RESEARCH ARTICLE Quality Improvement Initiative to ...€¦ · RESEARCH ARTICLE Quality Improvement...
10
RESEARCH ARTICLE Quality Improvement Initiative to Increase the Use of Nasogastric Hydration in Infants With Bronchiolitis Mythili Srinivasan, MD, PhD, a Cassandra Pruitt, MD, a Erin Casey, MD, b Keerat Dhaliwal, MD, a Cori DeSanto, MD, a Richard Markus, MD, c Ayelet Rosen, MD a ABSTRACT BACKGROUND AND OBJECTIVES: Intravenous (IV) hydration is used primarily in children with bronchiolitis at our institution. Because nasogastric (NG) hydration can provide better nutrition, the goal of our quality improvement (QI) initiative was to increase the rate of NG hydration in eligible children 1 to 23 months old with bronchiolitis by 20% over 6 months. METHODS: We used Plan-Do-Study-Act cycles to increase the use of NG hydration in eligible children. Interventions included educational and system-based changes and sharing parental feedback with providers. Chart reviews were performed to identify the rates of NG hydration, which were plotted over time in a statistical process control p chart. The balancing measure was the rate of complications in children with NG versus IV hydration. RESULTS: Two hundred and ninety-three children who were hospitalized with bronchiolitis needed supplemental hydration during the QI initiative (January 2016–April 2016). Ninety-one children were candidates for NG hydration, and 53 (58%) received NG hydration. The rates of NG hydration increased from a baseline of 0% pre-QI bronchiolitis season (January 2015–April 2015) to 58% during the initiative. There was no aspiration and no accidental placement of the NG tube into a child’s airway. Nine patients (17%) in the NG group had a progression of disease requiring nil per os status, and 6 of these were transferred to the PICU whereas none of those in the IV group were transferred to the PICU. Post-QI initiative, the majority of nurses (63%) and physicians (95%) stated that they are more likely to consider NG hydration in children with bronchiolitis. CONCLUSIONS: We successfully increased the rates of NG hydration in eligible children with bronchiolitis by using educational and system-based interventions. a Department of Pediatrics, Washington University, St Louis, Missouri; b Department of Pediatrics, Stony Brook University, New York, New York; and c Department of Pediatrics, University of Texas Southwestern Medical School, Dallas, Texas www.hospitalpediatrics.org DOI:https://doi.org/10.1542/hpeds.2016-0160 Copyright © 2017 by the American Academy of Pediatrics Address correspondence to Mythili Srinivasan, MD, PhD, Department of Pediatrics, Washington University School of Medicine and St Louis Children’ s Hospital, One Children’ s Place, NWT 9113, St Louis, MO 63110. E-mail: [email protected] HOSPITAL PEDIATRICS (ISSN Numbers: Print, 2154-1663; Online, 2154-1671). FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose. FUNDING: The use of Research Electronic Data Capture (REDCap) was supported by the National Institutes of Health Clinical and Translational Science Award grant UL1 TR000448 from the National Institute of Health and the Siteman Comprehensive Cancer Center and NCI Cancer Center Support grant P30 CA091842. Funded by the National Institutes of Health (NIH). POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose. Dr Srinivasan is the principal investigator and conceptualized and designed the study, implemented the quality improvement (QI) initiative and interventions, designed the data collection instrument and surveys, coordinated and supervised data collection, collected and analyzed the data, drafted the initial manuscript, and critically reviewed the manuscript; Dr Rosen participated in the study design, development of data collection instrument and data collection, implementation of the QI initiative and interventions, data analysis, drafting of the initial manuscript, and critical review of the manuscript; Dr Pruitt participated in the study design, implementation of the QI initiative and interventions, development of data collection instrument and data collection, and critical review of the manuscript; Dr Casey participated in the study design, implementation of the QI initiative and interventions, and critical review of the manuscript; Drs Dhaliwal, Markus, and DeSanto participated in the implementation of the QI initiative and interventions, collected data, and critically reviewed the manuscript; and all authors approved the final manuscript as submitted. 436 SRINIVASAN et al by guest on May 23, 2020 http://hosppeds.aappublications.org/ Downloaded from
Transcript of RESEARCH ARTICLE Quality Improvement Initiative to ...€¦ · RESEARCH ARTICLE Quality Improvement...

RESEARCH ARTICLE
Quality Improvement Initiative to Increase theUse of Nasogastric Hydration in InfantsWith BronchiolitisMythili Srinivasan, MD, PhD,a Cassandra Pruitt, MD,a Erin Casey, MD,b Keerat Dhaliwal, MD,a Cori DeSanto, MD,a Richard Markus, MD,c Ayelet Rosen, MDa
A B S T R A C TBACKGROUND AND OBJECTIVES: Intravenous (IV) hydration is used primarily in children with bronchiolitisat our institution. Because nasogastric (NG) hydration can provide better nutrition, the goal of our qualityimprovement (QI) initiative was to increase the rate of NG hydration in eligible children 1 to 23 months old withbronchiolitis by 20% over 6 months.
