
Atrophic Rhinitis Slides 050330
32
Atrophic Atrophic Rhinitis Rhinitis UTMB Dept of Otolaryngology UTMB Dept of Otolaryngology March 30, 2005 March 30, 2005 Alan L. Cowan, M.D. Alan L. Cowan, M.D. Matthew Ryan, M.D. Matthew Ryan, M.D.
-
Upload
dansrirahmadani -
Category
Documents
-
view
39 -
download
2
description
rinitis
Transcript of Atrophic Rhinitis Slides 050330
Atrophic RhinitisAtrophic RhinitisUTMB Dept of OtolaryngologyUTMB Dept of Otolaryngology
March 30, 2005March 30, 2005
Alan L. Cowan, M.D.Alan L. Cowan, M.D.
Matthew Ryan, M.D.Matthew Ryan, M.D.
Atrophic RhinitisAtrophic Rhinitis
Common TermsCommon Terms OzenaOzena Dry RhinitisDry Rhinitis Rhinitis SiccaRhinitis Sicca
Atrophic RhinitisAtrophic Rhinitis Dr. Spencer Watson. Dr. Spencer Watson. Diseases of the nose and its Diseases of the nose and its
associated cavitiesassociated cavities. London, 1875.. London, 1875. 1) Accidental or Simple Ozoena1) Accidental or Simple Ozoena
““due to the retention of mucous.”due to the retention of mucous.” ““easily dealt with by the frequent employment of the nasal easily dealt with by the frequent employment of the nasal
douche …”douche …” 2) Idiopathic or constitutional2) Idiopathic or constitutional
““commences in early childhood ... And remains during the commences in early childhood ... And remains during the early years or throughout the whole adult life.”early years or throughout the whole adult life.”
““The patient is generally anosmic … and he is, therefore, The patient is generally anosmic … and he is, therefore, unaware of the offensive odor of his breath.”unaware of the offensive odor of his breath.”
““The nature of the inflammatory process is very probably The nature of the inflammatory process is very probably allied to that of lupus erythematosus of the face.”allied to that of lupus erythematosus of the face.”
3) Syphilitic Ozoena3) Syphilitic Ozoena ““the most common form”the most common form” ““These ulcers may be preceded or followed by caries or These ulcers may be preceded or followed by caries or
necrosis of the bones, and the stench is then more horribly necrosis of the bones, and the stench is then more horribly sickening than in any other form of this disgusting malady.”sickening than in any other form of this disgusting malady.”
Atrophic RhinitisAtrophic Rhinitis
Described in 1876 by Dr. Bernhard Fraenkel Described in 1876 by Dr. Bernhard Fraenkel as a triad of:as a triad of: FetorFetor CrustingCrusting Atrophy of nasal structuresAtrophy of nasal structures
Dr. Francke Bosworth. Dr. Francke Bosworth. A Manual of Diseases A Manual of Diseases of the Nose and Throat.of the Nose and Throat. 1881. 1881. ““the breath is often so penetrating as to render the breath is often so penetrating as to render
the near presence of the sufferer not only the near presence of the sufferer not only unpleasant but almost unendurable.”unpleasant but almost unendurable.”
Atrophic RhinitisAtrophic Rhinitis
Clinical FeaturesClinical Features AnosmiaAnosmia Ozena, i.e. foul odorOzena, i.e. foul odor Extensive nasal crustingExtensive nasal crusting Subjective nasal congestionSubjective nasal congestion Enlargement of the nasal cavityEnlargement of the nasal cavity Resorption or absence of turbinatesResorption or absence of turbinates Squamous metaplasia of nasal mucosaSquamous metaplasia of nasal mucosa DepressionDepression
Atrophic rhinitisAtrophic rhinitis
PrimaryPrimary History of prior sinus surgery, radiation, History of prior sinus surgery, radiation,
granulomatous disease, or nasal trauma are granulomatous disease, or nasal trauma are exclusions.exclusions.
Primary AR is rare in the USPrimary AR is rare in the US Most cases are reported in China, Egypt, and IndiaMost cases are reported in China, Egypt, and India Microbiology of primary AR is almost uniformly Microbiology of primary AR is almost uniformly
Klebsiella ozenaeKlebsiella ozenae.. Radiographic and clinical features similar to Radiographic and clinical features similar to
secondary AR.secondary AR.
Atrophic rhinitisAtrophic rhinitis
SecondarySecondary Complication of sinus surgery (89%)Complication of sinus surgery (89%) Complication of radiation (2.5%)Complication of radiation (2.5%) Following nasal trauma (1%)Following nasal trauma (1%) Sequela of granulomatous diseases (1%)Sequela of granulomatous diseases (1%)
SarcoidSarcoid LeprosyLeprosy RhinoscleromaRhinoscleroma
Sequlae of other infectious processesSequlae of other infectious processes TuberculosisTuberculosis SyphilisSyphilis
Moore & Kern. Amer J Rhin. 2001 15(6): 355-361.
Surgical causesSurgical causes
Based on review of 242 cases from Mayo Based on review of 242 cases from Mayo Clinic.Clinic. Procedures per patientProcedures per patient
2.32.3 Partial middle or inferior turbinectomyPartial middle or inferior turbinectomy
56%56% Total middle and inferior turbinectomyTotal middle and inferior turbinectomy
24%24% No turbinectomyNo turbinectomy
10%10% Partial maxillectomyPartial maxillectomy
6%6%
Moore & Kern. Amer J Rhin. 2001 15(6): 355-361.
