and nasopharynx, but it can also infect the larynx, trachea, middle ear or the orbit. 3 The first “catarrhal” exudative stage of disease progression causes nonspecific rhinitis/sinusitis symptoms with rhinorrhea, usually foul smelling and purulent, which persist for months. There could also be nasal obstruction, crusting and atrophic mucosal changes. Histological examination will reveal an evidence of squamous metaplasia, a subepithelial infiltrate of neutrophils and mild granulation tissue. Further crusting and nasal obstruction with intermittent epistaxis, hoarseness in laryngeal involvement, develop as the disease enters the second “granulomatous” stage. Histology exam shows pseudo-epitheliomatous hyperplasia with pathognomonic Mikulitz cells with viable or nonviable bacilli, Russell bodies - nonspecific accumulations of hyaline degeneration in the cytoplasm of plasma cells (Figure 5). Extensive scarring and nasal/laryngeal stenosis characterize the third “sclerotic” stage 4 . Histopathology examination confirms the diagnosis and management with long-term antibiotics (3-6 months) with the least side effects (Ciprofloxacin, Sulfamethoxazole/Trimethoprim) +/- surgical debridement with bulk disease are the mainstay of therapy, even though no randomized controlled trials exist to compare various treatment choices and their efficacy. 5 Long term follow up is vital due to high relapse rates up to 41% 6 . Retrospective chart review of rhinoscleroma cases at Ben Taub General Hospital in Houston, Texas, from 1.1.2010 to 12.31.2010 was performed. Institutional Review Board approval for Human Subject Research for Baylor College of Medicine and Affiliated Hospitals was obtained. We report 2 cases of nasal rhinoscleroma and one case of laryngeal rhinoscleroma in an urban non-endemic setting at Ben Taub General Hospital in Houston, Texas. Geographically, all patients were originally from endemic areas - El Salvador, Honduras and Mexico, and presented to our otolaryngology clinic in the spring of 2010. Two patients were female and the third patient was male. Their ages at presentation ranged from 35 to 56 years old. They were treated medically and/or surgically with an established follow up of more than 12 months. Rhinoscleroma is a chronic granulomatous disease caused by a coccobacillus Klebsiella rhinoscleromatis , affecting the respiratory tract and predominantly nasal cavity. It is endemic to areas of Europe, Central and South America, Africa and Middle East but increasing travel and immigration lead to an increasing incidence in non-endemic areas. Lack of awareness when disease presents in developed countries often leads to delay in diagnosis and can cause nasal deformities, airway obstruction and symptoms mimicking prolonged sinusitis. Management with long-term antibiotics with the least side effects (Ciprofloxacin, SMT/TMP) +/- surgical debridement/dilation/CO2 laser. Long term follow up is vital because relapses are common. Rhinoscleroma is a chronic , slowly progressive, granulomatous infection of the respiratory tract due to an encapsulated and nonmotile gram negative coccobacillus called Klebsiella rhiscleromatis . It is sometimes referred to as the "Frisch bacillus," named for Anton von Frisch, an Austrian urologist, who identified the organism in 1882. In his original description in 1870, Hans von Hebra – a Czech born dermatologist , thought this disease to be a neoplastic process, and coined the term rhinoscleroma. 1 It was also known as the “nasal leprosy of the Slavics”, “exuberant syphilis of the nose” and the “Hebra Nose”. In 1877, Mikulicz -a Polish pathologist, described the histological features of this disease in detail and established its nonneoplastic inflammatory nature. The “Mikulitz cells”, large foamy macrophages with intracellular coccobacilli (Figure 3) became pathognomonic. The bacilli are easily identifiable on silver stains (Figure 4). Rhinoscleroma is endemic to Central America , Egypt, tropical Africa, Indonesia, Eastern Europe and India. 