METHODS: We used Plan-Do-Study-Act cycles to increase the use of NG hydration in eligible children.Interventions included educational and system-based changes and sharing parental feedback with providers. Chartreviews were performed to identify the rates of NG hydration, which were plotted over time in a statistical processcontrol p chart. The balancing measure was the rate of complications in children with NG versus IV hydration.
RESULTS: Two hundred and ninety-three children who were hospitalized with bronchiolitis needed supplementalhydration during the QI initiative (January 2016–April 2016). Ninety-one children were candidates for NG hydration,and 53 (58%) received NG hydration. The rates of NG hydration increased from a baseline of 0% pre-QI bronchiolitisseason (January 2015–April 2015) to 58% during the initiative. There was no aspiration and no accidental placementof the NG tube into a child’s airway. Nine patients (17%) in the NG group had a progression of disease requiring nilper os status, and 6 of these were transferred to the PICU whereas none of those in the IV group were transferred tothe PICU. Post-QI initiative, the majority of nurses (63%) and physicians (95%) stated that they are more likely toconsider NG hydration in children with bronchiolitis.
CONCLUSIONS: We successfully increased the rates of NG hydration in eligible children with bronchiolitis byusing educational and system-based interventions.
aDepartment ofPediatrics, Washington
University, St Louis,Missouri; bDepartment ofPediatrics, Stony Brook
University, New York, NewYork; and cDepartment ofPediatrics, University of
Texas SouthwesternMedical School, Dallas,
Texas
www.hospitalpediatrics.orgDOI:https://doi.org/10.1542/hpeds.2016-0160Copyright © 2017 by the American Academy of Pediatrics
Address correspondence to Mythili Srinivasan, MD, PhD, Department of Pediatrics, Washington University School of Medicine and StLouis Children’s Hospital, One Children’s Place, NWT 9113, St Louis, MO 63110. E-mail: [email protected]
HOSPITAL PEDIATRICS (ISSN Numbers: Print, 2154-1663; Online, 2154-1671).
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: The use of Research Electronic Data Capture (REDCap) was supported by the National Institutes of Health Clinical andTranslational Science Award grant UL1 TR000448 from the National Institute of Health and the Siteman Comprehensive Cancer Centerand NCI Cancer Center Support grant P30 CA091842. Funded by the National Institutes of Health (NIH).
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Dr Srinivasan is the principal investigator and conceptualized and designed the study, implemented the quality improvement (QI)initiative and interventions, designed the data collection instrument and surveys, coordinated and supervised data collection, collectedand analyzed the data, drafted the initial manuscript, and critically reviewed the manuscript; Dr Rosen participated in the study design,development of data collection instrument and data collection, implementation of the QI initiative and interventions, data analysis,drafting of the initial manuscript, and critical review of the manuscript; Dr Pruitt participated in the study design, implementation of theQI initiative and interventions, development of data collection instrument and data collection, and critical review of the manuscript;Dr Casey participated in the study design, implementation of the QI initiative and interventions, and critical review of the manuscript;Drs Dhaliwal, Markus, and DeSanto participated in the implementation of the QI initiative and interventions, collected data, and criticallyreviewed the manuscript; and all authors approved the final manuscript as submitted.
436 SRINIVASAN et al
by guest on May 23, 2020http://hosppeds.aappublications.org/Downloaded from

Bronchiolitis is the leading cause ofhospitalization for children in their firstyear of life.1,2 A recent study showed that53% of children who were hospitalized withbronchiolitis required intravenous (IV) fluids.3
The American Academy of Pediatrics (AAP)and our hospital bronchiolitis guidelinesrecommend that fluids be administered viathe IV or nasogastric (NG) route in childrenwith bronchiolitis who cannot maintain oralhydration.1 Despite these recommendations,IV hydration is the modality used in childrenwith bronchiolitis at our institution.