Other suggested causesOther suggested causes Infectious (Ssali)Infectious (Ssali)
Case report of AR developed in 7 children of one family after contact with Case report of AR developed in 7 children of one family after contact with another known AR child.another known AR child.
Dietary Dietary (Bernat) Iron therapy found to benefit 50% of patients treated(Bernat) Iron therapy found to benefit 50% of patients treated (Han-Sen) Hypocholesterolemia present in 50% of patients.(Han-Sen) Hypocholesterolemia present in 50% of patients. (Han-Sen) Vitamin A therapy showed symptomatic improvement in 84%.(Han-Sen) Vitamin A therapy showed symptomatic improvement in 84%.
Hereditary (Barton, Sibert)Hereditary (Barton, Sibert) Proposed autosomal dominant disease due to father and 8 of 15 children Proposed autosomal dominant disease due to father and 8 of 15 children
contracting the disease.contracting the disease. Hormonal Hormonal
Symptoms known to worsen with menstraution or pregnancy.Symptoms known to worsen with menstraution or pregnancy. Developmental (Hagrass)Developmental (Hagrass)
Radiologic evidence of poor maxillary antrum pneumatization and short nasal Radiologic evidence of poor maxillary antrum pneumatization and short nasal lengthslengths
Vascular (Ruskin)Vascular (Ruskin) Postulated overactivation of sympathetic activity.Postulated overactivation of sympathetic activity.