2 If left untreated, it can lead to disfiguring nasal anatomy and laryngeal stenosis. Increased travel from endemic areas is increasing its incidence in a non-endemic setting and there is a need for an increased awareness of its clinical presentation, diagnosis and treatment options among practicing otolaryngologists. INTRODUCTION METHODS AND MATERIALS 1. Von Hebra F. Uber ein eigenthumliches neugebilde an der nase: rhinosklerom. Wien Med Wochenschr. 1870;20:1-5. 2. Miller RH, Shulman JB, Canalis RF, Ward PH. Klebsiella Rhinoscleromatis: a Clinical and Pathogenic Enigma. Otolaryngol Head Neck Surg. 1979;87:212-221. 3. Bhowate RR, Degwekar S, Rawlani S, Dangore S. Rhinoscleroma with Involvement of the Maxillary Sinus, Orbital Floor, and Temporomandibular Joint: A Case Report. J Oral Maxillofac Surg. 2011; article in the press. 4. Zhong Q, Guo W, Chen X, Ni X, et al. Rhinoscleroma: A Retrospective Study of Pathologic and Clinical Features. Otolaryngol Head Neck Surg. 2011;40:167-174. 5. N’gattia KV, Kacouchia N, Koffi-N’guessan L, Mobio NM, et al. Retrospective Study of the Rhinoscleroma about 14 cases in ENT Departments of University Hospitals. Europ Ann Otorhinolaryngol. 2011;128:7-10. 6. Fawaz S, Tiba M, Salman M, Othman H. Clinical, Radiological and Pathological Study of 88 of Typical and Complicated scleroma. Clinic Respir J. 2011;5:112-121. CONCLUSIONS RESULTS SELECTED REFERENCES Figure 2. Post-treatment CT sinus without contrast, axial. Figure 1. Pre-treatment CT sinus without contrast, axial. ABSTRACT ABSTRACT CONT ACT CONT ACT DISCUSSION Figure 7. Laryngeal lesions and anterior webbing pre and post – surgical debridement. Figure 6. Right nasal mass after 3 months of antibiotic treatment. Figure 5. Russell bodies. HE /100X. Figure 3. Mikulitz cells with intracellular bacilli . HE ,100X. Figure 4. Mikulitz cells with intracellular gram negative bacilli . Steiner silver stain, 100X.
-
Upload
truongcong -
Category
Documents
-
view
216 -
download
3
Transcript of Rhinoscleroma in an Urban Non-endemic Setting€¦ · He was previously treated for allergic...
Poster Design & Printing by Genigraphics® - 800.790.4001
Pavlina P. Suchanova, MD Bobby R. Alford Department of Otolaryngology-Head and Neck SurgeryEmail: [email protected]: 713-798-7217Website: www.bcm.edu/oto
Objectives: To increase awareness and understanding of the clinical presentation, diagnosis and treatment options of respiratory rhinoscleroma among otolaryngologists in non-endemic areas. Review current literature, including our clinical experience, and propose a treatment algorithm for rhinoscleroma cases in a non-endemic setting.
Study Design: Retrospective chart review of rhinoscleroma cases at Ben Taub General Hospital in Houston, Texas, from 1.1.2010 to 12.31.2010.
Subjects and Methods: Report two cases of nasal and one case of laryngeal rhinoscleroma in an urban non-endemic setting in Ben TaubGeneral Hospital in Houston, Texas. All patients presented in the spring of 2010 and were treated medically and /or surgically with an established follow up of more than 12 months.
Results: Rhinoscleroma is a chronic, slowly progressive, infectious disease of the respiratory tract that is rare in non-endemic countries. Increased travel from endemic areas is increasing its incidence in a non-endemic setting and there is a need for an increased awareness of its clinical presentation and treatment options. The condition can easily mimic other pathology and, if untreated, lead to disfiguring nasal anatomy and laryngeal stenosis. No comprehensive review exists as many case reports are published in their respective native languages only.
Conclusions: Treatment algorithm based on available literature review and our clinical experience is proposed with a full review of clinical presentation, diagnosis and the natural course of the disease, including its histopathology.