Likewise, NG hydration is not routinely usedin North America in infants with dehydration.4
In a survey of emergency physiciansregarding hydration practices for childrenwith gastroenteritis, only 0.7% of providerspreferred NG hydration.4 NG hydration is,however, used in infants with bronchiolitis inmany countries, including Australia, NewZealand, Israel, and countries throughoutEurope.5–7 Studies comparing IV and NGhydration in children with bronchiolitis haveshown NG hydration to be well tolerated, safe,and have no increased risk of complicationswhen compared with IV hydration.2,8,9
Breast milk or formula can be offered viaNG tube rather than the less nutritiousfluids that are commonly given via IV.Providing adequate nutrition to childrenwho are ill is important and can influencethe outcomes.10–13 Accordingly, we soughtto increase the use of NG hydration ineligible children who are admitted withbronchiolitis. Initial discussions withproviders at our hospital suggested that thepreferential use of IV hydration was due tolack of knowledge about NG hydration. Webelieved that educational interventions thatuse quality improvement (QI) methodologywould be successful in changing thehospital culture. Thus, the aim of our QIinitiative was to use educational andsystem-based interventions to increase theuse of NG hydration in eligible children1 to 23 months old with bronchiolitis anddehydration by 20% in 6 months.
METHODSContext
This initiative was conducted in theemergency department (ED) and inpatient
units at a 280-bed, tertiary care,free-standing children’s hospital with∼51 000 annual ED visits and 11 000 annualadmissions. Stakeholders for this QIinitiative included pediatric hospitalists,pediatric emergency medicine (PEM)physicians, nurses, and residents. Thepartnership between PEM physicians andhospitalists (who also staff the ED)facilitated the implementation of thishospitalist-led QI initiative. The bronchiolitispatients were admitted to 2 generalpediatric inpatient units or the pulmonaryunit, and any overflow was admitted tosurgical or neurology units. Inpatient teamsconsisted of a hospitalist or subspecialtyattending, a senior resident, and 2 or3 interns and/or nurse practitioners.
Survey of Stakeholders
Our initial step in this initiative was tosurvey stakeholders to understand theirattitudes and concerns regarding NGhydration. Surveys were administered pre-QIvia e-mail with a Web link to SurveyMonkey(SurveyMonkey Inc, Palo Alto, CA), and apaper version was distributed during staffand division meetings from November18, 2015 to December 21, 2015. Surveyresponses were anonymous and not linkedto e-mail addresses. We also surveyedstakeholders post-QI initiative (May 10,2016–June 20, 2016).
Interventions
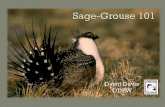
The study team included 3 pediatrichospitalists, a chief resident, and 3 pediatricresidents. Key drivers were identified bydiscussions with stakeholders at meetingsand analysis of information obtained bystakeholder surveys (Fig 1). We alsodiscussed with stakeholders the patienteligibility criteria for NG hydration based onthe studies by Oakley et al2 and modifiedthe criteria based on stakeholder feedback.We performed 3 Plan-Do-Study-Act (PDSA)cycles with a 3-week period at the end of thelast cycle to evaluate sustainability withoutfurther intervention.
Provider Education
Educational interventions were conductedon the basis of information gathered fromaforementioned meetings and survey data.Study team members attended PEM andhospitalist division meetings, residentconferences, and nursing staff meetings toprovide initial education, and informationwas sent via e-mail to providers who did notattend the meetings. Information wasfurther disseminated by posters, whichwere placed in key locations in the hospital,and pocket cards (Supplemental Figs 4and 5). These included information aboutNG hydration, NG placement protocols,parental talking points, and indications ofeligibility for NG hydration. To supplement
FIGURE 1 Key driver diagram.
HOSPITAL PEDIATRICS Volume 7, Issue 8, August 2017 437
by guest on May 23, 2020http://hosppeds.aappublications.org/Downloaded from

discussions with providers, parents weregiven a parental information sheet that wascreated in conjunction with the hospital’sfamily resource center (SupplementalFig 6). Important feedback regardingaccidental NG tube dislodgement wasreceived during the first 2 weeks of theinitiative. To address this, posters depictingthe proper NG tube-taping technique werecreated, presented to nursing staff, andplaced in key locations.
Ongoing provider education, reinforcement,and encouragement was provided by teammembers, who walked through the ED andinpatient units 2 to 3 times a week and metindividually and in groups to answer anyquestions about NG hydration and obtainverbal feedback from nurses and physicians.
Systems Based Changes
An NG feeding-tube order set was added tothe ED order sets. The ED had to be stockedwith NG feeding-tube supplies and pumps.
Sharing Results of PDSA Cycle
We shared run charts of the rates of NGhydration with all stakeholders after eachPDSA cycle. Laminated posters of the runcharts were placed in key locations.
Sharing Parent Feedback
Parental feedback data from weeks 4 to8 were presented to stakeholders duringweek 8 of the initiative. A laminated postershowing a graphic of the results was placedin key locations.
Study of the Interventions
Baseline Data
The baseline rates of NG hydrationwere obtained by analyzing data frombronchiolitis admissions from January 5,2015 to April 18, 2015.
QI Initiative
Data were collected from January 5, 2016 toApril 18, 2016, by chart reviews of childrenwho were admitted with bronchiolitis andreceived IV or NG hydration to determine therates of NG hydration and identifycomplications.