Environmental (Mickiewicz)Environmental (Mickiewicz) Chronic exposure to phosphorite and apatide dustChronic exposure to phosphorite and apatide dust
Autoimmune (Ricci)Autoimmune (Ricci)
Physical findingsPhysical findings Crusting Crusting
100% Present100% Present Inferior TurbinatesInferior Turbinates
62% Partial absence62% Partial absence 37% Total absence37% Total absence
Middle TurbinatesMiddle Turbinates 57% Absent57% Absent
Discharge Discharge 52% Present52% Present
SeptumSeptum 10% Perforations10% Perforations
Moore & Kern. Amer J Rhin. 2001 15(6): 355-361.
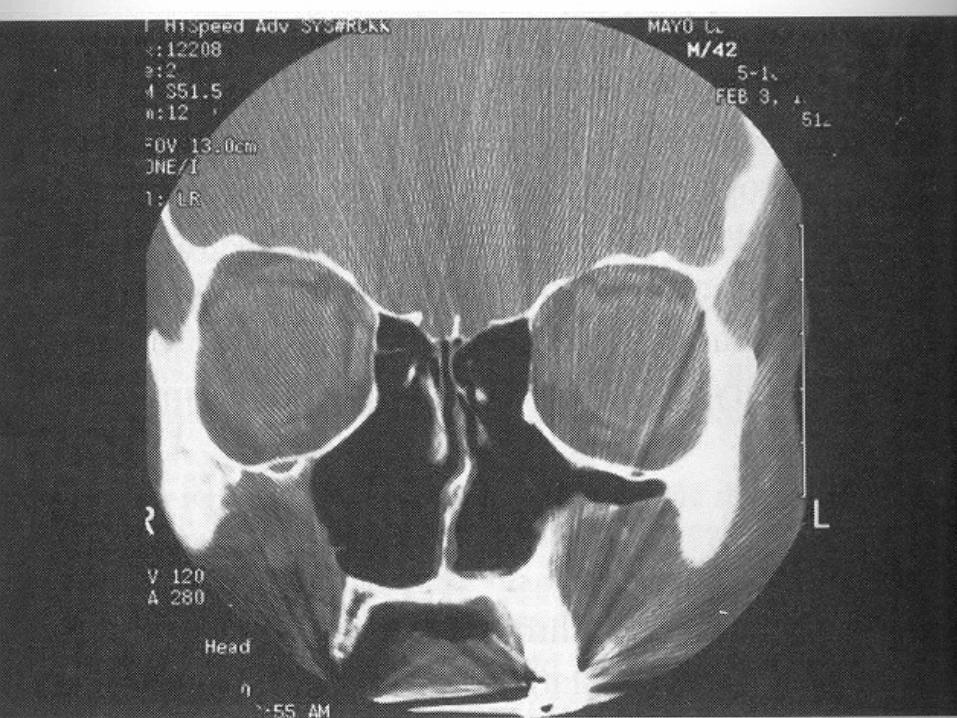
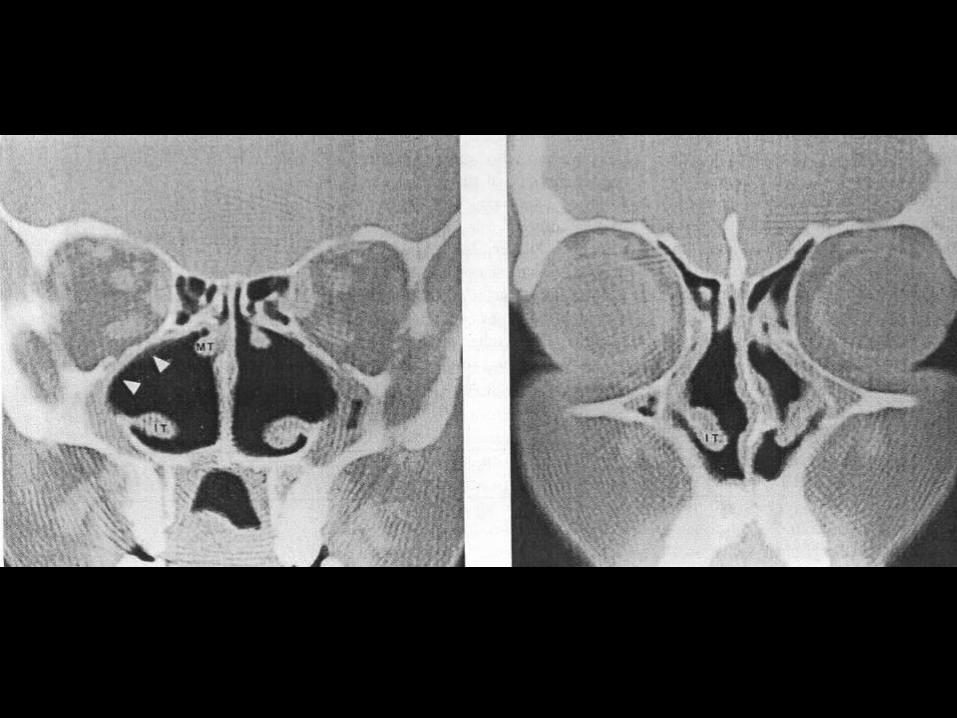
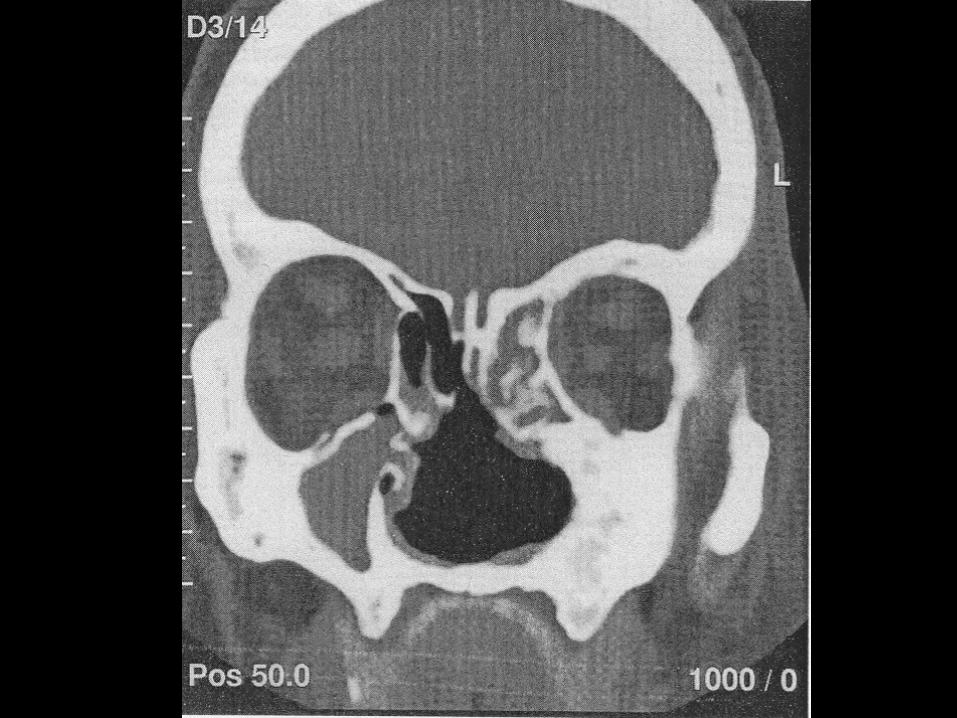
Radiographic FindingsRadiographic Findings
1.1. Mucoperiosteal thickening of the paranasal sinuses.Mucoperiosteal thickening of the paranasal sinuses.
2.2. Loss of definition of the OMC secondary to resorption Loss of definition of the OMC secondary to resorption of the ethmoid bulla and uncinate process.of the ethmoid bulla and uncinate process.
3.3. Hypoplasia of the maxillary sinuses.Hypoplasia of the maxillary sinuses.
4.4. Enlargement of the nasal cavities with erosion Enlargement of the nasal cavities with erosion and bowing of the lateral nasal wall.and bowing of the lateral nasal wall.
5.5. Bony resorption and mucosal atrophy of the inferior Bony resorption and mucosal atrophy of the inferior and middle turbinates.and middle turbinates.
Pace-Balzan, Shankar, Hawke. J Otolaryngol 1991; 20:428-32.