Rhinoscleroma in an Urban NonRhinoscleroma in an Urban Non--endemic Settingendemic SettingPavlina P. Suchanova, MD1,3; Nadia G. Mohyuddin, MD1,3; Susan A. Eicher, MD 1,3; Paul M. Rodriguez-Waitkus, MD/PhD 2,3
1Bobby R. Alford Department of Otolaryngology-Head and Neck Surgery; 2 Department of Pathology and Immunology;3Ben Taub General Hospital, Houston, TX; Baylor College of Medicine
Case 156-year-old female from Honduras, otherwise healthy, presented to our otolaryngology clinic in the spring of 2010 for an evaluation of a right sided thyroid nodule. A left fleshy nasal mass filling most of the inferior meatus was incidentally found on exam. Patient denied any nasal symptoms except for decreased nasal flow on the left. A biopsy taken in the clinic was consistent with rhinoscleroma on histopathology and patient was started on Sulfamethoxazole/ Trimethoprim (SMT/TMP) 500 mg twice daily for 6 months with a complete resolution of the lesion. She is currently scheduled for a right thyroid lobectomy with a possible total thyroidectomy for her multinodular goiter and will be followed closely .
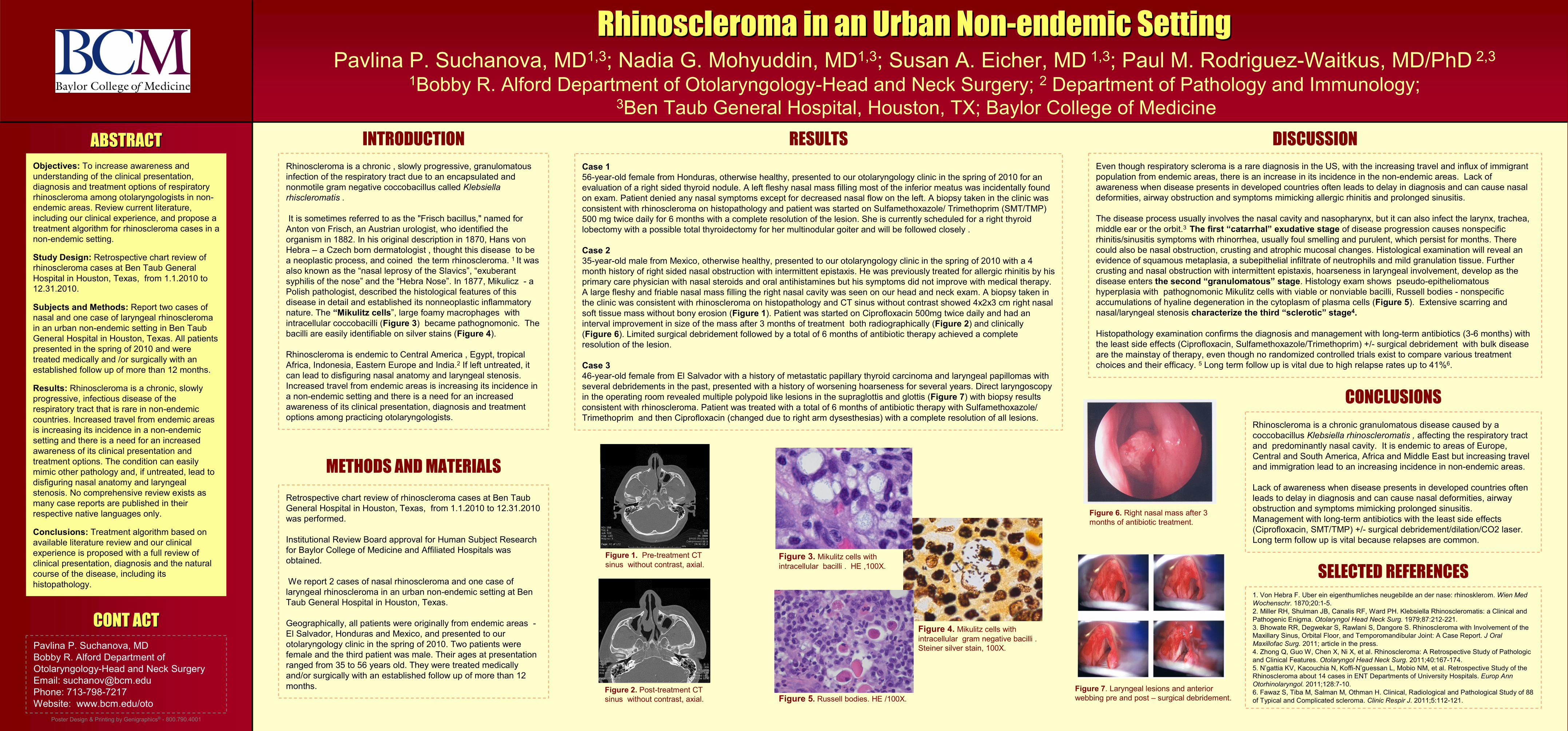
Case 235-year-old male from Mexico, otherwise healthy, presented to our otolaryngology clinic in the spring of 2010 with a 4 month history of right sided nasal obstruction with intermittent epistaxis. He was previously treated for allergic rhinitis by his primary care physician with nasal steroids and oral antihistamines but his symptoms did not improve with medical therapy. A large fleshy and friable nasal mass filling the right nasal cavity was seen on our head and neck exam. A biopsy taken in the clinic was consistent with rhinoscleroma on histopathology and CT sinus without contrast showed 4x2x3 cm right nasal soft tissue mass without bony erosion (Figure 1). Patient was started on Ciprofloxacin 500mg twice daily and had an interval improvement in size of the mass after 3 months of treatment both radiographically (Figure 2) and clinically (Figure 6). Limited surgical debridement followed by a total of 6 months of antibiotic therapy achieved a complete resolution of the lesion.
Case 346-year-old female from El Salvador with a history of metastatic papillary thyroid carcinoma and laryngeal papillomas with several debridements in the past, presented with a history of worsening hoarseness for several years. Direct laryngoscopy in the operating room revealed multiple polypoid like lesions in the supraglottis and glottis (Figure 7) with biopsy results consistent with rhinoscleroma. Patient was treated with a total of 6 months of antibiotic therapy with Sulfamethoxazole/ Trimethoprim and then Ciprofloxacin (changed due to right arm dysesthesias) with a complete resolution of all lesions.