We queried our inpatient clinical database(KIDDOS) for all children 1 to 23 months oldwho were admitted with an InternationalClassification of Diseases, 10th Revision
diagnosis of acute bronchiolitis (J21.9,J21.0, J21.1, J21.8, J20.9, J11.1), respiratorydistress (J80, R06.00), wheezing (R06.2,J98.8), respiratory syncytial virus (RSV)related infections (B97.4, J12.1, J20.5, B97.4,J02.9), and viral pneumonia (J12.9, J12.89).KIDDOS provided information on patientdemographics, whether a patient received IVfluids or was tube fed, admitting anddischarge diagnoses, and length of stay(LOS). Total charge data were obtainedfrom our hospital’s Health InformationManagement System, which is anadministrative database. ResearchElectronic Data Capture (REDCap), a secure,Web-based, data-capture application hostedat Washington University in St Louis, wasused for data collection and management.14
Six study team members reviewed thecharts, and the team leader audited 20%of the charts reviewed by each studymember. Chart reviews provided data onclinical presentation, hospital course, anddischarge diagnosis. As a measure ofculture change, we queried the charts forany documentation of consideration ofNG hydration. After the chart reviews,13 patients were excluded because theywere not admitted for bronchiolitis. Otherexclusion criteria are listed in Fig 2. A
patient was excluded because of respiratorydistress only if an independent reviewby 2 team members found physiciandocumentation in the chart that the patientwas in respiratory distress.
Gathering Parental Feedback
Parental feedback was obtained from theparents of children who received hydrationvia IV, NG, or both during weeks 4 to12 of the initiative. Feedback forms lackingpatient identifiers were given to the parentsto complete at the end of their children’shospitalization. We asked about theirperceptions of pain caused by IV or NGplacement in their children, overallsatisfaction with the care received duringthe hospitalization, and their preferencesfor IV or NG hydration during any futurehospitalizations. Because of the limitedavailability of team members, feedbackregarding IV hydration came from theparents of any patient with bronchiolitiswho received IV hydration, regardless ofwhether they were eligible for NG hydration.
Measures
Our primary outcome measure was the rateof NG hydration in eligible children whowere admitted with bronchiolitis and
FIGURE 2 A summary of the study population. Some patients had .1 disqualifying criteria.“Other” includes concerns about nasal hemangioma, a difficult airway, socialconcerns, or multiple laboratories obtained for concerns other than bronchiolitis. G-tube, gastric tube.
438 SRINIVASAN et al
by guest on May 23, 2020http://hosppeds.aappublications.org/Downloaded from

dehydration. The balancing measure wasthe rate of complications in children withNG versus IV hydration, which was assessedby chart reviews. Complications weredefined as outcomes that potentially couldbe attributed to NG hydration, such asaspiration, epistaxis, accidental placementof the NG tube in the airway, or worsening ofdisease severity. Change in hospital cultureregarding NG hydration after the QI initiativewas assessed by the post-QI surveydescribed above.
Data Analysis
Chart review data were used to calculatethe weekly rates of NG hydration in eligiblechildren, which were plotted over time in astatistical process control p chart by using
established rules for identifying specialcause variation.15,16 We compared parentalfeedback, survey responses, and thecharacteristics of patients who receivedNG or IV hydration. Categorical variableswere analyzed with exact x2 tests ofindependence and continuous variableswith the Kruskal-Wallis test. All analyseswere done with SAS/STAT software Version9.3 of the SAS System for Windows (SASInstitute Inc; Cary, NC).
Ethical Considerations
The Washington University InstitutionalReview Board determined that this QIinitiative was exempt from human-subjectreview. Institutional Review Board approvalwas obtained for administering the parental
feedback and provider surveys. Treatmentcourse (including NG versus IV hydration)was guided by provider discretion andshared decision-making between parentsand providers throughout the ED andinpatient hospital stays.
RESULTSInitial Survey of Stakeholders Pre-QI
One hundred and fifty-one physicians and166 nurses were surveyed with responserates of 75% and 52%, respectively(Supplemental Table 3). Before the QIinitiative, only 20% of physicians and 13% ofnurses had used or placed NG tubes forhydration in children with bronchiolitis, and12% of physicians and nurses preferred NGhydration (Supplemental Table 4). The
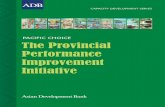
FIGURE 3 Weeks T1 to T15 correspond to data collection in 2015 (January 5–April 18). The break in the x-axis indicates the break in time between2015 and the 2016 data collection period. The 2016 data collection period was from January 5, 2016 to April 18, 2016. Each PDSA cyclewas 4 weeks long with a 3-week sustainment phase at the end of the last cycle. CL, control limit; LCL, lower control limit; UCL, uppercontrol limit.