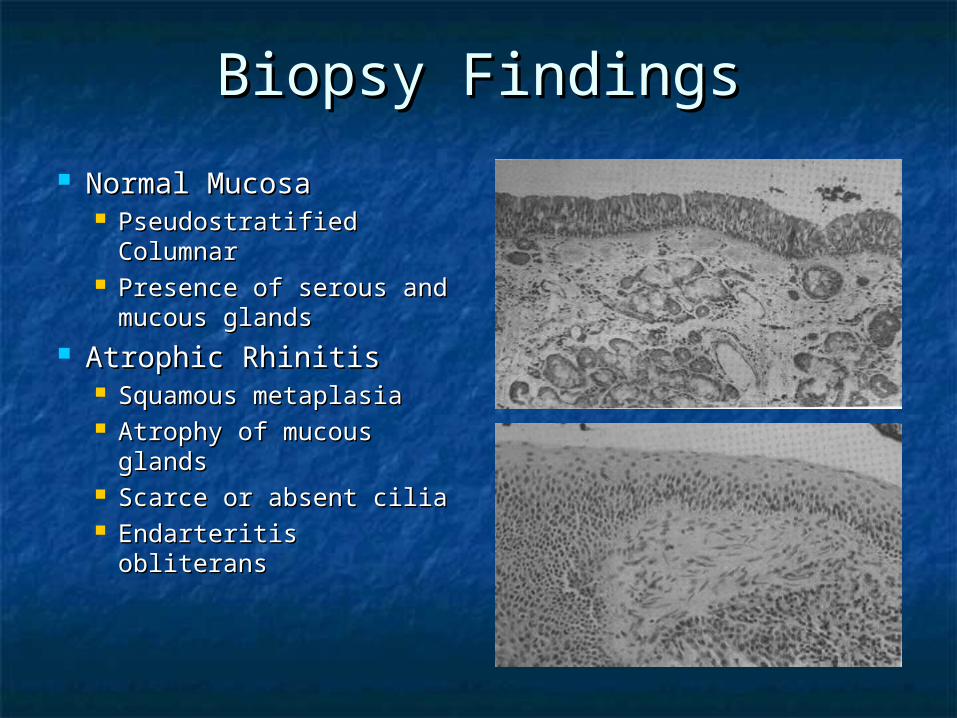
Biopsy FindingsBiopsy Findings
Normal MucosaNormal Mucosa Pseudostratified Pseudostratified
ColumnarColumnar Presence of serous and Presence of serous and
mucous glandsmucous glands Atrophic RhinitisAtrophic Rhinitis
Squamous metaplasiaSquamous metaplasia Atrophy of mucous Atrophy of mucous
glandsglands Scarce or absent ciliaScarce or absent cilia Endarteritis obliteransEndarteritis obliterans
MicrobiologyMicrobiology
Klebsiella ozenaeKlebsiella ozenae May be found in almost 100% of primary May be found in almost 100% of primary
ARAR No predominance in secondary ARNo predominance in secondary AR
Staphylococcus aureusStaphylococcus aureus Proteus mirabilisProteus mirabilis Escherichia coliEscherichia coli Corynebacterium diphtheriaeCorynebacterium diphtheriae
Current TherapiesCurrent Therapies
Goals of therapyGoals of therapy Restore nasal hydrationRestore nasal hydration Minimize crusting and debrisMinimize crusting and debris
Therapy optionsTherapy options Topical therapyTopical therapy Saline irrigationsSaline irrigations Antibiotic irrigationsAntibiotic irrigations Systemic antibioticsSystemic antibiotics Implants to fill nasal volumeImplants to fill nasal volume Closure of the nostrilsClosure of the nostrils
Local therapyLocal therapy IrrigationsIrrigations
SalineSaline MixturesMixtures
Sodium bicarbonateSodium bicarbonate Shehata: Sodium Carbonate 25g, Sodium Biborate 25g, and Shehata: Sodium Carbonate 25g, Sodium Biborate 25g, and
Sodium Chloride 50g in 250ml water.Sodium Chloride 50g in 250ml water. Antibiotic solutionAntibiotic solution
Moore: Gentamycin solution 80mg/LMoore: Gentamycin solution 80mg/L Anti-drying agentsAnti-drying agents
GlycerineGlycerine Mineral OilMineral Oil Paraffin with 2% MentholParaffin with 2% Menthol
OtherOther AcetylcholineAcetylcholine PilocarpinePilocarpine
Systemic therapySystemic therapy
Oral antibioticsOral antibiotics TetracyclineTetracycline CiprofloxacinCiprofloxacin AminoglycosidesAminoglycosides Streptomycin injectionsStreptomycin injections
Medication avoidanceMedication avoidance VasoconstrictorsVasoconstrictors Topical steroids *Topical steroids *
OtherOther Vitamin A (12,500 to 15,000 Units daily)Vitamin A (12,500 to 15,000 Units daily) Potassium Iodide (Increases nasal secretions)Potassium Iodide (Increases nasal secretions) VasodilatorsVasodilators Iron therapyIron therapy EstrogenEstrogen Corticosteroids *Corticosteroids *
VaccinesVaccines Antibacterial (Pasturella, Bordetella)Antibacterial (Pasturella, Bordetella) Autogenous Autogenous
Surgical therapiesSurgical therapies
Young procedureYoung procedure Modified Young procedureModified Young procedure Turbinate reconstructionTurbinate reconstruction Volume reduction proceduresVolume reduction procedures Denervating operationsDenervating operations
Nasal ClosureNasal Closure
Young’s procedureYoung’s procedure Circumferential flap elevation 1 cm cephalic to the alar Circumferential flap elevation 1 cm cephalic to the alar
rim.rim. Sutures placed in center of elevated flap to close the Sutures placed in center of elevated flap to close the
nostrilnostril Staged second side in 3 monthsStaged second side in 3 months
AdvantagesAdvantages Often provided relief of symptomsOften provided relief of symptoms
DisadvantagesDisadvantages Difficult to elevate circumferential flapDifficult to elevate circumferential flap Breakdown of central suture area commonBreakdown of central suture area common Does not allow for cleaningDoes not allow for cleaning Did not allow for periodic examinationDid not allow for periodic examination Recurrence after flap takedownRecurrence after flap takedownYoung. “Closure of the nostril in atrophic rhinitis.” Journal of
Laryngology and Otology, 81: 515-524.