Even though respiratory scleroma is a rare diagnosis in the US, with the increasing travel and influx of immigrant population from endemic areas, there is an increase in its incidence in the non-endemic areas. Lack of awareness when disease presents in developed countries often leads to delay in diagnosis and can cause nasal deformities, airway obstruction and symptoms mimicking allergic rhinitis and prolonged sinusitis.
The disease process usually involves the nasal cavity and nasopharynx, but it can also infect the larynx, trachea, middle ear or the orbit.3 The first “catarrhal” exudative stage of disease progression causes nonspecific rhinitis/sinusitis symptoms with rhinorrhea, usually foul smelling and purulent, which persist for months. There could also be nasal obstruction, crusting and atrophic mucosal changes. Histological examination will reveal an evidence of squamous metaplasia, a subepithelial infiltrate of neutrophils and mild granulation tissue. Further crusting and nasal obstruction with intermittent epistaxis, hoarseness in laryngeal involvement, develop as the disease enters the second “granulomatous” stage. Histology exam shows pseudo-epitheliomatous hyperplasia with pathognomonic Mikulitz cells with viable or nonviable bacilli, Russell bodies - nonspecific accumulations of hyaline degeneration in the cytoplasm of plasma cells (Figure 5). Extensive scarring and nasal/laryngeal stenosis characterize the third “sclerotic” stage4.
Histopathology examination confirms the diagnosis and management with long-term antibiotics (3-6 months) with the least side effects (Ciprofloxacin, Sulfamethoxazole/Trimethoprim) +/- surgical debridement with bulk disease are the mainstay of therapy, even though no randomized controlled trials exist to compare various treatment choices and their efficacy. 5 Long term follow up is vital due to high relapse rates up to 41%6.
Retrospective chart review of rhinoscleroma cases at Ben TaubGeneral Hospital in Houston, Texas, from 1.1.2010 to 12.31.2010was performed.
Institutional Review Board approval for Human Subject Research for Baylor College of Medicine and Affiliated Hospitals was obtained.
We report 2 cases of nasal rhinoscleroma and one case of laryngeal rhinoscleroma in an urban non-endemic setting at Ben Taub General Hospital in Houston, Texas.
Geographically, all patients were originally from endemic areas -El Salvador, Honduras and Mexico, and presented to our otolaryngology clinic in the spring of 2010. Two patients were female and the third patient was male. Their ages at presentation ranged from 35 to 56 years old. They were treated medically and/or surgically with an established follow up of more than 12 months.