HOSPITAL PEDIATRICS Volume 7, Issue 8, August 2017 439
by guest on May 23, 2020http://hosppeds.aappublications.org/Downloaded from

majority of providers did not know thatNG hydration was an option in the hospitalguidelines or in the AAP bronchiolitisguidelines, and they were concerned aboutparental resistance to NG hydration.
Baseline Data
There were 357 patients admitted forbronchiolitis or RSV infection from January5, 2015 to April 18, 2015. Of these,221 patients (62%) received supplementalhydration. Seventeen patients had an NGtube or a nasojejunal tube placed in thePICU for enteral feeding after intubation forrespiratory distress. No NG tube was placedfor hydration.
QI Initiative
Four hundred and fifty patients 1 to23 months old were admitted forbronchiolitis, RSV infection, or first episodeof wheezing from January 5, 2016 to April18, 2016. Of these, 293 patients (65%)needed supplemental hydration. Of those,202 (69%) were excluded because of thereasons listed in Fig 2. The final analysisincluded the 91 eligible patients (31%) whoreceived hydration via an IV, NG, or both. Ofthese 91 patients, 53 (58%) received NGhydration. Fifteen patients who received NGhydration eventually needed IV placementbecause of the reasons listed in Fig 2. Of the38 patients who received only IV hydration,there was documentation that NG hydrationwas considered in 20 (53%). Nine families(10%) refused NG hydration afterdiscussions with providers, and thenreceived IV hydration.
The primary outcome measure (the rates ofNG hydration) increased from a baseline of0% in 2015 to 58% during the entire periodof the QI initiative (Fig 3). The initialeducational interventions and system-based changes resulted in a significantincrease in the rates of NG hydration .20%,which was our target. No special causevariation that would result in centerlineshifts was noted during subsequentinterventions.
Parental feedback was obtained duringweeks 4 to 12 of the initiative (Table 1).There was no significant difference inparental perception of the pain caused by IVor NG tube placement in their children. The
majority of parents whose children receivedeither IV or NG hydration were very satisfiedwith the care they received, and there wasno significant difference in the overallsatisfaction between the groups. Themajority of parents (90%) of children whoreceived both IV and NG hydration were alsovery satisfied with the care received, andmost (80%) responded that they wouldprefer that their children receive NGhydration if they were hospitalized again.
Balancing Measures
There was no aspiration, death, or need forintubation in patients who received NG or IVhydration. Epistaxis was not noted in anyinfant who received NG hydration. Of the53 NG tubes, 17 (32%) were displaced orremoved (accidental displacement orremoval due to the patient having emesis),and 5 (9%) were replaced with IVs. Of 53 IVs,27 (51%) were displaced or removed(accidental displacement or removal due toinfiltration or a malfunctioning IV), and12 (23%) were replaced with IVs. Therewas no significant difference in ratesof IV versus NG dislodgement and/orremoval (P 5 .36).
We compared the characteristics of childrenwho initially received IV or NG hydration(Table 2). The NG group included all thechildren who started out with NG tubes,some of whom later required IVs. Children
in the NG group were significantly younger,and a greater proportion was white whencompared with those in the IV group. Thegroups had no significant differences in sex,presenting symptoms and examinations,viruses detected, day of illness atpresentation, discharge diagnosis, totalcharges, or LOS.
Nine patients (17%) in the NG group had aprogression of disease requiring nil peros status and IV placement for hydration.Two of those patients resumed NG hydrationafter an improvement in respiratorysymptoms was observed. Six of thosepatients were transferred to the PICU,5 of whom received noninvasive ventilation.None of the patients in the IV group receivednoninvasive ventilation or were transferredto the PICU. There was a significantdifference (P 5 .04) in the number ofpatients who were transferred to the PICUin the NG group when compared with the IVgroup (Table 1).
The median age of children in the NG groupwho were transferred to the PICU was2 months old. Their median day of illness atthe time of hospitalization was 2 days, andthe median day of illness at the time oftransfer to the PICU was 5 days. All wereRSV-positive and were born at .36 weeks’gestation. All except 2 infants werepreviously healthy. There was no reported
TABLE 1 Parental Feedback
IV, N (%) NG, N (%) P
No. of childrena 46 30
How was your child when the IV or NG was placed?b .65
Relaxed and comfortable 7 (13) 4 (10)
Mild pain, discomfort 17 (30) 16 (40)
Moderate pain, discomfort 20 (36) 8 (20)
Severe pain, discomfort 7 (13) 6 (15)
How satisfied are you with the care you received?c .15
Very satisfied 39 (85) 27 (90)
Somewhat satisfied 7 (15) 2 (7)
Not satisfied 0 0
No response 0 1 (3)
a Indicates the number of children who had only IV or only NG.b Was asked of all parents whose children had an IV, NG, or both. Thus, percentages were calculated withthe denominator being the total number of patients with IV or NG, including those with both IV and NG(N 5 10).
c Response is from only the parents of children who had either NG or IV. Response from parents of childrenwith both IV and NG are described in the article’s “Results” section.