Nasal ClosureNasal Closure Modified Young’sModified Young’s
Elevation of extended perichondrial flap through Elevation of extended perichondrial flap through contralateral hemitransfixion incision.contralateral hemitransfixion incision.
Short skin flap elevated from the intercartilaginous line Short skin flap elevated from the intercartilaginous line on the ipsilateral side.on the ipsilateral side.
Suture lateral and medial flaps with vicryl.Suture lateral and medial flaps with vicryl. Staged second side with first side takedown in 6 mon.Staged second side with first side takedown in 6 mon.
AdvantagesAdvantages Technically easier than Young procedureTechnically easier than Young procedure No suture line breakdownNo suture line breakdown No vestibular stenosis on takedownNo vestibular stenosis on takedown
DisadvantagesDisadvantages Not possible with large septal defectsNot possible with large septal defects Does not allow for cleaningDoes not allow for cleaning Does not allow for periodic examinationDoes not allow for periodic examination Recurrence after flap takedownRecurrence after flap takedown
El Kholy, Habib, Abdel-Monem, Safia. “Septal mucoperichondrial flap for El Kholy, Habib, Abdel-Monem, Safia. “Septal mucoperichondrial flap for closure of nostril in atrophic rhinitis.” Rhinology, 36, 202-203, 1998.closure of nostril in atrophic rhinitis.” Rhinology, 36, 202-203, 1998.