Rhinoscleroma is a chronic granulomatous disease caused by a coccobacillus Klebsiella rhinoscleromatis , affecting the respiratory tract and predominantly nasal cavity. It is endemic to areas of Europe, Central and South America, Africa and Middle East but increasing travel and immigration lead to an increasing incidence in non-endemic areas.
Lack of awareness when disease presents in developed countries often leads to delay in diagnosis and can cause nasal deformities, airway obstruction and symptoms mimicking prolonged sinusitis. Management with long-term antibiotics with the least side effects (Ciprofloxacin, SMT/TMP) +/- surgical debridement/dilation/CO2 laser. Long term follow up is vital because relapses are common.
Rhinoscleroma is a chronic , slowly progressive, granulomatous infection of the respiratory tract due to an encapsulated and nonmotile gram negative coccobacillus called Klebsiella rhiscleromatis .
It is sometimes referred to as the "Frisch bacillus," named forAnton von Frisch, an Austrian urologist, who identified the organism in 1882. In his original description in 1870, Hans von Hebra – a Czech born dermatologist , thought this disease to be a neoplastic process, and coined the term rhinoscleroma. 1 It was also known as the “nasal leprosy of the Slavics”, “exuberant syphilis of the nose” and the “Hebra Nose”. In 1877, Mikulicz - a Polish pathologist, described the histological features of this disease in detail and established its nonneoplastic inflammatorynature. The “Mikulitz cells”, large foamy macrophages with intracellular coccobacilli (Figure 3) became pathognomonic. The bacilli are easily identifiable on silver stains (Figure 4).
Rhinoscleroma is endemic to Central America , Egypt, tropical Africa, Indonesia, Eastern Europe and India.2 If left untreated, it can lead to disfiguring nasal anatomy and laryngeal stenosis. Increased travel from endemic areas is increasing its incidence in a non-endemic setting and there is a need for an increased awareness of its clinical presentation, diagnosis and treatment options among practicing otolaryngologists.
INTRODUCTION
METHODS AND MATERIALS
1. Von Hebra F. Uber ein eigenthumliches neugebilde an der nase: rhinosklerom. Wien Med Wochenschr. 1870;20:1-5.2. Miller RH, Shulman JB, Canalis RF, Ward PH. Klebsiella Rhinoscleromatis: a Clinical and Pathogenic Enigma. Otolaryngol Head Neck Surg. 1979;87:212-221.3. Bhowate RR, Degwekar S, Rawlani S, Dangore S. Rhinoscleroma with Involvement of the Maxillary Sinus, Orbital Floor, and Temporomandibular Joint: A Case Report. J Oral Maxillofac Surg. 2011; article in the press. 4. Zhong Q, Guo W, Chen X, Ni X, et al. Rhinoscleroma: A Retrospective Study of Pathologic and Clinical Features. Otolaryngol Head Neck Surg. 2011;40:167-174.5. N’gattia KV, Kacouchia N, Koffi-N’guessan L, Mobio NM, et al. Retrospective Study of the Rhinoscleroma about 14 cases in ENT Departments of University Hospitals. Europ Ann Otorhinolaryngol. 2011;128:7-10.6. Fawaz S, Tiba M, Salman M, Othman H. Clinical, Radiological and Pathological Study of 88 of Typical and Complicated scleroma. Clinic Respir J. 2011;5:112-121.
CONCLUSIONS
RESULTS
SELECTED REFERENCES
Figure 2. Post-treatment CTsinus without contrast, axial.
Figure 1. Pre-treatment CTsinus without contrast, axial.
ABSTRACTABSTRACT
CONT ACTCONT ACT
DISCUSSION
Figure 7. Laryngeal lesions and anterior webbing pre and post – surgical debridement.
Figure 6. Right nasal mass after 3 months of antibiotic treatment.
Figure 5. Russell bodies. HE /100X.
Figure 3. Mikulitz cells with intracellular bacilli . HE ,100X.
Figure 4. Mikulitz cells with intracellular gram negative bacilli . Steiner silver stain, 100X.