440 SRINIVASAN et al
by guest on May 23, 2020http://hosppeds.aappublications.org/Downloaded from

concern for aspiration in any of theseinfants, and none received IV antibioticsduring their hospitalization.
Final Survey of Stakeholders Post-QI
The post-QI survey of stakeholders showeda significant increase (P , .001) inexperience with NG use and placement and
knowledge regarding AAP and hospitalbronchiolitis guidelines about NG hydration(Supplemental Table 4). There was asignificant increase (P , .001) in thenumber of physicians (78%) and nurses(64%) who reported that they had used orplaced an NG tube for hydration after theinitiative. There was a 3.5-fold increase in
the proportion of physicians who reportedthey would choose NG hydration as theirpreferred method, and there was asignificant reduction in the proportion ofphysicians and nurses who stated that theywould choose IV hydration (SupplementalTable 4). Post-QI, 95% of physicians and63% of nurses responded they aremore likely to consider NG hydrationwhen appropriate in children withbronchiolitis.
DISCUSSION
Our QI interventions were successful inincreasing overall rates of NG hydration ineligible children from zero at baseline to58%, which was well beyond our goal of20%. In addition, our survey results showthat the educational interventions weresuccessful in increasing the knowledge ofproviders regarding NG hydration optionsin the AAP and hospital bronchiolitisguidelines. Our initiative did cause achange in hospital culture regarding NGhydration as indicated by the followingsurvey results: 95% of physicians and 63%of nurses answered in the post-QI surveythat they are more likely to consider NGhydration when appropriate in childrenwith bronchiolitis after participating inthe QI initiative. We effected a greaterchange in physician preferences for NGhydration when compared with nursepreferences, as evidenced by the 3.5-foldincrease in physician preference for NGhydration post-QI, which was not seenamong the nurses. Nurses in ourinstitution are highly proficient with IVplacement and are not as used to NG tubeplacement. We hope that continuededucation in addressing nursing concernsabout NG tube placement along withincreased familiarity with NG tubeplacement over a longer period of timemay alleviate nursing concerns andchange their preferences.
This is the first study to date to provide dataon parental perceptions regarding NG andIV hydration in bronchiolitis. Parentalfeedback was encouraging because therewas no difference in parental perception ofpain regarding NG placement versus IVplacement. Moreover, 80% of parents
TABLE 2 Characteristics, Clinical Presentation, and Hospital Course of IV and NG GroupPatients
IV Group NG group PN 5 38 (%) N 5 53 (%)
Age, mo, median (IQR 25th–75th) 8 (5–13) 4 (2–7) ,.001
Sex
Female 16 (42) 31 (58) .12
Ethnicity .001
White 12 (32) 31 (58) N/A
African American 22 (58) 14 (26) N/A
Unknown 4 (11) 4 (8) N/A
Virus detected .38
RSV 30 (79) 44 (83) N/A
Non-RSV viral infection 8 (21) 7 (13) N/A
Presenting symptoms
Respiratory 38 (100) 53 (100) N/A
Emesis 13 (34) 15 (28) .55
Dehydration 33 (87) 41 (77) .25
Presenting examination
Rhinorrhea 25 (66) 26 (49) .11
Wheezing 16 (42) 19 (36) .55
Tachypnea 18 (47) 23 (43) .71
Retractions 30 (79) 44 (83) .62
Oxygen requirement at time of admission 13 (34) 13 (25) .70
Hospital course
Oxygen by NC 20 (53) 26 (49) .41
IV antibiotics 3 (8) 3 (6) .69
Albuterol treatment 15 (39) 13 (25) .17
Transferred to PICU 0 (0) 6 (11) .04
Noninvasive ventilation 0 (0) 5 (9) .07
Discharge diagnosis
Bronchiolitis 37 (97) 50 (94) .64
Dehydration 2 (5) 11 (21) .07
Other 1 (3) 8 (15) .07
Total charges, $, median (IQR) 7189 (5417–9565) 7090 (4170–9884) .78
LOS, h, median (IQR)
ED LOS 5 (4–7) 5 (4–6) .26
Inpatient LOS 41 (26–88) 59 (27–93) .34
Total LOS 48 (32–92) 63 (34–97) .32
Day of illness at presentation, median (IQR) 5 (4–7) 5 (4–6) .88
IQR, interquartile range; N/A, not applicable; NC, nasal cannula.