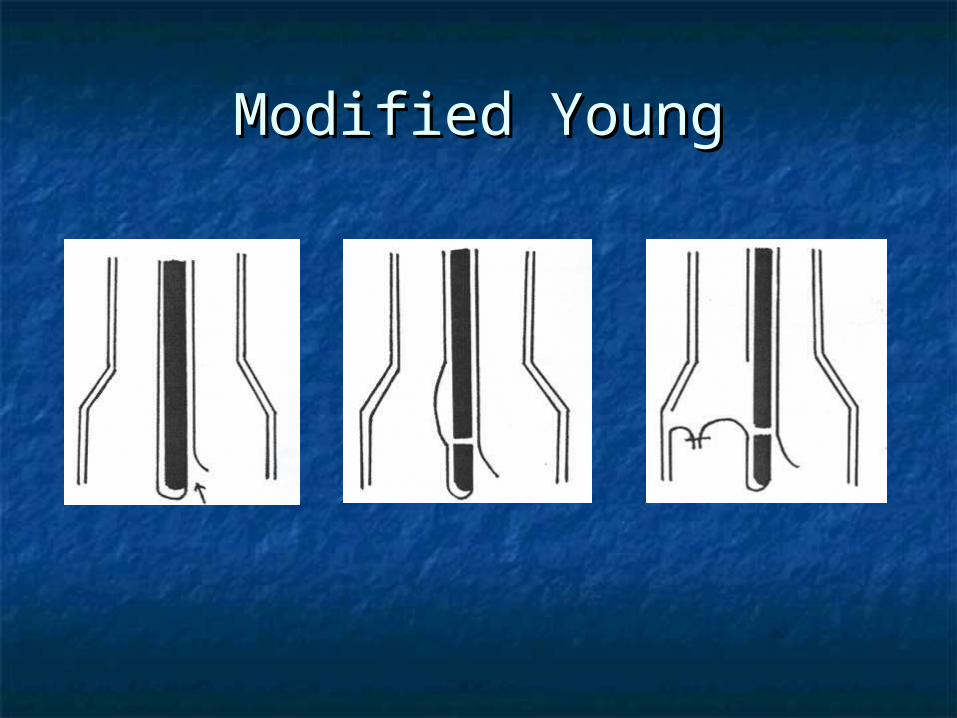
Modified YoungModified Young
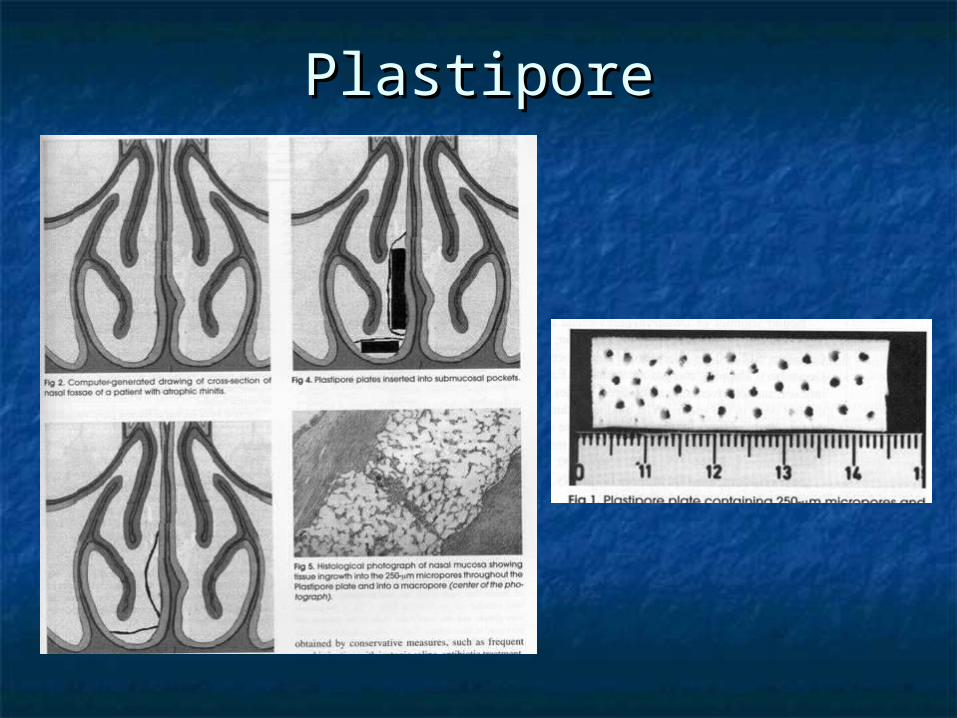
Volume reductionVolume reduction Plastipore implantationPlastipore implantation
Porus material allows tissue ingrowth.Porus material allows tissue ingrowth. Implants shaped then fenestrated for ingrowth.Implants shaped then fenestrated for ingrowth. Implants placed submucosally along the septum Implants placed submucosally along the septum
and nasal floor.and nasal floor. AdvantagesAdvantages
Easier than other surgical options (Young’s)Easier than other surgical options (Young’s) Plastipore has low extrusion/complication ratePlastipore has low extrusion/complication rate May be done under local anesthesiaMay be done under local anesthesia
DisadvantagesDisadvantages Possibility of extrusion (occurred in 1/8 pts)Possibility of extrusion (occurred in 1/8 pts) Requires septal mucosa (not discussed)Requires septal mucosa (not discussed)
Goldenberg, Danino, Netzer, Joachims. Oto HNS, Vol. 122 (6). pp. 794-97.
PlastiporePlastipore
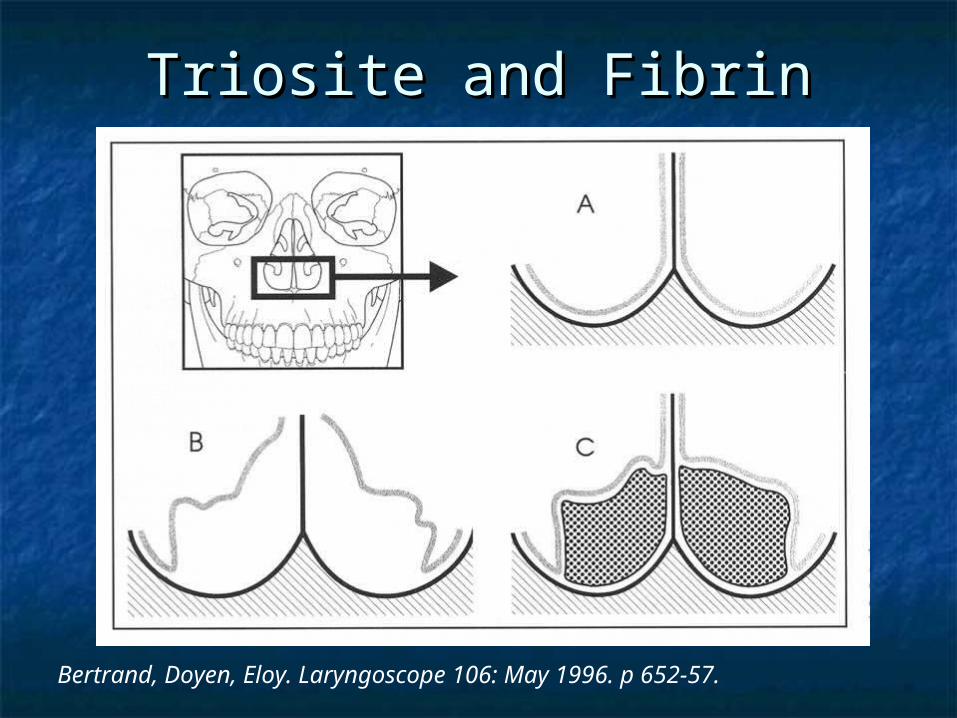
Volume Reduction (cont)Volume Reduction (cont) Triosite and FibrinTriosite and Fibrin
Triosite (60% hydroxyapetite, 40% calcium triphosphate) Triosite (60% hydroxyapetite, 40% calcium triphosphate) mixed with Fibrin 1:1.mixed with Fibrin 1:1.