HOSPITAL PEDIATRICS Volume 7, Issue 8, August 2017 441
by guest on May 23, 2020http://hosppeds.aappublications.org/Downloaded from

whose children received both NG and IVhydration stated they would chooseNG hydration if their children werehospitalized again.
There was no aspiration noted in anypatient with an NG or IV, nor was there anyaccidental placement of an NG tube into theairway, which is similar to other studiescomparing IV and NG hydration. A large,randomized controlled trial did not showany significant difference in rates of ICUadmission, need for ventilator support,duration of oxygen therapy, or LOS betweeninfants receiving IV versus NG hydration.2
A retrospective cohort study of infants 0 to2 months old with bronchiolitis whoreceived IV or NG hydration also did notshow any significant difference in adverseevents (such as desaturations, apnea, orbradycardia) between the 2 groups.9 Thesame study showed a positive associationbetween IV hydration with ICU admissionsand the use of ventilator support.9 In ourstudy, 15 patients in the NG groupsubsequently needed IVs. Of these, 6 weretransferred to the PICU, whereas none of thepatients in the IV group were transferred tothe PICU. Given the younger mean age andearlier mean day of illness of this subgroup,their transfers were probably caused by theusual worsening of RSV disease at day 4 to5 of the illness rather than the result ofany sequelae from NG hydration (such asaspiration). Chart reviews of these childrenalso supported the worsening of respiratorydistress being related to natural diseaseprogression. However, possiblecomplications of NG cannot be excluded as acontributing factor. We will evaluate thisfurther during the next bronchiolitis seasonand track complications including PICUtransfers in patients with IV versus NGhydration. On the basis of our results, itis important to discuss the possibility ofIV in case of worsening of the disease,especially with families of youngerchildren who are earlier in their diseasecourse.
This QI initiative was conducted at a singlefree-standing children’s hospital and maynot be generalizable to other institutions.Additionally, data were collected over only1 RSV season, and the changes may not be
sustainable through future seasons.Nursing or physician biases may haveinfluenced parental choices of NG or IVhydration. The sustainability period was atthe tail end of bronchiolitis season, with feweligible patients. A true measure of thesustainability of the culture change can onlybe obtained during future bronchiolitisseasons. Lastly, parental feedback datawere limited by the small number ofchildren who received both IV and NGhydration.
CONCLUSIONS
The rates of NG hydration in eligible childrenwith bronchiolitis increased through ourinterventions focused on educational andsystem-based changes during this QIinitiative. We plan to measure the ratesof NG hydration in the next bronchiolitisseason to assess its sustainability. We arecurrently implementing these interventionsat our community hospitals within ourwider hospital network by sharingour educational tools, and we planto eventually partner with hospitalsacross the nation to increase the useof NG hydration in eligible children withbronchiolitis.
Acknowledgments
We sincerely thank Jack Baty, BA, forassistance with statistical analysis;Charles Samson, MD, for assistance withthe control chart; Angela Niesen, BS,MPH, for obtaining data from the HealthInformation Management System; JudithWilliams, RN, BSN; and Janet Provinse, BS,for obtaining data from the KIDDOSdatabase.
REFERENCES
1. Ralston SL, Lieberthal AS, Meissner HC,et al; American Academy of Pediatrics.Clinical practice guideline: the diagnosis,management, and prevention ofbronchiolitis. Pediatrics. 2014;134(5).Available at: www.pediatrics.org/cgi/content/full/134/5/e1474
2. Oakley E, Borland M, Neutze J, et al;Paediatric Research in EmergencyDepartments InternationalCollaborative (PREDICT). Nasogastrichydration versus intravenous hydration
for infants with bronchiolitis: arandomised trial. Lancet Respir Med.2013;1(2):113–120
3. Florin TA, Byczkowski T, Ruddy RM,Zorc JJ, Test M, Shah SS. Utilizationof nebulized 3% saline in infantshospitalized with bronchiolitis.J Pediatr. 2015;166(5):1168–1174.e2
4. Nunez J, Liu DR, Nager AL. Dehydrationtreatment practices among pediatrics-trained and non-pediatrics trainedemergency physicians. Pediatr EmergCare. 2012;28(4):322–328
5. Babl FE, Sheriff N, Neutze J, Borland M,Oakley E. Bronchiolitis management inpediatric emergency departments inAustralia and New Zealand: a PREDICTstudy. Pediatr Emerg Care. 2008;24(10):656–658
6. Mecklin M, Hesselmar B, Qvist E,Wennergren G, Korppi M. Diagnosis andtreatment of bronchiolitis in Finnish andSwedish children’s hospitals. ActaPaediatr. 2014;103(9):946–950
7. Brand PL, Vaessen-Verberne AA; DutchPaediatric Respiratory Society.Differences in management ofbronchiolitis between hospitals in TheNetherlands. Eur J Pediatr. 2000;159(5):343–347
8. Kugelman A, Raibin K, Dabbah H, et al.Intravenous fluids versus gastric-tubefeeding in hospitalized infants with viralbronchiolitis: a randomized, prospectivepilot study. J Pediatr. 2013;162(3):640–642.e1
9. Oakley E, Bata S, Rengasamy S, et al.Nasogastric hydration in infants withbronchiolitis less than 2 months of age.J Pediatr. 2016;178:241–245.e1
10. Johnson WB, Aderele WI, Gbadero DA.Host factors and acute lower respiratoryinfections in pre-school children. J TropPediatr. 1992;38(3):132–136
11. Briassoulis G, Zavras N, Hatzis T.Malnutrition, nutritional indices, andearly enteral feeding in criticallyill children. Nutrition. 2001;17(7–8):548–557
12. Weisgerber MC, Lye PS, Nugent M, et al.Relationship between caloric intake and
442 SRINIVASAN et al
by guest on May 23, 2020http://hosppeds.aappublications.org/Downloaded from

length of hospital stay for infants withbronchiolitis. Hosp Pediatr. 2013;3(1):24–30
13. Weisgerber MC, Lye PS, Li SH, et al.Factors predicting prolonged hospitalstay for infants with bronchiolitis.J Hosp Med. 2011;6(5):264–270
14. Harris PA, Taylor R, Thielke R, Payne J,Gonzalez N, Conde JG. Research electronicdata capture (REDCap)–a metadata-driven methodology and workflowprocess for providing translationalresearch informatics support. J BiomedInform. 2009;42(2):377–381
15. Benneyan JC. Use and interpretationof statistical quality control charts.Int J Qual Health Care. 1998;10(1):69–73
16. Benneyan JC, Lloyd RC, Plsek PE.Statistical process control as a tool forresearch and healthcare improvement.Qual Saf Health Care. 2003;12(6):458–464
HOSPITAL PEDIATRICS Volume 7, Issue 8, August 2017 443
by guest on May 23, 2020http://hosppeds.aappublications.org/Downloaded from

DOI: 10.1542/hpeds.2016-0160 originally published online July 5, 2017; 2017;7;436Hospital Pediatrics
Richard Markus and Ayelet RosenMythili Srinivasan, Cassandra Pruitt, Erin Casey, Keerat Dhaliwal, Cori DeSanto,
Infants With BronchiolitisQuality Improvement Initiative to Increase the Use of Nasogastric Hydration in
ServicesUpdated Information &
http://hosppeds.aappublications.org/content/7/8/436including high resolution figures, can be found at:
Supplementary Material
2016-0160.DCSupplementalhttp://hosppeds.aappublications.org/content/suppl/2017/07/04/hpeds.Supplementary material can be found at:
Referenceshttp://hosppeds.aappublications.org/content/7/8/436.full#ref-list-1This article cites 15 articles, 2 of which you can access for free at:
Subspecialty Collections
provement_subhttp://classic.hosppeds.aappublications.org/cgi/collection/quality_imQuality Improvementgy_subhttp://classic.hosppeds.aappublications.org/cgi/collection/pulmonoloPulmonologyis_subhttp://classic.hosppeds.aappublications.org/cgi/collection/bronchiolitBronchiolitision:practice_management_subhttp://classic.hosppeds.aappublications.org/cgi/collection/administratAdministration/Practice Managementfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
https://shop.aap.org/licensing-permissions/in its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.hosppeds.aappublications.org/content/reprintsInformation about ordering reprints can be found online:
by guest on May 23, 2020http://hosppeds.aappublications.org/Downloaded from

DOI: 10.1542/hpeds.2016-0160 originally published online July 5, 2017; 2017;7;436Hospital Pediatrics
Richard Markus and Ayelet RosenMythili Srinivasan, Cassandra Pruitt, Erin Casey, Keerat Dhaliwal, Cori DeSanto,
Infants With BronchiolitisQuality Improvement Initiative to Increase the Use of Nasogastric Hydration in
http://hosppeds.aappublications.org/content/7/8/436located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 2154-1663. Illinois, 60143. Copyright © 2017 by the American Academy of Pediatrics. All rights reserved. published, and trademarked by the American Academy of Pediatrics, 345 Park Avenue, Itasca,publication, it has been published continuously since 2012. Hospital Pediatrics is owned, Hospital Pediatrics is the official journal of the American Academy of Pediatrics. A monthly
by guest on May 23, 2020http://hosppeds.aappublications.org/Downloaded from