Deglove the labial vestibuleDeglove the labial vestibule Elevate periosteum of the floor posteriorly to the end of Elevate periosteum of the floor posteriorly to the end of
the hard palate, extend medially onto the septum.the hard palate, extend medially onto the septum. Insert Triosite & Fibrin mixture (~3.3g per side)Insert Triosite & Fibrin mixture (~3.3g per side)
AdvantagesAdvantages Good to excellent result (7/9 patients)Good to excellent result (7/9 patients) Material can be molded easily Material can be molded easily
DisadvantagesDisadvantages Leakage of material (4/9 patients)Leakage of material (4/9 patients) Infection of material (3/9 patients)Infection of material (3/9 patients) Potential damage to lacrimal systemPotential damage to lacrimal system
Bertrand, Doyen, Eloy. Laryngoscope 106: May 1996. p 652-57.
Triosite and FibrinTriosite and Fibrin
Bertrand, Doyen, Eloy. Laryngoscope 106: May 1996. p 652-57.

Triosite and FibrinTriosite and Fibrin
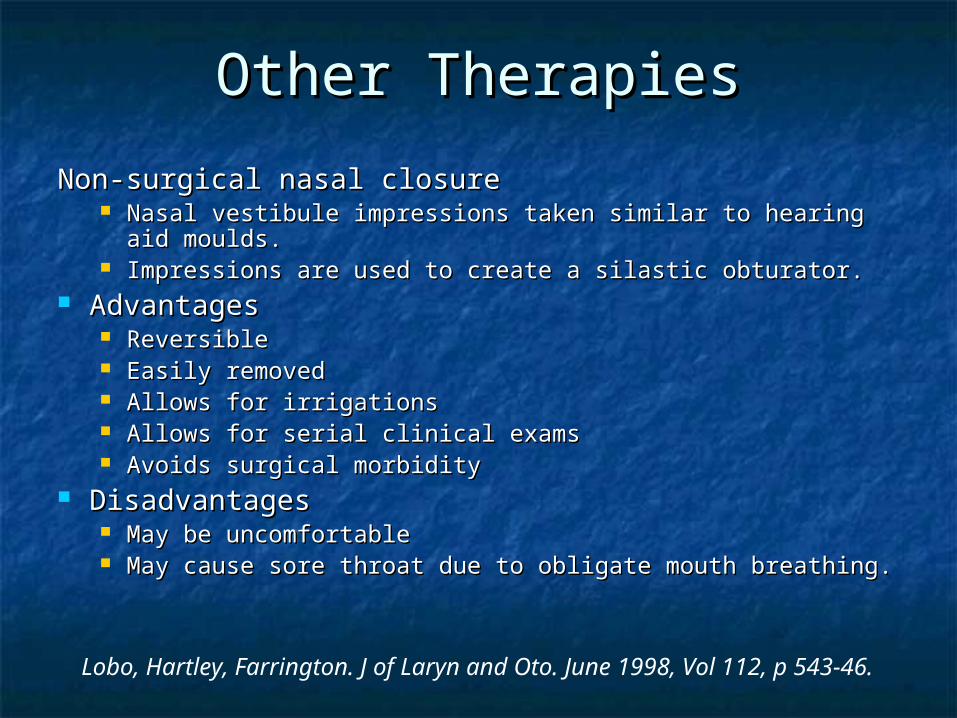
Other TherapiesOther Therapies
Non-surgical nasal closureNon-surgical nasal closure Nasal vestibule impressions taken similar to hearing aid Nasal vestibule impressions taken similar to hearing aid
moulds.moulds. Impressions are used to create a silastic obturator.Impressions are used to create a silastic obturator.
AdvantagesAdvantages ReversibleReversible Easily removedEasily removed Allows for irrigationsAllows for irrigations Allows for serial clinical examsAllows for serial clinical exams Avoids surgical morbidity Avoids surgical morbidity
DisadvantagesDisadvantages May be uncomfortableMay be uncomfortable May cause sore throat due to obligate mouth breathing.May cause sore throat due to obligate mouth breathing.
Lobo, Hartley, Farrington. J of Laryn and Oto. June 1998, Vol 112, p 543-46.
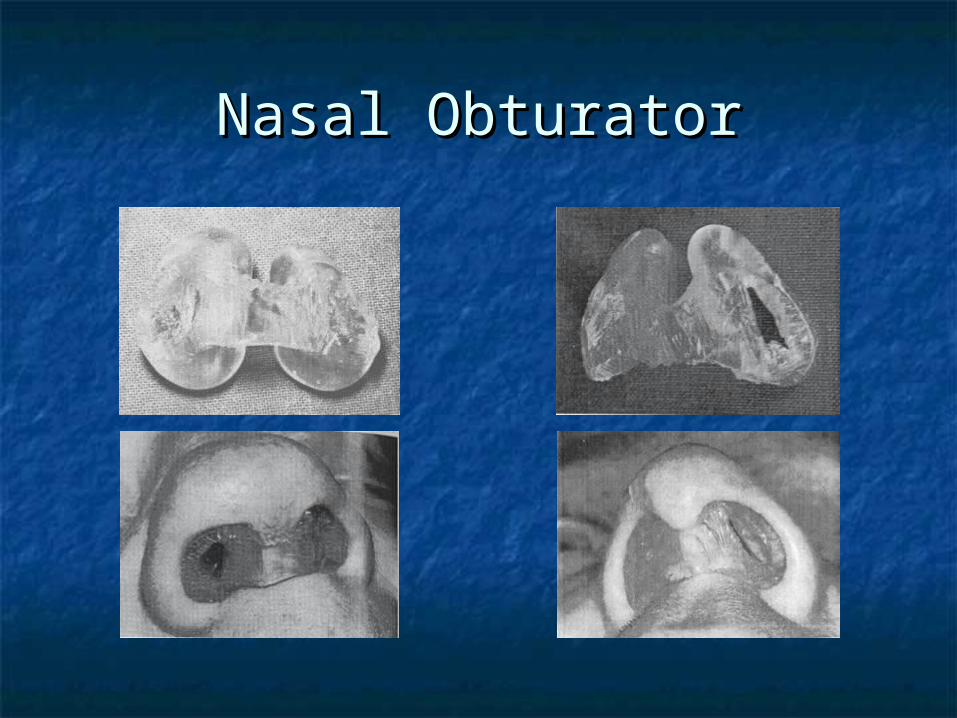
Nasal ObturatorNasal Obturator
Other TherapiesOther Therapies
Other ImplantsOther Implants AcrylicAcrylic SiliconeSilicone TeflonTeflon SilasticSilastic BoplantBoplant
DenervationDenervation Cervical sympathectomy (Bertein)Cervical sympathectomy (Bertein) Stellate ganglion block (Bahl)Stellate ganglion block (Bahl) Sphenopalatine ganglion block (Girgis)Sphenopalatine ganglion block (Girgis) Parasympathectomy, i.e. GSPN section (Krmptotic)Parasympathectomy, i.e. GSPN section (Krmptotic)
Salivary IrrigationSalivary Irrigation Involves reimplantation of parotid duct into the maxillary sinusInvolves reimplantation of parotid duct into the maxillary sinus
AccupunctureAccupuncture TimeTime
Disease often resolves spontaneously after age 40Disease often resolves spontaneously after age 40
BibliographyBibliography Lobo, Hartley, Farrington. “Closure of the nasal vestibule in Lobo, Hartley, Farrington. “Closure of the nasal vestibule in
atrophic rhinitis – a new non-surgical technique.” atrophic rhinitis – a new non-surgical technique.” The Journal of The Journal of Laryngology and OtologyLaryngology and Otology. June 1998, Vol. 112, pp. 543-46.. June 1998, Vol. 112, pp. 543-46.
Moore, Kern. “Atrophic Rhinitis: A Review of 242 cases.” Moore, Kern. “Atrophic Rhinitis: A Review of 242 cases.” American American Journal of RhinologyJournal of Rhinology. November-December 2001, Vol. 15, No. 6, p . November-December 2001, Vol. 15, No. 6, p 355-61.355-61.
Shehata. “Atrophic Rhinitis.” Shehata. “Atrophic Rhinitis.” American Journal of OtolaryngologyAmerican Journal of Otolaryngology, , Vol. 17, No. 2. March-April, 1996: pp 81-86.Vol. 17, No. 2. March-April, 1996: pp 81-86.
Chand, MacArthur. “Primary atrophic rhinitis: A summary of four Chand, MacArthur. “Primary atrophic rhinitis: A summary of four cases and review of the literature.” Otolaryngology – Head and cases and review of the literature.” Otolaryngology – Head and Neck Surgery. Vol. 116, No. 4: pp 554-57.Neck Surgery. Vol. 116, No. 4: pp 554-57.
Bertrand, Doyen, Eloy. “Triosite Implants and Fibrin Glue in the Bertrand, Doyen, Eloy. “Triosite Implants and Fibrin Glue in the Treatment of Atrophic Rhinitis: Technique and Results.” Treatment of Atrophic Rhinitis: Technique and Results.” Laryngoscope (106): May 1996: pp 652-57.Laryngoscope (106): May 1996: pp 652-57.
Goldenberg, Danino, Netzer, Joachims. “Plastipore implants in the Goldenberg, Danino, Netzer, Joachims. “Plastipore implants in the surgical treatment of atrophic rhinitis: Technique and results.” surgical treatment of atrophic rhinitis: Technique and results.” Otolaryngology Head and Neck Surgery. Vol 122 No 6: pp 794-97.Otolaryngology Head and Neck Surgery. Vol 122 No 6: pp 794-97.
Watson, Spencer. Watson, Spencer. Diseases of the nose and its accessory cavitiesDiseases of the nose and its accessory cavities. . London: 1875.London: 1875.
El Kholy, Habib, Abdel-Monem, Safia. “Septal mucoperichondrial El Kholy, Habib, Abdel-Monem, Safia. “Septal mucoperichondrial flap for closure of nostril in atrophic rhinitis.” flap for closure of nostril in atrophic rhinitis.” RhinologyRhinology, 36, 202-, 36, 202-203, 1998.203, 1998.







![Allergies from A to Z.ppt - Wellness Warriors · Definition of rhinitis: ... Atrophic WegenerWegeners’s , sarcoid. ... Allergies from A to Z.ppt [Compatibility Mode] Author:](https://static.fdocuments.in/doc/165x107/5acf46a47f8b9a56098cdb13/allergies-from-a-to-zppt-wellness-warriors-of-rhinitis-atrophic-wegenerwegenerss.jpg)








